chapter 5 health and physical development. learning objectives how is development of the endocrine...
TRANSCRIPT
CHAPTER 5HEALTH AND PHYSICAL DEVELOPMENT

Learning Objectives
• How is development of the endocrine system involved in growth across the lifespan?
• How do the brain and the nervous system develop across the lifespan?
• What are milestones in the development of the brain?

Building Blocks of Growth and Development
• Human growth is influenced by the interaction of genetic and environmental factors
– Inherit a genetic propensity for height (tall, short, medium), but the propensity is affected by environmental influence of nutrition (adequate or inadequate)

Building Blocks of Growth and Development – The Endocrine System
• Endocrine glands secrete hormones directly into the bloodstream
– Pituitary gland is the master endocrine gland and triggers the release of hormones from all other endocrine glands
• Pituitary produces growth hormone
– Thyroid gland influences physical growth and development of the central nervous system
• Thyroid deficiency can affect intellectual development and growth

Building Blocks of Growth and Development – The Endocrine System
• Androgens (including testosterone)– Influence the growth spurt, responsible for
development of male sex organs, contribute to sexual motivation
• Estrogen– Influences the growth spurt, responsible for
development of breasts, pubic hair, and female sex organs, controls the menstrual cycle
• Progesterone – the “pregnancy hormone”– Orchestrates changes that allow conception and then
supports pregnancy
• Adrenal glands secrete androgen-like hormones– Contribute to the maturation of bone and muscle and to
sexual motivation


Building Blocks of Growth and Development – The Nervous System
• Nervous system consists of the brain and spinal cord (central nervous system or CNS) and the body-wide neural tissue (peripheral nervous system)– Basic unit is the neuron
• Neurons have branching dendrites that receive signals from other neurons and a long axon that transmits electric signals to other neurons (or a muscle cell)
– Neuron-to-neuron connections are made at a synapse– Axons are covered in myelin, a fatty sheath
• Myelination begins prenatally and continues for many years
– Progressive myelination is responsible for aspects of development such as language, abstract thinking, concentration, and integration of thought and emotion

Caption: Parts of a neuron. (a) Although neurons differ in size and function, they all contain three main parts: the dendrites, which receive messages from adjacent neurons; the cell body; and the axon, which sends messages across the synapse to other neurons. (b) The formation of dendrites leading to new connections among existing neurons, as well as the myelination of neural pathways, accounts for much of the increase in brain weight during a baby’s first two years.

Building Blocks of Growth and Development – Brain Development
• Milestones of brain development
– At birth, the brain weighs 25% of its adult weight
– By age 2, the brain weighs 75% of its adult weight
– By age 5, the brain weighs 90% of its adult weight
• During early development, the brain has great plasticity, or responsiveness to experience
– Can be highly vulnerable to damage by teratogens
– Can often recover successfully from injuries
– The critical or sensitive period for brain development is during the late prenatal period and early infancy

Learning Objectives
• What is lateralization? How does it affect behavior
• How does the brain change with aging?
• What principles underlie growth?
• What are examples of each principle?
• How can we apply a lifespan developmental
approach to our understanding of health?

Brain Development
• Lateralization in brain development– The functions controlled by the two hemispheres diverge
• Typically, the left cerebral hemisphere controls the right side of the body
– Adept at the sequential processing needed for analytic reasoning and language processing; “thinking side” of the brain
• Typically, the right hemisphere controls the left side of the body – Skilled at the simultaneous processing needed for
understanding spatial information and for processing visual-motor information and the emotional content of information; the “emotional side” of the brain
– The hemispheres are connected by the neurons that make up the corpus callosum
• Signs of lateralization are evident at birth• Direction the head is turned, grasp reflex, hemispheric response to
speech sounds

Brain Development
• Brain development is never complete
– Evidence from research suggests that the brain is responsive to experience and capable of neurogenesis across the lifespan
• Process of generating new neurons

