changes to the medicines use review service pharmacy...1 changes to the medicines use review service...
TRANSCRIPT

1
CHANGES TO THE MEDICINES USE REVIEW SERVICE
Targeted Medicines Use Reviews The introduction of targeted Medicines Use Reviews (MURs) will better utilise the provision of this service and support the care of selected patient groups known to encounter medicine related problems. The current number of MURs is 400 per pharmacy and this figure will be retained: From December 2011 four national target groups will be introduced. In Wales these will be:
Patients taking antihypertensive medication; Patients taking medicines for respiratory disease; Patients taking high risk medicines; Patients prescribed a medicine no longer required.
At least 50% of all MURs undertaken in each pharmacy, each year must be with patients within the national target groups. As regards the financial year ending 31 March 2012, the pharmacy will need to ensure that at least 50% of MUR service consultations carried out on or after 1 December 2011 are with patients in one or more of the target groups. MURs will continue to be carried out with patients who are not within the target groups. Pharmacists will be able to provide the service to patients they consider will benefit from the MUR service. All patients who receive an MUR should experience the same level of service regardless of their condition. As now, MURs will cover all the patients’ medicines not just those falling within the target group(s). Target Group Specifications High risk medicines The medicines identified for the purpose of high risk targeted MURs are those listed in the chapters/sub-sections, detailed below, of the current edition of the British National Formulary.
BNF Reference BNF subsection descriptor
BNF 10.1.1 NSAIDs
BNF 2.8.2 Oral anticoagulants
BNF 2.9 Antiplatelets
BNF 2.2 Diuretics
Additionally the following specific medicines are identified for high risk targeted MUR.
BNF Reference BNF subsection descriptor
BNF 4.2.3 Lithium
BNF 10.1.3 Methotrexate
2
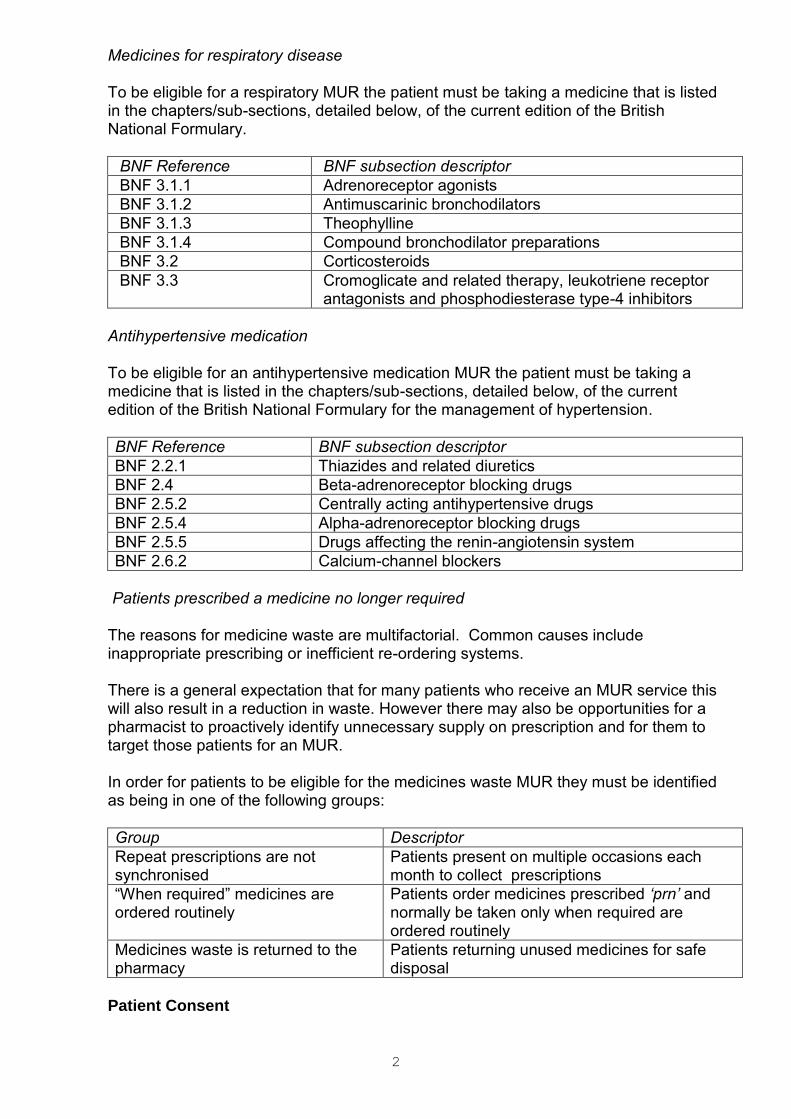
Medicines for respiratory disease To be eligible for a respiratory MUR the patient must be taking a medicine that is listed in the chapters/sub-sections, detailed below, of the current edition of the British National Formulary.
BNF Reference BNF subsection descriptor
BNF 3.1.1 Adrenoreceptor agonists
BNF 3.1.2 Antimuscarinic bronchodilators
BNF 3.1.3 Theophylline
BNF 3.1.4 Compound bronchodilator preparations
BNF 3.2 Corticosteroids
BNF 3.3 Cromoglicate and related therapy, leukotriene receptor antagonists and phosphodiesterase type-4 inhibitors
Antihypertensive medication To be eligible for an antihypertensive medication MUR the patient must be taking a medicine that is listed in the chapters/sub-sections, detailed below, of the current edition of the British National Formulary for the management of hypertension.
