chapter25! stroke’chapter25! stroke’ ... two major categories of ischemic stroke and hemorrhagic...
TRANSCRIPT
1
Chapter 25 Stroke Stroke is the third leading cause of death in the United States, surpassed only by heart disease and cancer. It represents an enormous public health and economic burden, estimated at $62.7 billion for direct and indirect costs. The 2007 update on stroke by the American Heart Association reports the following on an annual basis:
• Each year about 700,000 people experience a new or recurrent stroke (500,000 first attack and 200,000 recurrent); by gender about 46,000 more women than men have a stroke.
• Stroke incidence in men is greater than women at younger ages, but not at older ages. The ratio of
male-‐ to-‐female incidence is 1.25 at ages 55 to 64; 1.50 at ages 65 to 74; 1.07 at ages 75 to 84, and 0.76 at age 85 and older.
• First-‐time stroke for blacks is almost double that for whites. The age-‐adjusted stroke incidence
rates at ages 45 to 84 are 6.6 per 1000 in black males versus 3.6 in white males, and 4.9 in back females versus 2.3 in white females.
• Over 150,000 deaths (58,660 males, 91,487 females) related to stroke were reported in 2004. • Eighty-‐seven percent of all strokes are ischemic and 13% result from intracerebral and
subarachnoid hemorrhage.
• In the 45-‐ to 64-‐year-‐old age group, 8% to 12% of deaths resulted from ischemic stroke and 37% to 38% from hemorrhagic stroke within 30 days.
• The death rate from stroke in 2004 was reported at 48.1 per 1,000 for white males and 73.9 per
1,000 for black males, and 47.4 per 1,000 for white females and 64.9 per 1,000 for black females.
• The longer life span of women accounts for the fact that more women than men die of stroke each year. In 2004, 61% of U.S. stroke deaths were women.
In the past 15 years, management of stroke has undergone a fundamental transformation as a result of research and technological advances, including improved pathophysiologic models of stroke to understand changes in the biochemical and cellular levels; superior neuroimaging using magnetic resonance imaging (MRI), magnetic resonance angiography (MRA), magnetic resonance with diffusion-‐weighted and perfusion-‐weighted imaging, and improved computed tomography (CT) scanning techniques; the introduction of new pharmacologic agents and techniques such as hypothermia; the definitive role of thrombolytic agents in early treatment; advances in radiologic interventional procedures, such as angioplasty, cerebrovascular stenting, and embolic protection; the preventive benefit of carotid endarterectomy in patients with symptomatic high-‐grade stenosis; neurotransplantation; and other studies and investigative tools that continue to shape and refine patient management. The term brain attack is the preferred term for the lay press to align itself with heart attack, a concept that conveys early identification of symptoms followed by emergent transport for intervention that is often life saving. An appreciation has developed of the stroke timeline associated with the development of neurological deficits and the window of opportunity that exists for reversal of neurological deficits with new interventions. Cardiac resuscitation training programs in basic life support (BLS) and advanced cardiac life support (ACLS) have been revised and now include identification of stroke symptoms and rapid action to save brain tissue as well as save cardiac muscle. Improved emergency medical services'
2
(EMS) recognition of stroke symptoms and triage and the creation of dedicated stroke centers at selected hospitals have significantly enhanced rapid stroke interventions. Arepository of guidelines related to stroke is available at the American Heart Association website. Examples of evidence-‐based guidelines include primary prevention of ischemic stroke, early management of ischemic stroke, adult stroke rehabilitation care, and other guidelines that address the management of stroke patients along a continuum of care through rehabilitation. They are available at the American Heart Association website and are updated periodically to reflect the latest scientific information to assist health care providers in providing best practices in managing patients. Other respected groups such as the Veterans Administration have also published evidence-‐based guidelines that are available at a variety of websites. Interdisciplinary clinical pathways for stroke management are the norm in practice. The emphasis is on providing coordinated care focused on stabilization through acute care and treatment with early rehabilitation of patients for optimal recovery of function and prevention of recurrent stroke. The processes of care are driven by achievement of identified outcomes that are indicators of quality. This chapter is based on the most recent guidelines available in mid-‐2007 and reflects the guidelines posted on the American Heart Association website. DISEASE-SPECIFIC CERTIFICATION: PRIMARY STROKE CENTER The Joint Commission offers a program of certification for disease-‐specific care including stroke.7 Many institutions are seeking Primary Stroke Certification to distinguish themselves within the community. Whereas some state legislatures and other accrediting organizations have assumed the role of certifying body, the most widely recognized entity for Primary Stroke Certification is the Joint Commission. With more than 50 years of established expertise, the Joint Commission developed the disease-‐specific certification for Primary Stroke Centers based on the recommendations of the Brain Attack Coalition and the statements and guidelines of the American Stroke Association. Primary Stroke Certification, in which a Certificate of Distinction in Stroke Care is awarded, is valid for 2 years. The initial review, year 1, consists of both off-‐site and on-‐site evaluations, and the second-‐year review is an off-‐site evaluation of submitted descriptive material. To be eligible for Primary Stroke Certification, specific requirements must be met. The institution seeking certification must be located within the United States, operated by the U.S. government, or operated under the charter of the U.S. Congress. The stroke program must fit the Joint Commission certified program description and be in operation for a minimum of 4 months. A voluntary process, Primary Stroke Certification Review, is focused on quality and safety within the framework of standards, guidelines, and outcomes. Organized into five domains, the standards are Delivering or Facilitating Clinical Care, Performance Measurement and Improvement, Supporting Self-‐Management, Program Management, and Clinical Information System. While the Joint Commission does not dictate which clinical practice guidelines are used, the Primary Stroke program must demonstrate the selection, implementation, and integration of the clinical practice guidelines. These guidelines should be based on the same criteria as the National Guidelines Clearinghouse. In regard to Performance Management, the performance measurement and improvement activities must have an organized approach. As of 2007, four measures of the standardized measure set that was agreed upon by the American Stroke Association, the Joint Commission, and a jointly sponsored stroke advisory panel are required for data collection. The performance measures can be found on the Joint Commission website under stroke certification.
3
PUBLIC AND PROFESSIONAL EDUCATION Stroke is a preventable health care problem; it is a treatable condition, in most cases, if treatment is prompt and evidence based. Awell-‐developed public education program is critical to have an informed public who can recognize the signs and symptoms of a stroke and know how to respond. In addition, the health care system must be organized to provide evidence-‐based care provided by stroke-‐competent health care providers. The following recommendations are made by the American Heart Association:
• Activation of the 911 system by patients and others is strongly supported because it speeds treatment of stroke.
• Public education programs to increase public awareness of stroke is supported to increase the
number of patients who can be seen and treated in the first few hours after stroke.
• Education of all health care providers and EMS personnel will increase the number of patients promptly and properly treated.
• Since EMS personnel are often the first responders, education in brief assessment according to an
established protocol will facilitate communication of information for decisions about transport to the appropriate health care facility and needed care that alerts health providers.
• It is further recommended that EMS personnel begin the initial management of stroke in the field
according to approved protocols.
• The use of a stroke identification algorithm such as the Los Angeles or Cincinnati screens is encouraged.
• Patients should be transported for evaluation and treatment to the closest facility that provides
emergency stroke care, even if it means bypassing other health care facilities not prepared to provide emergency stroke care.
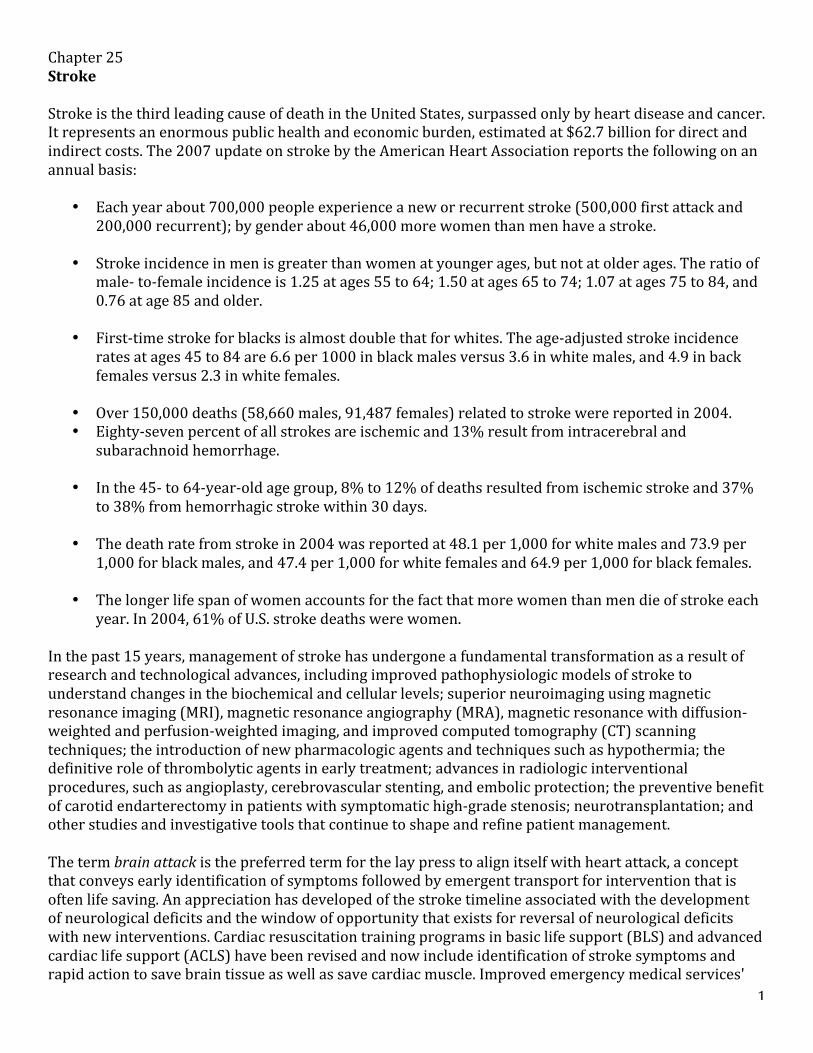
DEFINITION AND CLASSIFICATION OF STROKE Stroke is a heterogeneous, neurological syndrome characterized by gradual or rapid, nonconvulsive onset of neurological deficits that fit a known vascular territory and that last for 24 hours or more. Stroke occurs when oxygen supply to a localized area in the brain is interrupted, resulting in a series of intricate processes that lead to the destruction of neural tissue and consequent brain damage. Stroke includes cerebral infarction (ischemic stroke) and intracerebral hemorrhage and subarachnoid hemorrhage (hemorrhagic stroke). The two categories are further subdivided, as discussed later (Fig. 25-‐1). The type and severity of neurological deficits encompass a wide range and gradation of signs and symptoms. The severity and permanence of symptoms are the factors that differentiate between so-‐called minor stroke and major stroke. Classification of stroke is based on the underlying problem created within the cerebral artery. An analogy to home plumbing pipes can be made. Only two events create problems with household plumbing: plugging of the pipe so that effluence cannot proceed to its destination; and bursting or rupturing of the pipe so that fluid within the pipe flows into the surrounding areas. In the brain, plugging by atherosclerosis or a clot creates a narrow lumen, preventing adequate flow of blood to cerebral tissue. Alternatively, rupture resulting from a weakened vessel causes leakage of blood into the brain or subarachnoid space. Thus, stroke is divided into the two major categories of ischemic stroke and hemorrhagic stroke with subdivisions in each category.
4
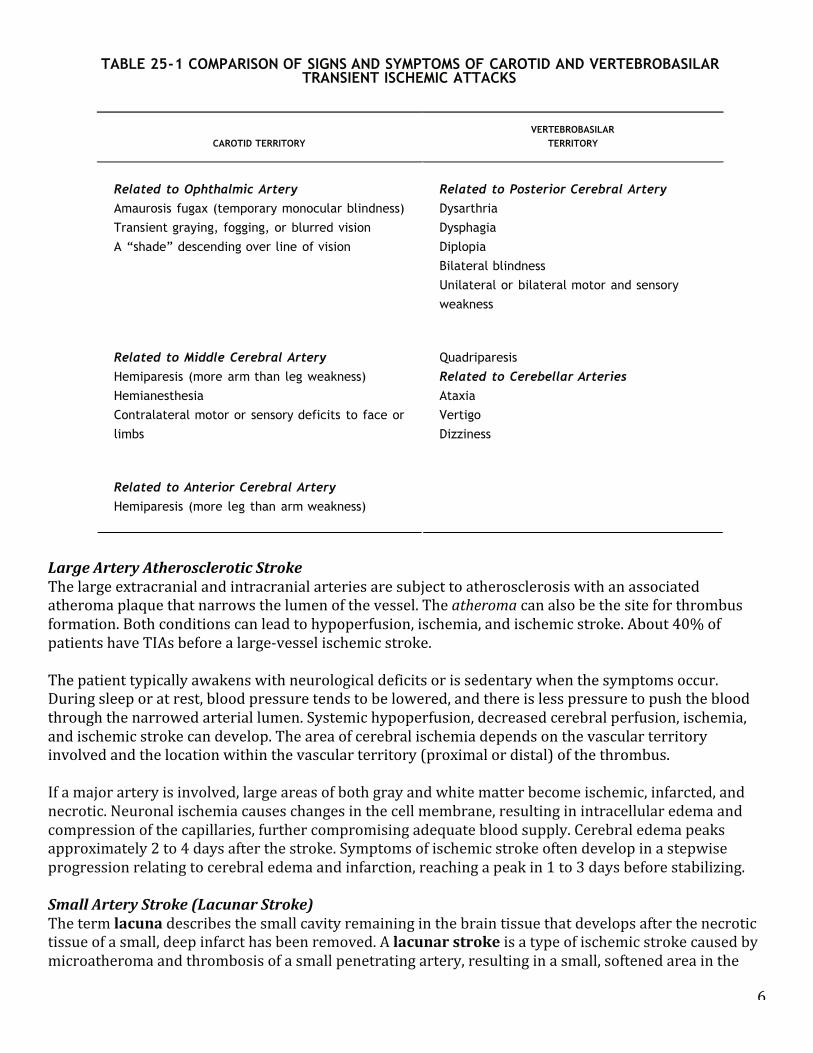
Terms Related to Cerebral Ischemic Events Transient ischemic attacks (TIAs) are temporary focal brain or retinal deficits, caused by vascular disease, which fit a known vascular territory and clear completely in less than 24 hours. Most TIAs are much shorter, reversing completely within 1 hour. TIAs are classified into TIAs associated with the carotid and TIAs associated with vertebrobasilar vascular territories. One of the most important warning signs of a stroke is a TIA. TIAs of the carotid (anterior circulation) cause lateralizing signs. When the carotid territory is involved, the symptoms reflect ischemia to the ipsilateral eye or cerebral hemisphere. A common visual deficit is called amaurosis fugax, defined as temporary blindness in one eye. Hemispherical ischemia usually causes weakness or numbness of the contralateral face or limb; language deficits and cognitive and behavioral changes may also occur. TIAs of the vertebrobasilar (posterior) circulation cause diffuse signs. When the vertebrobasilar territory is involved, the symptoms often include dysarthria, vertigo, dizziness, ataxia, abnormalities of eye movement resulting in diplopia, and unilateral or bilateral motor and sensory deficits (Table 25-‐1). A penumbra is a zone of compromised neuronal cells that are unable to function but remain viable and are located around an area of lethal injured cells; such a zone is amenable to reversal from ischemia (Fig. 25-‐2). A watershed or border zone infarction is an infarcted area that occurs between the terminal distributions of two adjacent cerebral arteries, such as the anterior cerebral and middle cerebral arteries. Because the terminal distributions are at the end of the pipeline, watershed areas are subject to low, marginally adequate arterial pressure under normal circumstances (Fig. 25-‐3). They are also the first to fail when systemic blood pressure drops further. If systemic hypotension occurs, there is failure to maintain adequate cerebral perfusion. Ischemic Stroke Ischemic stroke accounts for 87% of all strokes and is subdivided into thrombotic atherosclerotic large vessel disease (20%); small vessel (penetrating) artery disease, or “lacunae” (25%); cardiogenic embolic (20%); cryptogenic (30%); and other (5%). Note that these percentages are approximate for each category with variations noted depending on resource consulted. Atherosclerosis of large and small
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 4 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.590
stroke) and intracerebral hemorrhage and subarachnoid hemorrhage (hemorrhagic stroke). The two categoriesare further subdivided, as discussed later (Fig. 25-1). The type and severity of neurological deficits encompass awide range and gradation of signs and symptoms. The severity and permanence of symptoms are the factors thatdifferentiate between so-called minor stroke and major stroke.
Classification of stroke is based on the underlying problem created within the cerebral artery. An analogy tohome plumbing pipes can be made. Only two events create problems with household plumbing: plugging of thepipe so that effluence cannot proceed to its destination; and bursting or rupturing of the pipe so that fluidwithin the pipe flows into the surrounding areas. In the brain, plugging by atherosclerosis or a clot creates anarrow lumen, preventing adequate flow of blood to cerebral tissue. Alternatively, rupture resulting from aweakened vessel causes leakage of blood into the brain or subarachnoid space. Thus, stroke is divided into the
two major categories of ischemic stroke and hemorrhagic stroke with subdivisions in each category.
Figure 25-1 • Classification of stroke types.
Terms Related to Cerebral Ischemic Events
Transient ischemic attacks (TIAs) are temporary focal brain or retinal deficits, caused by vascular disease,which fit a known vascular territory and clear completely in less than 24 hours. Most TIAs are much shorter,reversing completely within 1 hour. TIAs are classified into TIAs associated with the carotid and TIAs associatedwith vertebrobasilar vascular territories. One of the most important warning signs of a stroke is a TIA.
TIAs of the carotid (anterior circulation) cause lateralizing signs. When the carotid territory is involved, thesymptoms reflect ischemia to the ipsilateral eye or cerebral hemisphere. A common visual deficit is calledamaurosis fugax, defined as temporary blindness in one eye. Hemispherical ischemia usually causes weakness ornumbness of the contralateral face or limb; language deficits and cognitive and behavioral changes may alsooccur. TIAs of the vertebrobasilar (posterior) circulation cause diffuse signs. When the vertebrobasilar territoryis involved, the symptoms often include dysarthria, vertigo, dizziness, ataxia, abnormalities of eye movement
5
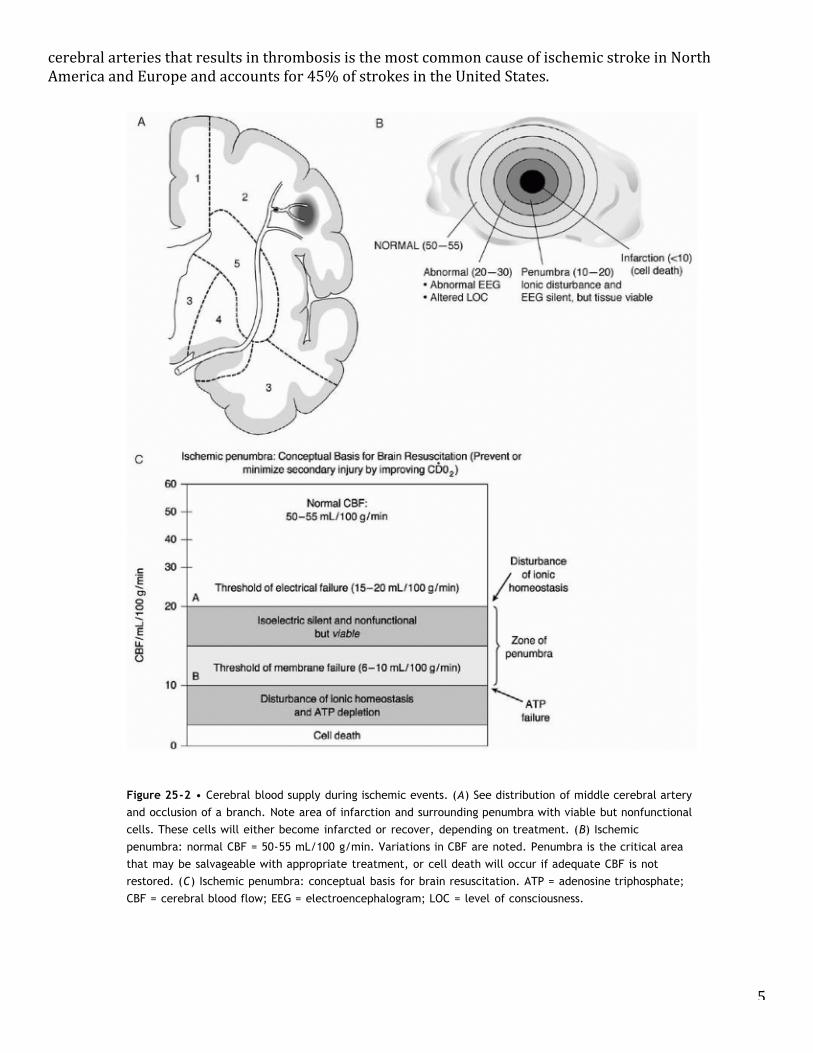
cerebral arteries that results in thrombosis is the most common cause of ischemic stroke in North America and Europe and accounts for 45% of strokes in the United States.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 6 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
Figure 25-2 • Cerebral blood supply during ischemic events. (A) See distribution of middle cerebral artery
and occlusion of a branch. Note area of infarction and surrounding penumbra with viable but nonfunctional
cells. These cells will either become infarcted or recover, depending on treatment. (B) Ischemic
penumbra: normal CBF = 50-55 mL/100 g/min. Variations in CBF are noted. Penumbra is the critical area
that may be salvageable with appropriate treatment, or cell death will occur if adequate CBF is not
restored. (C) Ischemic penumbra: conceptual basis for brain resuscitation. ATP = adenosine triphosphate;
CBF = cerebral blood flow; EEG = electroencephalogram; LOC = level of consciousness.
6
Large Artery Atherosclerotic Stroke The large extracranial and intracranial arteries are subject to atherosclerosis with an associated atheroma plaque that narrows the lumen of the vessel. The atheroma can also be the site for thrombus formation. Both conditions can lead to hypoperfusion, ischemia, and ischemic stroke. About 40% of patients have TIAs before a large-‐vessel ischemic stroke. The patient typically awakens with neurological deficits or is sedentary when the symptoms occur. During sleep or at rest, blood pressure tends to be lowered, and there is less pressure to push the blood through the narrowed arterial lumen. Systemic hypoperfusion, decreased cerebral perfusion, ischemia, and ischemic stroke can develop. The area of cerebral ischemia depends on the vascular territory involved and the location within the vascular territory (proximal or distal) of the thrombus. If a major artery is involved, large areas of both gray and white matter become ischemic, infarcted, and necrotic. Neuronal ischemia causes changes in the cell membrane, resulting in intracellular edema and compression of the capillaries, further compromising adequate blood supply. Cerebral edema peaks approximately 2 to 4 days after the stroke. Symptoms of ischemic stroke often develop in a stepwise progression relating to cerebral edema and infarction, reaching a peak in 1 to 3 days before stabilizing. Small Artery Stroke (Lacunar Stroke) The term lacuna describes the small cavity remaining in the brain tissue that develops after the necrotic tissue of a small, deep infarct has been removed. A lacunar stroke is a type of ischemic stroke caused by microatheroma and thrombosis of a small penetrating artery, resulting in a small, softened area in the
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 5 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.591
resulting in diplopia, and unilateral or bilateral motor and sensory deficits (Table 25-1).8
A penumbra is a zone of compromised neuronal cells that are unable to function but remain viable and are
located around an area of lethal injured cells; such a zone is amenable to reversal from ischemia (Fig. 25-2). A
watershed or border zone infarction is an infarcted area that occurs between the terminal distributions of two
adjacent cerebral arteries, such as the anterior cerebral and middle cerebral arteries. Because the terminal
distributions are at the end of the pipeline, watershed areas are subject to low, marginally adequate arterial
pressure under normal circumstances (Fig. 25-3). They are also the first to fail when systemic blood pressure
drops further. If systemic hypotension occurs, there is failure to maintain adequate cerebral perfusion.
Ischemic StrokeIschemic stroke accounts for 87% of all strokes and is subdivided into thrombotic atherosclerotic large vessel
disease (20%); small vessel (penetrating) artery disease, or “lacunae” (25%); cardiogenic embolic (20%);
cryptogenic (30%); and other (5%). Note that these percentages are approximate for each category with
variations noted depending on resource consulted. Atherosclerosis of large and small cerebral arteries that
results in thrombosis is the most common cause of ischemic stroke in North America and Europe and accounts
for 45% of strokes in the United States.
TABLE 25-1 COMPARISON OF SIGNS AND SYMPTOMS OF CAROTID AND VERTEBROBASILARTRANSIENT ISCHEMIC ATTACKS
CAROTID TERRITORYVERTEBROBASILAR
TERRITORY
Related to Ophthalmic Artery
Amaurosis fugax (temporary monocular blindness)
Transient graying, fogging, or blurred vision
A “shade” descending over line of vision
Related to Posterior Cerebral Artery
Dysarthria
Dysphagia
Diplopia
Bilateral blindness
Unilateral or bilateral motor and sensory
weakness
Related to Middle Cerebral Artery
Hemiparesis (more arm than leg weakness)
Hemianesthesia
Contralateral motor or sensory deficits to face or
limbs
Quadriparesis
Related to Cerebellar Arteries
Ataxia
Vertigo
Dizziness
Related to Anterior Cerebral Artery
Hemiparesis (more leg than arm weakness)
7
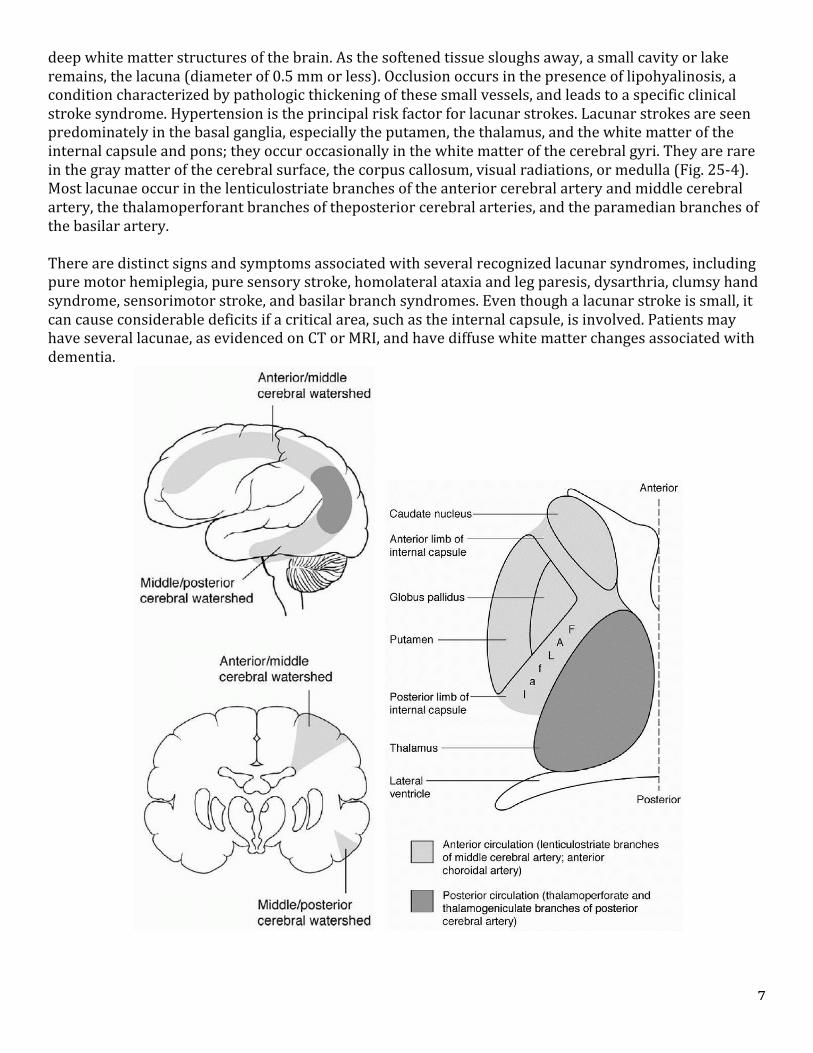
deep white matter structures of the brain. As the softened tissue sloughs away, a small cavity or lake remains, the lacuna (diameter of 0.5 mm or less). Occlusion occurs in the presence of lipohyalinosis, a condition characterized by pathologic thickening of these small vessels, and leads to a specific clinical stroke syndrome. Hypertension is the principal risk factor for lacunar strokes. Lacunar strokes are seen predominately in the basal ganglia, especially the putamen, the thalamus, and the white matter of the internal capsule and pons; they occur occasionally in the white matter of the cerebral gyri. They are rare in the gray matter of the cerebral surface, the corpus callosum, visual radiations, or medulla (Fig. 25-‐4). Most lacunae occur in the lenticulostriate branches of the anterior cerebral artery and middle cerebral artery, the thalamoperforant branches of theposterior cerebral arteries, and the paramedian branches of the basilar artery. There are distinct signs and symptoms associated with several recognized lacunar syndromes, including pure motor hemiplegia, pure sensory stroke, homolateral ataxia and leg paresis, dysarthria, clumsy hand syndrome, sensorimotor stroke, and basilar branch syndromes. Even though a lacunar stroke is small, it can cause considerable deficits if a critical area, such as the internal capsule, is involved. Patients may have several lacunae, as evidenced on CT or MRI, and have diffuse white matter changes associated with dementia.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 10 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
8
Cardiogenic Embolic Stroke About 20% of ischemic strokes result from cardiogenic embolism from atrial fibrillation (the most common), patent foramen ovale (PFO), valvular disease, ventricular thrombi, myocardial infarction, congestive heart failure, atrial septal aneurysm, and other cardiac problems. Atherosclerosis and atherogenic plaques of the proximal aorta are another source of cardiac emboli detectable with the use of transesophageal echocardiography (TEE). The atherogenic plaques commonly found in coronary vessels, in the heart, and at the bifurcation of the aorta are precursors for hypertension and atrial fibrillation. Unstable plaques can break off and become microemboli to the brain, causing stroke. Microemboli from the heart are mobilized and enter the cerebral system most often through the carotid arteries, flowing until the vessel is too narrow to allow further passage of the embolus and the vessel becomes occluded. The left middle cerebral artery is affected most often because it is a relatively straight vessel and provides the path of least resistance for the embolus. Cardiogenic strokes associated with PFO occur in approximately 20% to 25% of persons older than 30 years of age and usually occur when the patient is awake and active. The development of the ischemia is very rapid with maximal deficit present within minutes. Cryptogenic Stroke About 30% of ischemic strokes are cryptogenic in origin, which means that no cause of the stroke could be found after diagnostic evaluation. Stroke From Other Causes About 5% of ischemic strokes result from nonatherosclerotic vasculopathies, hypercoagulable states, hematologic disorders, arteritis, migraine/vasospasm, and cocaine use. Hemorrhagic Stroke Intracerebral hemorrhage (ICH), or ICH stroke, represents 13% of all strokes and involves primary rupture of a blood vessel. Although ICH represents a relatively small percentage of total strokes, it is a serious disease, with a 30-‐day mortality rate threefold to fivefold higher than that for ischemic stroke. The mortality rate in the first 30 days after ICH is 37% to 38%, with more than half of these deaths occurring in the first 2 days and 6% of patients dying before they reach the hospital. The high mortality and morbidity associated with ICH are caused primarily by the blood mass itself and by the mechanical effects it creates. Hemorrhagic stroke is divided into two categories based on the underlying mechanism. Intracerebral stroke, also called intraparenchymal stroke, is caused by bleeding into the brain tissue as a result of rupture of a small artery, most often a deep, penetrating vessel. Subarachnoid hemorrhage (SAH) is the result of bleeding into the subarachnoid space, most often in relation to a ruptured aneurysm or arteriovenous malformation—in both cases, the result of hemorrhage. In this chapter, only intracerebral hemorrhagic stroke is discussed. Cerebral aneurysms and arteriovenous malformations were addressed in Chapters 23 and 24. The cause of intracerebral hemorrhagic stroke is a spontaneous hemorrhage related to hypertension and cerebral amyloid angiopathy. The typical profile is that of an older person with a long history of poorly controlled hypertension. At the moment of hemorrhage, the person is active and usually has not experienced any warning signs. Atypical situation is one of a patient straining at stool, and then developing a severe headache, decreased consciousness, hemiplegia, and possible focal seizures and vomiting. Subarachnoid hemorrhage is commonly seen in younger people. Hemorrhagic stroke occurs rapidly, with steady development of symptoms over a period of minutes to hours (1 to 24 hours). The most common sites of intracerebral hemorrhage, each of which has distinguishing signs and symptoms, are the following: putamen (part of the basal ganglia) and adjacent internal capsule (50%); thalamus (30%); cerebellum (10%); and pons (10%).
9
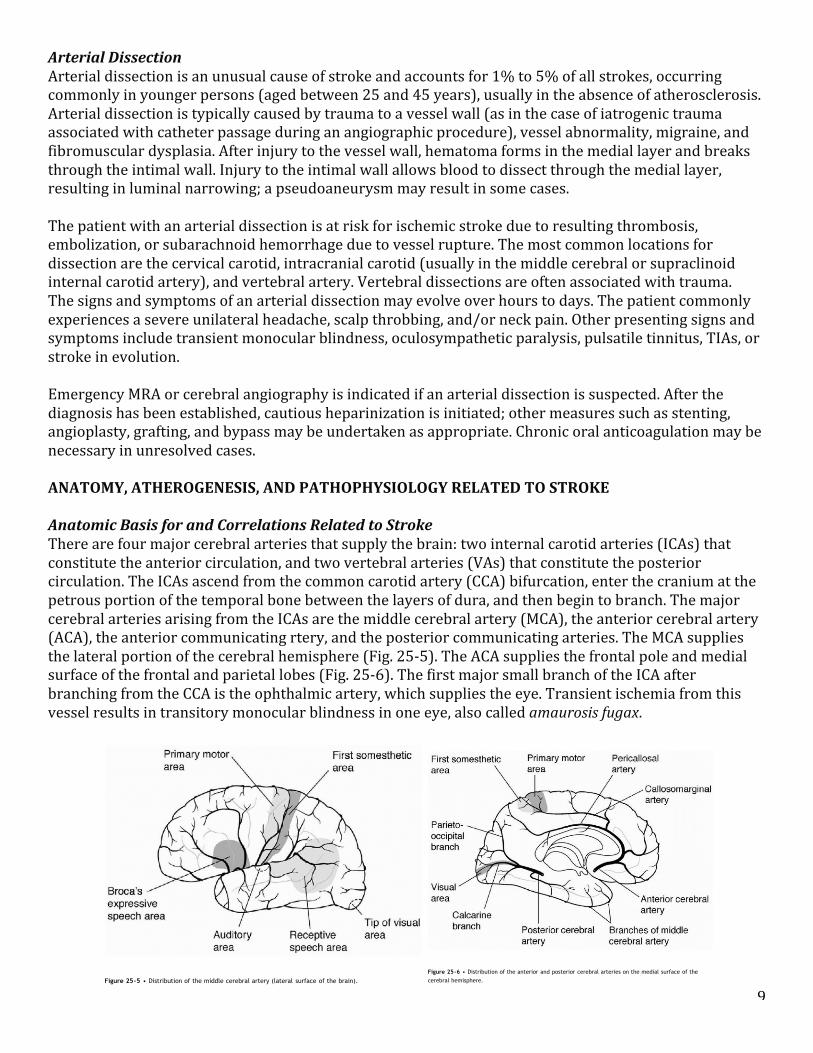
Arterial Dissection Arterial dissection is an unusual cause of stroke and accounts for 1% to 5% of all strokes, occurring commonly in younger persons (aged between 25 and 45 years), usually in the absence of atherosclerosis. Arterial dissection is typically caused by trauma to a vessel wall (as in the case of iatrogenic trauma associated with catheter passage during an angiographic procedure), vessel abnormality, migraine, and fibromuscular dysplasia. After injury to the vessel wall, hematoma forms in the medial layer and breaks through the intimal wall. Injury to the intimal wall allows blood to dissect through the medial layer, resulting in luminal narrowing; a pseudoaneurysm may result in some cases. The patient with an arterial dissection is at risk for ischemic stroke due to resulting thrombosis, embolization, or subarachnoid hemorrhage due to vessel rupture. The most common locations for dissection are the cervical carotid, intracranial carotid (usually in the middle cerebral or supraclinoid internal carotid artery), and vertebral artery. Vertebral dissections are often associated with trauma. The signs and symptoms of an arterial dissection may evolve over hours to days. The patient commonly experiences a severe unilateral headache, scalp throbbing, and/or neck pain. Other presenting signs and symptoms include transient monocular blindness, oculosympathetic paralysis, pulsatile tinnitus, TIAs, or stroke in evolution. Emergency MRA or cerebral angiography is indicated if an arterial dissection is suspected. After the diagnosis has been established, cautious heparinization is initiated; other measures such as stenting, angioplasty, grafting, and bypass may be undertaken as appropriate. Chronic oral anticoagulation may be necessary in unresolved cases. ANATOMY, ATHEROGENESIS, AND PATHOPHYSIOLOGY RELATED TO STROKE Anatomic Basis for and Correlations Related to Stroke There are four major cerebral arteries that supply the brain: two internal carotid arteries (ICAs) that constitute the anterior circulation, and two vertebral arteries (VAs) that constitute the posterior circulation. The ICAs ascend from the common carotid artery (CCA) bifurcation, enter the cranium at the petrous portion of the temporal bone between the layers of dura, and then begin to branch. The major cerebral arteries arising from the ICAs are the middle cerebral artery (MCA), the anterior cerebral artery (ACA), the anterior communicating rtery, and the posterior communicating arteries. The MCA supplies the lateral portion of the cerebral hemisphere (Fig. 25-‐5). The ACA supplies the frontal pole and medial surface of the frontal and parietal lobes (Fig. 25-‐6). The first major small branch of the ICA after branching from the CCA is the ophthalmic artery, which supplies the eye. Transient ischemia from this vessel results in transitory monocular blindness in one eye, also called amaurosis fugax.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 13 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.594
artery, and the posterior communicating arteries. The MCA supplies the lateral portion of the cerebral
hemisphere (Fig. 25-5). The ACA supplies the frontal pole and medial
surface of the frontal and parietal lobes (Fig. 25-6). The first major small branch of the ICA after branching
from the CCA is the ophthalmic artery, which supplies the eye. Transient ischemia from this vessel results in
transitory monocular blindness in one eye, also called amaurosis fugax.
