china’s healthcare system and...
TRANSCRIPT

CHINA’S HEALTHCARE SYSTEM
AND REFORMEdited by
Lawton Robert Burns and Gordon G. Liu

C:/ITOOLS/WMS/CUP-NEW/8947020/WORKINGFOLDER/BURNSL/9781107164598PRE.3D i [1–24] 17.11.2016 2:55PM
China’s Healthcare System and Reform
This volume provides a comprehensive review ofChina’s healthcare system and policy reforms in thecontext of the global economy. Following a value-chain framework, the 16 chapters cover the payers, theproviders, and the producers (manufacturers) inChina’s system. It also provides a detailed analysis ofthe historical development of China’s healthcaresystem, the current state of its broad reforms, and theuneasy balance between China’s market-drivenapproach and governmental regulation. Mostimportantly, it devotes considerable attention to themajor problems confronting China, including chronicillness, public health, and long-term care and economicsecurity for the elderly. Burns and Liu have assembledthe latest research from leading health economists andpolitical scientists, as well as senior public healthofficials and corporate executives, making this book anessential read for industry professionals, policy-makers, researchers, and students studyingcomparative health systems across the world.
lawton robert burns is James Joo-Jin KimProfessor in the Health Care Management Departmentat the Wharton School, Co-Director of the Roy &Diana Vagelos Program in Life Sciences andManagement at the University of Pennsylvania, andProgramme Leader for Healthcare Management at theIndian School of Business. He is co-editor of thepopular textbook Health Care Management:Organization Design and Behavior (2012) and theauthor of India’s Healthcare Industry (Cambridge,2014), The Business of Healthcare Innovation(Cambridge, 2012), and The Health Care Value Chain(2002).
gordon g. liu is a PKU Yangtze River ScholarProfessor of Economics at Peking University NationalSchool of Development and Director of PKU ChinaCenter for Health Economic Research (CCHER). Hesits on China’s State Council Health Reform Expert

C:/ITOOLS/WMS/CUP-NEW/8947020/WORKINGFOLDER/BURNSL/9781107164598PRE.3D ii [1–24] 17.11.2016 2:55PM
Advisory Committee and the UN Leadership Councilof Sustainable Development Solution Network(SDSN). He was the president of Chinese EconomistsSociety (CES) for 2004–2005. He has served asassociate editor for academic journals includingHealth Economics, China Economic Quarterly, andValue in Health.
C:/ITOOLS/WMS/CUP-NEW/8947020/WORKINGFOLDER/BURNSL/9781107164598PRE.3D iii [1–24] 17.11.2016 2:55PM
China’sHealthcareSystem andReform
Edited by
LAWTON ROBERT BURNSThe Wharton School, University of Pennsylvania
GORDON G. LIUPeking University National School of Development,Beijing

C:/ITOOLS/WMS/CUP-NEW/8947020/WORKINGFOLDER/BURNSL/9781107164598PRE.3D iv [1–24] 17.11.2016 2:55PM
University Printing House, Cambridge CB2 8BS, United Kingdom
One Liberty Plaza, 20th Floor, New York, NY 10006, USA
477 Williamstown Road, Port Melbourne, VIC 3207, Australia
4843/24, 2nd Floor, Ansari Road, Daryaganj, Delhi – 110002, India
79 Anson Road, #06–04/06, Singapore 079906
Cambridge University Press is part of the University of Cambridge.
It furthers the University’s mission by disseminating knowledge in the pursuit ofeducation, learning and research at the highest international levels of excellence.
www.cambridge.orgInformation on this title: www.cambridge.org/9781107164598DOI: 10.1017/9781316691113
© Cambridge University Press 2017
This publication is in copyright. Subject to statutory exceptionand to the provisions of relevant collective licensing agreements,no reproduction of any part may take place without the writtenpermission of Cambridge University Press.
First published 2017
Printed in the United Kingdom by Clays, St Ives plc
A catalogue record for this publication is available from the British Library
Library of Congress Cataloging-in-Publication DataBurns, Lawton Robert, editor | Liu, Gordon G., editorChina’s healthcare system and reform / edited by Lawton Robert Burns, Gordon G. Liu.Cambridge, United Kingdom : New York : Cambridge University Press, 2017. | Includesbibliographical references and index.LCCN 2016031778 | ISBN 9781107164598 (hardback) | ISBN 9781316616468 (pbk.)MESH: Health Care Reform | Health Policy | ChinaLCC RA395.C53 | NLM WA 540 JC6 | DDC 362.10951–dc23LC record available at https://lccn.loc.gov/2016031778
ISBN 978-1-107-16459-8 HardbackISBN 978-1-316-61646-8 Paperback
Additional password-protected resources for lecturers at www.cambridge.org/burns
Cambridge University Press has no responsibility for the persistence or accuracy ofURLs for external or third-party internet websites referred to in this publication,and does not guarantee that any content on such websites is, or will remain,accurate or appropriate.

C:/ITOOLS/WMS/CUP-NEW/8947020/WORKINGFOLDER/BURNSL/9781107164598PRE.3D v [1–24] 17.11.2016 2:55PM
Contents
List of Figures viiList of Tables xiList of Contributors xiiiForewordby William C. Hsiao, PhD
xix
Preface xxiAcknowledgments xxiii
PART I INTRODUCTION: ANALYTICFRAMEWORK, HISTORY, ANDPUBLIC HEALTH
1 China’s Healthcare Industry: A SystemPerspective 3Lawton Robert Burns and Gordon G. Liu
2 History of China’s Healthcare System 31Lawton Robert Burns and Yanzhong Huang
3 China’s Public Health System andInfrastructure 75Xiaofeng Liang and Lawton Robert Burns
PART II HEALTHCARE REFORM
4 Epidemiological Transition and Health SystemReforms in China 119Gordon G. Liu and Sam Krumholz
5 China’s Healthcare Reform: Status andOutlook 137Claudia Süssmuth-Dyckerhoff and FlorianThen
6 The Challenge of Non-communicable Diseases(NCDs) in China: Government Responses andOpportunities for Reform 150Tsung-Mei Cheng
v