BNF Reference BNF subsection descriptor
BNF 2.2.1 Thiazides and related diuretics
BNF 2.4 Beta-adrenoreceptor blocking drugs
BNF 2.5.2 Centrally acting antihypertensive drugs
BNF 2.5.4 Alpha-adrenoreceptor blocking drugs
BNF 2.5.5 Drugs affecting the renin-angiotensin system
BNF 2.6.2 Calcium-channel blockers
Patients prescribed a medicine no longer required
The reasons for medicine waste are multifactorial. Common causes include inappropriate prescribing or inefficient re-ordering systems. There is a general expectation that for many patients who receive an MUR service this will also result in a reduction in waste. However there may also be opportunities for a pharmacist to proactively identify unnecessary supply on prescription and for them to target those patients for an MUR. In order for patients to be eligible for the medicines waste MUR they must be identified as being in one of the following groups:
Group Descriptor
Repeat prescriptions are not synchronised
Patients present on multiple occasions each month to collect prescriptions
“When required” medicines are ordered routinely
Patients order medicines prescribed ‘prn’ and normally be taken only when required are ordered routinely
Medicines waste is returned to the pharmacy
Patients returning unused medicines for safe disposal
Patient Consent

3
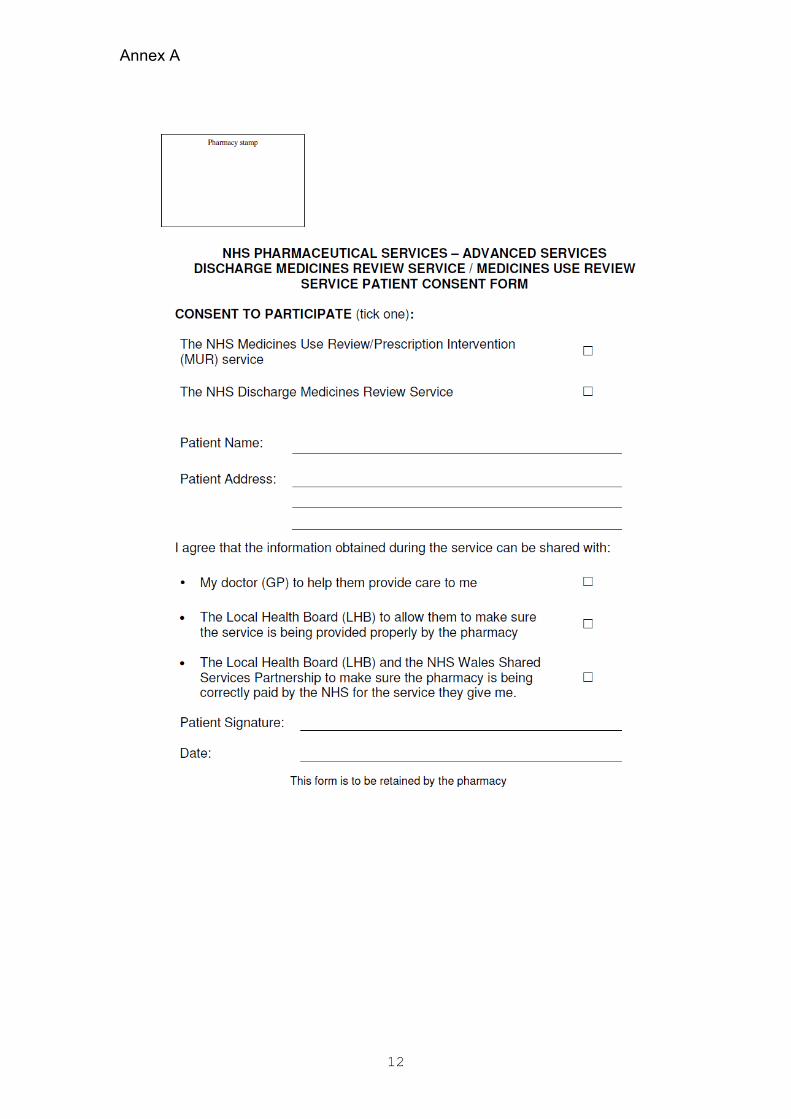
From December 2011 patients who receive an MUR must give signed consent to share the MUR record form with their GP, the LHB and the NHS Shared Services Partnership. This is an anti-fraud measure designed to provide assurance to NHS Wales that MUR services are being provided appropriately. If a patient does not consent to their MUR record form being shared then they will not normally be able to access the service other than in exceptional circumstances. Pharmacies will need to maintain a record of patient consent for each MUR service consultation completed. The record should be retained for at least 2 years from the date of the MUR service consultation. Suggested wording for patient consent forms is included at Annex A. Patient Eligibility As now the MUR service comprises structured adherence-centred reviews with patients on multiple medicines, particularly those receiving medicines for long term conditions. MURs must only be carried out with patients taking two or more medicines the only exception to this is when a patient is prescribed a high risk medicine (i.e. a medicine in the national list of high risk medicines).
