chapter 9 - acs i & ii
TRANSCRIPT
BASE HOSPITAL GROUPONTARIO
Chapter 9 for 12 Lead Training
- Acute Coronary Syndromes – I & II-
Ontario Base Hospital GroupEducation Subcommittee
2008
TIME IS MUSCLE

OBHG Education Subcommittee
Acute Coronary Syndromes – I & II
REVIEWERS/CONTRIBUTORS
Neil Freckleton, AEMCA, ACPHamilton Base Hospital
Jim Scott, AEMCA, PCPSault Area Hospital
Ed Ouston, AEMCA, ACPOttawa Base Hospital
Laura McCleary, AEMCA, ACPSOCPC
Tim Dodd, AEMCA, ACPHamilton Base Hospital
Dr. Rick Verbeek, Medical DirectorSOCPC2008 Ontario Base Hospital Group
AUTHOR
Greg Soto, BEd, BA, ACPNiagara Base Hospital
OBHG Education Subcommittee
Chapter 9 Objectives
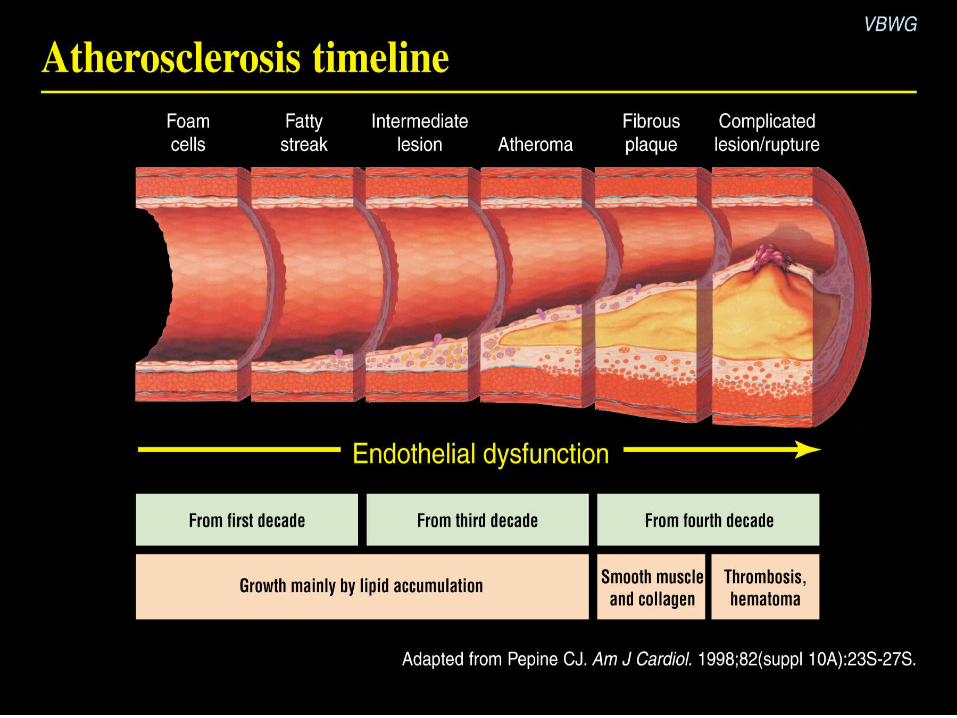
Define ACSDescribe the timeline for atherosclerosis
and thrombus formation in ACSList the 3 initiating events in an ACSDifferentiate stable and vulnerable
plagues.

OBHG Education Subcommittee
Chapter 9 Objectives
Describe the process of thrombus formation
List and differentiate the 3 I’s of ACSDescribe the myocardial coronary blood
supplyName the major coronary arteries and
locations they serve

BASE HOSPITAL GROUPONTARIO
Acute Coronary Syndromes I
Pathophysiology and Anatomy

OBHG Education Subcommittee
Acute Coronary Syndromes
Definition:Sudden ischemic disorders of the
heartInclude unstable angina and acute
myocardial infarctionRepresent a continuum of a similar
disease process
OBHG Education Subcommittee
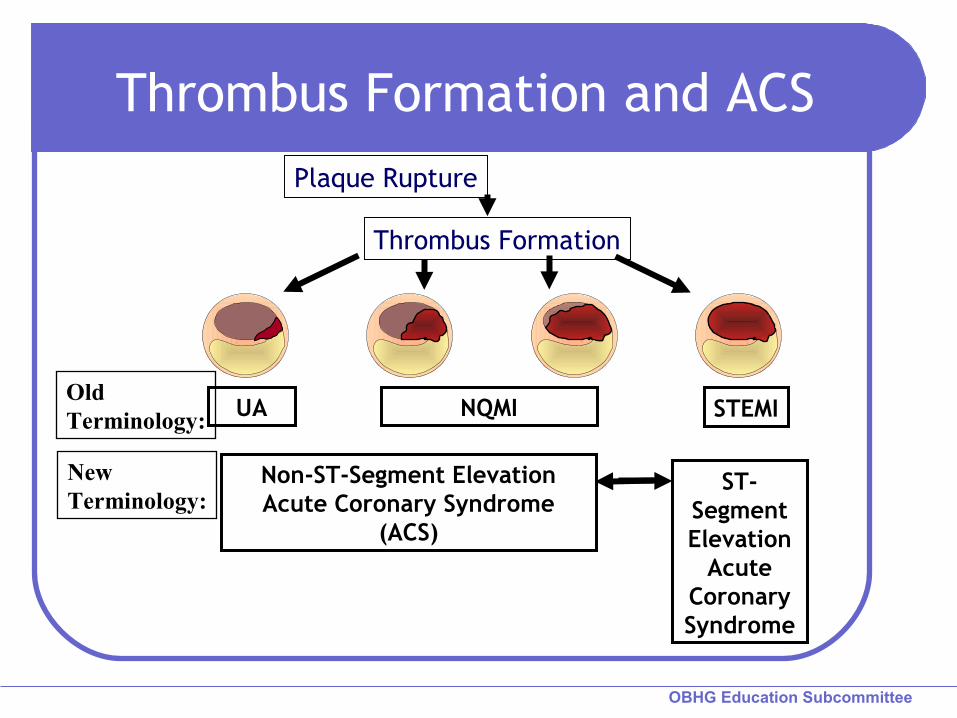
Thrombus Formation and ACS
UA NQMI STEMI
Plaque Rupture
Thrombus Formation
Non-ST-Segment Elevation Acute Coronary Syndrome
(ACS)
ST-Segment Elevation
Acute Coronary Syndrome
Old Terminology:
NewTerminology:
OBHG Education Subcommittee

