chapter 136 · test for determining a person’s vitamin d status. 1 usually 1,25(oh) 2 d ......
TRANSCRIPT
Vitamin D Treatment Guidelines
Michael F Holick
DEFINITION OF VITAMIN D DEFICIENCY AND INSUFFICIENCYMeasurement of 25(OH)D in the circulation is the best diagnostic test for determining a person’s vitamin D status.1 Usually 1,25(OH)2D levels in the circulation are normal or elevated in vitamin D deficient patients and thus should not be used to determine a person’s vitamin D status. However, 1,25(OH)2D measurement is of value in acquired and inherited disorders of vitamin D metabolism including pseudovitamin D deficiency rickets, vitamin D resistant rickets, granulomatous disorders and some lymphomas.1
The Institute of Medicine (IOM) and the Endocrine Society have defined vitamin D deficiency as it relates to bone health as a 25(OH)D less than 20 ng/mL (50 nmol/L).7,8 However, the Endocrine Society concluded that vitamin D improves muscle function and based on many association studies may also have some additional benefit in reducing several chronic illnesses. As a result, they defined vitamin D insufficiency as a 25(OH)D of 21–29 ng/mL.8
The Endocrine Society revisited its recommendations9 in light of concerns raised by the IOM committee.10 One of the publications that the IOM committee relied on heavily regarding recommending that a blood level of 25(OH)D greater than 20 ng/mL was sufficient to maintain a healthy skeleton was by Priemel et al.11 The IOM committee concluded that 99% of healthy adult Germans aged 20–70 years who died prematurely in an accident had no evidence of vitamin D deficiency, osteomalacia, i.e. unmineralized osteoid, if their blood level of 25(OH)D was greater than 20 ng/mL. However, the authors reported that 21% of otherwise healthy men and women with a 25(OH)D between 20 ng/mL and 30 ng/mL had evidence of increased osteoid and therefore concluded that to guarantee no evidence of vitamin D deficiency bone disease, a blood level of 25(OH)D should be greater than 30 ng/mL. There was a remarkable between-individual variability of the 25(OH)D/osteoid relationship that is similar to the wide variability reported for the relationship between 25(OH)D and parathyroid hormone (PTH).12-15 Most studies, however, have suggested that when 25(OH)D is between 30 ng/mL and 40 ng/mL, PTH levels continue to decline and finally plateau suggesting that for maintaining maximum effect of vitamin D on calcium metabolism and bone health, 25(OH)D should be at least 30 ng/mL. In one study of over 1,500 postmenopausal women, a serum 25(OH)D of 21 ng/mL was associated with a two fold higher risk of having secondary hyperparathyroidism compared to women who had a blood level of 25(OH)D greater than 30 ng/mL (Figures 1A and B).15
The Endocrine Society also conducted a meta-analysis of 23 trials of fall risk and found that vitamin D supplementation above 800 IUs
Chapter 136
INTRODUCTIONVitamin D, the sunshine vitamin, has been recognized as being essential for children’s and adults’ bone health for more than 100 years. The revelation that vitamin D needs to be metabolized to 25-hydroxyvitamin D [25(OH)D] in the liver is followed by its activation in the kidneys to 1,25-dihydroxyvitamin D [1,25(OH)2D] by all definitions makes vitamin D a hormone.1 1,25(OH)2D interacts with its nuclear vitamin D receptor (VDR) in the small intestine to increase the efficiency of intestinal calcium absorption. In the kidneys, this hormone increases tubular reabsorption of calcium. 1,25(OH)2D’s function in the bone is to interact with the VDR in osteoblasts resulting in the expression of receptor activator of NF-κB ligand (RANKL). The interaction of RANK on monocytes with RANKL results in signal transduction resulting in the formation of mature multinucleated osteoclasts, which release HCl and collagenases in order to digest the bone and release precious calcium into the circulation. Thus, the endocrine function for vitamin D is to maintain serum calcium within a physiologically acceptable range in order to maintain a wide variety of metabolic functions through signal transduction mechanisms as well as neuromuscular activity. 1,25(OH)2D also stimulates intestinal phosphorus absorption. Therefore, by 1,25(OH)2D maintaining an adequate serum calcium and phosphorus product, the newly formed collagen matrix in the skeleton is mineralized.1
It is now recognized that essentially every tissue and cell in the body has a VDR. In vitro studies have revealed that when cell lines are incubated with 1,25(OH)2D more than 200 genes are directly affected. It has been estimated that upwards of 2,000 genes may be directly or indirectly influenced by 1,25(OH)2D.2,3 In addition, there is mounting evidence that 1,25(OH)2D has epigenetic influences on gene expression.3 Of particular interest is that 1,25(OH)2D can decrease proliferation of hyperproliferative cells and malignant cells, induce terminal differentiation of psoriatic skin cells and malignant cells including some leukemic cell lines, induce apoptosis, decrease angiogenesis, decrease renin production, increase insulin secretion, increase insulin sensitivity and cause vascular relaxation.4 In addition, it is a major regulator of immune function.5 1,25(OH)2D is known to increase the production of T2 lymphocytes, inhibit immunoglobulin synthesis and stimulate macrophage production of cathelicidin.5,6 These observations may help explain many association studies linking sunlight deficiency and vitamin D deficiency with a wide range of diseases including many deadly cancers, several autoimmune diseases including Type 1 diabetes, multiple sclerosis, rheumatoid arthritis and Crohn’s disease, cardiovascular disease, Type 2 diabetes and infectious diseases.1,4,5