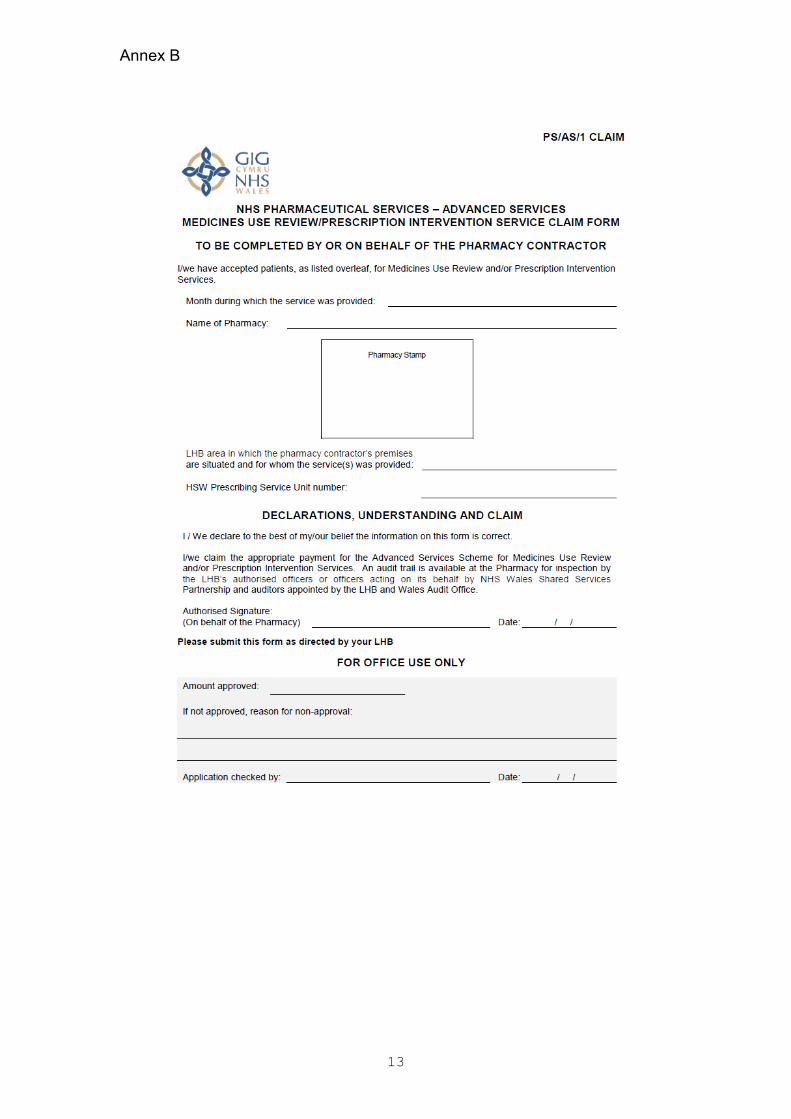
Claim Form The current MUR form has been revised and is included at Annex B. Pharmacy contractors are advised to use the revised form with immediate effect and in any case for all claims for MUR services provided on or after December 1, 2011. After December 1, 2011 any claim made using the current form will be returned to contractors without payment for resubmission. Further information and copies of all revised paperwork related to the MUR service can be accessed at: http://www.wales.nhs.uk/sites3/page.cfm?orgid=498&pid=7551
4
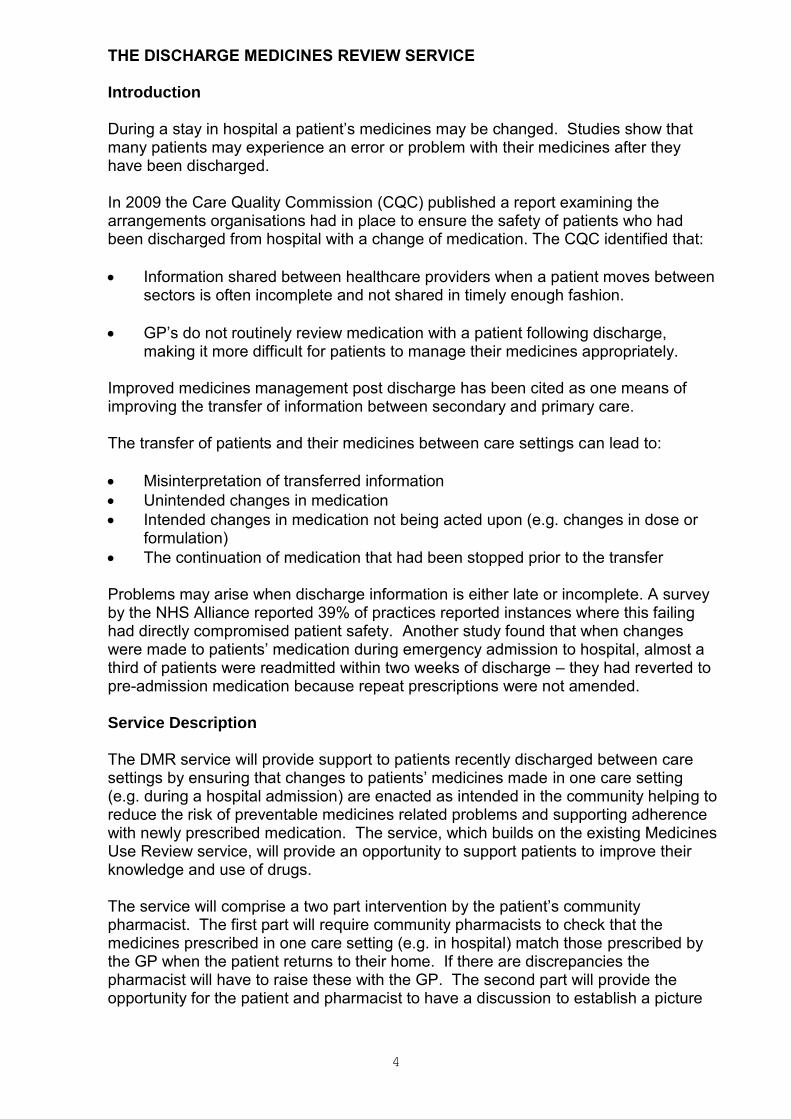
THE DISCHARGE MEDICINES REVIEW SERVICE
Introduction During a stay in hospital a patient’s medicines may be changed. Studies show that many patients may experience an error or problem with their medicines after they have been discharged. In 2009 the Care Quality Commission (CQC) published a report examining the arrangements organisations had in place to ensure the safety of patients who had been discharged from hospital with a change of medication. The CQC identified that:
Information shared between healthcare providers when a patient moves between sectors is often incomplete and not shared in timely enough fashion.
GP’s do not routinely review medication with a patient following discharge, making it more difficult for patients to manage their medicines appropriately.
Improved medicines management post discharge has been cited as one means of improving the transfer of information between secondary and primary care. The transfer of patients and their medicines between care settings can lead to:
Misinterpretation of transferred information
Unintended changes in medication
Intended changes in medication not being acted upon (e.g. changes in dose or formulation)
The continuation of medication that had been stopped prior to the transfer Problems may arise when discharge information is either late or incomplete. A survey by the NHS Alliance reported 39% of practices reported instances where this failing had directly compromised patient safety. Another study found that when changes were made to patients’ medication during emergency admission to hospital, almost a third of patients were readmitted within two weeks of discharge – they had reverted to pre-admission medication because repeat prescriptions were not amended.
