changes in metabolism and blood flow in peripheral tissue
TRANSCRIPT

Changes in metabolism and blood �ow inperipheral tissue (skeletal muscle) duringcardiac surgery with cardiopulmonarybypass: the biochemical microdialysis studyJ Mand’ak1, P ZV ivny2, V Lonsky1, V PalicVka2, D Kakrdova2, M MarsV õkova2, P KunesV1 and J KubõcVek1
1Department of Cardiac Surgery, Charles University Hospital, Hradec Kralove, Czech Republic;2Institute of Clinical Biochemistry and Diagnoses, Charles University Hospital, Hradec Kralove, Czech Republic
The aim of this study was to monitor the metabolism andblood flow in the interstitium of the skeletal muscleduring cardiac surgery with cardiopulmonary bypass(CPB) and in the early postoperative period by means ofmicrodialysis and to compare metabolic changes duringCPB at normothermia (NT) and hypothermia (HT).
Surgical revascularization using CPB was performed in50 patients, 25 patients (group HT) were operated usinghypothermic CPB, 25 (group NT) using normothermicCPB. Interstitial microdialysis was performed by twoCMA 60 probes (CMA Microdialysis AB, Solna, Sweden)inserted into the patient’s deltoid muscle. Constituentsanalysed in the obtained dialysates, collected at intervals,were glucose, urea, glycerol and lactate. Tissue bloodflow was monitored by dynamic microdialysis withgentamicin as a marker.
In both groups, NT versus HT, similar dynamics ofconcentrations were found. Low initial concentrationswere followed by gradual increases during CPB and in
the following phase of the operation. Concentrations werehigher in the NT group. Immediately after the operation,the decrease in values continued, with a gradual increasein the succeeding postoperative period in both groups.Similar dynamic changes in the lactate concentrationwere found in both groups. The gentamicin concentra-tions were lower in the NT group (versus the HT group).
The results showed dynamic changes in the interstitialconcentrations of glucose, urea, glycerol and lactate,which depend on the phase of the surgery in the CPBand early postoperative phase in the both groups ofpatients. Higher tissue perfusion of the skeletal musclewas noted in those patients operated on in normothermia.The dynamics of the concentration changes of thesesubstances in the interstitium of the skeletal muscle hasbeen proven to be caused by both the metabolic activity ofthe tissue and by the blood flow through the interstitiumof the muscle. Perfusion (2004) 19, 53¡63.
Introduction
Surgical revascularization of myocardium duringcardiopulmonary bypass (CPB), extracorporeal cir-culation, ranks among contemporary routine treat-ment methods of ischaemic heart disease. Theoperated patients, however, run a certain risk dueto both complications of the surgery and theirgeneral condition, resulting either from the primarydisease or from the accompanying secondary dis-eases.1
One of the precipitating causes of the complica-tions can be the systemic and organ changes, whichdevelop due to the changes of blood circulationduring surgery. At the operation, but mainly during
the CPB, blood flow in the peripheral and splanch-nic circulation is redistributed. Hypoperfusion ofperipheral tissues and splanchnic organs caused byvasoconstriction, centralization of the circulation,and possibly by hypothermia, can lead to severecomplications.2 The decrease of blood pressure withconstant cardiac output, controlled haemodilution,and, first of all, the total (body) hypothermiadecreases energy demands of the cells, but, at thesame time, leads to the activation of the adrenergicsystem with consequent deterioration of the vaso-constriction of the peripheral and splanchnic ves-sels. These changes may lead to severe renal,gastrointestinal or hepatopancreatic complications,or to ischaemia of extremities, mainly if the arteriesare affected prior to surgery.
It is difficult to assess local changes of bloodcirculation in these areas, or to describe the meta-bolic changes. Direct measurement of the flowthrough the splanchnic or skeletal muscles during
Address for correspondence: JirVõ Mand’ak, MD, PhD, ConsultantCardiac Surgeon, Department of Cardiac Surgery, CharlesUniversity Hospital, 50005 Hradec Kralove, Czech Republic.E-mail: [email protected]
Perfusion 2004; 19: 53¡63
# Arnold 2004 10.1191/0267659104pf704oa
routine cardiac surgery is both technically andethically impracticable. The evaluation of the stan-dard biochemical and haemodynamic parameters(blood pressure, heart rate, O2 saturation in thecapillary bed, temperature, diuresis, peripheral ves-sel resistance, etc.) yields general results, but doesnot give information on regional changes or changesin the interstitial space.
One of the methods enabling biochemical mon-itoring of metabolic changes and blood flow in theinterstitial space of organs and tissues is micro-dialysis.
