case presentation - suny downstate medical center · case presentation diagnosis of large ......
TRANSCRIPT
Case Presentation
Joseph M Brandel, MDKings County Hospital CenterDepartment of SurgeryFriday, July 15, 2005

Case Presentation
52-year-old African American male presenting with a 5-day history of abdominal distention associated with nausea, vomiting, and absence of passage of feces or flatus
PMHx: NonePSHx: NoneMeds: NoneSocial: Nonsmoker, occasional drinker

Case Presentation
Vitals:Temp 98.2°F HR 88 BP 131/70 RR 20
Physical exam:General: Thin male, alert, in mild distressHEENT: NC/ATHeart: RegularLungs: ClearAbdomen: Grossly distended, tympanic, nontender, absent bowel soundsRectal: Normal tone, guaiac (+)
Case Presentation
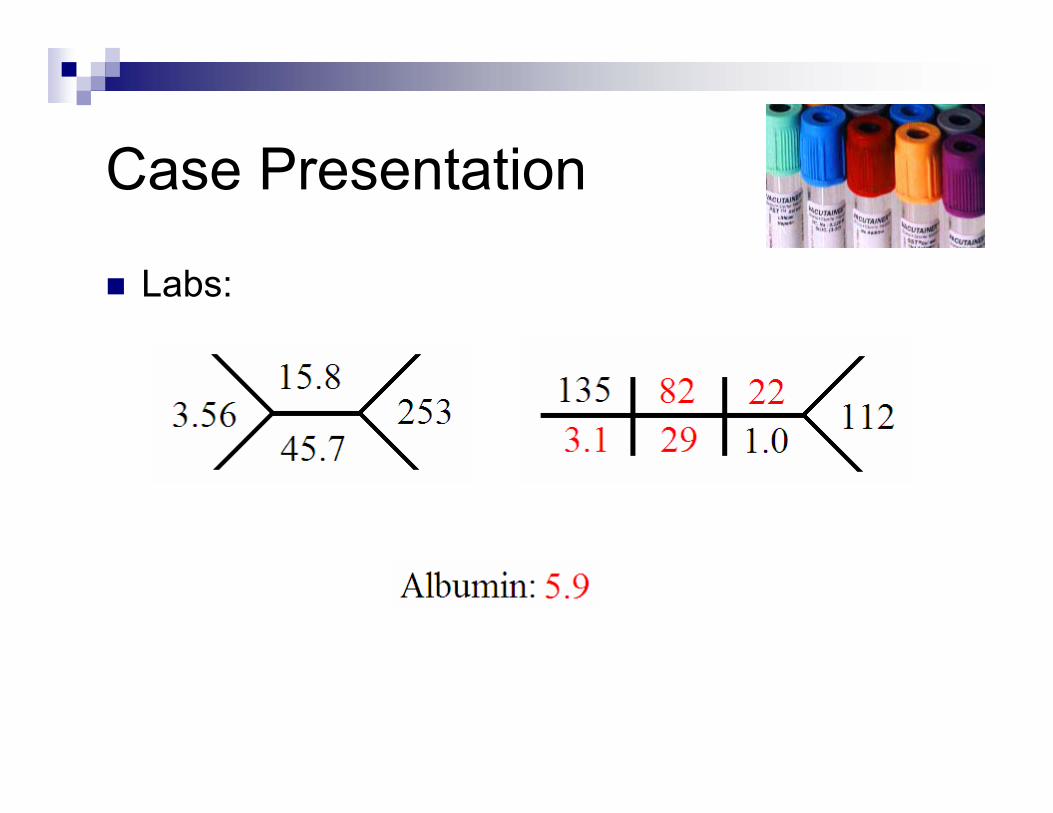
Labs:

Case Presentation

Case Presentation

Case Presentation

Case Presentation

Case PresentationDiagnosis of large bowel obstruction madeResuscitation
Intravenous salineFoley catheter
Taken to ORExploratory laparotomy through midline approachProminent small bowel dilatation, ascitesDiscrete mass in sigmoid colon identifiedMass resectedPrimary stapled anastomosis performed
PathologyColonic adenocarcinoma, T3N1

Case Presentation
Post-op coursePOD #0: Fever, hypotensionPOD #6: Enteral feeding initiatedPOD #12: ExtubatedPOD #22: Discharged home

Obstructing Colon Cancers

IntroductionColorectal cancer #2 cause of cancer mortality among men and women in the United States Surgery should ideally be electiveOver 15% of colorectal cancers present as acute colonic perforation or obstruction Emergency surgery associated with poorer prognosis
Postop mortality rate of 8.2% Lower 5-year survival
McArdle CS, Hole DJ. Emergency presentation of colorectal cancer is associated with poor 5 year survival.Br J Surg 2004;91(5):605–9.

