child safety seat misuse: home visiting assessment and intervention
TRANSCRIPT
Public Health Nursing Vol. 15 No. 4, pp. 250-256
0 Blackwell Science, Inc. 0737- 1 209/98/$10.50
Child Safety Seat Misuse: Home Visiting Assessment and
Intervention Derryl E. Block, Ph.D., M.P.H., R.N.,
Tabitha K. Hanson, M.P.H., M.S., R.N., and Anne Keane, Ed.D., FAAN, R.N.
Abstract This project piloted the use of nurse-initiated home visits for child safety seat (CSS) assessment and intervention. Nurses made home visits to 149 rural and suburban Wisconsin women with children under 2 years of age, and assessed CSS misuse through observation and physical manipulation. Over three-quarters of CSSs were misused, although mothers were aware of only one-quarter of the instances of incorrect use. Nurses taught proper CSS use through verbal instruction, demonstration with parent’s own vehicle and CSS, and supervised parental manipulation of CSS. While mothers were receptive to home visiting for CSS assessment and education, this project involved substantial nurse training. Because thorough CSS assessment and intervention during home visits is resource-intensive, other options for improving correct CSS use and parental awareness are discussed.
Derryl E. Block is an Assistant Professor with the University of Minnesota School of Nursing in Duluth, Minnesota; Tabithu K. Hunson is a Public Health Nursing Supervisor at Stevens Traverse Public Health in Morris, Minnesota; and Anne Keane is an Associate Professor with the University of Pennsylvania School of Nursing in Philadelphia, Pennsylvania.
Address correspondence to Derryl E. Block, Ph. D., M. PH., R.N., School of Nursing, University of Minnesota, 135 Campus Center; 10 University Drive, Duluth, MN, 55812.
Accidents continue to be the leading cause of death among children under age 5 in the United States (Anderson, Ko- charek, & Murphy, 1997). Over 600 children under 5 years of age were killed as motor vehicle passengers in 1996 and about half of these children were unrestrained by child safety seats (CSSs) (National Highway Traffic Safety Ad- ministration [NHTSA], 1996a, 1996b). Approximately 3,300 children were saved by the use of child restraints from 1982 through 1996 (NHTSA, 1996a, 1996b). CSSs reduce fatal injury among children under five years of age by 71% and reduce the need for hospitalization by 69% (NHTSA, 1997a). Each year, increasing numbers of chil- dren are saved as a result of using CSSs (NHTSA, 1996a).
The decline in occupant fatality rate for children reflects positive changes in passenger safety laws. The first manda- tory child restraint law was implemented in Tennessee in 1978 (NHTSA, 1996a). Since 1985, all states and the Dis- trict of Columbia have “primary” child restraint laws, meaning that police may stop a vehicle for child restraint law violations (National Center for Injury Prevention and Control, 1997). NHTSA reports that 61.2% of child passen- gers under 5 years old are restrained in CSSs (NHTSA, 1997b). While CSSs are highly effective at preventing injury or death when used correctly, it has been estimated that up to 80% of CSSs are misused (NHTSA, 1996c, 1996d, 1997a).
Despite laws in states requiring CSS use, nonuse and misuse of CSSs are of continuing concern to public health nurses. This project piloted the use of nurse-initiated home visits for CSS assessment and intervention.
RELATED LITERATURE
Correct use of CSSs is not simple. While some parents may consider CSSs inconvenient, expensive, or too difficult to
250
Block et al.: Child Safety Seat Misuse 251
difficult to comprehend. In addition, instructions are not always available when parents purchase or otherwise ac- quire secondhand CSSs.
Other factors found to be correlated with proper CSS use include ( I ) parental demographics such as race (white), martial status (married), increased education, and increased income; (2) parental use of seat belts; (3) use of instructions to install CSS; (4) purchase of CSS versus receiving it as a gift; (5) physical characteristics of the CSS; and (6) awareness level of parents (NHTSA, 1996d). Additionally, rural rates of CSS use have been found to be lower (35.6%) than urban (68.9%) and suburban (78.6%) rates (NHTSA, 1996b).