Service Description
The DMR service will provide support to patients recently discharged between care settings by ensuring that changes to patients’ medicines made in one care setting (e.g. during a hospital admission) are enacted as intended in the community helping to reduce the risk of preventable medicines related problems and supporting adherence with newly prescribed medication. The service, which builds on the existing Medicines Use Review service, will provide an opportunity to support patients to improve their knowledge and use of drugs. The service will comprise a two part intervention by the patient’s community pharmacist. The first part will require community pharmacists to check that the medicines prescribed in one care setting (e.g. in hospital) match those prescribed by the GP when the patient returns to their home. If there are discrepancies the pharmacist will have to raise these with the GP. The second part will provide the opportunity for the patient and pharmacist to have a discussion to establish a picture
5
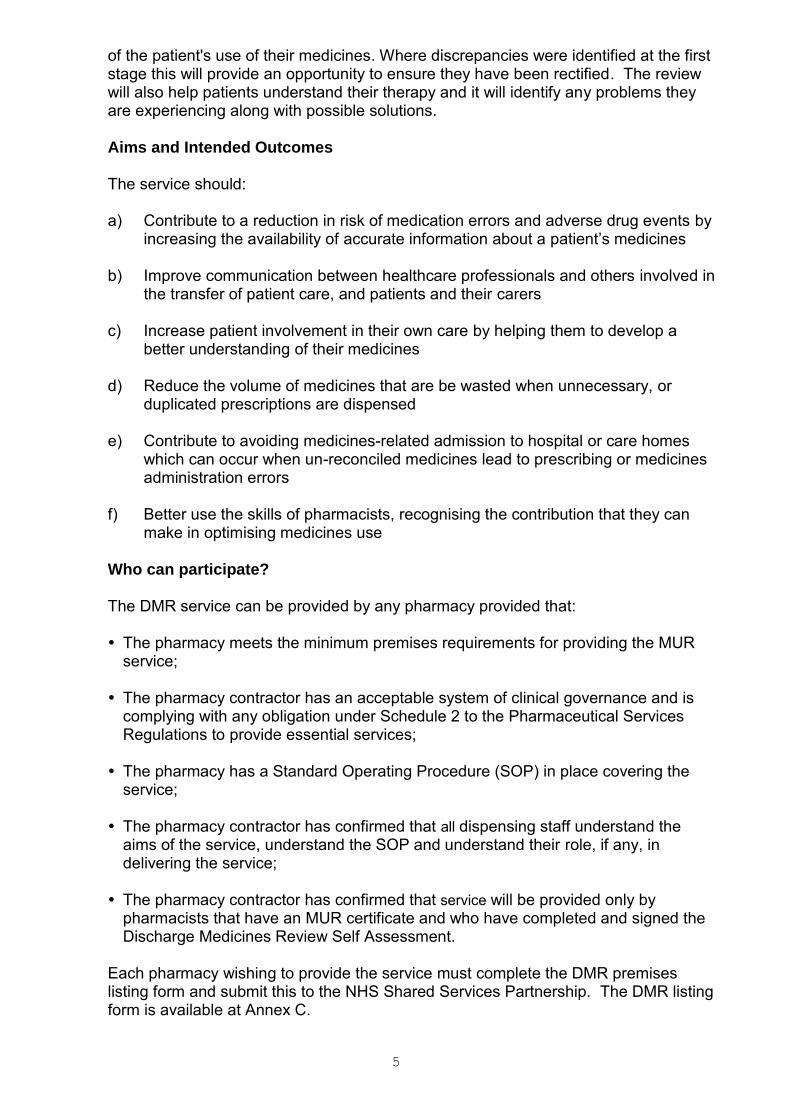
of the patient's use of their medicines. Where discrepancies were identified at the first stage this will provide an opportunity to ensure they have been rectified. The review will also help patients understand their therapy and it will identify any problems they are experiencing along with possible solutions. Aims and Intended Outcomes
The service should: a) Contribute to a reduction in risk of medication errors and adverse drug events by
increasing the availability of accurate information about a patient’s medicines b) Improve communication between healthcare professionals and others involved in
the transfer of patient care, and patients and their carers
c) Increase patient involvement in their own care by helping them to develop a better understanding of their medicines
d) Reduce the volume of medicines that are be wasted when unnecessary, or
duplicated prescriptions are dispensed e) Contribute to avoiding medicines-related admission to hospital or care homes
which can occur when un-reconciled medicines lead to prescribing or medicines administration errors
f) Better use the skills of pharmacists, recognising the contribution that they can
make in optimising medicines use Who can participate? The DMR service can be provided by any pharmacy provided that: The pharmacy meets the minimum premises requirements for providing the MUR
service; The pharmacy contractor has an acceptable system of clinical governance and is
complying with any obligation under Schedule 2 to the Pharmaceutical Services Regulations to provide essential services;
The pharmacy has a Standard Operating Procedure (SOP) in place covering the
service; The pharmacy contractor has confirmed that all dispensing staff understand the
aims of the service, understand the SOP and understand their role, if any, in delivering the service;
The pharmacy contractor has confirmed that service will be provided only by
pharmacists that have an MUR certificate and who have completed and signed the Discharge Medicines Review Self Assessment.
