case report antenatal so no graphic diagnosis of meconium
TRANSCRIPT
8/3/2019 Case Report Antenatal So No Graphic Diagnosis of Meconium
http://slidepdf.com/reader/full/case-report-antenatal-so-no-graphic-diagnosis-of-meconium 1/3
CASE REPORTS 47 7
Clinical Radiology (1997) 52, 477-479
Case Report: Antenatal Sonographic Diagnosis of Meconium
Peritonitis and Subsequent Evolving Meconium Pseudocyst
Formation Without Peritoneal Calcification
W. T. YANG , S . S . Y. HO* and C . MET REW EL I t
Department of Diagnostic Radiology, *Department of Diagnostic Radiology and Organ Imaging and ~Department ofDiagnostic Radiology and Organ Imaging, Chinese University of Hong Kong Prince of Wales Hospital, Shatin, Hong
Kong
A case of g iant meconium pseudocyst secondary to rupture
from in tes t inal obstruct ion d iagnosed by in utero sonogra-
phy is presented_ The diagnosis of intestinal obstruction was
made in the late second t r imester before development of
polyhydramnois , and the d iagnosis of meconium cyst made
in the th ird t r imester despi te the abse nce of in tra-abdom inal
calcif icat ion . Exploratory laparotomy immediately after
b ir th revealed a g iant pseudocyst at the s i te of rupture
immediately proximal to d is tal i leal at res ia with associated
in utero volvulus .
Conventional radiographic features of meconium peri to-
ni t is with secondary meconium cyst formation are well
described [1- 6]. With the advent of h igh resolut ion real
t ime ul t rasound (US), the special ro le of sonography in
detect ing congenital malformations in utero has been es tab-
l ished. We p resent a case in which sonographic d iagnosis of
in test inal obstruct ion was m ade at 27 weeks gestat ion before
the developmen t of polyhydram nois , and a sonographic
d iagnos i s o f mecon ium pseudocys t was made a t 36 weeks
gestat ion despi te the absence of in tra-abdominal
calcification.
Laparotomy at 10 h of life conf irmed ileal atresia wi th associated volvulus
and a large pseudocyst at the rupture site in the distil ileum. Small bowel
resection and anastomosis were performed after 500 ml of greenish brown
fluid were drained fi'om the pseudocyst. Patholog y of the resecte d small
bowel spec imen did not reveal a ny calcification intraluminally or on the
serosal surface. The baby recovere d well postoperati vely and has achieved
normal developmental milestones. Subsequently, a sweat test was normal.
Discussion
The incidence of congenital small bo wel atres ia is 0.38 in
10 000 newborn s [7] and the preva lence of neonatal me co-
nium peritonitis is estimated at one in 30 000 live births [8].
On sonography, fetal bowel obstruct ion characteris t ical ly
consis ts of d i lated sonolucent masses occupying the fetal
abdominal cavi ty asymmetrical ly , with associated polyhy-
dramnois [7]. The differential diagnosis includes a dis-
tended urinary b ladder, usual ly in the middle of the lower
abdomen, and mesenteric and ovarian cysts , usual ly located
to one s ide of the abd ominal cavi ty . Dilated loops f i l l ing the
abdominal c avi ty suggest obstruct ion of the small bowel .