620
Metabolic Disorders Section 18
colon, prostate and breast cancer.22 Follow-up studies suggested that a multitude of cancers are associated with lack of sun exposure and vitamin D deficiency.23 As these observations were being published other investigators began to report on associations with vitamin D deficiency and increased risk for autoimmune diseases including Type 1 diabetes, multiple sclerosis and rheumatoid arthritis.23-27 Other reports suggested that a blood level of 25(OH)D greater than 30 ng/mL reduced risk for peripheral vascular disease by more than 80%.28 Vitamin D deficiency was associated with increased risk not only for myocardial infarction29 but also for decreased cardiovascular mortality by 15–25%.30 A meta-analysis of calcium and vitamin D intake from the National Health Nutritional Survey revealed a 33% reduced risk of developing Type II diabetes.31 In addition, other studies have suggested that vitamin D deficiency was associated with an increased decline in neurocognitive function and increased risk for depression, Alzheimer’s disease and schizophrenia.32,33
Although there are few well-controlled randomized controlled trials to support many of these beneficial association effects of vitamin D for overall health and well-being, there are several recent trials that corroborate these association studies. A study in postmenopausal women who received 1,500 mg of calcium and 1,100 IUs of vitamin D3 supplementation daily for 4 years reduced overall risk of developing cancer by more than 60%.34 Gagnon et al.35 reported in a prospective study of 4,164 adults (mean age 50 years) that after 5 years of follow-up, adults with a blood level of 25(OH)D less than 18 ng/mL and 18–23 ng/mL had a 141% and 174% increased risk for developing metabolic syndrome compared to adults who had a blood level of 25(OH)D greater than 34 ng/mL. This is consistent with Deleskog et al.36 who provided compelling evidence that vitamin D deficiency accelerates the progression from metabolic syndrome to Type II diabetes. After a full adjustment for confounding variables, a 42% reduction in risk of progression to Type II diabetes was found in adults who had the highest circulating levels of 25(OH)D. When comparing those adults with the lowest blood levels of 25(OH)D to those with the highest blood levels the reduction in risk of progression to Type II diabetes was 62%.
daily was associated with a statistically significant reduction in risk of falls [odds ratio (OR) 0.84; 95% confidence interval (CI) 0.76–0.93; inconsistency (12 equal 61%; 23 studies)].16 This effect was most prominent in patients who were vitamin D deficient at baseline. In one randomized controlled trial, nursing home residents who received either 200, 400 or 600 IUs of vitamin D daily for 5 months demonstrated no significant fall reduction whereas residents who received 800 IUs of vitamin D daily for 5 months had a 72% reduced risk of falls.17 The IOM on the other hand concluded that there was no benefit of vitamin D supplementation on fall risk although the overall meta-analysis of 12 randomized controlled trials showed a significant benefit of vitamin D supplementation on fall prevention [OR 0.89; 95% CI 0.80–0.99].7,9 The beneficial effect of vitamin D in reduced risk for falls is consistent with the 2010 assessment by the International Osteoporosis Foundation and the 2011 assessment of the Agency for Healthcare Research and Quality for the US Preventative Services Task Force who concluded that vitamin D was an effective intervention for preventing falls in older adults.18,19
ASSOCIATION STUDIES RELATED TO NONCALCEMIC HEALTH BENEFITS OF VITAMIN DThere is a long and sustained history regarding lack of sun exposure and vitamin D deficiency being associated with increased risk for many acute and chronic illnesses. The first observation was made by Finsen in the late 1800s and early 1900s. He demonstrated that exposure to sunlight was an effective method for treating tuberculosis of the skin. It was also realized that living above 5,000 feet altitude in the Swiss Alps was effective in preventing and treating tuberculosis. In 1915, it was reported that men and women who worked indoors were more likely to die of cancer than those who worked outdoors.20 A study in United States revealed that people living in the Northeast were more likely to die of cancer than those who lived in southern sunny states including Texas and Georgia among others.21
In the early 1990s, reports appeared suggesting that a higher intake of vitamin D or living at lower latitudes resulted in reduced risk for
Figures 1A and B: (A) Mean (±SE) serum parathyroid hormone (PTH) (picograms per milliliter) by serum 25(OH)D subgroups. Subject PTH concentrations (pg/mL) relative to serum 25(OH)D concentrations sorted by subgroups delineated by predefined cutoffs for analyses of 25(OH)D inadequacy. Serum PTH values began to increase with 25(OH)D concentrations less than 29.8 ng/mL; (B) Percent of subjects with secondary hyperparathyroidism by 25(OH)D level. The percent of subjects with secondary hyperparathyroidism (PTH > 40 pg/mL) sorted by subgroups with serum 25(OH)D concentrations delineated by predefined cutoffs for analyses of 25(OH)D inadequacy.Source: Reproduced with permission from Holick MF, Siris ES, Binkley N, et al. Prevalence of vitamin D inadequacy among postmenopausal North American women receiving osteoporosis therapy. J Clin Endocrinol Metab. 2005;90:3215-24.