OBHG Education Subcommittee
Acute Coronary Syndromes
All have sudden ischemia
Often can not be differentiated in the first hours
All have the same initiating events

OBHG Education Subcommittee
Initiating Events
Plaque rupture
Thrombus formation
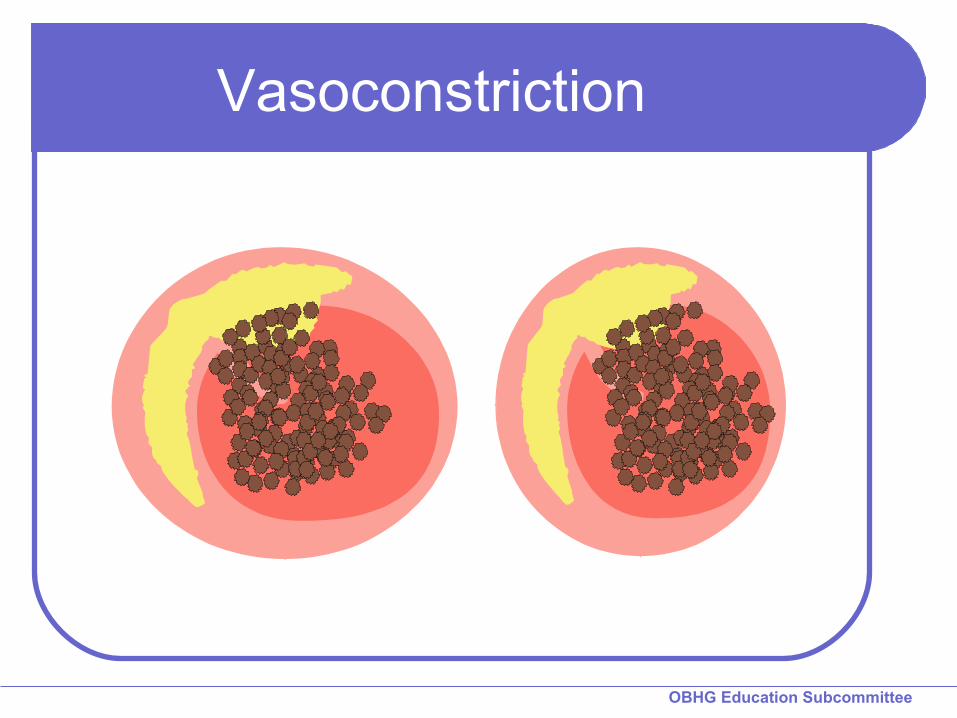
Vasoconstriction

OBHG Education Subcommittee
Lumen
Plaque Rupture
Lipid Core
Fibrous Cap
Stable Vulnerable
LumenLipid Core
Fibrous Cap

OBHG Education Subcommittee
Plaque Rupture
Lipid Core
Fibrous Cap
Lumen
OBHG Education Subcommittee
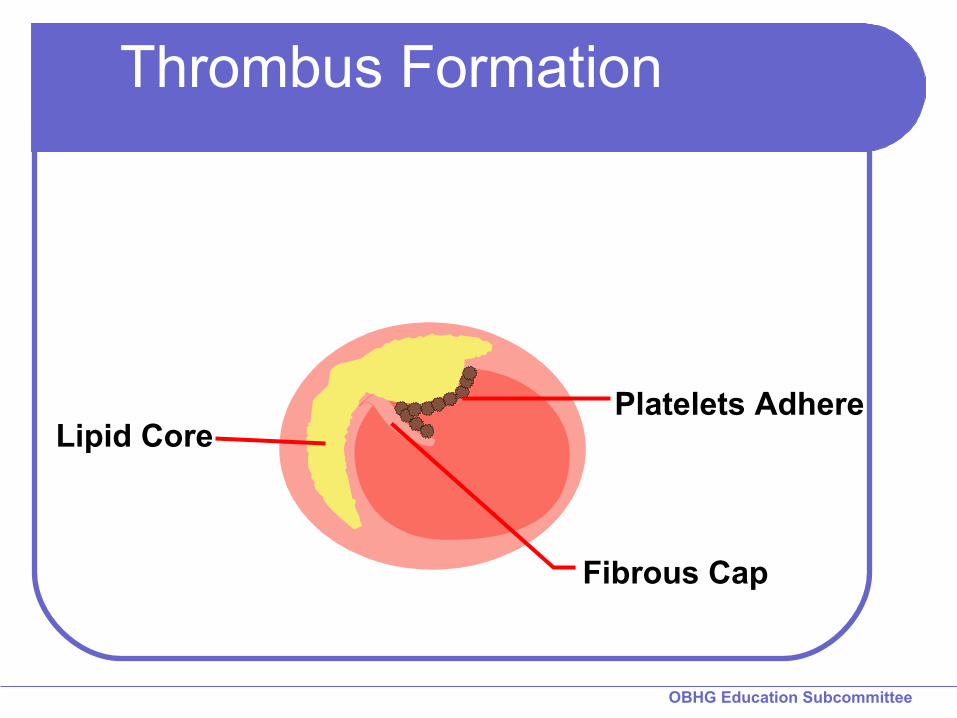
Thrombus Formation
Lipid Core
Fibrous Cap
Platelets Adhere
OBHG Education Subcommittee
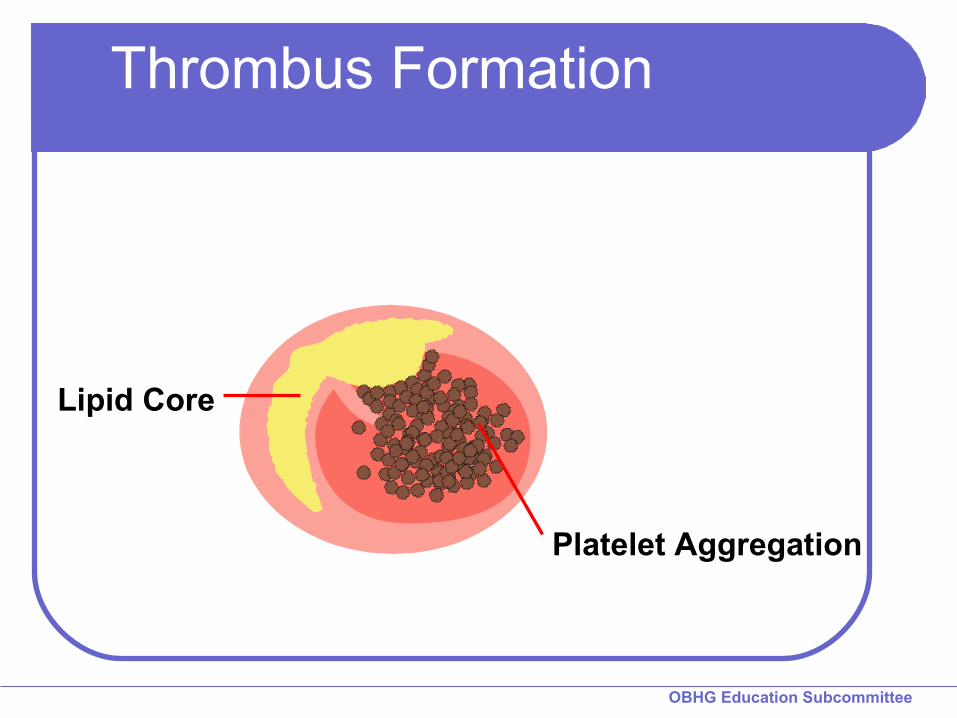
Thrombus Formation
Platelet Aggregation
Lipid Core