Brain Development
• As a result of gradual and relatively mild degeneration within the nervous system, the aging brain typically processes information more slowly than does a younger brain– Some loss of neurons, diminished functioning of neurons,
and changes to related tissues, such as myelin• Greatest loss in the areas that control sensory and
motor activities– Decrease in brain weight and volume– Transmission of signals by atrophied neurons is less
effective– Declines in levels of neurotransmitters– Formation of “senile plaques”– Reduced blood flow to the brain

Brain Development
• Plasticity and growth make up for degeneration in the brain until people are in their 70s and 80s
• A key to maintaining or improving performance in old age is to avoid the many diseases that can interfere with nervous system functioning
• Another key is to remain intellectually active

Building Blocks of Growth and Development - Principles of Growth
• Three principles that underlie growth– Cephalocaudal principle
• Head-to-tail direction– Proximodistal principle
• From the center outward to the extremities
– Orthogenic principle• Development starts globally and
undifferentiated and proceeds toward hierarchal integration and differentiation

Building Blocks of Growth and Development -
A Lifespan Developmental Model of Health• Health is a lifelong process
• Health is determined by both genetic and environmental influences
• Health is multidimensional
• Includes physical, mental, and social well-being, not merely the absence of disease or infirmity
• Changes in health involve both gains and losses
• Health occurs in a sociohistorical context
• Socioeconomic status is particularly important

Learning Objectives
• What is the typical pattern of growth during the first year of life?
• What is the difference between survival and primitive reflexes? What are examples of each type of reflex?
• What other capabilities do newborns have?• How do locomotion and manipulation of objects
evolve during infancy?• What factors influence the development of
infant’s’ motor skills?• What health issues should be considered during
the first two years of life?

The Infant – Rapid Growth
• Newborns typically weigh 7 to 7½ pounds and are about 20 inches long
• By age 2, are about half their eventual adult height and weigh 27-30 pounds on average
• Growth occurs in fits and starts and often is accompanied by irritability
• Infants whose overall weight gain outpaces gains in height are at risk of childhood obesity

The Infant – Newborn Capabilities
• Reflexes are unlearned, involuntary responses to stimuli• Survival reflexes are adaptive
• Examples: breathing, eye-blink, sucking• Primitive reflexes are less adaptive and
typically disappear in early infancy–Examples: Babinski reflex, grasping
reflex–Persistence of primitive reflexes can
suggest neurological problems


The Infant – Behavioral States
• Organized and individualized patterns of daily activity that suggest the baby is integrating biological, physiological, and psychosocial functions– Initial short sleep-wake cycles become more
predictable and stable between 3-6 months– Rapid eye movement (REM) sleep
• Newborns spend 50% of their sleep in REM• Infants older than 6 months spend 25-30%
of their sleep in REM• May be useful for regulating sensory
stimulation


The Infant – Locomotor Development
• Developmental norms• Average age of mastery
• Early motor development follows the cephalocaudal and proximodistal principles• Can sit before they can walk• The trunk is controlled before the arms and
legs• Gross motor skills are mastered before fine
motor skills
The Infant – Locomotor Development
• Early motor development also demonstrates the orthogenetic principle• An infant will make a global response
before a differentiated response
• Crawling may take many forms or may not occur
• Walking – a major milestone of about 1 year• A more mature nervous system, more
muscle, and a less top-heavy stature are necessary for walking

The Infant – Grasping and Reaching
• Progression from reflexive response to more voluntary, coordinated behavior
• Infants use an ulnar grasp with palm and fingers pressed together
• Between 6 and 12 months, reaching and grasping become more proficient• Adjusted to the characteristics of an object
• Pincer grasp is reliable by one year of age• Thumb and forefinger

The Infant – Motor Skills as Dynamic Action Systems
• Rhythmic stereotypies are performed before a new motor skill emerges• Repetitive movements such as rocking,
swaying, bouncing, mouthing objects, banging arms up and down
• Dynamic systems theory explains motor developments• A “self-organizing” process in which children
use the sensory feedback they receive when they try different movements to modify their motor behavior in adaptive ways