A B

621
Chapter 136 Vitamin D Treatment GuidelinesSection 18
The IOM concluded that improvement in vitamin D status significantly reduced risk for mortality.7 However, there was concern by the IOM that blood levels of 25(OH)D greater than 30 ng/mL could increase risk for mortality. One of the studies that was reported by the IOM, in fact, stated that there was a significant reduction in mortality until a blood level of 50 ng/mL was reached and then only in women was there possibly an increased risk for mortality.37 In a recent study of 1,801 adults with documented metabolic syndrome, 92% had a 25(OH)D less than 30 ng/mL. After adjusting for confounding variables, the investigators observed a 75% reduction in all-cause mortality and 66% reduction in cardiovascular disease mortality in adults who had blood levels of 25(OH)D greater than 30 ng/mL compared to adults who were vitamin D deficient with a 25(OH)D less than 10 ng/mL.30
MECHANISMS FOR NONCALCEMIC BENEFITS OF VITAMIN DEssentially every tissue and cell in the body has a vitamin D receptor. There have been a multitude of in vitro studies suggesting that the active form of vitamin D, 1,25(OH)2D, locally produced in many tissues and cells in the body is able to directly or indirectly regulate up to 2,000 genes.2,3 Our recent study in healthy adults receiving vitamin D supplementation revealed that 291 genes were directly influenced by improvement in serum 25(OH)D levels. 1,25(OH)2D is a potent regulator of cellular proliferation and differentiation, induces apoptosis and inhibits angiogenesis, which may help explain its antimalignant properties.38 It is a potent immunomodulator39 and plays a critical role in helping macrophages kill ineffective agents such as TB.5,6 This may help explain observations that maintenance of blood levels of 25(OH)D greater than 30 ng/mL reduces risk for upper respiratory tract infections.40 Beta islet cells have a VDR and 1,25(OH)2D enhances insulin secretion. Vascular smooth muscle has a VDR as do cardiomyocytes, and 1,25(OH)2D not only causes vascular relaxation but also inhibits cholesterol oxidation in foam cells.41-44 A recent study in teenage African Americans revealed that supplementation of 2,000 IUs of vitamin D3 for 4 months, which raised their blood level of 25(OH)D greater than 30 ng/mL, also resulted in a decrease in vascular resistance.45
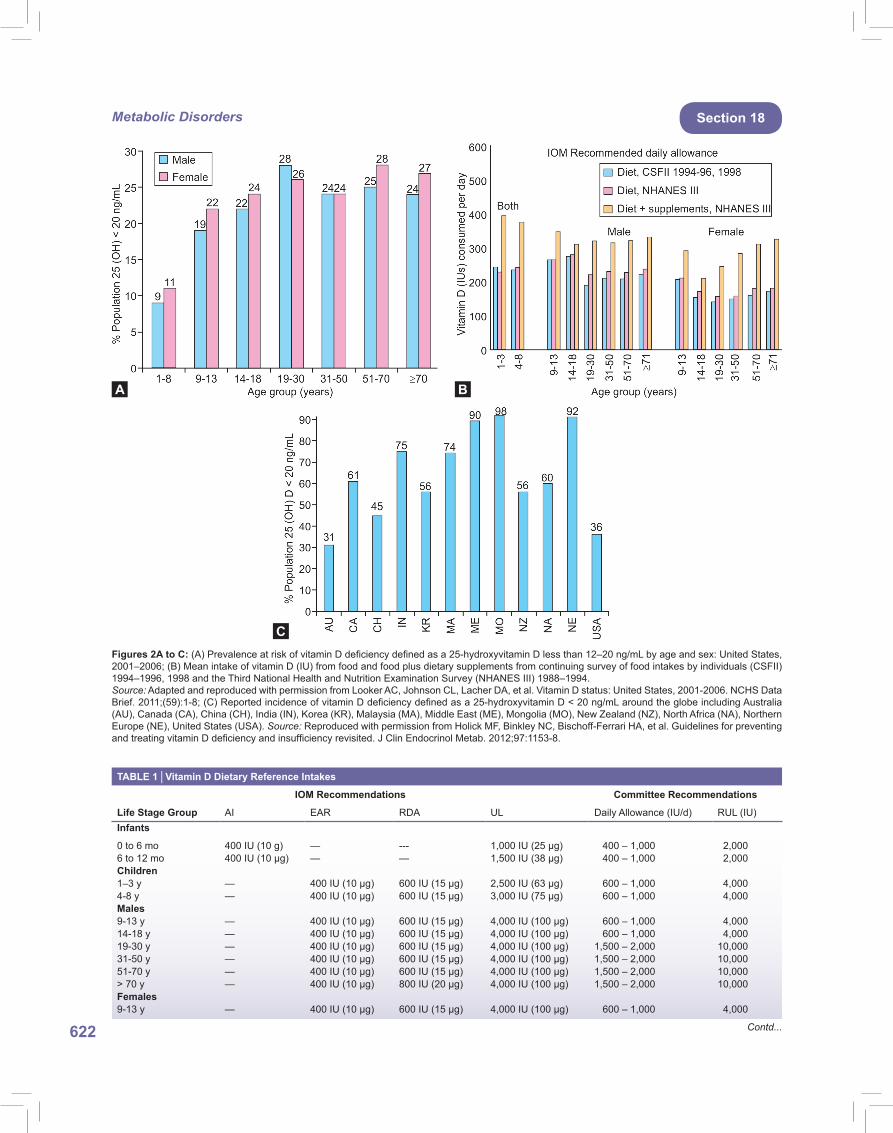
VITAMIN D DEFICIENCY PANDEMICEssentially all children and adults throughout the world are at risk for vitamin D deficiency and insufficiency.1 Even in the US where some foods are fortified with vitamin D it is estimated that on average 32% of children and adults have a blood level of 25(OH)D less than 20 ng/mL (Figure 2).46 The study in young children in the US revealed that 50% of children 1–5 years old and 70% of children 6–11 years old had evidence of vitamin D deficiency or insufficiency, i.e. a 25(OH)D less than 30 ng/mL.47 It has been estimated that 50 million teenagers in the US are at risk for vitamin D deficiency or insufficiency and have a more than 2.4 fold increased risk of having an elevated blood pressure and blood sugar and a four fold increased risk for metabolic syndrome.48 This differs from the conclusion by the IOM that widespread vitamin D deficiency is not a concern in the North American population.7 These results are similar to what has been observed in Canada, Brazil, Australia, India, New Zealand, Mongolia, Africa and even in the Middle East where more than 90% of both children and adults have been reported to be vitamin D deficient or insufficient (Figure 2).49-62
Causes for the Vitamin D Deficiency PandemicThe major cause for the vitamin D deficiency pandemic is the lack of appreciation that very few foods naturally contain vitamin D and
that most children and adults have always depended throughout evolution on sun exposure for their vitamin D requirement. Skin pigmentation evolved for people living near the equator to prevent them from developing skin cancer. However, even their dark skin pigmentation permitted vitamin D synthesis. Healthy black children in South Africa have a blood level of 25(OH)D of 49 ± 4 ng/mL,63 similar to adult Maasai herders who are reported to have a blood level of 47 ± 10 ng/mL.64 Pigmentation devolved as people moved north and south of the equator in order for them to produce enough vitamin D in their skin to maintain a healthy skeleton. This was especially true for females. If they were