Figure 25-5 • Distribution of the middle cerebral artery (lateral surface of the brain).
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 14 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
Figure 25-6 • Distribution of the anterior and posterior cerebral arteries on the medial surface of the
cerebral hemisphere.
10
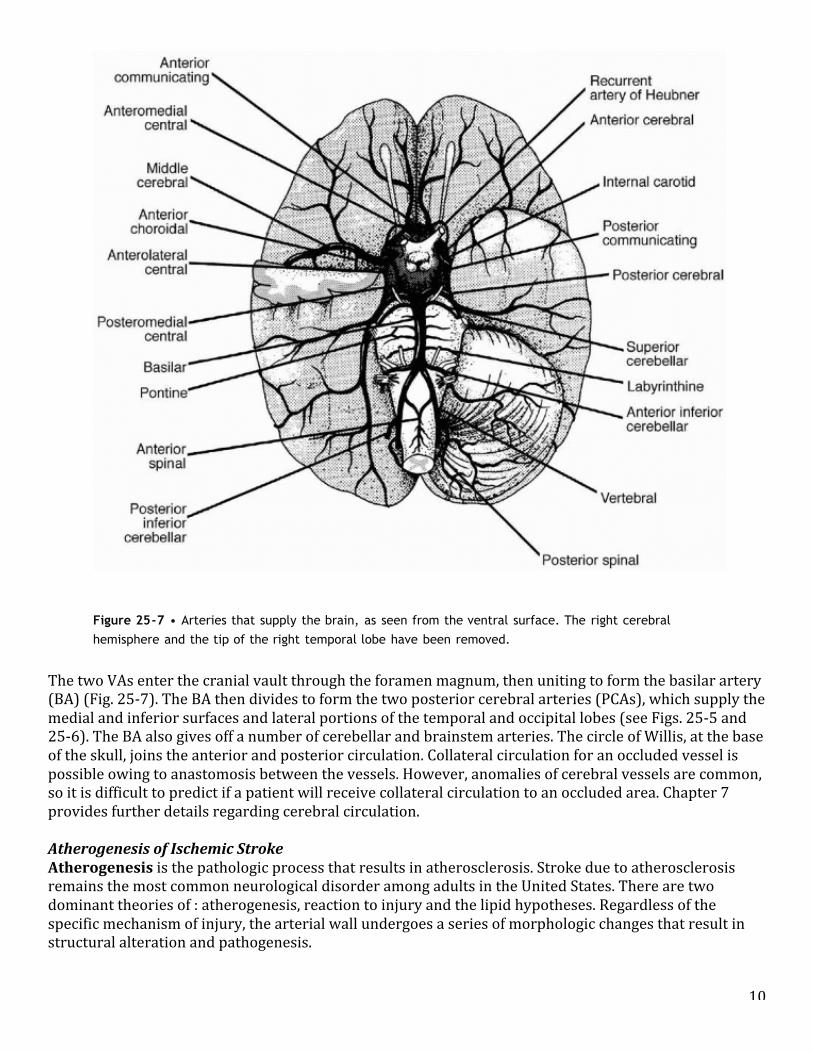
The two VAs enter the cranial vault through the foramen magnum, then uniting to form the basilar artery (BA) (Fig. 25-‐7). The BA then divides to form the two posterior cerebral arteries (PCAs), which supply the medial and inferior surfaces and lateral portions of the temporal and occipital lobes (see Figs. 25-‐5 and 25-‐6). The BA also gives off a number of cerebellar and brainstem arteries. The circle of Willis, at the base of the skull, joins the anterior and posterior circulation. Collateral circulation for an occluded vessel is possible owing to anastomosis between the vessels. However, anomalies of cerebral vessels are common, so it is difficult to predict if a patient will receive collateral circulation to an occluded area. Chapter 7 provides further details regarding cerebral circulation. Atherogenesis of Ischemic Stroke Atherogenesis is the pathologic process that results in atherosclerosis. Stroke due to atherosclerosis remains the most common neurological disorder among adults in the United States. There are two dominant theories of : atherogenesis, reaction to injury and the lipid hypotheses. Regardless of the specific mechanism of injury, the arterial wall undergoes a series of morphologic changes that result in structural alteration and pathogenesis.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 15 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.595
Figure 25-7 • Arteries that supply the brain, as seen from the ventral surface. The right cerebral
hemisphere and the tip of the right temporal lobe have been removed.
The two VAs enter the cranial vault through the foramen magnum, then uniting to form the basilar artery (BA)
(Fig. 25-7). The BA then divides to form the two posterior cerebral arteries (PCAs), which supply the medial and
inferior surfaces and lateral portions of the temporal and occipital lobes
(see Figs. 25-5 and 25-6). The BA also gives off a number of cerebellar and brainstem arteries. The circle of
Willis, at the base of the skull, joins the anterior and posterior circulation. Collateral circulation for an occluded
vessel is possible owing to anastomosis between the vessels. However, anomalies of cerebral vessels are
common, so it is difficult to predict if a patient will receive collateral circulation to an occluded area. Chapter
7 provides further details regarding cerebral circulation.
Atherogenesis of Ischemic Stroke
Atherogenesis is the pathologic process that results in atherosclerosis. Stroke due to atherosclerosis remains the
most common neurological disorder among adults in the United States. There are two dominant theories of
11
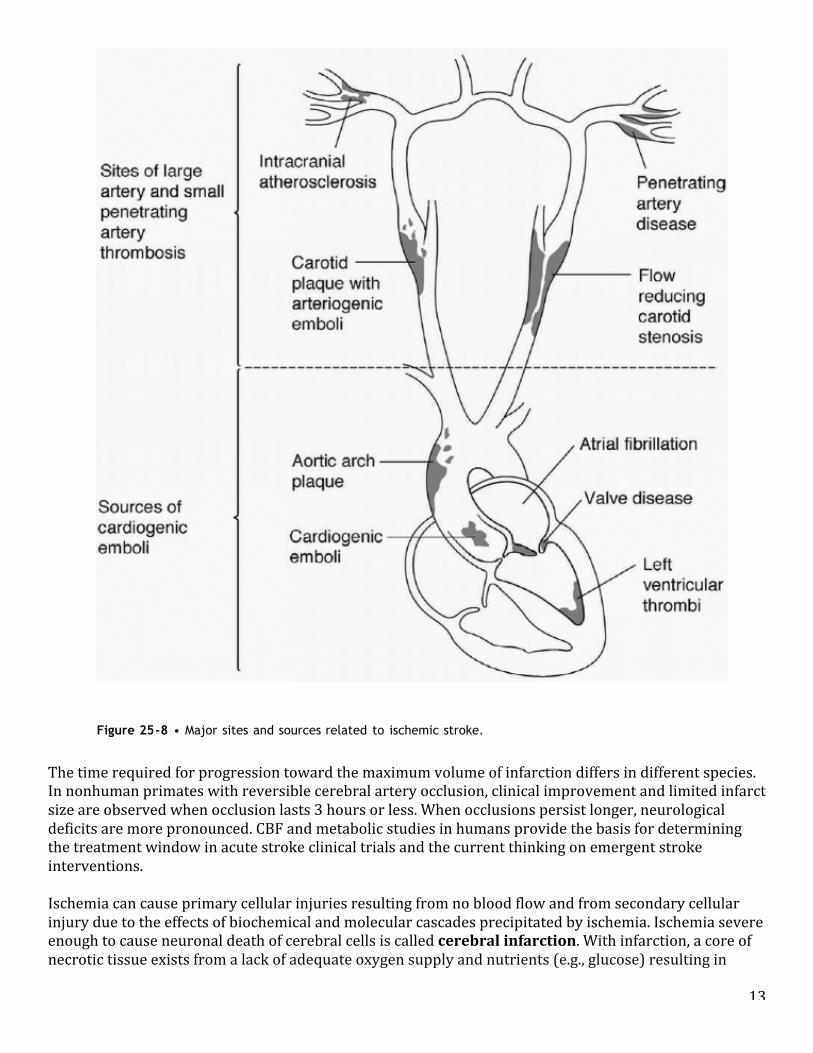
In larger vessels, the earliest lesions of atherosclerosis are seen as yellowish, fatty streaks of the intimal surface of large to medium arteries, which are widely distributed throughout the arterial vasculature and may be seen as early as late childhood or early adolescence. On microscopic examination, the fatty streaks consist of lipid-‐ laden macrophages known as foam cells (some foam cells are smooth muscle cells and some come from circulating monocytes) and extracellular lipid. Over the course of years the fatty streaks progress, and by middle to older age, fibrosis plaques (atheromas) begin to develop in more localized sites than fatty streaks, typically occurring at arterial branches or opposite arterial bifurcation of extracranial vessels. The maturated fibrous plaque consists of an intact endothelial lining overlaying a fibrous cap (containing foam cells, transformed smooth muscle cells, lymphocytes, a connective tissue matrix, and a central necrotic core of cellular debris, free extracellular lipid, and cholesterol crystals) extruding from the intima and producing varying degrees of alterations in blood flow. As plaques advance, there may be central necrosis and associated changes such as fibrosis, intraplaque hemorrhage, ulceration, and mineralization. Platelet adhesion and aggregation may occur at this later stage, increasing the plaque size. Fibrin and fibrinogen may also be incorporated into the plaque. Small arterioles, commonly observed at the plaque periphery, may be the genesis of possible hemorrhagic transformation in some fibrous plaques that contain hemosiderin, areas of intraplaque calcification, and disruption of the endothelial lining. The plaque destabilization, luminal thrombi, and endothelial injury result in clinical symptoms. Plaque enlargement occurs slowly over decades, and the person is asymptomatic until the plaque intrudes on a substantial percentage of the arterial lumen diameter. Typically, luminal thrombi are associated with luminal surface disruption or ulceration of the endothelial lining, leading to arterial obstruction. Blood within the plaque or intraplaque hemorrhage appears to be secondary to the luminal disruption, with dissection of luminal blood into the plaque. In smaller arteries, the underlying pathologic process for smaller penetrating arteries, such as the lenticulostriate arteries, basilar penetrating arteries, and medullary arteries that supply deep cerebral white matter, is different than for atherosclerosis found in the larger arteries. The underlying pathologic changes in the small penetrating arteries are attributable to a process called lipohyalinosis, in which a hyaline-‐lipid material coats the small penetrating arteries causing thickening of the walls. Eventually, the vessel thromboses create a lacunar stroke. Pathophysiology of Ischemic Stroke The pathophysiology of ischemic stroke due to atheromas, thrombi, or emboli is the same. The lumen of the blood vessel becomes narrowed or occluded, resulting in ischemia in that vascular territory (Fig. 25-‐8). As shown mainly in animal models, occlusion seldom completely abolishes the delivery of oxygen and glucose to the affected vascular territory because cerebral blood flow (CBF) to the affected vascular territory is usually partly maintained by dense vascular collaterals. Normally, the rate of CBF to the entire brain is relatively constant, and it does not change in response to alterations in mean systemic blood pressure over a range of 50 to 150 mm Hg. This phenomenon, known as autoregulation, protects the brain from possible hypotension or cerebrovascular hemorrhage caused by excessive intravascular pressure. The severity of neuronal injury in ischemic brain tissue is proportional to the reduction of CBF (Table 25-‐2). In the center of an infarct, blood flow is greatly reduced or absent, whereas at its margin, maximum vasodilation results from the lactic acid formed during anaerobic glycolysis. When CO2 is inhaled or a cerebral vasodilator is administered to patients with focal infarction, only the vessels in normal areas of the brain dilate, resulting in an intracerebral steal of blood away from the infarcted zone. This same phenomenon can result if hypertension is treated too aggressively during an acute infarct. Judicious use of antihypertensive agents is critical during an
12
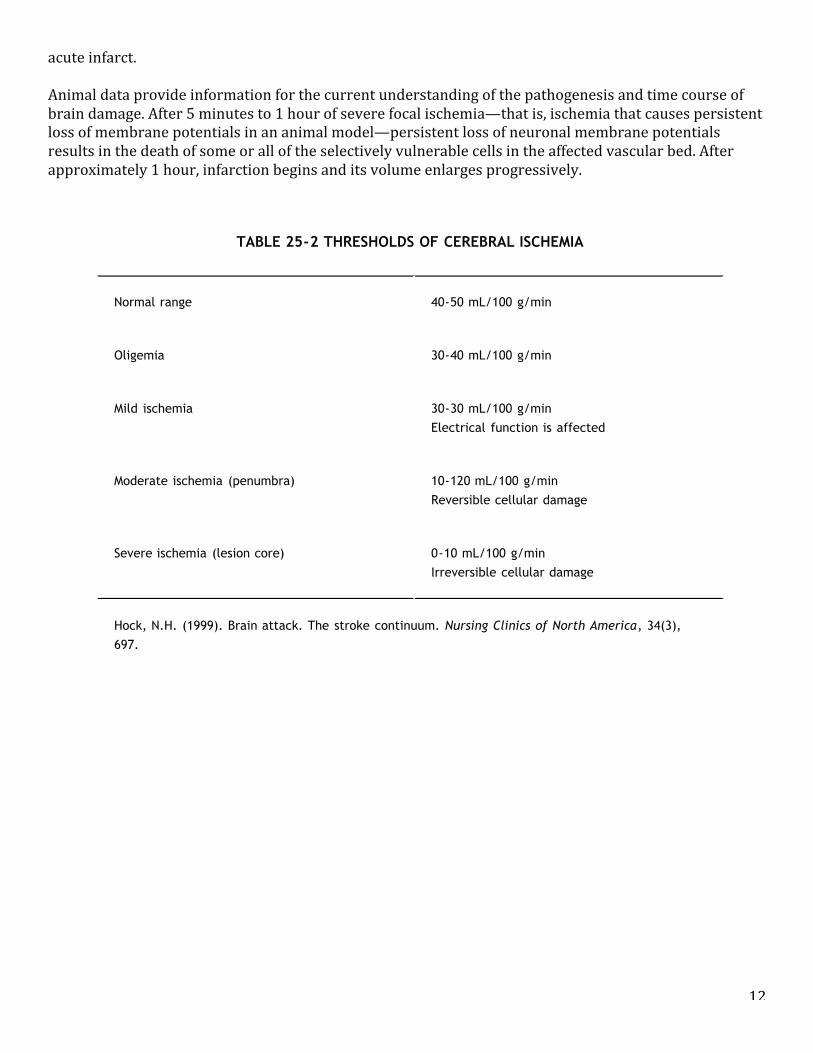
acute infarct. Animal data provide information for the current understanding of the pathogenesis and time course of brain damage. After 5 minutes to 1 hour of severe focal ischemia—that is, ischemia that causes persistent loss of membrane potentials in an animal model—persistent loss of neuronal membrane potentials results in the death of some or all of the selectively vulnerable cells in the affected vascular bed. After approximately 1 hour, infarction begins and its volume enlarges progressively.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 17 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.596
cerebral vasodilator is administered to patients with focal infarction, only the vessels in normal areas of thebrain dilate, resulting in an intracerebral steal of blood away from the infarcted zone. This same phenomenoncan result if hypertension is treated too aggressively during an acute infarct. Judicious use of antihypertensiveagents is critical during an acute infarct.
Animal data provide information for the current understanding of the pathogenesis and time course of braindamage. After 5 minutes to 1 hour of severe focal ischemia—that is, ischemia that causes persistent loss ofmembrane potentials in an animal model—persistent loss of neuronal membrane potentials results in the deathof some or all of the selectively vulnerable cells in the affected vascular bed. After
approximately 1 hour, infarction begins and its volume enlarges progressively.15
TABLE 25-2 THRESHOLDS OF CEREBRAL ISCHEMIA
Normal range 40-50 mL/100 g/min
Oligemia 30-40 mL/100 g/min
Mild ischemia 30-30 mL/100 g/minElectrical function is affected
Moderate ischemia (penumbra) 10-120 mL/100 g/minReversible cellular damage
Severe ischemia (lesion core) 0-10 mL/100 g/minIrreversible cellular damage
Hock, N.H. (1999). Brain attack. The stroke continuum. Nursing Clinics of North America, 34(3),697.
13
The time required for progression toward the maximum volume of infarction differs in different species. In nonhuman primates with reversible cerebral artery occlusion, clinical improvement and limited infarct size are observed when occlusion lasts 3 hours or less. When occlusions persist longer, neurological deficits are more pronounced. CBF and metabolic studies in humans provide the basis for determining the treatment window in acute stroke clinical trials and the current thinking on emergent stroke interventions. Ischemia can cause primary cellular injuries resulting from no blood flow and from secondary cellular injury due to the effects of biochemical and molecular cascades precipitated by ischemia. Ischemia severe enough to cause neuronal death of cerebral cells is called cerebral infarction. With infarction, a core of necrotic tissue exists from a lack of adequate oxygen supply and nutrients (e.g., glucose) resulting in
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 18 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
Figure 25-8 • Major sites and sources related to ischemic stroke.
The time required for progression toward the maximum volume of infarction differs in different species. In
nonhuman primates with reversible cerebral artery occlusion, clinical improvement and limited infarct size are
observed when occlusion lasts 3 hours or less. When occlusions persist longer, neurological deficits are more
pronounced. CBF and metabolic studies in humans provide the basis for determining the treatment window in
acute stroke clinical trials and the current thinking on emergent stroke interventions.
Ischemia can cause primary cellular injuries resulting from no blood flow and from secondary cellular injury due
to the effects of biochemical and molecular cascades precipitated by ischemia. Ischemia severe enough to cause
neuronal death of cerebral cells is called cerebral infarction. With infarction, a core of necrotic tissue exists
14
rapid depletion of energy stores. However, around the necrotic core is another circumscribed area called the ischemic penumbra (see Fig. 25-‐2). Although the neuronal cells of the penumbra do not function normally due to a decreased blood supply, they remain viable. However, cells in this region die if reperfusion is not re-‐established. The penumbra is the target for pharmacologic interventions to re-‐establish adequate perfusion, thus salvaging neuronal cells from infarction. Neuroprotective agents, including the use of mild to moderate brain cooling, are being tested in clinical trials to assess their safety and efficacy in protecting the cells from the secondary injury associated with ischemia. Thus far, there are no drugs tested that provide neuroprotection against ischemia. The blood supply to the brain can be compromised due to the so-‐called no-‐flow phenomenon (e.g., following cardiac arrest resulting in global ischemia) or a low-‐flow phenomenon (e.g., following stroke resulting in focal ischemia). Lowperfusion states can result in more tissue damage than noperfusion states because the presence of glucose in an inadequately oxygenated area enhances lactate production. Brain tissue lactate causes severe tissue necrosis and extracellular acidosis that result in infarction. In addition, low-‐flow states provide a continued supply of both water, which exacerbates edema, and activated white blood cells, platelets, and coagulation factors, which contribute to tissue damage by further impeding the microcirculation. Secondary cellular injury associated with ischemia occurs in response to deprivation of oxygen and cessation of oxidative metabolism. Complex biochemical and molecular cascades result in ischemic damage to neurons. From 2 and 5 minutes of complete oxygen deprivation is the general benchmark for irreversible neuronal damage. However, extreme hypothermia can significantly increase the viability time, and hypothermia has been used therapeutically to save neurons. Without oxygen, adenosine triphosphate (ATP) energy-‐dependent cell functions (e.g., the cellular respiratory chain, lipid metabolism, and maintenance of the transmembrane ion channels) rapidly cease. Impairment of the respiratory chain results in anaerobic glycolysis of remaining available glucose. Anaerobic glycolysis proceeds only to pyruvate, which reduces to lactate. Lactic acid and free fatty acid accumulation causes intracellular acidosis, further inhibiting mitochondrial function. Concurrently, other cell destruction processes occur that include excitotoxicity, increased intracellular calcium, and generation of free radicals. Hypoxia impairs the reuptake of the excitatory neurotransmitter glutamate at the presynaptic membrane. The excessive extracellular glutamate opens sodium, chloride, and calcium channels, resulting in an influx of sodium and chloride ions with water into the cell, causing acute cellular swelling; the voltage-‐dependent calcium channels allow influx of calcium into the cytosol and efflux of potassium. (Intracellular calcium is normally maintained at a low level by active transport mechanisms.) The high intracellular calcium activates calcium-‐dependent degradative enzymes (proteases, phospholipases, and endonucleases) that attack the cell membranes and DNA and further inhibit mitochondrial function. Oxygen free radicals with resultant lipid peroxidation occur in inadequately perfused areas and during reperfusion of previously ischemic areas. Oxygen free radicals, superoxide peroxide, and hydroxyl ions destroy fatty acids and disrupt calcium homeostasis, further contributing to cellular demise. Approximately 8 to 12 hours after the insult, the neuron becomes smaller and more angular. The cytoplasm and nucleus shrink, followed by complete dissolution of the cell and cell death. The ischemic cascade and cellular changes that follow oxygen deprivation are outlined earlier in this chapter. Reperfusion Injury in Stroke During ischemia, hypoxic cell injury and death occur distal to the occluded vessel. The injured and dying cells produce proinflammatory mediators that cause inflammation in the area around the infarction. As inflammation subsides, scar tissue develops in the infarcted region. Neurons that have died are replaced by fibrogliotic scar tissue, and neurological function is lost.
15
Another type of injury to neurons results from reperfusion to previously ischemic areas. The cellular injury due to activated oxygen free radicals that occurs after the blood supply to the ischemic area has been restored is called reperfusion injury. Although reperfusion has been shown to be beneficial in experimental systems, evidence suggests that the process of reperfusion may also injure the ischemic brain. This injury involves acute inflammation in the ischemic tissue. During periods of ischemia, endothelial cells secrete many proinflammatory cytokines that attract and activate leukocytes. When reperfusion occurs, neutrophils migrate through the vessel wall into the ischemic brain tissue, potentially releasing various toxic substances, such as oxygen free radicals and proteinases, that may further injure the compromised but viable tissue. Oxygen free radicals, which are partially reduced oxygen molecules that are highly reactive with other molecules, are implicated in postischemic membrane injury. The accumulation of adenosine diphosphate (ADP) and pyruvate during ischemia results in rapid production of electrons when the oxygen supply is re-‐established. The oxygen free radicals are formed when the electrons are transferred to oxygen. They allegedly injure the cell membrane by stealing hydrogen molecules and by forming abnormal molecular bonds. As a result of reperfusion injury, additional injury to neuronal cells is incurred. Although reperfusion is best exemplified by the use of thrombolytic therapy, it is also likely to be relevant even without pharmacologic thrombolysis. Advanced imaging studies have demonstrated increased uptake in the brain following a stroke and correlate with neurological outcome. Presumably, circulating leukocytes reach the infarcted area as a result of either spontaneous reperfusion or collateral circulation. It is important to note that when pharmacologic thrombolytic therapy is used, the patient may manifest new or identical stroke symptoms after a successful recanalization. It is therefore critical to observe the patient for reperfusion injury following thrombolytic therapy. Another example of perfusion injury is the natural break-‐up of an embolic thrombus and the onset of expanded deficits. Pathophysiology of Hemorrhagic Stroke The pathophysiology of hemorrhagic stroke is associated with an immediate rise in intracranial pressure (ICP), ischemic cellular responses, cerebral edema, compromised cerebral perfusion pressure, and possible herniation. With ICH, the usual hemorrhage sites are small, deep cortical arteries or subarachnoid hemorrhage due to aneurysmal rupture (see Chap. 23). At the time of ICH, blood is forced into the surrounding cerebral parenchyma, creating a hematoma. The pathology is dynamic and continues to evolve over the first few days after onset. In 20% to 30% of cases, clot volume increases over the first 24 hours. The hematoma displaces and compresses the adjacent cerebral tissue, and ischemic cellular responses and cerebral edema occur, resulting in increased ICP. The final outcome of ICH could also include potential neurotoxicity from the blood degradation products and associated neuronal ischemia. A major ICH can cause midline displacement and herniation syndromes and has a high mortality rate of about 50%. Hemorrhagic Conversion of an Ischemic Stroke An embolus that represents all or part of a thrombus has a spontaneous tendency to lysis and dispersion; thrombotic occlusions may also lyse spontaneously. In hemorrhagic infarction, or hemorrhagic conversion or transformation, varying amounts of red blood cells are found among the necrotic tissues, with hemorrhagic foci ranging from a few scattered petechiae to petechial hemorrhages that merge to form a significant hemorrhagic mass. The timing of hemorrhagic infarction varies from a few hours to as late as 2 weeks or longer after an arterial occlusion. Surges of arterial hypertension or rapid rise of blood pressure might explain hemorrhagic infarction in many cases. Marked hyperglycemia has also been implicated in some cases.23 Examination of biochemical changes that correlate with hemorrhage into infarcts suggested that marked tissue energy depletion accompanied by acidosis damages brain vessels and renders them penetrable by edema fluid and, ultimately, red blood cell extravasation.
16
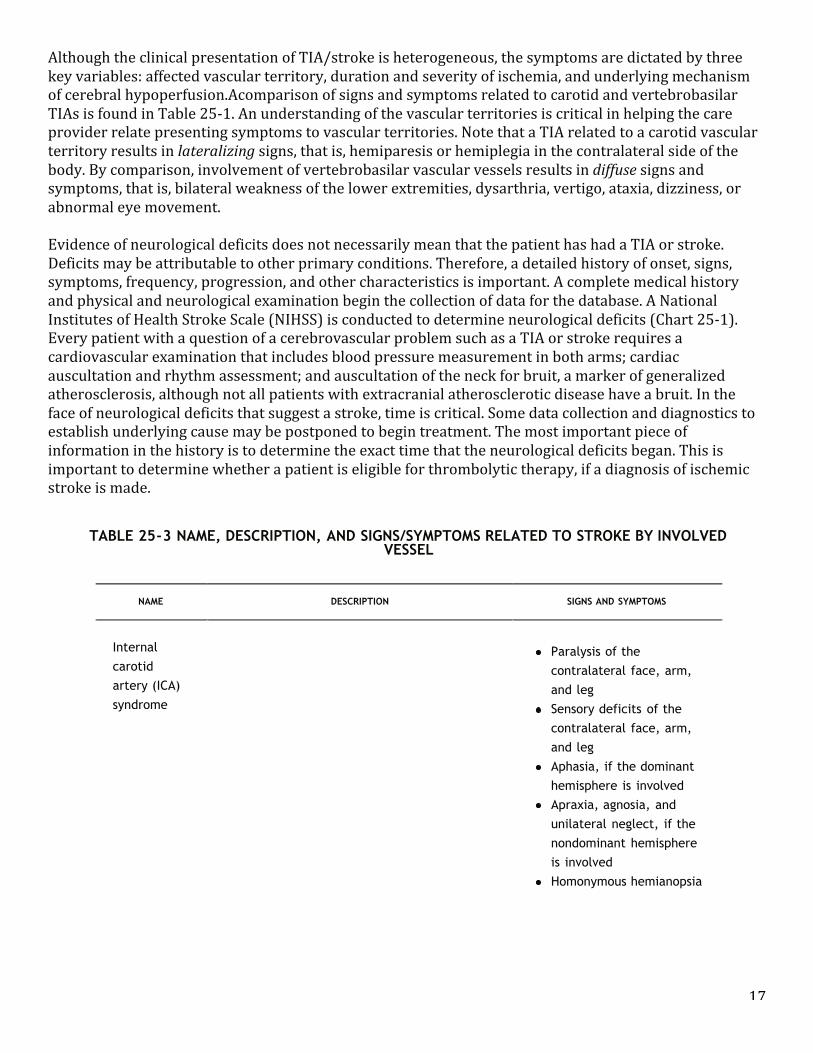
SIGNS AND SYMPTOMS OF STROKE SYNDROMES ACCORDING TO THE INVOLVED VESSEL The presenting signs and symptoms of stroke depend on the extent of CBF compromise and the particular cerebral vessel involved. When a cerebral artery is occluded by a thrombus or embolus, classic syndromes are said to develop. The clinical features of stroke are commonly classified as carotid artery (anterior circulation) syndromes and vertebrobasilar (posterior circulation) syndromes. Table 25-‐3 summarizes the signs and symptoms associated with stroke according the cerebral vessel involved. Comparison of Left-Sided and Right-Sided Stroke Some generalizations can be made about the deficits incurred with left-‐sided and right-‐sided stroke (Table 25-‐ 4). A stroke is a form of cerebral injury. The injury to the brain results from ischemia that develops over time or suddenly, as may be the case in thrombotic or embolic strokes, or from a ruptured blood vessel, in the case of hemorrhagic stroke. In all cases of stroke, areas of the brain are deprived of an adequate oxygen supply. The particular type and degree of neurological deficits incurred depends on the particular area of the brain involved, because the brain is composed of the most highly specialized tissue in the body. If the blood supply is cut off for an extended period, the involved cerebral tissue may become necrotic, resulting in permanent neurological deficits. In instances of ischemia, temporary neurological impairment may result. Diagnostics for Transient Ischemic Attack or Stroke Anumber of diagnostic studies are useful for the investigation of TIA and stroke patients. Diagnostic testing proceeds in a stepwise fashion. When the most common tests fail to uncover the cause of the stroke, other less common tests are ordered. For example, stroke in a young person without the usual stroke risk factors suggests other causes such as PFO or antiphospholipid abnormalities. Table 25-‐5 describes the commonly recommended diagnostic procedures and laboratory tests. Initially, the following tests are recommended for all patients: noncontrast brain CT or brain MRI, blood glucose, electrolytes, renal function tests (blood urea nitrogen, creatinine), complete blood count (CBC), platelets, prothrombin time/international normalized ratio (INR), activated partial thromboplastin time, and markers of cardiac ischemia. Oxygen saturation is also monitored. Selected patients may require hepatic function tests, toxicology screen, blood alcohol level, pregnancy test, arterial blood gases, chest x-‐ray (only if lung disease is suspected), and lumbar puncture (only if subarachnoid hemorrhage is suspected and a CT scan is negative for blood). Other tests may be ordered in the course of treatment for special reasons. Besides neuroimaging tests (CT or MRI), blood flow studies (transcranial Doppler) may be ordered. If a vascular anomaly is suspected, a cerebral angiography or MRA may be ordered. Recent reports recommend replacement of CT with MRI as the primary neuroimaging technique for evaluation of acute stroke. The multimodal MRI provides more information about brain ischemic pathophysiology, can localize perfusion deficits and ischemic injury including the penumbra within minutes after onset of ischemia, and are useful to guide treatment decisions. Diffusion-‐weighted imaging (DWI) and perfusion-‐weighted imaging (PWI) are distinctly different techniques; they are interrelated physiologic parameters, and both are usually performed during the same MRI examination. However, the standard initial diagnostic imaging procedure is an emergency CT scan without contrast medium to differentiate ischemic stroke from hemorrhagic stroke. Finally, diagnostics associated with cardiovascular risk may be ordered. These tests may include electrocardiogram (ECG) and possibly transthoracic echocardiography (TTE), TEE, or 24-‐hour ambulatory ECG. If continuing to pursue a cardiogenic source (for silent myocardial ischemia), an exercise ECG or a thallium perfusion may be ordered. The history of the present illness, past medical history including risk factors, and neurological examination are critical for diagnosis (Table 25-‐6).
17
Although the clinical presentation of TIA/stroke is heterogeneous, the symptoms are dictated by three key variables: affected vascular territory, duration and severity of ischemia, and underlying mechanism of cerebral hypoperfusion.Acomparison of signs and symptoms related to carotid and vertebrobasilar TIAs is found in Table 25-‐1. An understanding of the vascular territories is critical in helping the care provider relate presenting symptoms to vascular territories. Note that a TIA related to a carotid vascular territory results in lateralizing signs, that is, hemiparesis or hemiplegia in the contralateral side of the body. By comparison, involvement of vertebrobasilar vascular vessels results in diffuse signs and symptoms, that is, bilateral weakness of the lower extremities, dysarthria, vertigo, ataxia, dizziness, or abnormal eye movement. Evidence of neurological deficits does not necessarily mean that the patient has had a TIA or stroke. Deficits may be attributable to other primary conditions. Therefore, a detailed history of onset, signs, symptoms, frequency, progression, and other characteristics is important. A complete medical history and physical and neurological examination begin the collection of data for the database. A National Institutes of Health Stroke Scale (NIHSS) is conducted to determine neurological deficits (Chart 25-‐1). Every patient with a question of a cerebrovascular problem such as a TIA or stroke requires a cardiovascular examination that includes blood pressure measurement in both arms; cardiac auscultation and rhythm assessment; and auscultation of the neck for bruit, a marker of generalized atherosclerosis, although not all patients with extracranial atherosclerotic disease have a bruit. In the face of neurological deficits that suggest a stroke, time is critical. Some data collection and diagnostics to establish underlying cause may be postponed to begin treatment. The most important piece of information in the history is to determine the exact time that the neurological deficits began. This is important to determine whether a patient is eligible for thrombolytic therapy, if a diagnosis of ischemic stroke is made.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 23 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
neurological deficits that suggest a stroke, time is critical. Some data collection and diagnostics to establish
underlying cause may be postponed to begin treatment. The most important piece of information in the history
is to determine the exact time that the neurological deficits began. This is important to determine whether a
patient is eligible for thrombolytic therapy, if a diagnosis of ischemic stroke is made.