The Infant – Motor Skills as Dynamic Action Systems
• According to dynamic systems theory, when children learn to walk• The learning takes into account their
biomechanical properties and the characteristics of the environment they must navigate
• Nature (the child’s central nervous system) and nurture (sensory and motor experiences) are essential and integral
• Action and thought are integrated

The Infant – Health and Wellness
• Typical health issues of infancy• Health problems associated with
prematurity and low birth weight may persist• Complications of prematurity are second
leading cause of death; 1/3 of infant deaths
• Congenital malformations, including heart defects, spina bifida, Down syndrome, cleft palate, etc. are leading cause of death

The Infant – Health and Wellness
• Infant health has been dramatically improved by the administration of vaccinations against diphtheria, pertussis, polio, and measles• Socioeconomic status is a determinant of
access to healthcare and vaccinations
• Postnatal health is enhanced by well-baby healthcare to ensure that development is proceeding normally and by following recommendations for prevention of illness

Learning Objectives
• What are the typical patterns of growth and physical development in childhood?
• What factors influence children’s health?
• How can health be optimized during childhood?

The Child – Steady Growth
• From age 2 until puberty, children gain 2-3 inches in height and 5-6 pounds annually
• Cephalocaudal and proximodistal principles of growth continue to prevail
The Child – Physical Behavior
• Children learn to move capably in a changing environment
• By age 3, walk or run in a straight line
• By age 4, perform a different activity with each hand
• Kindergartners can integrate motor skills into a higher-level skill
• Motor skills are responsive to practice
• Boys are more skilled in throwing and kicking
• Girls are more skilled in hopping and in manual dexterity

The Child – Physical Behavior
• From age 3 to age 5, eye-hand coordination and control of small muscles improve
• By age 8 or 9, children can use tools such as a screwdriver and are skilled at games requiring eye-hand coordination
• Reaction time improves steadily throughout childhood

The Child – Health and Wellness
• Parents’ education and socioeconomic status are factors that influence children’s health
• Accidents are the leading cause of death during childhood• Motor vehicle crashes cause the most fatal
injuries
• Nutrition continues to contribute to health• Children need a well-balanced diet, but
societal influences inadvertently encourage poor eating habits

Caption: Among white and black families, parent’s education level influences the extent to which children’s activities are limited by poor or fair health. Children have more limitations when their parents are less educated. This is not true among Hispanic and Asian families.

The Child – Health and Wellness: Nutrition
• Parents can influence children’s nutrition by offering healthy foods and modeling healthy eating habits
• Schools influence children’s eating habits and health– Breakfast programs– School lunches often have higher than
recommended levels of fat and sodium and lower than recommended levels of fiber

