case presentation · fetal pulmonary blood flow is characterized as a low-flow high-resistance...
TRANSCRIPT

Case Presentation 4yF with trisomy 21 p/w cough, congestion, wheezing for several days. Intermittent difficulty breathing for last two months. No fever, chills, N/V/D/C. PMH: trisomy 21, seizures; full term vaginal delivery PSH: repair VSD and coarctation DOL#5, reaugmentation coarctation DOL#150, repair chylothorax DOL#152, plication of left hemidiaphragm for paresis DOL#158, gastrostomy DOL#172 Meds: albuterol, pulmicort, prednisolone, azithromycin
www.downstatesurgery.org

Physical and Labs • T98.8, HR103, BP104/62, RR22, Sat97 • 33inch (<3%), 22.7lb (<3%) • NAD • Coarse breath sounds left side • Abdomen soft NT ND • Well healed sternotomy, left posterolateral
thoracotomy and gastrostomy scars
• CBC 17/13/39/319
www.downstatesurgery.org

Chest XR www.downstatesurgery.org

Chest CT www.downstatesurgery.org

Operation
• Left subcostal incision • Left posterolateral diaphragmatic defect identified • Small and large bowel reduced • Hernia sac excised • Chest tube placed • Defect closed with interrupted 0 and 2-0 silk • No malrotation identified
www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

Postoperative Course
• POD#0 Admitted to PICU • POD#3 Return of bowel function • POD#4 Chest and nasogastric tubes removed • POD#5 Discharged home
www.downstatesurgery.org

Congenital Diaphragmatic Hernia
Christopher Turner 05.15.14
www.downstatesurgery.org

Overview
• History • Epidemiology • Embryology • Diagnosis • Management • Outcomes
www.downstatesurgery.org

History
1754, McCauley: First description 1925, Hedblom: First review (33/44 mortality, 75%) 1940, Ladd and Gross: First single series with consistent survival (7/16 mortality, 44%) 1946, Gross: First report of successful operative repair in infant younger than 24h
Immediate neonatal surgery standard of care until the 1980s
www.downstatesurgery.org

Ladd and Gross NEJM 1940
www.downstatesurgery.org

Epidemiology
• Incidence 1:2000-5000 • 1/3 die in utero, “hidden mortality” • 90% posterolateral • 85% left, 13% right, 2% bilateral • 50% isolated defect • 27.5% cardiovascular, 17.7% urogenital, 15.7%
musculoskeletal, 9.8% central nervous
www.downstatesurgery.org
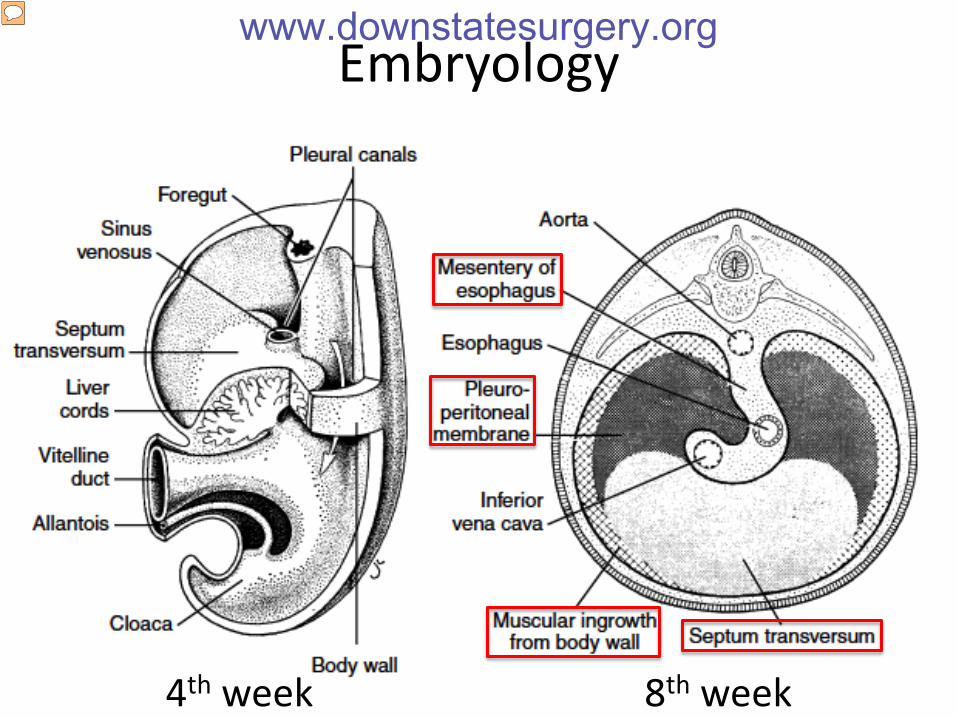
Embryology
4th week 8th week
www.downstatesurgery.org