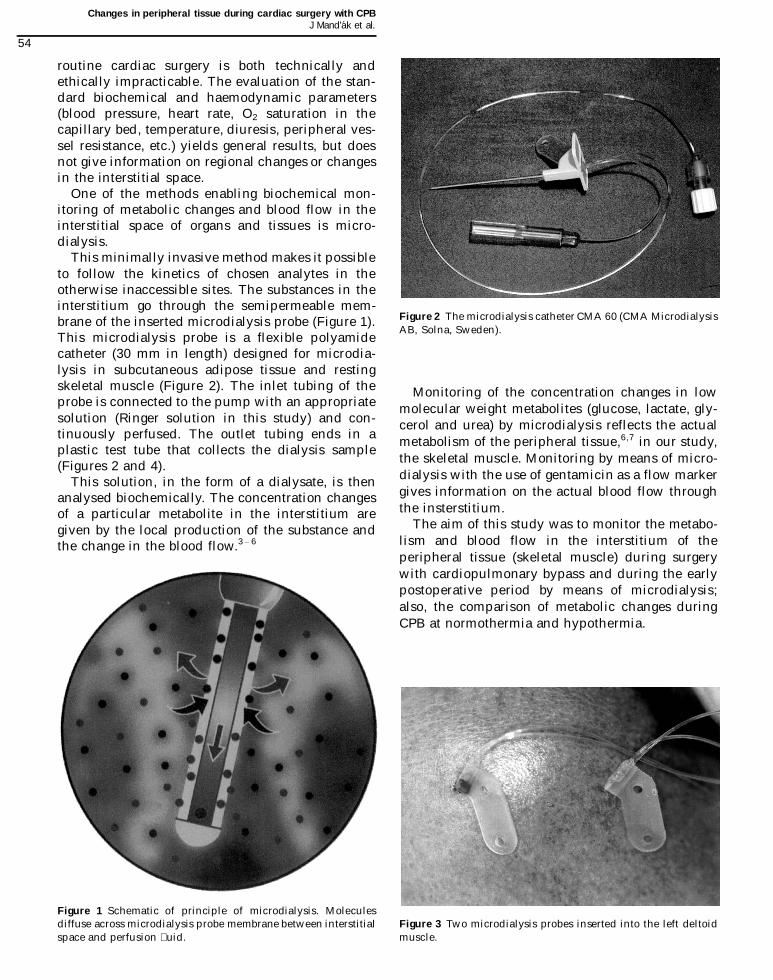
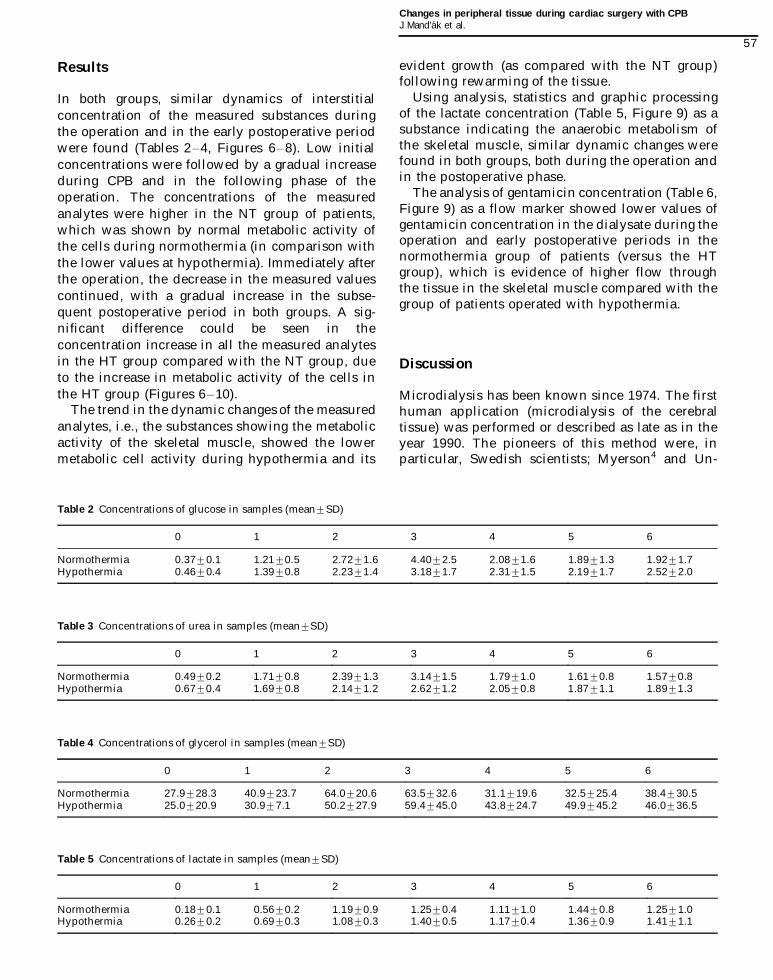
This minimally invasive method makes it possibleto follow the kinetics of chosen analytes in theotherwise inaccessible sites. The substances in theinterstitium go through the semipermeable mem-brane of the inserted microdialysis probe (Figure 1).This microdialysis probe is a flexible polyamidecatheter (30 mm in length) designed for microdia-lysis in subcutaneous adipose tissue and restingskeletal muscle (Figure 2). The inlet tubing of theprobe is connected to the pump with an appropriatesolution (Ringer solution in this study) and con-tinuously perfused. The outlet tubing ends in aplastic test tube that collects the dialysis sample(Figures 2 and 4).
