case reports - japi.orgjapi.org/november_2016/pdf/12_cr_metronidazole.pdf · typical of metabolic...
TRANSCRIPT
Journal of The Association of Physicians of India ■ Vol. 64 ■ November 201672
Metronidazole Induced Encephalopathy Nisarg Thakkar1, Bhaarat1, Ramesh Chand1, Raman Sharma2, Sunil Mahavar3, Swati Srivastava4, Arvind Palawat5
Introduction
Me t r o n i d a z o l e , t i n i d a z o l e , secn idazo le and orn idazo le
are 5-nitroimidazole group of drugs which are widely prescribed, believed to be safe and pr imari ly used to treat infections caused by susceptible a n a e r o b i c o r g a n i s m s s u c h a s Bacteroides, Fusobacterium, Clostridium, Peptostreptococcus and Prevotella species and parasite such as Entamoeba histolytica, giardia and trichomonas vaginalis.1
Serious nervous system adverse effects like ataxia, encephalopathy, dysarthria, seizures, aseptic meningitis, and peripheral neuropathy, usually with prolonged therapy have recently been reported, though reviews suggest that they are reversible. The most common neurological complication caused by metronidazole is peripheral neuropathy.1 Caution should be used when prescribing metronidazole in patients with history of seizure disorder. Mild central nervous system effects include dizziness, headache, confusion, vertigo, and insomnia. Other, rare and serious adverse effects seen with metronidazole therapy include Stevens-Johnson syndrome, hemolytic uremic syndrome, pancreatitis, ototoxicity, and ophthalmologic toxicity.2
MRI has proven to be the most i m p o r t a n t d i a g n o s t i c t o o l a n d reversibility is the most important feature of MIE, with reversal of both CNS effects and MRI findings. Most
Abstract Metronidazole is an antimicrobial used for the treatment of anaerobic bacterial and protozoal infections. Neurological toxicity due to metronidazole use has been a matter of concern and many case reports of neurotoxicity are being published. We report here a case of a 32 years old male chronic alcoholic with multiple liver abscesses and history of 6 weeks use of metronidazole presenting with multiple episodes of seizures, burning sensation of feet and altered sensorium. MRI Brain revealed characteristic and reversible involvement of dentate nuclei and splenium of corpus callosum, typical of metronidazole induced encephalopathy (MIE).
1Resident, 2Sr. Professor, 3Assistant Professor, 4Professor, 5Junior Specialist, Department of Medicine, SMS Medical College, Jaipur, RajasthanReceived: 06.07.2015; Revised: 31.12.2015; Accepted: 07.06.2015
left side of body and bilateral grade I horizontal nystagmus suggestive of left sided cerebellar involvement. Sensory examination revealed hyperesthesia in both soles and altered joint position sense in small joints of both feet. Rest of the CNS examination including fundus examination was normal and there was no neck rigidity. Abdominal e x a m i n a t i o n r e v e a l e d t e n d e r hepatomegaly and there was no ascites.
C o m p l e t e b l o o d c o u n t , r e n a l function test, serum electrolytes, blood sugar, liver function test including serum bilirubin, serum transaminases, prothrombin time and serum proteins were normal. Urine examination was found to be normal. Serum ammonia level was 36 µgm/dl. HIV, HBsAg and Hepatitis C tests were negative. Vitamin B12 and folate levels were normal. Thyroid function tests were within normal limits.
CSF examination revealed cell count less than 5 cells, all being mononuclear cells, proteins- 41 mg/dl and sugars-66 mg/dl. Abdominal ultrasound showed presence of multiple liver abscesses, one of which was aspirated and found to be sterile on culture.
EEG was suggestive of generalized e p i l e p t i f o r m d i s c h a r g e s . N e r v e conduction study showed sensory axonal affection of bi lateral sural nerves and right ulnar nerve. Since the patient’s metabolic parameters were normal, clinical examination, normal LFT and serum ammonia levels ruled out hepatic encepathlopathy, prolonged metronidazole use was thought to be cause of the neurological features.
