case based discussion of copd guidelines 2004 diagnosis dr anne mcgown mar 2008
TRANSCRIPT

Case based discussion of COPD guidelines 2004
Diagnosis
Dr Anne McGown
Mar 2008

Case 1
• Mrs J.W
• Aged 81
• complaining about SOB on 50-100yards
• SOB 1 flight of stairs
• no cough or sputum
• no antibiotics for chest
• Hypertension, no IHD, no childhood asthma

What associated symptoms/factors should you ask
about

What associated symptoms/factors should you ask
about• Weight loss
• waking at night
• ankle swelling
• fatigue
• occupational hazards
• chest pain*
• haemoptysis*

How can you grade breathlessness?

MRC Dyspnoea scale
• 1 Not troubled by breathlessness except on strenuous exercise
• 2 Short of breath when hurrying or walking up a slight hill
• 3 Walks slower than contemporaries on level ground because of breathlessness, or has to stop for breath when walking at own pace
• 4 Stops for breath after walking about 100m or after a few minutes on level ground
• 5 Too breathless to leave the house, or breathless when dressing or undressing

SH
• Lives alone
• Ex-waitress/barmaid
• gave up smoking aged 65, started in her teens and smoked 10/day = 25 pack years

TH
• Eprosartan
• Aspirin
• Omacor
• bendrofluazide
• doxazosin
• serevent

Examination
• No clubbing or oedema
• pulse 72 and regular
• heart sounds normal
• chest clear
• CXR - NAD
• FEV1 1.13 53% pred
• FVC 1.5l 64% pred, ratio FEV1/FVC 74%

Differential diagnosis?

Differential diagnosis?
• Respiratory - asthma/COPD
• Cardiac
• Anaemia
• Other rare

Flow volume loop

Case 1

Main differential
• Asthma
• COPD
• Peak flow chart no variation
• Mild COPD
• Improved with addition of tiotropium (could walk and talk at the same time which was what she wanted)
• Discharged.

Spirometry
• (a) - normal• (b) - obstructive
– dashed - asthma after bronchodilator
• (c) - restrictive compared to normal– From Johns Pocket
Guide to Spirometry

Spirometry
• Airflow obstruction if FEV1/FVC <0.7– FEV1<80% predicted
• Severity of airflow obstruction– mild - FEV1 50-80% predicted– moderate - FEV1 30-49% predicted– severe - FEV1 <30% predicted– spirometry predicts prognosis in COPD, but not
disability or quality of life

Spirometry in COPD• COPD definition - presence of airflow limitation
that is not fully reversible and does not change markedly over several months.
• Distinguish from asthma on basis of history, examination, longitudinal observation (+/- reversibility testing and PEFR charts).
• Chest pain and haemoptysis, or disproportionate SOB/cyanosis in mild cases - look for alternative diagnosis
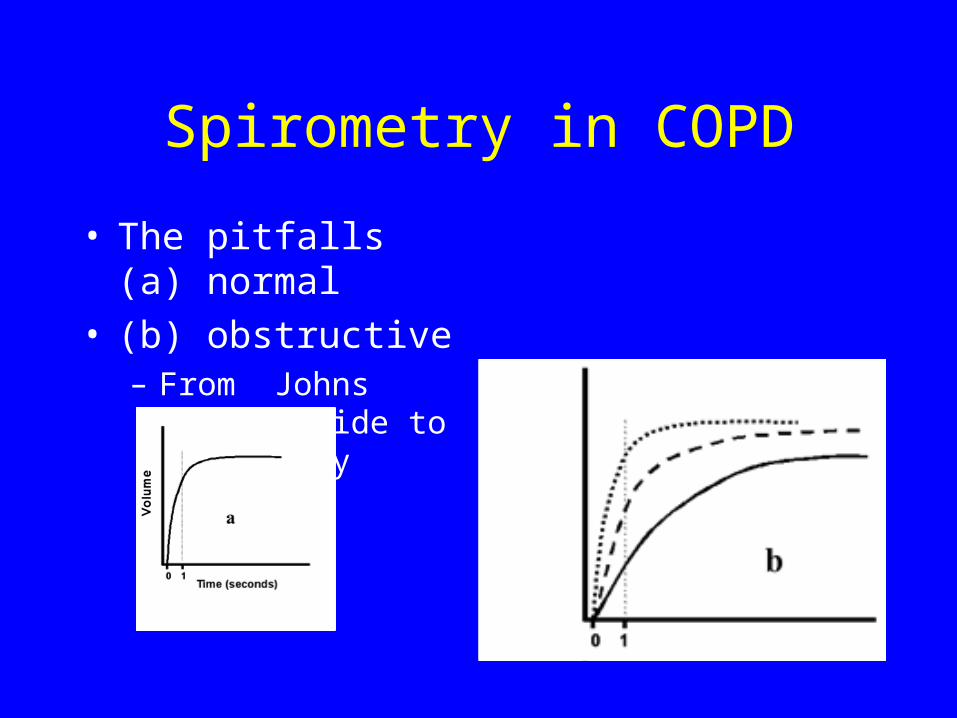
Spirometry in COPD
• The pitfalls (a) normal• (b) obstructive
– From Johns Pocket Guide to Spirometry

