case study in heuristic failure case represents an example based on real case. some details have...
TRANSCRIPT
CASE STUDY IN CASE STUDY IN HEURISTIC FAILUREHEURISTIC FAILURE
Case represents an example Case represents an example based on real case. Some details based on real case. Some details have been changed and case de-have been changed and case de-
identified to preserve patient identified to preserve patient confidentialityconfidentiality
Ethan Cumbler M.D.Assistant Professor of Medicine
Hospitalist SectionUniversity of Colorado Hospital
2007

CASECASE
60 y/o male 60 y/o male presents with 4 presents with 4 days of progressive days of progressive dyspneadyspnea
Cough productive of Cough productive of dark brown sputumdark brown sputum
Hypoxia, Hypoxia, tachycardia, and tachycardia, and tachypneatachypnea
Subjective feversSubjective fevers
CXR demonstrates CXR demonstrates right lower lobe right lower lobe infiltrative density in infiltrative density in keeping with keeping with pneumoniapneumonia

What Is Your Most Likely Diagnosis?What Is Your Most Likely Diagnosis?

CASECASE
60 y/o with 60 y/o with multiple risk multiple risk factors for PE:factors for PE:
Prior Pulmonary Prior Pulmonary emboliemboli
Recent extended Recent extended plane tripplane trip
Presents with:Presents with:
DyspneaDyspnea Pleuritic chest painPleuritic chest pain TachycardiaTachycardia TachypneaTachypnea HypoxiaHypoxia Right heart strain Right heart strain
on EKGon EKG

What Is Your Most Likely Diagnosis?What Is Your Most Likely Diagnosis?

These are both the These are both the same patientsame patient
What heuristic trap did I just What heuristic trap did I just demonstratedemonstrate

Framing EffectFraming Effect

A CASE OF MISSED A CASE OF MISSED EMBOLIEMBOLI Despite four medical professionals Despite four medical professionals
considering PE, the patient did not have a CT considering PE, the patient did not have a CT scan for 3 days.scan for 3 days.
By the 3By the 3rdrd day the patient was tachycardic to day the patient was tachycardic to the 120s-130s, had increasing hypoxia and the 120s-130s, had increasing hypoxia and worsening tachypnea to 28 resps/minworsening tachypnea to 28 resps/min
At this point the patient was found to have At this point the patient was found to have massive pulmonary emboli, severe PHTN, massive pulmonary emboli, severe PHTN, Right heart failureRight heart failure
Required ICU transfer for thrombolytics Required ICU transfer for thrombolytics (with good response. Pt discharged on warfarin one week later)(with good response. Pt discharged on warfarin one week later)
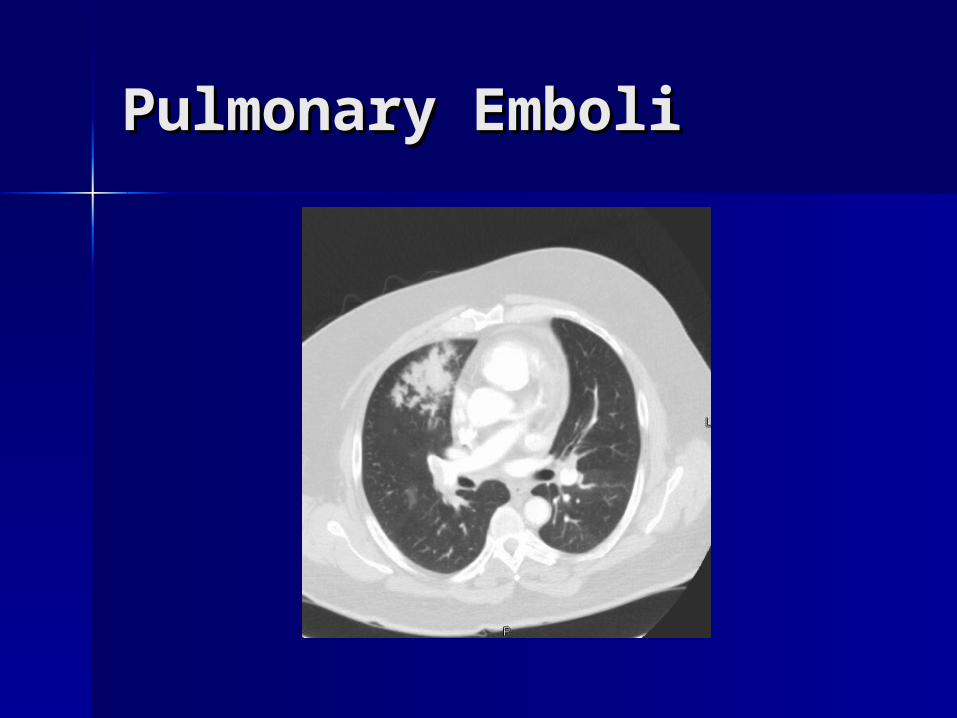
Pulmonary EmboliPulmonary Emboli