This solution, in the form of a dialysate, is thenanalysed biochemically. The concentration changesof a particular metabolite in the interstitium aregiven by the local production of the substance andthe change in the blood flow.3 ¡ 6
Monitoring of the concentration changes in lowmolecular weight metabolites (glucose, lactate, gly-cerol and urea) by microdialysis reflects the actualmetabolism of the peripheral tissue,6,7 in our study,the skeletal muscle. Monitoring by means of micro-dialysis with the use of gentamicin as a flow markergives information on the actual blood flow throughthe insterstitium.
The aim of this study was to monitor the metabo-lism and blood flow in the interstitium of theperipheral tissue (skeletal muscle) during surgerywith cardiopulmonary bypass and during the earlypostoperative period by means of microdialysis;also, the comparison of metabolic changes duringCPB at normothermia and hypothermia.
Figure 1 Schematic of principle of microdialysis. Moleculesdiffuse across microdialysis probe membrane between interstitialspace and perfusion �uid.
Figure 2 The microdialysis catheter CMA 60 (CMA MicrodialysisAB, Solna, Sweden).
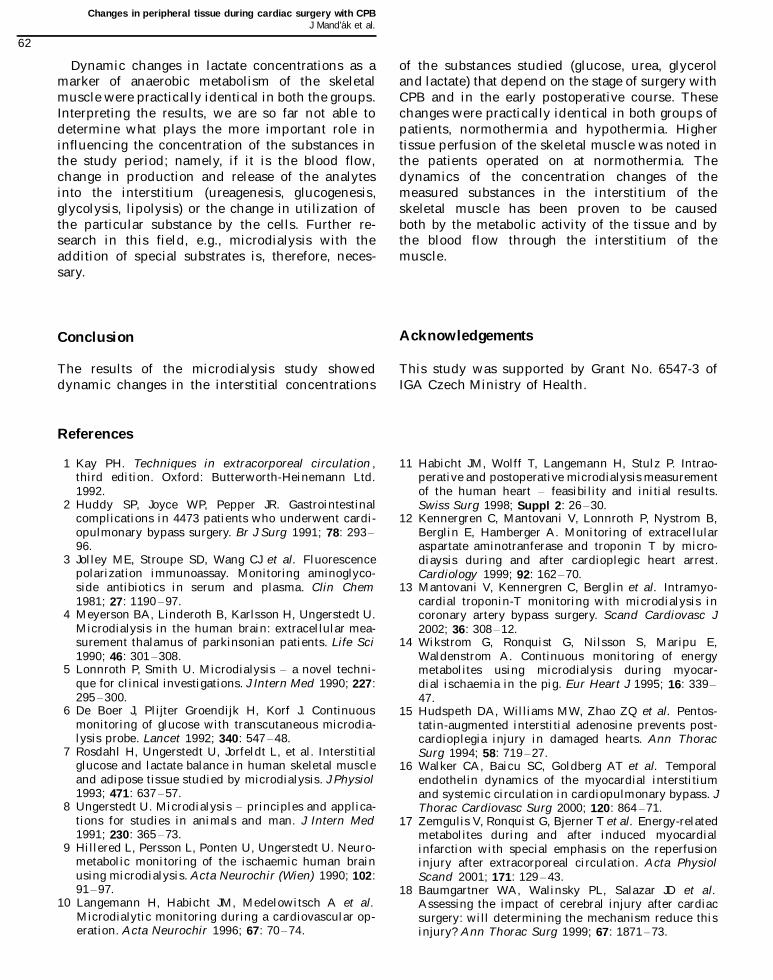
Figure 3 Two microdialysis probes inserted into the left deltoidmuscle.
Changes in peripheral tissue during cardiac surgery with CPBJ Mand’ak et al.
54

Patients
Fifty randomly chosen patients with ischaemicheart disease, on whom cardiac surgery ¡ surgicalrevascularization of the myocardium with CPB ¡was performed at the Department of Cardiac Surgeryin the Charles University Hospital in Hradec Kra-love, Czech Republic. There were 41 men and ninewomen with ages ranging from 51 to 79 years in thispopulation.
The patients were randomized into two groups:
Group one ¡ NT ¡ consisted of 25 patients, onwhom the revascularization of the heart wasperformed with standard CPB and normothermia(368C).Group two ¡ HT ¡ consisted of 25 patients, onwhom the surgery was performed with standardCPB and hypothermia (328C).