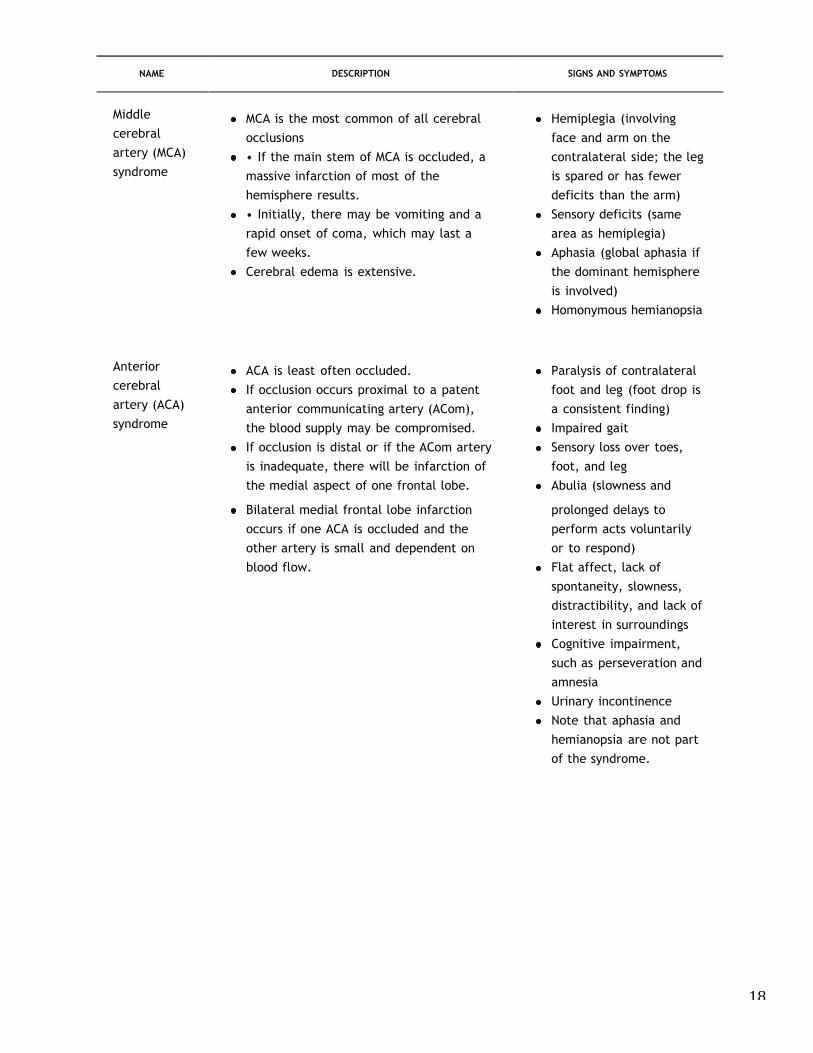
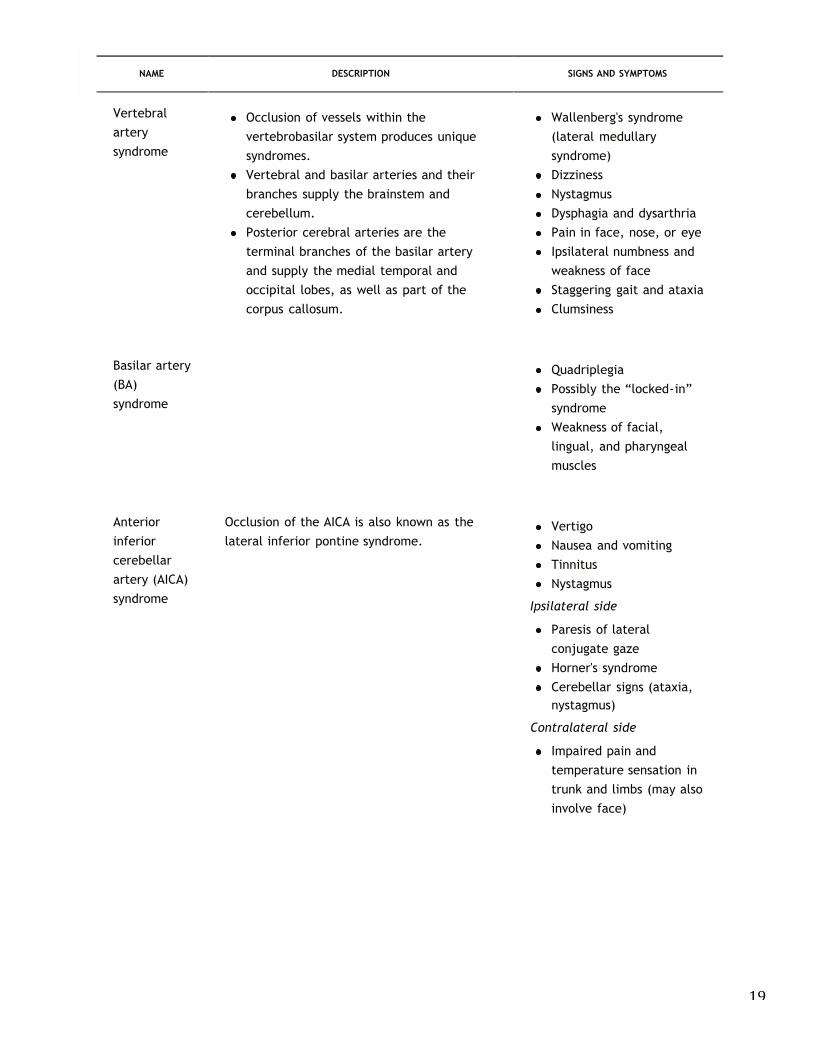
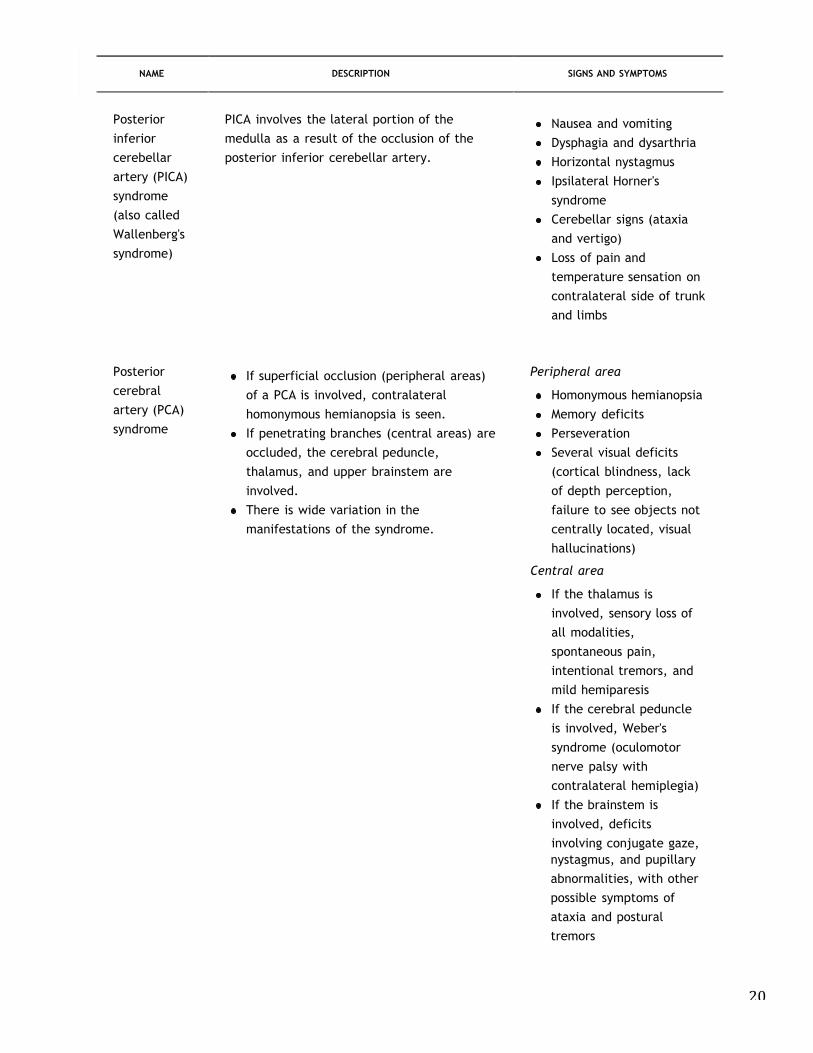
TABLE 25-3 NAME, DESCRIPTION, AND SIGNS/SYMPTOMS RELATED TO STROKE BY INVOLVEDVESSEL
NAME DESCRIPTION SIGNS AND SYMPTOMS
Internal
carotid
artery (ICA)
syndrome
Paralysis of the
contralateral face, arm,
and leg
Sensory deficits of the
contralateral face, arm,
and leg
Aphasia, if the dominant
hemisphere is involved
Apraxia, agnosia, and
unilateral neglect, if the
nondominant hemisphere
is involved
Homonymous hemianopsia
Middle
cerebral
artery (MCA)
syndrome
MCA is the most common of all cerebral
occlusions
• If the main stem of MCA is occluded, a
massive infarction of most of the
hemisphere results.
• Initially, there may be vomiting and a
rapid onset of coma, which may last a
few weeks.
Cerebral edema is extensive.
Hemiplegia (involving
face and arm on the
contralateral side; the leg
is spared or has fewer
deficits than the arm)
Sensory deficits (same
area as hemiplegia)
Aphasia (global aphasia if
the dominant hemisphere
is involved)
Homonymous hemianopsia
Anterior
cerebral
artery (ACA)
syndrome
ACA is least often occluded.
If occlusion occurs proximal to a patent
anterior communicating artery (ACom),
the blood supply may be compromised.
If occlusion is distal or if the ACom artery
is inadequate, there will be infarction of
the medial aspect of one frontal lobe.
Paralysis of contralateral
foot and leg (foot drop is
a consistent finding)
Impaired gait
Sensory loss over toes,
foot, and leg
Abulia (slowness and
18
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 23 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
neurological deficits that suggest a stroke, time is critical. Some data collection and diagnostics to establish
underlying cause may be postponed to begin treatment. The most important piece of information in the history
is to determine the exact time that the neurological deficits began. This is important to determine whether a
patient is eligible for thrombolytic therapy, if a diagnosis of ischemic stroke is made.
TABLE 25-3 NAME, DESCRIPTION, AND SIGNS/SYMPTOMS RELATED TO STROKE BY INVOLVEDVESSEL
NAME DESCRIPTION SIGNS AND SYMPTOMS
Internal
carotid
artery (ICA)
syndrome
Paralysis of the
contralateral face, arm,
and leg
Sensory deficits of the
contralateral face, arm,
and leg
Aphasia, if the dominant
hemisphere is involved
Apraxia, agnosia, and
unilateral neglect, if the
nondominant hemisphere
is involved
Homonymous hemianopsia
Middle
cerebral
artery (MCA)
syndrome
MCA is the most common of all cerebral
occlusions
• If the main stem of MCA is occluded, a
massive infarction of most of the
hemisphere results.
• Initially, there may be vomiting and a
rapid onset of coma, which may last a
few weeks.
Cerebral edema is extensive.
Hemiplegia (involving
face and arm on the
contralateral side; the leg
is spared or has fewer
deficits than the arm)
Sensory deficits (same
area as hemiplegia)
Aphasia (global aphasia if
the dominant hemisphere
is involved)
Homonymous hemianopsia
Anterior
cerebral
artery (ACA)
syndrome
ACA is least often occluded.
If occlusion occurs proximal to a patent
anterior communicating artery (ACom),
the blood supply may be compromised.
If occlusion is distal or if the ACom artery
is inadequate, there will be infarction of
the medial aspect of one frontal lobe.
Paralysis of contralateral
foot and leg (foot drop is
a consistent finding)
Impaired gait
Sensory loss over toes,
foot, and leg
Abulia (slowness and
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 23 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
neurological deficits that suggest a stroke, time is critical. Some data collection and diagnostics to establish
underlying cause may be postponed to begin treatment. The most important piece of information in the history
is to determine the exact time that the neurological deficits began. This is important to determine whether a
patient is eligible for thrombolytic therapy, if a diagnosis of ischemic stroke is made.
TABLE 25-3 NAME, DESCRIPTION, AND SIGNS/SYMPTOMS RELATED TO STROKE BY INVOLVEDVESSEL
NAME DESCRIPTION SIGNS AND SYMPTOMS
Internal
carotid
artery (ICA)
syndrome
Paralysis of the
contralateral face, arm,
and leg
Sensory deficits of the
contralateral face, arm,
and leg
Aphasia, if the dominant
hemisphere is involved
Apraxia, agnosia, and
unilateral neglect, if the
nondominant hemisphere
is involved
Homonymous hemianopsia
Middle
cerebral
artery (MCA)
syndrome
MCA is the most common of all cerebral
occlusions
• If the main stem of MCA is occluded, a
massive infarction of most of the
hemisphere results.
• Initially, there may be vomiting and a
rapid onset of coma, which may last a
few weeks.
Cerebral edema is extensive.
Hemiplegia (involving
face and arm on the
contralateral side; the leg
is spared or has fewer
deficits than the arm)
Sensory deficits (same
area as hemiplegia)
Aphasia (global aphasia if
the dominant hemisphere
is involved)
Homonymous hemianopsia
Anterior
cerebral
artery (ACA)
syndrome
ACA is least often occluded.
If occlusion occurs proximal to a patent
anterior communicating artery (ACom),
the blood supply may be compromised.
If occlusion is distal or if the ACom artery
is inadequate, there will be infarction of
the medial aspect of one frontal lobe.
Paralysis of contralateral
foot and leg (foot drop is
a consistent finding)
Impaired gait
Sensory loss over toes,
foot, and leg
Abulia (slowness and5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 24 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
Bilateral medial frontal lobe infarctionoccurs if one ACA is occluded and theother artery is small and dependent onblood flow.
prolonged delays toperform acts voluntarilyor to respond)Flat affect, lack ofspontaneity, slowness,distractibility, and lack ofinterest in surroundingsCognitive impairment,such as perseveration andamnesiaUrinary incontinenceNote that aphasia andhemianopsia are not partof the syndrome.
Vertebralarterysyndrome
Occlusion of vessels within thevertebrobasilar system produces uniquesyndromes.Vertebral and basilar arteries and theirbranches supply the brainstem andcerebellum.Posterior cerebral arteries are theterminal branches of the basilar arteryand supply the medial temporal andoccipital lobes, as well as part of thecorpus callosum.
Wallenberg's syndrome(lateral medullarysyndrome)DizzinessNystagmusDysphagia and dysarthriaPain in face, nose, or eyeIpsilateral numbness andweakness of faceStaggering gait and ataxiaClumsiness
Basilar artery(BA)syndrome
QuadriplegiaPossibly the “locked-in”syndromeWeakness of facial,lingual, and pharyngealmuscles
Anteriorinferiorcerebellarartery (AICA)syndrome
Occlusion of the AICA is also known as thelateral inferior pontine syndrome.
VertigoNausea and vomitingTinnitusNystagmus
Ipsilateral side
Paresis of lateralconjugate gazeHorner's syndromeCerebellar signs (ataxia,
19
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 23 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
neurological deficits that suggest a stroke, time is critical. Some data collection and diagnostics to establish
underlying cause may be postponed to begin treatment. The most important piece of information in the history
is to determine the exact time that the neurological deficits began. This is important to determine whether a
patient is eligible for thrombolytic therapy, if a diagnosis of ischemic stroke is made.
TABLE 25-3 NAME, DESCRIPTION, AND SIGNS/SYMPTOMS RELATED TO STROKE BY INVOLVEDVESSEL
NAME DESCRIPTION SIGNS AND SYMPTOMS
Internal
carotid
artery (ICA)
syndrome
Paralysis of the
contralateral face, arm,
and leg
Sensory deficits of the
contralateral face, arm,
and leg
Aphasia, if the dominant
hemisphere is involved
Apraxia, agnosia, and
unilateral neglect, if the
nondominant hemisphere
is involved
Homonymous hemianopsia
Middle
cerebral
artery (MCA)
syndrome
MCA is the most common of all cerebral
occlusions
• If the main stem of MCA is occluded, a
massive infarction of most of the
hemisphere results.
• Initially, there may be vomiting and a
rapid onset of coma, which may last a
few weeks.
Cerebral edema is extensive.
Hemiplegia (involving
face and arm on the
contralateral side; the leg
is spared or has fewer
deficits than the arm)
Sensory deficits (same
area as hemiplegia)
Aphasia (global aphasia if
the dominant hemisphere
is involved)
Homonymous hemianopsia
Anterior
cerebral
artery (ACA)
syndrome
ACA is least often occluded.
If occlusion occurs proximal to a patent
anterior communicating artery (ACom),
the blood supply may be compromised.
If occlusion is distal or if the ACom artery
is inadequate, there will be infarction of
the medial aspect of one frontal lobe.
Paralysis of contralateral
foot and leg (foot drop is
a consistent finding)
Impaired gait
Sensory loss over toes,
foot, and leg
Abulia (slowness and
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 24 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
Bilateral medial frontal lobe infarctionoccurs if one ACA is occluded and theother artery is small and dependent onblood flow.
prolonged delays toperform acts voluntarilyor to respond)Flat affect, lack ofspontaneity, slowness,distractibility, and lack ofinterest in surroundingsCognitive impairment,such as perseveration andamnesiaUrinary incontinenceNote that aphasia andhemianopsia are not partof the syndrome.
Vertebralarterysyndrome
Occlusion of vessels within thevertebrobasilar system produces uniquesyndromes.Vertebral and basilar arteries and theirbranches supply the brainstem andcerebellum.Posterior cerebral arteries are theterminal branches of the basilar arteryand supply the medial temporal andoccipital lobes, as well as part of thecorpus callosum.
Wallenberg's syndrome(lateral medullarysyndrome)DizzinessNystagmusDysphagia and dysarthriaPain in face, nose, or eyeIpsilateral numbness andweakness of faceStaggering gait and ataxiaClumsiness
Basilar artery(BA)syndrome
QuadriplegiaPossibly the “locked-in”syndromeWeakness of facial,lingual, and pharyngealmuscles
Anteriorinferiorcerebellarartery (AICA)syndrome
Occlusion of the AICA is also known as thelateral inferior pontine syndrome.
VertigoNausea and vomitingTinnitusNystagmus
Ipsilateral side
Paresis of lateralconjugate gazeHorner's syndromeCerebellar signs (ataxia,
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 25 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
nystagmus)
Contralateral side
Impaired pain and
temperature sensation in
trunk and limbs (may also
involve face)
Posterior
inferior
cerebellar
artery (PICA)
syndrome
(also called
Wallenberg's
syndrome)
PICA involves the lateral portion of the
medulla as a result of the occlusion of the
posterior inferior cerebellar artery.
Nausea and vomiting
Dysphagia and dysarthria
Horizontal nystagmus
Ipsilateral Horner's
syndrome
Cerebellar signs (ataxia
and vertigo)
Loss of pain and
temperature sensation on
contralateral side of trunk
and limbs
Posterior
cerebral
artery (PCA)
syndrome
If superficial occlusion (peripheral areas)
of a PCA is involved, contralateral
homonymous hemianopsia is seen.
If penetrating branches (central areas) are
occluded, the cerebral peduncle,
thalamus, and upper brainstem are
involved.
There is wide variation in the
manifestations of the syndrome.
Peripheral area
Homonymous hemianopsia
Memory deficits
Perseveration
Several visual deficits
(cortical blindness, lack
of depth perception,
failure to see objects not
centrally located, visual
hallucinations)
Central area
If the thalamus is
involved, sensory loss of
all modalities,
spontaneous pain,
intentional tremors, and
mild hemiparesis
If the cerebral peduncle
is involved, Weber's
syndrome (oculomotor
nerve palsy with
contralateral hemiplegia)
If the brainstem is
involved, deficits
involving conjugate gaze,
20
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 23 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
neurological deficits that suggest a stroke, time is critical. Some data collection and diagnostics to establish
underlying cause may be postponed to begin treatment. The most important piece of information in the history
is to determine the exact time that the neurological deficits began. This is important to determine whether a
patient is eligible for thrombolytic therapy, if a diagnosis of ischemic stroke is made.
TABLE 25-3 NAME, DESCRIPTION, AND SIGNS/SYMPTOMS RELATED TO STROKE BY INVOLVEDVESSEL
NAME DESCRIPTION SIGNS AND SYMPTOMS
Internal
carotid
artery (ICA)
syndrome
Paralysis of the
contralateral face, arm,
and leg
Sensory deficits of the
contralateral face, arm,
and leg
Aphasia, if the dominant
hemisphere is involved
Apraxia, agnosia, and
unilateral neglect, if the
nondominant hemisphere
is involved
Homonymous hemianopsia
Middle
cerebral
artery (MCA)
syndrome
MCA is the most common of all cerebral
occlusions
• If the main stem of MCA is occluded, a
massive infarction of most of the
hemisphere results.
• Initially, there may be vomiting and a
rapid onset of coma, which may last a
few weeks.
Cerebral edema is extensive.
Hemiplegia (involving
face and arm on the
contralateral side; the leg
is spared or has fewer
deficits than the arm)
Sensory deficits (same
area as hemiplegia)
Aphasia (global aphasia if
the dominant hemisphere
is involved)
Homonymous hemianopsia
Anterior
cerebral
artery (ACA)
syndrome
ACA is least often occluded.
If occlusion occurs proximal to a patent
anterior communicating artery (ACom),
the blood supply may be compromised.
If occlusion is distal or if the ACom artery
is inadequate, there will be infarction of
the medial aspect of one frontal lobe.
Paralysis of contralateral
foot and leg (foot drop is
a consistent finding)
Impaired gait
Sensory loss over toes,
foot, and leg
Abulia (slowness and
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 25 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
nystagmus)
Contralateral side
Impaired pain and
temperature sensation in
trunk and limbs (may also
involve face)
Posterior
inferior
cerebellar
artery (PICA)
syndrome
(also called
Wallenberg's
syndrome)
PICA involves the lateral portion of the
medulla as a result of the occlusion of the
posterior inferior cerebellar artery.
Nausea and vomiting
Dysphagia and dysarthria
Horizontal nystagmus
Ipsilateral Horner's
syndrome
Cerebellar signs (ataxia
and vertigo)
Loss of pain and
temperature sensation on
contralateral side of trunk
and limbs
Posterior
cerebral
artery (PCA)
syndrome
If superficial occlusion (peripheral areas)
of a PCA is involved, contralateral
homonymous hemianopsia is seen.
If penetrating branches (central areas) are
occluded, the cerebral peduncle,
thalamus, and upper brainstem are
involved.
There is wide variation in the
manifestations of the syndrome.
Peripheral area
Homonymous hemianopsia
Memory deficits
Perseveration
Several visual deficits
(cortical blindness, lack
of depth perception,
failure to see objects not
centrally located, visual
hallucinations)
Central area
If the thalamus is
involved, sensory loss of
all modalities,
spontaneous pain,
intentional tremors, and
mild hemiparesis
If the cerebral peduncle
is involved, Weber's
syndrome (oculomotor
nerve palsy with
contralateral hemiplegia)
If the brainstem is
involved, deficits
involving conjugate gaze,
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 26 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.600
nystagmus, and pupillaryabnormalities, with otherpossible symptoms ofataxia and posturaltremors
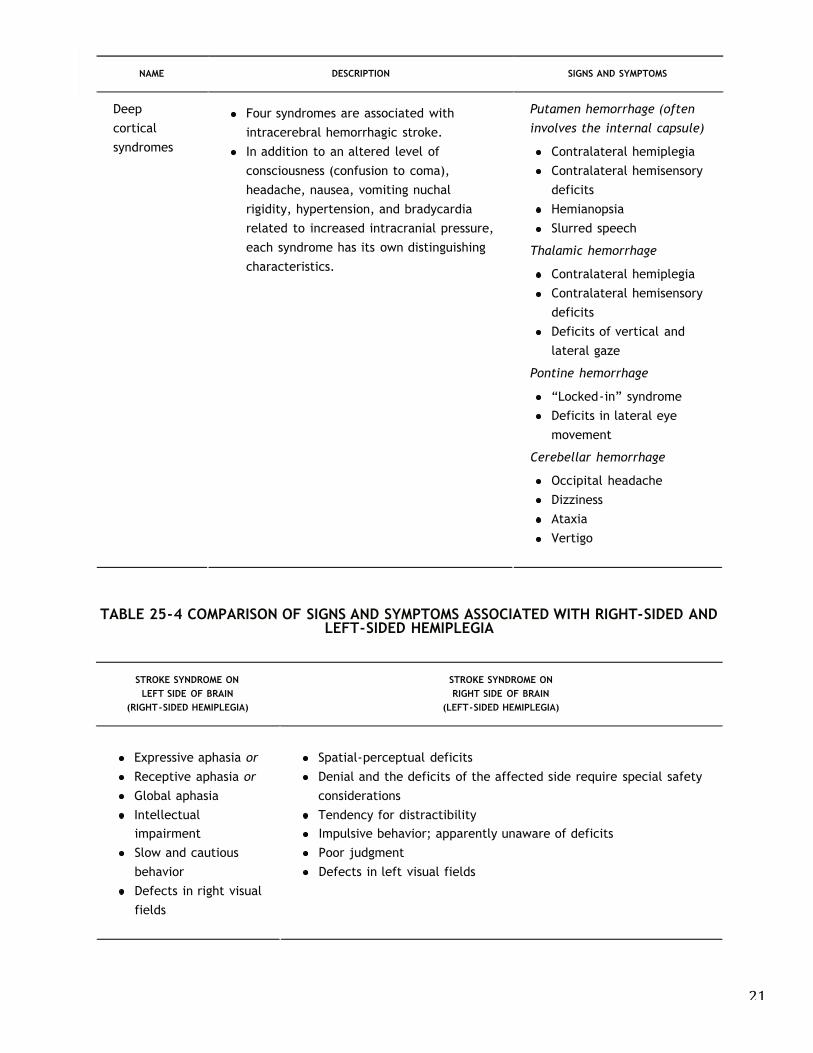
Deepcorticalsyndromes
Four syndromes are associated withintracerebral hemorrhagic stroke.In addition to an altered level ofconsciousness (confusion to coma),headache, nausea, vomiting nuchalrigidity, hypertension, and bradycardiarelated to increased intracranial pressure,each syndrome has its own distinguishingcharacteristics.
Putamen hemorrhage (often
involves the internal capsule)
Contralateral hemiplegiaContralateral hemisensorydeficitsHemianopsiaSlurred speech
Thalamic hemorrhage
Contralateral hemiplegiaContralateral hemisensorydeficitsDeficits of vertical andlateral gaze
Pontine hemorrhage
“Locked-in” syndromeDeficits in lateral eyemovement
Cerebellar hemorrhage
Occipital headacheDizzinessAtaxiaVertigo
TABLE 25-4 COMPARISON OF SIGNS AND SYMPTOMS ASSOCIATED WITH RIGHT-SIDED ANDLEFT-SIDED HEMIPLEGIA
STROKE SYNDROME ONLEFT SIDE OF BRAIN
(RIGHT-SIDED HEMIPLEGIA)
STROKE SYNDROME ONRIGHT SIDE OF BRAIN
(LEFT-SIDED HEMIPLEGIA)
Expressive aphasia or
Receptive aphasia or
Global aphasiaIntellectual
Spatial-perceptual deficitsDenial and the deficits of the affected side require special safetyconsiderationsTendency for distractibility
21
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 23 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
neurological deficits that suggest a stroke, time is critical. Some data collection and diagnostics to establish
underlying cause may be postponed to begin treatment. The most important piece of information in the history
is to determine the exact time that the neurological deficits began. This is important to determine whether a
patient is eligible for thrombolytic therapy, if a diagnosis of ischemic stroke is made.
TABLE 25-3 NAME, DESCRIPTION, AND SIGNS/SYMPTOMS RELATED TO STROKE BY INVOLVEDVESSEL
NAME DESCRIPTION SIGNS AND SYMPTOMS
Internal
carotid
artery (ICA)
syndrome
Paralysis of the
contralateral face, arm,
and leg
Sensory deficits of the
contralateral face, arm,
and leg
Aphasia, if the dominant
hemisphere is involved
Apraxia, agnosia, and
unilateral neglect, if the
nondominant hemisphere
is involved
Homonymous hemianopsia
Middle
cerebral
artery (MCA)
syndrome
MCA is the most common of all cerebral
occlusions
• If the main stem of MCA is occluded, a
massive infarction of most of the
hemisphere results.
• Initially, there may be vomiting and a
rapid onset of coma, which may last a
few weeks.
Cerebral edema is extensive.
Hemiplegia (involving
face and arm on the
contralateral side; the leg
is spared or has fewer
deficits than the arm)
Sensory deficits (same
area as hemiplegia)
Aphasia (global aphasia if
the dominant hemisphere
is involved)
Homonymous hemianopsia
Anterior
cerebral
artery (ACA)
syndrome
ACA is least often occluded.
If occlusion occurs proximal to a patent
anterior communicating artery (ACom),
the blood supply may be compromised.
If occlusion is distal or if the ACom artery
is inadequate, there will be infarction of
the medial aspect of one frontal lobe.
Paralysis of contralateral
foot and leg (foot drop is
a consistent finding)
Impaired gait
Sensory loss over toes,
foot, and leg
Abulia (slowness and
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 26 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.600
nystagmus, and pupillaryabnormalities, with otherpossible symptoms ofataxia and posturaltremors
Deepcorticalsyndromes
Four syndromes are associated withintracerebral hemorrhagic stroke.In addition to an altered level ofconsciousness (confusion to coma),headache, nausea, vomiting nuchalrigidity, hypertension, and bradycardiarelated to increased intracranial pressure,each syndrome has its own distinguishingcharacteristics.
Putamen hemorrhage (often
involves the internal capsule)
Contralateral hemiplegiaContralateral hemisensorydeficitsHemianopsiaSlurred speech
Thalamic hemorrhage
Contralateral hemiplegiaContralateral hemisensorydeficitsDeficits of vertical andlateral gaze
Pontine hemorrhage
“Locked-in” syndromeDeficits in lateral eyemovement
Cerebellar hemorrhage
Occipital headacheDizzinessAtaxiaVertigo
TABLE 25-4 COMPARISON OF SIGNS AND SYMPTOMS ASSOCIATED WITH RIGHT-SIDED ANDLEFT-SIDED HEMIPLEGIA
STROKE SYNDROME ONLEFT SIDE OF BRAIN
(RIGHT-SIDED HEMIPLEGIA)
STROKE SYNDROME ONRIGHT SIDE OF BRAIN
(LEFT-SIDED HEMIPLEGIA)
Expressive aphasia or
Receptive aphasia or
Global aphasiaIntellectual
Spatial-perceptual deficitsDenial and the deficits of the affected side require special safetyconsiderationsTendency for distractibility
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 26 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.600
nystagmus, and pupillaryabnormalities, with otherpossible symptoms ofataxia and posturaltremors
Deepcorticalsyndromes
Four syndromes are associated withintracerebral hemorrhagic stroke.In addition to an altered level ofconsciousness (confusion to coma),headache, nausea, vomiting nuchalrigidity, hypertension, and bradycardiarelated to increased intracranial pressure,each syndrome has its own distinguishingcharacteristics.
Putamen hemorrhage (often
involves the internal capsule)
Contralateral hemiplegiaContralateral hemisensorydeficitsHemianopsiaSlurred speech
Thalamic hemorrhage
Contralateral hemiplegiaContralateral hemisensorydeficitsDeficits of vertical andlateral gaze
Pontine hemorrhage
“Locked-in” syndromeDeficits in lateral eyemovement
Cerebellar hemorrhage
Occipital headacheDizzinessAtaxiaVertigo
TABLE 25-4 COMPARISON OF SIGNS AND SYMPTOMS ASSOCIATED WITH RIGHT-SIDED ANDLEFT-SIDED HEMIPLEGIA
STROKE SYNDROME ONLEFT SIDE OF BRAIN
(RIGHT-SIDED HEMIPLEGIA)
STROKE SYNDROME ONRIGHT SIDE OF BRAIN
(LEFT-SIDED HEMIPLEGIA)
Expressive aphasia or
Receptive aphasia or
Global aphasiaIntellectual
Spatial-perceptual deficitsDenial and the deficits of the affected side require special safetyconsiderationsTendency for distractibility
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 27 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.601
impairmentSlow and cautiousbehaviorDefects in right visualfields
Impulsive behavior; apparently unaware of deficitsPoor judgmentDefects in left visual fields
Diagnosis of Transient Ischemic Attacks
By definition, symptoms associated with a TIA clear completely in less than 24 hours; most clear within minutes.The diagnosis of TIA is a clinical diagnosis based on clinical evidence. TIAs are forewarnings of a potential strokeand thus should be investigated aggressively to determine cause before a stroke occurs. The focus of careincludes diagnosing TIAs versus other problems; determining the cerebral vessel involved based on symptoms ifpossible, or recognizing whether presenting symptoms are related to the anterior or posterior cerebralcirculation; instituting prevention measures for stroke by modification of risk factors; providing antiplateletdrugs; considering surgical intervention if indicated; providing comprehensive patient education including riskmodification; and providing ongoing monitoring for change in risk factors or condition.
The American Heart Association has published a number of guidelines and recommendations for the diagnosis
and treatment of TIAs.4,27,28,29,30 These guidelines are updated periodically
to reflect new scientific evidence that is then translated into practice guidelines.
TABLE 25-5 DIAGNOSTIC PROCEDURES FOR TRANSIENT ISCHEMIC ATTACKS (TIAs) ANDSTROKE*
DIAGNOSTIC PROCEDURE INFORMATION PROVIDED
Computedtomography (CT)scan withoutcontrast
Important immediate diagnostic to differentiate between ischemic andhemorrhagic stroke; if hemorrhagic, antiplatelets or anticoagulants are notgiven because of the increased risk of more bleeding; important fortreatment decisions
CT scan withcontrast
Useful to rule out lesions that many mimic a TIA, especially when symptomsare related to hemispheric deficits; hypodense areas on CT scan suggestinfarction
Magneticresonanceimaging (MRI)
Offers excellent soft-tissue contrast discrimination with superiordemarcation of mass lesion from surrounding structures including areas ofischemia and infarction; good visualization of vascular structures whenquestioning a vascular lesion; useful for diagnosis of stroke in first 72 h; adiffusion-weighted MRI can show ischemia in first few hours
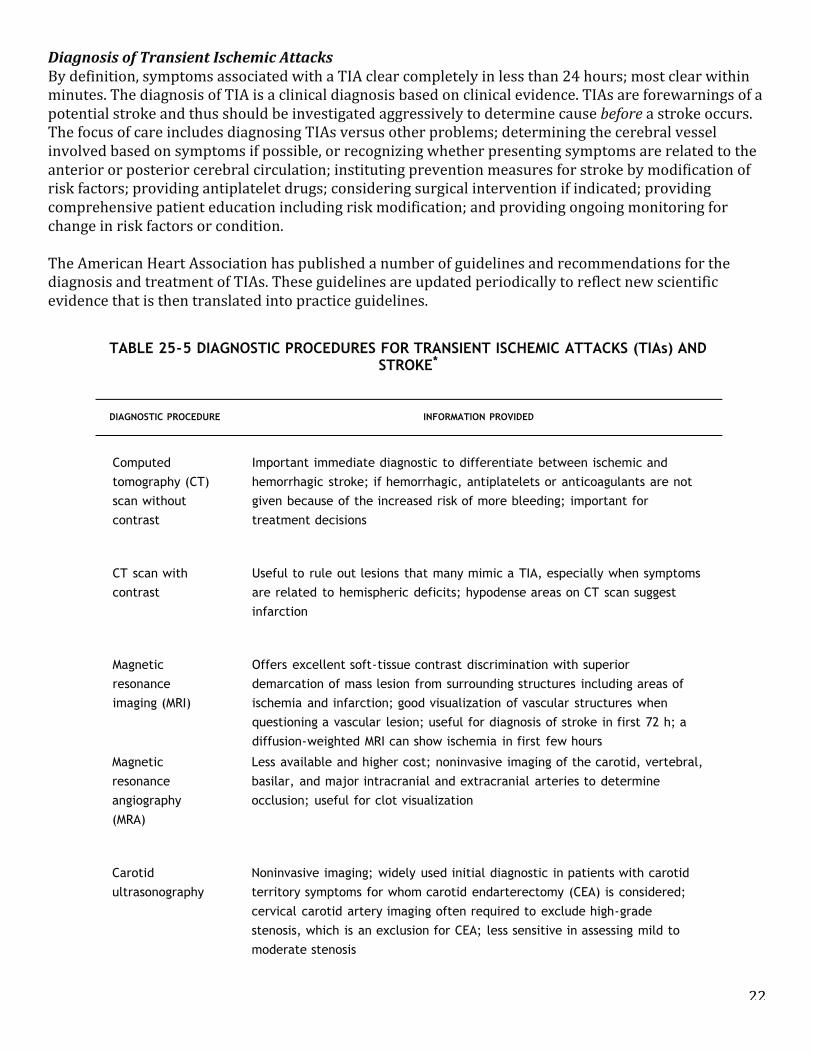
22
Diagnosis of Transient Ischemic Attacks By definition, symptoms associated with a TIA clear completely in less than 24 hours; most clear within minutes. The diagnosis of TIA is a clinical diagnosis based on clinical evidence. TIAs are forewarnings of a potential stroke and thus should be investigated aggressively to determine cause before a stroke occurs. The focus of care includes diagnosing TIAs versus other problems; determining the cerebral vessel involved based on symptoms if possible, or recognizing whether presenting symptoms are related to the anterior or posterior cerebral circulation; instituting prevention measures for stroke by modification of risk factors; providing antiplatelet drugs; considering surgical intervention if indicated; providing comprehensive patient education including risk modification; and providing ongoing monitoring for change in risk factors or condition. The American Heart Association has published a number of guidelines and recommendations for the diagnosis and treatment of TIAs. These guidelines are updated periodically to reflect new scientific evidence that is then translated into practice guidelines.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 27 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.601
impairmentSlow and cautiousbehaviorDefects in right visualfields
Impulsive behavior; apparently unaware of deficitsPoor judgmentDefects in left visual fields
Diagnosis of Transient Ischemic Attacks
By definition, symptoms associated with a TIA clear completely in less than 24 hours; most clear within minutes.The diagnosis of TIA is a clinical diagnosis based on clinical evidence. TIAs are forewarnings of a potential strokeand thus should be investigated aggressively to determine cause before a stroke occurs. The focus of careincludes diagnosing TIAs versus other problems; determining the cerebral vessel involved based on symptoms ifpossible, or recognizing whether presenting symptoms are related to the anterior or posterior cerebralcirculation; instituting prevention measures for stroke by modification of risk factors; providing antiplateletdrugs; considering surgical intervention if indicated; providing comprehensive patient education including riskmodification; and providing ongoing monitoring for change in risk factors or condition.
The American Heart Association has published a number of guidelines and recommendations for the diagnosis
and treatment of TIAs.4,27,28,29,30 These guidelines are updated periodically
to reflect new scientific evidence that is then translated into practice guidelines.