HOW DO FOUR SMART HOW DO FOUR SMART MEDICAL MEDICAL
PROFESSIONALS MISS PROFESSIONALS MISS WHAT SEEMS IN WHAT SEEMS IN
RETROSPECT LIKE AN RETROSPECT LIKE AN OBVIOUS DIAGNOSIS?OBVIOUS DIAGNOSIS?
AND WHAT COULD BE DONE AND WHAT COULD BE DONE DIFFERENTLY TO PREVENT SIMILAR DIFFERENTLY TO PREVENT SIMILAR
ERRORS IN THE FUTURE?ERRORS IN THE FUTURE?

Lets Take a Closer Look Lets Take a Closer Look At the Case to See What At the Case to See What
Went WrongWent Wrong

HISTORYHISTORY
60 y/o presents for 60 y/o presents for evaluation of chest pain, evaluation of chest pain, SOB, DOESOB, DOE
Progressively increasing Progressively increasing SOB x 2 weeks since SOB x 2 weeks since returning from a trip to returning from a trip to AlabamaAlabama
+Productive cough- +Productive cough- initially clear then browninitially clear then brown
+Subjective fevers+Subjective fevers +Pleuritic chest pain+Pleuritic chest pain No calf edemaNo calf edema
PE 1995- warfarin PE 1995- warfarin x 6 mox 6 mo
DM II with DM II with neuropathyneuropathy
HyperlipidemiaHyperlipidemia HTNHTN OSA-not on CPAPOSA-not on CPAP GoutGout

HistoryHistory
NKDANKDA
atenololatenolol simvastatinsimvastatin famotidinefamotidine colchicinecolchicine ibuprofen prnibuprofen prn
Family Hx-Family Hx- Hyperlipidemia, Hyperlipidemia,
Strokes, CAD, CancerStrokes, CAD, Cancer
Social Hx-Social Hx- + Tobacco, No ETOH, + Tobacco, No ETOH,
no drug use. no drug use. Administrative Administrative assistantassistant
ROS-ROS- otherwise negativeotherwise negative
ED PHYSICIAN ED PHYSICIAN ASSESSMENTASSESSMENT 60 y/o male with h/o PE years ago 60 y/o male with h/o PE years ago
treated with 6 months of warfarin treated with 6 months of warfarin presents to the ED with several presents to the ED with several days of dyspnea after airplane days of dyspnea after airplane flightflight

DOES THIS DOES THIS SOUND LIKE A SOUND LIKE A
FRAMING FRAMING EFFECT EFFECT
PROBLEM?PROBLEM?