The differences between the two groups (age, dura-tion of CPB, accompanying diseases) were notstatistically significant (Table 1). All routine ther-apeutic and monitoring steps commonly used withthis diagnosis and method of treatment were per-formed. In all the patients, surgery was elective;patients operated on as emergencies were excludedfrom the study. Before the start of the investigation, adetailed description of the study was given to thepatients, who gave their informed consent.
Methods
The anaesthetic managements, CPB and surgicalprocedures were standardized in both groups.Anaesthesia was induced with sufentanil and mid-azolam, muscle relaxation with pipecuronium bro-mide. The extracorporeal circuit consisted of amembrane oxygenator (Dideco D 704, DidecoS.p.A., Mirandola, Italy or Macchi Oxim Ultra,Edwards Lifesciences Macchi Ltd., Sao Paulo, Bra-zil) and Polystan roller pumps (Polystan A/S,Vaerlose, Denmark). The pumps were operated in a
continuous flow manner. Oxygenators and tubingwere primed with Hartmann’s solution, low mole-cular weight dextran, 10% mannitol solution, gela-tin solution, 8.4% sodium bicarbonate, magnesiumsulphate, methylprednisolone, heparin 2500 u andaprotinin (Gordox, Gedeon Richter, Hungary)500 000 KIU. Patients were heparinized before CPB(2.5 mg/kg). Additional doses of heparin were givenwhen the ACT was shorter than 400 seconds. AfterCPB, heparin was neutralized with protamine sul-phate at a 1:1 ratio (controlled by ACT). A standardaortic and a two-stage venous cannula were used.Moderate hypothermia (328C) and calculated bloodflow of 2.4 L/min/m2 during CPB, cold crystalloidpotassium cardioplegia (St. Thomas’s Hospital Solu-tion) and topical cooling for myocardial protectionwere employed in the HT group. Normothermia(368C), calculated blood flow of 2.8¡3.0 L/min/m2
and warm blood cardioplegia (St.Thomas’s Solution4:1) were employed in the NT group.
The microdialysis described in this study wasperformed by two CMA 60 microdialysis probes(CMA Microdialysis AB, Solna, Sweden) (Figure 2)inserted into the deltoid muscle (musculus deltoi-deus) of the operated patient in the operating theatreafter introduction of anaesthesia (Figures 3¡5). Theprobes were perfused using Ringer’s solution at theconstant flow rate of 0.3 mL/hour.
Table 1 Groups of patients, NT versus HT
NT (n¾ 25) HT (n¾25) p
Age 69.596.5 66.398.1 nsCPB time 77.6919.4 74.9916.9 nsMyocardial infarction 11 14 nsHypertension 13 15 nsDiabetes mellitus 10 9 nsDyslipidaemia 18 16 nsObesity 11 12 ns
Figure 4 Test tubes in special holder.
Changes in peripheral tissue during cardiac surgery with CPBJ Mand’ak et al.
55

Dialysates were taken at the following intervals: atthe beginning of surgery, at the beginning of CPB, atthe end of CPB, at the end of the surgery and everytwo hours in the postoperative period. Sampleswere taken into special tubes and transported intoa biochemical laboratory. The amounts of dialysatesin the single samples were recorded as well. Theblood flow through the interstitium was monitoredby means of dynamic microdialysis of gentamicin asthe flow marker in the dialysates taken from thesecond probe. A known amount of gentamicin(Gentamicin, Lek, Slovenia), 80 mg/1000 mL ofRinger’s solution (167.2 mmol/L) was added intothe dialysis solution of the second probe, and, at theoutlet of the microdialysis probe, the changes in itsconcentration were monitored biochemically. Bloodflow through the interstitium of the skeletal muscleis directly proportional to the decrease in gentami-cin at the outlet of the probe.
We excluded possible changes of concentration ofthe analytes resulting from the dilution of thedialysates during CPB by means of simultaneousmicrodialysis using the dialysation solution withthe addition of dextran (Ringer’s solution withdextran in the ratio of 1:1). The concentrations ofanalytes found were the same as in the dialysates,where only the Ringer’s solution had been used.There was practically no difference found in the
amount of dialysate, therefore, the method with thesolution enriched by dextran has been discontinued.
The analyses of glucose, urea and lactate levelswere assessed by a Hitachi 917 analyser (RocheDiagnostics GmbH, Mannheim, Germany), glycerolconcentration by a colourimetric method (Randox)on a Cobas MIRA Plus analyser (Roche DiagnosticsGmbH, Mannheim, Germany). Gentamicin in themicrodialysate was determined by the AxSYManalyser (Abbott Laboratories, Abbott Park, USA)using the Fluorescence Polarization ImmunoAssay(FPIA) method.3
After evaluation of the results of microdialysis,these were statistically processed using the SIGMASTAT software (Jandel Scientific Corporation, SanRaphael, USA). The unpaired t -test, ANOVA, linearregression and Pearson’s correlation were used. Dataprocessing was done in co-operation with theDepartment of Computer Systems and the Centreof Medical Informatics of the University Hospital inHradec Kralove. The analysis results of the dialy-sates of both groups were evaluated, statisticallycompared and arranged into graphs.