Case Report
A 31-year-old Chinese gravida 2 para I with an uneventful previous
pregnancy and delivery, who was visiting Hong Kong presented to the
antenatal US scree ning clinic at 27 weeks gestati on for fetal anoma ly
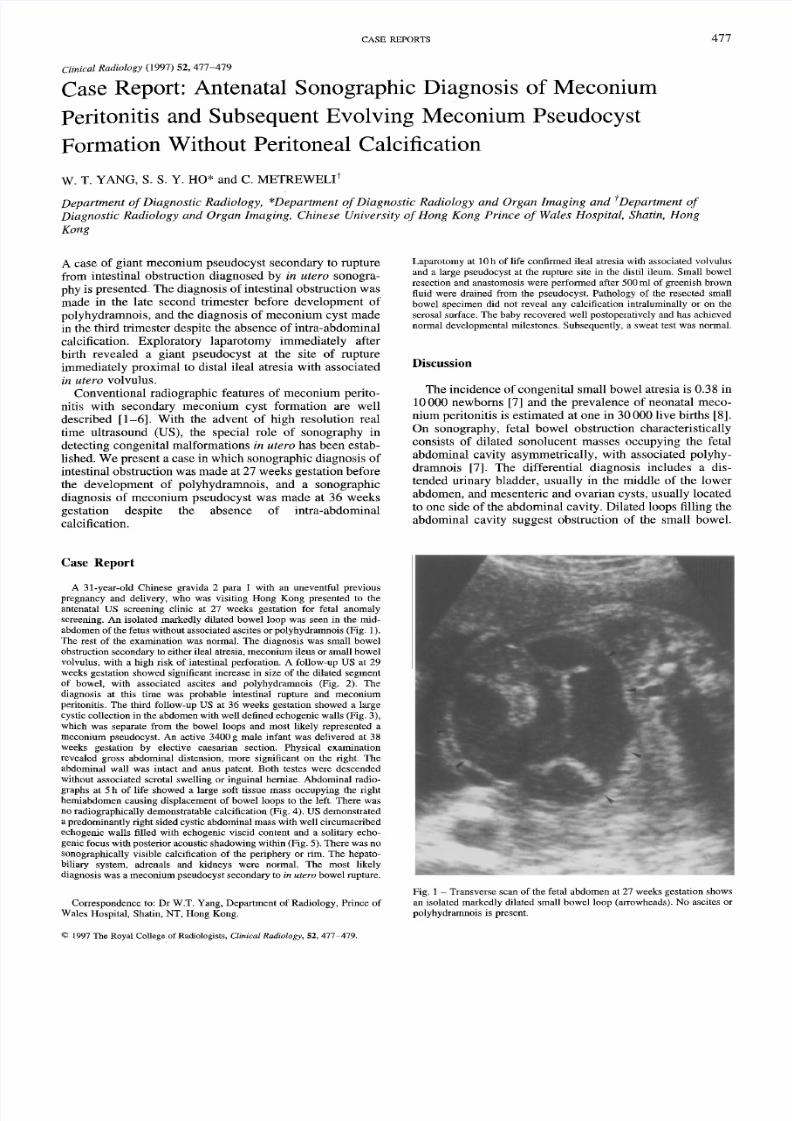
screening. A n isolated markedly dilated b owel loop was see n in the mid-
abdomen of the fetus without associated ascites or polyhydra mnois (Fig. 1).
The rest of the examination was normal. The diagnosis was small bowel
obstructi on seconda ry to either ileal atresia, me conium ileus or small bowel
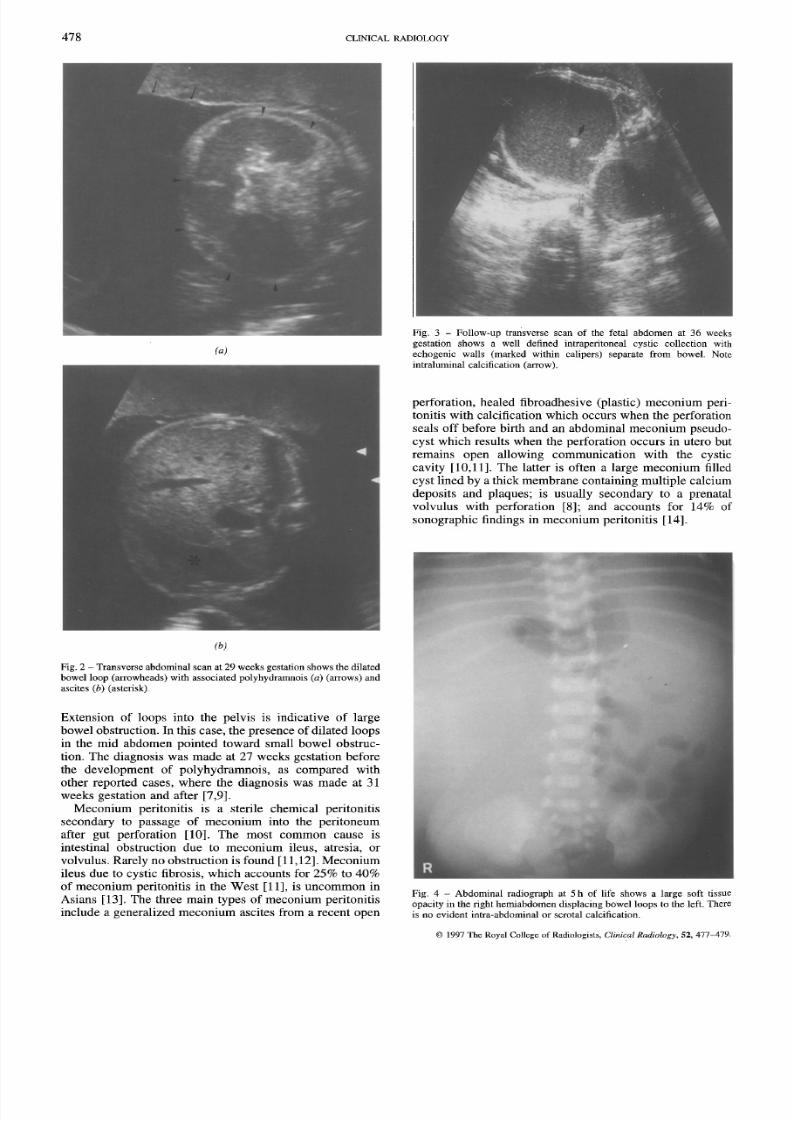
volvulus, wi th a high risk of intestinal perforation. A follow-up US at 29
weeks gestation sh owe d significant increase in size of the dilated segme nt
of bowel, with associated ascites and polyhydranmois (Fig. 2). The
diagnosis at this time was probable intestinal rupture and meco niumperitonitis. The third follow-up US at 36 week s gestation sho wed a large
cystic collection in the abdomen with well defined echogenic walls (Fig. 3),
which was separate from the bowel loops and mos t likely represented a
meco nium pseudocys t. An active 3400 g male infant was delive red at 38
weeks gestation by elective caesari an section. Physical examina tion
revealed gro ss abdominal distension, more significant on the fight The
abdominal wall was intact and anus patent. Both testes were descende d
without associa ted scrotal swe lling or inguinal herniae_ Abdomin al radio-
graphs at 5 h o f life showed a large soft tissue mass occupying the right
hemiabdomen causing displacement of bowel loops to the left_ There w as
no radiograplucally demonstra table calcification (Fig. 4). US demonstrated
a predominantly right sided cystic abdominal mass with well circ umscribed