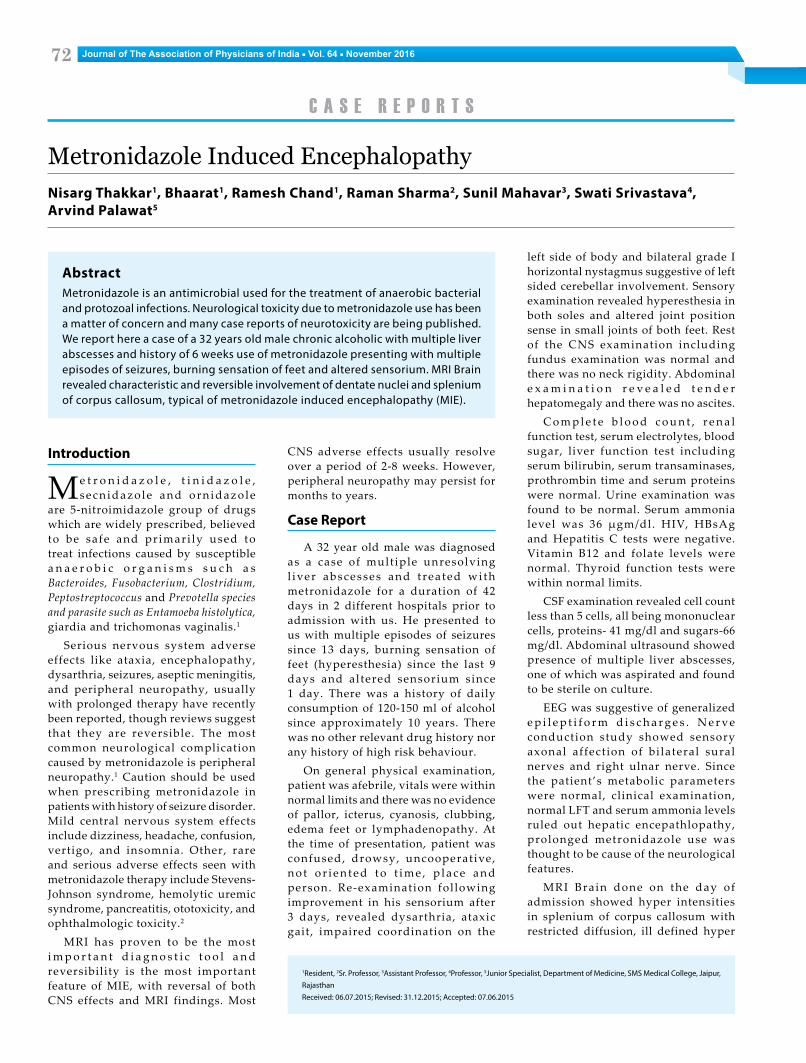
MRI Brain done on the day of admission showed hyper intensities in splenium of corpus callosum with restricted diffusion, ill defined hyper
CNS adverse effects usually resolve over a period of 2-8 weeks. However, peripheral neuropathy may persist for months to years.
Case Report
A 32 year old male was diagnosed as a case of mult iple unresolving l iver abscesses and t rea ted wi th metronidazole for a duration of 42 days in 2 different hospitals prior to admission with us. He presented to us with multiple episodes of seizures since 13 days, burning sensation of feet (hyperesthesia) since the last 9 days and altered sensorium since 1 day. There was a history of daily consumption of 120-150 ml of alcohol since approximately 10 years. There was no other relevant drug history nor any history of high risk behaviour.
On general physical examination, patient was afebrile, vitals were within normal limits and there was no evidence of pallor, icterus, cyanosis, clubbing, edema feet or lymphadenopathy. At the time of presentation, patient was confused, drowsy, uncooperative, n o t o r i e n t e d t o t i m e , p l a c e a n d person. Re-examination fol lowing improvement in his sensorium after 3 days, revealed dysarthria, ataxic gait, impaired coordination on the
c a S e r e P o r t S

Journal of The Association of Physicians of India ■ Vol. 64 ■ November 2016 73
Fig. 1: MRI brain showing T2-hyper intensities in corpus callosum and cerebellum
intensi t ies were seen in bi lateral dentate nuc le i (L>R) wi thout any evidence of restricted diffusion in T2 weighted image (Figure 1). These MRI findings were consistent with the diagnosis of metronidazole induced encephalopathy.
M e t r o n i d a z o l e t h e r a p y w a s discontinued following which there was a considerable improvement in his sensorium and he was able to walk with support in 4 days and without support in 10 days. Seizures were controlled by phenytoin but peripheral neuropathy persisted.
A fol low up MRI after 10 days showed resolution of hyper intensities of dentate nuclei with reduced hyper intensi t ies in splenium of corpus cal losum (Figure 2) suggestive of reversibility and further confirming the likelihood of Metronidazole being the culprit.