TABLE 25-5 DIAGNOSTIC PROCEDURES FOR TRANSIENT ISCHEMIC ATTACKS (TIAs) ANDSTROKE*
DIAGNOSTIC PROCEDURE INFORMATION PROVIDED
Computedtomography (CT)scan withoutcontrast
Important immediate diagnostic to differentiate between ischemic andhemorrhagic stroke; if hemorrhagic, antiplatelets or anticoagulants are notgiven because of the increased risk of more bleeding; important fortreatment decisions
CT scan withcontrast
Useful to rule out lesions that many mimic a TIA, especially when symptomsare related to hemispheric deficits; hypodense areas on CT scan suggestinfarction
Magneticresonanceimaging (MRI)
Offers excellent soft-tissue contrast discrimination with superiordemarcation of mass lesion from surrounding structures including areas ofischemia and infarction; good visualization of vascular structures whenquestioning a vascular lesion; useful for diagnosis of stroke in first 72 h; adiffusion-weighted MRI can show ischemia in first few hours
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 28 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
Magneticresonanceangiography(MRA)
Less available and higher cost; noninvasive imaging of the carotid, vertebral,basilar, and major intracranial and extracranial arteries to determineocclusion; useful for clot visualization
Carotidultrasonography
Noninvasive imaging; widely used initial diagnostic in patients with carotidterritory symptoms for whom carotid endarterectomy (CEA) is considered;cervical carotid artery imaging often required to exclude high-gradestenosis, which is an exclusion for CEA; less sensitive in assessing mild tomoderate stenosis
TranscranialDoppler (TCD)
TCDs are now part of standard work-up for stroke, especially when CEA isconsidered; useful to detect severe intracranial stenosis, evaluate thecarotid and vertebrobasilar vessels, assess patterns and extent of collateralcirculation in patients with known arterial stenosis or occlusion, and detectmicroemboli
Cerebralangiography
Ordered for patients considered candidates for CEA to define precisely thepercentage of occlusion and in patients with unusual presentation withaneurysm, vasculitis, and high-grade stenosis
Transthoracicechocardiography(TTE)
Helpful in search for cardioemboli sources; TTE is particularly helpful fordiagnosing left ventricular thrombi, left atrial myxomas, and thrombi thatprotrude into the atrial cavity; they are less reliable for small tumors,laminated thrombi, and thrombi limited to the left or right atrium
Transesophagealechocardiography(TEE)
Benefit of TEE is in greater sensitivity for source of cardioemboli (exceptventricular disease); TEE provides better visualization of cardiac structures,especially those at greater depth from chest wall and lesions of the atria(atrial appendage thrombi associated with atrial fibrillation), interarterialseptum defects (patent foramen ovale, atrial septal defects), mitral valvularvegetation, and atherosclerotic disease of ascending aortic arch
Electrocardiogram(ECG); 12-lead isrecommendedinitially
12-lead ECG recommended immediately because of the high incidence ofheart disease in patients with stroke; ECG also useful when cardiogenicembolic stroke or concurrent coronary artery disease is suspected
Ambulatory ECGmonitoring
Reserved for patients who have suspicious palpitations, arrhythmias, orenlarged left atrium
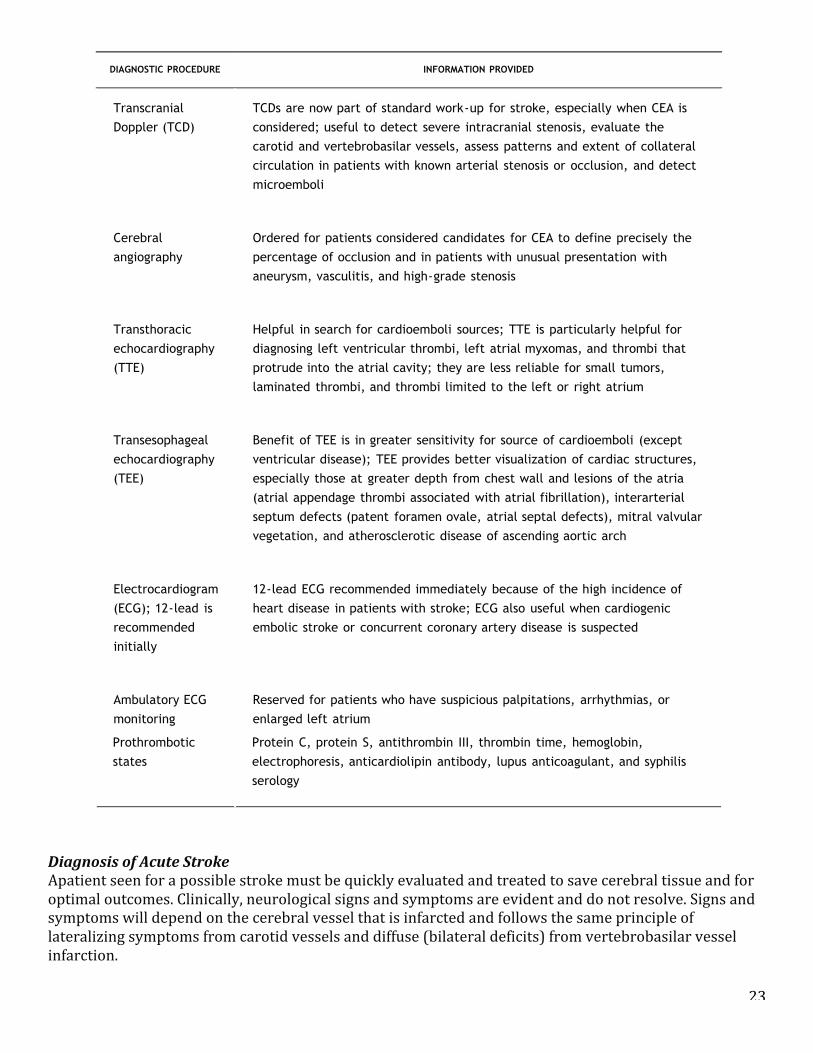
23
Diagnosis of Acute Stroke Apatient seen for a possible stroke must be quickly evaluated and treated to save cerebral tissue and for optimal outcomes. Clinically, neurological signs and symptoms are evident and do not resolve. Signs and symptoms will depend on the cerebral vessel that is infarcted and follows the same principle of lateralizing symptoms from carotid vessels and diffuse (bilateral deficits) from vertebrobasilar vessel infarction.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 27 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.601
impairmentSlow and cautiousbehaviorDefects in right visualfields
Impulsive behavior; apparently unaware of deficitsPoor judgmentDefects in left visual fields
Diagnosis of Transient Ischemic Attacks
By definition, symptoms associated with a TIA clear completely in less than 24 hours; most clear within minutes.The diagnosis of TIA is a clinical diagnosis based on clinical evidence. TIAs are forewarnings of a potential strokeand thus should be investigated aggressively to determine cause before a stroke occurs. The focus of careincludes diagnosing TIAs versus other problems; determining the cerebral vessel involved based on symptoms ifpossible, or recognizing whether presenting symptoms are related to the anterior or posterior cerebralcirculation; instituting prevention measures for stroke by modification of risk factors; providing antiplateletdrugs; considering surgical intervention if indicated; providing comprehensive patient education including riskmodification; and providing ongoing monitoring for change in risk factors or condition.
The American Heart Association has published a number of guidelines and recommendations for the diagnosis
and treatment of TIAs.4,27,28,29,30 These guidelines are updated periodically
to reflect new scientific evidence that is then translated into practice guidelines.
TABLE 25-5 DIAGNOSTIC PROCEDURES FOR TRANSIENT ISCHEMIC ATTACKS (TIAs) ANDSTROKE*
DIAGNOSTIC PROCEDURE INFORMATION PROVIDED
Computedtomography (CT)scan withoutcontrast
Important immediate diagnostic to differentiate between ischemic andhemorrhagic stroke; if hemorrhagic, antiplatelets or anticoagulants are notgiven because of the increased risk of more bleeding; important fortreatment decisions
CT scan withcontrast
Useful to rule out lesions that many mimic a TIA, especially when symptomsare related to hemispheric deficits; hypodense areas on CT scan suggestinfarction
Magneticresonanceimaging (MRI)
Offers excellent soft-tissue contrast discrimination with superiordemarcation of mass lesion from surrounding structures including areas ofischemia and infarction; good visualization of vascular structures whenquestioning a vascular lesion; useful for diagnosis of stroke in first 72 h; adiffusion-weighted MRI can show ischemia in first few hours
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 28 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
Magneticresonanceangiography(MRA)
Less available and higher cost; noninvasive imaging of the carotid, vertebral,basilar, and major intracranial and extracranial arteries to determineocclusion; useful for clot visualization
Carotidultrasonography
Noninvasive imaging; widely used initial diagnostic in patients with carotidterritory symptoms for whom carotid endarterectomy (CEA) is considered;cervical carotid artery imaging often required to exclude high-gradestenosis, which is an exclusion for CEA; less sensitive in assessing mild tomoderate stenosis
TranscranialDoppler (TCD)
TCDs are now part of standard work-up for stroke, especially when CEA isconsidered; useful to detect severe intracranial stenosis, evaluate thecarotid and vertebrobasilar vessels, assess patterns and extent of collateralcirculation in patients with known arterial stenosis or occlusion, and detectmicroemboli
Cerebralangiography
Ordered for patients considered candidates for CEA to define precisely thepercentage of occlusion and in patients with unusual presentation withaneurysm, vasculitis, and high-grade stenosis
Transthoracicechocardiography(TTE)
Helpful in search for cardioemboli sources; TTE is particularly helpful fordiagnosing left ventricular thrombi, left atrial myxomas, and thrombi thatprotrude into the atrial cavity; they are less reliable for small tumors,laminated thrombi, and thrombi limited to the left or right atrium
Transesophagealechocardiography(TEE)
Benefit of TEE is in greater sensitivity for source of cardioemboli (exceptventricular disease); TEE provides better visualization of cardiac structures,especially those at greater depth from chest wall and lesions of the atria(atrial appendage thrombi associated with atrial fibrillation), interarterialseptum defects (patent foramen ovale, atrial septal defects), mitral valvularvegetation, and atherosclerotic disease of ascending aortic arch
Electrocardiogram(ECG); 12-lead isrecommendedinitially
12-lead ECG recommended immediately because of the high incidence ofheart disease in patients with stroke; ECG also useful when cardiogenicembolic stroke or concurrent coronary artery disease is suspected
Ambulatory ECGmonitoring
Reserved for patients who have suspicious palpitations, arrhythmias, orenlarged left atrium
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 29 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.602
Prothrombotic
states
Protein C, protein S, antithrombin III, thrombin time, hemoglobin,
electrophoresis, anticardiolipin antibody, lupus anticoagulant, and syphilis
serology
* Adams, H. P. Jr., del Zoppo, G., Alberts, M. J., Bhatt, D. L; Brass, L., Furlan, A., et al. (2007).
Guidelines for the early management of adults with ischemic stroke. Stroke, 38, 1655-1711.
CLINICAL VIGNETTE:A68-year-old woman has had some episodes of numbness in her right arm and word-findingdifficulty, but they don't last long and disappear. Today was different; the episode lastedlonger and she could not speak for 10 minutes, but she was able to speak later, althoughshe had difficulty finding words. Her alarmed spouse took her to the emergency department(ED). The physical and neurological examinations were normal. A 12-lead ECG, cardiacenzyme panel, and all other blood work were normal. After questioning the patient aboutdrug allergies, she was placed on 325 mg of aspirin daily. An appointment was made withher primary care physician for the following week.
Diagnosis of Acute Stroke
Apatient seen for a possible stroke must be quickly evaluated and treated to save cerebral tissue and for
optimal outcomes. Clinically, neurological signs and symptoms are evident and do not resolve. Signs and
symptoms will depend on the cerebral vessel that is infarcted and follows the same principle of lateralizing
symptoms from carotid vessels and diffuse (bilateral deficits) from vertebrobasilar vessel infarction.
CLINICAL VIGNETTE*:Forty-seven-year-old Mrs. CS awoke early in the morning, made a visit to the bathroom,and was returning to bed. About halfway back to bed she experienced an abrupt, severebout of vertigo, requiring her to grab onto the wall and furniture to get back to bed. Thevertigo continued, and was soon
accompanied by nausea and vomiting. Her husband, recognizing that something wasseriously wrong, took her to the nearest ED. In the ED, her initial assessment revealedsome mild left upper extremity weakness and dysmetria. Anurse conducted a neurologicalassessment and checked “neuro status stable” on the assessment form. The vertigo andnausea persisted in spite of antiemetic medications; the patient was admitted to a medicalfloor and a gastrointestinal (GI) consult ordered. The GI work-up was negative; the vertigopersisted. The ear, nose, and throat (ENT) service was consulted for a possible inner earproblem. This avenue of investigation was also negative. More than 48 hours afterpresenting to the ED, a neurology consult was ordered. A CT scan of the head revealed a4.5-cm left cerebellar infarct.
TABLE 25-6 MAJOR RISK FACTORS FOR STROKE
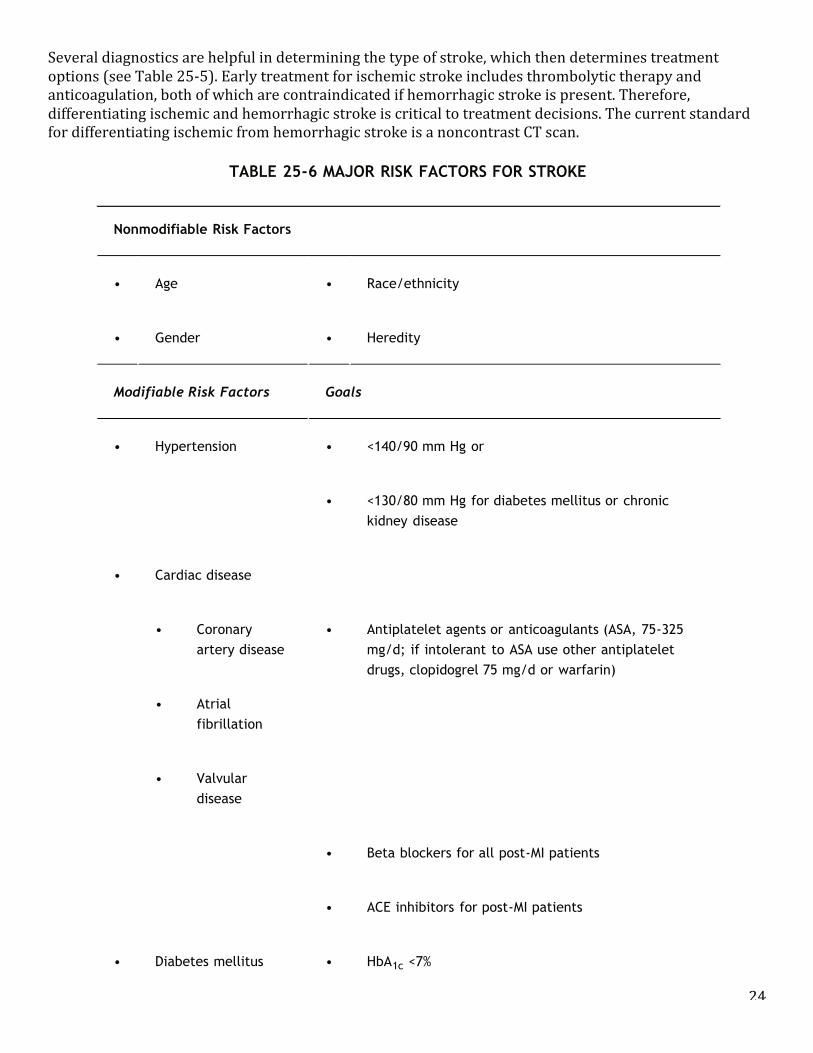
24
Several diagnostics are helpful in determining the type of stroke, which then determines treatment options (see Table 25-‐5). Early treatment for ischemic stroke includes thrombolytic therapy and anticoagulation, both of which are contraindicated if hemorrhagic stroke is present. Therefore, differentiating ischemic and hemorrhagic stroke is critical to treatment decisions. The current standard for differentiating ischemic from hemorrhagic stroke is a noncontrast CT scan.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 29 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.602
Prothrombotic
states
Protein C, protein S, antithrombin III, thrombin time, hemoglobin,
electrophoresis, anticardiolipin antibody, lupus anticoagulant, and syphilis
serology
* Adams, H. P. Jr., del Zoppo, G., Alberts, M. J., Bhatt, D. L; Brass, L., Furlan, A., et al. (2007).
Guidelines for the early management of adults with ischemic stroke. Stroke, 38, 1655-1711.
CLINICAL VIGNETTE:A68-year-old woman has had some episodes of numbness in her right arm and word-findingdifficulty, but they don't last long and disappear. Today was different; the episode lastedlonger and she could not speak for 10 minutes, but she was able to speak later, althoughshe had difficulty finding words. Her alarmed spouse took her to the emergency department(ED). The physical and neurological examinations were normal. A 12-lead ECG, cardiacenzyme panel, and all other blood work were normal. After questioning the patient aboutdrug allergies, she was placed on 325 mg of aspirin daily. An appointment was made withher primary care physician for the following week.
Diagnosis of Acute Stroke
Apatient seen for a possible stroke must be quickly evaluated and treated to save cerebral tissue and for
optimal outcomes. Clinically, neurological signs and symptoms are evident and do not resolve. Signs and
symptoms will depend on the cerebral vessel that is infarcted and follows the same principle of lateralizing
symptoms from carotid vessels and diffuse (bilateral deficits) from vertebrobasilar vessel infarction.
CLINICAL VIGNETTE*:Forty-seven-year-old Mrs. CS awoke early in the morning, made a visit to the bathroom,and was returning to bed. About halfway back to bed she experienced an abrupt, severebout of vertigo, requiring her to grab onto the wall and furniture to get back to bed. Thevertigo continued, and was soon
accompanied by nausea and vomiting. Her husband, recognizing that something wasseriously wrong, took her to the nearest ED. In the ED, her initial assessment revealedsome mild left upper extremity weakness and dysmetria. Anurse conducted a neurologicalassessment and checked “neuro status stable” on the assessment form. The vertigo andnausea persisted in spite of antiemetic medications; the patient was admitted to a medicalfloor and a gastrointestinal (GI) consult ordered. The GI work-up was negative; the vertigopersisted. The ear, nose, and throat (ENT) service was consulted for a possible inner earproblem. This avenue of investigation was also negative. More than 48 hours afterpresenting to the ED, a neurology consult was ordered. A CT scan of the head revealed a4.5-cm left cerebellar infarct.
TABLE 25-6 MAJOR RISK FACTORS FOR STROKE 5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 30 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
Nonmodifiable Risk Factors
• Age • Race/ethnicity
• Gender • Heredity
Modifiable Risk Factors Goals
• Hypertension • <140/90 mm Hg or
• <130/80 mm Hg for diabetes mellitus or chronic
kidney disease
• Cardiac disease
• Coronary
artery disease
• Antiplatelet agents or anticoagulants (ASA, 75-325
mg/d; if intolerant to ASA use other antiplatelet
drugs, clopidogrel 75 mg/d or warfarin)
• Atrial
fibrillation
• Valvular
disease
• Beta blockers for all post-MI patients
• ACE inhibitors for post-MI patients
• Diabetes mellitus • HbA1c <7%
• Hypercholesterolemia • LDL 100 mg/dL
• If total cholesterol !200 mg/dL, then non-HDL should
be <130 mg/dL
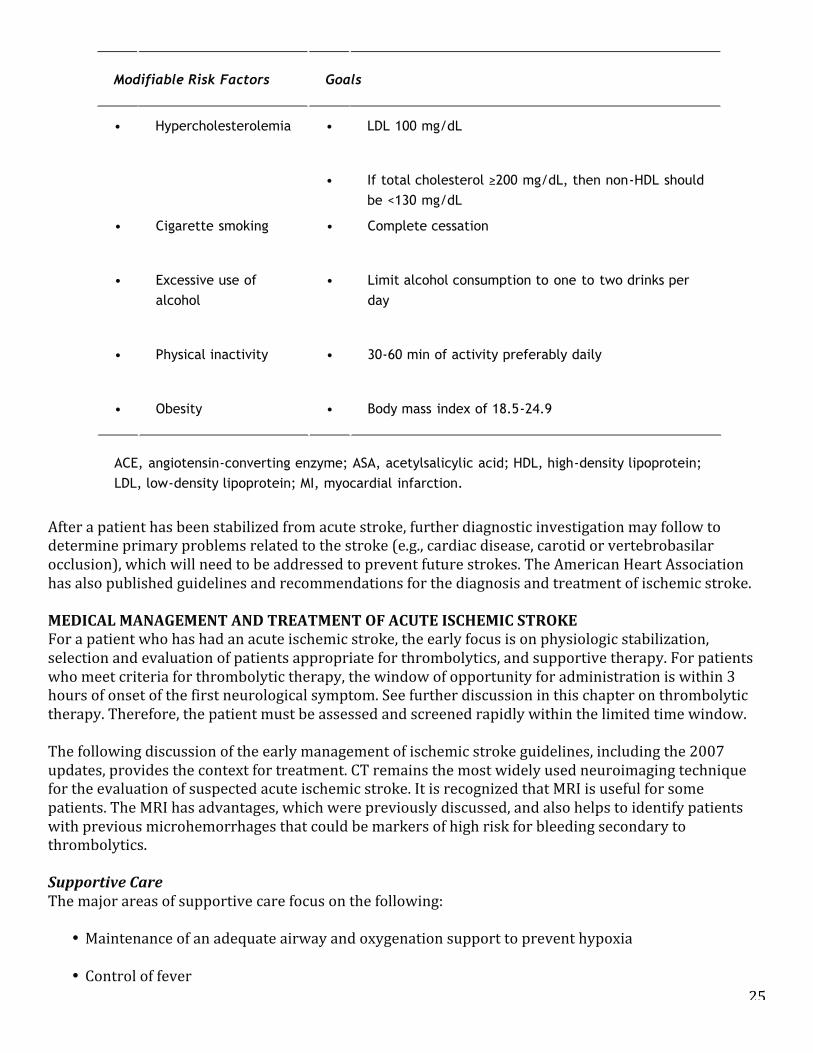
25
After a patient has been stabilized from acute stroke, further diagnostic investigation may follow to determine primary problems related to the stroke (e.g., cardiac disease, carotid or vertebrobasilar occlusion), which will need to be addressed to prevent future strokes. The American Heart Association has also published guidelines and recommendations for the diagnosis and treatment of ischemic stroke. MEDICAL MANAGEMENT AND TREATMENT OF ACUTE ISCHEMIC STROKE For a patient who has had an acute ischemic stroke, the early focus is on physiologic stabilization, selection and evaluation of patients appropriate for thrombolytics, and supportive therapy. For patients who meet criteria for thrombolytic therapy, the window of opportunity for administration is within 3 hours of onset of the first neurological symptom. See further discussion in this chapter on thrombolytic therapy. Therefore, the patient must be assessed and screened rapidly within the limited time window. The following discussion of the early management of ischemic stroke guidelines, including the 2007 updates, provides the context for treatment. CT remains the most widely used neuroimaging technique for the evaluation of suspected acute ischemic stroke. It is recognized that MRI is useful for some patients. The MRI has advantages, which were previously discussed, and also helps to identify patients with previous microhemorrhages that could be markers of high risk for bleeding secondary to thrombolytics. Supportive Care The major areas of supportive care focus on the following:
• Maintenance of an adequate airway and oxygenation support to prevent hypoxia
• Control of fever
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 30 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
Nonmodifiable Risk Factors
• Age • Race/ethnicity
• Gender • Heredity
Modifiable Risk Factors Goals
• Hypertension • <140/90 mm Hg or
• <130/80 mm Hg for diabetes mellitus or chronic
kidney disease
• Cardiac disease
• Coronary
artery disease
• Antiplatelet agents or anticoagulants (ASA, 75-325
mg/d; if intolerant to ASA use other antiplatelet
drugs, clopidogrel 75 mg/d or warfarin)
• Atrial
fibrillation
• Valvular
disease
• Beta blockers for all post-MI patients
• ACE inhibitors for post-MI patients
• Diabetes mellitus • HbA1c <7%
• Hypercholesterolemia • LDL 100 mg/dL
• If total cholesterol !200 mg/dL, then non-HDL should
be <130 mg/dL
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 30 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
Nonmodifiable Risk Factors
• Age • Race/ethnicity
• Gender • Heredity
Modifiable Risk Factors Goals
• Hypertension • <140/90 mm Hg or
• <130/80 mm Hg for diabetes mellitus or chronic
kidney disease
• Cardiac disease
• Coronary
artery disease
• Antiplatelet agents or anticoagulants (ASA, 75-325
mg/d; if intolerant to ASA use other antiplatelet
drugs, clopidogrel 75 mg/d or warfarin)
• Atrial
fibrillation
• Valvular
disease
• Beta blockers for all post-MI patients
• ACE inhibitors for post-MI patients
• Diabetes mellitus • HbA1c <7%
• Hypercholesterolemia • LDL 100 mg/dL
• If total cholesterol !200 mg/dL, then non-HDL should
be <130 mg/dL
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 31 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.603
• Cigarette smoking • Complete cessation
• Excessive use ofalcohol
• Limit alcohol consumption to one to two drinks perday
• Physical inactivity • 30-60 min of activity preferably daily
• Obesity • Body mass index of 18.5-24.9
ACE, angiotensin-converting enzyme; ASA, acetylsalicylic acid; HDL, high-density lipoprotein;LDL, low-density lipoprotein; MI, myocardial infarction.
From Adams, R. J., Chimowitz, M. I., Alpert, J. S., et al. (2003). Coronary risk evaluation inpatients with transient ischemic attack and ischemic stroke. Stroke, 108, 1278-1290.
The most commonly recognized signs of stroke involve unilateral weakness and numbness,altered mental status, and speech changes. Strokes can present in atypical presentationsand may not fit the stereotype of deficits. Had the ED staff noted the abrupt onset ofsymptoms and the early neurological signs of left upper
extremity weakness along with dysmetria, they may have considered cerebellar stroke as apossible diagnosis in spite of the patient's young age and the unusual presentation ofsymptoms.
CHART 25-1 National Institutes of Health Stroke Scale
1a. Level of consciousness (LOC)
alert 0
drowsy 1
stuporous 2
coma 3
1b. LOC questions
answers both correctly 0
answers one correctly 1
26
• Ongoing assessment for cardiac arrhythmia and cardiac ischemia/infarction
• Blood pressure management to maximize cerebral perfusion
• Glycemia management to maintain glucose less than 140 mg/dL to decrease risk of cerebral edema
and hemorrhage
• Prevention of complications such as aspiration pneumonia, deep vein thrombosis, nosocomial infections, and device-‐related infections (urinary tract infections, intravascular line infections)
Maintenance of adequate cerebral tissue oxygenation is critical to prevent hypoxia and potential exacerbation or advancement of further neurological injury. A patent airway must be maintained. If the patient cannot maintain patency independently due to a decreased level of consciousness or brainstem stroke, an artificial airway is used along with measures to prevent aspiration. Supplemental oxygen may be provided, and ventilatory support may be necessary for some patients. A pulse oximeter is used for ongoing monitoring of peripheral oxygenation. Control of fever is associated with better patient outcomes and therefore, aggressive fever control is recommended. Hyperthermia (temperature >37.5°C) has been associated with poorer outcome and poorer prognosis following acute stroke. This finding is consistent with experimental studies, which consistently indicate that increased temperature is associated with more severe neuronal injury. Vigilant nursing observation of the patient's temperature and taking active and immediate measures to prevent and control fever are key functions in the care of the stroke patient. Myocardial infarction and cardiac arrhythmias are potential complications associated with ischemic stroke. The most common arrhythmia is atrial fibrillation. The patient should have continual cardiac monitoring to identify arrhythmias to allow for prompt treatment. The target level of hypertension at which treatment should be treated with antihypertensives in a stroke patient is not known. However, treatment is generally avoided unless the systolic blood pressure is greater than 220 mm Hg or diastolic blood pressure is greater than 120 mm Hg. If it is necessary to administer antihypertensives, short-‐duration drugs that have little effect on cerebral blood vessels are selected. The blood pressure must be lowered slowly and cautiously. Labetalol is the drug of choice for intravenous treatment because it can be easily titrated and has minimal vasodilator effect on cerebral blood vessels. In some cases sodium nitroprusside may be required for adequate control. Captopril or nicardipine may be administered by the oral route. If a patient is a candidate for thrombolytics, the blood pressure must be carefully managed before and after administration of thrombolytics. Thrombolytics are not given if the systolic blood pressure is greater than 185 mm Hg or diastolic blood pressure is greater than 110 mm Hg at the time of treatment. Treatment with short-‐acting antihypertensives may be necessary before administering recombinant tissue plasminogen activator (rt-‐PA). It is well recognized that glycemia control within a targeted range is important because either hypoglycemia or hyperglycemia can lead to additional cerebral injury. The blood glucose levels can be easily monitored using a fingerstick. According to the guidelines, a judicious approach to management of hyperglycemia is recommended. The data are limited to determine how this statement should be translated into practice.31 Lowering the blood glucose to targeted levels can be accomplished with saline solution and regular insulin intravenous drip therapy. Many stroke centers have established lower glucose levels and use less than 140 mg/dL as a target.
27
Preventions of complications related to stroke are clear. Aspiration pneumonia continues to be a serious and mostly preventable problem. Keeping the patient on nothing by mouth (NPO) status until a bedside swallowing screen is conducted and passed is critical to prevent aspiration pneumonia. Removing indwelling devices such as urinary catheters and intravascular devices as soon as possible, and vigilant strict aseptic precautions while in use, decreases the incidence of hospital-‐acquired infections. Medical Management In addition to supportive care, medical management options for ischemic stroke include hypervolemic-‐ hemodilution therapy, thrombolytics, anticoagulants, antiplatelets, neuroprotective drugs, and hypothermia. Although all of these options are not recommended in published guidelines, each category is addressed to briefly discuss the state of the science. The goal of treatment is to rapidly assess and stabilize the patient to optimize outcomes and to prevent recurrent stroke. Prevention of recurrent stroke includes immediate careful management in the acute phase to prevent complications that will result in cerebral ischemia, hemorrhage, and extension of the stroke or a new stroke. The long-‐term perspective of secondary prevention is based on risk factor identification and modification to prevent recurrent stroke. This begins in the acute care setting with identification of the patient's risk factors and developing an individualized plan of care based on the most current evidence-‐based practice recommendations. Guidelines for the prevention of stroke in patients with ischemic stroke or TIAs are found in Table 25-‐7. Hypervolemic-Hemodilution Therapy To support cerebral hemodynamics, hypervolemic-‐hemodilution therapy has been used (see Chap. 23). This therapy is alleged to help maintain a stable, slightly higher blood pressure, which increases and maintains cerebral perfusion pressure by lowering blood viscosity. According to the 2007 guidelines, at present drug-‐induced hypertension is not recommended for the treatment of most patients with ischemic stroke. Thrombolytics Reperfusion drug therapy continues to be a useful option for selected patients with acute ischemic stroke. According to the 2007 guidelines, intravenous administration of rt-‐PA is the treatment of choice for thrombolytics in acute stroke. Treatment with streptokinase is not recommended, and reteplase, urokinase, and other thrombolytic agents should not be used outside of the setting of a clinical trial. The thrombolytic therapy with rt-‐PA is used in acute ischemic stroke to restore cerebral blood flow, reduce ischemia, and limit neurological disability. Re-‐establishing perfusion in an occluded cerebral artery may result in the recovery of ischemic tissue within a brief time span after onset of acute stroke. The major concern with thrombolytic agents is the possibility of hemorrhagic transformation of the infarction. Intravenous rt-‐PA should be considered for all patients with acute ischemic stroke who meet criteria and who can be treated within 3 hours of stroke symptom onset. Careful selection is imperative in safe drug administration. Chart 25-‐2 outlines inclusion and exclusion criteria. The recommended dose is 0.9 mg/kg (maximum 90 mg). The initial 10% is given as an intravenous bolus over 1 minute and the remaining rt-‐PA infused over 60 minutes. Anticoagulants or aspirin should not be given in the first 24 hours after rt-‐PAtreatment. Thrombolytic therapy with rt-‐PA is not without risk. Following initiation of therapy, patients must be assessed in an intensive care setting or unit with nurses skilled in monitoring patients. More and more patients are being admitted to non-‐intensive care units after rt-‐PAas long as drips that need adjusting or ventilator support is ordered for the patient. Frequent assessment of blood pressure during the first 24 hours, with treatment of blood pressure elevations of more than 185 mm Hg systolic or 110 mm Hg diastolic, helps prevent thrombolysis-‐ related ICH. Frequent neurological assessment can allow early
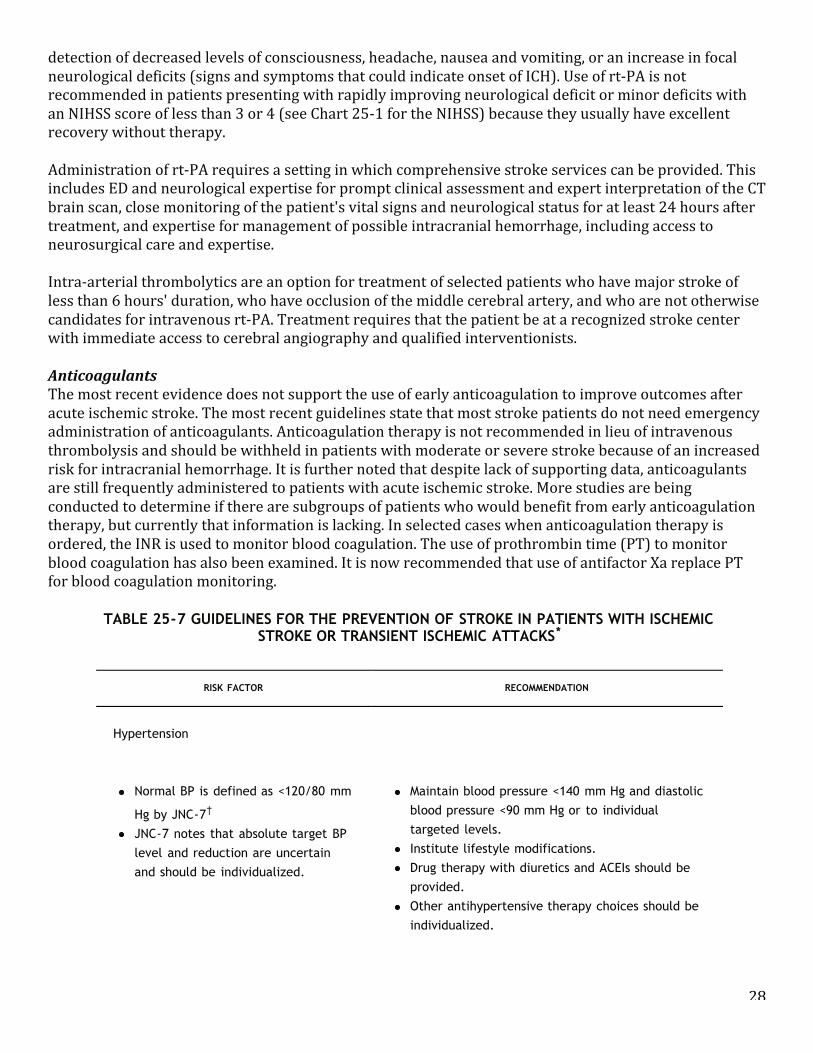
28
detection of decreased levels of consciousness, headache, nausea and vomiting, or an increase in focal neurological deficits (signs and symptoms that could indicate onset of ICH). Use of rt-‐PA is not recommended in patients presenting with rapidly improving neurological deficit or minor deficits with an NIHSS score of less than 3 or 4 (see Chart 25-‐1 for the NIHSS) because they usually have excellent recovery without therapy. Administration of rt-‐PA requires a setting in which comprehensive stroke services can be provided. This includes ED and neurological expertise for prompt clinical assessment and expert interpretation of the CT brain scan, close monitoring of the patient's vital signs and neurological status for at least 24 hours after treatment, and expertise for management of possible intracranial hemorrhage, including access to neurosurgical care and expertise. Intra-‐arterial thrombolytics are an option for treatment of selected patients who have major stroke of less than 6 hours' duration, who have occlusion of the middle cerebral artery, and who are not otherwise candidates for intravenous rt-‐PA. Treatment requires that the patient be at a recognized stroke center with immediate access to cerebral angiography and qualified interventionists. Anticoagulants The most recent evidence does not support the use of early anticoagulation to improve outcomes after acute ischemic stroke. The most recent guidelines state that most stroke patients do not need emergency administration of anticoagulants. Anticoagulation therapy is not recommended in lieu of intravenous thrombolysis and should be withheld in patients with moderate or severe stroke because of an increased risk for intracranial hemorrhage. It is further noted that despite lack of supporting data, anticoagulants are still frequently administered to patients with acute ischemic stroke. More studies are being conducted to determine if there are subgroups of patients who would benefit from early anticoagulation therapy, but currently that information is lacking. In selected cases when anticoagulation therapy is ordered, the INR is used to monitor blood coagulation. The use of prothrombin time (PT) to monitor blood coagulation has also been examined. It is now recommended that use of antifactor Xa replace PT for blood coagulation monitoring.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 37 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.605
The most recent evidence does not support the use of early anticoagulation to improve outcomes after acute
ischemic stroke.4,35 The most recent guidelines state that most stroke patients do not need emergency
administration of anticoagulants.4,31,36 Anticoagulation therapy is not recommended in lieu of intravenousthrombolysis and should be withheld in patients with moderate or severe stroke because of an increased risk forintracranial hemorrhage. It is further noted that despite lack of supporting data, anticoagulants are stillfrequently administered to patients with acute ischemic stroke. More studies are being conducted to determineif there are subgroups of patients who would benefit from
early anticoagulation therapy, but currently that information is lacking. In selected cases when anticoagulationtherapy is ordered, the INR is used to monitor blood coagulation. The use of prothrombin time (PT) to monitorblood coagulation has also been examined. It is now recommended that use of antifactor Xa replace PT for
blood coagulation monitoring.37
TABLE 25-7 GUIDELINES FOR THE PREVENTION OF STROKE IN PATIENTS WITH ISCHEMICSTROKE OR TRANSIENT ISCHEMIC ATTACKS*
RISK FACTOR RECOMMENDATION
Hypertension
Normal BP is defined as <120/80 mm
Hg by JNC-7†
JNC-7 notes that absolute target BPlevel and reduction are uncertainand should be individualized.