OBHG Education Subcommittee
Thrombus Formation
Platelet Aggregation
Lipid Core

OBHG Education Subcommittee
Thrombus Formation
Platelet Aggregation
Lipid Core
Fibrin
OBHG Education Subcommittee
Vasoconstriction

OBHG Education Subcommittee
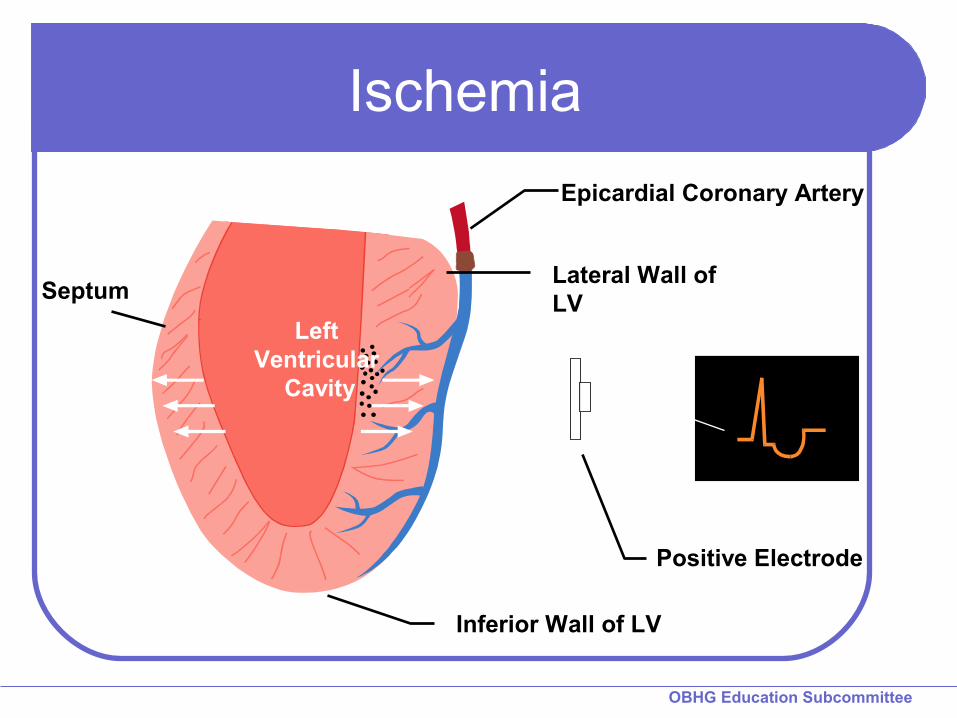
Epicardial Coronary Artery
Lateral Wall of LV
Positive Electrode
Septum
Left Ventricular
Cavity
Inferior Wall of LV
Well Perfused Myocardium

OBHG Education Subcommittee
Normal ECG
OBHG Education Subcommittee
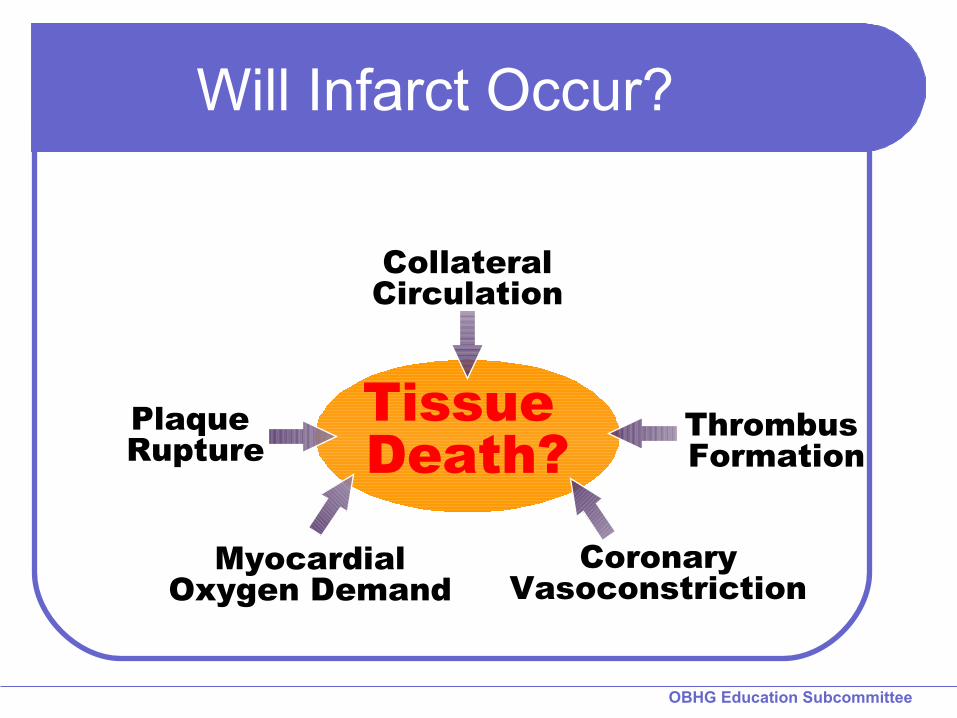
Will Infarct Occur?
Tissue Death?
Plaque Rupture
Thrombus Formation
CoronaryVasoconstriction
CollateralCirculation
MyocardialOxygen Demand

