chest pain in the rural setting - .net framework
TRANSCRIPT
Emergency MedicineEmergency Medicine
Chest Pain in the Rural Setting
Prof Tony Celenza

Emergency Medicine
Overview
• Chest Pain Assessment– WACHS Process
• Acute Management of ACS• Other Causes of Serious Chest Pain
• Acknowledge Prof Yusuf Nagree, FSH

Emergency Medicine
Chest Pain in the ED
• Chest pain ~10% ED presentations (tertiary) or 4% (rural)
• Symptom of benign or life-threatening conditions
• 10-15% are serious conditions
– About 10-12% cardiac
– About 2-3% other serious causes (PE, dissection)
• Incidence depends on casemix
• Need safe process to accurately identify sinister causes

Emergency Medicine
WACHS Chest Pain Pathway in the ED
• To move risk stratification to international best practice
• Assess ACS risk using combination of:
– TIMI score
– High risk clinical features
– Troponin
• Awareness of non-cardiac sinister causes of chest pain

Emergency Medicine
Serious Causes of Chest Pain (non-traumatic)
• Acute coronary syndrome
• Pulmonary embolus
• Aortic Dissection
• Oesophageal Rupture
• Myocarditis / Pericarditis
• Spontaneous Pneumothorax

Emergency Medicine
• Possible cardiac pain 23%• Non-cardiac chest pain 17%• Musculoskeletal pain 15% (lower than other studies)• Respiratory condition 10%• ACS/STEMI 4.5%• 40% admitted, <1% transferred

Emergency Medicine
Acute Coronary Syndromes (ACS)
• Ischaemia– Reduced blood flow due to spasm or blockages– Reversible– ST depression, T inversion or no ECG changes– No troponin rise
• Infarct– Complete blood flow occlusion leads to tissue necrosis– Irreversible– Associated with troponin rises
– +/- ST/T changes/elevation
Emergency Medicine
Acute Coronary Syndromes
• Chest pain is most common symptom of ACS
• But not all chest pain is ACS, not all ACS have chest pain
• Some ACS have “typical” chest pain
– Central Crushing / Squeezing / Pressure +/- radiation
– May resolve / decrease with rest
• However, mostly get “atypical” chest pain
• 1st step is to decide whether “possible” ACS
– Get ECG within 10 minutes
Emergency Medicine

Emergency Medicine

Emergency Medicine

Emergency Medicine

Emergency Medicine
ACS Diagnosis/Risk Stratification
• If possible ACS, need to determine likelihood of an adverse outcome (MACE)
– Difficult– 1-2% miss rate– Single clinical features not helpful– Response to GTN or antacids is misleading– Experienced clinician Gestault useful
• Diagnostic pathways useful
Emergency Medicine
Risk Scores
• A number of risk stratification tools out there now:
– HEART score – simple but degree of subjectivity
– EDACS – relatively complex to calculate but good specificity
– TIMI – simple. Not designed for ED use (but has been validated in ED)
• Balance between sensitivity and specificity