C:/ITOOLS/WMS/CUP-NEW/8947020/WORKINGFOLDER/BURNSL/9781107164598PRE.3D vi [1–24] 17.11.2016 2:55PM
PART III HEALTHCARE PROVIDERS
7 China’s Physician and Nurse Workforce 179Lawton Robert Burns
8 China’s Hospital Sector 219Gerard M. La Forgia and Winnie Yip
9 United Family Healthcare (Chindex International):A Case Study 250Vanessa Folkerts and Roberta Lipson
10 Providing and Financing Elder Care inChina 269John Whitman and Lawton Robert Burns
PART IV INSURERS AND REIMBURSEMENT
11 Health Insurance in China 291Ambar La Forgia and Lawton Robert Burns
12 Health Insurance and Chronic Disease Control:Quasi-experimental Evidence from Hypertension inRural China 321Karen Eggleston, M. Kate Bundorf,Margaret Triyana, YanWang, and Sen Zhou
13 Drug Pricing and Health Technology Assessment inChina and Other Asian Markets 335Gordon G. Liu, Nan Luo, and ZhongyunZhao
PART V PRODUCT MANUFACTURERS
14 China’s Pharmaceutical Sector 351Rachel Lee and Lawton Robert Burns
15 China’s Medical Technology Sector 383James Deng and Lawton Robert Burns
16 Life Sciences Investment and Biotechnology inChina 428Stephen M. Sammut and Lawton RobertBurns
Index 451
vi Contents

C:/ITOOLS/WMS/CUP-NEW/8909712/WORKINGFOLDER/BURNSL/9781107164598C05.3D 137 [137–149] 10.11.2016 7:56PM
CHAPTER
5 China’s Healthcare ReformStatus and OutlookCLAUDIA SÜSSMUTH-DYCKERHOFF AND FLORIANTHEN
Introduction
China’s healthcare system is undergoing a majorreform, one of the most complex and far-reachingefforts ever undertaken by any public health systemin the world. It is designed to tackle a number ofissues, including substantial inconsistencies inhealthcare provision, the burden of chronic dis-eases, and rising costs.
This chapter provides an overview of China’shealthcare context, the reforms that the governmenthas put in place at national, provincial, and citylevels, and the outlook for the next stages of reform.It is intended to inform discussion on future choicesand actions taken by government, healthcare leadersand professionals, and private sector players.
The reforms are rooted in the specific context forhealthcare in the country. First, China’s healthcareservices vary considerably between rural and urbanareas, between one city and another, and even withinone city. Second, the country faces a major challengefrom chronic diseases: for instance, diabetes affects11.6 percent of the population compared with theUS rate of 9.3 percent. One in four Chinese hashigh blood pressure. China also accounts for a thirdof the world’s smokers.1 Third, healthcare costs arerising, out-of-pocket expenditures still account for34 percent of all healthcare spending, and inequal-ities in income mean that advanced medical treat-ment and drugs are still out of reach for many people.
Healthcare reform deliberations conductedbetween 2005 and 2009 drew on internal inputfrom the Ministry of Health (which has sinceevolved into today’s National Health and FamilyPlanning Commission, or NHFPC) along withexternal input from Peking University and FudanUniversity, the State Council’s Development
Research Center, the World Bank, and the WorldHealth Organization. In 2009, the governmentannounced a new system. The overall objective ofthe reform was defined as providing every Chinesecitizen with access to healthcare at an affordablecost by establishing a basic universal system of safe,effective, convenient, and low-cost services – withfull rollout by 2020. To achieve this objective, thegovernment set five priorities:
1. Medical insurance: Expand basic medicalinsurance programs
2. Drug supply security: Establish a national sys-tem for essential drugs
3. Medical service provision: Develop a primaryhealthcare service
4. Public health service: Provide equal access tourban and rural dwellers
5. Operating environment: Accelerate reform ofpublic hospitals
Figure 5.1 shows the key milestones of the reformand the progress achieved to date.
While formulated at a high level by the centralgovernment, the implementation of healthcare hasbeen, and still is, carried out at provincial or citylevels. This approach allows provinces the flexibil-ity to tailor healthcare to their socio-demographicand fiscal needs. It also creates an ecosystem of pilotprojects that might eventually uncover best prac-tices relevant for the broader system. Not surpris-ingly, the healthcare reform landscape has evolvedinto a heterogeneous patchwork. A few examplesillustrate this variety:
• Elimination of drug markups in all public hospitalsis a key policy designed to curb physicians’ over-prescription of drugs and to limit use of expensive
137

C:/ITOOLS/WMS/CUP-NEW/8909712/WORKINGFOLDER/BURNSL/9781107164598C05.3D 138 [137–149] 10.11.2016 7:56PM
drugs. While 100 pilot cities can claim that theyhave carried out this policy, others have yet to do so.
• Changing patients’ self-referral to Class III hos-pitals is another important policy. Guangzhouinitiated a guideline in April 2015 to promotethe establishment of referrals from primary careclinics to Class II/III hospitals. Reimbursement atClass II/III is only available for patients if theyhave been referred through primary care facilities.Only a few cities follow this model.
• Fee-for-service hospital reimbursement is alsoa big issue. While most hospitals in the countryare reimbursed on a fee-for-service basis, Beijinghas been experimenting with diagnosis-relatedgroups (DRGs) for several years. Tianjin is pilot-ing capitation models (fixed annual budget foreach patient treated) to encourage preventionand cost-effective care.
• Implementation of the Provincial ReimbursableDrug List (PRDL) varies. The list may feature2,342 molecules, as in Jiangxi, or include 2,051traditional Chinese medicine (TCM) products, asin Shanghai.
• There is also considerable variation in drug reim-bursement. Drugs may be fully reimbursableaccording to one city’s ruling, but may be an out-of-pocket expense for patients in a nearby city.
Heterogeneity has thus become a key characteristicof China’s healthcare system – an important fact tokeep in mind as we reflect on the progress of reformand consider what developments to expect in thisdynamic stage of the process.
The Chinese government has taken numeroussteps to accelerate the healthcare reform since thefirst announcement in 2009. These adjustmentshave been consistent with the initial objectivesand overall direction of the program. Table 5.1describes the key announcements around the mainschemes.
Medical Insurance: Objective 1
The backbone of China’s public health insurancesystem consists of three insurance schemes: UrbanEmployee Basic Medical Insurance (UEBMI) cov-ering city dwellers who are employed, UrbanResident Basic Medical Insurance (URBMI) cov-ering retirees and students in cities, and the NewCooperative Medical Scheme (NCMS) coveringrural residents. The three programs cover morethan 95 percent of the Chinese population,but how they work varies widely betweendifferent cities and rural areas. For instance,
priority areas for improvement
Medical insuranceExpand basic medical insurance programs
1
Drug supply securityEstablish a national system for essential drugs
2
Medical service provisionDevelop a primary healthcare service
3
Public health serviceProvide equal access to urban and rural dwellers
4
Operating environmentAccelerate reform in public hospitals
5
Establish a basic universal system that provides safe, effective, convenient, and low-cost healthcare services
Overall objective 2020
3251
43251
4
3251
43251
4
3251
43251
4
3251
43251
4
3251
43251
4
Progress Meter – Scale 1 – 5
Figure 5.1 Progress on the five key prioritiesSource: Healthcare reform 12th Five-Year Plan; McKinsey analysis.
138 Claudia Süssmuth-Dyckerhoff and Florian Then