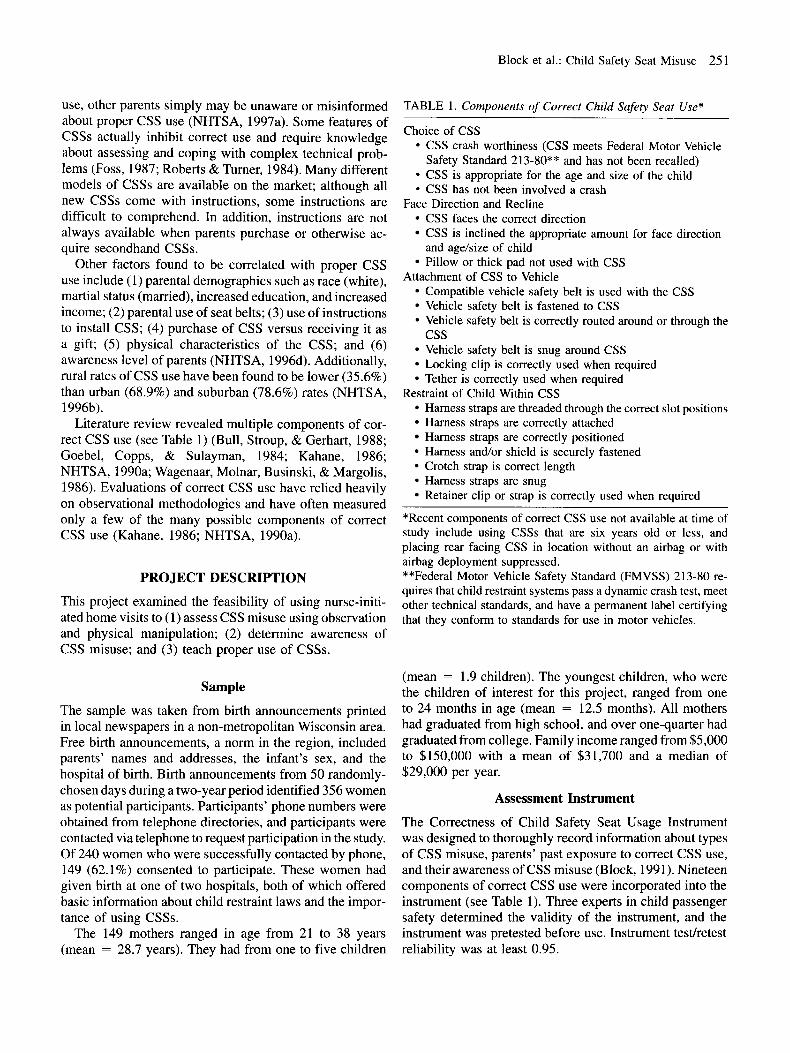
Literature review revealed multiple components of cor- rect CSS use (see Table 1) (Bull, Stroup, & Gerhart, 1988; Goebel, Copps, & Sulayman, 1984; Kahane, 1986; NHTSA, 1990a; Wagenaar, Molnar, Businski, & Margolis, 1986). Evaluations of correct CSS use have relied heavily on observational methodologies and have often measured only a few of the many possible components of correct CSS use (Kahane, 1986; NHTSA, 1990a).
PROJECT DESCRIPTION
This project examined the feasibility of using nurse-initi- ated home visits to (1) assess CSS misuse using observation and physical manipulation; (2) determine awareness of CSS misuse; and (3) teach proper use of CSSs.