Discussion
Metronidazole i s avai lable for treatment in anaerobic infections but may produce a number of neurologic side effects particularly after prolonged use, such as cerebellar involvement, encephalopathy, seizures, autonomic n e u r o p a t h y , o p t i c n e u r o p a t h y , a n d p e r i p h e r a l n e u r o p a t h y . T h e neuropathy induced by metronidazole is predominantly sensory. Symptoms of neuropathy may recover completely or partially after discontinuation of metronidazole.3
The incidence of MIE is unknown. Patients who already have risk factors like alcoholism and uremia are more p r o n e t o d e ve l o p m e t r o n i d a z o l e toxicity.4 The duration of treatment with metronidazole before appearance of CNS toxicity is variable (1 week to 6
months), and cumulative doses range from 25 g to 110 g.5 Patients with severe hepatic dysfunction are at an increased risk of accumulation and may be at an increased risk of metronidazole-induced encephalopathy, even with short-course therapy.1 In our case, total dose of metronidazole that the patient received was 39.3 gm and total duration was 42 days. It has been suggested that metabolites of metronidazole may bind to RNA instead of DNA, possibly inhibiting RNA protein synthesis, which could potentially lead to axonal degenera t ion . Another proposed mechanism involves the modulation of the inhibitory neurotransmitter gamma-aminobutyric acid(GABA) receptor within the cerebellar and vestibular systems.6,7 Although the mechanism of metronidazole neurotoxicity remains unclear , most les ions induced by metronidazole neurotoxicity may be reversible. The reversible changes associated with the acute toxic effects of metronidazole are most likely due to axonal swelling with increased water content rather than a demyelinating process. Another suggested mechanism involves vascular spasm that could produce mild reversible localized ischemia.
Characteristic MRI Brain findings are best visualised in T2 weighted images. Hyperintense lesions most commonly involve the cerebellar dentate nuclei. The midbrain, dorsal pons, dorsal medulla, and corpus callosum can also be affected. Uncommon locations include the inferior olivary nucleus and the white matter of the cerebral hemispheres.5,8 Lesions are always symmetric and bilateral, a pattern typical of metabolic encephalopathy. The differential diagnosis of, bilaterally symmetrical hyperintense lesions in T2
dentate nuclei includes methyl bromide intoxication, maple syrup urine disease and enteroviral encephalomyelitis, m u l t i p l e s c l e r o s i s a n d a c u t e disseminated encephalomyelitis. The differential diagnosis of T2 hyperintense lesions in the splenium of the corpus callosum includes Marchiafava-Bignami disease, encephalitis (demyelination, influenza, Escherichia coli , mumps, adenovirus, Epstein-Barr virus and Rota virus), osmotic myelinolysis, acute toxic encephalopathy and anti-epileptic drugs.9
Data extrac t ion of 64 pat ients o f n e u r o l o g i c a l t o x i c i t y d u e t o metronidazole, from 1965 to 2011 by Kuriyama et al revealed cerebellar dysfunction in 48 (77%), encephalopathy in 21 (33%) and seizures in 8 (15%).11
J . C h a c k o e t a l d i s c u s s e d 2 cases of 5- nitroimidazole induced encephaloneuropathy. Characteristic MRI findings along with reversibility was also a feature in their reports.11
Discontinuing metronidazole and supportive measures is the primary treatment, no specific therapy however is available for MIE. There has been no evidence of usefulness of steroid therapy for MIE. Most patients recover between 3 and 16 weeks after stopping the drug with resolution of abnormal MRI lesions.10
In our case, on the basis of history of unresolving multiple liver abscesses and chronic alcoholism, differential diagnosis of HIV Encephalopathy a n d We r n i c k e ’ s e n c e p h a l o p a t h y respectively were considered. However, MRI Brain findings and absence of ophthalmoplagia were not in favour of wernicke’s encephalopathy and HIV serology was negative. Chronic alcoholism being an additional cause of peripheral neuropathy in our case could not be ruled out.
Conclusion
M e t r o n i d a z o l e i n d u c e d e n c e p h a l o p a t h y a n d p e r i p h e r a l neuropathy should be considered in any patient who presents with seizures, cerebellar features, altered sensorium, symptoms of distal pure sensory involvement and is receiving prolonged therapy with metronidazole. MRI should be performed for definitive diagnosis and reversibility of lesion in MRI should be looked for.
M e t r o n i d a z o l e s h o u l d b e