C:/ITOOLS/WMS/CUP-NEW/8909712/WORKINGFOLDER/BURNSL/9781107164598C05.3D 139 [137–149] 10.11.2016 7:56PM
a worker in Shanghai will have a different publichealth insurance scheme from a worker inGuangzhou. Chapters 4 and 11 describe the threemain national medical insurance schemes in detail(see Table 11.1).
The National Reimbursement Drug List (NRDL)plays an important role in the insurance system.The NRDL is issued by the Ministry of HumanResources and Social Security (MoHRSS).The NRDL determines which drug is reimbursedand to what extent. The current list, which dates to2009, covers 2,127 molecules in two sublists. Its“A list” is centrally determined; a “B list” is alsocentrally determined but allows up to 15 percent
substitution by the provincial government. Forpatients with basic medical insurance, drugs onRDLA are fully reimbursable, whereas drugs onRDLB are 50–80 percent reimbursable.
The government’s stated goal is to cover 100 per-cent of the population by 2020. Recent statisticsindicate that coverage has already reached morethan 95 percent.2 The government has advanceda goal to reduce out-of-pocket spending from thecurrent levels – in 2013, out-of-pocket spendingstood at 34 percent of healthcare expenses – tobelow 30 percent. The effective reimbursementcoverage through the basic insurance schemesstill varies significantly by city and province, and
Table 5.1 Key announcements on major themes
Major Themes Key Announcements
Medical insurance • “Opinions on Further Implementing Critical Disease Insurance (CDI) for Urban andRural Residents” released by the central government in 2015 to push for the full rolloutof CDI
• Supportive policies for Private Health Insurance (PHI) development released bycentral government, including encouragement for PHI to offer CDI service and run PHIpre-tax deduction pilots
• Convergence of three BMI schemes is under way, while the combination of URBMIand NCMS has been successfully piloted in many regions
Drug supply security • First national Essential Drugs List (EDL) published in 2009 with updates and expansionin 2013
• Low-cost drug list released by NDRC in 2014 to ensure the supply of low-margin drugs
• NDRC lifts price controls on most medicines in 2015 to promote medicine price reformand encourage reasonable prices
Public health service • “Opinions on Establishing General Practitioners System” released in 2011 to addresstalent shortage in primary care facilities
• “Opinions on Further Improving Drug Supply and Management in Primary CareFacilities” released in 2014 to permit Non-EDL drug usage in primary care facilities, thusimproving access to medication
• Mandatory referral system announced in pilot regions (e.g., Guangzhou:reimbursement ratio at Class III/II is lowered if patient is not referred throughprimary care institutions)
Hospital reform • “Guidance on the comprehensive reform of city public hospitals” released in 2015to increase the number of public hospital reform pilot cities from 33 to 100 nationally
• Pilot reform to separate management and operation in hospitals has alreadybeen implemented in some regions (e.g., Shanghai Shenkang Hospital DevelopmentCenter)
• “National Planning Guideline for the Healthcare Service System (2015–2020)” releasedin 2015 with emphasis on the opening up of the hospital space to private investments
Compliance environment • NHFPC issued two sets of regulations in 2013 to prohibit misconduct and to pushfor ethical behavior
– “Blacklist Regulations” targeting pharmaceutical manufacturers and distributors
– “9 Prohibitions” targeting healthcare providers and institutions
Source: Government policies.
China’s Healthcare Reform: Status and Outlook 139

C:/ITOOLS/WMS/CUP-NEW/8909712/WORKINGFOLDER/BURNSL/9781107164598C05.3D 140 [137–149] 10.11.2016 7:56PM
co-payments (the fixed amount that the healthinsurer requires a patient to pay for a medical ser-vice) can be hefty. Figure 5.2 illustrates the burdenusing an example of a retiree with diabetes.The differences are more marked for patients need-ing high-priced oncology drugs, where the effectivereimbursement rates vary between 15 percent and30 percent depending on provincial policies and thecost of the drug treatment.
Gradual Improvement of Basic InsuranceSchemes
Overall, reimbursement levels have risen andannual caps raised in many areas over the past fewyears. For example, the URBMI schemes inKunming and Shaoxing have reduced co-paymentsfor outpatient services. Kunming has reduced theco-pay from 80 percent to 50 percent and increasedthe annual cap by 50 percent to 400 RMB; Shaoxinghas reduced the co-pay from65 percent to 50 percentand increased the annual cap to 500 RMB.3
In addition, Kunming has increased the annual
inpatient cap to 60,000 RMB, while Shaoxing haslowered the deductible for inpatient service from400 to 200 RMB. Reimbursement now covers atleast 50 percent of self-paid bills for proceduralcosts, drugs, and medical devices.
Critical Disease Insurance
Another high-impact initiative has been the imple-mentation of Critical Disease Insurance (CDI).The intent is to provide the groups most vulnerableto large healthcare expenses – such as individualsinsured under NCMS and URBMI –with additionalprotection against catastrophic illnesses.The government set up a funding and operationalmodel for this “top-up insurance” that providessecondary reimbursement for all or part of patients’out-of-pocket spending over the standard basicmedical insurance reimbursement ceiling. It askedprivate insurance companies to bid for providing thedesired coverage, essentially using public funds tobuy private group insurance at scale for certainpopulations. Several large, local private health
Example: Mr Wang, a retired employee under the UEBMI scheme in Shanghai receiving treatment for diabetes in a Class III hospital Out of pocketReimbursed
1 Average fund in a Shanghai resident’s personal BMI account is estimated at 1,217 RMB2 (7,550 RMB–700 RMB deductible line) x 70% = 4,795 RMB
9,1303,1156,015
~35%
Total treatment cost
~65%
Total reimbursed
4,795
Personal BMI a/c
1,220
Out of pocketBMI pooled a/c for outpatient coverage
1
23
Effective reimbursement rate under different schemes
City UEBMI (staff)
UEBMI (retired) URBMI NCMS
Hangzhou 67% 81% 15% 10%
Nantong 31% 37% 6% 2%
Shanghai 65% 12% 7%60%
Treatment cost: 9,130 RMB per year, 8,770 RMB of which iscovered by prescriptions and treatment under the outpatient reimbursement scheme
Assume Mr Wang has 1,220 RMB in his personal BMI account1
Payment from personal BMI account: 1,220 RMBRemaining 7,550 RMB is the “reimbursable portion”Check: 7,550 is >Deductible line (700 RMB for SH) and<Annual cap
Payment from BMI pooled account = 4,795 RMB based on 70% reimbursement rate for Shanghai2
Out-of-pocket expense = 3,115 RMB
1
2
3
Figure 5.2 Reimbursement rates vary even at the same locationSource: Government policies.
140 Claudia Süssmuth-Dyckerhoff and Florian Then