Sample
The sample was taken from birth announcements printed in local newspapers in a non-metropolitan Wisconsin area. Free birth announcements, a norm in the region, included parents’ names and addresses, the infant’s sex, and the hospital of birth. Birth announcements from 50 randomly- chosen days during a two-year period identified 356 women as potential participants. Participants’ phone numbers were obtained from telephone directories, and participants were contacted via telephone to request participation in the study. Of 240 women who were successfully contacted by phone, 149 (62.1%) consented to participate. These women had given birth at one of two hospitals, both of which offered basic information about child restraint laws and the impor- tance of using CSSs.
The 149 mothers ranged in age from 21 to 38 years (mean = 28.7 years). They had from one to five children
CSS faces the correct direction CSS is inclined the appropriate amount for face direction
Pillow or thick pad not used with CSS
Compatible vehicle safety belt is used with the CSS Vehicle safety belt is fastened to CSS Vehicle safety belt is correctly routed around or through the
Vehicle safety belt is snug around CSS Locking clip is correctly used when required Tether is correctly used when required
Harness straps are threaded through the correct slot positions Harness straps are correctly attached Harness straps are correctly positioned Harness and/or shield is securely fastened Crotch strap is correct length Harness straps are snug Retainer clip or strap is correctly used when required
and age/size of child
Attachment of CSS to Vehicle
css
Restraint of Child Within CSS
*Recent components of correct CSS use not available at time of study include using CSSs that are six years old or less, and placing rear facing CSS in location without an airbag or with airbag deployment suppressed. **Federal Motor Vehicle Safety Standard (FMVSS) 213-80 re- quires that child restraint systems pass a dynamic crash test, meet other technical standards, and have a permanent label certifying that they conform to standards for use in motor vehicles.
(mean = 1.9 children). The youngest children, who were the children of interest for this project, ranged from one to 24 months in age (mean = 12.5 months). All mothers had graduated from high school, and over one-quarter had graduated from college. Family income ranged from $5,000 to $150,000 with a mean of $31,700 and a median of $29,000 per year.
Assessment Instrument
The Correctness of Child Safety Seat Usage Instrument was designed to thoroughly record information about types of CSS misuse, parents’ past exposure to correct CSS use, and their awareness of CSS misuse (Block, 1991). Nineteen components of correct CSS use were incorporated into the instrument (see Table 1). Three experts in child passenger safety determined the validity of the instrument, and the instrument was pretested before use. Instrument testhetest reliability was at least 0.95.

252 Public Health Nursing Volume 15 Number 4 August 1998
Nurse Training
Assessment and intervention were conducted by a public health nurse holding a master’s degree and by two regis- tered nurses who had finished their public health nursing rotation in a B.S.N. completion program. Nurse training was provided by the public health nurse, a child passenger safety advocate who had undergone CSS “Train the Trainer” education.
Training for this project included 10 hours of intensive prefieldwork instruction, and six hours of hands-on field- work including assessment, interview, and intervention. There were also three hours of supervised fieldwork mid- way through the project. Training included intensive in- struction on child passenger protection, types of CSSs, brands of CSSs, and proper installation and use. Nurses received user’s instructions that were provided with every model of child safety seat sold in the United States since 1981 (NHTSA, 1990b). Nurses were also given field manu- als, CSS educator materials, and a CSS assessment instru- ment (Block, 1991; Los Angeles Area Child Passenger Safety Association, 1990; Zeigler, 1987).
CSS assessment procedures were reviewed. Sample seats were examined and installed in cars. Supervised prac- tice observations and interviews were conducted at a day- care center and a discount store parking lot. At the midpoint of the project, supervised practice observations and inter- views were again conducted at a daycare center. Interrater reliability was 0.95 or higher for each pair of observers, for three observations, at the conclusion of the initial and midpoint practice sessions.
Procedure
Assessment and intervention occurred during scheduled visits to the women’s homes. One observation was con- ducted at a neighborhood health-center parking lot at the request of the mother. After giving written informed con- sent, each mother got her youngest child ready for a car ride and put the child in her car as if they were going on a short ride. The nurse read a prepared statement encourag- ing the mother to do what she normally does when prepar- ing her child for a car ride.