The Child – Health and Wellness: Nutrition
• Regular physical activity fosters health during childhood• Children should have at least 60 minutes of
moderate or vigorous physical activity daily• The average child spends 5-6 hours in
sedentary activities each day
• Obesity rates have tripled over the past 30 years and are especially high among ethnic minority children• Obesity – being 20% or more above the ideal
weight for one’s height, age, and sex
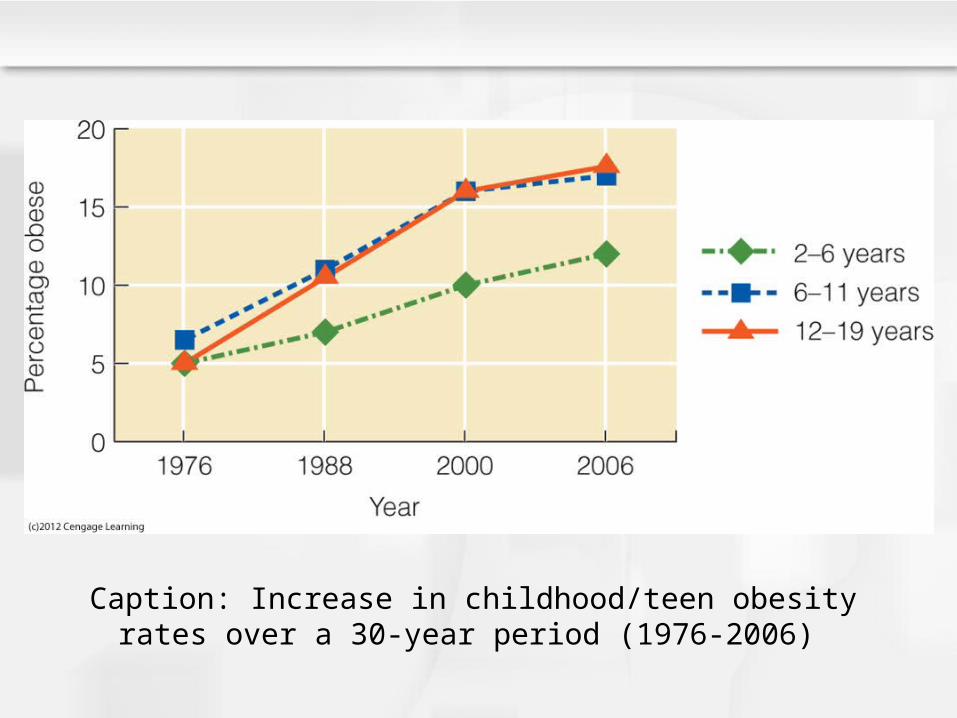
Caption: Increase in childhood/teen obesity rates over a 30-year period (1976-2006)
Learning Objectives
• What physical changes occur during adolescence?
• What factors contribute to sexual maturity of males and females?
• What psychological reactions accompany variations in growth spurt and the timing of puberty?

The Adolescent – The Growth Spurt
• The growth spurt is triggered by an increase in the level of growth hormones– Girls’ peak rates of growth
• For height – not quite 12 years of age • For weight – 12.5 years
– Boys’ peak rates of growth• For height – 13.4 years of age• For weight – 13.9 years
• Girls achieve adult height around 16; boys continue to grow until 18, 19, or 20

The Adolescent – Sexual Maturation
• Increased production of adrenal androgens (adrenarche) contributes to secondary sex characteristic of pubic/axillary hair
• Increased production of gonadal hormones primarily responsible for secondary sex characteristics and sexual maturation
• “Tanner Scale” used to measure progression through five stages of sexual maturity• Menarche is the most dramatic event in
girls’ sexual maturation process

The Adolescent – Sexual Maturation
• Girls’ sexual maturation is influenced by ethnicity, weight at birth, and weight gain during childhood
• The lighter a girl is at birth and the more weight she gains during childhood, the earlier she begins menstruating
• Boys’ sexual maturation process begins at age 11-11½ with growth of testes and scrotum
• The marker of sexual maturation for boys is semenarche, first emission of seminal fluid, around age 13

The Adolescent – Sexual Maturation
• The rate of development during adolescence is determined by– Genes that trigger production of hormones– Environment
• The secular trend– The historical trend in industrialized
societies toward earlier maturation and greater body size (caused by improved nutrition and advances in medical care)
– For girls, family situation • Presence of an unrelated male in the
household, family disruption, harsh mothering

Sexual Maturation – Psychological Implications
• Girls become concerned with appearance and worry about the responses of others– Individual reactions vary widely– May develop negative views about
menstruation and poor body images as a result of weight gain
• Boys are likely to welcome weight gain and voice changes and to react positively to semenarche

Sexual Maturation – Psychological Implications
• Puberty typically prompts changes in family relations• Physical distancing is typical• Teens may become more independent and
less close to parents• Conflict is likely but about minor issues• Family relations will be influenced by cultural
beliefs about the significance of becoming an adult
• Parents can facilitate the adjustment to puberty by maintaining close relationships and helping adolescents accept themselves

Sexual Maturation – Early versus Late Development
• Early development for boys • Advantages – judged to be socially
competent, attractive, and self-assured• Disadvantages – increased risk of earlier
involvement in substance use and problem behaviors such as bullying, delinquency
• Late maturation in boys • More negative effects – more anxious, less
sure of themselves, more behavior and adjustment problems, lower achievement test scores
• Positive effect – less likely to use alcohol