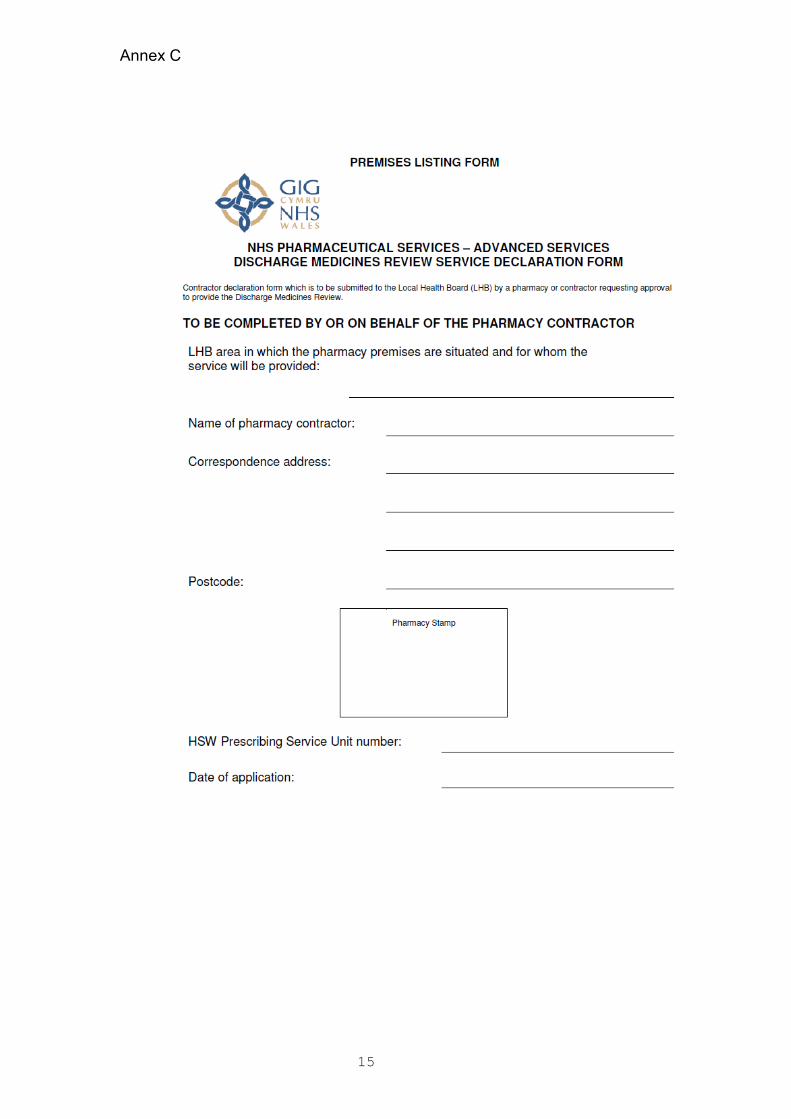
Each pharmacy wishing to provide the service must complete the DMR premises listing form and submit this to the NHS Shared Services Partnership. The DMR listing form is available at Annex C.

6

7
Training Requirements There are no specific training requirements for the DMR service, however the service may only be provided by pharmacists who have an MUR certificate and that have their name included in the list of pharmacists approved to provide MUR services in Wales which is maintained by the NHS Wales Shared Services Partnership. For pharmacists who do not have an MUR certificate there are a number of providers who run courses and/or competency assessments. Additionally some academic institutions that provide post-graduate clinical programmes, such as diplomas, have ensured their courses develop and test the skills of students in order to meet the requirements of the MUR competencies. For those pharmacists who have existing skills in this area of practice, the completion of any course prior to undertaking a competency assessment is not obligatory, i.e. pharmacists may put themselves through a competency assessment whenever they feel fit to do so. Further information in MUR accreditation is available at: http://www.psnc.org.uk/pages/pharmacist_mur_accreditation.html Pharmacists with an MUR certificate who are not yet included in the list of pharmacists approved to provide MUR services in Wales should contact the NHS Shared Services Partnership regarding the approval process. Service Outline
The service will comprise a two part intervention described below: Part One - Patient Identification and Medicines Reconciliation 1. Following discharge from a care setting patients will be identified and recruited to
the service either by referral by a healthcare professional, by patients or their nominated carer presenting in the pharmacy, or opportunistically by the pharmacy (e.g. where the pharmacy is able to offer the service to patients that meet the necessary criteria). In the case of planned admissions pharmacies may be in a position to identify potential patients prior to their admission.
2. Patients discharged from a care setting will be eligible for the service:
Where the pharmacy is in receipt of the Discharge Advice Letter (DAL) resulting from the most recent discharge, either from the patient, their carer, or from a healthcare professional;
And where any of the following criteria are met:
The patient’s medicines have been changed during their stay in the care setting from which they are being discharged;
The patient is taking four or more medicines
The patient’s medicine requires dispensing into a multi-compartment compliance device;
The pharmacist has, in their professional opinion, reason to consider that the patient would benefit from the service

8
3. The intervention will take place either with the patient in the pharmacy’s consultation area or by the pharmacy contacting the patient by telephone from the pharmacy if the patient is unable to attend the pharmacy (as is likely to be the case). The part one service must be completed within four weeks of the most recent discharge. The pharmacy will provide the patient with information about the service, which will include an explanation that the information may be shared with their GP as necessary.
4. The patient will need to consent to the sharing of this information in order to
access the service. If the patient does not consent to share information with the LHB and the NHS Wales Shared Services Partnership then the intervention will not normally be provided other than in exceptional circumstances. Exceptional circumstances may arise when, despite the patient withholding consent to share their information with the NHS, the pharmacist believes there will be significant benefit to patient care from undertaking a DMR. In this situation the pharmacist will need to annotate the claims form accordingly whilst also ensuring no patient specific data is submitted. In all cases the patient must consent to sharing relevant information with their GP.
5. At this stage the pharmacy will collect relevant information regarding the patients’
medication and check the medicines prescribed by the primary care team following discharge correspond to those the patient should be receiving, and that they are prescribed at the correct dose. The pharmacy will collect relevant information from the repeat prescription, the repeat prescription order form and from the patient or their carer in order to establish a complete picture of the medicines being taken by the patient. The pharmacist will complete the relevant information using the DMR forms agreed for the service.