Visual observations of CSS use were made. Nurses also manipulated CSSs to assess types of misuse. Data were obtained regarding the mother’s previous knowledge of CSS use. Each mother was then asked about her awareness of the specific types of misuse detected by the researchers.
Based on the assessment of CSS misuse, nurses provided intervention during the home visit to answer questions, give information, and demonstrate proper CSS use. Nurses taught the mothers about the importance of correct CSS use, informed them of any CSS misuse observed, and ver- bally and/or physically helped to address the identified
problem. Teaching included verbal instruction, written handouts, and physical manipulation of the CSS, vehicle safety belts, and/or child by the nurse andor parent. Moth- ers were invited to do a return demonstration. Home visits took between 25 and 105 minutes. The assessment portion lasted about 15 minutes, while the intervention portion often took much longer.
ANALYSIS AND RESULTS
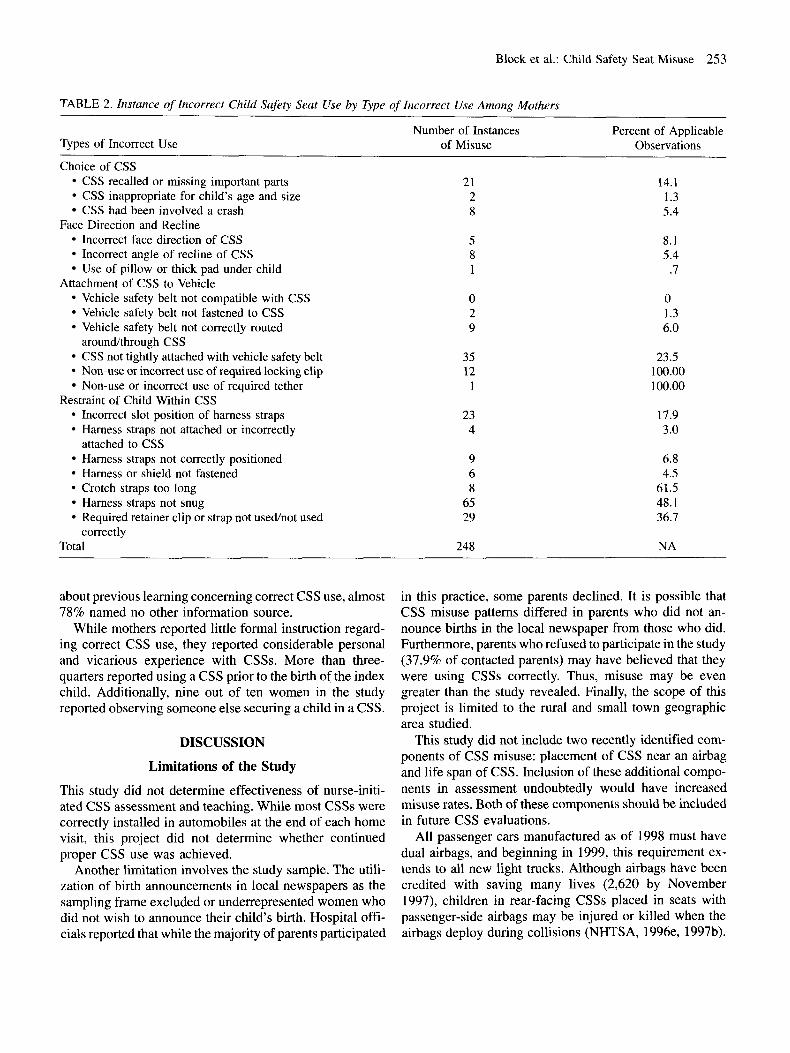
For analysis purposes, types of misuse were collapsed into four categories: (1) choice of CSS (including crashworthi- ness of the CSS, appropriateness of the CSS for the child’s size and age, and crash experience of the CSS); (2) face direction and recline of the CSS (including face direction of the CSS, angle of recline of the CSS, and use of a pillow or thick pad); (3) attachment of the CSS to the vehicle interior (including compatibility of the vehicle safety belt, routing of vehicle safety belt, fastening of the vehicle safety belt around the CSS, snugness of the vehicle safety belt, use of a required locking clip, and use of a required tether); and (4) restraint of the child within the CSS (including slot position of the harness straps, attachment of the harness straps to the CSS, positioning of harness straps, fastening of harness or shield, length of crotch strap, snugness of harness straps, and use of required retainer clip or strap). See Table 2.