OBHG Education Subcommittee
The Three I’s of ACS
Ischemia - permanent damage avoidable lack of oxygenationST depression or T wave inversion
Injury - permanent damage avoidableprolonged ischemiaST elevation
Infarctdeath of myocardial tissuemay have Q wave

OBHG Education Subcommittee
Evolution of AMI
A - pre-infarct
B - Tall T wave
C - Tall T wave & ST elevation
D - Elevated ST, inverted T wave, Q wave
E - Inverted T wave, Q wave
F - Q wave
OBHG Education Subcommittee
Epicardial Coronary Artery
Lateral Wall of LV
Positive Electrode
Septum
Left Ventricular
Cavity
Inferior Wall of LV
Ischemia
OBHG Education Subcommittee
Ischemia
Inadequate oxygen to tissue
Subendocardial
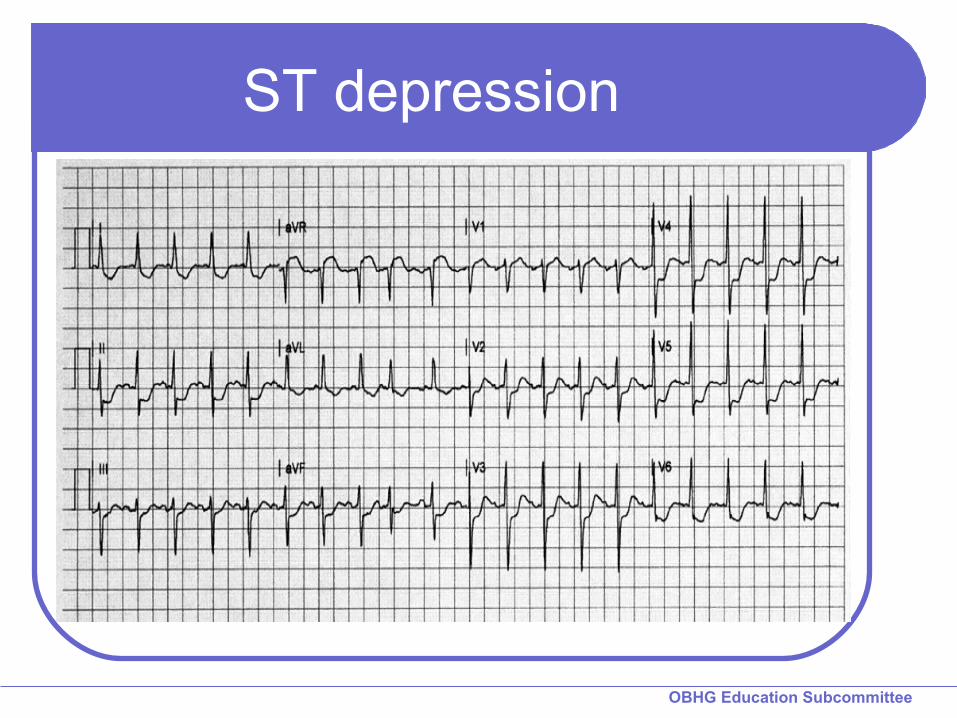
Represented by ST depression or T inversion
May or may not result in infarct
OBHG Education Subcommittee
ST depression
OBHG Education Subcommittee
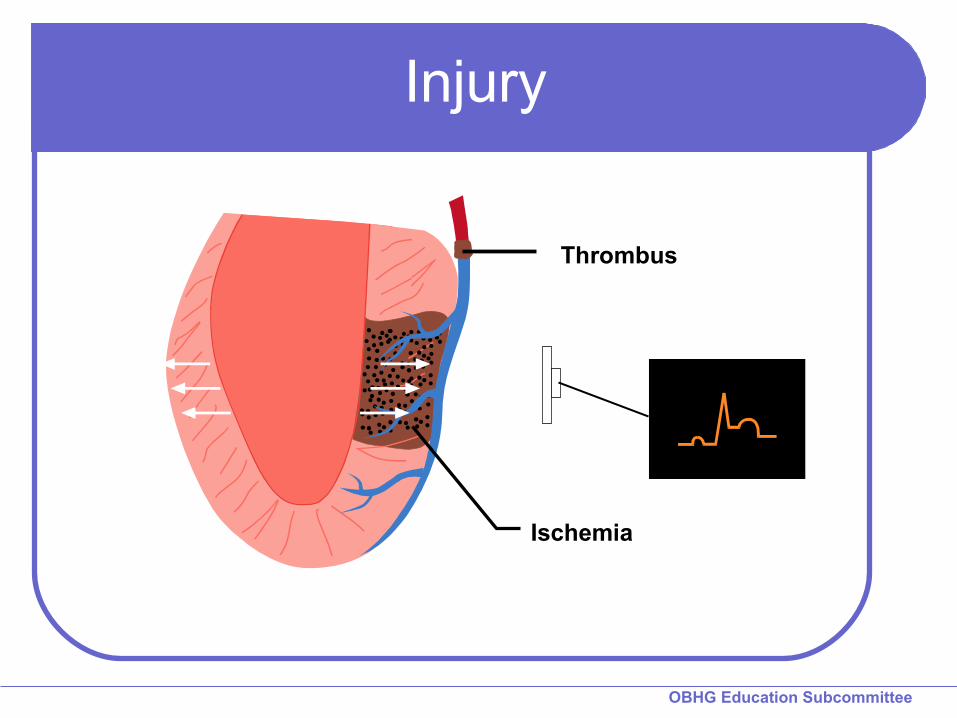
Thrombus
Ischemia
Injury

OBHG Education Subcommittee
Injury
Prolonged ischemia
Transmural
Represented by ST elevation
Usually results in infarct