Sexual Maturation – Early versus Late Development
• Early development for females• More disadvantageous – subject of
ridicule; higher level of body dissatisfaction• Socialization with older peer group can
lead to dating, substance use, sexual activity.
• Girls who experience early puberty and early sex report higher levels of depression
• Late development for females• Advantage – good school performance• Disadvantage – some anxiety

Sexual Maturation – Early versus Late Development
• Late-maturing boys and early-maturing girls are especially likely to find adolescence to be disruptive
• Differences between early and late developers tend to fade with time
• Effects of timing of puberty depend upon the adolescent’s perception of whether puberty events are experienced early, on time, or late
• Reactions of peers and family members to an adolescent’s pubertal changes are instrumental in determining the adolescent’s adjustment

The Adolescent – Physical Behavior
• Dramatic physical growth makes teens more physically competent, stronger, than children
• Adolescents are less physically active than they should be
- Girls are more sedentary than boys
• Gender-role socialization may be partly responsible
• The male-female gap in physical performance among top athletes has narrowed

The Adolescent – Health and Wellness
• Many adolescents are strong, fit, and energetic, but 1/3 have poor physical fitness
• High blood pressure, cholesterol, and blood sugar put teens at risk for heart disease at earlier ages
• Heredity, poor eating habits, inactivity, and parent behaviors contribute to risk for obesity

The Adolescent – Health and Wellness
• The leading causes of death among teens are unintentional injuries and violence
- Injuries mostly from motor vehicles
- Violence associated with homicides and suicides
• Other health risks that originate in adolescence include alcohol and drug use and cigarette smoking

The Adolescent – Health and Wellness
• One of four high school students report occasional heavy or binge-drinking
• Risky choices associated with alcohol use include– More likely to smoke and to become addicted to
nicotine– More likely to engage in risky sexual behaviors– More likely to get into a car where the driver
has been drinking– More likely to get into fights, have academic
problems, and engage in illegal behaviors

Learning Objectives
• What physical changes occur during adulthood?
• What are the psychological implications of the physical changes that occur with aging?
• What health concerns arise as adults age?
• How can health of older adults be preserved?

The Adult
• The body of a mature adolescent or young adult is strong and fit– Its organs are functioning efficiently– Considered to be in peak health
• But physical aging occurs slowly and steadily over the lifespan

The Adult – Appearance and Physical Functioning
• Only minor changes in physical appearance the 20s and 30s
• Signs of aging are noticeable by the 40s
- Wrinkled skin, gray, thinning hair
- Extra weight or the “middle-aged spread” is associated with slower metabolism and insufficient physical exercise

The Adult – Appearance and Physical Functioning
• Health burdens of obesity include heart disease, type 2 diabetes, certain cancers, and stroke
• Healthcare cost of obesity in the U.S. is estimated at $147 billion
• Public health strategies for combating obesity– Promoting health foods and beverages– Discouraging consumption of
foods/beverages that add calories but not nutrition
– Increasing physical activity

The Adult – Appearance and Physical Functioning
• As people move into their 60s and beyond, they typically lose weight by losing muscle and bone
- Due to sedentary lifestyle
• Aging also involves a gradual decline in the efficiency of most bodily systems
• Handgrip strength in middle age is a good predictor of disability and ability to function in later life

The Adult – Appearance and Physical Functioning
• Individual differences in physiological functioning increase with age – measures vary widely among 70-year-olds– Not all older people have poor physiological
functioning
• Reserve capacity of many organ systems declines– Ability to respond to demands for extraordinary
output
• Older adults are often less fit than younger adults because they have less vigorous physical activity as they age
• Tire more quickly and need more time to recover

The Adult – Psychological Implications
• Aging occurs within the context of a society that values youth and devalues old age and the physical changes of aging
• Negative stereotypes about aging can lead to ageism– Prejudice against elderly people
• For aging individuals, the concern seems to be the ability to continue functioning at a desirable level