CSS Misuse
More than three-quarters (78%) of the CSSs were used incorrectly. A total of 248 instances of misuse were found in the 149 observed child safety seats for an average of 1.7 instances of misuse per subject (Table 2). The most frequently observed type of incorrect use was loose harness straps (48.1% of CSSs). Almost one-quarter (23.5%) of CSSs were not tightly attached via the vehicle safety belt. Retainer clips or straps were not used or were misused in over one-third (36.7%) of the 79 CSSs where they were required. In all (100%) of the 12 cases requiring a locking clip to secure the vehicle safety belt, locking clips were not used or used incorrectly. One out of every seven CSSs (14.7%) was recalled or missing important parts.
Awareness of Misuse and Previous Learning
Despite the high rate of misuse, mothers were aware of only one-quarter (26.9%) of the incorrect use observed by nurses. Only 2% of the parents in this study reported receiving information from health workers about how to correctly use a CSS. Only three-quarters of the parents reported receiving a manufacturer’s instruction booklet, and even fewer (71.3%) reported ever referring to the booklet. Fewer than one in five of the women had the manufacturer’s instruction booklet on hand. When asked
Block et al.: Child Safety Seat Misuse 253
TABLE 2. Instance of Incorrect Child Safety Seat Use by Type of Incorrect Use Among Mothers
Number of Instances Percent of Applicable Types of Incorrect Use of Misuse Observations
Choice of CSS CSS recalled or missing important parts 21 14.1 CSS inappropriate for child’s age and size 2 1.3 CSS had been involved a crash 8 5.4
Incorrect face direction of CSS 5 8.1 Incorrect angle of recline of CSS 8 5.4 Use of pillow or thick pad under child .7
Vehicle safety belt not compatible with CSS 0 0
Face Direction and Recline
1 Attachment of CSS to Vehicle
Vehicle safety belt not fastened to CSS I .3 Vehicle safety belt not correctly routed 9 6.0
CSS not tightly attached with vehicle safety belt 23.5 100.00
2
aroundkhrough CSS 35 12 Non-use or incorrect use of required locking clip
Non-use or incorrect use of required tether 1 100.00 Restraint of Child Within CSS
Incorrect slot position of harness straps 23 17.9 Harness straps not attached or incorrectly 4 3 .O
Harness straps not correctly positioned 9 6.8 Harness or shield not fastened 6 4.5 Crotch straps too long 8 61.5 Harness straps not snug 65 48.1 Required retainer clip or strap not usedhot used 36.7
Total 248 NA
attached to CSS
29 correctly
about previous learning concerning correct CSS use, almost 78% named no other information source.
While mothers reported little formal instruction regard- ing correct CSS use, they reported considerable personal and vicarious experience with CSSs. More than three- quarters reported using a CSS prior to the birth of the index child. Additionally, nine out of ten women in the study reported observing someone else securing a child in a CSS.
DISCUSSION
Limitations of the Study
This study did not determine effectiveness of nurse-initi- ated CSS assessment and teaching. While most CSSs were correctly installed in automobiles at the end of each home visit, this project did not determine whether continued proper CSS use was achieved.