C:/ITOOLS/WMS/CUP-NEW/8909712/WORKINGFOLDER/BURNSL/9781107164598C05.3D 141 [137–149] 10.11.2016 7:56PM
insurance companies followed suit and have sincebecome important parts of the CDI system includ-ing China Pacific Insurance Group (CPIC) andChina Life.
The CDI system was issued in 2012 for theNCMS-covered population and started with a listof 20 critical diseases to be reimbursed at higherrates.4 It has evolved toward an add-on insurancebroadly covering healthcare costs for life-threatening diseases that exceed certain limits, irre-spective of the diagnosis. The government hasrequested that CDI reimburse at least 50 percent ofthe total medical bill for critical diseases for ruraland non-working urban residents. Participants donot need to pay extra fees for the new insurancecoverage. By April 2015, CDI had been piloted inall 31 provinces, covering roughly 700 million peo-ple. At the recent State Council summit (July 22,2015) hosted by Premier Li Keqiang, the govern-ment announced that CDI programs should berolled out to all provinces by the end of 2015 tocover all rural and non-working residents. By 2017,a robust CDI system should be established to forma solid network with other existing medical assis-tance programs.
Risk-sharing Arrangements withPharmaceutical Companies
Some cities have explored innovative ways towork with pharmaceutical companies to improveaccess to expensive therapies that are not yetcovered by the NRDL or the PRDL. For instance,Qingdao has negotiated access programs inwhich the pharmaceutical company donatesa proportion of the medication used in the cityto patients who meet certain physician evaluationand financial criteria. The remainder of the treat-ment cost is covered by the Qingdao government.Diseases and drug treatments covered by theseschemes include multiple sclerosis (recombinantinterferon beta-1b), leukemia (Dasatinib), breastcancer (Trastuzumab), and rheumatoid arthritis(Adalimumab). Established in 2012, theQingdao scheme was extended to additionaldrugs in 2015, suggesting that the model is sus-tainable for both the public payer and partneringcompanies alike.
Convergence of NCMS and URBMI
The government is now contemplating a mergerof the NCMS and URBMI schemes that wouldelevate NCMS coverage to URBMI standards.Just as important, the administration of NCMSwould move under the umbrella of MoHRSS,creating a large “super-payer” in charge of allpublic insurance in China (at present, NCMS isadministered by the NHFPC). Pilots are underway in several regions, including Sichuan,Tianjin, and Zhejiang.
Promotion of Private Health Insurance
While China has executed its public health insur-ance agenda, the government also sees an importantrole for private health insurance (PHI). For exam-ple, it has initiated measures such as tax breaks forPHI plans and relaxation of long-standing ruleslimiting foreign health insurers to minority owner-ship or 50–50 joint ventures with local players.Foreign insurers can now operate majority-ownedbusinesses in Shanghai’s Free-Trade Zone.
There is a clear need for approaches that promotefaster access to appropriate care, guaranteed qualityof care, and (for select consumer segments)improved hardware and infrastructure (such asadvanced diagnosis and treatment devices and high-end hospital wards). Nevertheless, the PHI marketin China is still nascent (see Chapter 11). This stemsfrom several systematic challenges, such as differ-ing standards of treatment in public hospitals, lackof data transparency required for needs-based pro-duct design and proper claims management, andhigh-cost distribution models.
Outlook for Reform Objective 1
The government’s stated goal is to expand the cov-erage of basic medical insurance and steadilyimprove the level of security it provides. However,each province or city has to work within basicmedical insurance budgets that could limit thedepth of coverage that can be achieved. This hasled to a fragmentation of reimbursement schemes.Whether innovative patented drugs, which areexpensive yet potentially lifesaving, will ever be
China’s Healthcare Reform: Status and Outlook 141

C:/ITOOLS/WMS/CUP-NEW/8909712/WORKINGFOLDER/BURNSL/9781107164598C05.3D 142 [137–149] 10.11.2016 7:56PM
reimbursed at the national level, local level, or not atall is unclear. Innovative approaches like Qingdao’spatient access programs for specific therapies willtherefore be of interest to manufacturers of high-cost drugs and medical devices. We expect furtheractivity and innovation as industry and publicpayers explore win–win partnerships to provideaccess to patients. Basic medical insurance seemsto have found its way as a pillar of health insurance,making full coverage by end of 2015 a crediblescenario.
As for PHI, several local and multinational com-panies are excited about its future, and substantialinvestments are being made in the quest for poleposition in this largely untapped market.The emergence of digital channels and a growingprivate healthcare sector offer support for the opti-mism of PHI players.
Drug Supply Security: Objective 2
In 2004, the Chinese government set up a nationalEssential Drugs List (EDL) to define the minimumnumber of molecules needed to cure the broadestspectrum of diseases at the lowest possible cost.At that time, China had no systems to manage thecost, availability, and quality of these drugs, nor didit have any policies in place to cover tendering,supply, or distribution.
The initial EDL was revised in 2009 followingthe announcement of the healthcare reform.The revised list covered 307 molecules with morethan 2,600 formulations, outlined new policies fortendering, and described a purchasing and deliverysystem that would be linked to the reimbursementsystem. All 307 molecules were fully reimbursed,and all community health centers (CHCs) wereexpected to use the EDL for all medicationneeds. Pharmaceutical companies with moleculeson the EDL had to decide if they wanted to bid.If they chose to participate and won, they had toaccept price cuts. While they would almost cer-tainly see an increase in sales volume, they had noguarantee that the gain would compensate for theprice cuts.
In 2010, the market was dominated by theAnhui model, which was initially supported bythe central government, and which specified“double envelope” bidding and “the lowest pricewins.” Double envelope refers to the biddingmethod: “first envelope” covers the technicalevaluation focusing on product quality, whilethe “second envelope” covers the price evalua-tion. Under this model, price was the initialcriterion for screening, and the offer with thelowest price made it to the next round. Onlythen were criteria such as quality and guaranteedsupply amount considered. However, downwardpressures on price prompted some manufacturersto stop supplying at low cost, creating shortagesof some drugs. Moreover, some CHC physicianswanted more drug options or were concernedabout the quality of EDL drugs. Concerns aboutaccess and quality stirred a public debate. Somepharmaceutical companies argued that quality begiven a higher priority than cost.
In response, the government adjusted its initialpolicy. In March 2012, the government issueda new document (State Council No. 11) thataltered the winning criterion from “lowestprice” to “quality first, appropriate price.”In March 2013, the State Council General Officeissued a revised EDL policy (State CouncilNo. 16) that contained further adjustments. First,quality was reaffirmed as the primary criterion andreasonable price as the second, with evaluationtaking place through the “double envelope”process. Second, the EDL was to be adjustedevery three years to reflect actual usage andneeds. Finally, there was to be a centralized pur-chasing mechanism for certain types of drug, nota-bly EDL drugs that (a) have been on the market fora long time and (b) have relatively stable prices,enabling uniform prices to be determined by thegovernment. National pricing advocates are alsosupporting experiments with price and volumeagreements as a way to reduce prices further.These policies would help to increase transpar-ency over EDL procedures.
In May 2013, a new version of the EDL wasreleased with 520 molecules. Disease coverage
142 Claudia Süssmuth-Dyckerhoff and Florian Then

