cell therapies in heart failure
TRANSCRIPT

STEM CELL THERAPY FOR
HEART FAILURE:
THEY WORK!
LESLIE W MILLER, MD
Leslie Miller, MD

REGENERATIVE MEDICINE
• Use of Stem Cells or Genes to
activate the body’s Native Repair
To
• Recover or Repair Any damaged
or dysfunctional organs, tissues,
or vessels

Stem Cell
Endothelium
Adipose
Neural/Brain
Cardiac Myocytes Fibroblasts
WHAT DEFINES A STEM CELL?
Blood Cells*
Skeletal Muscle Bone
Smooth Muscle
Endless SELF RENEWAL
DIFFERENTIATE into ALL Cell Types

SOURCES OF STEM CELLS: 2010
STEM
CELLS Embryonic
Bone
Marrow
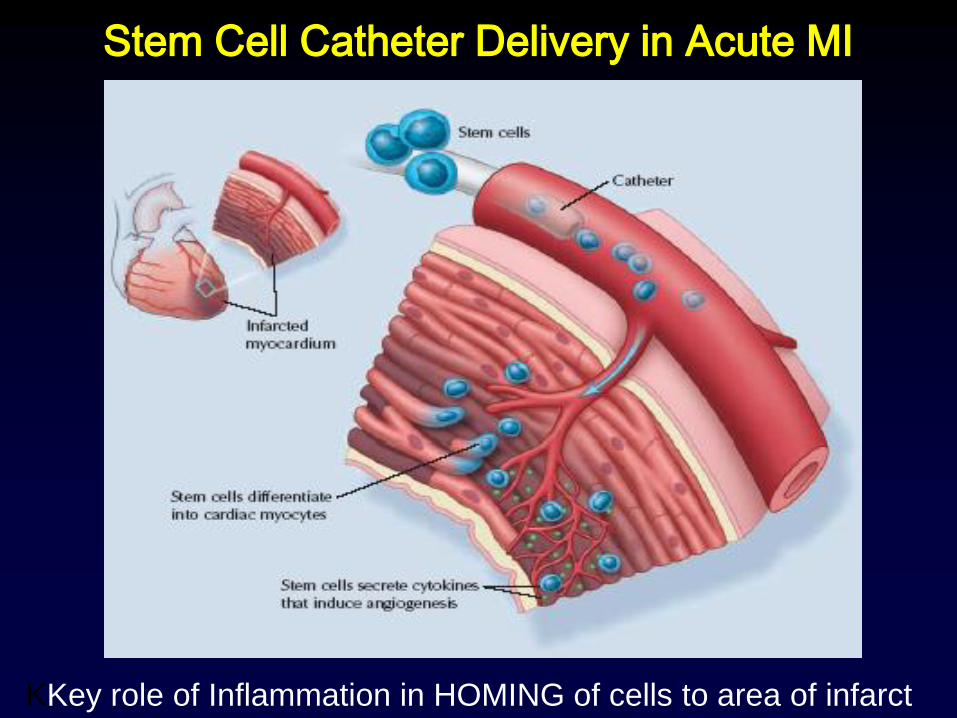
Stem Cell Catheter Delivery in Acute MI
KKey role of Inflammation in HOMING of cells to area of infarct

Cell Therapy for Acute MI
Bone Marrow Source • 17 RPC trials to date, including NIH trials
• Small-modest sample size trials (60-120)
• Variable time of delivery post MI, # cells, prep
• Nearly all Autologous Bone Marrow:
• Entire Mononuclear Cells > CD 34+ or CD 133+
• Variable results: EF change= + 2% (0-4%)*
• Best in those with lowest EF/greatest injury
• BAMI Trial of 3,000 pt Europe
*Jeevananthum Circ 2012

Impact of AGE on Frequency of
Stem Cells in Bone Marrow
AJ Caplan et al J Path 2009; 217: 318-324

Bone Marrow Stem Cells in
Heart Failure: NIH FOCUS Trial
• Phase II Randomized, Placebo controlled
• 92 patients with stable Ischemic HF (EF=27%)
• Randomized 2:1 to Autologous BM: Placebo
• 100 million cells delivered
• NOGA catheter endocardial cell delivery
• No inflammatory signal to direct homing of SCs
• Follow up at 6, 12, and 24 months
• E Perrin et al JAMA March 2012
E Perin et al JAMA 2012

NOGA Catheter

2D 3D
Endoventricular Stem Cell Delivery

FOCUS Trial
• Results: No change in SPECT, EF, LVEDV,
• No difference in Angina score
• Patients > 62 yrs Change in EF= 0 %
• Patients < 62 yrs EF increased 4.7%
• Autologous Bone Marrow is safe
• AGE may be a significant limitation Signature of
• Signature of Responders: (DA Taylor core lab)
Higher Number and Percentage of CD34+ cells

