case 9 bode sgpath 2015 5 9 final on line
TRANSCRIPT

Gynecological CytologyHistology correlation
HPV
Slide seminar SGZyt / SGPath
Bern, May 9th, 2015
Beata BODE‐LESNIEWSKAInstitute of Surgical PathologyUniversity HospitalZurich, Switzerland

Case 9• 22 years old woman
• Cystic fibrosis (dx at birth)• Worsening of the lung function since the age of 12 y
• At the age of 19 y – bilateral lung transplantation
• First cervical PAP smear at the age of 20 y – normal• Follow up
– Three consecutive PAP mears over the next 2 y: LSIL– PAP 3 y post TPL our Case 9

Representative smear
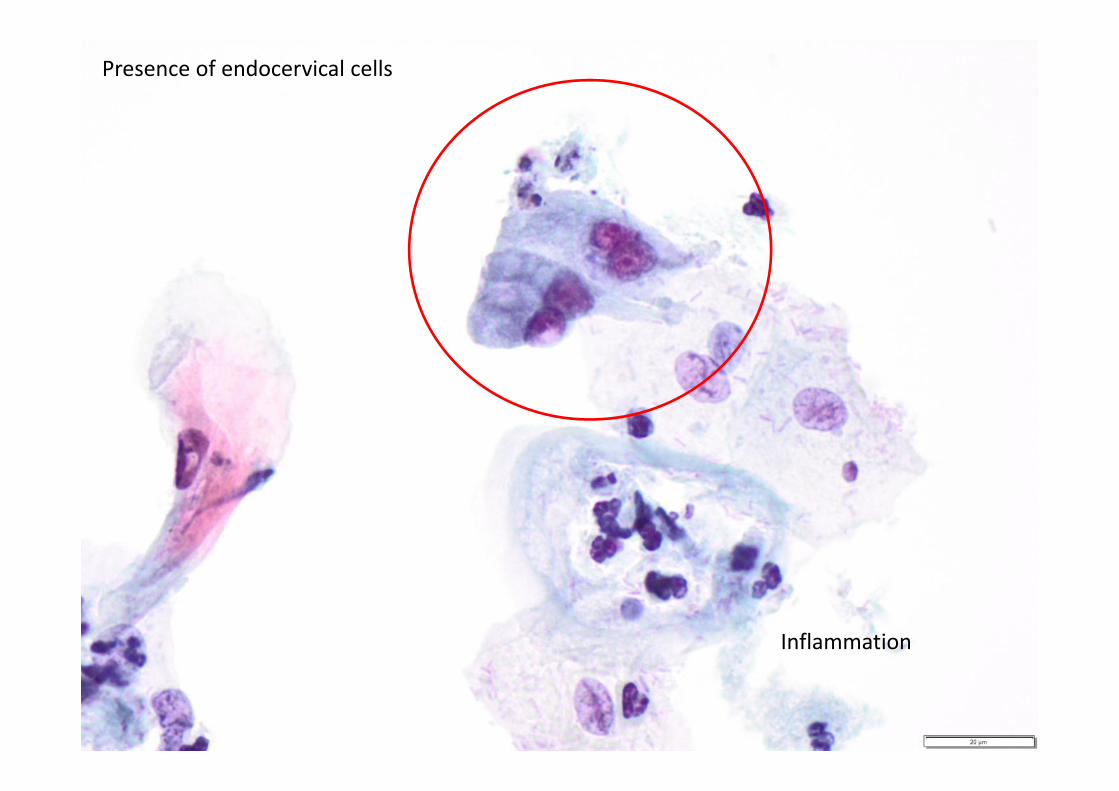
Presence of endocervical cells
Inflammation