C:/ITOOLS/WMS/CUP-NEW/8909712/WORKINGFOLDER/BURNSL/9781107164598C05.3D 143 [137–149] 10.11.2016 7:56PM
was broadened to include cancer and involved moredrugs for certain areas such as blood disease andpsychiatric disorders. The government furtherextended access to EDL drugs and pricing beyondgrassroots institutions to Class II/III hospitals. Morethan 20 provinces launched EDL usage require-ments for their hospitals. Provinces followed therequirements set by the central government onEDL revenue share (by value): 100 percent in grass-roots institutions, at least 40 percent in Class IIhospitals, and 25–30 percent in Class III hospitals.In September 2014, the NHFPC released a guidelineallowing the use of non-essential drugs in grassrootsmedical facilities, although essential drugs werestill given priority.
An important trend causing concern amongpharma companies is the proposed linkage betweenEDL and non-EDL tendering, which has beenimplemented on a pilot basis in regions such asQinghai and Shandong. As a result of this linkage,a pharmaceutical company that loses an EDL tender(or decides not to participate in the EDL) will auto-matically lose the RDL tender altogether if themolecule is EDL listed. Another concern triggeredby the current tendering dynamic is that prices couldbe driven down to levels that are simply not sustain-able for pharmaceutical companies, eventually put-ting supply of medication at risk.
Outlook for Reform Objective 2
Although we cannot predict what future versions ofEDL will look like, we can safely assume that themolecule list will expand further and that the gov-ernment will continue to push for its adoption asa mainstay of hospital prescribing beyond grass-roots facilities and Class III maximum-care provi-ders. Hospitals’ tendency to prescribe drugs outsidethe EDL is likely to be challenged by a mandate fora specific percentage of prescribed value to comefrom EDL drugs. Given the much lower prices ofthese drugs, the great majority of prescribed dailydoses and volumes would be EDL drugs under sucha mandate. The impact of these trends will dependon the number of molecules included on EDL, therelative weighting of quality and price, and theextent of EDL adoption across hospital levels(classes).
Medical Service Provision: Objective 3
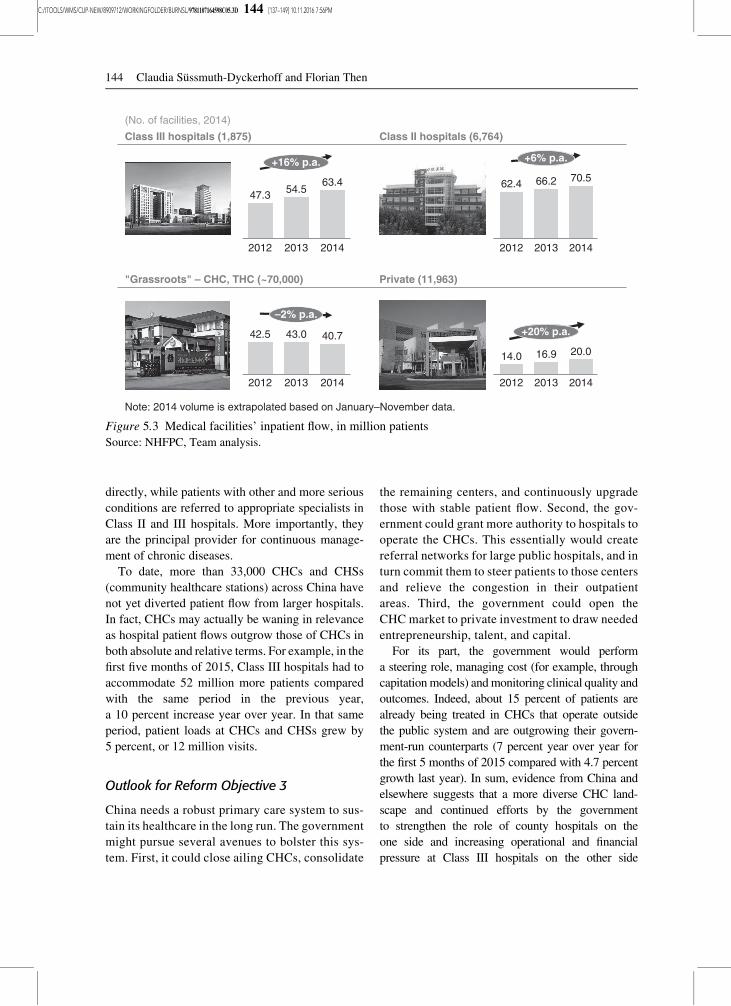
Public institutions underlie China’s healthcare sys-tem. According to the recent available data, 90 per-cent of inpatient cases were treated in the publicsystem in the first five months of 2015. The publicsystem is organized by levels, with Class III hospi-tals representing large maximum-care providers andacademic medical centers, often with over 1,000beds, and boasting China’s best medical talent.The lack of any steering mechanism for referralshas led to over-use and crowding of these hospitals –at the expense of Class I and II hospitals which areunder-utilized (see Figure 5.3). This likely impedesthe achievement of good patient outcomes, as ClassIII hospitals are neither designed nor able to providethe continuous care and patient education needed totreat the millions of people suffering from chronicdiseases (for example, diabetes, hypertension, andcardiovascular disease).
The mismatch of care settings partly explainswhy some diseases are under-diagnosed, or diag-nosed at a relatively late stage, in China.The unbalanced medical allocation leads to thelow efficiency of disease treatment and manage-ment. For example, 70 percent of cancers are mid-or end-stage at the time of first diagnosis.5 Fewerthan 20 percent of patients suffering from depres-sion are diagnosed.6 The control rate of hyperten-sion is less than 10 percent across the nation,compared with 48 percent in the United States.7
Beyond poor clinical outcomes, the lack ofa patient referral network leads to several economicinefficiencies: minor diseases are treated inmaximum-care settings, tests and examinations areduplicated across multiple healthcare facilities,and patients fail to comply with the treatments thathave been prescribed and paid for. Moreover, thecombination of long wait times and time-short phy-sicians has stressed patient–doctor relationships(see Chapter 7).
From a reform perspective, one government pol-icy to redress this misallocation of demand andsupply is the establishment of a primary careinfrastructure. The government envisions a broadnetwork of CHCs that act as primary care units.They are designed as the first point of contact forhealthcare where some minor diseases are treated
China’s Healthcare Reform: Status and Outlook 143
C:/ITOOLS/WMS/CUP-NEW/8909712/WORKINGFOLDER/BURNSL/9781107164598C05.3D 144 [137–149] 10.11.2016 7:56PM
directly, while patients with other and more seriousconditions are referred to appropriate specialists inClass II and III hospitals. More importantly, theyare the principal provider for continuous manage-ment of chronic diseases.
To date, more than 33,000 CHCs and CHSs(community healthcare stations) across China havenot yet diverted patient flow from larger hospitals.In fact, CHCs may actually be waning in relevanceas hospital patient flows outgrow those of CHCs inboth absolute and relative terms. For example, in thefirst five months of 2015, Class III hospitals had toaccommodate 52 million more patients comparedwith the same period in the previous year,a 10 percent increase year over year. In that sameperiod, patient loads at CHCs and CHSs grew by5 percent, or 12 million visits.
Outlook for Reform Objective 3
China needs a robust primary care system to sus-tain its healthcare in the long run. The governmentmight pursue several avenues to bolster this sys-tem. First, it could close ailing CHCs, consolidate
the remaining centers, and continuously upgradethose with stable patient flow. Second, the gov-ernment could grant more authority to hospitals tooperate the CHCs. This essentially would createreferral networks for large public hospitals, and inturn commit them to steer patients to those centersand relieve the congestion in their outpatientareas. Third, the government could open theCHC market to private investment to draw neededentrepreneurship, talent, and capital.
For its part, the government would performa steering role, managing cost (for example, throughcapitationmodels) andmonitoring clinical quality andoutcomes. Indeed, about 15 percent of patients arealready being treated in CHCs that operate outsidethe public system and are outgrowing their govern-ment-run counterparts (7 percent year over year forthe first 5 months of 2015 compared with 4.7 percentgrowth last year). In sum, evidence from China andelsewhere suggests that a more diverse CHC land-scape and continued efforts by the governmentto strengthen the role of county hospitals on theone side and increasing operational and financialpressure at Class III hospitals on the other side
Class III hospitals (1,875)
(No. of facilities, 2014)
Class II hospitals (6,764)
"Grassroots" – CHC, THC (~70,000) Private (11,963)
Note: 2014 volume is extrapolated based on January–November data.
+6% p.a.
2014
66.2 70.5
2013
62.4
2012
–2% p.a.
40.742.5 43.0
20142012 2013 2012
16.914.0
+20% p.a.
2013
20.0
2014
54.5
+16% p.a.
2012 2014
47.3
2013
63.4
Figure 5.3 Medical facilities’ inpatient flow, in million patientsSource: NHFPC, Team analysis.
144 Claudia Süssmuth-Dyckerhoff and Florian Then

