case 3 - bemedtech catheter • indwelling urinary catheters are generally considered to be short...
TRANSCRIPT

Case 3Fight Against Nosocomial Infections
Catheter-associated Urinary Tract Infections
Old but still new
Dr. Radu Ciprian Ṭincu, MD, PhD.
Senior consultant Anesthesiology and Critical Care Department
Clinical Emergency Hospital Bucharest, Romania
What we know?
• A urinary tract infection (UTI) is an infection involving any part of the urinary system, including
urethra, bladder, ureters, and kidney.
• UTIs are the most common type of healthcare-associated infection reported to the National
Healthcare Safety Network (NHSN).
• Among UTIs acquired in the hospital, approximately 75% are associated with a urinary catheter.
• Between 15-25% of hospitalized patients receive urinary catheters during their hospital stay.
• The most important risk factor for developing a catheter-associated UTI (CAUTI) is prolonged use
of the urinary catheter.
www.cdc.gov
National and State Healthcare-Associated Infections Progress Report (HAI Progress Report)
• No change in overall catheter-associated urinary tract infections (CAUTI) between 2009 and 2014
• Some surveillance studies reported reduction of CA-UTI- it is a truth
• This decrease is attributable to more intense prevention efforts, but modification of definitions to exclude asymptomatic bacteriuria has also contributed.

Global implication
• 17.5% of patients in 66 European hospitals having a catheter
• 23.6% in 183 US hospitals
• In the NHSN 2011 surveillance report, 45–79% of patients in adult critical care units had an indwelling catheter
• Prevention of infections attributable to these devices is an important goal of health-care infection prevention programs.