Maintain blood pressure <140 mm Hg and diastolicblood pressure <90 mm Hg or to individualtargeted levels.Institute lifestyle modifications.Drug therapy with diuretics and ACEIs should beprovided.Other antihypertensive therapy choices should beindividualized.
Diabetes mellitus
ACEIs and ARBs are effective inreducing progression of renaldisease.Near normal glycemic levels reducemicrovascular complications.
More rigorous control of BP and lipidsFor people with diabetes mellitus, target blood
pressure levels to <130/80 mm Hg†
Most patients will require more than one agent tocontrol BP (first-choice medications are ACEIs andARBs).Diet and oral hypoglycemics or insulin to keepfasting blood glucose levels <126 mg/dL or tomaintain hemoglobin A1c level <7.0%
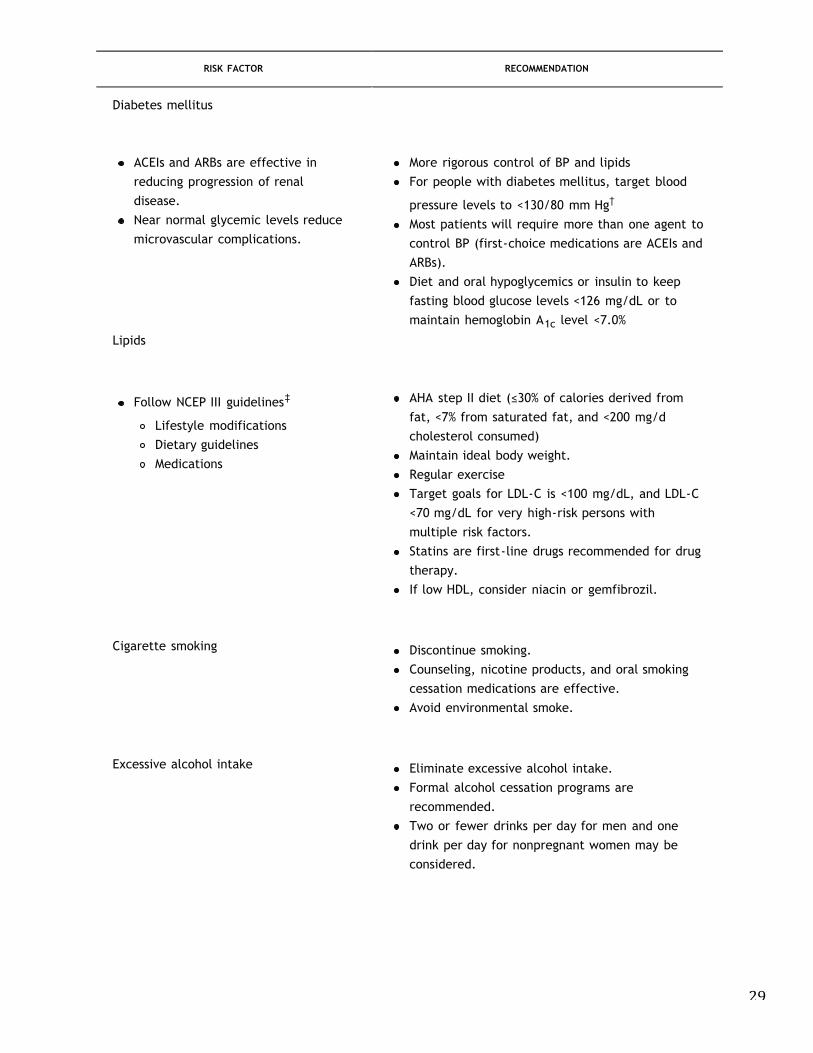
29
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 37 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.605
The most recent evidence does not support the use of early anticoagulation to improve outcomes after acute
ischemic stroke.4,35 The most recent guidelines state that most stroke patients do not need emergency
administration of anticoagulants.4,31,36 Anticoagulation therapy is not recommended in lieu of intravenousthrombolysis and should be withheld in patients with moderate or severe stroke because of an increased risk forintracranial hemorrhage. It is further noted that despite lack of supporting data, anticoagulants are stillfrequently administered to patients with acute ischemic stroke. More studies are being conducted to determineif there are subgroups of patients who would benefit from
early anticoagulation therapy, but currently that information is lacking. In selected cases when anticoagulationtherapy is ordered, the INR is used to monitor blood coagulation. The use of prothrombin time (PT) to monitorblood coagulation has also been examined. It is now recommended that use of antifactor Xa replace PT for
blood coagulation monitoring.37
TABLE 25-7 GUIDELINES FOR THE PREVENTION OF STROKE IN PATIENTS WITH ISCHEMICSTROKE OR TRANSIENT ISCHEMIC ATTACKS*
RISK FACTOR RECOMMENDATION
Hypertension
Normal BP is defined as <120/80 mm
Hg by JNC-7†
JNC-7 notes that absolute target BPlevel and reduction are uncertainand should be individualized.
Maintain blood pressure <140 mm Hg and diastolicblood pressure <90 mm Hg or to individualtargeted levels.Institute lifestyle modifications.Drug therapy with diuretics and ACEIs should beprovided.Other antihypertensive therapy choices should beindividualized.
Diabetes mellitus
ACEIs and ARBs are effective inreducing progression of renaldisease.Near normal glycemic levels reducemicrovascular complications.
More rigorous control of BP and lipidsFor people with diabetes mellitus, target blood
pressure levels to <130/80 mm Hg†
Most patients will require more than one agent tocontrol BP (first-choice medications are ACEIs andARBs).Diet and oral hypoglycemics or insulin to keepfasting blood glucose levels <126 mg/dL or tomaintain hemoglobin A1c level <7.0%
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 37 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.605
The most recent evidence does not support the use of early anticoagulation to improve outcomes after acute
ischemic stroke.4,35 The most recent guidelines state that most stroke patients do not need emergency
administration of anticoagulants.4,31,36 Anticoagulation therapy is not recommended in lieu of intravenousthrombolysis and should be withheld in patients with moderate or severe stroke because of an increased risk forintracranial hemorrhage. It is further noted that despite lack of supporting data, anticoagulants are stillfrequently administered to patients with acute ischemic stroke. More studies are being conducted to determineif there are subgroups of patients who would benefit from
early anticoagulation therapy, but currently that information is lacking. In selected cases when anticoagulationtherapy is ordered, the INR is used to monitor blood coagulation. The use of prothrombin time (PT) to monitorblood coagulation has also been examined. It is now recommended that use of antifactor Xa replace PT for
blood coagulation monitoring.37
TABLE 25-7 GUIDELINES FOR THE PREVENTION OF STROKE IN PATIENTS WITH ISCHEMICSTROKE OR TRANSIENT ISCHEMIC ATTACKS*
RISK FACTOR RECOMMENDATION
Hypertension
Normal BP is defined as <120/80 mm
Hg by JNC-7†
JNC-7 notes that absolute target BPlevel and reduction are uncertainand should be individualized.
Maintain blood pressure <140 mm Hg and diastolicblood pressure <90 mm Hg or to individualtargeted levels.Institute lifestyle modifications.Drug therapy with diuretics and ACEIs should beprovided.Other antihypertensive therapy choices should beindividualized.
Diabetes mellitus
ACEIs and ARBs are effective inreducing progression of renaldisease.Near normal glycemic levels reducemicrovascular complications.
More rigorous control of BP and lipidsFor people with diabetes mellitus, target blood
pressure levels to <130/80 mm Hg†
Most patients will require more than one agent tocontrol BP (first-choice medications are ACEIs andARBs).Diet and oral hypoglycemics or insulin to keepfasting blood glucose levels <126 mg/dL or tomaintain hemoglobin A1c level <7.0%
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 38 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
Lipids
Follow NCEP III guidelines‡
Lifestyle modificationsDietary guidelinesMedications
AHA step II diet (!30% of calories derived fromfat, <7% from saturated fat, and <200 mg/dcholesterol consumed)Maintain ideal body weight.Regular exerciseTarget goals for LDL-C is <100 mg/dL, and LDL-C<70 mg/dL for very high-risk persons withmultiple risk factors.Statins are first-line drugs recommended for drugtherapy.If low HDL, consider niacin or gemfibrozil.
Cigarette smoking Discontinue smoking.Counseling, nicotine products, and oral smokingcessation medications are effective.Avoid environmental smoke.
Excessive alcohol intake Eliminate excessive alcohol intake.Formal alcohol cessation programs arerecommended.Two or fewer drinks per day for men and onedrink per day for nonpregnant women may beconsidered.
ObesityGoal is BMI of 18.5-24.9 kg/m2 and waistcircumference <35 for women and <40 for menWeight reduction programs that include diet,physical activity, and behavior counseling areencouraged.
Physical activity At least 30 min of moderate-intensity physicalexercise most daysFor those with disabilities after ischemic stroke, asupervised therapeutic exercise program
Coronary artery disease, cardiacdysrhythmias, congestive heart failure,and valvular disease
Treat disease and underlying cause asappropriate.
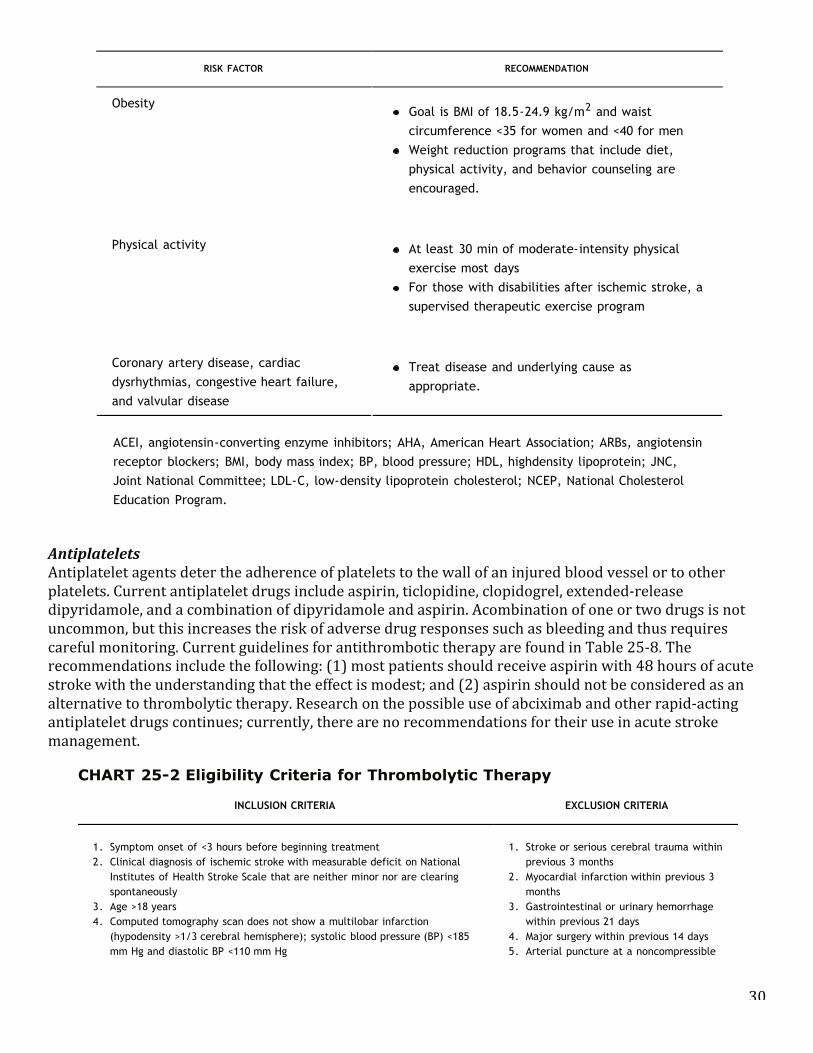
30
Antiplatelets Antiplatelet agents deter the adherence of platelets to the wall of an injured blood vessel or to other platelets. Current antiplatelet drugs include aspirin, ticlopidine, clopidogrel, extended-‐release dipyridamole, and a combination of dipyridamole and aspirin. Acombination of one or two drugs is not uncommon, but this increases the risk of adverse drug responses such as bleeding and thus requires careful monitoring. Current guidelines for antithrombotic therapy are found in Table 25-‐8. The recommendations include the following: (1) most patients should receive aspirin with 48 hours of acute stroke with the understanding that the effect is modest; and (2) aspirin should not be considered as an alternative to thrombolytic therapy. Research on the possible use of abciximab and other rapid-‐acting antiplatelet drugs continues; currently, there are no recommendations for their use in acute stroke management.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 37 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.605
The most recent evidence does not support the use of early anticoagulation to improve outcomes after acute
ischemic stroke.4,35 The most recent guidelines state that most stroke patients do not need emergency
administration of anticoagulants.4,31,36 Anticoagulation therapy is not recommended in lieu of intravenousthrombolysis and should be withheld in patients with moderate or severe stroke because of an increased risk forintracranial hemorrhage. It is further noted that despite lack of supporting data, anticoagulants are stillfrequently administered to patients with acute ischemic stroke. More studies are being conducted to determineif there are subgroups of patients who would benefit from
early anticoagulation therapy, but currently that information is lacking. In selected cases when anticoagulationtherapy is ordered, the INR is used to monitor blood coagulation. The use of prothrombin time (PT) to monitorblood coagulation has also been examined. It is now recommended that use of antifactor Xa replace PT for
blood coagulation monitoring.37
TABLE 25-7 GUIDELINES FOR THE PREVENTION OF STROKE IN PATIENTS WITH ISCHEMICSTROKE OR TRANSIENT ISCHEMIC ATTACKS*
RISK FACTOR RECOMMENDATION
Hypertension
Normal BP is defined as <120/80 mm
Hg by JNC-7†
JNC-7 notes that absolute target BPlevel and reduction are uncertainand should be individualized.
Maintain blood pressure <140 mm Hg and diastolicblood pressure <90 mm Hg or to individualtargeted levels.Institute lifestyle modifications.Drug therapy with diuretics and ACEIs should beprovided.Other antihypertensive therapy choices should beindividualized.
Diabetes mellitus
ACEIs and ARBs are effective inreducing progression of renaldisease.Near normal glycemic levels reducemicrovascular complications.
More rigorous control of BP and lipidsFor people with diabetes mellitus, target blood
pressure levels to <130/80 mm Hg†
Most patients will require more than one agent tocontrol BP (first-choice medications are ACEIs andARBs).Diet and oral hypoglycemics or insulin to keepfasting blood glucose levels <126 mg/dL or tomaintain hemoglobin A1c level <7.0%
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 38 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
Lipids
Follow NCEP III guidelines‡
Lifestyle modificationsDietary guidelinesMedications
AHA step II diet (!30% of calories derived fromfat, <7% from saturated fat, and <200 mg/dcholesterol consumed)Maintain ideal body weight.Regular exerciseTarget goals for LDL-C is <100 mg/dL, and LDL-C<70 mg/dL for very high-risk persons withmultiple risk factors.Statins are first-line drugs recommended for drugtherapy.If low HDL, consider niacin or gemfibrozil.
Cigarette smoking Discontinue smoking.Counseling, nicotine products, and oral smokingcessation medications are effective.Avoid environmental smoke.
Excessive alcohol intake Eliminate excessive alcohol intake.Formal alcohol cessation programs arerecommended.Two or fewer drinks per day for men and onedrink per day for nonpregnant women may beconsidered.
ObesityGoal is BMI of 18.5-24.9 kg/m2 and waistcircumference <35 for women and <40 for menWeight reduction programs that include diet,physical activity, and behavior counseling areencouraged.
Physical activity At least 30 min of moderate-intensity physicalexercise most daysFor those with disabilities after ischemic stroke, asupervised therapeutic exercise program
Coronary artery disease, cardiacdysrhythmias, congestive heart failure,and valvular disease
Treat disease and underlying cause asappropriate.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 39 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.606
ACEI, angiotensin-converting enzyme inhibitors; AHA, American Heart Association; ARBs, angiotensin
receptor blockers; BMI, body mass index; BP, blood pressure; HDL, highdensity lipoprotein; JNC,
Joint National Committee; LDL-C, low-density lipoprotein cholesterol; NCEP, National Cholesterol
Education Program.
* Sacco, R. L., Adams, R., Albers, G., et al. (2006). Guidelines for prevention of stroke in patients
with ischemic stroke or transient ischemic attack: A statement for healthcare professionals from the
American Heart Association/American Stroke Association Council on Stroke: Co-sponsored by the
Council on Cardiovascular Radiology and Intervention: The American Academy of Neurology affirms
the value of this guideline. Stroke, 37, 577-617.
† Chobanian, A. V., Bakris, G. L., Black, H. R., et al. (2004). The seventh report of the Joint
National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure:
The JNC 7 Report. JAMA, 289, 2560-2571.
‡ US National Heart, Lung, and Blood Institute, National Institutes of Health. (2001). The Third
Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation,
and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). NIH Publication No.
01-3670. Bethesda, MD: Author.
AntiplateletsAntiplatelet agents deter the adherence of platelets to the wall of an injured blood vessel or to other platelets.
Current antiplatelet drugs include aspirin, ticlopidine, clopidogrel, extended-release dipyridamole, and a
combination of dipyridamole and aspirin. Acombination of one or two drugs is not uncommon, but this increases
the risk of adverse drug responses such as bleeding and thus requires careful monitoring. Current guidelines for
antithrombotic therapy are found in Table 25-8.4 The recommendations include the following: (1) most patients
should receive aspirin with 48 hours of acute stroke with the understanding that the effect is modest; and (2)
aspirin should not be considered as an alternative to thrombolytic therapy. Research on the possible use of
abciximab and other rapid-acting antiplatelet drugs continues;
currently, there are no recommendations for their use in acute stroke management.
CHART 25-2 Eligibility Criteria for Thrombolytic Therapy
INCLUSION CRITERIA EXCLUSION CRITERIA
1. Symptom onset of <3 hours before beginning treatment
2. Clinical diagnosis of ischemic stroke with measurable deficit on National
Institutes of Health Stroke Scale that are neither minor nor are clearing
spontaneously
3. Age >18 years
4. Computed tomography scan does not show a multilobar infarction
(hypodensity >1/3 cerebral hemisphere); systolic blood pressure (BP) <185
mm Hg and diastolic BP <110 mm Hg
1. Stroke or serious cerebral trauma within
previous 3 months
2. Myocardial infarction within previous 3
months
3. Gastrointestinal or urinary hemorrhage
within previous 21 days
4. Major surgery within previous 14 days
5. Arterial puncture at a noncompressible
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 39 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.606
ACEI, angiotensin-converting enzyme inhibitors; AHA, American Heart Association; ARBs, angiotensin
receptor blockers; BMI, body mass index; BP, blood pressure; HDL, highdensity lipoprotein; JNC,
Joint National Committee; LDL-C, low-density lipoprotein cholesterol; NCEP, National Cholesterol
Education Program.
* Sacco, R. L., Adams, R., Albers, G., et al. (2006). Guidelines for prevention of stroke in patients
with ischemic stroke or transient ischemic attack: A statement for healthcare professionals from the
American Heart Association/American Stroke Association Council on Stroke: Co-sponsored by the
Council on Cardiovascular Radiology and Intervention: The American Academy of Neurology affirms
the value of this guideline. Stroke, 37, 577-617.
† Chobanian, A. V., Bakris, G. L., Black, H. R., et al. (2004). The seventh report of the Joint
National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure:
The JNC 7 Report. JAMA, 289, 2560-2571.
‡ US National Heart, Lung, and Blood Institute, National Institutes of Health. (2001). The Third
Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation,
and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). NIH Publication No.
01-3670. Bethesda, MD: Author.
AntiplateletsAntiplatelet agents deter the adherence of platelets to the wall of an injured blood vessel or to other platelets.
Current antiplatelet drugs include aspirin, ticlopidine, clopidogrel, extended-release dipyridamole, and a
combination of dipyridamole and aspirin. Acombination of one or two drugs is not uncommon, but this increases
the risk of adverse drug responses such as bleeding and thus requires careful monitoring. Current guidelines for
antithrombotic therapy are found in Table 25-8.4 The recommendations include the following: (1) most patients
should receive aspirin with 48 hours of acute stroke with the understanding that the effect is modest; and (2)
aspirin should not be considered as an alternative to thrombolytic therapy. Research on the possible use of
abciximab and other rapid-acting antiplatelet drugs continues;
currently, there are no recommendations for their use in acute stroke management.
CHART 25-2 Eligibility Criteria for Thrombolytic Therapy
INCLUSION CRITERIA EXCLUSION CRITERIA
1. Symptom onset of <3 hours before beginning treatment
2. Clinical diagnosis of ischemic stroke with measurable deficit on National
Institutes of Health Stroke Scale that are neither minor nor are clearing
spontaneously
3. Age >18 years
4. Computed tomography scan does not show a multilobar infarction
(hypodensity >1/3 cerebral hemisphere); systolic blood pressure (BP) <185
mm Hg and diastolic BP <110 mm Hg
1. Stroke or serious cerebral trauma within
previous 3 months
2. Myocardial infarction within previous 3
months
3. Gastrointestinal or urinary hemorrhage
within previous 21 days
4. Major surgery within previous 14 days
5. Arterial puncture at a noncompressible

31
Neuroprotective Agents A number of potential neuroprotective agents have been considered that represent a broad spectrum of drugs with disparate mechanisms of action: sodium channel blockers, calcium channel antagonists, free radical scavengers, membrane stabilizers, glutamate receptor antagonists, and gammaaminobutyric acid (GABA) agonists. Currently, new drugs are being investigated. However, no agent has demonstrated clinical benefit, andno drug is currently recommended as a useful neuroprotective agent.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 39 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.606
ACEI, angiotensin-converting enzyme inhibitors; AHA, American Heart Association; ARBs, angiotensin
receptor blockers; BMI, body mass index; BP, blood pressure; HDL, highdensity lipoprotein; JNC,
Joint National Committee; LDL-C, low-density lipoprotein cholesterol; NCEP, National Cholesterol
Education Program.
* Sacco, R. L., Adams, R., Albers, G., et al. (2006). Guidelines for prevention of stroke in patients
with ischemic stroke or transient ischemic attack: A statement for healthcare professionals from the
American Heart Association/American Stroke Association Council on Stroke: Co-sponsored by the
Council on Cardiovascular Radiology and Intervention: The American Academy of Neurology affirms
the value of this guideline. Stroke, 37, 577-617.
† Chobanian, A. V., Bakris, G. L., Black, H. R., et al. (2004). The seventh report of the Joint
National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure:
The JNC 7 Report. JAMA, 289, 2560-2571.
‡ US National Heart, Lung, and Blood Institute, National Institutes of Health. (2001). The Third
Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation,
and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). NIH Publication No.
01-3670. Bethesda, MD: Author.
AntiplateletsAntiplatelet agents deter the adherence of platelets to the wall of an injured blood vessel or to other platelets.
Current antiplatelet drugs include aspirin, ticlopidine, clopidogrel, extended-release dipyridamole, and a
combination of dipyridamole and aspirin. Acombination of one or two drugs is not uncommon, but this increases
the risk of adverse drug responses such as bleeding and thus requires careful monitoring. Current guidelines for
antithrombotic therapy are found in Table 25-8.4 The recommendations include the following: (1) most patients
should receive aspirin with 48 hours of acute stroke with the understanding that the effect is modest; and (2)
aspirin should not be considered as an alternative to thrombolytic therapy. Research on the possible use of
abciximab and other rapid-acting antiplatelet drugs continues;
currently, there are no recommendations for their use in acute stroke management.
CHART 25-2 Eligibility Criteria for Thrombolytic Therapy
INCLUSION CRITERIA EXCLUSION CRITERIA
1. Symptom onset of <3 hours before beginning treatment
2. Clinical diagnosis of ischemic stroke with measurable deficit on National
Institutes of Health Stroke Scale that are neither minor nor are clearing
spontaneously
3. Age >18 years
4. Computed tomography scan does not show a multilobar infarction
(hypodensity >1/3 cerebral hemisphere); systolic blood pressure (BP) <185
mm Hg and diastolic BP <110 mm Hg
1. Stroke or serious cerebral trauma within
previous 3 months
2. Myocardial infarction within previous 3
months
3. Gastrointestinal or urinary hemorrhage
within previous 21 days
4. Major surgery within previous 14 days
5. Arterial puncture at a noncompressible
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 40 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
5. If received heparin in previous 48 hours, activated partial thromboplastin
time must be in normal range
6. Platelet count !100,000 mm3
7. Blood glucose !50 mg/dL (2.7 mmol/L)
8. No seizures with postictal residual neurological impairment
site within previous 7 days
6. History of previous intracranial
hemorrhage
7. Systolic BP >185 mm Hg or diastolic BP
>110 mm Hg or BP readings that require
aggressive treatment
8. Evidence of active bleeding or acute
trauma (fracture) on examination
9. Taking oral anticoagulants or if
anticoagulant being taken, international
normalized ratio >1.7
10. Woman of childbearing age who has a
positive pregnancy test result
From Adams, H. P, Adams, R. J., Brott, T., et al. (2003). Guidelines for the early management of patients with ischemic stroke: A
scientific statement from the Stroke Council of the American Stroke Association. Stroke, 34, 1056-1083; and Adams, H., Adams, R.,
Del Zappo, G., & Goldstein, L. B. (2005). Guidelines for the early management of patients with ischemic stroke: 2005 Guidelines
update. Stroke, 36, 916-921.
Neuroprotective Agents
A number of potential neuroprotective agents have been considered that represent a broad spectrum of drugs
with disparate mechanisms of action: sodium channel blockers, calcium channel antagonists, free radical
scavengers, membrane stabilizers, glutamate receptor antagonists, and gammaaminobutyric acid (GABA)
agonists. Currently, new drugs are being investigated. However, no agent has demonstrated clinical benefit, and
no drug is currently recommended as a useful neuroprotective agent.4,31
TABLE 25-8 USE OF ANTITHROMBOTIC AGENTS FOR PATIENTS WITH ISCHEMIC STROKE ORTIAs (ORAL ANTICOAGULANT AND ANTIPLATELET THERAPIES)
EVENT RECOMMENDED THERAPY COMMENT
TIAs or noncardioembolic
ischemic stroke
Any of the following
are recommended:
ASA 50-325 mg/d
ASA and ER-DP
(single
formulation)
Clopidogrel 75 mg
Antiplatelet agents rather than oral
anticoagulation are recommended
to reduce risk of recurrent stroke
or cardiovascular events.
Compared to ASA alone, both the
combination of ASA and ER-DP or
clopidogrel is safe.
The combination of ASA and ER-DP
is suggested over ASA alone.
Selection of an antiplatelet should
be individualized based on risk
factors, tolerance, and clinical
characteristics.
For patients allergic to ASA,
clopidogrel is used.
If patient has an ischemic
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 40 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
5. If received heparin in previous 48 hours, activated partial thromboplastin
time must be in normal range
6. Platelet count !100,000 mm3
7. Blood glucose !50 mg/dL (2.7 mmol/L)
8. No seizures with postictal residual neurological impairment
site within previous 7 days
6. History of previous intracranial
hemorrhage
7. Systolic BP >185 mm Hg or diastolic BP
>110 mm Hg or BP readings that require
aggressive treatment
8. Evidence of active bleeding or acute
trauma (fracture) on examination
9. Taking oral anticoagulants or if
anticoagulant being taken, international
normalized ratio >1.7
10. Woman of childbearing age who has a
positive pregnancy test result
From Adams, H. P, Adams, R. J., Brott, T., et al. (2003). Guidelines for the early management of patients with ischemic stroke: A
scientific statement from the Stroke Council of the American Stroke Association. Stroke, 34, 1056-1083; and Adams, H., Adams, R.,
Del Zappo, G., & Goldstein, L. B. (2005). Guidelines for the early management of patients with ischemic stroke: 2005 Guidelines
update. Stroke, 36, 916-921.
Neuroprotective Agents
A number of potential neuroprotective agents have been considered that represent a broad spectrum of drugs
with disparate mechanisms of action: sodium channel blockers, calcium channel antagonists, free radical
scavengers, membrane stabilizers, glutamate receptor antagonists, and gammaaminobutyric acid (GABA)
agonists. Currently, new drugs are being investigated. However, no agent has demonstrated clinical benefit, and
no drug is currently recommended as a useful neuroprotective agent.4,31
TABLE 25-8 USE OF ANTITHROMBOTIC AGENTS FOR PATIENTS WITH ISCHEMIC STROKE ORTIAs (ORAL ANTICOAGULANT AND ANTIPLATELET THERAPIES)
EVENT RECOMMENDED THERAPY COMMENT
TIAs or noncardioembolic
ischemic stroke
Any of the following
are recommended:
ASA 50-325 mg/d
ASA and ER-DP
(single
formulation)
Clopidogrel 75 mg
Antiplatelet agents rather than oral
anticoagulation are recommended
to reduce risk of recurrent stroke
or cardiovascular events.
Compared to ASA alone, both the
combination of ASA and ER-DP or
clopidogrel is safe.
The combination of ASA and ER-DP
is suggested over ASA alone.
Selection of an antiplatelet should
be individualized based on risk
factors, tolerance, and clinical
characteristics.
For patients allergic to ASA,
clopidogrel is used.
If patient has an ischemic5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 41 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.607
cerebrovascular event while on
ASA, there is no evidence
supporting benefit from increasing
dose.
Patients with ischemic
stroke or TIA with
persistent or paroxysmal
(intermittent) atrial
fibrillation
Anticoagulation with
adjusted dose of
warfarin is
recommended:
Warfarin (target
2.5) with a range
of 2.0-3.0 INR
For patient
unable to take
oral
anticoagulants,
ASA 325 mg/d
recommended
INR must be monitored periodically.
Patient education is important to
inform patient about diet, side
effects, safety, and adherence to
dosage based on INR.
Inform patient of bleeding risk.
ASA, acetylsalicylic acid; ER-DP, extended-release dipyridamole; INR, international normalized ratio;
TIA, transient ischemic attack.
From Sacco, R. L., Adams, R., Albers, G., et al. (2006). Guidelines for prevention of stroke in
patients with ischemic stroke or transient ischemic attack: A statement for healthcare professionals
from the American Heart Association/American Stroke Association Council on Stroke: Co-sponsored
by the Council on Cardiovascular Radiology and Intervention: The American Academy of Neurology
affirms the value of this guideline. Stroke, 37, 577-617.
HypothermiaIn recent years there has been increasing interest in the use of hypothermia in acute stroke patients.
Hypothermia (i.e., 32_C to 34_C) has been used in the setting of neurosurgical and cardiothoracic surgery for its
neuroprotective benefits, and also in the management of severe brain injury and cardiac arrest. However,
hypothermia also carries risks of fatal cardiac dysrhythmias, coagulopathies, electrolyte derangement, and other
problems. Although hypothermia research for stroke is promising, the current state of the science is insufficient
to recommend its use for the management of stroke patients.4,31
Surgical and Endovascular InterventionsSelected patients with extracranial or intracranial atherosclerotic disease located in accessible sites may be
good candidates for surgery. The goal of the surgical procedures is to prevent TIAs or stroke. Carotid
endarterectomy (CEA) and extracranial/intracranial (EC-IC) arterial bypass are designed to improve cerebral
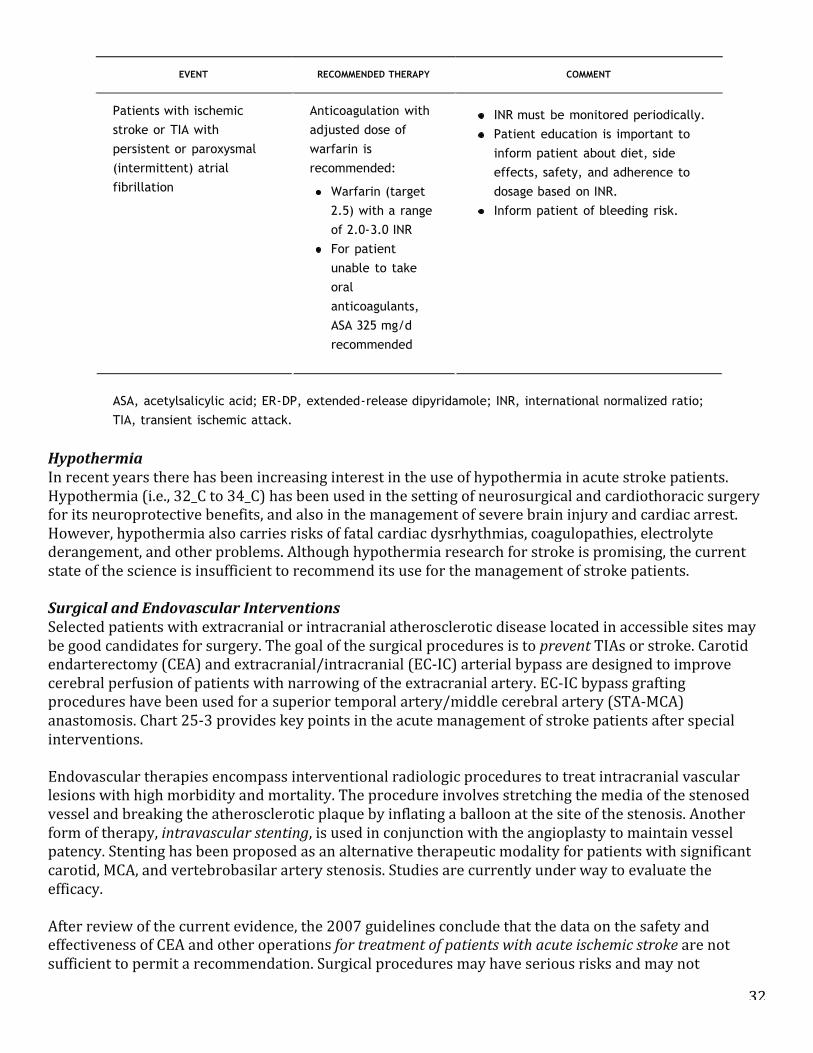
32
Hypothermia In recent years there has been increasing interest in the use of hypothermia in acute stroke patients. Hypothermia (i.e., 32_C to 34_C) has been used in the setting of neurosurgical and cardiothoracic surgery for its neuroprotective benefits, and also in the management of severe brain injury and cardiac arrest. However, hypothermia also carries risks of fatal cardiac dysrhythmias, coagulopathies, electrolyte derangement, and other problems. Although hypothermia research for stroke is promising, the current state of the science is insufficient to recommend its use for the management of stroke patients. Surgical and Endovascular Interventions Selected patients with extracranial or intracranial atherosclerotic disease located in accessible sites may be good candidates for surgery. The goal of the surgical procedures is to prevent TIAs or stroke. Carotid endarterectomy (CEA) and extracranial/intracranial (EC-‐IC) arterial bypass are designed to improve cerebral perfusion of patients with narrowing of the extracranial artery. EC-‐IC bypass grafting procedures have been used for a superior temporal artery/middle cerebral artery (STA-‐MCA) anastomosis. Chart 25-‐3 provides key points in the acute management of stroke patients after special interventions. Endovascular therapies encompass interventional radiologic procedures to treat intracranial vascular lesions with high morbidity and mortality. The procedure involves stretching the media of the stenosed vessel and breaking the atherosclerotic plaque by inflating a balloon at the site of the stenosis. Another form of therapy, intravascular stenting, is used in conjunction with the angioplasty to maintain vessel patency. Stenting has been proposed as an alternative therapeutic modality for patients with significant carotid, MCA, and vertebrobasilar artery stenosis. Studies are currently under way to evaluate the efficacy. After review of the current evidence, the 2007 guidelines conclude that the data on the safety and effectiveness of CEA and other operations for treatment of patients with acute ischemic stroke are not sufficient to permit a recommendation. Surgical procedures may have serious risks and may not
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 40 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
5. If received heparin in previous 48 hours, activated partial thromboplastin
time must be in normal range
6. Platelet count !100,000 mm3
7. Blood glucose !50 mg/dL (2.7 mmol/L)
8. No seizures with postictal residual neurological impairment
site within previous 7 days
6. History of previous intracranial
hemorrhage
7. Systolic BP >185 mm Hg or diastolic BP
>110 mm Hg or BP readings that require
aggressive treatment
8. Evidence of active bleeding or acute
trauma (fracture) on examination
9. Taking oral anticoagulants or if
anticoagulant being taken, international
normalized ratio >1.7
10. Woman of childbearing age who has a
positive pregnancy test result
From Adams, H. P, Adams, R. J., Brott, T., et al. (2003). Guidelines for the early management of patients with ischemic stroke: A
scientific statement from the Stroke Council of the American Stroke Association. Stroke, 34, 1056-1083; and Adams, H., Adams, R.,
Del Zappo, G., & Goldstein, L. B. (2005). Guidelines for the early management of patients with ischemic stroke: 2005 Guidelines
update. Stroke, 36, 916-921.