ED PHYSICIAN NOTEED PHYSICIAN NOTE
Story initially concerning for PE, however on Story initially concerning for PE, however on further questions do not feel PE likely with this further questions do not feel PE likely with this patient:patient:
No leg painNo leg pain Symptoms developed gradually with progressive Symptoms developed gradually with progressive
cough and change in color of sputumcough and change in color of sputum Chest pain is felt to be musculoskeletal. No PND, Chest pain is felt to be musculoskeletal. No PND,
DOE, peripheral edema, or diaphoresisDOE, peripheral edema, or diaphoresis Chest pain is ?pleuritic and worse with movementChest pain is ?pleuritic and worse with movement Pt is a smoker and moving air poorlyPt is a smoker and moving air poorly Rales heard in RLLRales heard in RLL CXR revealing RLL infiltrate with pt desaturating.CXR revealing RLL infiltrate with pt desaturating.

ED PHYSICIAN NOTEED PHYSICIAN NOTE
After reviewing history, exam, labs, After reviewing history, exam, labs, and imaging; I do not feel pt has and imaging; I do not feel pt has ongoing acute coronary syndrome, ongoing acute coronary syndrome, pulmonary emboli, or aortic pathologypulmonary emboli, or aortic pathology
DIAGNOSIS- DIAGNOSIS- PneumoniaPneumonia
Treatment-Treatment- ASA, Azithromycin, CeftriaxoneASA, Azithromycin, Ceftriaxone

INPATIENT PHYSICIAN #1INPATIENT PHYSICIAN #1
60 y/o gentleman with a hx of OA, 60 y/o gentleman with a hx of OA, Gout, DM, remote idiopathic Gout, DM, remote idiopathic pulmonary embolism admitted with pulmonary embolism admitted with RLL PNA, chest pain and ECG RLL PNA, chest pain and ECG changes.changes.
1.1. RLL PNA-hypoxic and tachycardic. No hx RLL PNA-hypoxic and tachycardic. No hx aspiration. Will start him on ceftriaxone aspiration. Will start him on ceftriaxone and azithromycin, support him with oxygen and azithromycin, support him with oxygen and provide Pneumonia vaccineand provide Pneumonia vaccine
INPATIENT PHYSICIAN #1INPATIENT PHYSICIAN #1
2.2. ECG changes and chest pain. With ECG changes and chest pain. With DM,HTN,Hyperlipidemia he is at risk for CAD. DM,HTN,Hyperlipidemia he is at risk for CAD. However, his hx of exertional C.P coincides However, his hx of exertional C.P coincides with his likely development of PNA. ECG with his likely development of PNA. ECG changes are noted as is his normal troponin.changes are noted as is his normal troponin.
• Monitor troponins, ASA, StatinMonitor troponins, ASA, Statin• Hold his B-B given tachycardia and moderate Hold his B-B given tachycardia and moderate
hypotensionhypotension• No stress test given the likely alternative No stress test given the likely alternative
explanation of symptoms from his pneumonia. explanation of symptoms from his pneumonia. However, we will consider getting an inpatient However, we will consider getting an inpatient stress test should his symptoms change.stress test should his symptoms change.

INPATIENT PHYSICIAN #1INPATIENT PHYSICIAN #1
3.3. Hx of PE and questionable right heart Hx of PE and questionable right heart strain. His ECG changes are noted. He strain. His ECG changes are noted. He has chronic OSA not on CPAP.has chronic OSA not on CPAP.
We will defer PE workup at this point We will defer PE workup at this point given the likely alternative diagnosis of given the likely alternative diagnosis of RLL PNA as the etiology of his symptoms RLL PNA as the etiology of his symptoms hypoxia and tachycardia. However, if hypoxia and tachycardia. However, if no improvement with antibiotics then no improvement with antibiotics then will proceed with CT pulmonary will proceed with CT pulmonary angiography. We will not proceed with angiography. We will not proceed with empiric anticoagulation at this point.empiric anticoagulation at this point.