New Stem Cell Trials for HF
CardiAMP
• Phase III Pivotal trial
• 275 Patients with Ischemic HF
• Bone marrow source; 2:1 randomization
• Intramyocardial Delivery
• Enrollment based on BM markers
• Maximize odds of identifying Responders
• End Points: Survival and Remodeling

Autologous CD 34 + Cells for
Non-Ischemic Heart Failure
• 131 patients screened 2005-2006
• Average Age= 54 yrs; 80% males;
• EF = 25%; LVEDD= 7.0 cm; NT-BNP= 2400
• No CAD by cath
• Nuclear Scan all patients; Many had reversible Isch
• Bone Marrow source CD 34+ cells after GCSF
• Randomize 1:1 Cells vs Placebo
• Intracoronary Delivery
Vrtovec et al Circ Res Jan 2013

CD 34+ Stem Cells for
Non-Ischemic Heart Failure:
• 5 yr follow up Results:
• EF: increase 6% (24-30%, p=0.02)
• 6 Min Walk: increase (344-477, p<0.001)
• BNP: decreased 54% (2322-1011, p<0.01)
• Total Mortality: lower (14 vs 35%, p=0.01)
• Pump Failure Death: lower (5 vs 18%, p=0.03)
• Sudden Death: lower (9 vs 16%, p=0.39)
• Most benefit seen by 1 yr; persisted 5 yrs
• Vrtovec et al Circ Res 2013

N= 59 patients with Ischemic HF
Average Age = 65.5 years
Average EF = 28.1 ± 8.8%
Randomized 2:1, Cells(n=39) : Placebo(n=20)
Autol BM Aspirate Mesenchymal SCs
Endocardial Delivery of Cells
6 month follow up EP’s
Autologous Bone Marrow Mesenchymal SC’s
for Ischemic Heart Failure
Bruun, Methiason et al. EHJ Aug 2014

Stem Cells Placebo P Value
(n = 39) (n = 20)
LV End Syst Vol - 8.2 ± 14.2 + 6.0 ± 13.4 0.001
Ejection Fraction + 5.5 ± 3.8% - 1.4 ± 4.0% < 0.0001
Stroke Volume + 17.4 ± 14 - 3.1 ± 12.1 < 0.0001
End Syst Mass, g +10.1 ± 10 - 2.1 ± 8.9 < 0.0001
Scar Mass gm - 5.4 ± 5.1 - 4.4 ± 5.1 0.017 (MRI)
Age may be less important that cell type
Bone Marrow MNC’s for Ischemic Heart Failure
Bruun et al. EHJ July 2014

Allogenic Mesenchymal SC’s
• Any Allogenic (foreign) cell was thought to
require long term immunosuppression
• Mesenchymal SCs are “Immune Privileged”
• Minimal Alloimmune(antibody) response- trials*
• Cardiotrophic: Endothelium, Cardiomyocytes,
Smooth Muscle, Skel Muscle
• Equally effective as Autologous cells*
• Off-the-shelf therapy for any age or need
*Hare JAMA 2013