Introduction
c
8%Stage IV
44%Stage IIIC
64%Stage IIIB
83%Stage IIIA
72%Stage IIB
85%Stage IIA
93%Stage I
M1 means distant metastasis has occurred.M1
M0 signifies no distant metastasis.M0
MX means distant metastasis cannot be assessed.MX
N2 means metastasis has occurred in 4 or more regional lymph nodes.
N2
N1 signifies metastasis in 1 to 3 regional lymph nodes.
N1
NO means no regional lymph node metastases.NO
NX means regional lymph nodes cannot be assessed.NX
The tumor has invaded other organs or structures.T4
The tumor has invaded through the muscularispropria into the subserosa or into non-peritonealizedpericolic or perirectal tissues.
T3
The tumor has invaded the muscularis propria.T2
The tumor has invaded the submucosa.T1
Tis means carcinoma in situ; the cancer cells are localized and superficial, but have no capacity to spread; it is considered high-grade or severe dysplasia.
Tis
There is no evidence of primary tumor.TO
The primary tumor cannot be assessedTX
any T, any N, and M1Stage IVDukes D
any T, N1 or 2, and M0Stage IIIDukes C
T3, N0, M0 and T4, N0, M0Stage IIDukes B
T1, N0, M0 and T2, N0, M0Stage IDukes A

Introduction
Patients presenting as emergencies:
More advanced tumorsOlderWidowedWorse pre-existing cardiopulmonary disease
Scott NA, Jeacock J, Kingston RD. Risk factors in patients presenting as an emergency with colorectal cancer. Br J Surg 1995;82(3):321–3.

Physiology of LBOCirculatory changes
Increased intraluminalpressure → decreased venous return → mucosal ischemia
MicroorganismsIncreased intraluminalmicrobiomassTranslocation to mesenteric nodes common
In 43% of patients with post-op sepsis cultures of mesenteric nodes and peripheral blood grow out the same organism

Physiology of LBO
MotilityInitial increase proximal to obstruction followed by decrease
Fluids and electrolytesIntraluminal fluid sequestrationVomiting if ileocecalvalve incompetent

PresentationSymptoms of large bowel obstruction:
Abdominal painDistentionConstipationVomiting
Symptoms may occur acutely or chronically May present in extremis:
Severe dehydrationMassive abdominal distentionPeritonitis
Perforation at either at tumor site or at cecum

Presentation
Etiology:Colorectal cancer (50%) VolvulusDiverticular diseaseHerniaFecal impaction

Diagnosis
CBCMay reveal leukocytosisHemoglobin may be low or high
X-rayMay demonstrate LBOCannot exclude pseudo-obstruction
CTMay elucidate nature of obstruction± Contrast enema
OR
Treatment: ResuscitationPhysiologic status upon presentation is primary determinant of outcomeColonic obstruction is associated with volume depletion, electrolyte imbalances
Administration of crystalloid or colloid, Foley, central lineBlood transfusion?
More than two units may be associated with increased death from colorectal cancer1
Extended resuscitation not helpfulNo significant difference between those having immediate surgery and those in whom it was delayed 24 hours2
1 Edna T, Bjerkeset T. Perioperative blood transfusions reduce long-term survival following surgery for colorectal cancer. Dis Colon Rectum 1998;41(4):451–9.2 Kingston RD, Jeacock J, Walsh SH. Physical status is the principal determinant ofoutcome after emergency admission of patients with colorectal cancer. Ann RCS of England 1993;75(5):335–8.

Treatment: Surgery
Leon Ginzburg (1955)“Opinion almost unanimously favors preliminary decompression for acute obstruction.”However, “in the right colon, indications for elective staging arise very rarely… in my opinion the only indication for such a procedure would be free perforation…”For left-sided lesions, on the other hand, only “three types of stage operations are available”.
References: None
Ginzberg L. The role of stage procedures in resection or carcinoma of the large bowel. Surg Clin of NA 1955
October:1307-1314

Treatment: Surgery
Questionnaires sent to 500 US-based surgeons to assess prevailing practices for obstructing cancers of the left colon
For “good-risk” patients:47% staged resection26% segmental resection with on-table lavage18% segmental resection without on-table lavage10% subtotal colectomy
For “poor-risk” patients94% staged resection
Goyal A, Schein M. Current practices in left-sided colonic emergencies: a survey of US gastrointestinal surgeons. Dig Surg. 2001;18(5):399-402.

Tradition

Treatment: Surgery
Right-sided lesions25% of colorectal cancers are right-sidedMultiple nonrandomized, noncontrolledcase series demonstrated right hemicolectomy with anastomosis is safe and effective
Anastomotic leakage rate ~5%Performing anastomosis dependent on the patient's general condition
Otchy D, Hyman NH, Simmang C, Anthony T, Buie WD, Cataldo P, Church J, Cohen J, Dentsman F, Ellis CN,
Kilkenny JW 3rd, Ko C, Moore R, Orsay C, Place R, Rafferty J, Rakinic J, Savoca P, Tjandra J, Whiteford M.
Practice parameters for colon cancer. Dis Colon Rectum 2004 Aug;47(8):1269-84.