Pathophysiology
• Diaphragmatic hernia – Posterolateral or Bochdalek – Anterior or Morgagni – Central septum transversum
• Pulmonary hypoplasia • Pulmonary hypertension
www.downstatesurgery.org

Fetal Circulation
• Ductus venosus • Foramen ovale • Ductus arteriosus
www.downstatesurgery.org

Prenatal Diagnosis
• 50-70% diagnosed in pregnancy • US diagnosis as early as 11wks • Findings include polyhydramnios, bowel loops
in chest, echogenic chest mass, intrathoracic stomach, cardiac shift
• Features to risk stratify – Lung-to-head ratio – Liver herniation into chest
www.downstatesurgery.org

Ultrasound www.downstatesurgery.org

MRI www.downstatesurgery.org
Clinical Presentation
• Tachypnea, chest wall retractions, grunting, cyanosis, pallor
• Scaphoid abdomen, increased chest diameter, decreased breath sounds, presence of bowel sounds in chest, displacement of heart sounds
• Typically confirmed with CXR showing bowel loops in chest
• 20% may present outside neonatal period
www.downstatesurgery.org

CXR www.downstatesurgery.org

Prenatal Care
• Advanced US to determine associated anomalies and signs of fetal compromise
• Chromosomal screening • Maternal counseling • Referral to tertiary perinatal center
• Prenatal glucocorticoids not currently
recommended
www.downstatesurgery.org

Stabilization and Monitoring
• Tracheal intubation • CPAP contraindicated • Large bore NGT or OGT • H2 blockers or PPIs • Pulse oximetry probes placed preductally (right
arm or earlobe) and postductally (lower extremities) indicate presence of RL shunt and PHTN
• Consider arterial and venous catheters
www.downstatesurgery.org

ICU Management
• Pressure support with minimal sedation • Limit tidal volume to 4-6cc/kg and peak airway
pressure to 25-30 cm H2O • Maintain preductal pO2>60 and pCO2<60 • Alkalosis with NaHCO3 or THAM improves PHTN • Dopamine or dobutamine may be needed • Systemic antibiotics with ampicillin and
gentamicin • ECMO for persistent hypoxemia or hypotension
www.downstatesurgery.org

Surgery
• Repair is delayed until cardiopulmonary stability
• Open abdominal approach is gold standard • Thoracic or minimally invasive also options • Diaphragmatic replacements include non-
absorbable synthetic, absorbable biosynthetic, autologous tissue, tissue engineered
• 50% require replacement • 50% will recur
www.downstatesurgery.org

www.downstatesurgery.org

Fetal Therapies
• Harrison et al. Correction of Congenital Diaphragmatic Hernia in utero: A Prospective Trial. Journal of Pediatric Surgery, 1997.
• Harrison et al. A Randomized Trial of Fetal Endoscopic Tracheal Occlusion for Severe Fetal Congenital Diaphragmatic Hernia. New England Journal of Medicine, 2003.
www.downstatesurgery.org

Fetal Endoscopic Tracheal Occlusion (FETO)
• Clinical observation: infants with congenital high airway obstruction develop hyperplastic lungs
• Animal model: tracheal ligation in the fetus accelerates lung growth beyond normal limits and prevents pulmonary hypoplasia associated with CDH
www.downstatesurgery.org

Animal Model of Tracheal Occlusion www.downstatesurgery.org

FETO www.downstatesurgery.org

FETO www.downstatesurgery.org

FETO Clinical Trials
• US, 2003: n=24, LHR<1.4 and liver in chest, survival 73% vs 77%, terminated early
• Europe, 2009: n=210, LHR<1 and liver in chest, survival 49% vs 24%
• Brazil, 2012: n=41, LHR<1 and liver in chest, survival 50% vs 4.8%
• Multicenter RCT currently in process
www.downstatesurgery.org

Outcomes, JPS 2007 www.downstatesurgery.org

Standardized Reporting System, JPS 2013
A: Entirely surrounded by muscle B: <50% devoid C: >50% devoid D: complete or near complete absence
www.downstatesurgery.org

Follow-Up Guidelines www.downstatesurgery.org

Conclusion
• CDH leads to pulmonary hypoplasia and pulmonary hypertension
• Stabilize with intubation and NGT/OGT • Volutrauma and barotrauma kills these babies • Delay operation until cardiopulmonary
stability • Outcomes predicted by size of defect and
major cardiac anomalies
www.downstatesurgery.org

SESAP Question
Which of the following statements about neonatal CDH is correct? A. Defect size is not an important factor in overall
survival B. HFOV is a contraindication for thoracoscopic repair C. Primary repair has a survival rate of 90% D. Patch repair has equivalent long term morbidity
compared with primary closure E. ECMO does not improve overall survival
www.downstatesurgery.org

Snickers Award for Most Presentations*
#1 Dr Stefan Kénel-Pierre, 15
(also most languages spoken, 6)
#2 Dr Aliu Sanni, 13 #3 Multiple, 12
* Through June 2014 according to downstatesurgery.org
www.downstatesurgery.org