OBHG Education Subcommittee
ST elevation

OBHG Education Subcommittee
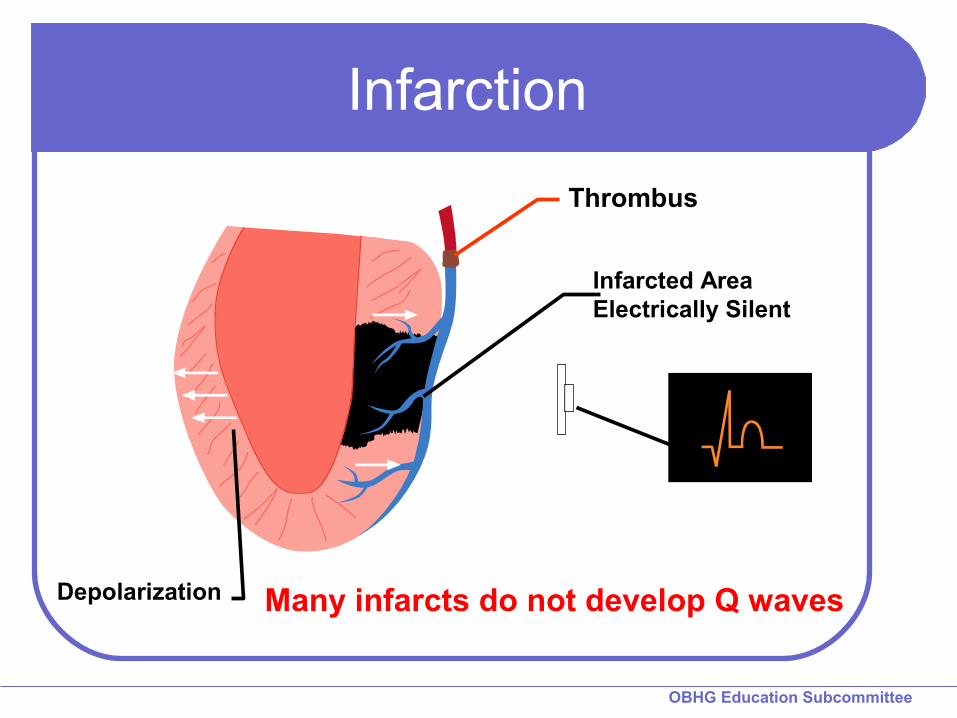
Infarct
Death of tissue
Represented by Q wave
Not all infarcts develop Q waves
OBHG Education Subcommittee
Infarcted AreaElectrically Silent
Depolarization Many infarcts do not develop Q waves
Infarction
Thrombus
OBHG Education Subcommittee
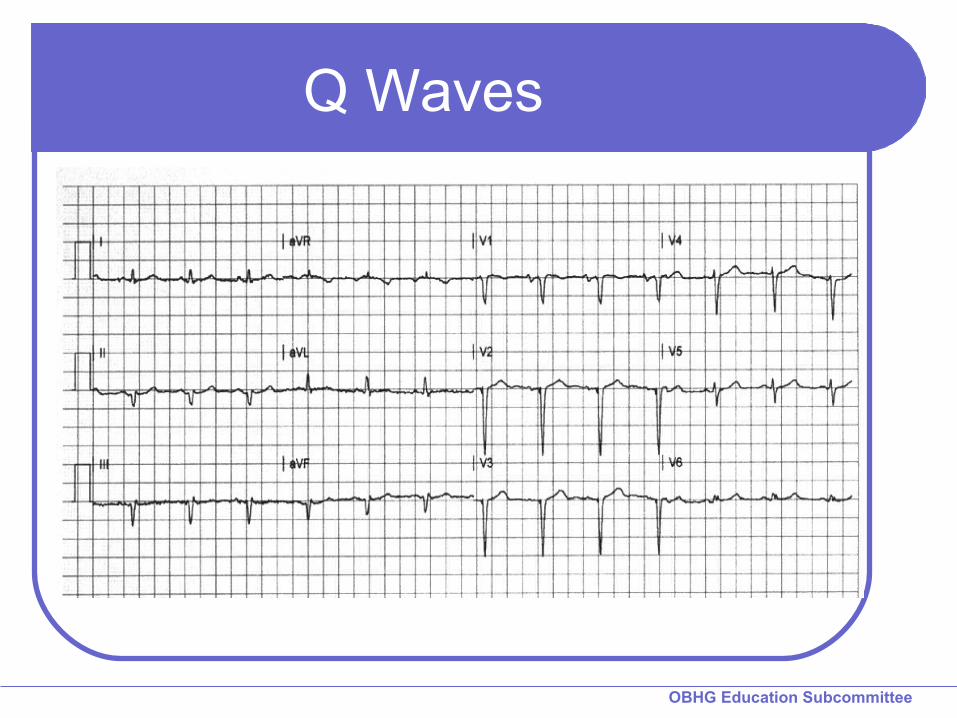
Q Waves

OBHG Education Subcommittee
Infarcted Area Electrically Silent
Thrombus
Depolarization
Ischemia
A bit of everything

OBHG Education Subcommittee
Summary
A normal ECG does NOT rule out ACSST segment depression represents
ischemia Possible infarct
ST segment elevation is evidence of AMI
Q wave MI may follow ST elevation or depression

OBHG Education Subcommittee
Coronary Arteries
Branch off of the aorta, just above the leaflets of the aortic valve
Three major arteries
Each supplies a specific area

OBHG Education Subcommittee
Right Coronary Artery
Inferior wall of LV Right ventricle Posterior LV Posterior fascicle of
LBB SA and AV node
OBHG Education Subcommittee
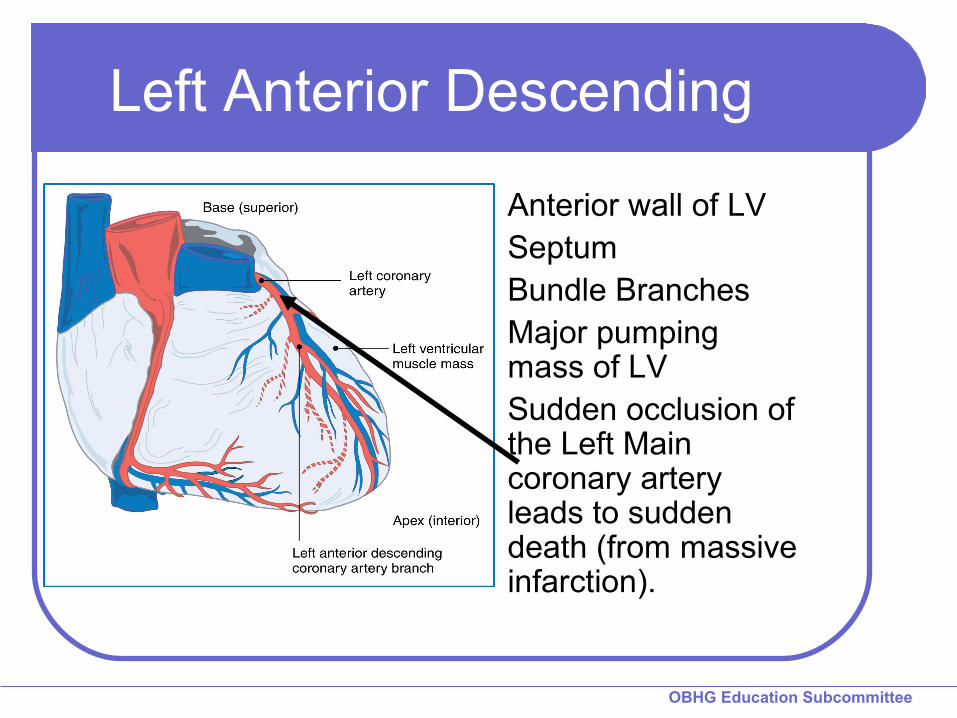
Left Anterior Descending
Anterior wall of LV Septum Bundle Branches Major pumping
mass of LV Sudden occlusion of
the Left Main coronary artery leads to sudden death (from massive infarction).