Emergency Medicine

Emergency Medicine

SCGH Acute Coronary Syndrome (ACS) Assessment and Treatment Algorithm
Chestpain/
symptomsconsistentwithACS
Considerimportantdifferentialssuchas
Aorticdissection,PE,pneumothorax…
UNSTABLEORDISTRESSEDPATIENTMANDATES
IMMEDIATESENIORMEDICALREVIEW
ECGImmediate12leadECG–reviewbyEDregor
consultantwithin10minutes
ECGchangesconsistentwithSTEMI• STelevation>1mmin2contiguouslimbleadsor
• STelevation>2mmin2contiguouschestleads
• NewLBBB(fordiscussionwithcardiologyconsultant)
SEESCGHEDCODESTEMIPROTOCOL
Evaluateandriskstratify
• Clinicalhistory
• Examination
• Initialtroponin
• ECG(repeatevery20minsifongoingpain)
• CXR
• EvaluateclinicallikelihoodofACSusing
EDACSscoreandanyhighriskfeatures?
• Considerothercausesandinvestigate
appropriately
• Ensureaspirin300mggiven
• GTN(SLthenIVifrequired)(bewarehypotension,phosphodiesteraseinhibitors(Sildenafil),severeAS)
• Otheranalgesia–e.g.titratedmorphine
Ifthefirsttroponinistaken>4hoursaftermaximalpainandisnegative,repeattroponinisnotrequired(considerasserialtroponinnegativepatient).
Repeattroponin2hoursafterinitialbloodsandatleast4hoursaftermaximalpain;alsoperformserialECG
STEMI STEMI
Care• Triage1or2asperACEMguidelines
• Directtoresuscitationarea
• MonitorECGandO2stats
• Observations–BP(bilateralifdissectionconsidered),temp,pulse,resps,SpO2,painassessment
• Bloods–FBP,U&E,BSL,troponin(takepurple,greenandbluetop(soseniordoctorcanaddD-dimerifindicated))
• CXR
• Aspirin300mgunlessalreadygivenorcontraindicated
• Oxygenonlyifhypoxia(SpO2<93%)orshock;ifthereinhypercapnoeicrespfailureaimatsats88-92%.
AnyhighriskfeaturesforACS?
• ECGchanges
o ischaemic/dynamicchanges
o ifindoubtseeksenioropinion
• Chestpain
o Ischaemicsoundingchestpainonminimalexertion
o Recentaccelerationofanginapatternor�threshold
o Ongoingischaemicsoundingchestpain
• Otherhighriskfeatures
o Syncope
o SystolicBPlessthan90mmHg(notduetoGTN)
o Haemodynamicinstability(shock)
o Signsandsymptomsheartfailure/pulmonaryoedema
o RecentPCIlessthan6monthsorpriorCABG
o SustainedarrhythmiaVT(>3beats)/anyVF
LowriskACSgroupNegativeinitialtroponin
EDACSScore<16andNohighriskfeatures
EDUslip,EDreviewafter2ndtroponin/ECG
NotlowriskACSgroupNegativeinitialtroponin
EDACSScore≥16andNohighriskfeaturesEDUslip,callforcardiologyreview
UndifferentiatedhighriskgroupSlightlyraisedtroponin
wherenon-ACScauseofraisedtroponinislikely
IxforPE,dissection,AF,sepsis,renalfailure…
Appropriatebookingslipassoonaspossible
HighriskACSgroupPositiveinitialtroponinOR
AnyhighriskfeatureforACS(seeabove)
• ≤80yoandrelativelywellandindependent
Informcardiologyreg,putinbookingslipandsend
towardwhenbedready(asperadmissionpolicy)
*IfunstablecardiologyreviewinEDisrequired
• 81-85yo
� Wellandindependent
Informcardiologyregasfor≤80yogroup
� Notwellandindependent
MAUadmit
• >85yoormultiplenon-cardiaccomorbidities
Non-invasivestrategyappropriate-admitMAU
• WherethereisdisagreementordelaytheED
consultantorSRmayadmitattheirdiscretion
1. Initialnegative
troponinbecomes
positive
2. Ifinitialtroponinwas
slightlyraisedand
alternativediagnosis
wasbeingconsidered
butnotfound,and
troponinrises>50%
frombaseline
ManageasHighriskACS
group(seeboxaboveright)
• Ensureaspirin300mg
• Ticagrelor180mgloadthen90mgbdunless
contraindication(ifbradycardia<50use
Clopidogrel600mgloadthen75mgdaily)
• NoEnoxaparininEDunlessspecifiedby
cardiology
• NoneedforB-blockerinED(espnotIV)
1. Negativeserial
troponin
2. SerialECGnot
ischaemic
3. LowriskACSgroup
Alternatediagnosislikely
onclinicalassessment.
ProbableNon-ACS.
Manageothercauses,
likelydischarge.
GPfollowup.
1. Negativeserial
troponin
2. SerialECGnot
ischaemic
3. LowriskACSgroup
Alternatediagnosisnot
apparent.
Riskmajoradversecardiac
event<1/100
Givewrittenadvice,
returniffurtherpain,
GPreview,furtherIx
discretionary.
1. Minimallyraisedstable
troponin(<50%rise)
Clinicallyconsidered
unlikelytobeofACSorigin
Investigateandmanage
otherconditionsandadmit
asappropriate.
ReconsiderNSTEMIas
possiblediagnosis&seek
cardiolreviewifACS
remainsapossibility
1. Negativeserialtroponin
2. SerialECGnotischaemic
3. Nohighriskfeatures
4. NotlowriskACSgroup
becauseEDACS>=16
Cardiologyreviewand
expeditedinvestigationeither
asinpatientoroutpatient.
Cardiologyregwillarrange
investigationandfollowup
MinimalriskACSLowriskACS
stableandpainfree
NotlowriskACSgroup Alternatediagnosis
likely
Age Score
18-45 +2
46-50 +4
51-55 +6
56-60 +8
61-65 +10
66-70 +12
71-75 +14
76-80 +16
81-85 +18
86+ +20
SCORE1
TOTALSCORE= SCORE1+SCORE2=
*Riskfactors:family history of premature CAD, dyslipidaemia, diabetes, hypertension, current smoker. **Pain that caused presentation to hospital.
Otherfactors Score
Malesex +6
Aged18-50yearsandeither:
• Knowncoronaryarterydiseaseor
• 3ormoreriskfactors*
+4
Symptomsandsigns
• Diaphoresis +3
Radiatestoarmorshoulder +5
Pain**occurredorworsenedwith
inspiration
-4
Pain**isreproducedbypalpation -6
SCORE2
E
D
A
C
S
S
C
O
R
E
Assess
Care1
Triageand
initialcare
2
ECG
3
Evaluate,risk
stratifyand
starttreatment
4
Assesspost
1sttroponin
5
Repeattrop
&ECG
6
FinalED
Assessment
&Plan
HighriskACS
Non-STelevationACS
ManagementinED