The catheter
• Indwelling urinary catheters are generally considered to be short term if they are in
situ for less than 30 days
• Chronic or long term when in situ for 30 days or more
• Indwelling catheter use in acute care facilities is usually short term
• Chronic catheters are most common for residents of long term care facilities
• Clinical and microbiologic considerations may vary for short and long term catheters.
• Urinary catheter acquired infection is usually manifested as asymptomatic bacteriuria
(CA-ASB).
• Catheter associated urinary tract infection (CA-UTI) is used to refer to individuals with
symptomatic infection
Asymptomatic bacteriuria
• Duration of catheterization is the most important determinant of bacteriuria
• The daily risk of acquisition of bacteriuria when an indwelling catheter in situ is 3–7%.
• The rate of acquisition is higher for women and older persons
• Bacteriuria is universal once a catheter remains in place for several weeks.
• Patients with chronic indwelling catheters are assumed to be continuously bacteriuric.
• From 60–80% of hospitalized patients with an indwelling catheter receive antimicrobials, usually for
indications other than urinary tract infection
• This intense antimicrobial exposure means antimicrobial resistant organisms
• Bacteria colonizing the drainage bags of catheterized patients have been reported to be a source
for outbreaks of resistant organisms in acute care facilities
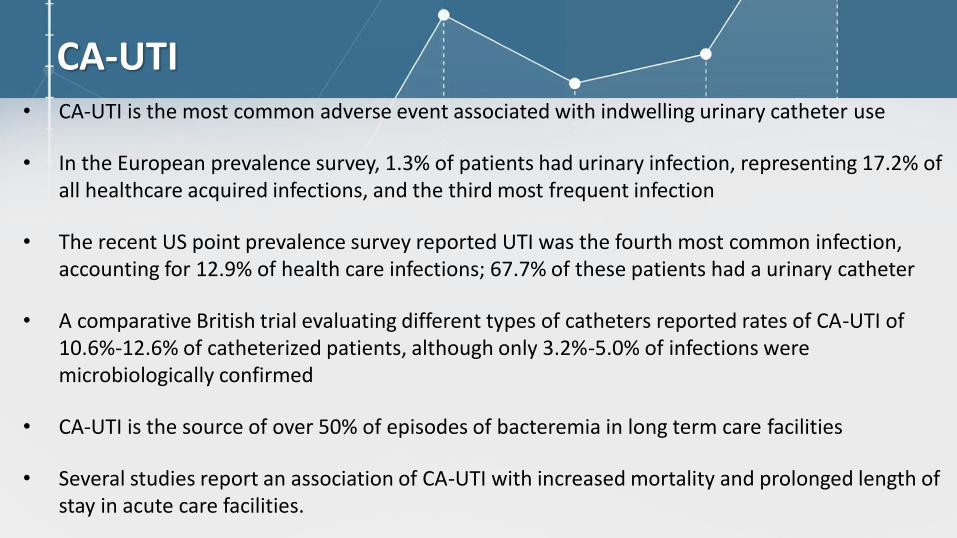
CA-UTI • CA-UTI is the most common adverse event associated with indwelling urinary catheter use
• In the European prevalence survey, 1.3% of patients had urinary infection, representing 17.2% of all healthcare acquired infections, and the third most frequent infection
• The recent US point prevalence survey reported UTI was the fourth most common infection, accounting for 12.9% of health care infections; 67.7% of these patients had a urinary catheter
• A comparative British trial evaluating different types of catheters reported rates of CA-UTI of 10.6%-12.6% of catheterized patients, although only 3.2%-5.0% of infections were microbiologically confirmed
• CA-UTI is the source of over 50% of episodes of bacteremia in long term care facilities
• Several studies report an association of CA-UTI with increased mortality and prolonged length of stay in acute care facilities.
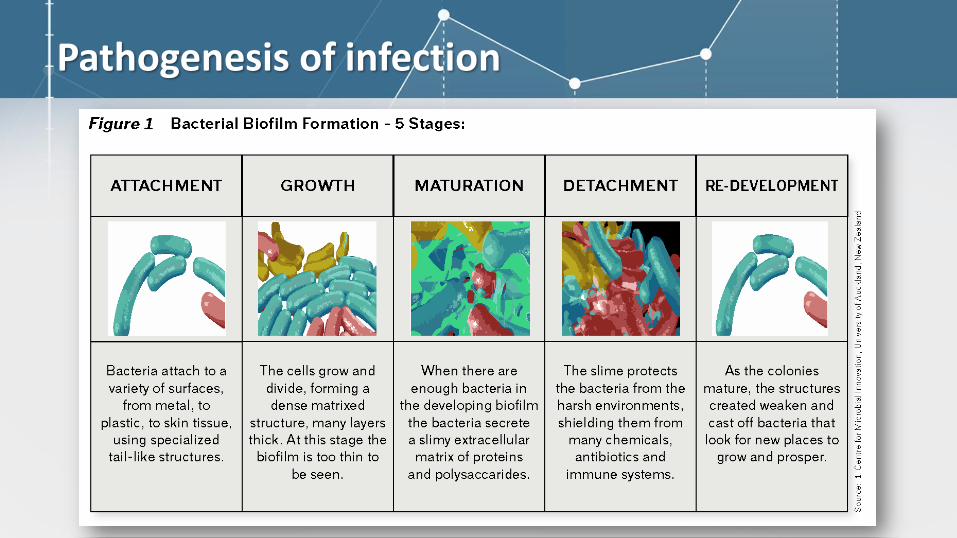
Pathogenesis of infection
Biofilm
• Biofilm formation along the catheter surface is the most important cause of bacteriuria.
• Biofilm is a complex organic material consisting of micro-organisms growing in colonies within an extra-cellular mucopolysaccharide substance which they produce.
• Urine components, magnesium and calcium ions, are incorporated into this material.
• Biofilm formation begins immediately after catheter insertion, when organisms adhere to a conditioning film of host proteins which forms along the catheter surface.
• Both the interior and exterior catheter surfaces are involved.
• Bacteria usually originate from the periurethral area or ascend the drainage tubing following colonization of the drainage bag.

Biofilm – reloaded • Bacterial species which produce urease may facilitate the formation of a crystalline biofilm.
• This material is similar to struvite stones in patients with urolithiasis.
• Crusts of this material form along the catheter and are the major cause of obstruction.
• Catheter obstruction are well recognized precipitating events for CA-UTI.
• The urease of P. mirabilis hydrolyzes urea several times faster than the urease produced by
other organisms.
• This species is isolated from 80% of obstructed catheters.
• Other urease producing species include P. aeruginosa, Klebsiella pneumoniae, Morganella
morganii, other Proteus species, some Providencia spp, some Staphylococcus aureus and
coagulase negative staphylococci.
Biofilm evolution • Organisms growing in the biofilm are relatively protected from antimicrobials and host
defenses.
• A single species is usually identified with the initial episode of bacteriuria.
• If the catheter remains in situ and a mature biofilm develops, polymicrobial bacteriuria
becomes the norm.
• For individuals with long term indwelling catheters, 3–5 organisms are usually isolated
• The microbiology of biofilm on an indwelling catheter is dynamic with continuing
turnover of organisms in the biofilm.
• Patients continue to acquire new organisms at a rate of about 3–7%/day.