Allogenic Mesenchymal SCs for HF
DREAM trial
• PHASE III Pivotal trial of Allogeneic MSCs
• 1700 patients International trial-Class II/III
• Both Ischemic and Non-Ischemic HF etiology
• Intramyocardial Delivery of 150 M MSCs
• Ideal 20 yo donor for all patients
• Primary End Point:Composite Event Driven
• Secondary EPs include Echo Remodeling
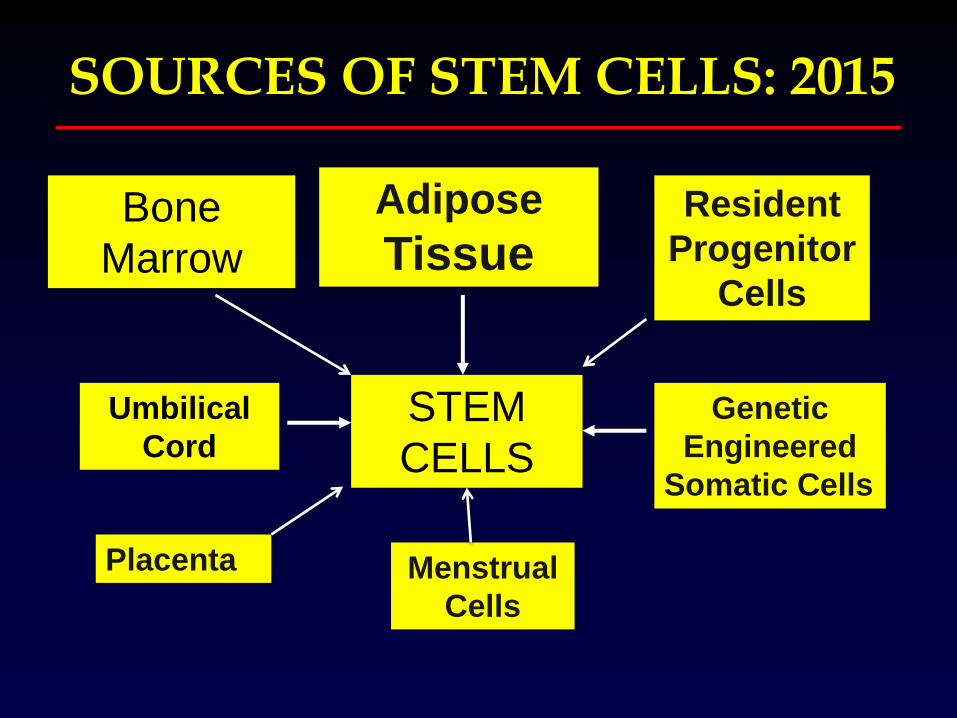
SOURCES OF STEM CELLS: 2015
STEM
CELLS
Umbilical
Cord
Adipose
Tissue Bone
Marrow
Genetic
Engineered
Somatic Cells
Menstrual
Cells
Resident
Progenitor
Cells
Placenta

Adipose Derived Stem Cells for Ht Failure
PRECISE Trial*
• Phase IIB Trial at 2 centers in Belgium
• 40 Patients Prior MI; EF < 40%
• 2:1 randomization: Cells : Placebo
• Liposuction, processing in O.R.
• Endocardial Delivery via NOGA system
• End Point is Change in EF
• Follow up at 6, 12 months
•
•
•
E Duckers et al AHJ May, 2014

PRECISE Trial of Adipose Derived Stem Cells for HF
24.4 cc
Difference
(-72,2%)
P=0.03
Perin et al Am Ht J May 2014;
End
Diastolic
Volume

Baseline 6 Mos 18 Mos
Transplant List
20.0 18.0 16.0 14.0
ADRCs for Ischemic HF: PRECISE Trial
Impact on Peak VO2:
19.0
15.5 15.3
16.6
17.1 17.2
ADRC’s Standard of Care
P<0.05 P<0.05
Pe
ak V
O2
Perin et al
AHJ May 2014 ATHENA Trial now enrolling in US same protocol
8 yrs older

Cardiac Progenitor Cells for HF:
CADUCEUS Trial • Phase IIA trial: 31 Pts < 30 days post MI, EF < 45%
• Endomyocardial Biopsy- Autologous source
• Cardiospheres: Cultured into millions cells-weeks
• Randomized 3:1 to CSP Cells vs Placebo
• Endocardial Delivery via NOGA catheter
• Results: Reduced scar mass by MRI by 24%
• Increased myocardial mass*(myogenesis)
Reduced LVESV and LVEDV
Improved EF by 39%
ALLSTAR Trial: 274 pts-Allogeneic Phase IIB
Maraban et al Lancet ‘12

Genetic Engineering Cell
Transformation
Cardiomyocyte
Fibroblast
iPSCs
Reprogramming
Oct3,4;SOX;MFT, cMyk
TranscriptionFactors
Differentiation Using
small molecules/GF’s
Direct
Reprogramming
Additional TF’s
Step1
Step 2
Unresolved Issues: Heterogeneity; Immune reactivity; Arrhythmia

Genetic Engineering of Lineage Specific
Cardiopoietic SCs: C-CURE study
• Skin fibroblasts exposed to a “cocktail” of growth
factors (4 genes) and tropic substances that
• Drives the cells into functioning cardiomyocytes
• Pilot of 45 patients; MI < 6 months; EF 40-50%
• Endocardial catheter delivery
• RESULTS: Decrease LVEDV, LVESV,
• Decrease LV Scar, increase Mass
• Increase EF % 26%
• Phase III Euro enrolling; US Phase II Andre Terzic et al JACC