C:/ITOOLS/WMS/CUP-NEW/8909712/WORKINGFOLDER/BURNSL/9781107164598C05.3D 145 [137–149] 10.11.2016 7:56PM
will eventually lead to a sustainable primary caresystem.
Public Health Service: Objective 4
While patients in urban areas face significant chal-lenges to obtain access to the right level of health-care, they pale in comparison with the daunting taskChina confronts in providing access to its vast anddispersed rural population. Rural patients must dealwith both a lack of hospitals (3.4 beds per 1,000inhabitants in rural areas compared with 7.4 in cities)and a low ratio of healthcare workers to local people(3.6 healthcare workers per 1,000 inhabitants in ruralareas compared with 9.2 in cities).8 Logistics areespecially challenging in more remote areas.
In its desire to provide more equal access tohealthcare, the government has invested massivelyin rural provider infrastructure. An initiative from1965 to 1970 undertook the construction of about56,500 township healthcare centers (THCs); thesewere intended to be the cornerstone of frontlinehealthcare delivery in rural areas. The extensivebricks-and-mortar infrastructure suffered froma lack of clinical talent, modern equipment,and patient acceptance. As part of the currentFive Year Plan 2011–2015 (FYP), the governmenthas invested another 30 billion RMB (roughly$5 billion) in improving infrastructure, upgradingmedical talent, and implementing population healthprograms; the latter programs include increasing theexamination rate of common diseases among ruralwomen to deepen the impact of rural healthcarereform. The number of THCs fell from roughly38,500 to 37,000 between 2009 and 2013, sincethe government focuses more on the quality ofTHC instead of pursuing blind expansion; 94 per-cent of those remaining were upgraded to complywith the latest standards and requirements of health-care reform.9
To develop talent, the government has investedin rural training programs, including 2–3 billionRMB of spending by the end of 2012.10
The programs encompass (a) clinical training for4.95 million physicians, nurses, and other health-care workers, (b) training in common diseases forsome 4 million healthcare workers, and (c) general
practitioner training for 36,000 physicians ingrassroots medical institutions. The governmenthas also introduced a subsidy of 6,000 RMB perperson to encourage medical students to work ingrassroots medical institutions. The proportion ofthose physicians with undergraduate degreesworking in CHCs increased from 30.8 percent to35.3 percent in 2013. A notice on national basicpublic health services issued on June 5, 2013,specifies several targets to be met by the end of2013; many have been revised in the new 2015plan. The goals were (are):
• Increase health information record system cover-age to 80 percent of the population, and electronicmedical record (EMR) coverage to 65 percent(75 percent in the 2015 plan)
• Cover 30 percent of the population with TCM-based health management offerings such asproviding regular TCM-based consultation andoffering healthcare instruction to the elderly(40 percent in the 2015 plan)
• Extend the national immunization program tovaccinate more than 90 percent of children,including the migrant population
• Extend health management to more than 80 per-cent of children such as regular family visits offamilies with newborn babies and health checkprograms for those in early childhood (85 percentin the 2015 plan)
• Extend health management to more than 80 per-cent of pregnant women (85 percent in the 2015plan), ensuring that each receives five prenatalexaminations and two postnatal checks; alsoimprove provision for pregnant women in grass-roots medical institutions
• Extend health management to 65 percent of peo-ple over the age of 65
• Secure the health management of 70 millionhypertensive patients and 20 million diabetespatients (80 million and 30 million, respectively,in the 2015 plan)
• Enhance health education, mental illness manage-ment, communicable diseases and public healthemergency management, health supervision,funding management, and evaluation programs
• Improve the role of grassroots medical institu-tions in all the above areas.
China’s Healthcare Reform: Status and Outlook 145