vitamin D deficient during their first few years of life, their pelvis would be flat and deformed making it difficult if not impossible for childbirth. Because sunlight played such a critical role in providing humans with their vitamin D requirement, there was no need for there to be natural sources of vitamin D in the food with the exception of people living far North and South of the equator where fish, seal blubber, polar bear liver and whale blubber provided an adequate source of vitamin D. Even in the US where many dairy products, including milk and cheese, are fortified with vitamin D, as well as some orange juices and cereals, it was reported that neither children nor adults were able to obtain an adequate amount of vitamin D from dietary sources (Figures 2A to C).65
Prevention and Treatment of Vitamin D DeficiencyAs seen in Table 1, the IOM has suggested7 that most children and adults only require 600 IUs of vitamin D daily. Based on a review of literature, the Endocrine Society recommended8 higher amounts of vitamin D for the treatment and prevention of vitamin D deficiency (Table 1). For example, studies in adults revealed that 1,000 IUs of vitamin D daily during the winter in Boston was incapable of raising their blood levels of 25(OH)D above 30 ng/mL.66 It is estimated that for every 100 IUs of vitamin D ingested, blood levels of 25(OH)D increase on average by 0.5–1.0 ng/mL. To treat vitamin D deficiency in children 2,000 IUs of vitamin D daily for 6–8 weeks or 50,000 IUs of vitamin D once a week for 8 weeks is both effective and safe.67 In adults, 50,000 IUs of vitamin D once a week for 8 weeks (equivalent to approximately 6,500 IUs of vitamin D daily) is often adequate to treat vitamin D deficiency and fill the empty vitamin D tank.68 To maintain vitamin D sufficiency, i.e. to keep the vitamin D tank full, adults can take 50,000 IUs of vitamin D once every 2 weeks (equivalent to approximately 3,300 IUs of vitamin D daily) for at least 6 years without any concern for vitamin D toxicity (Figures 3A to C).69
Vitamin D toxicity has been of great concern especially for children. However, it is now recognized even by the IOM that vitamin D is not as toxic as once thought.7 They recommended that up to 4,000 IUs of vitamin D daily for most children and adults was safe. A study in healthy adult males receiving 10,000 IUs of vitamin D3 daily for 5 months did not cause any untoward toxicity.70 The IOM and the Endocrine Society also recognize that patients with kidney stones or with primary hyperparathyroidism can receive vitamin D supplementation without concern for increased risk for developing kidney stones or increased blood calcium respectively.7,8
CONCLUSIONFor more than 40 years, it has been recommended by both the dermatology societies and the World Health Organization that sunlight should be avoided because of increased risk for skin cancer. However, little concern was voiced about the significant health burden that has resulted in this recommendation. There is very little, if any, vitamin D in the diet and therefore most children and adults on this planet have and continue to obtain most of their vitamin D from casual sun exposure. A healthy adult in a bathing suit exposed to an amount of sunlight that causes a mild pinkness to the skin, i.e. one minimal erythemal dose, is equivalent to
622
Metabolic Disorders Section 18
Figures 2A to C: (A) Prevalence at risk of vitamin D deficiency defined as a 25-hydroxyvitamin D less than 12–20 ng/mL by age and sex: United States, 2001–2006; (B) Mean intake of vitamin D (IU) from food and food plus dietary supplements from continuing survey of food intakes by individuals (CSFII) 1994–1996, 1998 and the Third National Health and Nutrition Examination Survey (NHANES III) 1988–1994.Source: Adapted and reproduced with permission from Looker AC, Johnson CL, Lacher DA, et al. Vitamin D status: United States, 2001-2006. NCHS Data Brief. 2011;(59):1-8; (C) Reported incidence of vitamin D deficiency defined as a 25-hydroxyvitamin D < 20 ng/mL around the globe including Australia (AU), Canada (CA), China (CH), India (IN), Korea (KR), Malaysia (MA), Middle East (ME), Mongolia (MO), New Zealand (NZ), North Africa (NA), Northern Europe (NE), United States (USA). Source: Reproduced with permission from Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Guidelines for preventing and treating vitamin D deficiency and insufficiency revisited. J Clin Endocrinol Metab. 2012;97:1153-8.