Adherence and colonization• Adherence is a key event initiating each step in UTI pathogenesis.
• A UTI typically starts with periurethral contamination, followed by colonization of the urethra and subsequent migration of the pathogen to the bladder, an event that requires appendages such as flagella and pili.
• In the bladder, the consequences of complex host–pathogen interactions ultimately determine whether uropathogens are successful in colonization or eliminated.
• Multiple bacterial adhesins recognize receptors on the bladder epithelium and mediate colonization.
• uropathogenic Escherichia coli (UPEC) invading the bladder epithelium, producing
toxins and proteases to release nutrients from the host cells, and synthesizing
siderophores to obtain iron.
• In the renal epithelium and then producing tissue-damaging toxins and are able to
cross the tubular epithelial barrier initiating bacteraemia.
• UPEC forms biofilm-like intracellular bacterial communities, that protect their members
from neutrophils, antibiotics.
• Type 1 pili, antigen 43 and adhesive surface fibres called curli induce
biofilm formation by mediating interbacterial interactions and attachment to surfaces.

Microbiology
• The most common infecting organism is Escherichia coli.
• Other Enterobacteriaceae as well as Enterococci spp, coagulase negative Staphylococcus, Pseudomonas
aeruginosa, other non-fermenters, and Candida spp are also frequently isolated.
• Antimicrobial-resistant organisms are common.
• The urine of patients with indwelling catheters is the major site of isolation of resistant gram negative
organisms, including extended spectrum beta-lactamase (ESBL) producing Enterobacteriaceae.
• Proteus mirabilis is an organism of unique that produces urease, which hydrolyses urea to carbon dioxide
and ammonia.
• P. mirabilis produces more copious biofilm than other bacteria, forming
crystalline biofilms on the catheter.

How and when make the diagnosis?
• A mature biofilm has usually formed once the catheter has been in situ for longer than
2 weeks.
• Urine collected through these catheters are contaminated by organisms present in the
biofilm.
• There is a greater number of species and quantity of organisms isolated than these
specimens compared with bladder urine collected simultaneously.
• It is recommended that the catheter be removed and a new catheter inserted, with
specimen collection from the freshly placed catheter

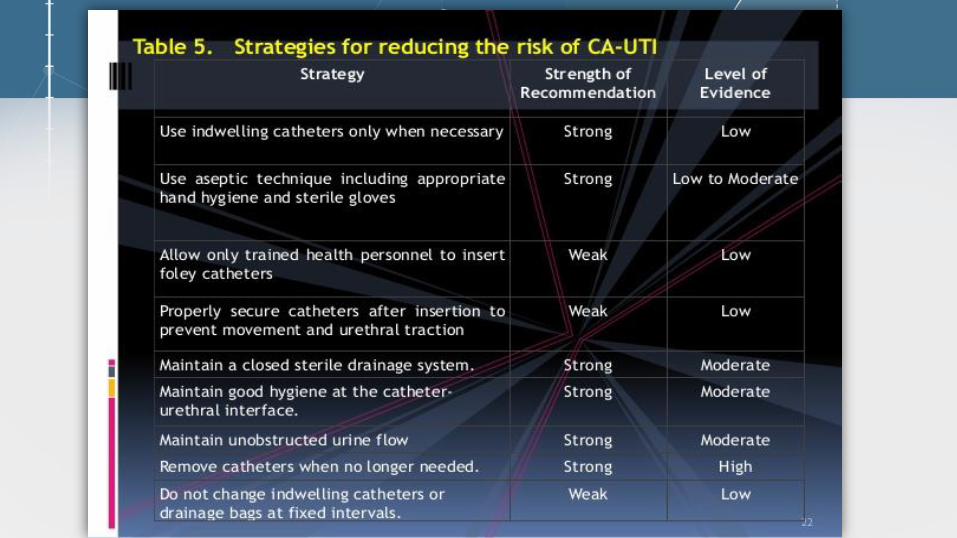
Prevention
1) The single most important intervention to prevent CA-UTI is to avoid use of an
indwelling urinary catheter.
2) When a catheter is indicated, it should be removed promptly once it is no longer
required. Ask daily: Is the urinary catheter needed?
3) Catheters have been reported to frequently remain in situ beyond necessary,
sometimes because health-care personnel are not aware the catheter is present.
4) Use aseptic technique for insertion.
5) Minimize manipulation or opening of drainage systems.
6) Urinary catheter should not be used for the management of urinary incontinence.
When it is used?
• Monitoring of hourly urine output in acutely ill patients.
• Perioperative use for selected surgical procedures:
– Urologic surgery
– Large volume infusions or diuretics during surgery
– Requirement for intraoperative monitoring of urine output
!!! Management of acute urinary retention and urinary obstruction.
In exceptional circumstances (e.g. end-of-life care), at patient request to improve comfort.
What type of catheter is indicated?
• The smallest gauge catheter possible should be used, to minimize
urethral trauma.
• Infection risks are similar with latex or silicone catheters, and whether or
not there is hydrogel coating of the catheter.
Risk factors
• Female gender
• Advanced age
• Other active site of infection
• Diabetes mellitus
• Renal insufficiency
• Duration of catheterization
• Retrograde flow urine from drainage bag
• Errors in catheter insertion
• Not doing pericare routinely
• Absence use of urimeter
• Microbial colonization of the drainage bag