OBHG Education Subcommittee
Left Circumflex ArteryUpper lateral wall
of LV (Leads I and aVL)
SA node in 45%AV node in 10%Posterior fascicle
of LBB
BASE HOSPITAL GROUPONTARIO
QUESTIONS?

BASE HOSPITAL GROUPONTARIO
Acute Coronary Syndromes II
Rapid Recognition and
Treatment of ACS

OBHG Education Subcommittee
Goal for ACS II
Rapidly recognize and treat patients with sudden myocardial ischemia

OBHG Education Subcommittee
Small Group Task
List and rank risk factors
Describe symptoms of the last AMI patient attended
Describe the symptoms of a friend or relative when they suffered an AMI
OBHG Education Subcommittee
Immediate Evaluation
O2, Cardiac monitor, SPO2
Incident history
Risk factors
Treatment?
12 Lead ECG
OBHG Education Subcommittee
Clinical Presentations of ACS
Classic ischemic chest pain
Atypical chest pain
Ischemic equivalents
OBHG Education Subcommittee
Classic Anginal Chest Pain
Central anterior chest
Dull, fullness, pressure, tightness, crushing
Radiates to arms, neck, back

OBHG Education Subcommittee
Atypical Pain
Musculoskeletal, positional or pleuritic features
Often unilateral
May be described as sharp or stabbing
Includes epigastric discomfort
Females often express atypical pain

OBHG Education Subcommittee
Ischemic Equivalents
Dyspnea
Palpitations
Generalized weakness
Dizziness
Syncope or pre-syncope
OBHG Education Subcommittee
Who do you wanna be? A case in point about syncope and AMI60 yr old ♂; CC= syncope alone at home
am; awoke feeling well1000: bilateral shoulder pain; pt thought it
due to new exercise programWent to mall, returned home, had 4 drinks
and laid on couch.Had syncopal episode at 1530 while rising
from couch; hit forehead on floor → laceration.
Pt activated EMS at 15:40 hours
OBHG Education Subcommittee
EMS encounter1550: Found by crew sitting on couch,
CAOx3 O/E: skin = pink, warm, dry; P = 80 NSR,
BP=110/68, spo2=96% on room air, PEARL; airway patent, denied headache, minor ½” lac + hematoma to forehead, denied chest pain or SOB
Pmhx: smoker, ↑BP, ↑cholesterolCurrently ASYMPTOMATICResistant to 12 LECG but agreed if crew
would then leave him at home…
OBHG Education Subcommittee
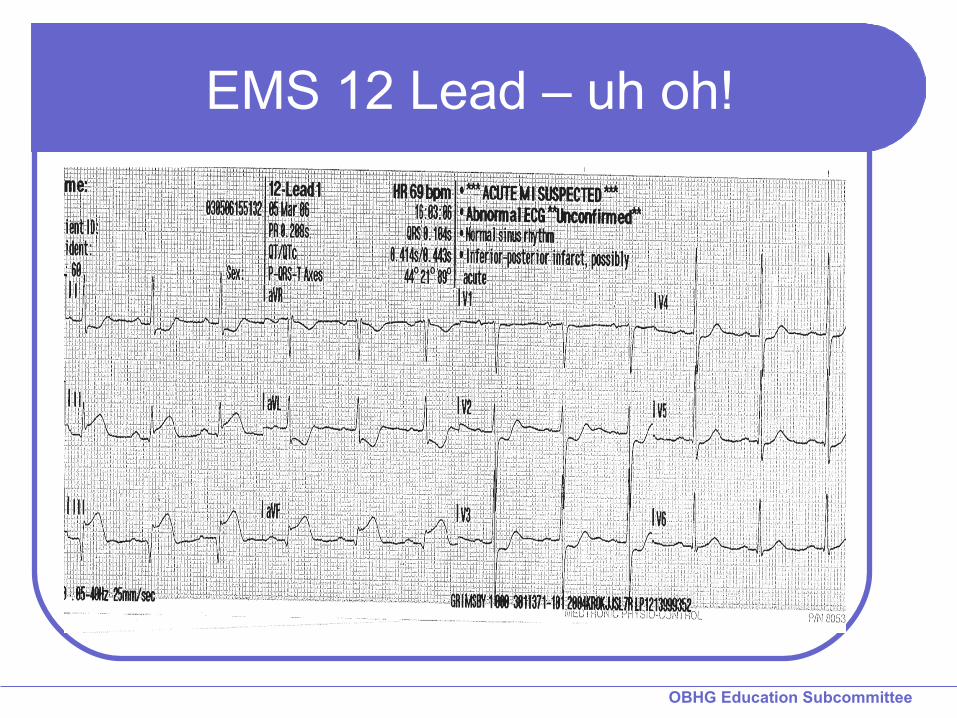
EMS 12 Lead – uh oh!