A B
C
TABLE 1 │Vitamin D Dietary Reference Intakes
IOM Recommendations Committee Recommendations
Life Stage Group AI EAR RDA UL Daily Allowance (IU/d) RUL (IU)Infants
0 to 6 mo 400 IU (10 g) — --- 1,000 IU (25 µg) 400 – 1,000 2,0006 to 12 mo 400 IU (10 µg) — — 1,500 IU (38 µg) 400 – 1,000 2,000Children1–3 y — 400 IU (10 µg) 600 IU (15 µg) 2,500 IU (63 µg) 600 – 1,000 4,0004-8 y — 400 IU (10 µg) 600 IU (15 µg) 3,000 IU (75 µg) 600 – 1,000 4,000Males9-13 y — 400 IU (10 µg) 600 IU (15 µg) 4,000 IU (100 µg) 600 – 1,000 4,00014-18 y — 400 IU (10 µg) 600 IU (15 µg) 4,000 IU (100 µg) 600 – 1,000 4,00019-30 y — 400 IU (10 µg) 600 IU (15 µg) 4,000 IU (100 µg) 1,500 – 2,000 10,00031-50 y — 400 IU (10 µg) 600 IU (15 µg) 4,000 IU (100 µg) 1,500 – 2,000 10,00051-70 y — 400 IU (10 µg) 600 IU (15 µg) 4,000 IU (100 µg) 1,500 – 2,000 10,000> 70 y — 400 IU (10 µg) 800 IU (20 µg) 4,000 IU (100 µg) 1,500 – 2,000 10,000Females9-13 y — 400 IU (10 µg) 600 IU (15 µg) 4,000 IU (100 µg) 600 – 1,000 4,000
Contd...

623
Chapter 136 Vitamin D Treatment GuidelinesSection 18
IOM Recommendations Committee Recommendations
Life Stage Group AI EAR RDA UL Daily Allowance (IU/d) RUL (IU)14-18 y — 400 IU (10 µg) 600 IU (15 µg) 4,000 IU (100 µg) 600 – 1,000 4,00019-30 y — 400 IU (10 µg) 600 IU (15 µg) 4,000 IU (100 µg) 1,500 – 2,000 10,00031-50 y — 400 IU (10 µg) 600 IU (15 µg) 4,000 IU (100 µg) 1,500 – 2,000 10,00051-70 y — 400 IU (10 µg) 600 IU (15 µg) 4,000 IU (100 µg) 1,500 – 2,000 10,000> 70 y — 400 IU (10 µg) 800 IU (20 µg) 4,000 IU (100 µg) 1,500 – 2,000 10,000Pregnancy14-18 y — 400 IU (10 µg) 600 IU (15 µg) 4,000 IU (100 µg) 600 – 1,000 4,00019-30 y — 400 IU (10 µg) 600 IU (15 µg) 4,000 IU (100 µg) 1,500 – 2,000 10,00031-50 y — 400 IU (10 µg) 600 IU (15 µg) 4,000 IU (100 µg) 1,500 – 2,000 10,000Lactation*
14-18 y — 400 IU (10 µg) 600 IU (15 µg) 4,000 IU (100 µg) 600 – 1,000 4,00019-30 y — 400 IU (10 µg) 600 IU (15 µg) 4,000 IU (100 µg) 1,500 – 2,000 10,00031-50 y — 400 IU (10 µg) 600 IU (15 µg) 4,000 IU (100 µg) 1,500 – 2,000 10,000
* Mother’s requirement 4,000 – 6,000 (mother’s intake for infant’s requirement if infant is not receiving 400 IU/d)Abbreviations: AI, Adequate intake; EAR, Estimated average requirement; IU, International units; RDA, Recommended dietary allowance; UL, Tolerable upper intake level.
Figures 3A to C: (A) Mean serum 25-hydroxyvitamin D [25(OH)D] levels in all patients. Includes patients treated with 50,000 IU vitamin D2 every 2 weeks (maintenance therapy, n = 81), including those patients with vitamin D insufficiency who were initially treated with 8 weeks of 50,000 IU vitamin D2 weekly prior to maintenance therapy (n = 39). Error bars represent standard error of the mean, mean result over 5 years shown. Time 0 is initiation of treatment, results shown as mean values averaged for 6-month intervals. When mean 25(OH)D in each 6-month group was compared to mean initial 25(OH)D, p < 0.001 up until month 43; p < 0.001 when all remaining values after month 43 were compared to mean initial 25(OH)D; (B) Mean serum 25(OH)D levels in patients receiving maintenance therapy only: levels for 37 patients who were vitamin D insufficient [25(OH)D levels < 30 ng/mL] and 5 patients who were vitamin D sufficient [25(OH)D levels ≥ 30 ng/mL] who were treated with maintenance therapy of 50,000 IU vitamin D2 every 2 weeks. Error bars represent standard error of the mean, mean result over 5 years shown. Time 0 is initiation of treatment, results shown as mean values averaged for 6-month intervals. When mean 25(OH)D in each 6-month group was compared to mean initial 25(OH)D, p < 0.001 up until month 37; p < 0.001 when all remaining values after month 43 were compared to mean initial 25(OH)D; (C) Serum calcium levels: results for all 81 patients who were treated with 50,000 IU of vitamin D2. Error bars represent standard error of the mean. Time 0 is initiation of treatment, results shown as mean values averaged for 6-month intervals. Normal serum calcium: 8.5–10.2 mg/dL.Source: Reproduced with permission from Pietras SM, Obayan BK, Cai MH, et al. Vitamin D2 treatment for vitamin D deficiency and insufficiency for up to 6 years. Arch Intern Med. 2009;169:1806-8.