Neuroprotective Agents
A number of potential neuroprotective agents have been considered that represent a broad spectrum of drugs
with disparate mechanisms of action: sodium channel blockers, calcium channel antagonists, free radical
scavengers, membrane stabilizers, glutamate receptor antagonists, and gammaaminobutyric acid (GABA)
agonists. Currently, new drugs are being investigated. However, no agent has demonstrated clinical benefit, and
no drug is currently recommended as a useful neuroprotective agent.4,31
TABLE 25-8 USE OF ANTITHROMBOTIC AGENTS FOR PATIENTS WITH ISCHEMIC STROKE ORTIAs (ORAL ANTICOAGULANT AND ANTIPLATELET THERAPIES)
EVENT RECOMMENDED THERAPY COMMENT
TIAs or noncardioembolic
ischemic stroke
Any of the following
are recommended:
ASA 50-325 mg/d
ASA and ER-DP
(single
formulation)
Clopidogrel 75 mg
Antiplatelet agents rather than oral
anticoagulation are recommended
to reduce risk of recurrent stroke
or cardiovascular events.
Compared to ASA alone, both the
combination of ASA and ER-DP or
clopidogrel is safe.
The combination of ASA and ER-DP
is suggested over ASA alone.
Selection of an antiplatelet should
be individualized based on risk
factors, tolerance, and clinical
characteristics.
For patients allergic to ASA,
clopidogrel is used.
If patient has an ischemic
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 41 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.607
cerebrovascular event while on
ASA, there is no evidence
supporting benefit from increasing
dose.
Patients with ischemic
stroke or TIA with
persistent or paroxysmal
(intermittent) atrial
fibrillation
Anticoagulation with
adjusted dose of
warfarin is
recommended:
Warfarin (target
2.5) with a range
of 2.0-3.0 INR
For patient
unable to take
oral
anticoagulants,
ASA 325 mg/d
recommended
INR must be monitored periodically.
Patient education is important to
inform patient about diet, side
effects, safety, and adherence to
dosage based on INR.
Inform patient of bleeding risk.
ASA, acetylsalicylic acid; ER-DP, extended-release dipyridamole; INR, international normalized ratio;
TIA, transient ischemic attack.
From Sacco, R. L., Adams, R., Albers, G., et al. (2006). Guidelines for prevention of stroke in
patients with ischemic stroke or transient ischemic attack: A statement for healthcare professionals
from the American Heart Association/American Stroke Association Council on Stroke: Co-sponsored
by the Council on Cardiovascular Radiology and Intervention: The American Academy of Neurology
affirms the value of this guideline. Stroke, 37, 577-617.
HypothermiaIn recent years there has been increasing interest in the use of hypothermia in acute stroke patients.
Hypothermia (i.e., 32_C to 34_C) has been used in the setting of neurosurgical and cardiothoracic surgery for its
neuroprotective benefits, and also in the management of severe brain injury and cardiac arrest. However,
hypothermia also carries risks of fatal cardiac dysrhythmias, coagulopathies, electrolyte derangement, and other
problems. Although hypothermia research for stroke is promising, the current state of the science is insufficient
to recommend its use for the management of stroke patients.4,31
Surgical and Endovascular InterventionsSelected patients with extracranial or intracranial atherosclerotic disease located in accessible sites may be
good candidates for surgery. The goal of the surgical procedures is to prevent TIAs or stroke. Carotid
endarterectomy (CEA) and extracranial/intracranial (EC-IC) arterial bypass are designed to improve cerebral
33
favorably alter the outcome of the patient. Carotid Endarterectomy The North American Symptomatic Carotid Endarterectomy Trial (NASCET) clearly demonstrated that CEA is superior to medical therapy alone for stroke prevention in patients with 70% or greater symptomatic internal carotid artery stenosis. Patients with 70% or greater carotid stenosis, without major operative risk factors, have a relative reduction of about 60% and absolute risk reduction of 5% to 10% per year within the subsequent 2 years. In one study, patients with 50% to 69% stenosis with a recent TIA or minor stroke had a reduced stroke rate with endarterectomy versus medical treatment. However, the absolute benefit of surgery is less than that for patients with higher degrees of stenosis and among women and patients with retinal TIAs. When CEA is indicated, surgery within 2 weeks is suggested rather than delay. Patients with less than 50% stenosis with recent symptoms do not benefit from CEA. Antiplatelet therapy is recommended for these patients. The “hot spots” for atheroma build-‐up are noted in Figure 25-‐8. ACEA consists of careful removal of the atherosclerotic plaque from the artery after a temporary bypass shunt has been created to provide adequate cerebral perfusion. The plaque is removed after the artery is temporarily occluded both above and below the atheroma. The bypass graft also improves circulation. The major danger during surgery is embolization of atherogenic plaque and thrombi from excessive manipulation of the carotid bifurcation. On completion, a Jackson-‐Pratt is usually inserted at the operative site to prevent development of a hematoma. The major postoperative concerns are blood pressure instability, stroke or transient neurological deficits, cranial nerve injury (facial, vagal), wound hematoma, suture line rupture, TIAs, and hyperperfusion syndromes. After surgery, patients experience a period of postoperative blood pressure instability that lasts for approximately 12 to 24 hours, probably as a result of a carotid sinus malfunction and loss of effective baroreceptor action. After blood flow has been restored, maintenance of the systolic pressure at a constant level of approximately 150 mm Hg is critical. The sudden restoration of high flow, especially after removal of a tight stenosis and in the presence of heparin (used during surgery) or antiplatelets, can lead to intracerebral hemorrhage. Hypotensive episodes are just as disastrous and can result in ischemic stroke or TIAs. The potential for cranial nerve injury results from the proximity of these nerves to the operative site. Hyperperfusion syndromes are related to the marked increase in cerebral blood flow after CEA. Patients often have paralysis of autoregulation ipsilateral to the surgical site so that the profound increase in blood flow is not blunted. When this occurs, blood pressure must be meticulously maintained in the 120 to 130 mm Hg range. Patients may experience vascular headaches or catastrophic intracerebral hemorrhage. Seizures may occur about 7 to 10 days postoperatively. Finally, a leading cause of death after CEA is myocardial infarction, either immediate or delayed. The patient should be monitored carefully for evidence of myocardial ischemia or infarction. There is no evidence to recommend emergent CEA or other surgical procedures in management of acute ischemic stroke. Currently, CEA is recommended for selected patients who meet criteria as a stroke preventive measure. Superficial Temporal Artery-Middle Cerebral Artery Anastomosis EC-‐IC arterial bypass, most often of the STAto the MCA, is a microsurgical procedure used in the past to allegedly provide collateral circulation to the areas of the brain supplied by the MCA. Currently, this procedure is used infrequently because of the negative results reported in the EC/IC Bypass Trial and other clinical experience. National guidelines do not recommended it for acute stroke management.
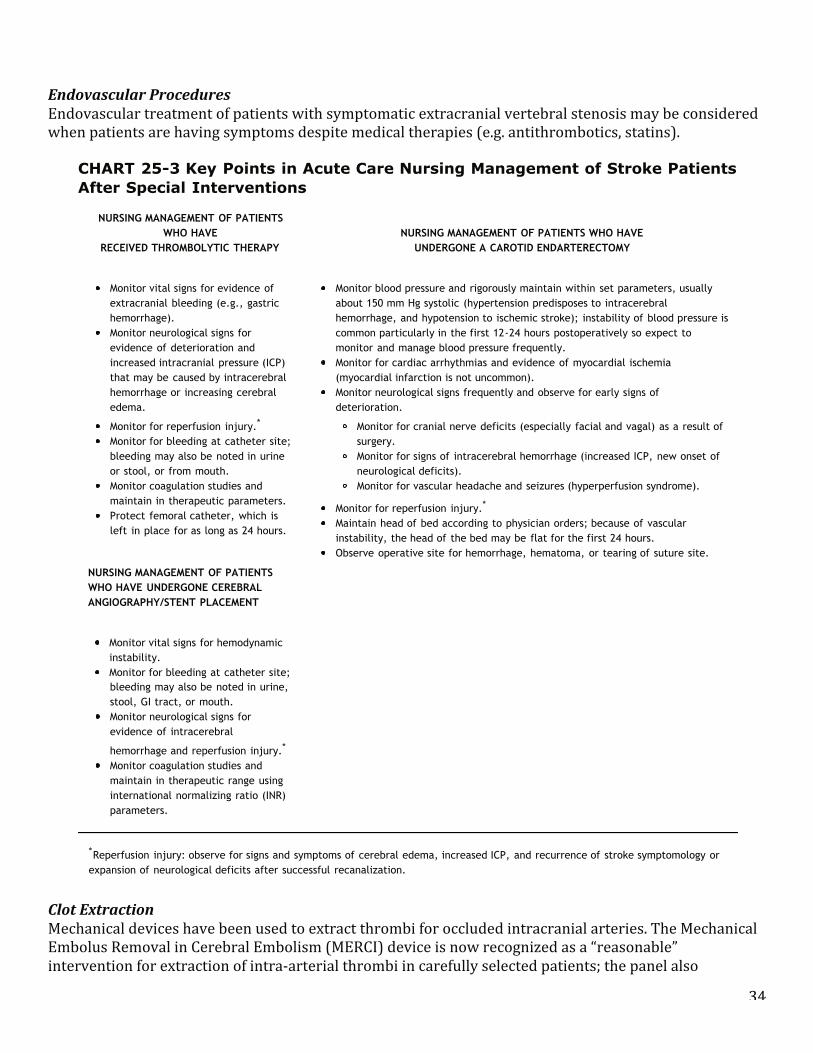
34
Endovascular Procedures Endovascular treatment of patients with symptomatic extracranial vertebral stenosis may be considered when patients are having symptoms despite medical therapies (e.g. antithrombotics, statins).
Clot Extraction Mechanical devices have been used to extract thrombi for occluded intracranial arteries. The Mechanical Embolus Removal in Cerebral Embolism (MERCI) device is now recognized as a “reasonable” intervention for extraction of intra-‐arterial thrombi in carefully selected patients; the panel also
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 43 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.608
7 to 10 days postoperatively. Finally, a leading cause of death after CEA is myocardial infarction, eitherimmediate or delayed. The patient should be monitored carefully for evidence of myocardial ischemia orinfarction.
There is no evidence to recommend emergent CEA or other surgical procedures in management of acuteischemic stroke. Currently, CEA is recommended for selected patients who meet criteria as a stroke preventivemeasure.
Superficial Temporal Artery-Middle Cerebral Artery Anastomosis
EC-IC arterial bypass, most often of the STAto the MCA, is a microsurgical procedure used in the past toallegedly provide collateral circulation to the areas of the brain supplied by the MCA. Currently, this procedureis used infrequently because of the negative results reported in the EC/IC Bypass Trial and other clinical
experience.43,44 National guidelines do not recommended it for acute stroke management.4,31,41
Endovascular Procedures
Endovascular treatment of patients with symptomatic extracranial vertebral stenosis may be considered when
patients are having symptoms despite medical therapies (e.g. antithrombotics, statins).41
CHART 25-3 Key Points in Acute Care Nursing Management of Stroke PatientsAfter Special Interventions
NURSING MANAGEMENT OF PATIENTSWHO HAVE
RECEIVED THROMBOLYTIC THERAPYNURSING MANAGEMENT OF PATIENTS WHO HAVE
UNDERGONE A CAROTID ENDARTERECTOMY
Monitor vital signs for evidence ofextracranial bleeding (e.g., gastrichemorrhage).Monitor neurological signs forevidence of deterioration andincreased intracranial pressure (ICP)that may be caused by intracerebralhemorrhage or increasing cerebraledema.
Monitor for reperfusion injury.*
Monitor for bleeding at catheter site;bleeding may also be noted in urineor stool, or from mouth.Monitor coagulation studies andmaintain in therapeutic parameters.Protect femoral catheter, which isleft in place for as long as 24 hours.
Monitor blood pressure and rigorously maintain within set parameters, usuallyabout 150 mm Hg systolic (hypertension predisposes to intracerebralhemorrhage, and hypotension to ischemic stroke); instability of blood pressure iscommon particularly in the first 12-24 hours postoperatively so expect tomonitor and manage blood pressure frequently.Monitor for cardiac arrhythmias and evidence of myocardial ischemia(myocardial infarction is not uncommon).Monitor neurological signs frequently and observe for early signs ofdeterioration.
Monitor for cranial nerve deficits (especially facial and vagal) as a result ofsurgery.Monitor for signs of intracerebral hemorrhage (increased ICP, new onset ofneurological deficits).Monitor for vascular headache and seizures (hyperperfusion syndrome).
Monitor for reperfusion injury.*
Maintain head of bed according to physician orders; because of vascularinstability, the head of the bed may be flat for the first 24 hours.Observe operative site for hemorrhage, hematoma, or tearing of suture site.
NURSING MANAGEMENT OF PATIENTSWHO HAVE UNDERGONE CEREBRALANGIOGRAPHY/STENT PLACEMENT
Monitor vital signs for hemodynamicinstability.Monitor for bleeding at catheter site;
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 43 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.608
7 to 10 days postoperatively. Finally, a leading cause of death after CEA is myocardial infarction, eitherimmediate or delayed. The patient should be monitored carefully for evidence of myocardial ischemia orinfarction.
There is no evidence to recommend emergent CEA or other surgical procedures in management of acuteischemic stroke. Currently, CEA is recommended for selected patients who meet criteria as a stroke preventivemeasure.
Superficial Temporal Artery-Middle Cerebral Artery Anastomosis
EC-IC arterial bypass, most often of the STAto the MCA, is a microsurgical procedure used in the past toallegedly provide collateral circulation to the areas of the brain supplied by the MCA. Currently, this procedureis used infrequently because of the negative results reported in the EC/IC Bypass Trial and other clinical
experience.43,44 National guidelines do not recommended it for acute stroke management.4,31,41
Endovascular Procedures
Endovascular treatment of patients with symptomatic extracranial vertebral stenosis may be considered when
patients are having symptoms despite medical therapies (e.g. antithrombotics, statins).41
CHART 25-3 Key Points in Acute Care Nursing Management of Stroke PatientsAfter Special Interventions
NURSING MANAGEMENT OF PATIENTSWHO HAVE
RECEIVED THROMBOLYTIC THERAPYNURSING MANAGEMENT OF PATIENTS WHO HAVE
UNDERGONE A CAROTID ENDARTERECTOMY
Monitor vital signs for evidence ofextracranial bleeding (e.g., gastrichemorrhage).Monitor neurological signs forevidence of deterioration andincreased intracranial pressure (ICP)that may be caused by intracerebralhemorrhage or increasing cerebraledema.
Monitor for reperfusion injury.*
Monitor for bleeding at catheter site;bleeding may also be noted in urineor stool, or from mouth.Monitor coagulation studies andmaintain in therapeutic parameters.Protect femoral catheter, which isleft in place for as long as 24 hours.
Monitor blood pressure and rigorously maintain within set parameters, usuallyabout 150 mm Hg systolic (hypertension predisposes to intracerebralhemorrhage, and hypotension to ischemic stroke); instability of blood pressure iscommon particularly in the first 12-24 hours postoperatively so expect tomonitor and manage blood pressure frequently.Monitor for cardiac arrhythmias and evidence of myocardial ischemia(myocardial infarction is not uncommon).Monitor neurological signs frequently and observe for early signs ofdeterioration.
Monitor for cranial nerve deficits (especially facial and vagal) as a result ofsurgery.Monitor for signs of intracerebral hemorrhage (increased ICP, new onset ofneurological deficits).Monitor for vascular headache and seizures (hyperperfusion syndrome).
Monitor for reperfusion injury.*
Maintain head of bed according to physician orders; because of vascularinstability, the head of the bed may be flat for the first 24 hours.Observe operative site for hemorrhage, hematoma, or tearing of suture site.
NURSING MANAGEMENT OF PATIENTSWHO HAVE UNDERGONE CEREBRALANGIOGRAPHY/STENT PLACEMENT
Monitor vital signs for hemodynamicinstability.Monitor for bleeding at catheter site;
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 44 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.609
bleeding may also be noted in urine,stool, GI tract, or mouth.Monitor neurological signs forevidence of intracerebral
hemorrhage and reperfusion injury.*
Monitor coagulation studies andmaintain in therapeutic range usinginternational normalizing ratio (INR)parameters.
*Reperfusion injury: observe for signs and symptoms of cerebral edema, increased ICP, and recurrence of stroke symptomology orexpansion of neurological deficits after successful recanalization.
Clot Extraction
Mechanical devices have been used to extract thrombi for occluded intracranial arteries.45 The MechanicalEmbolus Removal in Cerebral Embolism (MERCI) device is now recognized as a “reasonable” intervention forextraction of intra-arterial thrombi in carefully selected patients; the panel also recognized that the utility ofthe device in improving outcomes after stroke is unclear. Further study is recommended to define its role in
emergency stroke management.4
Acute Management of Intracerebral Hemorrhage StrokeAmerican Heart Association guidelines have been updated for the management of spontaneous intracerebral
hemorrhage in adults and are the basis for current evidence-based practice.46 The general principles andrecommendations include an intensive care unit environment for the monitoring and treatment of patients withICH stroke because of the emergent nature of the condition and the frequent elevations in ICP and bloodpressure, frequent need for intubation and assisted ventilation, and multiple complicating medical problems.The management of the increased ICP is based on a continuum from simple measures such as elevation of thehead of the bed 30 degrees to mannitol, ventriculostomy, and hyperventilation based on the clinical condition.Acute management of increased ICP is outlined in Chapter 13. Other recommendations include maintainingnormal blood glucose (_300 mg/dL), normothermia (treatment of fever to normal body temperature),management of blood pressure (although it is clear that evidence is incomplete in blood pressure managementin ICH), and use of antiepileptic drugs to treat seizures. For management of blood pressure of a systolic pressuregreater than 200 mm Hg, intravenous antihypertensive therapy should be considered with a target of 160/90 mmHg.
Other recommendations focus on management of coagulation and fibrinolysis issues related to ICH. This includesthe use of protamine sulfate to reverse heparin-associated ICH; intravenous vitamin K for warfarin-associatedICH; and fresh frozen plasma as an option to address the coagulopathies that occur with ICH. Restartingantithrombotic therapy after ICH depends on the risk of possible arterial or venous thromboembolism andrecurrent ICH. Low-molecular-weight
heparin may be considered 3 to 4 days after ICH for prophylaxis. Elastic hose and intermittent pneumaticcompression stockings should be provided for patients with hemiparesis or hemiplegia. In treating patients withICH caused by thrombolytics, urgent therapies are directed at replacing clotting factors and platelets.
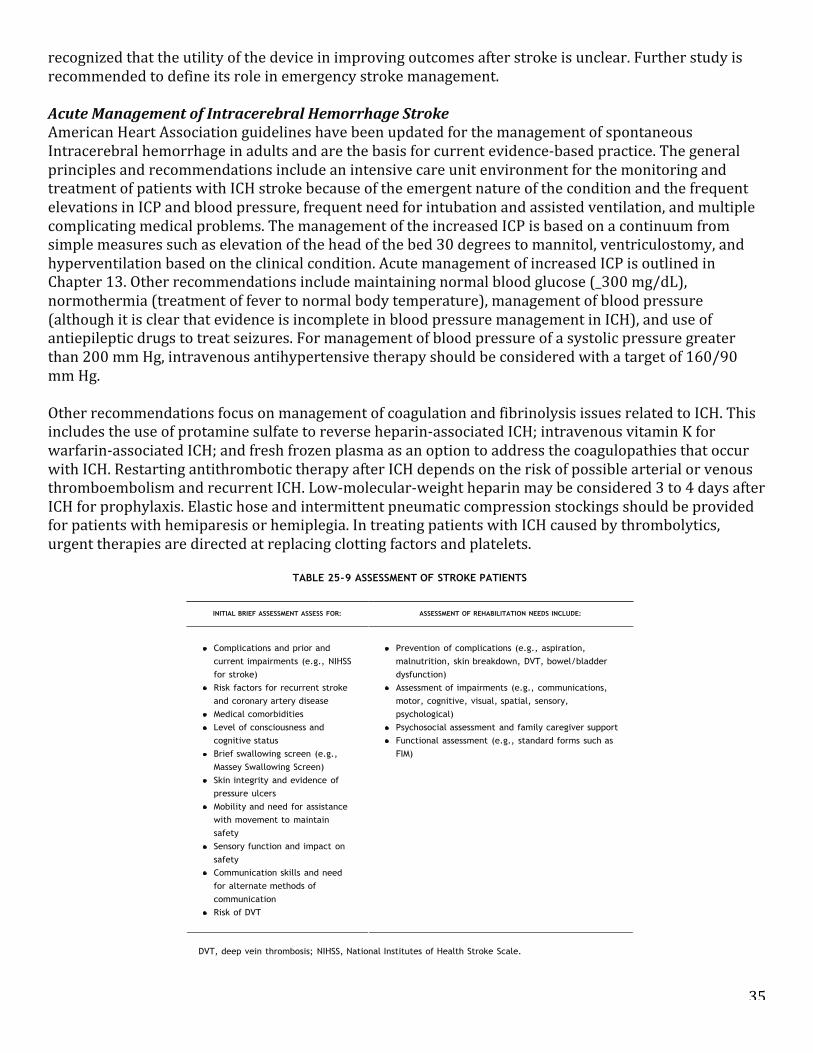
35
recognized that the utility of the device in improving outcomes after stroke is unclear. Further study is recommended to define its role in emergency stroke management. Acute Management of Intracerebral Hemorrhage Stroke American Heart Association guidelines have been updated for the management of spontaneous Intracerebral hemorrhage in adults and are the basis for current evidence-‐based practice. The general principles and recommendations include an intensive care unit environment for the monitoring and treatment of patients with ICH stroke because of the emergent nature of the condition and the frequent elevations in ICP and blood pressure, frequent need for intubation and assisted ventilation, and multiple complicating medical problems. The management of the increased ICP is based on a continuum from simple measures such as elevation of the head of the bed 30 degrees to mannitol, ventriculostomy, and hyperventilation based on the clinical condition. Acute management of increased ICP is outlined in Chapter 13. Other recommendations include maintaining normal blood glucose (_300 mg/dL), normothermia (treatment of fever to normal body temperature), management of blood pressure (although it is clear that evidence is incomplete in blood pressure management in ICH), and use of antiepileptic drugs to treat seizures. For management of blood pressure of a systolic pressure greater than 200 mm Hg, intravenous antihypertensive therapy should be considered with a target of 160/90 mm Hg. Other recommendations focus on management of coagulation and fibrinolysis issues related to ICH. This includes the use of protamine sulfate to reverse heparin-‐associated ICH; intravenous vitamin K for warfarin-‐associated ICH; and fresh frozen plasma as an option to address the coagulopathies that occur with ICH. Restarting antithrombotic therapy after ICH depends on the risk of possible arterial or venous thromboembolism and recurrent ICH. Low-‐molecular-‐weight heparin may be considered 3 to 4 days after ICH for prophylaxis. Elastic hose and intermittent pneumatic compression stockings should be provided for patients with hemiparesis or hemiplegia. In treating patients with ICH caused by thrombolytics, urgent therapies are directed at replacing clotting factors and platelets.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 45 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
TABLE 25-9 ASSESSMENT OF STROKE PATIENTS
INITIAL BRIEF ASSESSMENT ASSESS FOR: ASSESSMENT OF REHABILITATION NEEDS INCLUDE:
Complications and prior andcurrent impairments (e.g., NIHSSfor stroke)Risk factors for recurrent strokeand coronary artery diseaseMedical comorbiditiesLevel of consciousness andcognitive statusBrief swallowing screen (e.g.,Massey Swallowing Screen)Skin integrity and evidence ofpressure ulcersMobility and need for assistancewith movement to maintainsafetySensory function and impact onsafetyCommunication skills and needfor alternate methods ofcommunicationRisk of DVT
Prevention of complications (e.g., aspiration,malnutrition, skin breakdown, DVT, bowel/bladderdysfunction)Assessment of impairments (e.g., communications,motor, cognitive, visual, spatial, sensory,psychological)Psychosocial assessment and family caregiver supportFunctional assessment (e.g., standard forms such asFIM)
DVT, deep vein thrombosis; NIHSS, National Institutes of Health Stroke Scale.
Surgical interventions for ICH are also addressed. The following are recommended for possible surgicalapproaches for patients with cerebellar hemorrhages greater than 3 cm with neurological deterioration orbrainstem compression: compression and/or hydrocephalus from ventricular obstruction need evacuation of thehemorrhage as soon as possible; and supratentorial ICH should undergo standard craniotomy for a lobar clotlocated within 1 cm of the surface. Other combined surgical and direct drug infusion therapies are underinvestigation, but are not a recommended standard for care currently.
As mentioned above, surgical decompression and stereotactically guided removal of the hematoma may be
necessary in certain cases.12 Care of the postoperative neurosurgical patient is discussed in Chapter 14.Vasospasms are not considered a problem with ICH. Chapter 23 provides guidance for patient management. Forpatients who survive, rehabilitation is necessary. In addition, identification and modification of risk factors needto be undertaken. Nursing management is outlined in Chapters 13 and 23.
For patients with catastrophic stroke, palliative care may be an option for patients with severe morbidity thatwill have a significant impact on quality of life and severe disability. Continuation of aggressive treatment maylead to placement in a long-term chronic care facility. Difficult discussions with and decisions by the patient
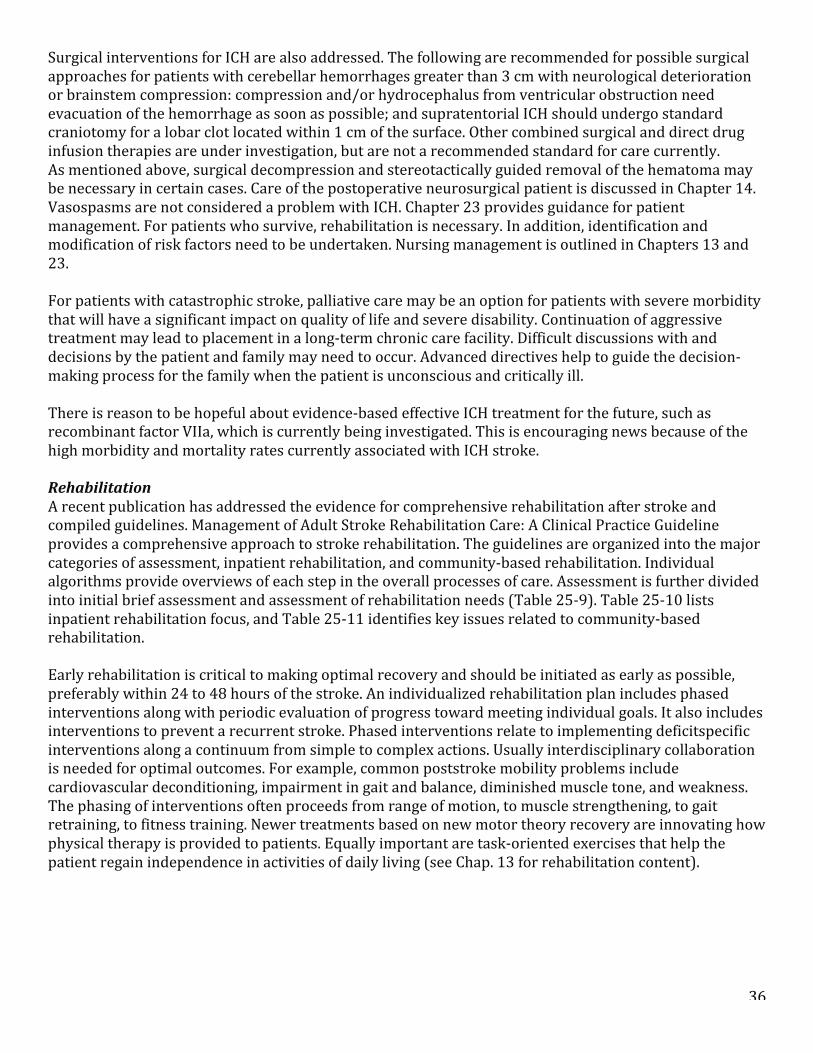
36
Surgical interventions for ICH are also addressed. The following are recommended for possible surgical approaches for patients with cerebellar hemorrhages greater than 3 cm with neurological deterioration or brainstem compression: compression and/or hydrocephalus from ventricular obstruction need evacuation of the hemorrhage as soon as possible; and supratentorial ICH should undergo standard craniotomy for a lobar clot located within 1 cm of the surface. Other combined surgical and direct drug infusion therapies are under investigation, but are not a recommended standard for care currently. As mentioned above, surgical decompression and stereotactically guided removal of the hematoma may be necessary in certain cases. Care of the postoperative neurosurgical patient is discussed in Chapter 14. Vasospasms are not considered a problem with ICH. Chapter 23 provides guidance for patient management. For patients who survive, rehabilitation is necessary. In addition, identification and modification of risk factors need to be undertaken. Nursing management is outlined in Chapters 13 and 23. For patients with catastrophic stroke, palliative care may be an option for patients with severe morbidity that will have a significant impact on quality of life and severe disability. Continuation of aggressive treatment may lead to placement in a long-‐term chronic care facility. Difficult discussions with and decisions by the patient and family may need to occur. Advanced directives help to guide the decision-‐making process for the family when the patient is unconscious and critically ill. There is reason to be hopeful about evidence-‐based effective ICH treatment for the future, such as recombinant factor VIIa, which is currently being investigated. This is encouraging news because of the high morbidity and mortality rates currently associated with ICH stroke. Rehabilitation A recent publication has addressed the evidence for comprehensive rehabilitation after stroke and compiled guidelines. Management of Adult Stroke Rehabilitation Care: A Clinical Practice Guideline provides a comprehensive approach to stroke rehabilitation. The guidelines are organized into the major categories of assessment, inpatient rehabilitation, and community-‐based rehabilitation. Individual algorithms provide overviews of each step in the overall processes of care. Assessment is further divided into initial brief assessment and assessment of rehabilitation needs (Table 25-‐9). Table 25-‐10 lists inpatient rehabilitation focus, and Table 25-‐11 identifies key issues related to community-‐based rehabilitation. Early rehabilitation is critical to making optimal recovery and should be initiated as early as possible, preferably within 24 to 48 hours of the stroke. An individualized rehabilitation plan includes phased interventions along with periodic evaluation of progress toward meeting individual goals. It also includes interventions to prevent a recurrent stroke. Phased interventions relate to implementing deficitspecific interventions along a continuum from simple to complex actions. Usually interdisciplinary collaboration is needed for optimal outcomes. For example, common poststroke mobility problems include cardiovascular deconditioning, impairment in gait and balance, diminished muscle tone, and weakness. The phasing of interventions often proceeds from range of motion, to muscle strengthening, to gait retraining, to fitness training. Newer treatments based on new motor theory recovery are innovating how physical therapy is provided to patients. Equally important are task-‐oriented exercises that help the patient regain independence in activities of daily living (see Chap. 13 for rehabilitation content).
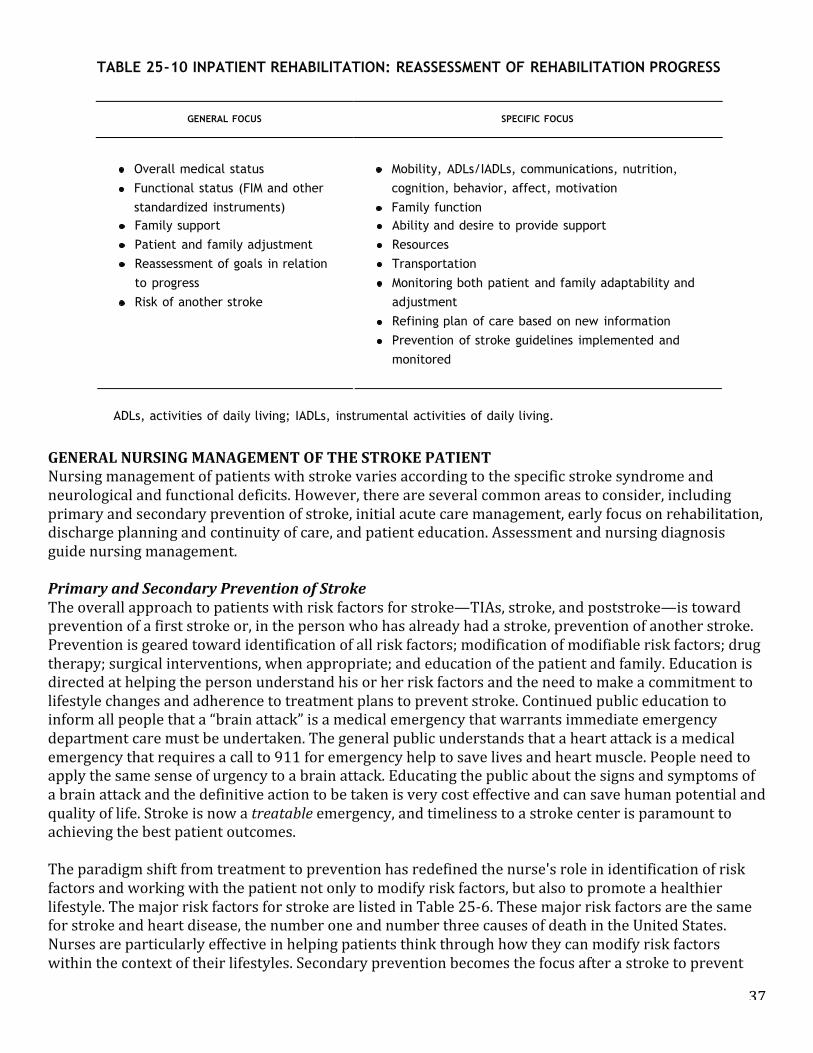
37
GENERAL NURSING MANAGEMENT OF THE STROKE PATIENT Nursing management of patients with stroke varies according to the specific stroke syndrome and neurological and functional deficits. However, there are several common areas to consider, including primary and secondary prevention of stroke, initial acute care management, early focus on rehabilitation, discharge planning and continuity of care, and patient education. Assessment and nursing diagnosis guide nursing management. Primary and Secondary Prevention of Stroke The overall approach to patients with risk factors for stroke—TIAs, stroke, and poststroke—is toward prevention of a first stroke or, in the person who has already had a stroke, prevention of another stroke. Prevention is geared toward identification of all risk factors; modification of modifiable risk factors; drug therapy; surgical interventions, when appropriate; and education of the patient and family. Education is directed at helping the person understand his or her risk factors and the need to make a commitment to lifestyle changes and adherence to treatment plans to prevent stroke. Continued public education to inform all people that a “brain attack” is a medical emergency that warrants immediate emergency department care must be undertaken. The general public understands that a heart attack is a medical emergency that requires a call to 911 for emergency help to save lives and heart muscle. People need to apply the same sense of urgency to a brain attack. Educating the public about the signs and symptoms of a brain attack and the definitive action to be taken is very cost effective and can save human potential and quality of life. Stroke is now a treatable emergency, and timeliness to a stroke center is paramount to achieving the best patient outcomes. The paradigm shift from treatment to prevention has redefined the nurse's role in identification of risk factors and working with the patient not only to modify risk factors, but also to promote a healthier lifestyle. The major risk factors for stroke are listed in Table 25-‐6. These major risk factors are the same for stroke and heart disease, the number one and number three causes of death in the United States. Nurses are particularly effective in helping patients think through how they can modify risk factors within the context of their lifestyles. Secondary prevention becomes the focus after a stroke to prevent
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 46 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.610
and family may need to occur. Advanced directives help to guide the decision-making process for the familywhen the patient is unconscious and critically ill.
CLINICAL PEARLS:Palliative care is a legitimate treatment option for patients with severe stroke with a poorprognosis.
There is reason to be hopeful about evidence-based effective ICH treatment for the future, such as recombinantfactor VIIa, which is currently being investigated. This is encouraging news because of the high morbidity and
mortality rates currently associated with ICH stroke.46
CLINICAL PEARLS:Repeated vomiting after an acute mental status decline is highly indicative of intracranialhemorrhage; be prepared for deterioration, possible intubation, or surgery.
Rehabilitation
A recent publication has addressed the evidence for comprehensive rehabilitation after stroke and compiledguidelines. Management of Adult Stroke Rehabilitation Care: A Clinical Practice Guideline provides a
comprehensive approach to stroke rehabilitation.47 The guidelines are organized into the major categories ofassessment, inpatient rehabilitation, and community-based rehabilitation. Individual algorithms provideoverviews of each step in the overall processes of care. Assessment is further divided into initial briefassessment and assessment of rehabilitation needs (Table 25-9). Table 25-10 lists inpatient rehabilitation focus,and Table 25-11 identifies key issues related to community-based rehabilitation.