Multipotent Adult Progenitor Cells (MAPCs)v
Penn et al JACC 2011

Stem Cell or Gene Therapy for Heart Failure

Delivery
Delivery Routes for Stem Cell/Gene
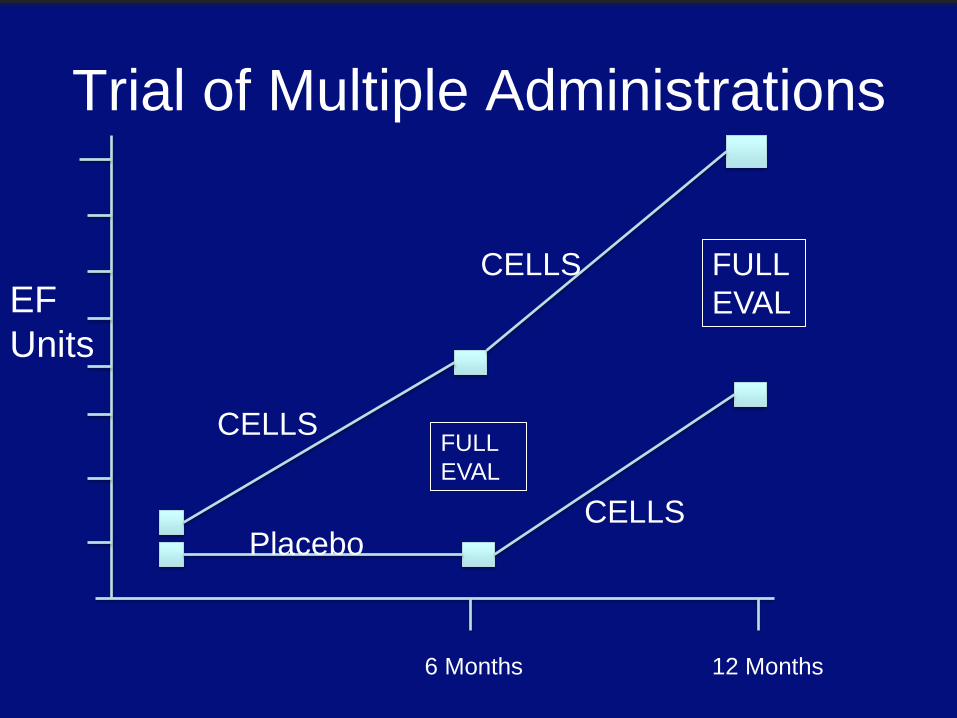
Trial of Multiple Administrations
EF
Units
6 Months 12 Months
CELLS
Placebo
FULL
EVAL
CELLS
CELLS
FULL
EVAL

Assmus, Zeiher
Euro HJ May, 2014
LONG TERM SURVIVAL/REHOSPITALIZATION BENEFIT OF BMMNC FOR AMI

FUNCTIONAL ASSAY TO PREDICT STEM CELL RESPONSE
Assmus,Zeiher
Euro J HF 2014

STEM CELL/GENE VENDORS-CV PHASE I
CardioCell
Medistem
Pleuristem
Celladon
HFPEF
PAH
* Cell
PHASE IIA
PHASE IIB
Mesoblast
Capricor
Cardio-3
Cytori
Bioheart
Neostem
Cell Prothera
Athersys
Aastrom
NIH LVAD-Allo MSC
NIH Allo Vs Auto MSC
NIH C-Kit + Allo MSC
Juventas
PHASE III
Teva
Cell Prothera
Zensun
Celladon
Harvest
Athersys
Baxter
Arteriocyte
Aldagen
Multigeyi
Cook
Renova
Juventas
PAD,
NSTEMI
Ottawa
Stem Cell Therapy for HF:
THEY WORK
• Learning to utilize the body’s native repair
• Stem Cells are clearly SAFE
• Multiple studies showing significant benefit
• New Era in Stem Cell therapy
• New Cells, Sources, Delivery, Doses, Frequency
• Many Phase IIB and III Clinical trials enrolling
• Will rewrite to potential benefit of
• Stem Cell Therapy for all of CV Disease

STEM CELL/GENE TRIALS
PHASE I
Hypoxia MSC
Umbilical Cord
Placental MSC
Endometrium
* Viral *Cell
PHASE IIA
PHASE IIB
Cardiosphere CPC
C-kit Card Progen
Genet Transf MSC
LVAD-ALLO MSC
LVAD-ADRCs
Allo Vs Auto MSC
C-Kit + Allo MSC
Adipose Derived SC
Bone Marrow Modif
Bone Marrow CD34+
SERCA 2-a*
SDF-1*
Neuregulin
PHASE III
Allo MSC
Auto CD34/
BM Select
Neuregulin*
MAPCs
Adenyl
Cyclase*
CD34+/eN
OS *
SDF-PAD
SDF-
NSTEMI

TISSUE ENGINEERING in RM
ENHANCED RETENTION
BEADS
PATCHES
SCAFFOLDS
STENTS
ORGANOGENESIS
PROTEIN ENGINEERING