echogenic walls filled with echogenic viscid content and a solitary echo-
genic focus with poster ior acoustic sha dowing within (Fig. 5). There was no
sonogra phicall y visible calcification of the periphery or rim. The hepato-
biliary system, adrenals and kidneys were normal. The most likely
diagnosis was a mec onium pseudocyst secondary to in utero bowel rupture.
Corres pondenc e to: Dr W.T. Yang, Department of Radiology, Prince of
Wales Hospital, Shatin, NT, Hong Kong.
© 1997 The Royal College of Radiologists,Clinical Radiology, 52, 477 479.
Fig. 1 - Transverse scan of the fetal abdomen at 27 weeks gestation shows
an isolated markedly dilated small bowel loop (arrowheads). No ascites or
polyhydrarnnois is present.
8/3/2019 Case Report Antenatal So No Graphic Diagnosis of Meconium
http://slidepdf.com/reader/full/case-report-antenatal-so-no-graphic-diagnosis-of-meconium 2/3
8/3/2019 Case Report Antenatal So No Graphic Diagnosis of Meconium
http://slidepdf.com/reader/full/case-report-antenatal-so-no-graphic-diagnosis-of-meconium 3/3
CASE REPORTS 4 79
the third antenatal ul t rasound was performed soon after the
deve lopm ent of the pseud ocys t and before ca lc i f ica t ion had
been deposi ted in sufficient quant i ty to be vis ible radio-
graphical ly or echographical ly. Although calcif icat ion may
develop within days his tological ly, radiographic and sono-
graphic eviden ce of calcif icat ion usual ly requires weeks
[4,21].
In conc lus ion , the d iagnos i s of mecon ium pseudo-
cyst should be considered in the set t ing of fetal bowe lobstruct ion with sequent ial polydramnois , asci tes and
cys t format ion , even in the absence of in t ra -abdomina l
calcification.