BA
C
Contd...

624
Metabolic Disorders Section 18
ingesting approximately 20,000 IUs of vitamin D.4 Thus, the skin has a huge capacity to produce vitamin D. Sensible sun exposure, i.e. 25–50% of the time it would take to get a mild sunburn of arms, legs, abdomen and back, when possible 2–3 times a week at times of the year when sunlight produces vitamin D in the skin71 is a reasonable approach to help maintain healthy blood levels of 25(OH)D. There is no question that excessive exposure to the sun especially on the face and top of the hands increases risk for nonmelanoma skin cancer, which is easy to detect and easy to treat.72 Melanoma, the most deadly skin cancer, curiously is found mainly on the least sun exposed areas and remarkably occupational sun exposure decreases risk for melanoma.72 Thus, the message of avoidance of any sun exposure should be modified. Even the skin cancer capital of the world, Australia, now recommends sensible sun exposure as a source of vitamin D since it is estimated that up to 40% of Australians are vitamin D deficient. The bottom line is that we need to have global recognition that to improve the overall health and well-being of children and adults as it relates to their vitamin D status, vitamin D fortification programs should be enhanced not only in dairy and juice products but also in grains such as flour and corn meal. In addition, recommendations for sensible sun exposure should also be embraced by health care providers and regulators. It has been estimated that there could be as much as a 25% reduction in all health care costs just by improving the vitamin D status of children and adults worldwide.
REFERENCES
1. Holick MF. Vitamin D deficiency. New Engl J Med. 2007;357:266-81. 2. Nagpal S, Na S, Rathnachalam R. Noncalcemic actions of vitamin D
receptor ligands. Endocr Rev. 2005;26:662-87. 3. Hossein-Nezhad A, Holick MF. Optimize dietary intake of vitamin D:
an epigenetic perspective. Curr Opin Clin Nutr Metab Care. 2012;15: 567-79.
4. Holick MF. Vitamin D and health: evolution, biologic functions, and recommended dietary intakes for vitamin D. Clin Rev Bone Miner Metab. 2009;7(1):2-19.
5. Adams JS, Hewison M. Update in Vitamin D. J Clin Endocrinol Metab. 2010;95(2):471-8.
6. Liu PT, Stenger S, Li H, et al. Toll-like receptor triggering of a vitamin D-mediated human antimicrobial response. Science. 2006;311:1770-3.
7. Ross AC, Taylor CL, Yaktine AL, et al. (2011). Dietary reference intakes for calcium and vitamin D. Committee to review dietary reference intakes for calcium and vitamin D. [online]. Washington DC: The National Academies Press. Available from http://books.nap.edu/openbook.php?record_id=13050 [Accessed November, 2012].
8. Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(7):1911-30.
9. Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Guidelines for preventing and treating vitamin D deficiency and insufficiency revisited. J Clin Endocrinol Metab. 2012;97:1153-8.
10. Rosen CJ, Abrams SA, Aloia JF, et al. IOM committee members respond to Endocrine Society vitamin D guideline. J Clin Endocrinol Metab. 2012. 97(4):1146-52.
11. Priemel M, von Domarus C, Klatte TO, et al. Bone mineralization defects and vitamin D deficiency: histomorphometric analysis of iliac crest bone biopsies and circulating 25-hydroxyvitamin D in 675 patients. J Bone Miner Res. 2010;25(2):305-12.
12. Heaney RP. Vitamin D and bone health—discussion points following the Recent Institute of Medicine recommendations. US Endocrinology. 2011;7(2):137-40.
13. Rucker D, Allan JA, Fick GH, et al. Vitamin D insufficiency in a population of healthy western Canadians. CMAJ. 2002;166(12):1517-24.
14. Holick MF. The D-batable parathyroid hormone plateau. Am J Med. 2011;124(12):1095-6.
15. Holick MF, Siris ES, Binkley N, et al. Prevalence of vitamin D inadequacy among postmenopausal North American women receiving osteoporosis therapy. J Clin Endocrinol Metab. 2005;90:3215-24.
16. Murad MH, Elamin KB, Abu Elnour NO, et al. The Effect of Vitamin D on falls: A systematic review and meta-analysis. J Clin Endocrinol Metab. 2011;96(10):2997-3006.
17. Broe KE, Chen TC, Weinberg J, et al. A higher dose of vitamin D reduces the risk of falls in nursing home residents: a randomized, multiple-dose study. J Am Geriatr Soc. 2007;55(2):234-9.
18. Michael YL, Whitlock EP, Lin JS, et al. Primary care-relevant interventions to prevent falling in older adults: A systematic evidence review for the U.S. Preventive Services Task Force. Ann Intern Med. 2010;153:815-25.
19. Pfeifer M, Begerow B, Minne HW, et al. Effects of a long-term vitamin D and calcium supplementation on falls and parameters of muscle function in community-dwelling older individuals. Osteoporos Int. 2009;20:315-22.
20. Hoffman FL. The mortality of cancer throughout the world. Appendix E, New York: Prudential Press; 1915.
21. Apperly FL. The relation of solar radiation to cancer mortality in North America. Cancer Res. 1941;1:191-5.
22. Garland CF, Garland FC, Gorham ED, et al. The role of vitamin D in cancer prevention. Am J Public Health. 2006;96(2):252-61.