INPATIENT TEAM #2INPATIENT TEAM #2DAY 2DAY 2 SubjectiveSubjective- slightly improved SOB. Continued - slightly improved SOB. Continued
DOE, no cough, no chest painDOE, no cough, no chest pain ObjectiveObjective- - BP 141/82 HR 103 RR 22 T 36.0 93% 4lBP 141/82 HR 103 RR 22 T 36.0 93% 4l
1) PNA- Slight improvement with ABX. 1) PNA- Slight improvement with ABX. WBC decreased 11.8-8.8. Plan continued WBC decreased 11.8-8.8. Plan continued ceftriaxone/azithromycinceftriaxone/azithromycin
2) SOB- most likely RLL PNA. h/o PE. No 2) SOB- most likely RLL PNA. h/o PE. No CT pulmonary angiogram for now unless CT pulmonary angiogram for now unless increased SOBincreased SOB
Note- inpatient team #2 no longer knows about recent travel as they obtained Note- inpatient team #2 no longer knows about recent travel as they obtained history from the dictated h+p which does not mention travel (although ED note history from the dictated h+p which does not mention travel (although ED note and handwritten H+P do list travel historyand handwritten H+P do list travel history

HR
0
20
40
60
80
100
120
140
160
HR
Liters O2
0
1
2
3
4
5
6
Liters O2
RR
0
5
10
15
20
25
30
RR
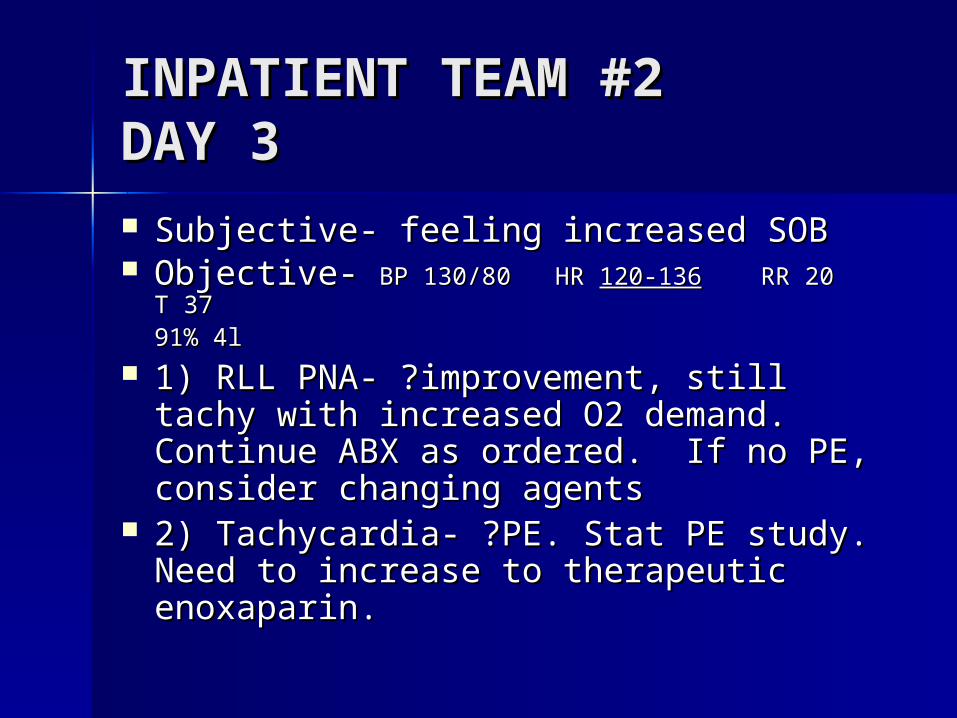
INPATIENT TEAM #2INPATIENT TEAM #2DAY 3DAY 3 Subjective- feeling increased SOBSubjective- feeling increased SOB Objective- Objective- BP 130/80 HR BP 130/80 HR 120-136120-136 RR 20 T 37 RR 20 T 37
91% 4l91% 4l
1) RLL PNA- ?improvement, still tachy 1) RLL PNA- ?improvement, still tachy with increased O2 demand. Continue with increased O2 demand. Continue ABX as ordered. If no PE, consider ABX as ordered. If no PE, consider changing agentschanging agents
2) Tachycardia- ?PE. Stat PE study. 2) Tachycardia- ?PE. Stat PE study. Need to increase to therapeutic Need to increase to therapeutic enoxaparin.enoxaparin.