OBHG Education Subcommittee
Still don’t want to go? Patient stated he felt fine and was reluctant of
further assessment/care; refused treatment or transport.
Crew encouraged patient to go to hospital and explained 12 Lead ECG findings and risks associated with STEMI.
BHP Patch for advice – pt still refused. ACP told patient the story of her parents who each
had an AMI Dad: no treatment for ischemic chest pain, late
ED presentation, no reperfusion therapy; despite quad bypass he experienced CHF & poor quality of life until he died prematurely.
OBHG Education Subcommittee
So who do you wanna be?Mom: had sudden onset of chest pain in the
presence of daughter (the ACP)Received early ED thrombolysisSuccessful reperfusion and is now living active
and fulfilling life (travelling, exercise, boyfriends)Medic asked the patient: “So who do you
wanna be…my dad or my mom?”The patient enthusiastically sided with the Mom.Patient reperfused (PCI) with an excellent
outcome and good left ventricle ejection fraction (>60%)
OBHG Education Subcommittee
Atypical Presentations
Often seen in:
FemaleDiabeticsElderly
OBHG Education Subcommittee
Reasons EMS were missing ACS treatment
Protocols get in the way 50% of AMI patients have classic
chest pain presentation 20% of AMI patients have atypical
pain presentation 30% don’t have any pain at all
If we focus assessment on classic ischemic presentation we miss half of AMI patients!

OBHG Education Subcommittee
Important Notation
Note EXACT time symptoms began
Duration of symptoms may effect therapeutic options and destination decisions

OBHG Education Subcommittee
Review Group Activity
How many had presentations with classic anginal pain?
How many had atypical pain?
How many were anginal equivalents?
How many risk factors did you list?

OBHG Education Subcommittee
Risk Factors of ACS
DiabetesSmokingHypertensionAge Cholesterol
Family history of CAD
ObesityStressSedentary

OBHG Education Subcommittee
Consider Risk FactorsPatients with severe or multiple risk
factors should be evaluated with a high index of suspicion for acute coronary syndrome
Don’t let the patient get burnedGet the 12 Lead!
OBHG Education Subcommittee
Age
Infarct can occur at any age
Increasing age = increasing risk
OBHG Education Subcommittee
Remember!!
Unstable angina and acute myocardial infarction are indistinguishable in the first few hours
“Atypical” presentations are common
Risk factor evaluation helps identify ACS patients
OBHG Education Subcommittee
Chronic Stable Angina vs. ACS
Not chronic stable angina if… New onsetLower exertion threshold Change in pattern of reliefNew or different associated
symptoms
OBHG Education Subcommittee
PCP General Therapy for ACS
AssessmentMonitor Lead II ECG & SP02
Vital signsStory and risksExpose & listen to the chest
12 Lead Acquisition*
TreatmentOxygenNTGAspirinIV if certified
OBHG Education Subcommittee
ACP General Therapy for ACS
AssessmentMonitor Lead II ECG & SP02
Vital signsStory and risksExpose & listen to the chest
12 Lead Acquisition*
TreatmentOxygenNTGAspirinIVMorphine
OBHG Education Subcommittee
Note from previous two slides
BLS and ALS Standards currently do not include 12 Lead as a standard of care.
12 Lead is an Auxiliary Medical Directive for ACP and PCPDecision to proceed is based upon the
cooperative effort and decisions by the Base Hospital and Service Operator
OBHG Education Subcommittee
General Therapy for ACS
Assessment and therapy occur simultaneously
Findings may alter therapeutic path
OBHG Education Subcommittee
Oxygen
High flow mask is indicated if ischemia is suspected
Advanced airway care for continued or severe hypoxia where indicated
OBHG Education Subcommittee
Vital Signs
Respiratory rate and effortPulse rate, rhythm, volumeBlood pressure in both arms,
manual then automaticCardiac monitor SP02 monitor
12 Lead ECG

OBHG Education Subcommittee
12 Lead ECG
Obtain after the first set of vital signs
Repeat as often as necessary (enroute to hospital)
OBHG Education Subcommittee
IV Access
Adequate line in a suitable vein
Follow approved Medical Directives

OBHG Education Subcommittee
Aspirin
ASA - chew & swallowAdhere to Medical Directive for
contraindications to ASAIssues:
Asthma patients may have been told to avoid ASA
Patients on anti-coagulantsTaken ASA already today

OBHG Education Subcommittee
Nitroglycerin
Dilates conduit arteries
Antagonizes vasospasm
Improves collateral circulation
Inhibits venous return
Reduces intra-myocardial wall tension

OBHG Education Subcommittee
Nitroglycerin
NTG sublingual Repeat every five minutes as per
Medical Directive
Contraindications include; Hypotension ED Rx within 48 hours
Known hypersensitivity
Check MD

OBHG Education Subcommittee
NTG Precautions
Avoid hypotension
Limit systolic drop
Don’t use NTG as an analgesic
Watch for right ventricular infarction (RVI)

OBHG Education Subcommittee
Morphine
Morphine as per protocol May require several doses for adequate
relief of pain
Decreases myocardial oxygen requirements
Watch for respiratory depression and hypotension

OBHG Education Subcommittee
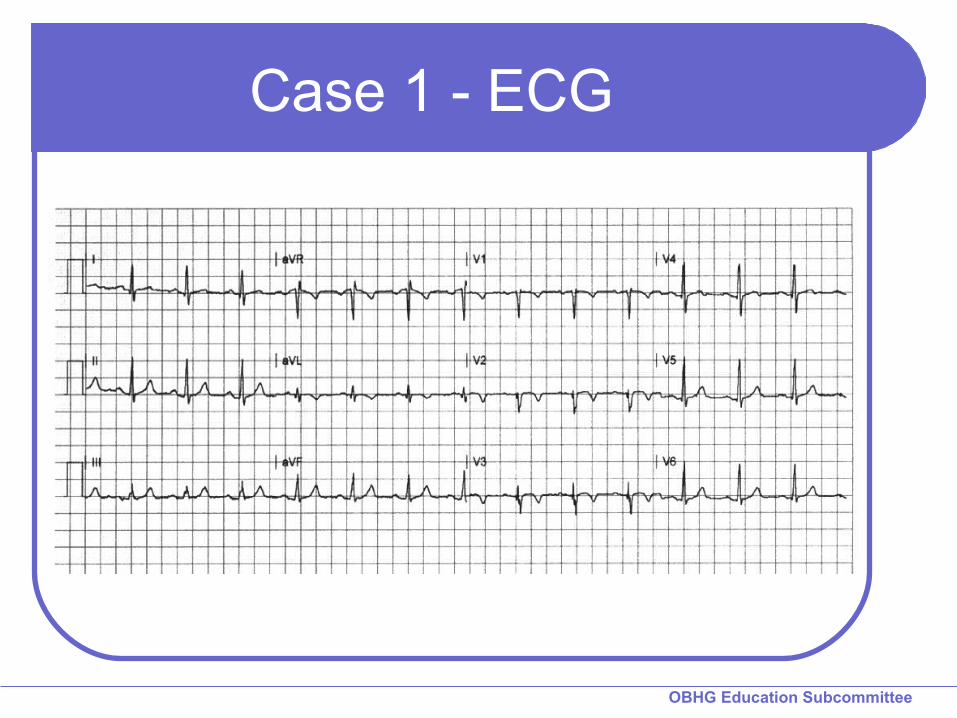
Case 1
48 year old male Sudden onset of dull central chest pain 2/10,
began at rest
Pale and wet
Overweight, smoker
Vital signs: RR 18, P 80, BP 180/110, Sa02 94% on room air