There was no case of a local complication at anycannula insertion site, and there were no signs ofgeneral infection or catheter sepsis.
The study was approved by the Ethical Committeeof the University Hospital and Medical Faculty ofCharles University, Hradec Kralove.
Figure 5 Situation in the operating room.
Changes in peripheral tissue during cardiac surgery with CPBJ Mand’ak et al.
56
Results
In both groups, similar dynamics of interstitialconcentration of the measured substances duringthe operation and in the early postoperative periodwere found (Tables 2¡4, Figures 6¡8). Low initialconcentrations were followed by a gradual increaseduring CPB and in the following phase of theoperation. The concentrations of the measuredanalytes were higher in the NT group of patients,which was shown by normal metabolic activity ofthe cells during normothermia (in comparison withthe lower values at hypothermia). Immediately afterthe operation, the decrease in the measured valuescontinued, with a gradual increase in the subse-quent postoperative period in both groups. A sig-nificant difference could be seen in theconcentration increase in all the measured analytesin the HT group compared with the NT group, dueto the increase in metabolic activity of the cells inthe HT group (Figures 6¡10).
The trend in the dynamic changes of the measuredanalytes, i.e., the substances showing the metabolicactivity of the skeletal muscle, showed the lowermetabolic cell activity during hypothermia and its
evident growth (as compared with the NT group)following rewarming of the tissue.
Using analysis, statistics and graphic processingof the lactate concentration (Table 5, Figure 9) as asubstance indicating the anaerobic metabolism ofthe skeletal muscle, similar dynamic changes werefound in both groups, both during the operation andin the postoperative phase.
The analysis of gentamicin concentration (Table 6,Figure 9) as a flow marker showed lower values ofgentamicin concentration in the dialysate during theoperation and early postoperative periods in thenormothermia group of patients (versus the HTgroup), which is evidence of higher flow throughthe tissue in the skeletal muscle compared with thegroup of patients operated with hypothermia.
Discussion
Microdialysis has been known since 1974. The firsthuman application (microdialysis of the cerebraltissue) was performed or described as late as in theyear 1990. The pioneers of this method were, inparticular, Swedish scientists; Myerson4 and Un-
Table 2 Concentrations of glucose in samples (mean9SD)
0 1 2 3 4 5 6
Normothermia 0.3790.1 1.2190.5 2.7291.6 4.4092.5 2.0891.6 1.8991.3 1.9291.7Hypothermia 0.4690.4 1.3990.8 2.2391.4 3.1891.7 2.3191.5 2.1991.7 2.5292.0
Table 3 Concentrations of urea in samples (mean9SD)
0 1 2 3 4 5 6
Normothermia 0.4990.2 1.7190.8 2.3991.3 3.1491.5 1.7991.0 1.6190.8 1.5790.8Hypothermia 0.6790.4 1.6990.8 2.1491.2 2.6291.2 2.0590.8 1.8791.1 1.8991.3
Table 4 Concentrations of glycerol in samples (mean9SD)
0 1 2 3 4 5 6
Normothermia 27.9928.3 40.9923.7 64.0920.6 63.5932.6 31.1919.6 32.5925.4 38.4930.5Hypothermia 25.0920.9 30.997.1 50.2927.9 59.4945.0 43.8924.7 49.9945.2 46.0936.5
Table 5 Concentrations of lactate in samples (mean9SD)
0 1 2 3 4 5 6
Normothermia 0.1890.1 0.5690.2 1.1990.9 1.2590.4 1.1191.0 1.4490.8 1.2591.0Hypothermia 0.2690.2 0.6990.3 1.0890.3 1.4090.5 1.1790.4 1.3690.9 1.4191.1
Changes in peripheral tissue during cardiac surgery with CPBJ Mand’ak et al.
57

gersted5 of the Karolinska University in Stockholm,Hillered6 at the University of Uppsala, or at the sametime Lonnroth et al.7 in Goteborg. At present, thisminimally invasive method is being used both inexperiments on animals and in the human clinical
practice. The experimental studies are directedmainly at the microdialysis of liver and cerebraltissue of laboratory animals and the study of theinfluence of single substances on their metabolism.In clinical practice, microdialysis analyses are used
Figure 6 Concentrations of glucose in intervals ¡ hypothermia versus normothermia.
Figure 7 Concentrations of urea in intervals ¡ hypothermia versus normothermia.
Changes in peripheral tissue during cardiac surgery with CPBJ Mand’ak et al.