23. Grant WB. An estimate of the global reduction in mortality rates through doubling vitamin D levels. Eur J Clin Nutr. 2011;65(9):1016-26.
24. Merlino LA, Curtis J, Mikuls TR, et al.; Iowa Women’s Health Study. Vitamin D intake is inversely associated with rheumatoid arthritis. Arthritis Rheum. 2004;50(1):72-7.
25. Mohr SB, Garland CF, Gorham ED, et al. The association between ultraviolet B irradiance, vitamin D status and incidence rates of type 1 diabetes in 51 regions worldwide. Diabetologia. 2008;51:1391-8.
26. Ponsonby AL, McMichael A, van der Mei I. Ultraviolet radiation and autoimmune disease: insights from epidemiological research. Toxicology. 2002;181-182:71-8.
27. Munger KL, Zhang SM, O’Reilly E, et al. Vitamin D intake and incidence of multiple sclerosis. Neurology. 2004;62(1):60-5.
28. Melamed ML, Muntner P, Michos ED, et al. Serum 25-hydroxyvitamin D levels and the prevalence of peripheral arterial disease: results from NHANES 2001 to 2004. Arterioscler Thromb Vasc Biol. 2008;28:1179-85.
29. Wang TJ, Pencina MJ, Booth SL, et al. Vitamin D deficiency and risk of cardiovascular disease. Circulation. 2008;117(4):503-11.
30. Thomas GN, Hartaigh BO, Bosch JA, et al. Vitamin D levels predicts all-cause and cardiovascular disease mortality in subjects with the metabolic syndrome: the Ludwigshafen Risk and Cardiovascular Health (LURIC) Study. Diabetes Care. 2012;35(5):1158-64.
31. Pittas AG, Lau J, Hu FB, et al. Review: the role of vitamin D and calcium in type 2 diabetes. A systematic review and meta-analysis. J Clin Endocrinol Metab. 2007;92:2017-29.
32. McGrath J, Selten JP, Chant D. Long-term trends in sunshine duration and its association with schizophrenia birth rates and age at first registration—data from Australia and the Netherlands. Schizophr Res. 2002;54:199-212.
33. Nimitphong H, Holick MF. Vitamin D, neurocognitive functioning and immunocompetence. Curr Opin Clin Nutr Metab Care. 2011;14:7-14.
34. Lappe JM, Travers-Gustafson D, Davies KM, et al. Vitamin D and calcium supplementation reduces cancer risk: results of a randomized trial. Am J Clin Nutr. 2007;85(6):1586-91.
35. Gagnon C, Lu ZX, Magliano DJ, et al. Low serum 25-hydroxyvitamin D is associated with increased risk of the development of the metabolic syndrome at five years: results from a national, population-based prospective study (The Australian Diabetes, Obesity and Lifestyle Study: AusDiab). J Clin Endocrinol Metab. 2012;97(6):1953-61.
36. Deleskog, A, Hilding, A, Brismar, K, Hamsten, A, Efendic, S and Ostenson, CG. Low Serum 25-Hydroxyvitamin D level predicts progression to type 2 diabetes in individuals with prediabetes but not with normal glucose tolerance. Diabetologia. 2012;5(6):1668-78.
37. Melamed ML, Michos ED, Post W et al. 25-hydroxyvitamin D levels and the risk of mortality in the general population. Arch Intern Med. 2008;168(15):1629-37.
38. Mantell DJ, Owens PE, Bundred NJ, et al. 1α,25-dihydroxyvitamin D3 inhibits angiogenesis in vitro and in vivo. Circ Res. 2000;87:412-20.
39. Cantorna MT, Zhu Y, Froicu M, et al. Vitamin D status, 1,25-dihydroxyvitamin D3, and the immune system. Am J Clin Nutr. 2004; 80(suppl):1717S-20S.
40. Ginde AA, Mansbach JM, Camargo CA. Association between serum 25-hydroxyvitamin D Level and upper respiratory tract infection in the

625
Chapter 136 Vitamin D Treatment GuidelinesSection 18
Third National Health and Nutrition Examination Survey. Arch Intern Med. 2009;169(4):384-90.
41. Zitterman A, Iodice S, Pilz S, et al. Vitamin D deficiency and mortality risk in the general population: a meta-analysis of prospective cohort studies. Am J Clin Nutr. 2012;95:91-100.
42. O’Keefe JH, Lavie CJ, Holick MF. Vitamin D supplementation for cardiovascular disease prevention. J Am Med Assoc. 2011;306(14):1546-7.
43. Pilz S, Tomaschitz A, Marz W, et al. Vitamin D, cardiovascular disease and mortality. Clin Endocrinol. 2011;75(5):575-84.
44. Oh J, Weng S, Felton SK, et al. 1,25(OH)2 vitamin D inhibits foam cell formation and suppresses macrophage cholesterol uptake in patients with type 2 diabetes mellitus. Circulation. 2009;120(8):687-98.
45. Dong Y, Stallmann-Jorgenson IS, Pollock NK, et al. A 16-week randomized clinical trial of 2,000 IU daily vitamin D3 supplementation in black youth: 25-hydroxyvitamin D, adiposity, and arterial stiffness. J Clin Endocrinol Metab. 2010;95(10):4584-91.
46. Looker AC, Johnson CL, Lacher DA, et al. Vitamin D status: United States, 2001-2006. NCHS Data Brief. 2011;(59):1-8.
47. Kumar J, Muntner P, Kaskel FJ, et al. Prevalence and associations of 25-hydroxyvitamin D deficiency in US children: NHANES 2001-2004. Pediatrics. 2009;124(3):e362-70.