Impact of CA-UTI
• Increased morbidity and mortality: 13.000 deaths annually
• Excess length of stay in hospital: 2-4 days
• Increased cost: 0.4-0.5 billion per year nationally
• Unnecessary antimicrobial use
• Bacteriuria or candiduria is almost inevitable in nearly half of the patients who require an indwelling urinary catheter for more than 5 days.
• Each episode of catheter-associated urinary tract infection costs at least $600
• Each episode of urinary tract-related bacteremia costs at least $2800
Tambyah PA. The direct costs of nosocomial catheter-associated urinary tract infection in the era of managed care. Infect Control Hosp Epidemiol. 2002Saint S. The clinical and economic consequences of nosocomial central venous catheter-related infection: are antimicrobial catheters useful? Infect Control Hosp
Epidemiol. 2000

Impact of CA-UTI

Financial: CMS - Show Me the Money!
• Starting October 1, 2008, the Centers for Medicare and Medicaid Services (CMS) under a revised Acute Care Hospital Inpatient Prospective Payment System (IPPS), would no longer reimburse hospitals for costs attributable to CAUTIs
• Starting in 2014, CMS began publically reporting rates of CAUTI for hospitals participating in the Hospital Inpatient Quality Reporting Program
• Starting in 2015, required reporting of CAUTIs in all settings, including adult and pediatric medical, surgical wards
• CMS will base penalties on NHSN CAUTI data
CMS. Medicare Program: hospital inpatient propsepctive payment systems for acute care hospitals and long-term care hospital prospective payment system and proposed fiscal year 2014 rates. Fed Regist 2013

Is Your Hospital Safe?
Would you want a loved one to be a patient at your hospital? Your unit?
Would you want to be a patient in the unit where you work?
Can you say with 100 percent certainty that you believe that your hospital does everything it can to protect its patients?
25
The CUSP Model
•Created through a collaborative effort of the Agency for Healthcare Research and Quality and state and national-level innovators in patient safety
•Dovetails with, and supports, a range of quality and safety improvement models
•Encompasses a wide range of safety tools and approaches
•Based on the understanding that all culture is local, and that work to improve culture must be owned at the unit level
•Believes that harm is not an acceptable “cost of doing business”
•Can be applied by anyone, anywhere 26
“The bulk of the evidence is consistent with the view that multimodal strategies could prevent between 25% and 75% of catheter-associated urinary tract
infections”
Saint S. Catheter-associated urinary tract infection and the Medicare Rule changes. Ann Intern Med 2009.