58

in terminally ill patients, e.g., after cerebraltraumas.8 ¡ 14
Microdialysis has been used, only rarely, incardiac surgery. Langemann et al. ,15 and Habicht16
have analysed the stage of myocardial ischaemia atcardiac arrest during cardiac surgery by means ofmicrodialysis probes inserted into the ventricularseptum. They analysed identical substances during
Figure 8 Concentrations of glycerol in intervals ¡ hypothermia versus normothermia.
Figure 9 Concentrations of lactate in intervals ¡ hypothermia versus normothermia.
Changes in peripheral tissue during cardiac surgery with CPBJ Mand’ak et al.
59

the study of cerebral ischaemia (glutathione, ascor-bic acid, cysteine, uric acid, glucose, lactate, etc.).Kennergen et al. ,17 as well as Mantovani andcolleagues,18 followed the T-troponin and aspartateaminotransferase levels in the myocardial intersti-tium of the left chamber prior to and after theoperation. Wilkstrom et al. ,19 as well as Hudspethet al. ,20 Walker et al.21 and Zemgulis et al. ,22 intheir experiments on animals, have similarly fol-lowed the influence of ischaemia and administereddrugs on the metabolism of cardiac muscle, theinfluence of acute ischaemia, the extent of theresulting injury on the myocardium, and the gradeof irreversibility. The studies of Baumgartner etal. ,23 Brock et al. 24 and Conroy et al. 25 deal withthe analysis of the grade of damage of the cerebraltissue in animals during extracorporeal circulation(CPB) or during the cardiac arrest by using micro-dialysis. The influence of CPB on metabolism andlocal blood flow in skeletal muscle during cardiacsurgery and in the early postoperative period has notbeen published in the world literature so far.
Microdialysis is a safe process. Changes in con-centration of certain metabolites in the interstitium
are given by three main factors: local production ofthe substance, local increase or decrease given bythe functions of the cells and by changes of bloodflow. Equilibrium of a substance between the inter-stitium and the dialysate is produced by the con-centration gradients, the velocity of the flow of thedialysis solution, the membrane properties, thehydrostatic pressure and the special ion conditionsthat develop on the internal and external sides ofmembrane.3,4,7,8
Microdialysis monitoring of the concentrationchanges of the low molecular weight metabolites,which in this study are glucose, lactate, glycerol andurea, reflect the actual metabolism in the peripheraltissues, the skeletal muscle.21 ¡ 25 Monitoring bymeans of microdialysis using gentamicin as amarker gives information of the actual blood flowthrough the interstitium.
Although it is possible to analyse practically anytissue by means of microdialysis, we come acrosscertain problems in the study of ‘peripheral tissues’in humans. Usually, it is not ethically acceptable toperform microdialysis of the splanchnic organsduring the cardiac operation via laparotomy. For
Figure 10 Concentrations of gentamicin in intervals ¡ hypothermia versus normothermia.
Table 6 Concentrations of gentamicin in samples (mean9SD)
0 1 2 3 4 5 6
Normothermia 146.3913.0 141.4932.4 138.9919.9 133.4920.3 144.7916.1 147.7922.1 137.7921.1Hypothermia 189.2950.5 191.8958.5 203.4964.3 191.8957.5 199.4971.8 207.7991.2 191.1984.6
Changes in peripheral tissue during cardiac surgery with CPBJ Mand’ak et al.
60

this reason, we have focused on microdialysis of theskeletal muscle as a typical peripheral tissue. Thechanges in the flow and metabolism, thus, representthe ‘whole periphery’.
In our study, we have selected the analysis of theflow and metabolism of the deltoid muscle. Thistypical skeletal muscle is easily accessible (forhandling by the samplers) throughout the course ofthe cardiac surgery (Figure 5).
In this study, the concentration changes of thesingle analytes in the skeletal muscle were studiedduring the operation and in the early postoperativeperiod. The absolute values, i.e., the real concentra-tions of the studied substances in the interstitium,can partially differ from the values we have ana-lysed. The fast dynamics of cardiac surgery produceintervals too short for standard microdialysis (theflow rate 0.01¡0.1 mL/hour). The amount of dialy-sate is usually so small in the single phases that itmay be insufficient for analysis by standard meth-ods. Microdialysis must be performed at higher flowrates of the dialysis solution (flow rate in this study0.3 mL/hour) or 100% recovery might not bereached (equilibrium between the interstitium ofthe tissue and the dialysate on the semipermeablemembrane). A smaller volume of single dialysissample can also be caused by loss of the dialysissolution due to the changes of interstitium osmol-ality. Adding dextran, as a high molecular weightsubstance to prevent this transfer of the solution (1:1with the Ringer’s solution), as recommended byRosdahl et al. ,13 did not improve the situation inour study. The amount of the dialysate in thesamples, and its possible decrease, remained practi-cally the same. Concentrations of the single analytesremained the same as well (Ringer’s solution withdextran versus without dextran). The CMA 600microdialysis analyser, which enables the analysisof a smaller volume in separate samples (circa 0.5mL), was not at our disposal at the time of the study.