CT PULMONARY CT PULMONARY ANGIOGRAMANGIOGRAM Numerous filling defects are noted within the Numerous filling defects are noted within the
pulmonary arteries bilaterally. Extensive pulmonary arteries bilaterally. Extensive thrombus is identified in the main pulmonary thrombus is identified in the main pulmonary artery. artery.
Associated hemorrhage Associated hemorrhage within lung tissuewithin lung tissue
Echo shows severely hypokinetic and dilated Echo shows severely hypokinetic and dilated right heart and flattened septumright heart and flattened septum
STRUCTURED STRUCTURED ANALYSIS OF MEDICAL ANALYSIS OF MEDICAL ERRORERROR Use (Use (Systematic Analysis of a Medical Error Systematic Analysis of a Medical Error
form to guide discussion)form to guide discussion)

Step 1Step 1
Adverse event, Medical error, Adverse event, Medical error, CausationCausation
Was There an Adverse Event?-Was There an Adverse Event?- Yes- Yes- the patient went into right heart failure the patient went into right heart failure with hemodynamic instability as a with hemodynamic instability as a result of an untreated embolismresult of an untreated embolism
Was there a Medical Error?Was there a Medical Error? Yes- a Yes- a delay of diagnosis of a life threatening delay of diagnosis of a life threatening disease represents a medical errordisease represents a medical error
Were the two related-Were the two related- Yes. Correct Yes. Correct diagnosis would have offered earlier diagnosis would have offered earlier treatment of the P.E. and potential for treatment of the P.E. and potential for prevention of new or extended emboliprevention of new or extended emboli
Step 2Step 2
Were There Systems Were There Systems Issues Which Issues Which
Contributed to This Contributed to This Error? Error?
-Communication-Communication-Information management-Information management-Technology-Technology-Supervision-Supervision-Workload-Workload-Human resources support issues (staffing)-Human resources support issues (staffing)

Systems issues.Systems issues.
WorkloadWorkload-- is a potential contributor if the physicians were too is a potential contributor if the physicians were too rushed with other patients to take time to contemplate the rushed with other patients to take time to contemplate the differential diagnosis.differential diagnosis.Inpatient team was covering increased patient load due to Inpatient team was covering increased patient load due to staffing shortfall and thus increased cross-covering workload staffing shortfall and thus increased cross-covering workload contributed.contributed.
Communication-Communication- No clear trigger for nursing to contact No clear trigger for nursing to contact physician team for changes in vital signs- HR rising, O2 sat physician team for changes in vital signs- HR rising, O2 sat falling, nursing did not have clear guidelines on when falling, nursing did not have clear guidelines on when physicians should be called. physicians should be called.
Information management-Information management- Medical record is split- information Medical record is split- information about recent travel was in the ED record and in the about recent travel was in the ED record and in the handwritten H+P but not in the dictated version.handwritten H+P but not in the dictated version.
Human resources-Human resources- Information attrition with handoffs. Staffing Information attrition with handoffs. Staffing model used causes multiple handoffs during typical hospital model used causes multiple handoffs during typical hospital stay.stay.
Step 3Step 3
Which Type of Individual Which Type of Individual Error Did This Represent?Error Did This Represent? Knowledge basedKnowledge based- mistake from - mistake from
inadequate or incomplete information inadequate or incomplete information or base of knowledge or base of knowledge
Skill basedSkill based- performance error. Not - performance error. Not doing the action which was intended. doing the action which was intended. We think of this as a “slip” We think of this as a “slip”
Rule basedRule based- the incorrect - the incorrect application of the information. We application of the information. We think of this as a “Judgment failure” think of this as a “Judgment failure”