Early rehabilitation is critical to making optimal recovery and should be initiated as early as possible, preferablywithin 24 to 48 hours of the stroke. An individualized rehabilitation plan includes phased interventions alongwith periodic evaluation of progress toward meeting individual goals. It also includes interventions to prevent arecurrent stroke. Phased interventions relate to implementing deficitspecific interventions along a continuumfrom simple to complex actions. Usually interdisciplinary collaboration is needed for optimal outcomes. Forexample, common poststroke mobility problems include cardiovascular deconditioning, impairment in gait andbalance, diminished muscle tone, and weakness. The phasing of interventions often proceeds from range ofmotion, to muscle strengthening, to gait retraining, to fitness training. Newer treatments based on new motortheory recovery are innovating how physical therapy is provided to patients. Equally important are task-orientedexercises that help the patient regain independence in activities of daily living (see Chap. 13 for rehabilitationcontent).
TABLE 25-10 INPATIENT REHABILITATION: REASSESSMENT OF REHABILITATION PROGRESS
GENERAL FOCUS SPECIFIC FOCUS
Overall medical statusFunctional status (FIM and otherstandardized instruments)
Mobility, ADLs/IADLs, communications, nutrition,cognition, behavior, affect, motivationFamily function
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 47 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
Family support
Patient and family adjustment
Reassessment of goals in relation
to progress
Risk of another stroke
Ability and desire to provide support
Resources
Transportation
Monitoring both patient and family adaptability and
adjustment
Refining plan of care based on new information
Prevention of stroke guidelines implemented and
monitored
ADLs, activities of daily living; IADLs, instrumental activities of daily living.
GENERAL NURSING MANAGEMENT OF THE STROKE PATIENTNursing management of patients with stroke varies according to the specific stroke syndrome and neurological
and functional deficits. However, there are several common areas to consider, including primary and secondary
prevention of stroke, initial acute care management, early focus on rehabilitation, discharge planning and
continuity of care, and patient education. Assessment and nursing diagnosis guide nursing management.
Primary and Secondary Prevention of Stroke
The overall approach to patients with risk factors for stroke—TIAs, stroke, and poststroke—is toward prevention
of a first stroke or, in the person who has already had a stroke, prevention of another stroke. Prevention is
geared toward identification of all risk factors; modification of modifiable risk factors; drug therapy; surgical
interventions, when appropriate; and education of the patient and family. Education is directed at helping the
person understand his or her risk factors and the need to make a commitment to lifestyle changes and
adherence to treatment plans to prevent stroke. Continued public education to inform all people that a “brain
attack” is a medical emergency that warrants immediate emergency department care must be undertaken. The
general public understands that a heart attack is a medical emergency that requires a call to 911 for emergency
help to save lives and heart muscle. People need to apply the same sense of urgency to a brain attack.
Educating the public about the signs and symptoms of a brain attack and the definitive action to be taken is
very cost effective and can save human potential and quality of life. Stroke is now a treatable emergency, and
timeliness to a stroke center is paramount to achieving the best patient outcomes.
TABLE 25-11 COMMUNITY-BASED REHABILITATION AND INTEGRATION
ASSESSMENT OF PATIENT READINESS ANDDISCHARGE ENVIRONMENT RELATED ACTIVITIES
Physiologically stabilized
Functional deficits identified and plan of care in place
Postcare options discussed based on resources and health
care plan
Home environment assessed for needed alterations to
All health problems
addressed and patient
knows plan of care
Interventions
implemented and
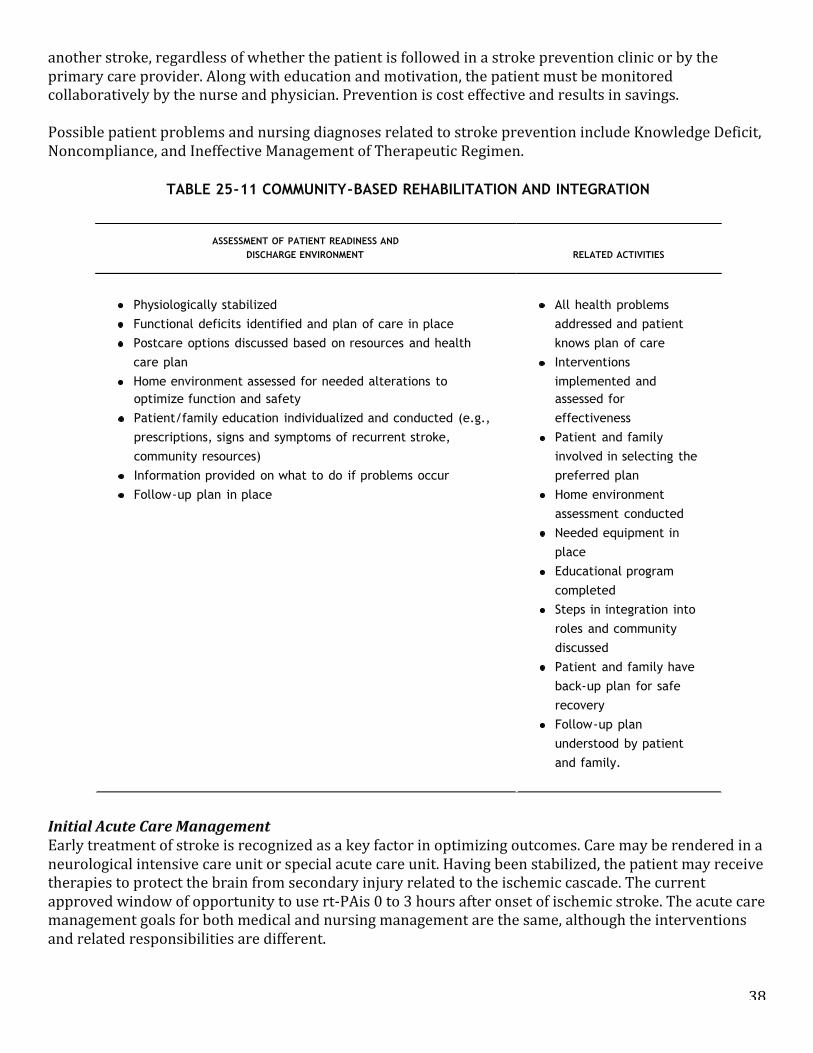
38
another stroke, regardless of whether the patient is followed in a stroke prevention clinic or by the primary care provider. Along with education and motivation, the patient must be monitored collaboratively by the nurse and physician. Prevention is cost effective and results in savings. Possible patient problems and nursing diagnoses related to stroke prevention include Knowledge Deficit, Noncompliance, and Ineffective Management of Therapeutic Regimen.
Initial Acute Care Management Early treatment of stroke is recognized as a key factor in optimizing outcomes. Care may be rendered in a neurological intensive care unit or special acute care unit. Having been stabilized, the patient may receive therapies to protect the brain from secondary injury related to the ischemic cascade. The current approved window of opportunity to use rt-‐PAis 0 to 3 hours after onset of ischemic stroke. The acute care management goals for both medical and nursing management are the same, although the interventions and related responsibilities are different.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 47 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
Family support
Patient and family adjustment
Reassessment of goals in relation
to progress
Risk of another stroke
Ability and desire to provide support
Resources
Transportation
Monitoring both patient and family adaptability and
adjustment
Refining plan of care based on new information
Prevention of stroke guidelines implemented and
monitored
ADLs, activities of daily living; IADLs, instrumental activities of daily living.
GENERAL NURSING MANAGEMENT OF THE STROKE PATIENTNursing management of patients with stroke varies according to the specific stroke syndrome and neurological
and functional deficits. However, there are several common areas to consider, including primary and secondary
prevention of stroke, initial acute care management, early focus on rehabilitation, discharge planning and
continuity of care, and patient education. Assessment and nursing diagnosis guide nursing management.
Primary and Secondary Prevention of Stroke
The overall approach to patients with risk factors for stroke—TIAs, stroke, and poststroke—is toward prevention
of a first stroke or, in the person who has already had a stroke, prevention of another stroke. Prevention is
geared toward identification of all risk factors; modification of modifiable risk factors; drug therapy; surgical
interventions, when appropriate; and education of the patient and family. Education is directed at helping the
person understand his or her risk factors and the need to make a commitment to lifestyle changes and
adherence to treatment plans to prevent stroke. Continued public education to inform all people that a “brain
attack” is a medical emergency that warrants immediate emergency department care must be undertaken. The
general public understands that a heart attack is a medical emergency that requires a call to 911 for emergency
help to save lives and heart muscle. People need to apply the same sense of urgency to a brain attack.
Educating the public about the signs and symptoms of a brain attack and the definitive action to be taken is
very cost effective and can save human potential and quality of life. Stroke is now a treatable emergency, and
timeliness to a stroke center is paramount to achieving the best patient outcomes.
TABLE 25-11 COMMUNITY-BASED REHABILITATION AND INTEGRATION
ASSESSMENT OF PATIENT READINESS ANDDISCHARGE ENVIRONMENT RELATED ACTIVITIES
Physiologically stabilized
Functional deficits identified and plan of care in place
Postcare options discussed based on resources and health
care plan
Home environment assessed for needed alterations to
All health problems
addressed and patient
knows plan of care
Interventions
implemented and
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 48 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.611
optimize function and safety
Patient/family education individualized and conducted (e.g.,
prescriptions, signs and symptoms of recurrent stroke,
community resources)
Information provided on what to do if problems occur
Follow-up plan in place
assessed for
effectiveness
Patient and family
involved in selecting the
preferred plan
Home environment
assessment conducted
Needed equipment in
place
Educational program
completed
Steps in integration into
roles and community
discussed
Patient and family have
back-up plan for safe
recovery
Follow-up plan
understood by patient
and family.
The paradigm shift from treatment to prevention has redefined the nurse's role in identification of risk factors
and working with the patient not only to modify risk factors, but also to promote a healthier lifestyle. The
major risk factors for stroke are listed in Table 25-6. These major risk factors are the same for stroke and heart
disease, the number one and number three causes of death in the United States. Nurses are particularly
effective in helping patients think through how they can modify risk factors within the context of their lifestyles.
Secondary prevention becomes the focus after a stroke to prevent another stroke, regardless of whether the
patient is followed in a stroke prevention clinic or by the primary care provider. Along with education and
motivation, the patient must be monitored collaboratively by the nurse and physician. Prevention is cost
effective and results in savings.
Possible patient problems and nursing diagnoses related to stroke prevention include Knowledge Deficit,
Noncompliance, and Ineffective Management of Therapeutic Regimen.
Initial Acute Care ManagementEarly treatment of stroke is recognized as a key factor in optimizing outcomes. Care may be rendered in a
neurological intensive care unit or special acute care unit. Having been stabilized, the patient may receive
therapies to protect the brain from secondary injury related to the ischemic cascade. The current approved
window of opportunity to use rt-PAis 0 to 3 hours after onset of ischemic stroke. The acute care management
goals for both medical and nursing management are the same, although the interventions and related
responsibilities are different.
CLINICAL PEARLS:A diagnosis of stroke does not require a critical care designation. Only stroke patients withimmediate or impending critical care needs require intensive care monitoring in a critical care
39
• Patient safety is an additional goal for which nurses assume a major responsibility. These goals include:
• Maintenance of an adequate airway and oxygenation support to prevent hypoxia
• Control of fever
• Ongoing assessment for cardiac arrhythmia and cardiac ischemia/infarction
• Blood pressure management to maximize cerebral perfusion
• Glycemia management to maintain glucose less than 150 mg/dL to decrease risk of cerebral edema
and hemorrhage
• Prevention of complications such as aspiration pneumonia, nosocomial infections, and device-‐related infections (urinary tract infections, intravascular line infections)
• Prevention of deep venous thrombosis and pulmonary embolism
• Fall prevention and patient safety
Many patients will be managed in a stroke unit for close monitoring by nurses with expertise with the stroke population. Some critically ill and unstable patients who require vasoactive intravenous drug therapy or who are on a ventilator will require admission to an intensive care unit. Regardless of the setting, the nurse works collaboratively with the physician and other health professionals to achieve optimal outcomes. The following patient problems and nursing diagnoses are common in the acute phase of illness: Ineffective Airway Clearance; Risk of Aspiration; Impaired Swallowing; Altered Cerebral Tissue Perfusion; Risk of Infection; Ineffective Breathing Pattern; Sensory Perceptual Alterations; Impaired Physical Mobility; Nutrition Deficits; and Impaired Verbal Communication. Common collaborative problems include hypoxemia; hypoglycemia or hyperglycemia; increased intracranial pressure; paresis/paresthesia/paralysis; gastrointestinal bleeding; hypertension; reperfusion injury; electrolyte imbalances; dysrhythmias; deep vein thrombosis or pulmonary embolism; anticoagulant therapy adverse effects; and thrombolytic therapy adverse effects. Frequent neurological, cardiac, hemodynamic, and respiratory monitoring is necessary to determine early changes and the need to adjust management. Cerebral edema generally develops with all ischemic strokes within 24 hours. The larger the stroke, the more edema occurs so that cerebral edema is a major concern with a larger stroke. Severe hypertension increases the risk of hemorrhage or recurrent bleeding. Both cerebral edema and hemorrhage are associated with increased ICP. Increased ICP may result from the original hemorrhage, but hemorrhage can also occur 2 to 4 days after massive infarction of the cerebral hemisphere. The development of edema is heralded by a gradual deterioration in neurological signs, such as drowsiness and sluggish pupillary response. Increased ICP is treated with supportive therapy and depends on the extent of the deficits and complications present. Frequent serial neurological assessment is important in monitoring the patient for onset of complications.
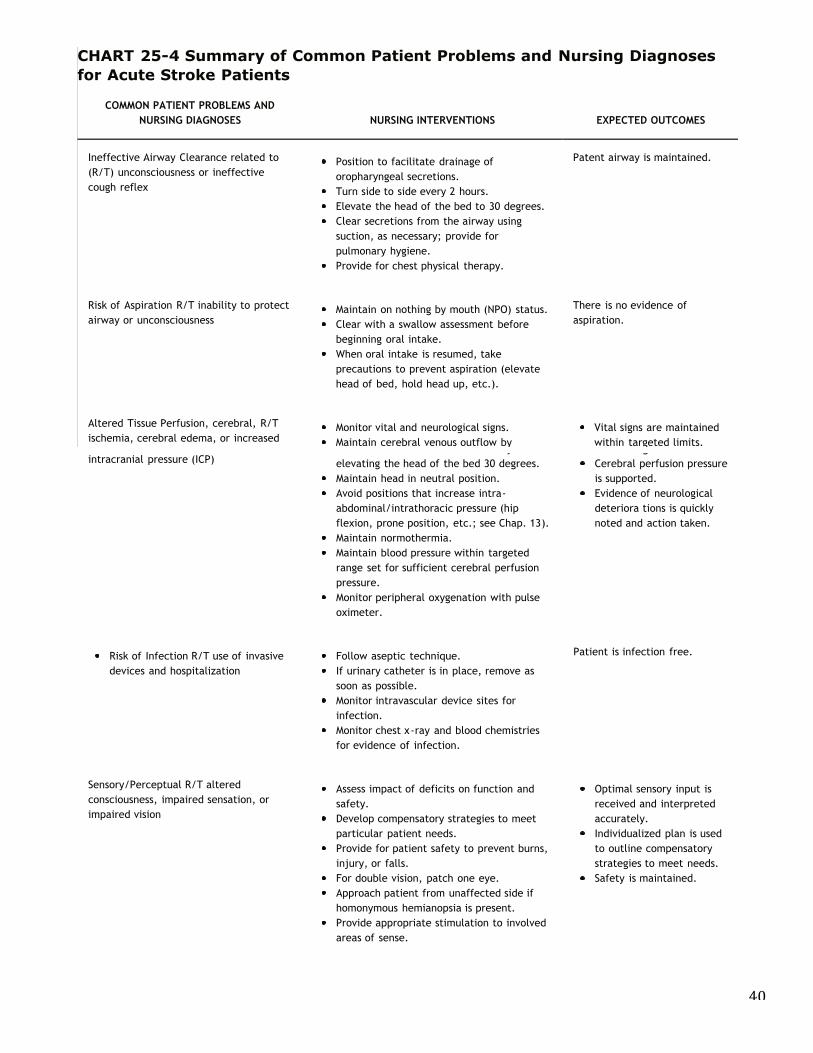
40
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 50 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.612
a larger stroke. Severe hypertension increases the risk of hemorrhage or recurrent bleeding. Both cerebral
edema and hemorrhage are associated with increased ICP. Increased ICP may result from the original
hemorrhage, but hemorrhage can also occur 2 to 4 days after massive infarction of the cerebral hemisphere. The
development of edema is heralded by a gradual deterioration in neurological signs, such as drowsiness and
sluggish pupillary response. Increased ICP is treated with supportive therapy and depends on the extent of the
deficits and complications present. Frequent serial neurological assessment is important in monitoring the
patient for onset of complications.
CLINICAL PEARLS:Patients with an NIHSS score of less than 7 have a good chance for complete or nearcomplete recovery. Stroke scores that range from 8 to 17 are highly indicative of the needfor some type of long-term assistance. Stroke scores greater than 18 are highly correlatedwith significant morbidity and mortality.
Careful cardiac monitoring is necessary to determine the need to adjust therapy to maximize hemodynamic
parameters and to identify cardiac arrhythmias and myocardial infarction. The level of the head of the bed will
depend on stability of hemodynamics and ICP, but it is generally elevated to 30 degrees. Respiratory parameters
are also monitored closely for evidence of secondary problems, such as
atelectasis and pneumonia. For patients on ventilatory support, weaning should begin as soon as possible. The
awake patient is maintained on NPO status until a swallowing study has been conducted and problems of
aspiration have been ruled out. In many facilities, an initial swallow screening is conducted in both the ED and
stroke center with follow-up with a speech evaluation. Although many screening tools are available, a
frequently used assessment tool is the Massey Screening Tool.32 This is one of the stroke performance measures
that may be difficult to ensure because patients in the ED are often given oral medications prior to the swallow
screening.
CHART 25-4 Summary of Common Patient Problems and Nursing Diagnosesfor Acute Stroke Patients
COMMON PATIENT PROBLEMS AND
NURSING DIAGNOSES NURSING INTERVENTIONS EXPECTED OUTCOMES
Ineffective Airway Clearance related to
(R/T) unconsciousness or ineffective
cough reflex
Position to facilitate drainage of
oropharyngeal secretions.
Turn side to side every 2 hours.
Elevate the head of the bed to 30 degrees.
Clear secretions from the airway using
suction, as necessary; provide for
pulmonary hygiene.
Provide for chest physical therapy.
Patent airway is maintained.
Risk of Aspiration R/T inability to protect
airway or unconsciousnessMaintain on nothing by mouth (NPO) status.
Clear with a swallow assessment before
beginning oral intake.
When oral intake is resumed, take
precautions to prevent aspiration (elevate
head of bed, hold head up, etc.).
There is no evidence of
aspiration.
Altered Tissue Perfusion, cerebral, R/T
ischemia, cerebral edema, or increasedMonitor vital and neurological signs.
Maintain cerebral venous outflow by
Vital signs are maintained
within targeted limits.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 51 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
intracranial pressure (ICP)Maintain cerebral venous outflow byelevating the head of the bed 30 degrees.Maintain head in neutral position.Avoid positions that increase intra-abdominal/intrathoracic pressure (hipflexion, prone position, etc.; see Chap. 13).Maintain normothermia.Maintain blood pressure within targetedrange set for sufficient cerebral perfusionpressure.Monitor peripheral oxygenation with pulseoximeter.
within targeted limits.Cerebral perfusion pressureis supported.Evidence of neurologicaldeteriora tions is quicklynoted and action taken.
Risk of Infection R/T use of invasivedevices and hospitalization
Follow aseptic technique.If urinary catheter is in place, remove assoon as possible.Monitor intravascular device sites forinfection.Monitor chest x-ray and blood chemistriesfor evidence of infection.
Patient is infection free.
Sensory/Perceptual R/T alteredconsciousness, impaired sensation, orimpaired vision
Assess impact of deficits on function andsafety.Develop compensatory strategies to meetparticular patient needs.Provide for patient safety to prevent burns,injury, or falls.For double vision, patch one eye.Approach patient from unaffected side ifhomonymous hemianopsia is present.Provide appropriate stimulation to involvedareas of sense.
Optimal sensory input isreceived and interpretedaccurately.Individualized plan is usedto outline compensatorystrategies to meet needs.Safety is maintained.
Impaired Verbal Communication R/Tcerebral injury/altered level ofconsciousness
Assess type of communication deficitpresent.• Develop and establish appropriatealternative methods for communication.
Alternative communicationmethod is developed basedon type of deficit.The patient's attempts tocommunicate aresupported.
Impaired Physical Mobility R/Tneurological deficits
Assess type and degree of impairment.Provide slings, braces, support shoes, etc.,as necessary.Support alternative methods of mobility.Collaborate with physical therapist tosupport exercise and mobility.
Type and impact onfunction are established.Safe compensatorymethods are established formotor function.
High risk for deep venous thrombosis(DVT) or pulmonary embolism (PE)
For bedridden patients, apply elasticstockings and compression boots.SQ heparin or low-molecular-weightheparins are alternatives; be sure someform of prophylaxis is provided.Monitor for signs and symptoms of DVT andPE.
Adequate DVT prophylaxisis provided.Patient is monitored forsigns and symptoms of DVTand PE.
Nutrition Deficit R/T swallowing deficits,NPO status, or unconsciousness
Order nutritional consult. Nutritional consult is
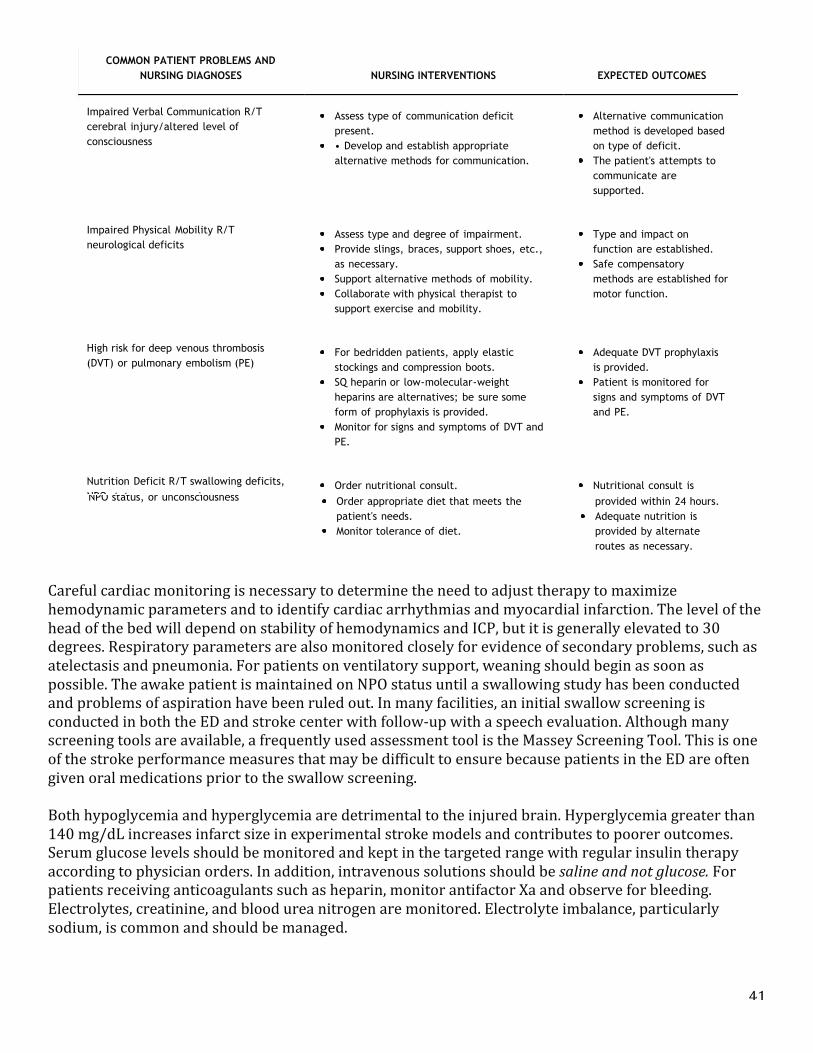
41
Careful cardiac monitoring is necessary to determine the need to adjust therapy to maximize hemodynamic parameters and to identify cardiac arrhythmias and myocardial infarction. The level of the head of the bed will depend on stability of hemodynamics and ICP, but it is generally elevated to 30 degrees. Respiratory parameters are also monitored closely for evidence of secondary problems, such as atelectasis and pneumonia. For patients on ventilatory support, weaning should begin as soon as possible. The awake patient is maintained on NPO status until a swallowing study has been conducted and problems of aspiration have been ruled out. In many facilities, an initial swallow screening is conducted in both the ED and stroke center with follow-‐up with a speech evaluation. Although many screening tools are available, a frequently used assessment tool is the Massey Screening Tool. This is one of the stroke performance measures that may be difficult to ensure because patients in the ED are often given oral medications prior to the swallow screening. Both hypoglycemia and hyperglycemia are detrimental to the injured brain. Hyperglycemia greater than 140 mg/dL increases infarct size in experimental stroke models and contributes to poorer outcomes. Serum glucose levels should be monitored and kept in the targeted range with regular insulin therapy according to physician orders. In addition, intravenous solutions should be saline and not glucose. For patients receiving anticoagulants such as heparin, monitor antifactor Xa and observe for bleeding. Electrolytes, creatinine, and blood urea nitrogen are monitored. Electrolyte imbalance, particularly sodium, is common and should be managed.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 50 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.612
a larger stroke. Severe hypertension increases the risk of hemorrhage or recurrent bleeding. Both cerebral
edema and hemorrhage are associated with increased ICP. Increased ICP may result from the original
hemorrhage, but hemorrhage can also occur 2 to 4 days after massive infarction of the cerebral hemisphere. The
development of edema is heralded by a gradual deterioration in neurological signs, such as drowsiness and
sluggish pupillary response. Increased ICP is treated with supportive therapy and depends on the extent of the
deficits and complications present. Frequent serial neurological assessment is important in monitoring the
patient for onset of complications.
CLINICAL PEARLS:Patients with an NIHSS score of less than 7 have a good chance for complete or nearcomplete recovery. Stroke scores that range from 8 to 17 are highly indicative of the needfor some type of long-term assistance. Stroke scores greater than 18 are highly correlatedwith significant morbidity and mortality.
Careful cardiac monitoring is necessary to determine the need to adjust therapy to maximize hemodynamic
parameters and to identify cardiac arrhythmias and myocardial infarction. The level of the head of the bed will
depend on stability of hemodynamics and ICP, but it is generally elevated to 30 degrees. Respiratory parameters
are also monitored closely for evidence of secondary problems, such as
atelectasis and pneumonia. For patients on ventilatory support, weaning should begin as soon as possible. The
awake patient is maintained on NPO status until a swallowing study has been conducted and problems of
aspiration have been ruled out. In many facilities, an initial swallow screening is conducted in both the ED and
stroke center with follow-up with a speech evaluation. Although many screening tools are available, a
frequently used assessment tool is the Massey Screening Tool.32 This is one of the stroke performance measures
that may be difficult to ensure because patients in the ED are often given oral medications prior to the swallow
screening.
CHART 25-4 Summary of Common Patient Problems and Nursing Diagnosesfor Acute Stroke Patients
COMMON PATIENT PROBLEMS AND
NURSING DIAGNOSES NURSING INTERVENTIONS EXPECTED OUTCOMES
Ineffective Airway Clearance related to
(R/T) unconsciousness or ineffective
cough reflex
Position to facilitate drainage of
oropharyngeal secretions.
Turn side to side every 2 hours.
Elevate the head of the bed to 30 degrees.
Clear secretions from the airway using
suction, as necessary; provide for
pulmonary hygiene.
Provide for chest physical therapy.
Patent airway is maintained.
Risk of Aspiration R/T inability to protect
airway or unconsciousnessMaintain on nothing by mouth (NPO) status.
Clear with a swallow assessment before
beginning oral intake.
When oral intake is resumed, take
precautions to prevent aspiration (elevate
head of bed, hold head up, etc.).
There is no evidence of
aspiration.
Altered Tissue Perfusion, cerebral, R/T
ischemia, cerebral edema, or increasedMonitor vital and neurological signs.
Maintain cerebral venous outflow by
Vital signs are maintained
within targeted limits.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 51 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
intracranial pressure (ICP)Maintain cerebral venous outflow byelevating the head of the bed 30 degrees.Maintain head in neutral position.Avoid positions that increase intra-abdominal/intrathoracic pressure (hipflexion, prone position, etc.; see Chap. 13).Maintain normothermia.Maintain blood pressure within targetedrange set for sufficient cerebral perfusionpressure.Monitor peripheral oxygenation with pulseoximeter.
within targeted limits.Cerebral perfusion pressureis supported.Evidence of neurologicaldeteriora tions is quicklynoted and action taken.
Risk of Infection R/T use of invasivedevices and hospitalization
Follow aseptic technique.If urinary catheter is in place, remove assoon as possible.Monitor intravascular device sites forinfection.Monitor chest x-ray and blood chemistriesfor evidence of infection.
Patient is infection free.
Sensory/Perceptual R/T alteredconsciousness, impaired sensation, orimpaired vision
Assess impact of deficits on function andsafety.Develop compensatory strategies to meetparticular patient needs.Provide for patient safety to prevent burns,injury, or falls.For double vision, patch one eye.Approach patient from unaffected side ifhomonymous hemianopsia is present.Provide appropriate stimulation to involvedareas of sense.
Optimal sensory input isreceived and interpretedaccurately.Individualized plan is usedto outline compensatorystrategies to meet needs.Safety is maintained.
Impaired Verbal Communication R/Tcerebral injury/altered level ofconsciousness
Assess type of communication deficitpresent.• Develop and establish appropriatealternative methods for communication.
Alternative communicationmethod is developed basedon type of deficit.The patient's attempts tocommunicate aresupported.
Impaired Physical Mobility R/Tneurological deficits
Assess type and degree of impairment.Provide slings, braces, support shoes, etc.,as necessary.Support alternative methods of mobility.Collaborate with physical therapist tosupport exercise and mobility.
Type and impact onfunction are established.Safe compensatorymethods are established formotor function.
High risk for deep venous thrombosis(DVT) or pulmonary embolism (PE)
For bedridden patients, apply elasticstockings and compression boots.SQ heparin or low-molecular-weightheparins are alternatives; be sure someform of prophylaxis is provided.Monitor for signs and symptoms of DVT andPE.
Adequate DVT prophylaxisis provided.Patient is monitored forsigns and symptoms of DVTand PE.
Nutrition Deficit R/T swallowing deficits,NPO status, or unconsciousness
Order nutritional consult. Nutritional consult is
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 52 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.613
P.614
NPO status, or unconsciousness Order appropriate diet that meets thepatient's needs.Monitor tolerance of diet.
provided within 24 hours.Adequate nutrition isprovided by alternateroutes as necessary.
Both hypoglycemia and hyperglycemia are detrimental to the injured brain. Hyperglycemia greater than 140mg/dL increases infarct size in experimental stroke models and contributes to poorer outcomes. Serum glucoselevels should be monitored and kept in the targeted range with regular insulin therapy according to physicianorders. In addition, intravenous solutions should be saline and not glucose. For patients receiving anticoagulantssuch as heparin, monitor antifactor Xa and observe for bleeding. Electrolytes, creatinine, and blood ureanitrogen are monitored. Electrolyte imbalance, particularly sodium, is common and should be managed.
Patient safety is always a primary priority in patient care. With the multiple functional deficits common withstroke, fall prevention becomes a major focus of care. There are a number of assessment tools to assist inidentifying patients at high risk for falls. However, the correlation of fall prediction and actual falls is notalways clear. Stroke patients are all high risk for falls, and a comprehensive fall prevention program must beused.
For details about the key points in acute care nursing management of stroke patients after treatment withspecial interventions, see Chart 25-3. Chart 25-4 summarizes the common patient problems and nursingdiagnoses associated with stroke. Chart 25-5 summarizes the common deficits and emotional reactions relatedto stroke. See also Chapter 15 for management of the unconscious patient and Chapter 13 for ICP management.After the patient's condition has stabilized, nursing management is refocused on rehabilitation and prevention ofanother stroke (Chart 25-6).
Early Focus on Rehabilitation
Rehabilitation begins as soon as the patient is stabilized. The nurse collaborates with other health careprofessionals to develop a plan of care. The case manager is an integral part of the interdisciplinary team whocan facilitate access to rehabilitation resources and community-based rehabilitation services. Nursingresponsibilities in the rehabilitation process are outlined in Chart 25-6. See Chapter 11 for information aboutrehabilitation.
The following patient problems and nursing diagnoses are common in stroke patients and are related to theneed for early rehabilitation: Self-Care Deficits; Sensory Perceptual Alterations; Impaired Verbal Communication;Impaired Physical Mobility; Altered Urinary Elimination; Disuse Syndrome; Altered Thought Processes; ImpairedAdjustment; Altered Role Performance; and Unilateral Neglect.
Discharge Planning and Continuity of Care
Discharge planning is taken into account early in the rehabilitative program. The plans for discharge are madewith the assistance of the case manager, who assists with continuity and facilitates access to the next level ofcare, whether rehabilitation or home care. The patient and family should be made aware of communityresources. A critical point in discharge planning is to be sure that the patient has an appointment for follow-upso that recovery, new problems, and drug therapy can be monitored (see the earlier section on rehabilitationand the Post-Stroke Rehabilitation clinical practice guidelines).
CHART 25-5 Common Deficits and Emotional Reactions to Stroke and Related
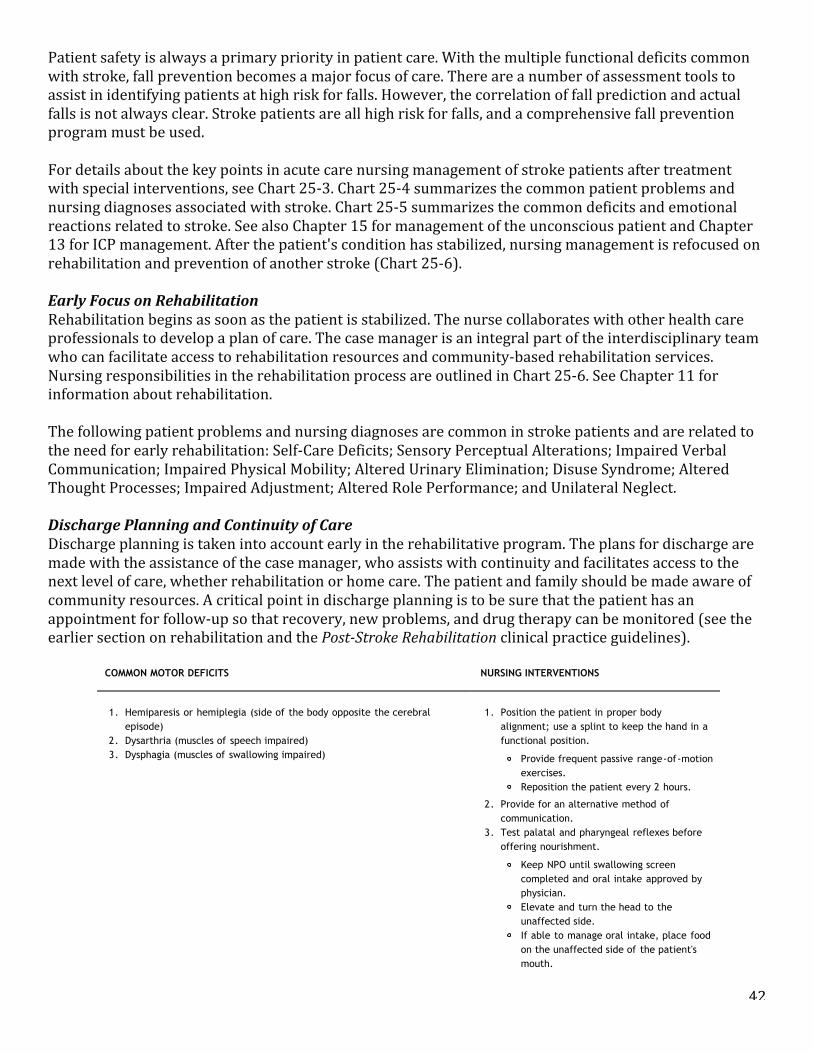
42
Patient safety is always a primary priority in patient care. With the multiple functional deficits common with stroke, fall prevention becomes a major focus of care. There are a number of assessment tools to assist in identifying patients at high risk for falls. However, the correlation of fall prediction and actual falls is not always clear. Stroke patients are all high risk for falls, and a comprehensive fall prevention program must be used. For details about the key points in acute care nursing management of stroke patients after treatment with special interventions, see Chart 25-‐3. Chart 25-‐4 summarizes the common patient problems and nursing diagnoses associated with stroke. Chart 25-‐5 summarizes the common deficits and emotional reactions related to stroke. See also Chapter 15 for management of the unconscious patient and Chapter 13 for ICP management. After the patient's condition has stabilized, nursing management is refocused on rehabilitation and prevention of another stroke (Chart 25-‐6). Early Focus on Rehabilitation Rehabilitation begins as soon as the patient is stabilized. The nurse collaborates with other health care professionals to develop a plan of care. The case manager is an integral part of the interdisciplinary team who can facilitate access to rehabilitation resources and community-‐based rehabilitation services. Nursing responsibilities in the rehabilitation process are outlined in Chart 25-‐6. See Chapter 11 for information about rehabilitation. The following patient problems and nursing diagnoses are common in stroke patients and are related to the need for early rehabilitation: Self-‐Care Deficits; Sensory Perceptual Alterations; Impaired Verbal Communication; Impaired Physical Mobility; Altered Urinary Elimination; Disuse Syndrome; Altered Thought Processes; Impaired Adjustment; Altered Role Performance; and Unilateral Neglect. Discharge Planning and Continuity of Care Discharge planning is taken into account early in the rehabilitative program. The plans for discharge are made with the assistance of the case manager, who assists with continuity and facilitates access to the next level of care, whether rehabilitation or home care. The patient and family should be made aware of community resources. A critical point in discharge planning is to be sure that the patient has an appointment for follow-‐up so that recovery, new problems, and drug therapy can be monitored (see the earlier section on rehabilitation and the Post-Stroke Rehabilitation clinical practice guidelines).