Although it is obviously impossible to work withreal concentrations of the analytes, the trends of themeasured substances during the particular phases ofsurgery, CPB and the postoperative period can beassessed accurately, and the different conditions ofCPB (NT versus HT) can be compared.
In both groups (NT versus HT), similar dynamicsof the interstitial concentrations of the measuredsubstances has been found. Low initial concentra-tions gradually rose during CPB. Further increasesin the levels could be seen after termination of CPB,in the postsurgery phase. Immediately after surgery,the levels decreased then increased gradually againin the next postoperative phase in both groups.
These changes, as mentioned above, are given notonly by the metabolism of the cells of interstitialtissues, but also by changes in local blood flowthrough the tissues.
To determine blood flow in our study, we havechosen the method of microdialysis of the so-calledflow marker. It is a substance added in a specificconcentration to the microdialysis solution (in ourstudy, the Ringer’s solution) and its concentration isdetermined at the outlet of the probe. It is held thatthe lower its concentration at the outlet is, thehigher is the blood flow in the interstitium, andvice versa. The flow marker must meet someessential criteria. It must be sterile, nontoxic, non-volatile and easily determinable in a laboratory. Itsmolecules must be of significantly smaller size thanthe pores of the microdialysis membranes, and, atthe same time, they must not bind to this membrane.It must not be liable to any active transport pro-cesses in the interstitium and the adjacent cellmembranes and its clearance must not depend onthe presence of a physiological carrier.
We have chosen gentamicin as the flow marker.This original choice has come from the fact that thebiochemical determination of other frequently usedsubstances, such as ethanol or lithium, is moredifficult and financially too demanding. During thestudy, gentamicin has proven to be an appropriatesubstance for microdialysis of tissue flow. In certaincircumstances (e.g., hyperosmolality of the intersti-tum in the region of the inserted MD probe or aconsiderably higher hydrostatic pressure in theprobe than in its surroundings), a perfusion solutionleaves the probe much more easily than gentamicinand it can paradoxically increase its concentrationat the outlet of the probe.
Nevertheless, it is necessary to emphasize that weassessed only the trends in blood flow changes. Thereal values in blood flow, related to, for example,surface or the mass of the tissue, cannot be deter-mined by any known means.
From the evaluated results of our study, it ispossible to state that the higher concentrations ofthe analytes in the NT group (versus HT) during theoperation and CPB are given by higher blood flowthrough the tissue and normal metabolic activity ofthe cells. On the contrary, the lower concentrationsin the HT group are given, not only by lower bloodflow, but by lower metabolic activity as well, whichis the result of controlled hypothermia. The risingconcentrations in this group in the early postopera-tive phase (versus NT) are, thus, given by increasedmetabolic activity of the tissue after reaching normaltemperature, because the tissue blood flow stays onthe same level (Figure 10).
Changes in peripheral tissue during cardiac surgery with CPBJ Mand’ak et al.
61
Dynamic changes in lactate concentrations as amarker of anaerobic metabolism of the skeletalmuscle were practically identical in both the groups.Interpreting the results, we are so far not able todetermine what plays the more important role ininfluencing the concentration of the substances inthe study period; namely, if it is the blood flow,change in production and release of the analytesinto the interstitium (ureagenesis, glucogenesis,glycolysis, lipolysis) or the change in utilization ofthe particular substance by the cells. Further re-search in this field, e.g., microdialysis with theaddition of special substrates is, therefore, neces-sary.
Conclusion
The results of the microdialysis study showeddynamic changes in the interstitial concentrations
of the substances studied (glucose, urea, glyceroland lactate) that depend on the stage of surgery withCPB and in the early postoperative course. Thesechanges were practically identical in both groups ofpatients, normothermia and hypothermia. Highertissue perfusion of the skeletal muscle was noted inthe patients operated on at normothermia. Thedynamics of the concentration changes of themeasured substances in the interstitium of theskeletal muscle has been proven to be causedboth by the metabolic activity of the tissue and bythe blood flow through the interstitium of themuscle.
Acknowledgements
This study was supported by Grant No. 6547-3 ofIGA Czech Ministry of Health.
References
1 Kay PH. Techniques in extracorporeal circulation ,third edition. Oxford: Butterworth-Heinemann Ltd.1992.
2 Huddy SP, Joyce WP, Pepper JR. Gastrointestinalcomplications in 4473 patients who underwent cardi-opulmonary bypass surgery. Br J Surg 1991; 78: 293¡96.
3 Jolley ME, Stroupe SD, Wang CJ et al. Fluorescencepolarization immunoassay. Monitoring aminoglyco-side antibiotics in serum and plasma. Clin Chem1981; 27: 1190 ¡97.