C:/ITOOLS/WMS/CUP-NEW/8909712/WORKINGFOLDER/BURNSL/9781107164598C05.3D 146 [137–149] 10.11.2016 7:56PM
Outlook for Reform Objective 4
The difficulty of assessing progress toward thesetargets makes it even harder to predict future devel-opments. As in other areas of the reform, the inter-pretation of the guidelines and the determination toimplement them vary widely across the country.Nevertheless, there are indications that progresshas been made. For example, the WHO estimatesthat vaccination rates for Class I vaccines (BCG,DTP3, HepB3, and HCV) have risen by about 5 per-cent since 2009 to reach almost 100 percent.The incidence of measles has plummeted frommore than 50,000 cases in 2009 to roughly 6,000in 2012, representing about five cases per millionpeople, an incidence lower than, e.g., Germany’s.
In other areas, the picture is more mixed. EMRshave been on the agenda since the tenth FYP2001–2005, but the development of a multitude ofapproaches in isolation has produced a fragmentedlandscape that lacks interoperability. That puts theinitial goal of EMR implementation – smooth andefficient documentation, storage, and exchange ofpatient data across hospitals – out of reach except ina few pilot areas in large cities.
Overall, progress seemsmostmarked in areas withone-dimensional goals and key performance indica-tors (KPIs) such as vaccination rates and infrastruc-ture delivery. These respond well to appropriatefunding and do not require a highly skilled workforceor complex coordination across regions and stake-holders. It remains to be seen whether similar successrates can be achieved in areas requiring longer-termcoordination and balanced incentives across differentstakeholders – such as disease management forchronic diseases, implementation of a truly inte-grated EMR system, and educational efforts capableof changing people’s behavior at scale.
Operating Environment: Objective 5
A main objective of the reform is to build a sustain-able, cost-effective, and high-quality public hospitalsystem. This involves four core elements:
• Funding mechanism: moving to a zero markup(ending the current margins on drugs and medicaldevices used in hospitals), increasing government
subsidies and medical service charges as the mainsources of funding, and reducing dependence ondrug sales
• Cost control: capping budgets and establishingpayer–provider relationships with effective cost-control mechanisms, such as DRGs and a cap ontotal costs
• Management transformation: setting clear KPIsfor service quality and operational efficiency
• Improvement in resource balance: reallocatingresources from large hospitals in big cities tograssroots institutions such as CHCs.
To date, none of these measures has been broadlyimplemented. However, major elements of thereform are being tested in pilots at the level ofhospital classes (such as Class III), counties, andindividual cities. An examination of a few examplesyields some insight into the depth and breadth of thereform.
Counties
The National Development and ReformCommission – China’s economic planning and man-agement agency – and the Ministry of Health plan toinvest RMB 40 billion in upgrading more than 2,000county hospitals. The first-wave pilot, including 311county hospitals, was planned in three phases:
• By the end of 2011, at least one hospital percounty should have reached the Class IIA level;county hospitals should have been capable oftreating common diseases, severe or emergencydiseases, and some complex diseases; and physi-cians should have been trained in THCs and vil-lage clinics.
• By the end of 2015, all county hospitals shouldreach the Class IIA level and be able to providesufficient care to their local population.
• By the end of 2020, the quality gap betweencounty and Class III hospitals should be closed;patient care conditions, treatment skills, and hos-pital management should have been upgraded;and there should be continuous improvement inmedical care to county level populations
Another 700 county hospitals joined the pilotin April 2014. In early 2015, NHFPC minister Li
146 Claudia Süssmuth-Dyckerhoff and Florian Then

C:/ITOOLS/WMS/CUP-NEW/8909712/WORKINGFOLDER/BURNSL/9781107164598C05.3D 147 [137–149] 10.11.2016 7:56PM
Bin commented on the 2015 healthcare reform plan,stating that the county hospital upgrade programwould be a priority for the coming year. The focuswould be implementing the zero mark-up policyand improving quality of county hospitals.
Cities
Building on the DRG model it set up in 2008,Beijing introduced a pilot in six Class III hospitalsin 2011 (there were still six pilot hospitals based onthe latest announcement). The results have beenencouraging (see Figure 5.4).
Shenzhen’s public hospital reform focuses onchanging the funding mechanism and introducingmeasures to control costs. The plan is to introducea zero markup in two stages, the first limited to localpatients and the second extended to all patients,including migrants. The funding mechanism willbe improved by gradually increasing governmentcontributions and increasing the service fee accord-ing to the hospital’s level (class). The paymentmechanism will be improved by moving to disease-or category-based payments for inpatients and tomostly capitation payments for outpatients.
Competition will be introduced by allowing patientsto use their prescriptions to purchase drugs at phar-macies: patients now can buy drugs in medicalinsurance-designated pharmacies, thus further low-ering the healthcare cost. Drug purchasing will bereformed by centralizing purchasing and distribu-tion and allowing manufacturers to sell directly tohospitals; this has been piloted in selected hospitalssuch as the University of Hong Kong-ShenzhenHospital.
Outlook for Reform Objective 5
Progress to date in hospital reform has been theslowest of the five pillars. Many pilots have beenlaunched, but they have not yet been fullyevaluated.
In addition, the government should considerfocusing on implementing treatment standards thatare unified and linked to an appropriate fundingmechanism that ensures hospital solvency. At thisstage, hospitals other than those in Class III seem tohave difficulty offering care at reimbursed fees;their real costs are higher than the sums they receivefrom the various public programs.
OOP
17.5
BMI
Class III average
4.9
12.6
Pilothospital
16.6
4.3
12.3
Average inpatient costThousand RMB
Rationale
Control costImprove service quality by giving each disease a clinical pathwayEnhance hospital management by changing the business model and mind-setSpeed up IT by standardizing the first page of medical records
Pilot situation
2004: launch of the management model for the DRG prospective payment system2007: standardization of the DRG medical record template2008: setting up of Beijing DRGs2011: official start of the DRG pilot in 6 hospitals,1 including 108 diseases in 26 major diagnostic categoriesInitial pricing based on historical data
Initial results
Average hospital stay – Pilot hospital: 7 days – Class III average: 10 days2 week rehospitalization rate – Pilot hospital: 6.5% – Class III average: 7.4%
Hospitals had 18% surplus
1 Peking University 3rd (the first to pilot, starting in November 2011),Peking University People’s, Youyi, Chaoyang, Xuanwu, and Tiantan
Figure 5.4 Early success with DRGs in Beijing Class III hospital pilotsSource: 2012 Xiamen H-CEO Conference.
China’s Healthcare Reform: Status and Outlook 147