6. Where the medicines prescribed by the primary care team following discharge do
not, in the opinion of the pharmacist, correspond to those the patient should be receiving, the pharmacist must bring this to the attention of the patient’s GP.
7. The pharmacist and patient will agree a time and method (i.e. by face to face
discussion or by telephone) for the second part of the service. This will normally be when the patient presents their next repeat prescription.
Part Two – Support for Adhering to Medication 8. The pharmacist and patient will, at the agreed time and by the agreed method,
discuss the patient’s use of medicines since discharge. The discussion will focus on (i) whether any problems identified in the first part of the service have been resolved; and (ii) any changes to the patient’s medicine regimen identified in the first part of the service.
9. The pharmacist will also discuss the patient’s use, understanding and experience
of taking their medicines drugs and complete the necessary section of the DMR 1 and DMR2 forms (the DMR2 form will be the same as the current MUR form).
10. The pharmacist will provide pharmaceutical care and advice leading to agreed
actions which support self care, promote adherence and reduce waste.
9
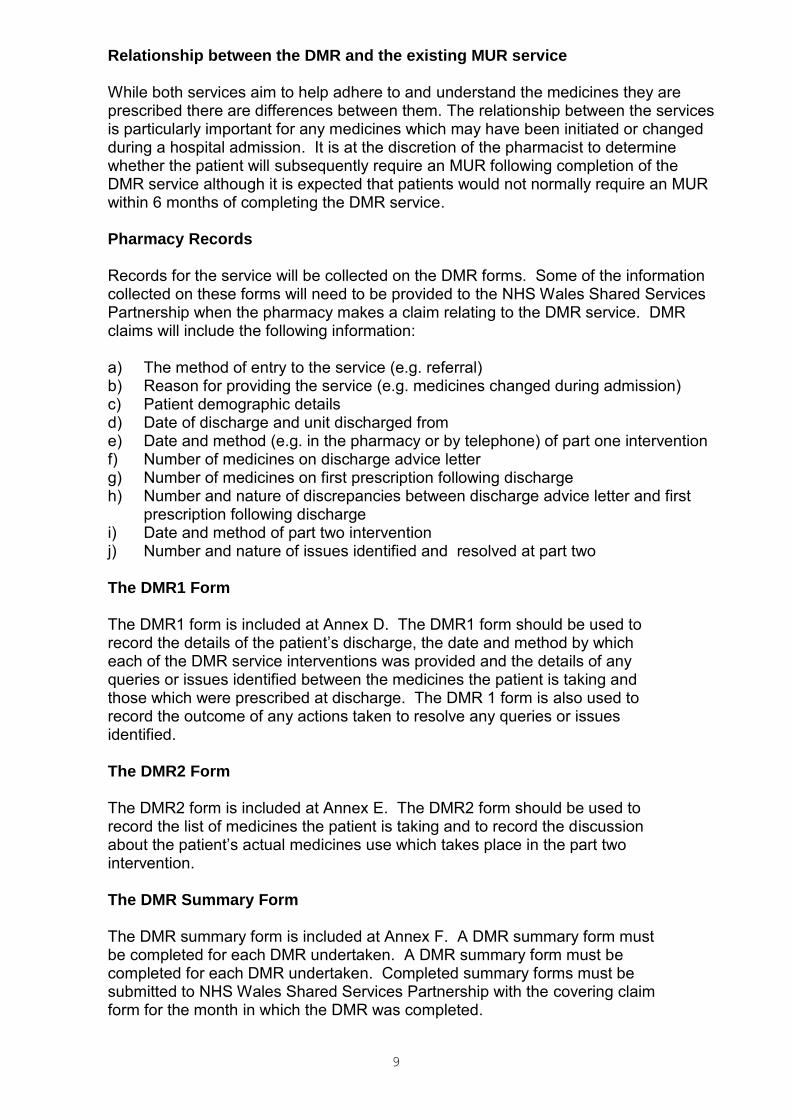
Relationship between the DMR and the existing MUR service While both services aim to help adhere to and understand the medicines they are prescribed there are differences between them. The relationship between the services is particularly important for any medicines which may have been initiated or changed during a hospital admission. It is at the discretion of the pharmacist to determine whether the patient will subsequently require an MUR following completion of the DMR service although it is expected that patients would not normally require an MUR within 6 months of completing the DMR service. Pharmacy Records