Another limitation involves the study sample. The utili- zation of birth announcements in local newspapers as the sampling frame excluded or underrepresented women who did not wish to announce their child’s birth. Hospital offi- cials reported that while the majority of parents participated
in this practice, some parents declined. It is possible that CSS misuse patterns differed in parents who did not an- nounce births in the local newspaper from those who did. Furthermore, parents who refused to participate in the study (37.9% of contacted parents) may have believed that they were using CSSs correctly. Thus, misuse may be even greater than the study revealed. Finally, the scope of this project is limited to the rural and small town geographic area studied.
This study did not include two recently identified com- ponents of CSS misuse: placement of CSS near an airbag and life span of CSS. Inclusion of these additional compo- nents in assessment undoubtedly would have increased misuse rates. Both of these components should be included in future CSS evaluations.
All passenger cars manufactured as of 1998 must have dual airbags, and beginning in 1999, this requirement ex- tends to all new light trucks. Although airbags have been credited with saving many lives (2,620 by November 1997), children in rear-facing CSSs placed in seats with passenger-side airbags may be injured or killed when the airbags deploy during collisions (NHTSA, 1996e, 1997b).

254 Public Health Nursing Volume 15 Number 4 August 1998
By November 1997, 49 children were killed as a result of crashes involving airbag deployment (NHTSA, 1997b). Almost all children involved in airbag fatalities were in rear-facing CSSs located in the front seat of vehicles with a passenger side airbag, were otherwise improperly re- strained, or were unrestrained (NHTSA, 1996e). Current recommendations emphasize seating all children under age 12 in the rear of the vehicle and never placing a rear-facing CSS in the front seat of a vehicle with a passenger side airbag (NHTSA, 1996e).
There are no clear guidelines based on scientific evi- dence for the life span of a child restraint. Until recently, the general rule has been to avoid seats made before 1/11 81, when the current federal standard became effective. Speculation about the effect of wear and tear, deterioration of plastic, and improvements in design and instructions have led advocates to caution against using CSSs that are more than 10 years old. In 1997, most manufacturers began recommending the general guideline that CSSs more than six years old should not be used (D. Stewart, personal communication, Dec. 19, 1997).
CSS Misuse Assessment
The use of observation and physical manipulation revealed CSS misuse among Wisconsin women equivalent to na- tional rates (80%). At least one type of incorrect use was observed in 116 out of 149 women (78%). Physical manip- ulation of CSSs allowed nurses to identify additional com- ponents of CSS misuse that were not assessed in observation studies. Future assessment of CSS misuse must incorporate visual observation and physical manipulation, as well as queries to parents about CSS use in order fully address the problem of CSS misuse.
Awareness of Misuse
Mothers were unaware of three-quarters of their errors in CSS use. This lack of awareness of incorrect use held true in choice of CSS, attachment of CSS to vehicle interior, restraint of child within CSS, and face direction and recline of CSS. Despite the CSS instruction reportedly available at the two hospitals where these women gave birth, almost no mothers reported receiving correct CSS instruction from health care workers. This may suggest that hospital-based postpartum CSS instruction may be ineffective for new parents, or that new parents are not receptive to learning such a complex subject in this environment. It is also possible that CSS instruction may not have been routinely provided or may not have covered correct use.
Teaching Proper CSS Use
Participating mothers were very receptive to learning about correct CSS use in their homes by nurses. Nurses were asked to examine seven additional CSSs that mothers
brought out of closets or garages. Mothers seemed espe- cially astonished at the list of recalled CSSs, and some women asked why the list is not prominent in physicians’ offices. Overall, the parents were excited about participat- ing in the project and interested in the topic of CSS misuse. One mother stated, “It’s so good to have a person to ask. The instruction book is impossible.”
Given that few of the women had the manufacturer’s instructional booklet on hand, project nurses often had to refer to their manuals. They also occasionally telephoned specific CSS manufacturers to ask about specific use prob- lems that were not described in the manufacturer’s instructions.
While no specific evaluation was conducted concerning the effectiveness of teaching proper CSS use, mothers were invited to do a return demonstration of correct CSS use. Most mothers were able to demonstrate proper CSS use after instruction; however, some needed to buy or otherwise obtain a different CSS for their vehicle. Future projects should incorporate evaluation of short- and long-term ef- fectiveness of intervention to improve correct CSS use.