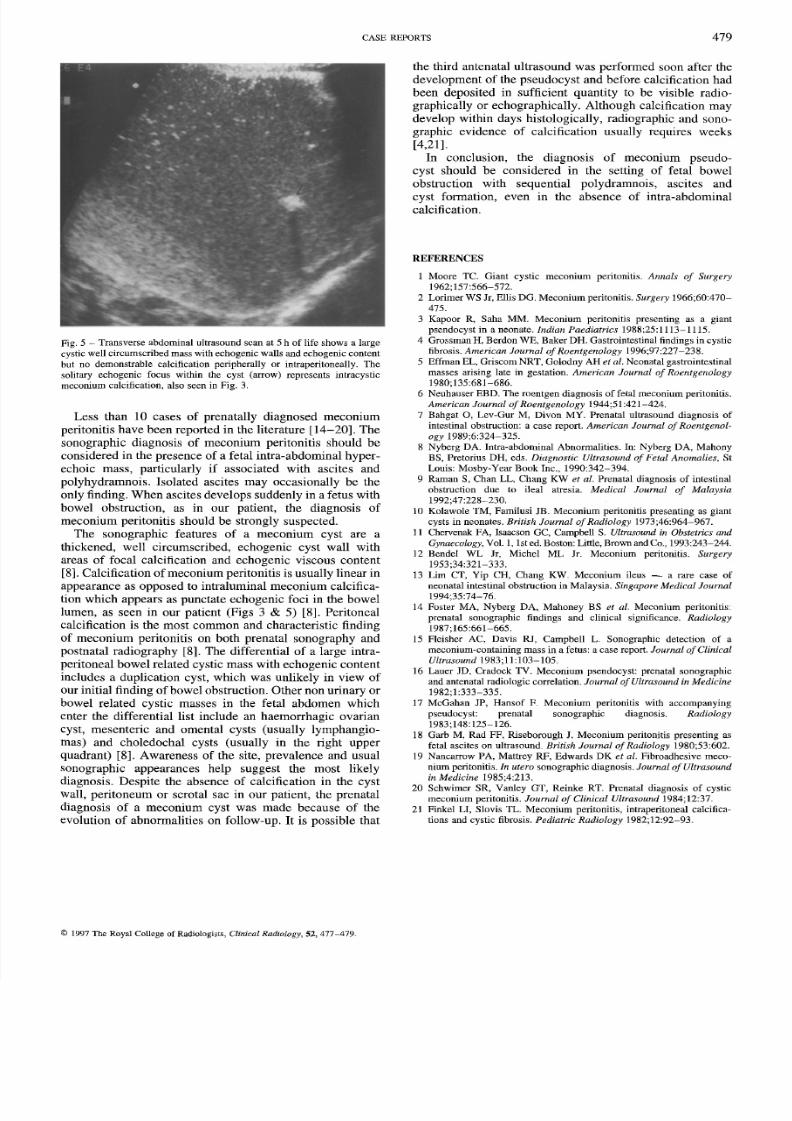
Fig . 5 - Transver se abdominal u l t rasound scan a t 5 h of l i fe shows a large
cyst ic wel l c i rcumscribed mas s wi th echogenic wal ls and echogenic content
but no demonst rab le ca lc i f ica t ion peripheral ly or in t raperi toneal ly . The
sol i tary echogenic focus wi th in the cyst (arrow) represents in t racyst ic
meco nium calc i f ica t ion , a l so seen in Fig . 3 .
Less than 10 cases of prena ta l ly d iagnosed m econium
peri toni t is have been reported in the l i terature [14-20]. The
sonographic d iagnos is of meconiu m per i toni t is should be
considered in the presence of a fetal intra-abdominal hyper-
echoic mass , part icularly i f associated with asci tes and
polyhydramnois . I so la ted asc i t es may occas iona l ly be the
only f inding. W hen asci tes develop s suddenly in a fetus with
bowel obstruct ion, as in our pat ient , the diagnosis of
meconium peri toni t is should be s t rongly suspected.The sonographic fea tures of a meconium cys t a re a
thickened, wel l c i rcumscribed, echo genic cys t wal l with
areas of focal calcif icat ion and echogenic viscous content
[8] . Calcif icat ion o f mecon ium peri toni t is is usual ly l inear in
appearance as opposed to in t ra lumina l me conium ca lci f ica -
t ion which appears as punctate echogenic foci in the bowel
lumen, as seen in our patient (Figs 3 & 5) [8]. Peritoneal
calcif icat ion is the most common and characteris t ic f inding
of meconium per itoni ti s on both prena ta l sonography and
postnatal radiography [8] . The different ial of a large intra-
peri toneal bowel related cys t ic mass with echogenic content
includes a dupl icat ion cys t , which was unl ikely in view of
our init ia l f inding of bow el obstruct ion. Other non u rinary or
bowel related cys t ic masses in the fetal abdomen which
enter the different ial l is t include an haemorrhagic ovarian
cyst , mesenteric and omental cys ts (usual ly lymphangio-
mas) and choledochal cys ts (usual ly in the f ight upper
quadrant) [8] . Awaren ess of the s i te , prevalence and usual
sonographic appearances he lp sugges t the mos t l ike ly
diagnosis . Despi te the absence of calcif icat ion in the cys t
wal l , peri toneum or scrotal sac in our pat ient , the prenatal
d iagnos i s of a meconium cys t was made because of the
evolut ion of abnormali t ies on fol low-up. I t i s poss ible that
REFERENCES
1 Moore TC. Giant cyst ic meconium peri ton i t i s . Annals of Surgery_
1962;157:566-572.