C:/ITOOLS/WMS/CUP-NEW/8909712/WORKINGFOLDER/BURNSL/9781107164598C05.3D 148 [137–149] 10.11.2016 7:56PM
Experience from other, more mature healthsystems suggests that it will be helpful for thegovernment to consider whether and howa division between medical and managerial lea-dership roles, supported by clear KPIs in servicequality and operational efficiency, could supportdelivery of its objectives for transforming hospi-tal management.
When discussing the status of hospital reformin China, we also must reflect on the progressmade in the private sector. The objective of treat-ing 20 percent of the patient population in privatehospitals by the end of 2015 may not beachieved. But several regulatory changes mayaccelerate the provision of private offerings: (1)the official guideline that allows physicians towork at multiple sites helps to relieve the talentchallenges of the private hospital sector; (2) theoption to set up private hospitals as whollyforeign-owned entities; and (3) the possibilitythat public insurance programs might also beused to pay for treatment at private hospitals.11
Regulatory changes are pointing in the rightdirection. Yet all the administrative requirementsfacing private hospitals and clinics in China cre-ate challenges and roadblocks.
Summary
There is an enormous effort under way at central,provincial, county, and city levels to implementthe main content areas of a universal healthcaresystem that ensures affordable access to qualitycare and offers choices in the private sector forthose who can afford it. The healthcare system’smajor stakeholders share an understanding of whathas to happen next to further implement the reformand to live up to its vision. While funding reform isa continuing issue among decision-makers, onecan argue that China, as an economy, has themeans to pay for a reasonable system offeringuniversal access to care. China is at present spend-ing 5.6 percent of its gross domestic product onhealthcare and has room to continue on its trajec-tory of offering access to quality healthcare for itspopulation.
The biggest challenges will involve managementof chronic diseases and rigorous prevention pro-grams, development of the medical workforce atthe speed required, and system levers (seeFigure 1.7) such as steering mechanisms to theappropriate level of care. The government’s reformprogram has identifiedmany of the healthcare systemlevers that have proven effective in other countries.These levers include an increase in public-privatepartnerships, which is leading to an acceleration ofthe private sector’s ability to offer increased health-care choices and improved outcomes.
We remain optimistic that China will select thesystem levers that have proven effective in othercountries. The open question is how long this journeywill take and how radical some of the changes willbe. The unique situation of population size, geo-graphic scale, and urban–rural dynamics createsa level of complexity that no other country faces.We anticipate a significant increase in public-private partnerships and acceleration of the privatesector’s ability to offer healthcare choices to indivi-duals. The sector will remain dynamic, providingprivate enterprise unique opportunities to participatein improving the healthcare of the Chinese people.
Notes
1. Xu Yu et al. 2013. “Prevalence and Control ofDiabetes in Chinese Adults,” Journal of theAmerican Medical Association 310(9):948–958. Centers for Disease Control andPrevention. 2014. National Diabetes Fact Sheet.
2. NHFPC of the People’s Republic of China.2014. China Health Statistics Yearbook 2014.
3. Local BoHRSS website.4. Including severe pediatric conditions, certain
cancers, infectious diseases such as tuberculosisand AIDS, and severe mental disorders.
5. China Anti-Cancer Association. Availableonline at: www.chinacdc.cn/jlm/mxfcrxjbxx/200612/t20061211_38640.htm.
6. Wei Hao, Chairman of Neurologist Society ofChinese Medical Doctor Association. Availableonline at: www.yiqib.net/car/2015/07/03/108.html. Accessed on November 21, 2015.
148 Claudia Süssmuth-Dyckerhoff and Florian Then

C:/ITOOLS/WMS/CUP-NEW/8909712/WORKINGFOLDER/BURNSL/9781107164598C05.3D 149 [137–149] 10.11.2016 7:56PM
7. Lisheng Liu, Honorary chairman of ChinaHypertension League. Available online at:www.heartonline.cn/HeartOnLine_web/servlet/MeetingController;jsessionid=A7265D164ED86A1F227E29A5385DCCEA?method=detail&id=b3865686-278b-46be-9a15-6ce0531451f6&type=10. Cathleen D. Gillespie and KimberlyA. Hurvitz. 2013. “Prevalence of Hypertensionand Controlled Hypertension – United States,2007–2010,” MMWR Surveill Summ 62(03):144–148.
8. NHFPC of the People’s Republic of China.2014. China Health Statistics Yearbook 2014.
9. NHFPC of the People’s Republic of China.2015. Healthcare Reform Progress Report, 83,
May 25, 2015. Available online at: www.nhfpc.gov.cn/tigs/ygjb/201505/2f9a3505457d4179b8822c7444da2f6a.
10. Bingli Zhang. 2013. Rural Medical SystemDevelopment and Reform Report. Availableonline at: www.ccms.org.cn/UpLoads/News/2013-07-03-10-34-22.ppt.
11. Ministry of Human Resources and SocialSecurity of the People’s Republic ofChina. 2014. Notice on ImplementingMarket-regulated Price for Service ofNon-public Medical Facilities, 503, NDRC,March 25, 2014. Available online at: www.mohrss.gov.cn/gkml/xxgk/201404/t20140422_128933.htm.
China’s Healthcare Reform: Status and Outlook 149