CONCLUSION
This project examined the feasibility of using one-on-one nurse-initiated home visits to (1) assess CSS misuse using observation and physical manipulation; (2) determine par- ents’ awareness of CSS misuse; and (3) teach proper use of csss.
Although parents were very amenable to home visiting for CSS assessment and intervention, it is doubtful whether the intensive technical training that this project required supports programmatic implementation. In order to con- duct thorough CSS assessments, the National Highway Traffic Safety Administration (NHTSA 1996d) now recom- mends a minimum of three days of classroom instruction; use of training manuals, other resource materials and CSS misuse videos; demonstration covering the full range of CSSs, safety belt, and vehicle seat combinations; a week of practice; and supervised assessment. It may be more cost-effective to centralize technical expertise regarding CSS misuse in one or two professionals in the community, rather than disperse this knowledge among many nurses. As part of the public health assurance function, public health departments should assure that technical expertise is available in their communities for helping parents with csss.
While one-on-one teaching during home visits was ap- preciated by parents, visits took longer than expected. It is recommended that all public health nurses involved in maternallchild health visits conduct a minimal assessment of and general teaching about CSS misuse as part of their general preventive practice. As a minimum, this includes (1 ) helping parents assess whether the CSS has been re-

Block et al.: Child Safety Seat Misuse 255
called or in a previous crash; (2) checking that the CSS is securely attached to the vehicle and away from airbags; and ( 3 ) seeing that the child is securely attached to the CSS and facing the correct direction. Even minimal assess- ment of and general teaching about CSS misuse will require a modicum of staff training. Referral to community-based technical expertise is the necessary next step.
The complexity of CSSs, the rapidly changing develop- ment of infants and young children, and the technological changes in CSSs and automobiles preclude a simplistic educational message (Richards, Shelness, & Tombrello, 1990). No single educational message, except perhaps, ‘‘Follow the manufacturer’s instructions exactly,” is suffi- cient for CSS safety in all automobiles, or even for a specific CSS in a specific automobile as the child grows. Parents must also read their vehicle owner’s manual (which contains information on airbags, vehiclehafety belt com- patibility with CSSs), and refer to labels on the dash and sun visors.
Correct CSS use continues to be an elusive goal. Thirty- nine different makes and models were found in this study, and even trained nurses encountered difficulties in as- sessing correctness of CSS use. Some of the problems found in this project have likely been mitigated by CSS design changes, but there is an increasing amount of incom- patibility between automobiles and CSSs. It is necessary for consumers, technical experts, industry leaders, and health professionals to advocate for easy-to-use CSSs that have simple and clear instructions and that are compatible with automobile seats and safety belt systems. While the cre- ation and use of compatible easy-to-use CSSs is an ultimate goal, presently available CSSs necessitate comprehensive assessment and intervention.
While the majority of children are now transported in CSSs, this project shows that incorrect use is a substantial problem and parents are often unaware of their CSS misuse. In order to educate parents effectively, and to be consumer advocates, nurses and other health professionals working with young children and their families should have basic knowledge about correct CSS use. Until CSS technology becomes user-friendly, there is an additional need for pro- fessionals with high-level technical expertise to assist par- ents in safely using CSSs. This project shows that dispersing such expertise may be time consuming and therefore costly. All public health nurses should have some basic CSS knowledge, however, and public health agencies should assure that high-level technical expertise is available in each community.
ACKNOWLEDGMENTS
The authors wish to acknowledge Muriel and Phillip Ber- man for fellowship support, Diane Vanderlin for project assistance, Stephanie M. Tombrello, LCSW, of SafetyBelt-
Safe U.S.A. for helpful comments, and Susan J. Hutton for editorial assistance.