48. Reis JP, von Muhlen D, Miller ER, et al. Vitamin D status and cardiometabolic risk factors in the United States adolescent population. Pediatrics. 2009;124(3):e371-9.
49. Whiting SJ, Langlois KA, Vatanparast H, et al. The vitamin D status of Canadians relative to the 2011 Dietary Reference Intakes: an examination in children and adults with and without supplement use. Am J Clin Nutr. 2011;94:128-35.
50. Hanley DA, Cranney A, Jones G, et al. Vitamin D in adult health and disease: a review and guideline statement from Osteoporosis Canada. Can Med Assoc J. 2010;182(12):E610-8.
51. Lips P. Vitamin D status and nutrition in Europe and Asia. J Steroid Biochem Mol Biol. 2007;103(3-5):620-5.
52. Rockell JE, Skeaff CM, Williams SM, et al. Serum 25-hydroxyvitamin D concentrations of New Zealanders aged 15 years and older. Osteoporos Int. 2006;17:1382-9.
53. Goswami R, Gupta N, Goswami D, et al. Prevalence and significance of low 25-hydroxyvitamin D concentrations in healthy subjects in Delhi. Am J Clin Nutr. 2000;72:472-5.
54. Prentice A. Vitamin D deficiency: a global perspective. Nutr Rev. 2008;66:S153-64.
55. Marwaha RK, Tandon N, Reddy D, et al. Vitamin D and bone mineral density status of healthy school children in northern India. Am J Clin Nutr. 2005;82:477-82.
56. Munns C, Zacharin MR, Rodda CP, et al. Prevention and treatment of infant and childhood vitamin D deficiency in Australia and New Zealand: a consensus statement. Med J Aust. 2006;185(5):268-72.
57. Maeda SS, Kunii IS, Hayashi L, et al. The effect of sun exposure on 25-hydroxyvitamin D concentrations in young healthy subjects living in the city of Sao Paulo, Brazil. Braz J Med Biol Res. 2007;40(12):1653-9.
58. Sedrani SH. Low 25-hydroxyvitamin D and normal serum calcium con-centrations in Saudi Arabia: Riyadh region. Ann Nutr Metab. 1984;28: 181-5.
59. El-Kaissi S, Sherbeeni, S. Vitamin D deficiency in the Middle East and its health consequences for adults. In: Holick MF (Ed). Vitamin D: Physiology, Molecular Biology, and Clinical Applications, 2nd edition. New York: Humana Press; 2010. pp. 495-504.
60. El-Hajj Fuleihan G. Vitamin D deficiency in the Middle East and its health consequences for children. In: Holick MF (Ed). Vitamin D: Physiology, Molecular Biology, and Clinical Applications, 2nd Edition. New York: Humana Press; 2010. pp. 469-94.
61. Daly RM, Gagnon C, Lu ZX, et al. Prevalence of vitamin D deficiency and its determinants in Australian adults aged 25 years and older: a national, population-based study. Clin Endocrinol. 2012;77(1):26-35.
62. Rich-Edwards JW, Ganmaa D, Kleinman K, et al. Randomized trial of fortified milk and supplements to raise 25-hydroxyvitamin D concentrations in school children in Mongolia. Am J Clin Nutr. 2011;94:578-84.
63. Prentice A, Schoenmakers I, Jones KS, et al. Vitamin D deficiency and its health consequences in Africa. In: Holick MF (Ed). Vitamin D: Physiology, Molecular Biology, and Clinical Applications, 2nd Edition. New York: Humana Press; 2010. pp. 505-28.
64. Luxwolda MF, Kuipers RS, Kema IP, et al. Traditionally living populations in East Africa have a mean serum 25-hydroxyvitamin D concentration of 115 nmol/l. Br J Nutr. 2012;108(9):1557-61.
65. Moore C, Murphy MM, Keast DR, et al. Vitamin D intake in the United States. J Am Diet Assoc. 2004;104:980-3.
66. Holick MF, Biancuzzo RM, Chen TC, et al. Vitamin D2 is as effective as Vitamin D3 in maintaining circulating concentrations of 25-hydroxyvitamin D. J Clin. Endocrinol Metab. 2008;93:677-81.
67. Gordon CM, Williams AL, Feldman HA, et al. Treatment of hypovitaminosis D in infants and toddlers. J Clin Endocrinol Metab. 2008;93(7):2716-21.
68. Malabanan A, Veronikis IE, Holick MF. Redefining vitamin D insufficiency. Lancet. 1998;351:805-6.
69. Pietras SM, Obayan BK, Cai MH, et al. Vitamin D2 treatment for vitamin D deficiency and insufficiency for up to 6 years. Arch Intern Med. 2009;169:1806-8.
70. Heaney RP, Davies KM, Chen TC, et al. Human serum 25-hydroxycholecalciferol response to extended oral dosing with cholecalciferol. Am J Clin Nutr. 2003;77:204-10.
71. Holick MF, Chen TC, Sauter E. Vitamin D and skin physiology: A D-lightful story. J Bone Miner Res. 2007; 22 Suppl 2:V28-33.
72. Kennedy C, Bajdik CD, Willemze R, et al. The influence of painful sunburns and lifetime of sun exposure on the risk of actinic keratoses, seborrheic warts, melanocytic nevi, atypical nevi, and skin cancer. J Invest Dermatol. 2003;120(6):1087-93.