Rule BasedRule Based
This was a classic judgment This was a classic judgment failurefailure
Step 4Step 4
List Heuristic Failures List Heuristic Failures Leading to Individual Leading to Individual
Judgment ErrorJudgment Error

Heuristics ErrorsHeuristics Errors Diagnosis MomentumDiagnosis Momentum
(potent factor in this case. Subsequent (potent factor in this case. Subsequent physicians continue original plan of care physicians continue original plan of care without reevaluation)without reevaluation)
Representativeness RestraintRepresentativeness Restraint(looks like a duck, quacks like a duck, goes (looks like a duck, quacks like a duck, goes into right heart failure like a PE)into right heart failure like a PE)
Base Rate Neglect- Base Rate Neglect- (Actual pretest probability 27.8% by Wells (Actual pretest probability 27.8% by Wells Criteria. What pretest probability for PE do Criteria. What pretest probability for PE do you think the physicians were assuming in you think the physicians were assuming in this case?) this case?)
Other VariablesOther Variables
One physician discussed how he/she was One physician discussed how he/she was working to order less tests in the setting of working to order less tests in the setting of the over-use of imaging which is common the over-use of imaging which is common in the hospital. in the hospital.
Over-reliance on the accuracy of CXR Over-reliance on the accuracy of CXR diagnosis of pneumonia. People tend to diagnosis of pneumonia. People tend to give lab tests greater weight than may be give lab tests greater weight than may be appropriate for the test’s sensitivity and appropriate for the test’s sensitivity and specificity. There is an authority which specificity. There is an authority which seems to come with the typed radiology seems to come with the typed radiology report or laboratory result listed to two report or laboratory result listed to two decimal pointsdecimal points

Step 5Step 5
What Level Harm Occurred As What Level Harm Occurred As a Result of The Adverse a Result of The Adverse
Event?Event?
1- No harm, error identified prior to affecting 1- No harm, error identified prior to affecting patientpatient2- Minor temporary harm2- Minor temporary harm3- Minor permanent harm3- Minor permanent harm4- Major temporary4- Major temporary5- Major permanent5- Major permanent6- Death6- Death
Harm score 4- Major TemporaryHarm score 4- Major Temporary

Step 6Step 6
What Would You Disclose What Would You Disclose In This Case?In This Case?

DisclosureDisclosure
In this case disclosure did occur.In this case disclosure did occur. The patient was told that the initial The patient was told that the initial
theory to explain the symptoms was theory to explain the symptoms was pneumonia but that his failure to pneumonia but that his failure to improve led the medical team to improve led the medical team to order the CT scan which revealed that order the CT scan which revealed that the initial diagnosis was incorrect and the initial diagnosis was incorrect and he actually had blood clots in the he actually had blood clots in the lungslungs
DisclosureDisclosure
The patient replied that he had The patient replied that he had suspected it was a blood clot.suspected it was a blood clot.
A simple apology and expression A simple apology and expression of regret for the delay in diagnosis of regret for the delay in diagnosis would have been appropriate.would have been appropriate.
Step 7Step 7
What Steps Could be What Steps Could be Taken to Prevent This Taken to Prevent This From Occurring in The From Occurring in The
FutureFuture

Concrete StepsConcrete Steps
Increased Meta-cognition.Increased Meta-cognition. Cultivate the sense of unease you get when you Cultivate the sense of unease you get when you
are not sure you are making the correct are not sure you are making the correct diagnosis. diagnosis.
(We have a tendency to silence this inner voice) (We have a tendency to silence this inner voice) When you realize you are making a questionable When you realize you are making a questionable
call, pause to mentally reframe the case in the call, pause to mentally reframe the case in the terms of the alternate diagnosisterms of the alternate diagnosis
Consider whether your reasoning would look Consider whether your reasoning would look appropriate if you were wrong and the alternate appropriate if you were wrong and the alternate diagnosis turned out to be the case.diagnosis turned out to be the case.