REFERENCES
Anderson, R. N., Kocharek, K. D., & Murphy, S. L. (1997). Report of final mortality statistics, 1995. Monthly Vital Statis- tics Report 45( 11)(S)2. Hyattsville, MD: National Center for Health Statistics.
Block, D. (1991). Correctness of child safety seat useage and rental program participation (Doctoral dissertation, University of Pennsylvania). Dissertation Abstracts International. 5243B.
Bull, M., Stroup, K. N., & Gerhart, S. (1988). Misuse of car safety seats. Pediatrics 18( l), 98-101.
Foss, R. D. (1987). Sociocultural perspective on child occupant protection. Pediatrics 80(6), 886-893.
Goebel, J. B., Copps, T. J., & Sulayman, R. F. (1984). Infant car seat usage: Effectiveness of a postpartum educational pro- gram. Journal of Obstetric, Gynecological, and Neonatal Nursing 13( l), 33-36.
Kahane, C. J. (1986). An evaluation of child passenger safety: The effectiveness and benefits of safety seats, summary (DOT HS 806, 889). Washington, DC: Office of Standards Evalua- tion, National Highway Traffic Safety Administration.
Los Angeles Area Child Passenger Safety Association. (1990). Child passenger safety educator materials. (Available from Los Angeles Area Child Passenger Safety Association, P.O. Box 553, Altadena, CA 91001).
National Center for Injury Prevention and Control. (1997). Unin- tentional injury fact sheet: Child passenger safety [On-line]. Available http://www.cdc.gov/ncipc/duip/childpas.htm
National Highway Traffic Safety Administration. (1990a). Occu- pant protection trends in 19 cities. Washington, DC: U.S. Department of Transportation.
National Highway Traffic Safety Administration. (1990b). Manu- facturers ’ instructions for child safety seats (Publication no. NTS-13). Washington, DC: U.S. Department of Trans- portation.
National Highway Traffic Safety Administration. (1996a). TrafJic safety facts 1996: Occupant protection. Washington, DC: U.S. Department of Transportation, National Center for Statistics and Analysis.
National Highway Traffic Safety Administration. (1996b). TrafJic safety facts 1996: Children. Washington, DC: U.S. Depart- ment of Transportation, National Center for Statistics and Analysis.
National Highway Traffic Safety Administration. (1996~). Child passengerprotection laws. Washington, DC: U.S. Department of Transportation.
National Highway Traffic Safety Administration. (1996d). Pat- terns of misuse of child safety seats. Final report (DOT HS 808, 440). Washington, DC: U.S. Department of Trans- portation.
National Highway Traffic Safety Administration. (1996e). Third report to congress: effectiveness of occupant protection sys- tems and their use. Washington, DC: U.S. Department of Transportation.
National Highway Traffic Safety Administration. (1997a). Presi-

256 Public Health Nursing Volume 15 Number 4 August 1998
dential Initiative for Increasing Seat Belt Use Nationwide- Recommendations from the Secretary of Transportation [On-line]. Available http://www.nhtsa.dot.gov/people/injury/ airbagslpresbeltl
National Highway Traffic Safety Administration. (1997b). Safety fact sheet [On-line]. Available http://www.nhtsa.dot.gov/ airbags/factsheets/numbers.html
Richards, D., Shelness, A., & Tombrello, S. (1990, May). Panel of founders: Where do we go next in child passenger safety? Paper presented at the meeting of LifesaversI8, San Diego, CA.
Roberts, M. C., & Turner, D. S. (1984). Preventing death and injury in childhood: A synthesis of child safety seat efforts. Health Education Quarterly 11(2), 181-193.
Wagenaar, A. C., Molnar, L. J., Businski, K. L., & Margolis, L. H. (1986). Correlates of child restraint use (UMTRI 86-47). Ann Arbor, MI: University of Michigan Transportation Re- search Institute.
Zeigler, P. N. (1987). Guidelines for observing child safety seat use (DOT HS, 807, 128). Washington, DC: U.S. Department of Transportation.