Emergency Medicine
• 21% of patients had MACE within 30 days– 28% of Indigenous cohort, 19% of non-Indigenous– Mean age 57 v 67– Lower HEART scores in Indigenous cohort with MACE– Diabetes 45% v 19%

Emergency Medicine
• The National Heart Foundation 2016 ACS guidelines recommend use of a tool but don’t recommend a particular one
• https://www.heartfoundation.org.au/for-professionals/clinical-information/acute-coronary-syndromes
• Most places use TIMI due to simplicity
– WACHS pathway adds other high risk factors and troponin

Emergency Medicine
TIMI Risk Stratification
• TIMI <3 – low risk of adverse outcome in 30 days• TIMI 3 – moderate risk of adverse outcome in 30 days • TIMI >3 – high risk of adverse outcome in 30 days
Calculate TIMI score
Age > 65 (> 45 for ATSI) 1 point
Aspirin use in last 7 days (excluding analgesic use) 1 point
> 2 episodes pain in last 24 hours 1 point
ST changes ≥ 0.5mm 1 point
Known stenosis ≥ 50% 1 point
≥ 3 coronary artery disease risk factors 1 point
Risk factors: Sedentary occupation, Hypertension, Diabetes, Current Smoker, Hypercholesterolaemia, High risk ethnic group

Emergency Medicine
High Risk Features
• Precipitated at rest or by minimal exertion• Diaphoresis• Syncope• CCF• Hypotension (BP<90) not associated with GTN• Shock• VF or VT• Angioplasty or CABG within 6 months

Emergency Medicine
Ischaemic ECG – ST Depression

Emergency Medicine
Ischaemic ECG – T wave inversion

Emergency Medicine
Cardiac Troponins
• Enzyme released by dying / ischaemic heart muscle
• Highly specific and sensitive – sort of!
• Basically three types of troponin testing now:
– Point of care
– Standard laboratory analyser
– Highly sensitive
• WACS only has the first two which are termed “standard sensitivity”