Inflammatory change


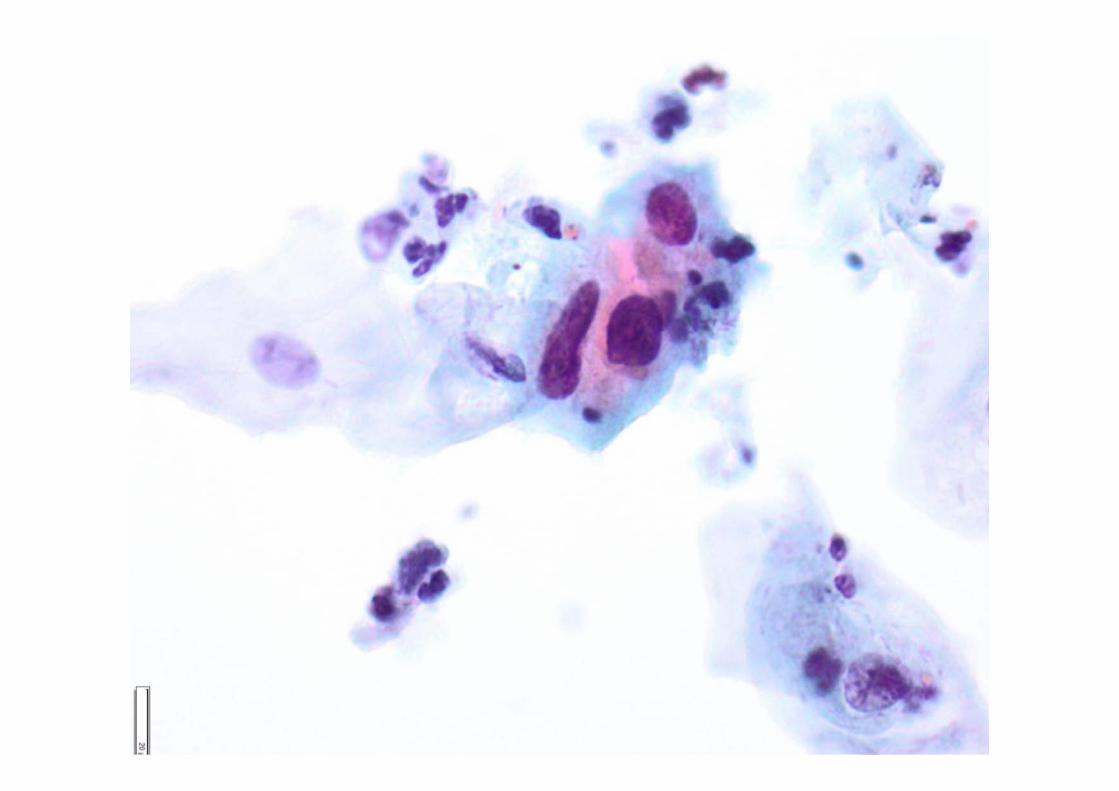
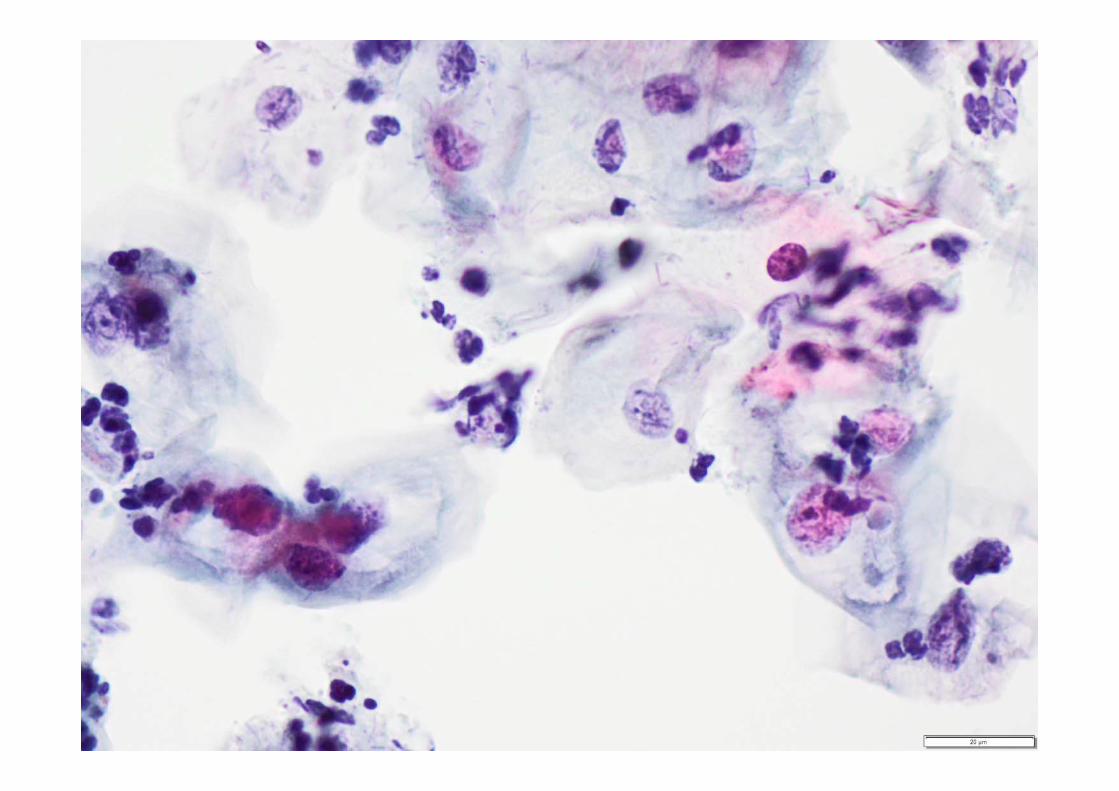