Records for the service will be collected on the DMR forms. Some of the information collected on these forms will need to be provided to the NHS Wales Shared Services Partnership when the pharmacy makes a claim relating to the DMR service. DMR claims will include the following information: a) The method of entry to the service (e.g. referral) b) Reason for providing the service (e.g. medicines changed during admission) c) Patient demographic details d) Date of discharge and unit discharged from e) Date and method (e.g. in the pharmacy or by telephone) of part one intervention f) Number of medicines on discharge advice letter g) Number of medicines on first prescription following discharge h) Number and nature of discrepancies between discharge advice letter and first
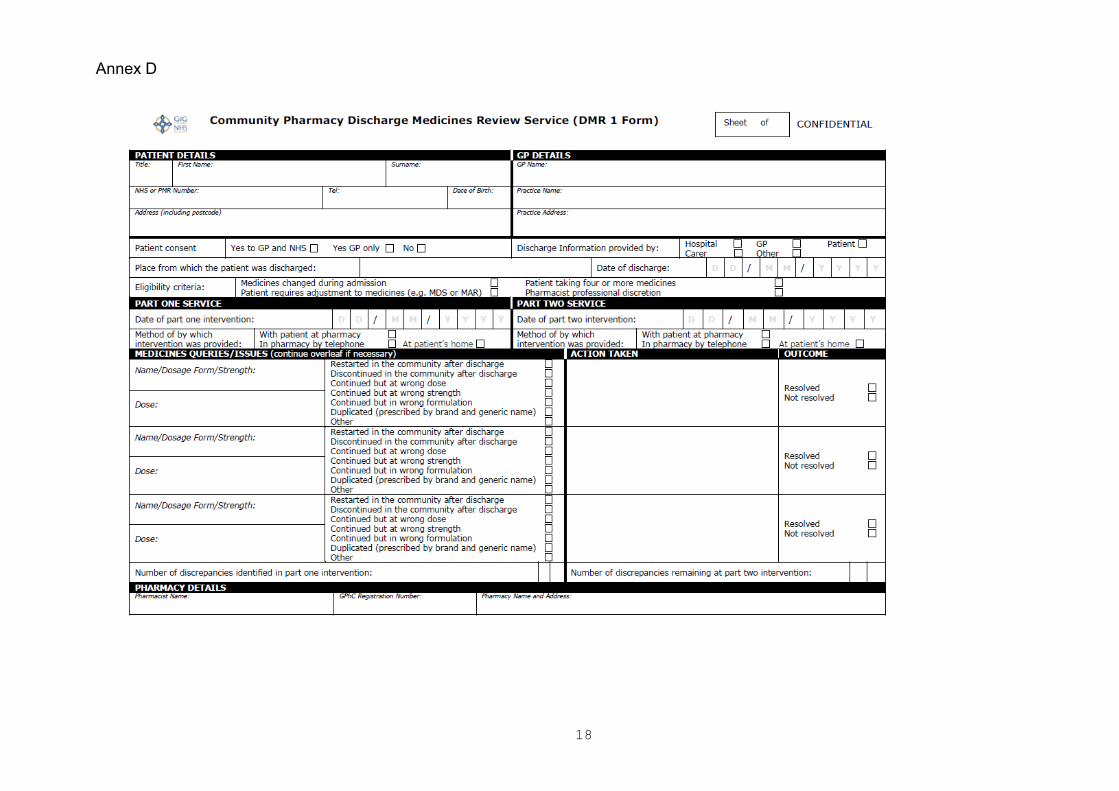
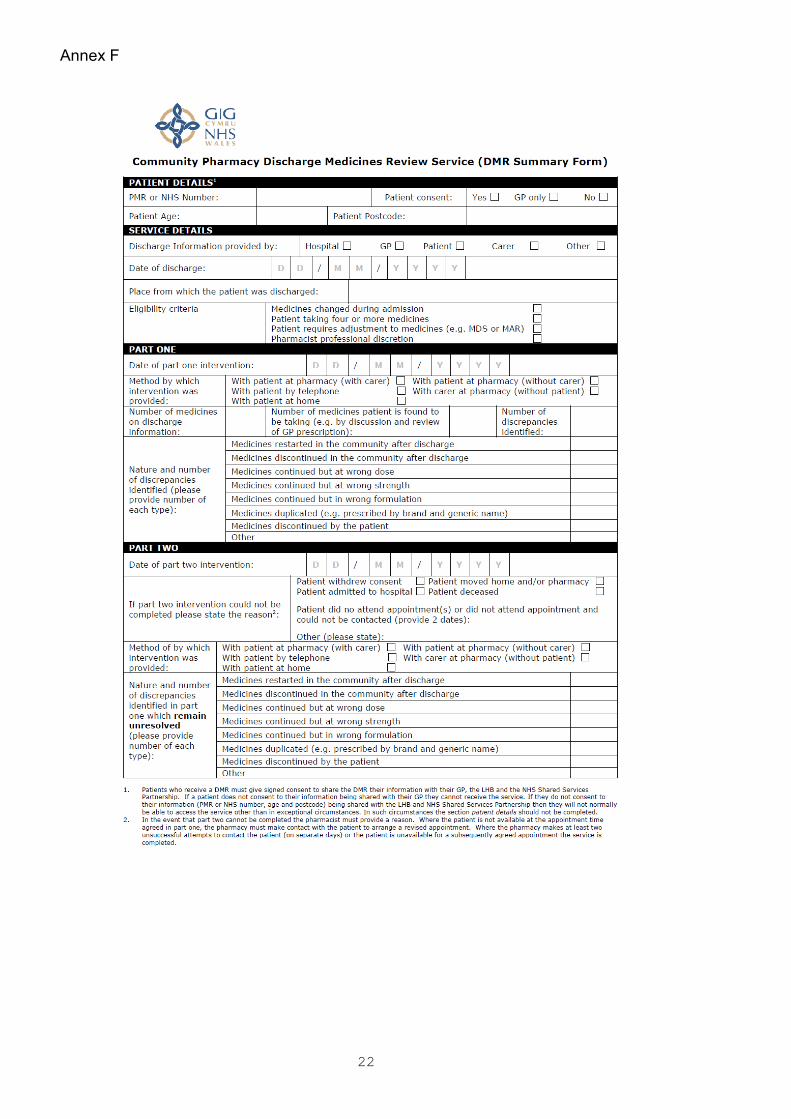
prescription following discharge i) Date and method of part two intervention j) Number and nature of issues identified and resolved at part two The DMR1 Form The DMR1 form is included at Annex D. The DMR1 form should be used to record the details of the patient’s discharge, the date and method by which each of the DMR service interventions was provided and the details of any queries or issues identified between the medicines the patient is taking and those which were prescribed at discharge. The DMR 1 form is also used to record the outcome of any actions taken to resolve any queries or issues identified. The DMR2 Form The DMR2 form is included at Annex E. The DMR2 form should be used to record the list of medicines the patient is taking and to record the discussion about the patient’s actual medicines use which takes place in the part two intervention. The DMR Summary Form The DMR summary form is included at Annex F. A DMR summary form must be completed for each DMR undertaken. A DMR summary form must be completed for each DMR undertaken. Completed summary forms must be submitted to NHS Wales Shared Services Partnership with the covering claim form for the month in which the DMR was completed.