Concrete StepsConcrete Steps
Increased Meta-cognition.Increased Meta-cognition. Be introspective about your clinical Be introspective about your clinical
reasoning. Recognize when factors reasoning. Recognize when factors such as feeling like you are ordering such as feeling like you are ordering “too many tests” can have subtle “too many tests” can have subtle influence on your decision making.influence on your decision making.
Concrete StepsConcrete Steps
Increased Meta-cognition.Increased Meta-cognition.
Some people imagine having their reasoning cross-examined by a skeptical reviewer.
“DR……. Can you explain to me why you felt a patient with a prior history of PE who presents with shortness of breath, tachycardia, and hypoxia did not merit even a D-dimer test?” This represents an exercise in meta-cognition as you examine whether the route you used to come to decide that the patient did not need the test can stand up to scrutiny

Concrete StepsConcrete Steps
Communication of uncertainty-Communication of uncertainty- Recognize when you are making a Recognize when you are making a
questionable call and pass this questionable call and pass this uncertainty along to the physicians uncertainty along to the physicians who will be assuming care during who will be assuming care during transitions to decrease impact of transitions to decrease impact of diagnosis momentumdiagnosis momentum
Think about the different message you send when you check Think about the different message you send when you check out “chest pain rule out MI” versus “chest pain of uncertain out “chest pain rule out MI” versus “chest pain of uncertain etiologyetiology

Concrete StepsConcrete Steps
Use of differential diagnosis- Use of differential diagnosis- Reduces impact of availability biasReduces impact of availability bias
This was done in this case.This was done in this case.

Concrete StepsConcrete Steps
Use of algorithms or clinical Use of algorithms or clinical prediction tools- cognitive forcing prediction tools- cognitive forcing strategy strategy
Wells Criteria would have been Wells Criteria would have been useful in this caseuseful in this case