2 Lorimer WS Jr , El l i s DG. M econ ium periton i ti s . Surgery 1966;60:470-
475.
3 Kapoor R, Saha MM. Mec onium peri ton i t is present ing as a g ian t
psendocyst in a neonate . Indian Paediatrics 1988;25:1113-1115.
4 Grossm an H, Berdon WE, Baker DH. Gast ro in test inal f ind ings in cyst ic
fibrosis. American Journal of Roentgenology 1996;97:227-238.
5 Ef fman EL, G r i sco m N R T, G o l o d n y A H et al. Neonata l gast ro in testinal
masses ari s ing la te in gesta t ion . American Journal of Roentgenology
1980;135:681-686.
6 Neuhause r EBD. The roentgen d iagnosis of fe tal mecon ium peri ton i ti s .
American Journal of Roentgenology 1944;51:421-424.
7 Bahgat O, Lev-Gur M, D ivon MY. Prenata l u l t rasound d iagnosis of
intestinal obstruction: a case report. American Journal of Roentgenol-
ogy 1989;6 :324-325.
8 Nyberg DA. In t ra-abdominal Abnormal i t ies . In : Nyberg DA, Mahony
BS, Pre torius DH, eds. Diagnostic Ultrasound of Fetal Anomalies, St
Louis: Mosby-Y ear Book Inc ., 19 90:342-394.
9 R aman S , C h an LL , C h an g K W et al. Prenata l d iagnosis of in test inal
obstruction due to i leal atresia. Medical Journal of Malaysia
1992;47:228-230,
10 Kolawole TM, Familusi JB. Meconium peri ton i t i s present ing as g ian t
cysts in neonates . British Journal of Radiology 1973;46:964-967.11 Chervenak FA, Isaacson GC, Cam pbell S. Ultrasound in Obstetrics and
Gynaecology, Vol. 1, 1st ed. Boston: Little, Bro wn and Co., 1993:24 3-24 4.
12 Bendel W L Jr, M ichel M L Jr . Mecon ium peri toni t is . Surgery
1953;34:321-333.
13 Li ra CT, Yip CH, Chang KW. Me coniu m i leus -- a rare case of
neonata l in tesUnal obst ruct ion in Malaysia . Singapore Medical Journal
1994;35:74-76 .
1 4 Fo s t e r M A , N y b e rg D A , M ah o n ey B S et al. Meconium peri ton i t i s :
prenata l sonographic f ind ings and c l in ical s ign i ficance. Radiology
1987;165:661-665.
15 Fle isher AC, Davis RJ, Campbel l L. Sonographic detect ion of a
meconium -conta in ing mass in a fe tus: a case report. Journal of Clinical
Ultrasound 1983; 11:103 - 105.
16 Laner JD, Cradock TV. Meconium psendocyst : p renata l sonographic
and antenatal radiologic correlation. Journal of Ultrasound in Medicine
1982;1 :333-335.
17 McGa han JP, Hansof F Mec onium peri ton it i s with accompan ying
pseudocyst : p renata l sonographic d iagnosis . Radiology
1983;148:125-126.
18 Garb M, R ad FF, Riseborou gh J . Mec onium peri ton it i s present ing as
fe ta l ase i tes on u l t rasou nd British Journal of Radiology 1980;53:602.
19 Nancarrow PA, Mat t rey RF, Edwards DK et al. Fibroadhesive meco-
nium peritonitis. In utero sonographic d iagnosis . Journal of Ultrasound
in Medicine 1985;4:213,
20 Schwimer SR, Vanley GT, Reinke RT. Prenata l d iagnosis of cyst ic
meco nium peri ton i t is . Journal of Clinical Ultrasound 1984;12:37.
21 Finkel LI, Slovis TL. M econi um peri ton i t is , in t raperitoneal ca lc if ica-
tions and cystic fibrosis. Pediatric Radiology 1982;12:92-93 .
© 1997 The Royal College of Radiologists, Clinical Radmlogy, 52, 477-479.