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 53 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.615
General Nursing Interventions
COMMON MOTOR DEFICITS NURSING INTERVENTIONS
1. Hemiparesis or hemiplegia (side of the body opposite the cerebralepisode)
2. Dysarthria (muscles of speech impaired)3. Dysphagia (muscles of swallowing impaired)
1. Position the patient in proper bodyalignment; use a splint to keep the hand in afunctional position.
Provide frequent passive range-of-motionexercises.Reposition the patient every 2 hours.
2. Provide for an alternative method ofcommunication.
3. Test palatal and pharyngeal reflexes beforeoffering nourishment.
Keep NPO until swallowing screencompleted and oral intake approved byphysician.Elevate and turn the head to theunaffected side.If able to manage oral intake, place foodon the unaffected side of the patient'smouth.
COMMON SENSORY DEFICITS NURSING INTERVENTIONS
1. Visual deficits (common because the visual pathways cut through muchof the cerebral hemispheres)
a. Homonymous hemianopsia (loss of vision in half of each visualfield)
b. Double vision (diplopia)c. Decreased visual acuity
2. Absent or diminished response to superficial sensation (touch, pain,pressure, heat, cold)
3. Absent or diminished response to proprioception (knowledge of positionof body parts)
4. Perceptual deficits (disturbance in perceiving and interpreting selfand/or environment)
a. Body scheme disturbance (denial of paralyzed extremities;unilateral neglect syndrome)
b. Disorientation (to time, place, and person)c. Apraxia (loss of ability to use objects correctly)d. Agnosia (inability to identify the environment by means of the
senses)e. Defects in localizing objects in space, estimating their size, and
1. Be aware that variations of visual deficitsmay exist and compensate for them.
a. Approach the patient from the unaffectedside; remind the patient to turn the headto compensate for visual deficits.
b. Apply an eye patch to the affected eye.c. Provide good light and assistance as
necessary.
2. Increase the amount of touch in administeringpatient care.
Protect the involved areas from injury.Protect the involved areas from burns.Examine the involved areas for signs ofskin irritation and injury.Provide patient with opportunity tohandle various objects of differentweight, texture, and size.If pain is present, assess its location andtype, as well as the duration of the pain.
3. Teach patient to check the position of bodyparts visually.
4. Compensate for patient's perceptual-sensorydeficits.
a. Protect the involved area.
Accept patient's self-perception.Position patient to face involvedarea.
b. Control amount of changes in patient'sschedule.
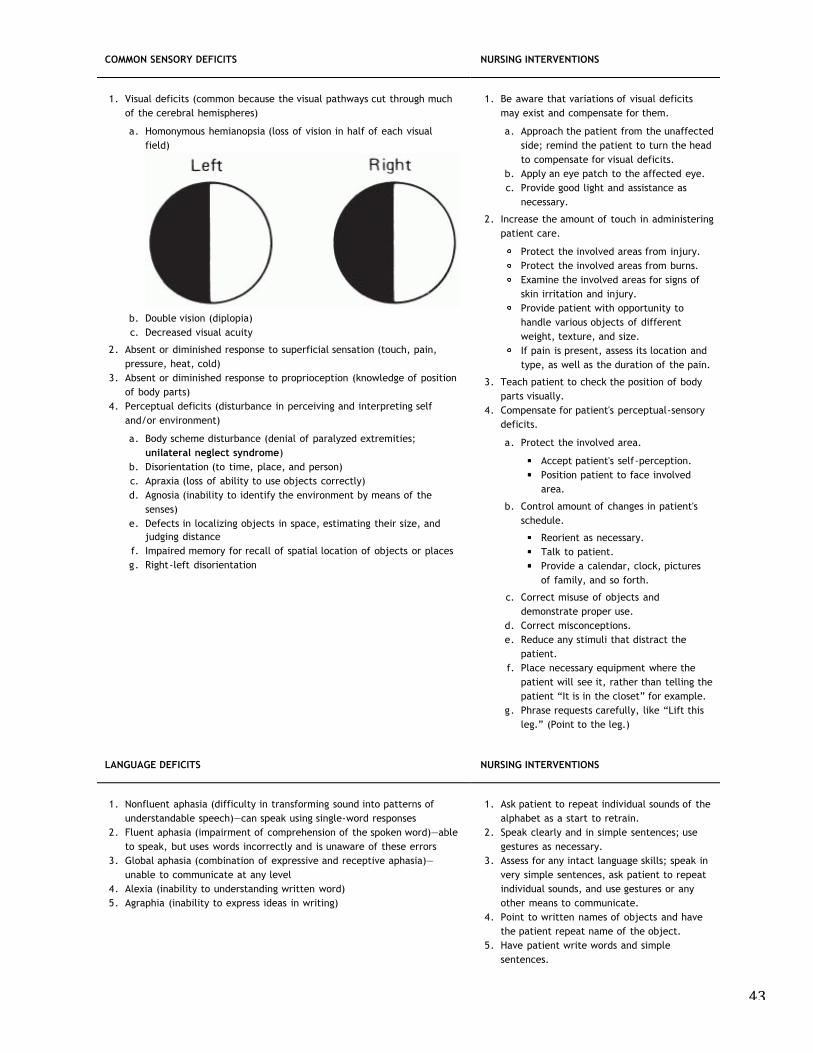
43
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 53 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.615
General Nursing Interventions
COMMON MOTOR DEFICITS NURSING INTERVENTIONS
1. Hemiparesis or hemiplegia (side of the body opposite the cerebralepisode)
2. Dysarthria (muscles of speech impaired)3. Dysphagia (muscles of swallowing impaired)
1. Position the patient in proper bodyalignment; use a splint to keep the hand in afunctional position.
Provide frequent passive range-of-motionexercises.Reposition the patient every 2 hours.
2. Provide for an alternative method ofcommunication.
3. Test palatal and pharyngeal reflexes beforeoffering nourishment.
Keep NPO until swallowing screencompleted and oral intake approved byphysician.Elevate and turn the head to theunaffected side.If able to manage oral intake, place foodon the unaffected side of the patient'smouth.
COMMON SENSORY DEFICITS NURSING INTERVENTIONS
1. Visual deficits (common because the visual pathways cut through muchof the cerebral hemispheres)
a. Homonymous hemianopsia (loss of vision in half of each visualfield)
b. Double vision (diplopia)c. Decreased visual acuity
2. Absent or diminished response to superficial sensation (touch, pain,pressure, heat, cold)
3. Absent or diminished response to proprioception (knowledge of positionof body parts)
4. Perceptual deficits (disturbance in perceiving and interpreting selfand/or environment)
a. Body scheme disturbance (denial of paralyzed extremities;unilateral neglect syndrome)
b. Disorientation (to time, place, and person)c. Apraxia (loss of ability to use objects correctly)d. Agnosia (inability to identify the environment by means of the
senses)e. Defects in localizing objects in space, estimating their size, and
1. Be aware that variations of visual deficitsmay exist and compensate for them.
a. Approach the patient from the unaffectedside; remind the patient to turn the headto compensate for visual deficits.
b. Apply an eye patch to the affected eye.c. Provide good light and assistance as
necessary.
2. Increase the amount of touch in administeringpatient care.
Protect the involved areas from injury.Protect the involved areas from burns.Examine the involved areas for signs ofskin irritation and injury.Provide patient with opportunity tohandle various objects of differentweight, texture, and size.If pain is present, assess its location andtype, as well as the duration of the pain.
3. Teach patient to check the position of bodyparts visually.
4. Compensate for patient's perceptual-sensorydeficits.
a. Protect the involved area.
Accept patient's self-perception.Position patient to face involvedarea.
b. Control amount of changes in patient'sschedule.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 54 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
judging distance
f. Impaired memory for recall of spatial location of objects or places
g. Right-left disorientation
Reorient as necessary.
Talk to patient.
Provide a calendar, clock, pictures
of family, and so forth.
c. Correct misuse of objects and
demonstrate proper use.
d. Correct misconceptions.
e. Reduce any stimuli that distract the
patient.
f. Place necessary equipment where the
patient will see it, rather than telling the
patient “It is in the closet” for example.
g. Phrase requests carefully, like “Lift this
leg.” (Point to the leg.)
LANGUAGE DEFICITS NURSING INTERVENTIONS
1. Nonfluent aphasia (difficulty in transforming sound into patterns of
understandable speech)—can speak using single-word responses
2. Fluent aphasia (impairment of comprehension of the spoken word)—able
to speak, but uses words incorrectly and is unaware of these errors
3. Global aphasia (combination of expressive and receptive aphasia)—
unable to communicate at any level
4. Alexia (inability to understanding written word)
5. Agraphia (inability to express ideas in writing)
1. Ask patient to repeat individual sounds of the
alphabet as a start to retrain.
2. Speak clearly and in simple sentences; use
gestures as necessary.
3. Assess for any intact language skills; speak in
very simple sentences, ask patient to repeat
individual sounds, and use gestures or any
other means to communicate.
4. Point to written names of objects and have
the patient repeat name of the object.
5. Have patient write words and simple
sentences.
INTELLECTUAL DEFICITS NURSING INTERVENTIONS
1. Loss of memory
2. Short attention span
3. Increased distractibility
4. Poor judgment
5. Inability to transfer learning from one situation to another
6. Inability to calculate, reason, or think abstractly
1. Provide information as necessary.
2. Divide activities into short steps.
3. Control any excessive environmental
distractions.
4. Protect patient from injury especially form
falls; institute a fall prevention program.
5. Repeat and reinforce instructions as
necessary.
6. Do not create unrealistic expectations in the
patient; accept patient as he or she is.
EMOTIONAL DEFICITS NURSING INTERVENTIONS
(Recognize that pattern is often inconsistent; patient may have good days
and bad days or even good hours and bad hours.)
1. Emotional lability (exhibits reactions easily or inappropriately)
2. Loss of self-control and social inhibitions (may speak inappropriately,
swear, expose self, or make sexual advances toward nurse)
3. Reduced tolerance for stress
4. Fear, hostility, frustration, or anger
5. Confusion and despair
6. Withdrawal, isolation
7. Depression
1. Disregard bursts of emotions; explain that
emotional lability is part of the illness.
2. Protect patient as necessary to preserve
dignity; recognize involuntary basis of
behavior and set limits; anticipate needs.
3. Control environment and maintain routines as
much as possible; remove stimuli that upset
the patient.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 54 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
judging distance
f. Impaired memory for recall of spatial location of objects or places
g. Right-left disorientation
Reorient as necessary.
Talk to patient.
Provide a calendar, clock, pictures
of family, and so forth.
c. Correct misuse of objects and
demonstrate proper use.
d. Correct misconceptions.
e. Reduce any stimuli that distract the
patient.
f. Place necessary equipment where the
patient will see it, rather than telling the
patient “It is in the closet” for example.
g. Phrase requests carefully, like “Lift this
leg.” (Point to the leg.)
LANGUAGE DEFICITS NURSING INTERVENTIONS
1. Nonfluent aphasia (difficulty in transforming sound into patterns of
understandable speech)—can speak using single-word responses
2. Fluent aphasia (impairment of comprehension of the spoken word)—able
to speak, but uses words incorrectly and is unaware of these errors
3. Global aphasia (combination of expressive and receptive aphasia)—
unable to communicate at any level
4. Alexia (inability to understanding written word)
5. Agraphia (inability to express ideas in writing)
1. Ask patient to repeat individual sounds of the
alphabet as a start to retrain.
2. Speak clearly and in simple sentences; use
gestures as necessary.
3. Assess for any intact language skills; speak in
very simple sentences, ask patient to repeat
individual sounds, and use gestures or any
other means to communicate.
4. Point to written names of objects and have
the patient repeat name of the object.
5. Have patient write words and simple
sentences.
INTELLECTUAL DEFICITS NURSING INTERVENTIONS
1. Loss of memory
2. Short attention span
3. Increased distractibility
4. Poor judgment
5. Inability to transfer learning from one situation to another
6. Inability to calculate, reason, or think abstractly
1. Provide information as necessary.
2. Divide activities into short steps.
3. Control any excessive environmental
distractions.
4. Protect patient from injury especially form
falls; institute a fall prevention program.
5. Repeat and reinforce instructions as
necessary.
6. Do not create unrealistic expectations in the
patient; accept patient as he or she is.
EMOTIONAL DEFICITS NURSING INTERVENTIONS
(Recognize that pattern is often inconsistent; patient may have good days
and bad days or even good hours and bad hours.)
1. Emotional lability (exhibits reactions easily or inappropriately)
2. Loss of self-control and social inhibitions (may speak inappropriately,
swear, expose self, or make sexual advances toward nurse)
3. Reduced tolerance for stress
4. Fear, hostility, frustration, or anger
5. Confusion and despair
6. Withdrawal, isolation
7. Depression
1. Disregard bursts of emotions; explain that
emotional lability is part of the illness.
2. Protect patient as necessary to preserve
dignity; recognize involuntary basis of
behavior and set limits; anticipate needs.
3. Control environment and maintain routines as
much as possible; remove stimuli that upset
the patient.
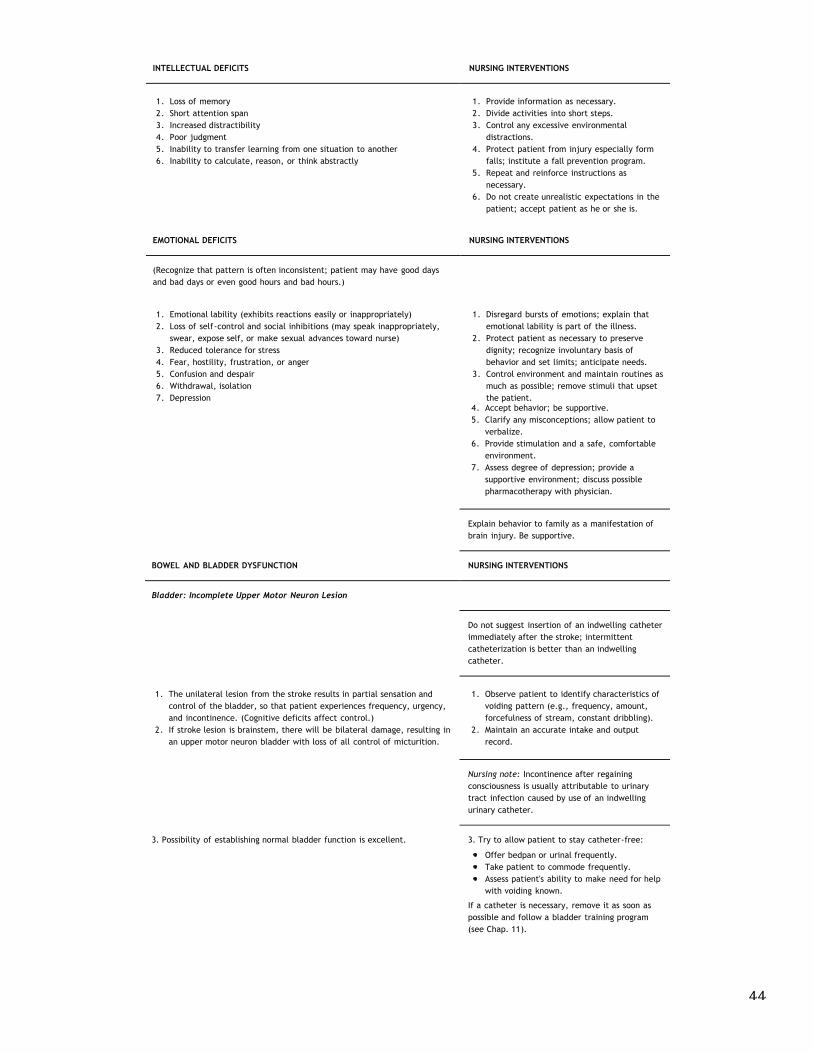
44
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 54 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
judging distance
f. Impaired memory for recall of spatial location of objects or places
g. Right-left disorientation
Reorient as necessary.
Talk to patient.
Provide a calendar, clock, pictures
of family, and so forth.
c. Correct misuse of objects and
demonstrate proper use.
d. Correct misconceptions.
e. Reduce any stimuli that distract the
patient.
f. Place necessary equipment where the
patient will see it, rather than telling the
patient “It is in the closet” for example.
g. Phrase requests carefully, like “Lift this
leg.” (Point to the leg.)
LANGUAGE DEFICITS NURSING INTERVENTIONS
1. Nonfluent aphasia (difficulty in transforming sound into patterns of
understandable speech)—can speak using single-word responses
2. Fluent aphasia (impairment of comprehension of the spoken word)—able
to speak, but uses words incorrectly and is unaware of these errors
3. Global aphasia (combination of expressive and receptive aphasia)—
unable to communicate at any level
4. Alexia (inability to understanding written word)
5. Agraphia (inability to express ideas in writing)
1. Ask patient to repeat individual sounds of the
alphabet as a start to retrain.
2. Speak clearly and in simple sentences; use
gestures as necessary.
3. Assess for any intact language skills; speak in
very simple sentences, ask patient to repeat
individual sounds, and use gestures or any
other means to communicate.
4. Point to written names of objects and have
the patient repeat name of the object.
5. Have patient write words and simple
sentences.
INTELLECTUAL DEFICITS NURSING INTERVENTIONS
1. Loss of memory
2. Short attention span
3. Increased distractibility
4. Poor judgment
5. Inability to transfer learning from one situation to another
6. Inability to calculate, reason, or think abstractly
1. Provide information as necessary.
2. Divide activities into short steps.
3. Control any excessive environmental
distractions.
4. Protect patient from injury especially form
falls; institute a fall prevention program.
5. Repeat and reinforce instructions as
necessary.
6. Do not create unrealistic expectations in the
patient; accept patient as he or she is.
EMOTIONAL DEFICITS NURSING INTERVENTIONS
(Recognize that pattern is often inconsistent; patient may have good days
and bad days or even good hours and bad hours.)
1. Emotional lability (exhibits reactions easily or inappropriately)
2. Loss of self-control and social inhibitions (may speak inappropriately,
swear, expose self, or make sexual advances toward nurse)
3. Reduced tolerance for stress
4. Fear, hostility, frustration, or anger
5. Confusion and despair
6. Withdrawal, isolation
7. Depression
1. Disregard bursts of emotions; explain that
emotional lability is part of the illness.
2. Protect patient as necessary to preserve
dignity; recognize involuntary basis of
behavior and set limits; anticipate needs.
3. Control environment and maintain routines as
much as possible; remove stimuli that upset
the patient.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 55 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.616
4. Accept behavior; be supportive.
5. Clarify any misconceptions; allow patient to
verbalize.
6. Provide stimulation and a safe, comfortable
environment.
7. Assess degree of depression; provide a
supportive environment; discuss possible
pharmacotherapy with physician.
Explain behavior to family as a manifestation of
brain injury. Be supportive.
BOWEL AND BLADDER DYSFUNCTION NURSING INTERVENTIONS
Bladder: Incomplete Upper Motor Neuron Lesion
Do not suggest insertion of an indwelling catheter
immediately after the stroke; intermittent
catheterization is better than an indwelling
catheter.
1. The unilateral lesion from the stroke results in partial sensation and
control of the bladder, so that patient experiences frequency, urgency,
and incontinence. (Cognitive deficits affect control.)
2. If stroke lesion is brainstem, there will be bilateral damage, resulting in
an upper motor neuron bladder with loss of all control of micturition.
1. Observe patient to identify characteristics of
voiding pattern (e.g., frequency, amount,
forcefulness of stream, constant dribbling).
2. Maintain an accurate intake and output
record.
Nursing note: Incontinence after regaining
consciousness is usually attributable to urinary
tract infection caused by use of an indwelling
urinary catheter.
3. Possibility of establishing normal bladder function is excellent. 3. Try to allow patient to stay catheter-free:
Offer bedpan or urinal frequently.
Take patient to commode frequently.
Assess patient's ability to make need for help
with voiding known.
If a catheter is necessary, remove it as soon as
possible and follow a bladder training program
(see Chap. 11).
Bowel
1. Altered bowel function in a stroke patient is attributable to:
Altered level of consciousness
Dehydration
Immobility
2. Constipation is the most common problem, along with potential
impaction.
1. Develop a bowel training program:
Provide high-fiber diet to stimulate
defecation (prune juice, roughage).
Initiate a suppository and laxative
regimen.
2. Institute a bowel program. Enemas are
avoided in the presence of increased
intracranial pressure.
After the patient has been discharged, integration back into community is important.
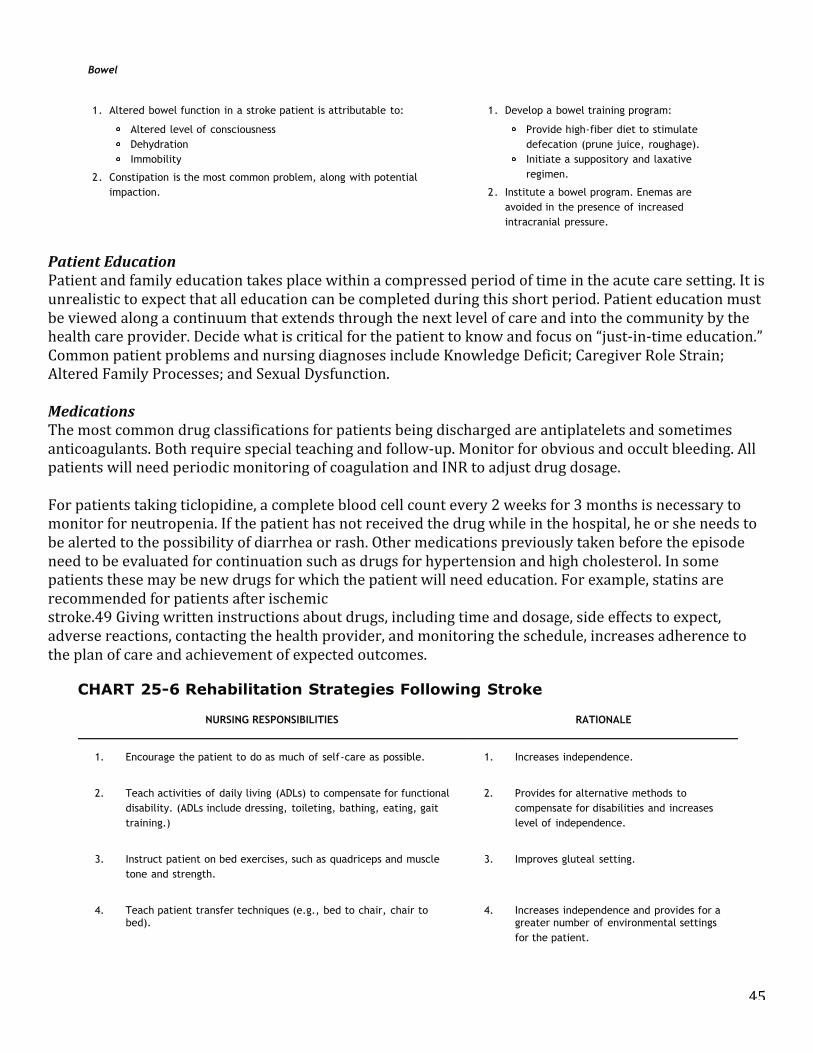
45
Patient Education Patient and family education takes place within a compressed period of time in the acute care setting. It is unrealistic to expect that all education can be completed during this short period. Patient education must be viewed along a continuum that extends through the next level of care and into the community by the health care provider. Decide what is critical for the patient to know and focus on “just-‐in-‐time education.” Common patient problems and nursing diagnoses include Knowledge Deficit; Caregiver Role Strain; Altered Family Processes; and Sexual Dysfunction. Medications The most common drug classifications for patients being discharged are antiplatelets and sometimes anticoagulants. Both require special teaching and follow-‐up. Monitor for obvious and occult bleeding. All patients will need periodic monitoring of coagulation and INR to adjust drug dosage. For patients taking ticlopidine, a complete blood cell count every 2 weeks for 3 months is necessary to monitor for neutropenia. If the patient has not received the drug while in the hospital, he or she needs to be alerted to the possibility of diarrhea or rash. Other medications previously taken before the episode need to be evaluated for continuation such as drugs for hypertension and high cholesterol. In some patients these may be new drugs for which the patient will need education. For example, statins are recommended for patients after ischemic stroke.49 Giving written instructions about drugs, including time and dosage, side effects to expect, adverse reactions, contacting the health provider, and monitoring the schedule, increases adherence to the plan of care and achievement of expected outcomes.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 55 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.616
4. Accept behavior; be supportive.
5. Clarify any misconceptions; allow patient to
verbalize.
6. Provide stimulation and a safe, comfortable
environment.
7. Assess degree of depression; provide a
supportive environment; discuss possible
pharmacotherapy with physician.
Explain behavior to family as a manifestation of
brain injury. Be supportive.
BOWEL AND BLADDER DYSFUNCTION NURSING INTERVENTIONS
Bladder: Incomplete Upper Motor Neuron Lesion
Do not suggest insertion of an indwelling catheter
immediately after the stroke; intermittent
catheterization is better than an indwelling
catheter.
1. The unilateral lesion from the stroke results in partial sensation and
control of the bladder, so that patient experiences frequency, urgency,
and incontinence. (Cognitive deficits affect control.)
2. If stroke lesion is brainstem, there will be bilateral damage, resulting in
an upper motor neuron bladder with loss of all control of micturition.
1. Observe patient to identify characteristics of
voiding pattern (e.g., frequency, amount,
forcefulness of stream, constant dribbling).
2. Maintain an accurate intake and output
record.
Nursing note: Incontinence after regaining
consciousness is usually attributable to urinary
tract infection caused by use of an indwelling
urinary catheter.
3. Possibility of establishing normal bladder function is excellent. 3. Try to allow patient to stay catheter-free:
Offer bedpan or urinal frequently.
Take patient to commode frequently.
Assess patient's ability to make need for help
with voiding known.
If a catheter is necessary, remove it as soon as
possible and follow a bladder training program
(see Chap. 11).
Bowel
1. Altered bowel function in a stroke patient is attributable to:
Altered level of consciousness
Dehydration
Immobility
2. Constipation is the most common problem, along with potential
impaction.
1. Develop a bowel training program:
Provide high-fiber diet to stimulate
defecation (prune juice, roughage).
Initiate a suppository and laxative
regimen.
2. Institute a bowel program. Enemas are
avoided in the presence of increased
intracranial pressure.
After the patient has been discharged, integration back into community is important.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 56 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.617
Rehabilitation continues over time and must be monitored. Depression is common after
stroke and is seen in 40% to 50% of patients.48 Patients and families need to be preparedfor this possibility. The patient should be screened for evidence of depression usingstandardized assessment scales (e.g., Geriatric Depression Scale, Hamilton Rating Scale forDepression). Pharmacotherapy is usually effective in the treatment of depression. Relatedpatient problems and nursing diagnoses are listed in the next section.
Patient Education
Patient and family education takes place within a compressed period of time in the acute care setting. It is
unrealistic to expect that all education can be completed during this short period. Patient education must be
viewed along a continuum that extends through the next level of care and into the community by the health
care provider. Decide what is critical for the patient to know and focus on “just-in-time education.” Common
patient problems and nursing diagnoses include Knowledge Deficit; Caregiver Role Strain; Altered Family
Processes; and Sexual Dysfunction.
CLINICAL PEARLS:Stroke and cardiac risk factors are identical because the vascular system is contiguous.Drawing the correlation between the two can be helpful in patient/family education.
Medications
The most common drug classifications for patients being discharged are antiplatelets and sometimes
anticoagulants. Both require special teaching and follow-up. Monitor for obvious and occult bleeding. All
patients will need periodic monitoring of coagulation and INR to adjust drug dosage.
For patients taking ticlopidine, a complete blood cell count every 2 weeks for 3 months is necessary to monitor
for neutropenia. If the patient has not received the drug while in the hospital, he or she needs to be alerted to
the possibility of diarrhea or rash. Other medications previously taken before the episode need to be evaluated
for continuation such as drugs for hypertension and high cholesterol. In some patients these may be new drugs
for which the patient will need education. For example, statins are recommended for patients after ischemic
stroke.49 Giving written instructions about drugs, including time and dosage, side effects to expect, adverse
reactions, contacting the health provider, and monitoring the schedule, increases adherence to the plan of care
and achievement of expected outcomes.
CHART 25-6 Rehabilitation Strategies Following Stroke
NURSING RESPONSIBILITIES RATIONALE
1. Encourage the patient to do as much of self-care as possible. 1. Increases independence.
2. Teach activities of daily living (ADLs) to compensate for functional
disability. (ADLs include dressing, toileting, bathing, eating, gait
training.)
2. Provides for alternative methods to
compensate for disabilities and increases
level of independence.
3. Instruct patient on bed exercises, such as quadriceps and muscle
tone and strength.
3. Improves gluteal setting.
4. Teach patient transfer techniques (e.g., bed to chair, chair to 4. Increases independence and provides for a
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 57 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
bed). greater number of environmental settings
for the patient.
5. Provide special skin care to maintain intact healthy skin. 5. Pressure ulcers and skin changes can occur
with neurological conditions.
6. Dress patient in own clothes rather than a hospital gown, if
possible.
6. Improves the patient's self-image and
dispels image of the “sick role.”
7. Provide for privacy by screening when the patient is learning new
skills (such as relearning to feed self).
7. Preserves self-esteem and decreases
embarrassment if “accidents” happen.
8. Provide emotional support and encouragement. 8. Helps to motivate the patient.
9. Encourage the patient to express feelings. 9. Decreases anxiety and allows for correction
of misinformation.
10. Be empathetic with the patient's feelings. 10. Increases the nurse's sensitivity to patient
needs.
11. Know what physiotherapist is doing with the patient. 11. Activities can be reinforced by the nurse.
12. Encourage the family to participate (e.g., demonstrate range-of-
motion exercises to the family).
12. Allows family members to feel that they are
“doing something to help.”
What to Expect
Both the patient and family need to know what to expect on discharge, community resources such as stroke
support groups, and reliable publications and websites. The nurse can provide some anticipatory guidance based
on the particular needs of the patient. However, the patient and family cannot be prepared for every
contingency. It is helpful to plan a time for the nurse to call to assess adjustment to the community and any
special problems or concerns. The nurse can triage some problems and manage others independently.
Recovery
Patients who survive a stroke have potential for recovery of function. The extent of the stroke and pre-existing
disease influence the degree of recovery. Most of natural recovery in motor function and speech occurs in the
first 3 to 6 months. However, recovery continues at a slower pace up to a year and beyond with therapy.
REFERENCES
1. American Heart Association. (2007). Heart disease and stroke statistics: 2007 update at a glance. (p.
37). Dallas, TX: American Heart Association.
2. American Heart Association. (2007). Heart disease and stroke statistics: 2007 update at a glance (p.
14). Dallas, TX: American Heart Association.
3. Goldstein, L. B., Adams, R., Alberts, M. J., Appel, L. J., Brass, L. M, Bushnell, C. D., et al. (2006).
46
What to Expect Both the patient and family need to know what to expect on discharge, community resources such as stroke support groups, and reliable publications and websites. The nurse can provide some anticipatory guidance based on the particular needs of the patient. However, the patient and family cannot be prepared for every contingency. It is helpful to plan a time for the nurse to call to assess adjustment to the community and any special problems or concerns. The nurse can triage some problems and manage others independently. Recovery Patients who survive a stroke have potential for recovery of function. The extent of the stroke and pre-‐existing disease influence the degree of recovery. Most of natural recovery in motor function and speech occurs in the first 3 to 6 months. However, recovery continues at a slower pace up to a year and beyond with therapy.
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 56 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
P.617
Rehabilitation continues over time and must be monitored. Depression is common after
stroke and is seen in 40% to 50% of patients.48 Patients and families need to be preparedfor this possibility. The patient should be screened for evidence of depression usingstandardized assessment scales (e.g., Geriatric Depression Scale, Hamilton Rating Scale forDepression). Pharmacotherapy is usually effective in the treatment of depression. Relatedpatient problems and nursing diagnoses are listed in the next section.
Patient Education
Patient and family education takes place within a compressed period of time in the acute care setting. It is
unrealistic to expect that all education can be completed during this short period. Patient education must be
viewed along a continuum that extends through the next level of care and into the community by the health
care provider. Decide what is critical for the patient to know and focus on “just-in-time education.” Common
patient problems and nursing diagnoses include Knowledge Deficit; Caregiver Role Strain; Altered Family
Processes; and Sexual Dysfunction.
CLINICAL PEARLS:Stroke and cardiac risk factors are identical because the vascular system is contiguous.Drawing the correlation between the two can be helpful in patient/family education.
Medications
The most common drug classifications for patients being discharged are antiplatelets and sometimes
anticoagulants. Both require special teaching and follow-up. Monitor for obvious and occult bleeding. All
patients will need periodic monitoring of coagulation and INR to adjust drug dosage.
For patients taking ticlopidine, a complete blood cell count every 2 weeks for 3 months is necessary to monitor
for neutropenia. If the patient has not received the drug while in the hospital, he or she needs to be alerted to
the possibility of diarrhea or rash. Other medications previously taken before the episode need to be evaluated
for continuation such as drugs for hypertension and high cholesterol. In some patients these may be new drugs
for which the patient will need education. For example, statins are recommended for patients after ischemic
stroke.49 Giving written instructions about drugs, including time and dosage, side effects to expect, adverse
reactions, contacting the health provider, and monitoring the schedule, increases adherence to the plan of care
and achievement of expected outcomes.
CHART 25-6 Rehabilitation Strategies Following Stroke
NURSING RESPONSIBILITIES RATIONALE
1. Encourage the patient to do as much of self-care as possible. 1. Increases independence.
2. Teach activities of daily living (ADLs) to compensate for functional
disability. (ADLs include dressing, toileting, bathing, eating, gait
training.)
2. Provides for alternative methods to
compensate for disabilities and increases
level of independence.
3. Instruct patient on bed exercises, such as quadriceps and muscle
tone and strength.
3. Improves gluteal setting.
4. Teach patient transfer techniques (e.g., bed to chair, chair to 4. Increases independence and provides for a
5/9/11 12:08 PMOvid: Clinical Practice of Neurological and Neurosurgical Nursing, The
Page 57 of 62http://ovidsp.tx.ovid.com.proxy.library.vanderbilt.edu/sp-3.4.1a/ovidweb.cgi
bed). greater number of environmental settings
for the patient.
5. Provide special skin care to maintain intact healthy skin. 5. Pressure ulcers and skin changes can occur
with neurological conditions.
6. Dress patient in own clothes rather than a hospital gown, if
possible.
6. Improves the patient's self-image and
dispels image of the “sick role.”
7. Provide for privacy by screening when the patient is learning new
skills (such as relearning to feed self).
7. Preserves self-esteem and decreases
embarrassment if “accidents” happen.
8. Provide emotional support and encouragement. 8. Helps to motivate the patient.
9. Encourage the patient to express feelings. 9. Decreases anxiety and allows for correction
of misinformation.
10. Be empathetic with the patient's feelings. 10. Increases the nurse's sensitivity to patient
needs.
11. Know what physiotherapist is doing with the patient. 11. Activities can be reinforced by the nurse.
12. Encourage the family to participate (e.g., demonstrate range-of-
motion exercises to the family).
12. Allows family members to feel that they are
“doing something to help.”
What to Expect
Both the patient and family need to know what to expect on discharge, community resources such as stroke
support groups, and reliable publications and websites. The nurse can provide some anticipatory guidance based
on the particular needs of the patient. However, the patient and family cannot be prepared for every
contingency. It is helpful to plan a time for the nurse to call to assess adjustment to the community and any
special problems or concerns. The nurse can triage some problems and manage others independently.
Recovery
Patients who survive a stroke have potential for recovery of function. The extent of the stroke and pre-existing
disease influence the degree of recovery. Most of natural recovery in motor function and speech occurs in the
first 3 to 6 months. However, recovery continues at a slower pace up to a year and beyond with therapy.
REFERENCES
1. American Heart Association. (2007). Heart disease and stroke statistics: 2007 update at a glance. (p.
37). Dallas, TX: American Heart Association.
2. American Heart Association. (2007). Heart disease and stroke statistics: 2007 update at a glance (p.
14). Dallas, TX: American Heart Association.
3. Goldstein, L. B., Adams, R., Alberts, M. J., Appel, L. J., Brass, L. M, Bushnell, C. D., et al. (2006).