Emergency Medicine
• Problem is that small increases in troponin can be seen with many non cardiac conditions:
• Including eating a hot curry!
• Acute and chronic heart failure• Myocarditis• Cardiac contusion from trauma• Cardioversion• Endomyocardial biopsy• Aortic dissection• Hypertrophic cardiomyopathy• Aortic valve disease (aortic stenosis or regurgitation)• Cardiotoxic drugs• Tachyarrhythmia (SVT, V-tach, atrial fibrillation)• Bradyarrhythmia or heart block
• Cardiac surgery• Cardioversion• Tako-tsubo cardiomyopathy• Rhabdomyolysis• Stenting or angioplasty
(percutaneous coronary intervention/PCI)
• Irukandji syndrome
• Renal failure• Pulmonary embolism• Severe pulmonary hypertension• Sepsis• Severe critical illness• Burns• Extreme exertion• Amyloidosis or other infiltrative diseases• Stroke• Subarachnoid hemorrhage
Cardiac Troponins

Emergency Medicine
Complex question – depends on risk stratification, duration of pain and type of assay (table 9, NHF guidelines)
Troponin Timing
Emergency Medicine
• Only have standard sensitivity and using TIMI
• Therefore, timing is 0, 4, 8 post arrival
• If pain occurred more than 12 hours ago and you are confident there has been no recurrence of pain, a single troponin may be adequate – beware of POC though
• Accelerated pathway. In certain low risk patients (TIMI 0 with no high risk features and low clinical suspicion of ACS, you can do 0 & 4 hours but only on LABORATORY troponin (not point of care) )
WACHS Pathway

Emergency Medicine
• TIMI < 4, then serial troponins and ECG. If serial troponins, ECGs normal, no ongoing or recurrent pain, then:
– TIMI 0,1,2 – refer back to GP for risk factor modification and stress test
– TIMI 3 – organise urgent cardiology outpatient– TIMI 4 or high risk features – admit/transfer
• ECG changes, positive troponins or TIMI > 5, then admit or transfer, ticagrelor (clopidogrel if HR<50), anti-coagulation, beta blocker
Presentation Suspicious of ACS

Emergency Medicine

Emergency Medicine
STEMI

Emergency Medicine
ST Elevation MI
• Early reperfusion the key– Ideally have angioplasty but not practical in WACHS – Therefore, most will get tenecteplase
• Thrombolysis packs and guideline in ED– Medications– Contraindications checklist– Administration checklist– Anticoagulation guidelines– Patient information sheet

Emergency Medicine

Emergency Medicine

Emergency Medicine

Emergency Medicine

Emergency Medicine
• Blood clot in lungs
• Pain – inspiratory, sharp, pleuritic. Often with SOB
• Risk factors– Past or family history of VTE
– Recent invasive surgery
– Prolonged immoblisation including leg plaster
– Malignancy
– Past or family history of thrombophilia
– Smoker taking exogenous oestrogen
– Recent Travel
– Pregnancy
Pulmonary Embolism