Noble metal alloy coated catheter
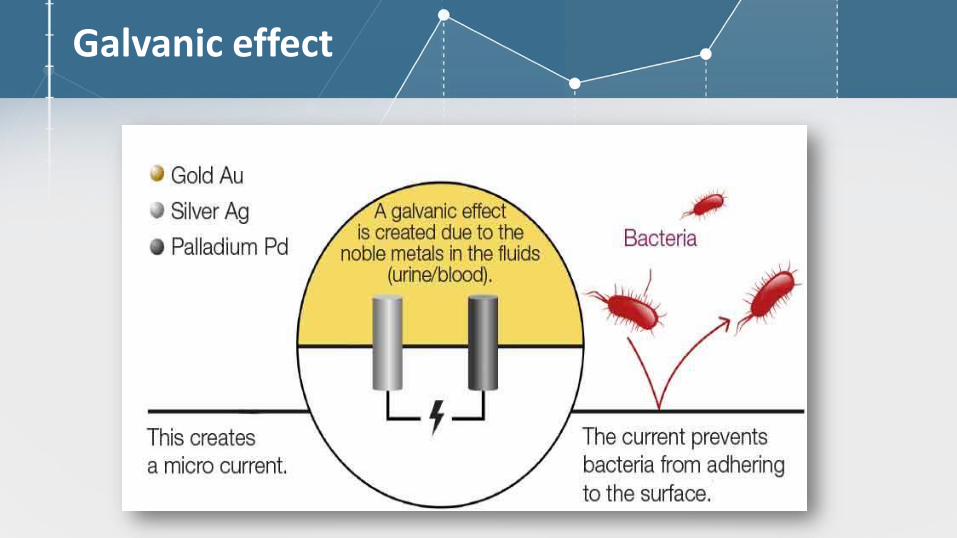
Galvanic effect

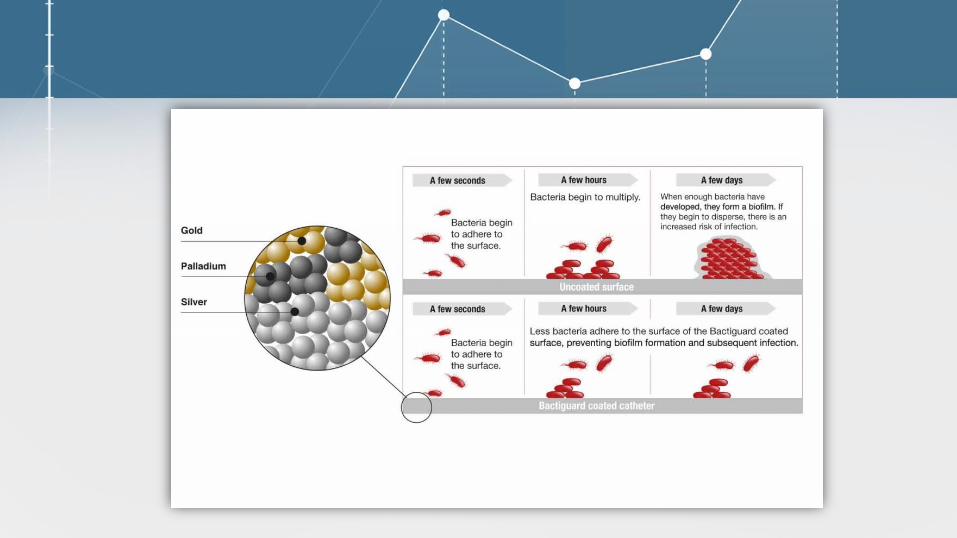
Bactiguard Catheter – Mechanism of action
➢ reducing adhesion of microorganisms to the medical device surface
➢ reducing biofilm formation as a consequence.
➢ the biofilm formation is a known pre-requisition for microbial infections caused by medical devices.
➢ once microbes have formed a biofilm they are much more resistant to antibiotics, which make such
infections difficult to treat and cure.
➢ galvanic elements formed by the coating metals: silver, gold and palladium with different electro-
potentials
➢ also safe and biocompatible in a number of pre-clinical and clinical studies
➢ silver released has no pharmacological effect in humans.