OBHG Education Subcommittee
Case 1
Incident Hx/Exam
Risk factors
Treatment
ECG
OBHG Education Subcommittee
Case 1 - ECG
OBHG Education Subcommittee
Case 268 year old female
Sudden onset of anxiety and restlessness,States she “can’t catch her breath”Denies chest pain or other discomfort
History of IDDM and hypertension
RR 22, P 110, BP 190/90, Sa02 88% on NRBM at 10 lpm.

OBHG Education Subcommittee
Case 2
Incident Hx/Exam
Risk factors
Treatment
ECG

OBHG Education Subcommittee
Case 2 - ECG

OBHG Education Subcommittee
Case 2
Now what is the order?StoryRisk factorsECGTreatment?
What is the pharmacological treatment plan for this patient?
Can you treat this patient under your medical directives?
OBHG Education Subcommittee
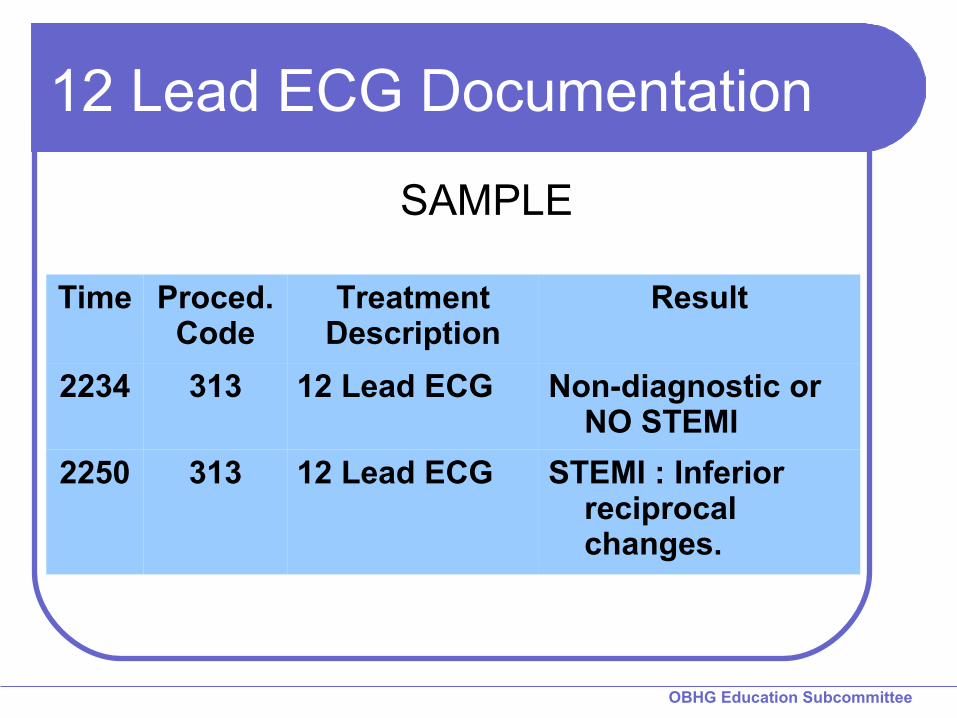
12 Lead ECG Documentation
Time Proced.Code
TreatmentDescription
Result
2234 313 12 Lead ECG Non-diagnostic or NO STEMI
2250 313 12 Lead ECG STEMI : Inferior reciprocal changes.
SAMPLE
OBHG Education Subcommittee
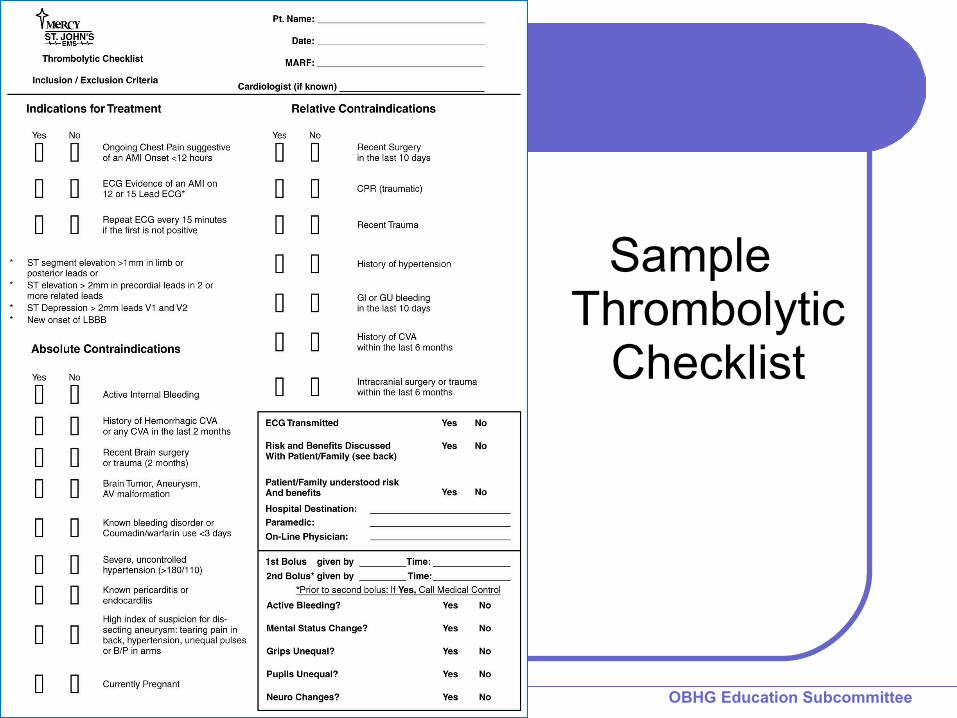
Sample Thrombolytic
Checklist
BASE HOSPITAL GROUPONTARIO
QUESTIONS?
BASE HOSPITAL GROUPONTARIO
Well Done!
Education Subcommittee
START QUIT