Emergency Medicine
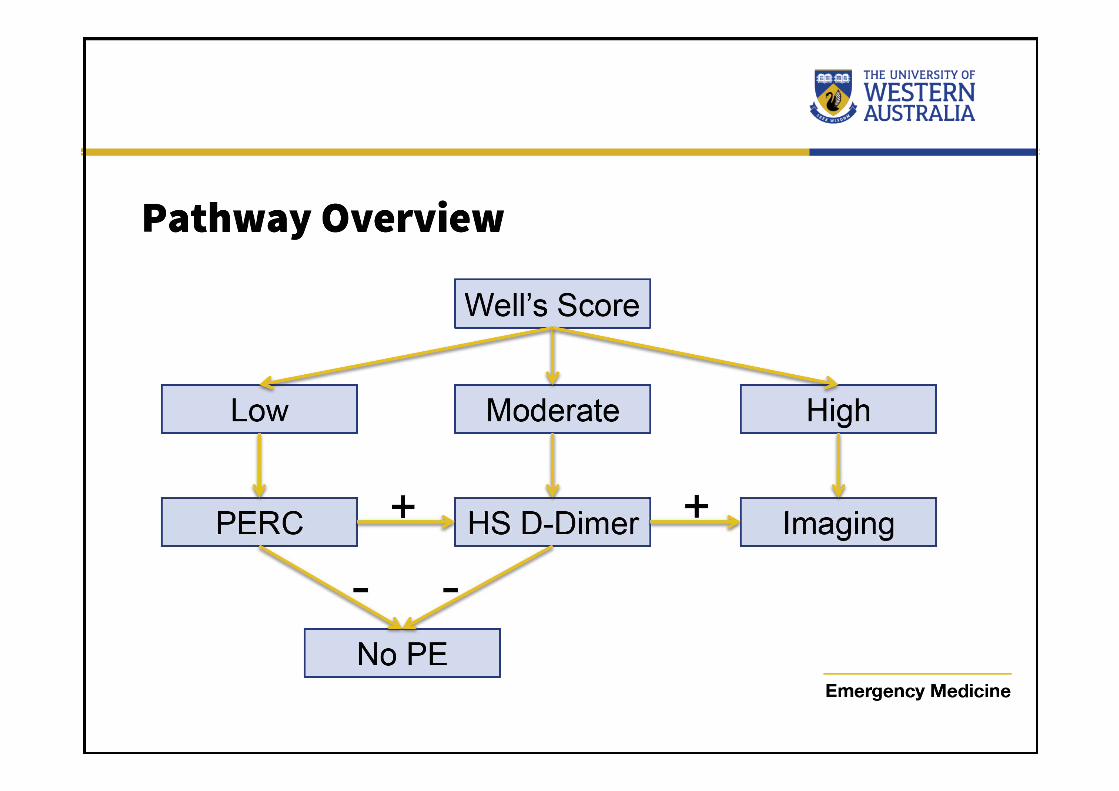
Wells Score
0-3 – low probability; 4-6 moderate probability; >6 high probability
If high probability, need to proceed straight to imaging
Clinical Signs and Symptoms of DVT 3 points
PE is most likely diagnosis, or Equally Likely 3 points
Heart Rate > 100 1.5 points
Immobilization > 3 days, or surgery < 4 weeks 1.5 points
Previous, objectively diagnosed PE or DVT 1.5 points
Malignancy with treatment within 6/12 or palliative 1 point

Emergency Medicine
PERC System
PE highly unlikely if all true:
• However, they must be low risk to start with.
• Exclude patients in whom shortness of breath is not the most important, or equally most important, presenting complaint, cancer, thrombophilia, strong family history of thrombophilia, beta blockers that may mask tachycardia, patients with transient tachycardia, patients with amputations, patients who are massively obese and in whom leg swelling cannot be reliably ascertained, with baseline hypoxemia in whom a pulse oximetry reading <95% is long-standing
• Age<50 • No unilateral leg swelling
• HR<100 • No previous VTE
• Sats ≥ 95% R/A • No haemoptysis
• No trauma or surgery < 4 weeks • No exogenous oestrogen

Emergency Medicine
D-Dimer• Non specific marker of clot breakdown products
• A positive value doesn’t mean much, but a negative value means a PE/DVT is unlikely in certain patients
• Two types of assay available – high sensitivity or standard sensitivity
• D-dimer is probably not useful in pregnancy, though may be in low risk/ first trimester
Emergency Medicine

Emergency Medicine


Emergency Medicine
Myocarditis/Pericarditis
Inflammation of cardiac muscle. Huge range of aetiologies:
Viral, Rickettsia, Bacterial, Spirochetes, Fungal, Post-MI, Bites, Drugs, Chemotherapy, Antibiotics (penicillin, chloramphenicol, sulfonamides), Antihypertensives(spironolactone, methyldopa), Antiepileptics (phenytoin, carbamazepine), Amphetamines, Chemicals, Acute rheumatic fever, Systemic inflammatory diseases (SLE, Kawasaki’s, Ulcerative Colitis)…...
Emergency Medicine
Myocarditis/Pericarditis
Clinical Presentation
• Chest Pain (often characteristic)
• SOB
• Palpitations
• Syncope
• Signs of heart failure
• Features of underlying cause (eg. Viral illness preceding, stigmata of rheumatic heart disease)