Typical koilocytes

DIAGNOSISPAP smear
LSIL (low grade squamous intraepithelial lesion)
HPV (signs of HPV infection)

Cervical biopsytaken at the same time





mib1

p16
DIAGNOSIScervical biopsy
LSIL (low grade squamous intraepithelial lesion)
CIN1 (cervical intraepithelial neoplasia 1)
HPV (signs of HPV infection)

HPV typing
• Performed on ThinPrep (PCR & sequencing)
• Positive – mixed infection– HPV type 6 – HPV type 82 (subtype MM4)

HPV 6 LR
HPV 58 HRHPV 82 HR
HPV 90 unknown
Several cytologic and histologic studies over 11 years post TPL:
‐ Recurring LSIL, CIN1 to HSIL, CIN3‐ Recurring VAIN1‐3 and VIN1‐3‐ 4 x conisation‐ Hysterectomy 6 y post TPL ‐ AIN 1‐3
‐ HPV testing: ‐ Specimen presented: HPV 6 and HPV 82‐ 4 repeats withnin further 9 years : HPV 82, HPV 90 and HPV 58

FOLLOW UP
Last visit pulmonology 11 y post TPL ‐ Pt doing well
Medication ‐ 19 different drugs a day
Close monitoring‐ Gynecology‐ Proctology
Extensive, persistent, mixed HPV infection
cervical / vaginal / vulvar / anal disease
IN AN IMMUNOSUPPRESED (TPL) PATIENT
• No invasiv carcinoma (FU 11 y)

Immunosuppression• Pregnancy• Malnourishment
• Non‐tumorous (eg. diabetes) and tumor diseases (eg. lymphoma)
• Infections (eg. HIV, Tbc)
• Cortison• Chemotherapy
• Transplantation– Kidney– Bone marrow– Liver– Lung– Heart– Pancreas

Organ transplantations• Continuous improvement in the results of TPL (quality of life
/ survival)– Immunosuppression drugs– Surgical techniques– Optimal utilisation of the donor organs (multiple recipients, life donors, crossover
transplantations)
• About 18,000 renal transplants are performed each year in the EU (500 million inhabitants) according to the European Committee on Organ Transplantation (CD‐P‐TO)
• There have been >575,000 solid organ transplants performed in the United States since 1954, – 38% among women

‐ Menstrual disorders‐ Contraception‐ Cervical cancer screening‐ HPV vaccination‐ STI screening
Organ transplantations
• The level of immune suppression varies by factors such as– type of organ, – level of HLA matching between donor and recipient,– drug regimen
• With improved long‐term survival in transplant recipients, an increased incidence of cancers has been noted
• Solid organ transplant recipients are at approximately 2 x increased risk of any type of cancer compared with thegeneral population