Wells Criteria for PEWells Criteria for PEClinical feature:Clinical feature: PointsPointsSymptoms DVTSymptoms DVT 33
Other Dx less likely than PEOther Dx less likely than PE 33
HR>100HR>100 1.51.5
Immobilization/surgery last Immobilization/surgery last 4 wks4 wks
1.51.5
Prior VTEPrior VTE 1.51.5
HemoptysisHemoptysis 11
MalignancyMalignancy 11
>6 points-High Risk (78.4%)2-6 points- Moderate Risk (27.8%)<2 points- Low Risk (3.4%)
Dichotomous algorithm splits this into:PE unlikely (<4)PE likely (>4)
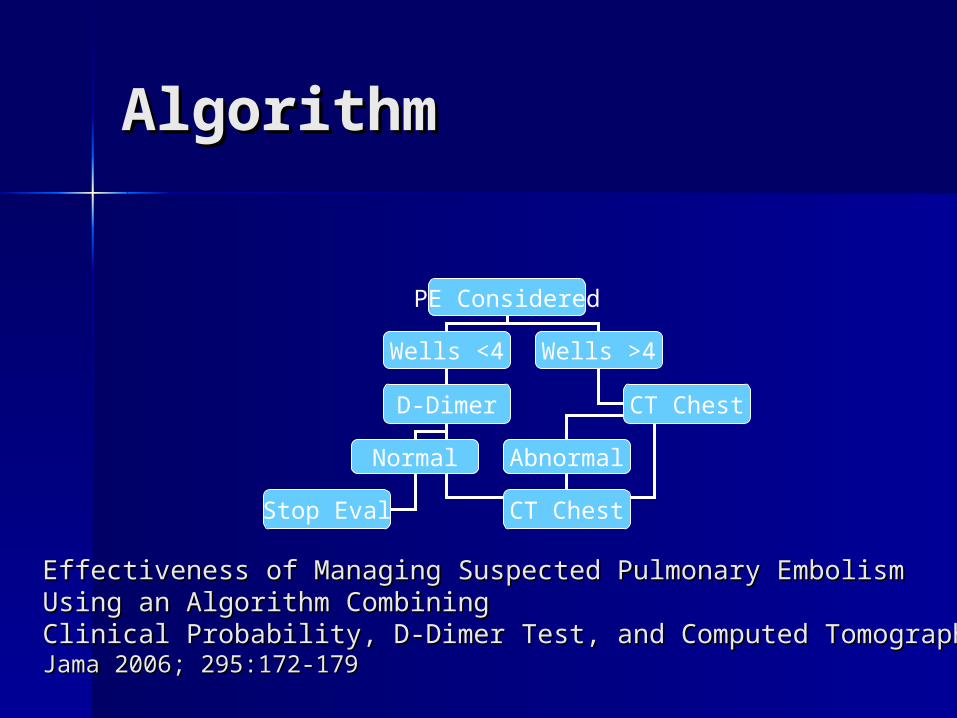
AlgorithmAlgorithm
PE Considered
Wells <4 Wells >4
CT ChestD-Dimer
Normal Abnormal
Stop Eval CT Chest
Effectiveness of Managing Suspected Pulmonary Embolism Effectiveness of Managing Suspected Pulmonary Embolism Using an Algorithm Combining Using an Algorithm Combining Clinical Probability, D-Dimer Test, and Computed TomographyClinical Probability, D-Dimer Test, and Computed TomographyJama 2006; 295:172-179Jama 2006; 295:172-179
ConclusionsConclusions
MetacognitionMetacognition is an important mechanism is an important mechanism to prevent heuristic errors (reframing, to prevent heuristic errors (reframing, visualizing justification of reasoning)visualizing justification of reasoning)
Communication of uncertaintyCommunication of uncertainty when you when you have made a “soft call” can reduce the have made a “soft call” can reduce the impact of diagnosis momentumimpact of diagnosis momentum
Use of a Use of a prediction toolprediction tool such as Wells Test such as Wells Test would likely have prevented base-rate would likely have prevented base-rate neglect in this caseneglect in this case
Use of an Use of an management algorithmmanagement algorithm would would likely have triggered a D-dimer test. Likely likely have triggered a D-dimer test. Likely would have prevented this delayed diagnosiswould have prevented this delayed diagnosis

ReferencesReferences
1.1. Croskerry P. The Importance of Cognitive Errors in Croskerry P. The Importance of Cognitive Errors in Diagnosis and Strategies to Minimize Them. Acad Diagnosis and Strategies to Minimize Them. Acad Med 2003;78:775-780Med 2003;78:775-780
2.2. Graber M, Gordon R, Franklin N. Reducing Graber M, Gordon R, Franklin N. Reducing Diagnostic Errors in Medicine: Whats the Goal? Acad Diagnostic Errors in Medicine: Whats the Goal? Acad Med 2002;77:981-992Med 2002;77:981-992
3.3. Redelmeier DA, Ferris LE, Tu JV, Hux JE, Schull MJ. Redelmeier DA, Ferris LE, Tu JV, Hux JE, Schull MJ. Problems For Clinical Judgement: Introducing Problems For Clinical Judgement: Introducing Cognitive Psychology as One More Basic Science. Cognitive Psychology as One More Basic Science. JAMC 2001;164:358-360JAMC 2001;164:358-360
4.4. Human Error. Reason, James. Cambridge University Human Error. Reason, James. Cambridge University Press, Cambridge 1990.Press, Cambridge 1990.
5.5. How Doctors Think. Groopman, Jerome. Houghton How Doctors Think. Groopman, Jerome. Houghton Mifflin Company, New York 2007.Mifflin Company, New York 2007.

ReferencesReferences
6.6. Redelmeler DA. The Cognitive Psychology of Missed Redelmeler DA. The Cognitive Psychology of Missed Diagnoses. Ann Intern Med 2005;142:115-120Diagnoses. Ann Intern Med 2005;142:115-120