Flow volume loops
• (a) Normal
• (b) - asthma
• (c) - emphysema
• (d) - restrictive
• (e) - upper airway obstruction

Spirometry summary
• Obstructive useful
• May miss diagnosis if technique poor or severe disease
• Restrictive less useful as more sensitive to technique, and cannot distinguish intrinsic lung disease from extrinsic lung disease (esp. obesity also chest wall, muscle)

Spirometry does not predict disability
• Other prognostic factors– Frequency of exacerbation
– FEV1 and TLCO
– MRC breathlessness
– Health status
– Exercise capacity
– BMI
– Arterial pO2
– Cor pulmonale

Case 2
• Mr CG
• Age 66
• Admitted acutely SOB
• No chest pain or palpitations
• History of wheeze with chest infections for several years
• Ex smoker

Examination findings
• Tachypnoea
• Saturations 85% on air
• Tachycardia 150bpm AF
• Raised JVP and peripheral oedema
• Widespread wheeze
• Bilateral inspiratory crackes

What are the possible causes of SOB?

What are the possible causes of SOB?
• LVF
• Decompensation from fast AF
• COPD
• Cor pulmonale

How can you distinguish cardiac and respiratory causes?
How can you distinguish cardiac and respiratory causes?
• Echo – good biventricular function, LVEF 65%, normal valves, mild TR
• ECG – no ischaemic changes• Spirometry – FEV1 1.62 (38% predicted),
FVC 3.09, ratio FEV1/FVC 52%• ABG when not acutely SOB – pH 7.426,
pO2 6.31, pCO2 7.19 SaO2 82%• CXR


Treatment at discharge
• Combivent
• Ramipril
• Furosemide
• Bisoprolol
• Digoxin
• Spironolactone

Treatment of cor pulmonale
• LTOT assessment
• Diuretics
• No evidence for ACEI, calcium channel blockers, alpha blockers or digoxin unless AF,
Follow up
• Definite symptomatic improvement when ramipril dose increased
• Still SOB on short distances
• Minor improvement in spirometry – still obstructive
• Sats improved to 92% on air – not keen on ambulatory oxygen assessment

Case 3• Age 46 female• Admitted with wheeze, productive cough, fever• Quite slow to recover – 4-5days as IP• Smoker• Operation for scoliosis aged 12• Discharged on combivent and becotide• Seen in OPD in 6 weeks• Felt back to normal, but still SOBOE

What sort of defect do you think her spirometry showed?

What sort of defect do you think her spirometry showed?
• Mixed defect• FEV1 1.10 (41% pred)• FVC 1.54 (49% pred)• FEV1/FVC 71%• After ventolin• FEV1 1.45l (132%)• PEFR from 170 to 240• sats 97% on air

How would you distinguish asthma and COPD in this
patient?

How would you distinguish asthma and COPD in this
patient?• Spirometry alone cannot separate
• clinical features
• longitudinal variation
• bronchodilator response (>400ml)
• Steroid response (>400ml)
• PEFR variability >20%

Clinical featuresCOPD Asthma
Smoker or ex smoker Nearly all Possibly
Symptoms under age 35
Rare Often
Chronic productive cough
Common Uncommon
Breathlessness Persistent and progressive
Variable
Night time waking Uncommon Common
Diurnal/day to day variability
Uncommon Common

Spirometric reversibility testing
• Not required routinely
• May be inconsistent, not reproducible
• Misleading unless change in FEV1 >400ml
• Arbitrary definition of significant change
• Response to long term therapy not predicted by acute reversibility testing

COPD vs asthma
• Clinically significant COPD not present if FEV1 and FEV1/FVC ratio return to normal with drug therapy
• Imaging and TLCO may help resolve difficult cases
• TLCO (gas transfer) may be reduced in COPD and may be increased in asthma.
• Clinical history as good as bronchial biopsies……

Opportunistic case finding
• Knowledge of abnormal lung function as part of a motivational package significantly affects the success of smoking cessation therapy.
• Cost effectiveness depends on prevalence of undetected COPD and smoking cessation success rate.
• Over 35 current or ex smokers with a chronic cough.

Specialist referral - 1
• Diagnostic uncertainty
• Suspected severe COPD
• Patient requests second opinion
• Onset of cor pulmonale
• Assessment for oxygen therapy
• Assessment for nebuliser
• Assessment for long term oral steroids

Specialist referral - 2
• Bullous lung disease• Rapid decline in FEV1• Assessment for pulmonary rehab• Assessment for thoracic surgery• Dysfunctional breathing• Aged under 40• Frequent infections• Haemoptysis

Summary
• Spirometry – pitfalls
• Assessing severity
• Main differentials – asthma and cardiac failure
• Reasons for specialist referral