• …….. are at increased risk of several pathogen‐associated cancers – Epstein Barr virus – Hepatitis B and C viruses – Human papillomavirus (HPV)– HHV8
• The mechanism by which HPV oncoproteins contribute to genetic instability and cancer in the transplant setting is likely similar to that in the immune competent population, but time to development of HPV‐related cancers may be accelerated by iatrogenic immune suppression– re‐activation of a latent infection– progression of an active infection

187 649 US recipients (F 38.4%) in the Transplant Cancer Match Study
• Kidney and/or pancreas 63.8 %• Liver 21.2 %• Heart and/or lung 13.8 %• Other 1.2 %
Transplant recipients have elevated cancer risk of (HPV)‐associated cancers:– Cervix,– Vagina– Vulva
– Penis
– Anus
– Oropharynx
2013

Elevated incidence of HPV‐related cancers
– SIR: in situ 3.3–20.3, – SIR: invasive 2.2–7.3 ,
except for invasive cervical cancer (SIR 1.0).
The absence of increased incidence of invasive cervical cancer highlights the success of cervical screening in this population and suggests a need for screening for other HPV‐related cancers.
Other findings– Incidence increased with time since transplant for vulvar, anal and penile cancers (IRRs 2.1–4.6 for 5þ vs. <2 years– Use of specific immunosuppressive medications variably associated with incidence; for example, tacrolimus: reduced incidence for some
anogenital cancers (IRRs 0.4–0.7) but increased incidence of oropharyngeal cancer (IRR 2.1).– Some HPV‐related cancers may occur more frequently in recipients with specificmedical conditions. For example, we observed an increased
incidence of oropharyngeal cancer among liver recipients compared with kidney recipients, and incidence was even higher in the subset who had alcoholic cirrhosis as the indication for liver transplant (IRR 5.4 vs. other indications among liver recipients

…. however…..Studies of the incidence of invasive cervical cancer (ICC) among transplant recipients in other centers have shown mixed results.
• Similarly to US data, a national cohort study from Sweden while finding excess tongue, anal, vulvar, and vaginal cancers among transplant recipients, did not find a greater incidence of cervical cancer
• A study from Korea showed the incidence of ICC to be 10 times higher than the general population; however, the prevalence of HPV in the general population of Korea is higher than in Western countries
• A study from the Netherlands revealed a fivefold increased risk of cervical cancer among transplant recipients; the majority of patients with anogenital cancer in this study had no cervical cytology prior to transplantation

Vaccination
• The HPV vaccine (VPL) is not live and is thus. safe to use in an immunosuppressed population
• Quadrivalent HPV vaccine is recommended for posttransplant patients (for patients within the indicated age group, who are candidates for transplantation or post‐transplant in those who have not previously received vaccine)
• Decreased immunogenicity has been documented among solid organ transplant recipients, but no adverse events have been reported

Conclusions:• vaccine has suboptimal immunogenicity in the posttransplant setting• significantly lower than in young men and women (97‐99%)• seropositivity after vaccination in HIV‐positive 95–100% (hv CD4 > 500)•• early posttransplant and lung transplant recipients had
especially low vaccine responses.
• similar to findings in studies of other vaccines such as influenza vaccine in organ transplants
• 47 pts (at least 3 mo posttransplant) were immunized with 3 doses (0, 2 and 6 mo) of 4‐valent HPV vaccine• M/ F 16/31 (34%/66%), median age 25.9 y (18– 35); median of 2.7 years from transplant. • kidney (30; 64%) or lung (11; 23%); heart 3; liver 1; other multi 2 transplants
Facit• HPV associated genito‐anal neoplasias are important side
effects of the long term immunosuppression in patientsfollowing transplantation
• HPV vaccination is recommended (time point?)
• …. however, immunisation may be less effective than in general or even HIV population
• Close follow up including cytological controls remainsimportant and is recommended for the transplantedpopulation ‐ the recommendation of cervical cancer screening does not change based on HPV vaccination status

Submitted diagnosesBiopsyCytology