Treatment: Surgery
Left-sided lesionsSurgical management subject to debate
3-stage2-stage Subtotal colectomy with ileo-rectal anastomosisSegmental resection with primary anastomosis
With or without on-table lavage

Treatment: Surgery
3-stage procedureProximal diversion, then resection, then reversalOf historic interest onlyHigh cumulative mortality (up to 31%)Worse long-term survival due to delay in resection
Fielding LP, Stewart-Brown S, Blesovsky L. Large-bowel obstruction caused by cancer: a prospective study. BMJ 1979;2: 515–517.

Treatment: Surgery2-stage procedure
Advantage: No risk of anastomotic leak at initial operation
Disadvantages:2 stagesRestoration of intestinal continuity inconsistent (17 to 70%)Complications of colostomy
Lee Y, Law W, Chu K, Poon R. Emergency surgery for obstructing colorectal cancers: a comparison between right sided and left sided lesions. Journal of the American College of Surgery 2001;192(6):719–25.

Complications of colostomy
Skin excoriationNecrosisRetractionStenosisProlapseParastomalhernia

Treatment: Surgery
1-stage: Subtotal colectomyAdvantages:
Remove synchronous tumorsPrevent metachronous tumorsGood results (mortality 3 to 11%; leak rate 5%)
Disadvantages:Increased bowel dysfunction (diarrhea)
Halevy A, Levi J,Orda R. Emergency subtotal colectomy. A new trend for treatment of obstructing carcinoma of the leftcolon. Ann Surg 1989;210:220–223.
Treatment: Surgery1-stage: Antegrade colonic lavage
Advantages:Duplicates bowel prep of elective surgeryMortality compares favorably with 2-stage procedureAnimal studies reveal higher anastomotic bursting pressures and higher hydroxyproline content
Disadvantages:Extends procedure by 30-45 minutesNot feasible in all patients
Meijer S, Hoitsma HFW, Van Loenhout RM. Intraoperative antegrade irrigation in complicated left sided colonic cancer. Journal of Surgical Oncology 1989;40(2):88–9.

Treatment: SurgeryLee, et al. (2001)
Retrospective review of 243 consecutive patients81% treated with 1-stage resectionNo difference in mortality for right- and left-sided obstructionIn line with historic controls
Lee Y, Law W, Chu K, Poon R. Emergency surgery for obstructing colorectal cancers: a comparison between right sided and left sided lesions. Journal of the American College of Surgery 2001;192(6):719–25.

Treatment: SurgeryLee, et al. (2001)
Retrospective review of 243 consecutive patients81% treated with 1-stage resectionNo difference in mortality for right- and left-sided obstructionIn line with historic controls
Lee Y, Law W, Chu K, Poon R. Emergency surgery for obstructing colorectal cancers: a comparison between right sided and left sided lesions. Journal of the American College of Surgery 2001;192(6):719–25.

Treatment: SurgerySegmental resection without lavage
Naraynsingh, et al. (1999) reported 58 consecutive patients with obstructing left-sided lesions
1 anastomotic leak1 death secondary to MI
Naraynsingh V, Rampaul R, Maharaj D, Kuruvilla T, Ramcharan K, Pouchet B. Prospective study of primary
anastomosis without colonic lavage for patients with an obstructed left colon. Br J Surg. 1999 Oct;86(10):1341-3.

Treatment: SurgerySegmental resection without lavage
Patriti, et al. (2005):44 consecutive patientsExclusion criteria were haemodynamicinstability, ASA > 3, or unresectable tumorLeak rate 4.5%Mortality rate 2.3% (MI)
Patriti A, Contine A, Carbone E, Gulla N, Donini A. One-stage resection without colonic lavage in emergency surgery
of the left colon. Colorectal Dis. 2005 Jul;7(4):332-8.
Treatment: Endoscopy
Indications:Palliation“Bridge to surgery”
Techniques:Pneumatic or mechanical dilatationElectrocoagulationNd-YAG laser
Effective palliation92% have symptoms relieved by Nd-Yag; 88% of survivors continue to experience relief at follow-up
Tan CC, Iftikhar SY, Allan A, Freeman JG. Local effects ofbcolorectal cancer are well palliated by endoscopiclaser therapy. European Journal ofSurgery 1995;21(6):648–52.

Treatment: EndoscopySelf-expanding metallic stents
Definitive for palliationOtherwise temporizing
Efficacy:“Technical success” rate 94%“Clinical success” rate 91%
Drops to 72% when used as bridge to surgery
Complications:Perforation (4%)Stent migration (12%)Reobstruction (7%)
Sebastian S, Johnston S, Geoghegan T, Torreggiani W, Buckley M. Pooled analysis of the efficacy and safety of self-expanding metal stenting in malignant colorectal obstruction. Am J Gastroenterol. 2004 Oct;99(10):2051-7.

Conclusions
Large bowel obstruction is a disease entity frequently encountered by the general surgeonThe choice of operation, particularly for malignant left-sided obstructions remains controversialA single-stage operation with primary resection and anastomosis can be performed in many patients with obstructive colonic cancers; however, the judgment of the surgeon is integral to the management of this entity