Emergency Medicine
Myocarditis/Pericarditis
Investigations
• ECG – pericarditis has a classic ECG, myocarditis often has abnormalities
• FBC
• Inflammatory markers (CRP, ESR)
• Troponin – elevated in 50%
• Echocardiography

Emergency Medicine

Emergency Medicine
Oesophageal Perforation
Potentially life threatening
• Notoriously difficult to diagnose• Usually from severe vomiting• Associated with haematemesis and painful swallowing

Emergency Medicine
Spontaneous Pneumothorax
Risk factors
• Sudden onset pleuritic chest pain with SOB
• Tall, thin male
• History of asthma / COPD
• Previous pneumothorax
• Smoker
Emergency Medicine
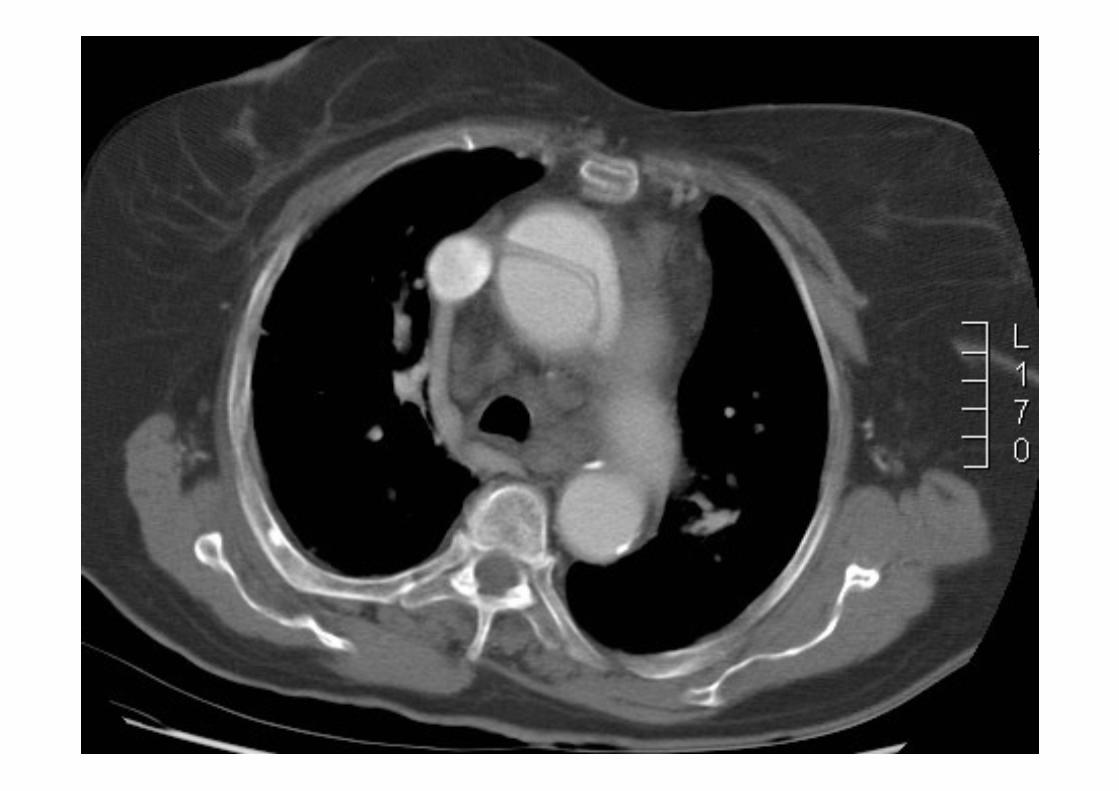
Split in the wall of the aorta and blood enters the wall
• Potentially life threatening
• Pain described as “tearing”, through to back
• Unequal blood pressures
• Radio-radio and/or radio-femoral pulse delays
• Think dissection in any patient with chest pain and some vague neurology or unusual symptom
Aortic Dissection

Emergency Medicine
Emergency Medicine

Emergency Medicine
Overview
• Chest Pain Assessment• Acute Management of ACS• Other Causes of Serious Chest Pain

Emergency Medicine