4 Meyerson BA, Linderoth B, Karlsson H, Ungerstedt U.Microdialysis in the human brain: extracellular mea-surement thalamus of parkinsonian patients. Life Sci1990; 46: 301 ¡308.
5 Lonnroth P, Smith U. Microdialysis ¡ a novel techni-que for clinical investigations. J Intern Med 1990; 227:295 ¡300.
6 De Boer J, Plijter Groendijk H, Korf J. Continuousmonitoring of glucose with transcutaneous microdia-lysis probe. Lancet 1992; 340: 547 ¡48.
7 Rosdahl H, Ungerstedt U, Jorfeldt L, et al. Interstitialglucose and lactate balance in human skeletal muscleand adipose tissue studied by microdialysis. J Physiol1993; 471: 637 ¡57.
8 Ungerstedt U. Microdialysis ¡ principles and applica-tions for studies in animals and man. J Intern Med1991; 230: 365 ¡73.
9 Hillered L, Persson L, Ponten U, Ungerstedt U. Neuro-metabolic monitoring of the ischaemic human brainusing microdialysis. Acta Neurochir (Wien) 1990; 102:91¡97.
10 Langemann H, Habicht JM, Medelowitsch A et al.Microdialytic monitoring during a cardiovascular op-eration. Acta Neurochir 1996; 67: 70¡74.
11 Habicht JM, Wolff T, Langemann H, Stulz P. Intrao-perative and postoperative microdialysis measurementof the human heart ¡ feasibility and initial results.Swiss Surg 1998; Suppl 2: 26¡30.
12 Kennergren C, Mantovani V, Lonnroth P, Nystrom B,Berglin E, Hamberger A. Monitoring of extracellularaspartate aminotranferase and troponin T by micro-diaysis during and after cardioplegic heart arrest.Cardiology 1999; 92: 162 ¡70.
13 Mantovani V, Kennergren C, Berglin et al. Intramyo-cardial troponin-T monitoring with microdialysis incoronary artery bypass surgery. Scand Cardiovasc J2002; 36: 308 ¡12.
14 Wikstrom G, Ronquist G, Nilsson S, Maripu E,Waldenstrom A. Continuous monitoring of energymetabolites using microdialysis during myocar-dial ischaemia in the pig. Eur Heart J 1995; 16: 339¡47.
15 Hudspeth DA, Williams MW, Zhao ZQ et al. Pentos-tatin-augmented interstitial adenosine prevents post-cardioplegia injury in damaged hearts. Ann ThoracSurg 1994; 58: 719 ¡27.
16 Walker CA, Baicu SC, Goldberg AT et al. Temporalendothelin dynamics of the myocardial interstitiumand systemic circulation in cardiopulmonary bypass. JThorac Cardiovasc Surg 2000; 120: 864 ¡71.
17 Zemgulis V, Ronquist G, Bjerner T et al. Energy-relatedmetabolites during and after induced myocardialinfarction with special emphasis on the reperfusioninjury after extracorporeal circulation. Acta PhysiolScand 2001; 171: 129 ¡ 43.
18 Baumgartner WA, Walinsky PL, Salazar JD et al.Assessing the impact of cerebral injury after cardiacsurgery: will determining the mechanism reduce thisinjury? Ann Thorac Surg 1999; 67: 1871 ¡73.
Changes in peripheral tissue during cardiac surgery with CPBJ Mand’ak et al.
62

19 Brock MV, Blue ME, Lowenstein CJ et al. Induction ofneuronal nitric oxide after hypothermic circulatoryarrest. Ann Thorac Surg 1996; 62: 1313 ¡20.
20 Conroy BP, Lin CY, Jenkins LW et al. Hypothermicmodulation of cerebral ischemic injury during cardio-pulmonary bypass in pigs. Anesthesiology 1998; 88:390¡402.
21 Arner P. Use of microdialysis to study metabolism inhumans. Microline 1997; 3: 6¡8.
22 Muller M, Schmid R, Nieszpaur-Los M et al. Keymetabolite kinetics in human skeletal muscle duringischaemia and reperfusion: measurement by microdia-lysis. Eur J Clin Invest 1995; 25: 601 ¡607.
23 De Boer J, Potthoff H, Mulder PO et al. Lactatemonitoring with subcutaneous microdialysis in pa-tients with shock: a pilot study. Circ Shock 1994; 43:57¡63.
24 Rosdahl H, Hamrin K, Ungerstedt U, Henriksson J.Metabolite levels in human skeletal muscle andadipose tissue studied with microdialysis at lowperfusion �ow. Am J Physiol 1998; 274: 936¡ 45.
25 Henriksson J. Microdialysis studies of interstitialmetabolite concentrations and blood �ow in skeletalmuscle. Abstract book of 2nd International Sympo-sium on Clinical Microdialysis, April 22¡25, 1997,Uppsala, Sweden.
Changes in peripheral tissue during cardiac surgery with CPBJ Mand’ak et al.
63