10
Patient Consent Patients who receive a DMR must give signed consent to share their relevant information with their GP, the LHB and the NHS Shared Services Partnership. The purpose of sharing the information with the LHB and the NHS Shared Services Partnership is to provide assurance to NHS Wales that the DMR services are being provided appropriately and to support understanding how and to whom the service is being provided. If a patient does not consent to their relevant information being shared then they will not normally be able to access the service other than in exceptional circumstances. Where it is the professional opinion of the pharmacist that, despite the patient not providing consent to share relevant information with the LHB and the NHS Wales Shared Services Partnership, the patient would benefit from a DMR then the service can be provided but the claim form should not include any patient identifiable information. In all cases the patient must consent to sharing relevant information with their GP. Pharmacies will need to maintain a record of patient consent for each DMR service consultation completed. The record should be retained for at least 2 years from the date of the DMR. Suggested wording for patient consent forms is included at Annex A. Patient Eligibility Patients discharged from a care setting will be eligible for the service:
Where the pharmacy is in receipt of the Discharge Advice Letter (DAL) resulting from the most recent discharge, either from the patient, their carer, or from a healthcare professional;
And where any of the following criteria are met:
The patient’s medicines have been changed during their stay in the care setting from which they are being discharged;
The patient is taking four or more medicines
The patient’s medicine requires dispensing into a multi-compartment compliance device;
The pharmacist has, in their professional opinion, reason to consider that the patient would benefit from the service
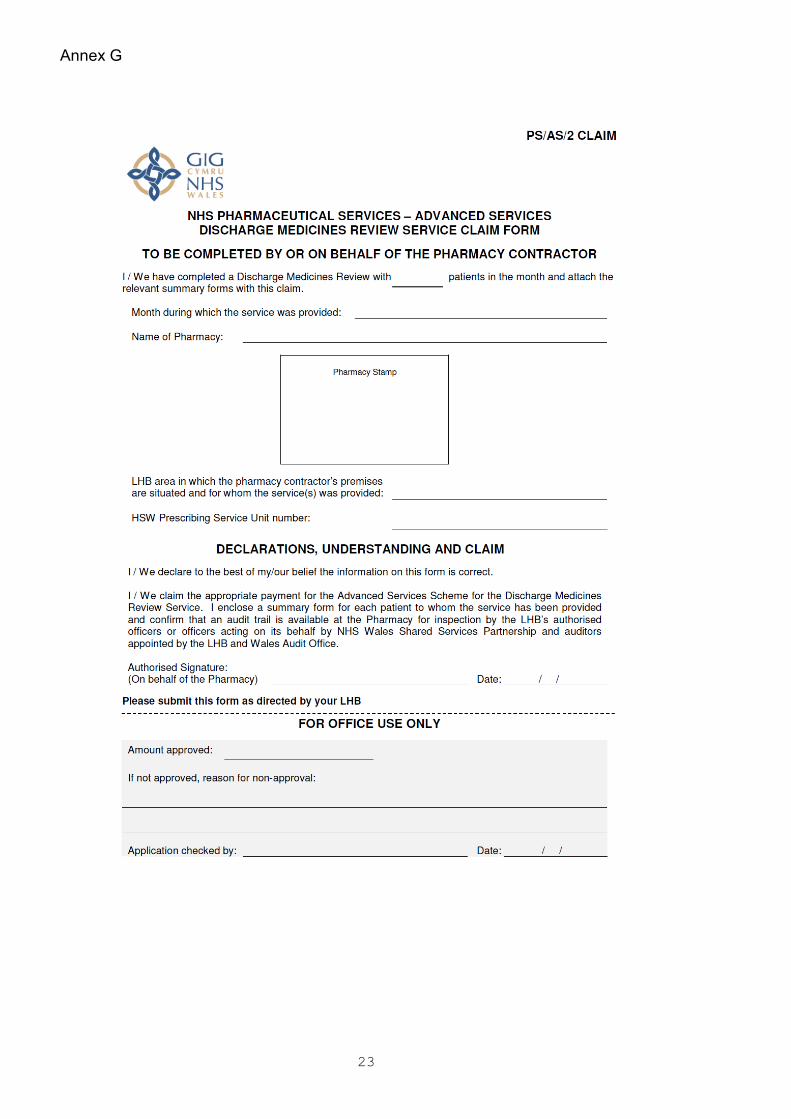
Claim Form The DMR claim form is included in Annex G. Claims should be submitted to the NHS Shared Services Partnership by the fifth of each month for all DMR service consultation completed in the previous month. Claims should only be made for completed DMR service consultations (i.e. once part one and part two of the service has been completed). The claim form must state the number of DMR service consultation completed in the relevant month and a copy of the DMR summary form for each patient must be provided. Where DMR summary forms are not submitted or are submitted incomplete claims will be returned to contractors without payment, for resubmission.
11
Further information and copies of all revised paperwork related to the DMR service can be accessed at: http://www.wales.nhs.uk/sites3/page.cfm?orgid=498&pid=7551
Structure of Fees Each DMR service consultation completed (i.e. where part one and part two of the service has been completed) will attract a fee of £37. Each pharmacy providing the DMR service may provide up to 100 DMR service consultations in 2011/12. This number will rise in 2012/13. In 2011/12 only, any pharmacy that initiates 10 DMS interventions before March 31, 2012 and goes on to complete those interventions will receive an implementation payment of £1,400. The one off payment is the same for all pharmacies and should be used to meet any set up costs incurred in implementing the service (this may include, amongst other things, undertaking MUR accreditation, changes to premises and printing DMR forms). An element of the implementation payment (£400 per pharmacy) is provided to meet the costs of a national evaluation of the service. CPW will lead on procuring this evaluation and will place a levy on contractors to ensure the funds are made available. Full details of fees and allowances will be published in the December 2011 Drug Tariff.
12
Annex A
13
Annex B

14
15
Annex C
16

17
18
Annex D

19

20
Annex E

21
22
Annex F
23
Annex G