The Adult – Psychological Implications
• The majority of people age 65 and older say they are in excellent, very good, or good health– Whites are more likely to report good
health than are blacks or Hispanics– Relatively few older adults say they
assistance with daily activities• Most older people retain their sense of well-
being and their ability to function independently despite an increased likelihood of impairments

The Adult – The Reproductive System
• Sex hormones have psychological implications– Men’s testosterone levels fluctuate
annually and daily– Men with high levels of testosterone tend
to be more sexually active and aggressive
• Otherwise, no link to men’s moods or behavior

The Adult – The Reproductive System
• Sex hormones have psychological implications– Cyclical changes in women’s hormone
levels are associated with premenstrual syndrome (PMS)
• Bloating, moodiness, breast tenderness, headaches in the days before menstruation
• Debate about the validity of PMS

The Adult – Female Menopause
• The ending of menstrual periods is menopause
• The average age is 51 and the usual age range is 45-54
• Society holds stereotypic views of menopausal women
• Experiences include hot flashes, vaginal dryness
• Typically no effect upon anxiety, perceived stress, anger, or job satisfaction
• Women who experience severe psychological problems during the menstrual transition often had problems before menopause

The Adult – Female Menopause
• Until 2002, hormone replacement therapy (HRT; estrogen and progestin) was a remedy for hot flashes and vaginal dryness
• In 2002 a large study found that HRT was associated with increased risk for breast cancer, heart attack, and stroke
• Lifestyle choices such as exercising and getting adequate sleep may be the best options for women

The Adult – Male Andropause
• Andropause is characterized by decreasing levels of testosterone and symptoms such as– Low libido– Fatigue and lack of energy– Erection problems– Memory problems– Loss of pubic hair
• Men experience fewer psychological effects with andropause than women do with menopause

The Adult – Slowing Down
• Walking slows with age
• Motor actions – especially fine motor tasks requiring object manipulation – are performed more slowly and with less coordination
• Cognitive tests that require speedy answers are performed more slowly
• Slowing of the nervous system explains slowed motor and mental functioning
• Reaction times of older adults vary greatly
• Experience helps people compensate for a slower nervous system

The Adult – Disease, Disuse, or Abuse? • How to explain declines of physical
functioning across adulthood? – Research suggests that aging in the
absence of disease has little effect on physical and psychological functioning
– Disuse contributes to steeper declines in physical functioning in some adults more than others
– Abuse – excessive alcohol, high-fat diet, smoking – contributes to declines in functioning in some people
The Adult – Health and Wellness
• From childhood, acute illnesses become less frequent but chronic diseases/disorders become more common
• Many 70-and-older adults have at least one chronic impairment– Arthritis, hypertension
• Among those who are impoverished, health problems and difficulties in day-to-day functioning are more common and more severe

The Adult – Health and Wellness
• Staying healthy in older adulthood– Exercise improves cardiovascular and
respiratory functioning, slows bone loss, and strengthens muscles
– Exercise benefits mood and can enhance cognitive functioning
– Physical activity is associated with a lower incidence of depression among older adults
– Regular exercise by older adults is estimated to delay the onset of physical disabilities by up to 7 years

The Adult – Health and Wellness
• Osteoporosis (“porous bone”) – loss of minerals
– Results in fragile, easily fractured bones
– Nearly 1/3 of elderly adults who fracture a hip die within one year
– Hip fractures are a leading cause of nursing home admissions
– Osteoporosis can be prevented with a diet sufficient in calcium during youth and by weight-bearing exercises such as jogging or walking

The Adult – Health and Wellness
• Osteoarthritis– The most common joint problem among
older adults– Results from gradual deterioration of the
cartilage that cushions the bones from rubbing together
– Joint disease is deforming, painful, and cause limitations of activities

The Adult – Successful Aging
• Results from a nun study – the level of education affected longevity and health– Those with a college degree lived longer and
were more likely to remain independent– The risk of death among college-educated
nuns was lower at every age– Nuns who were physically and mentally active
lived longer and were healthier than less active nuns
– Higher language proficiency in adulthood predicted mental functioning in late life