Galvanic currents
• Metals have different electro-potentials
• When metals with different electro-potential are placed in an electrolyte such as urine or blood,
a galvanic current will occur.
• Among coating metals, Pd has the highest electro-potential, then comes Au, and Ag has the
lowest.
• Effects depends on interference through electrical interaction with superficial structures of the
microorganisms.
• There is no dose-response relationship.
• The galvanic effect produced obstruct the adherence process of bacteria.
• Interferes with the proton (H+) electrochemical gradient that forms in the electron transport
chain/respiratory chain in microorganisms.
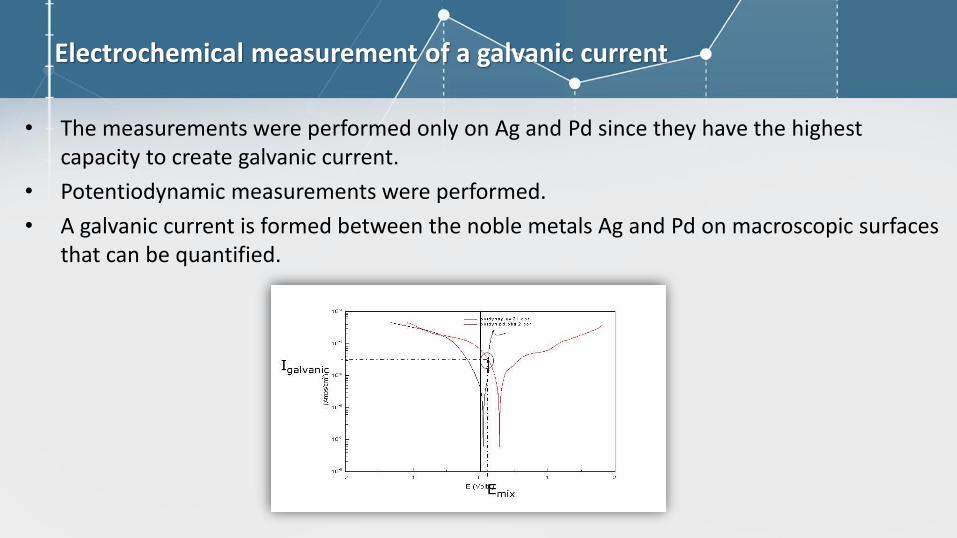
Electrochemical measurement of a galvanic current
• The measurements were performed only on Ag and Pd since they have the highest capacity to create galvanic current.
• Potentiodynamic measurements were performed.
• A galvanic current is formed between the noble metals Ag and Pd on macroscopic surfaces that can be quantified.
Metal composition
• coating consists of an extremely thin noble metal (Ag, Au, and Pd) alloy that can be firmly attached to the surface of a variety of materials by a patented wet chemical dipping process.
• the noble metals are firmly attached to the device surfaces, and very small amounts are released.
Silver release and antimicrobial properties
• the maximum release of silver from a catheter corresponds to a lower amount of silver than typically
passes the human body via the daily intake of food and water.
• minimum Inhibitory Concentration (MIC) is the lowest concentration of a substance that inhibits the
growth of microorganisms.
• the MIC values for silver ranged from 1,3 to 512 g/ml.
• the highest possible silver release from the coated products, it is still below the MIC level.
• is safe to say that the Bactiguard coating does not have an antimicrobial effect.
• effect of reduced microbial colonization of the Bactiguard coating is not due to an antimicrobial
effect, but rather a passive physico-chemical effect from the surface composition.

Silver resistance
Bactiguard Inhibition test reveal
that silver released did not have an
antimicrobial effect.

Studies data
• 37 clinical studies covering over 100 000 patients
• The results indicate that Bactiguard coating reduces symptomatic CAUTI, asymptomatic
Bacteriuria and a mixture of Asymptomatic Bacteremia and symptomatic CAUTI (CDC1 criteria
for CAUTI) by: 42% (bacteriuria), 24% (sCAUTI) and 41% (for CAUTI according to CDC).
• Bactiguard coating reduces CAUTI during short, medium and long term catheterization time.
• Bacteriuria (and consequently risk for sCAUTI) is reduced up to ~30 catheterization days.
• The overall review of the 37 referred studies indicates that BIP Foley Catheter reduces frequency
of infection and delays time to infection for both symptomatic Catheter Associated Urinary
Tracts Infections and bacteriuria during short, medium and long catheterization time.
What Can We Prevent?
• An estimated 17% to 69% of CAUTI may be preventable with recommended infection control measures, which means that up to 380,000 infections and 9000 deaths related to CAUTI per year could be prevented 1
• [The best quality studies] suggest that as many as 70% of all CAUTIs are preventable with current evidence-based strategies. CAUTI may be the most preventable HAI; the number of avoidable infections ranges from 95,483 to 387,550 per year. 2
CDC Guideline for the Prevention of CAUTI 2009.Umscheid CA, et al. Estimating the proportion of HAIs that are reasonably preventable and the related mortality and
cost. ICHE 2011;32:101-114.

Efficacy of noble metal alloy-coated catheter in prevention of bacteriuriaR. Tincu, C. Cobilinschi, D. Tomescu, Z. Ghiorghiu1, R. Al. Macovei
Methods:
• Prospective, randomized, controlled, independent study
• 120 patients – 60 BIP Foley + 60 silicone Foley; Oct-Dec 2015
• Patients admitted for drug poisoning with short term catheterization
(patients with urinary tract pre-contamination were excluded)
• Endpoints: Bacteriuria (≥ 105 CFU/ml), microbiology, risk factors for bacteriuria
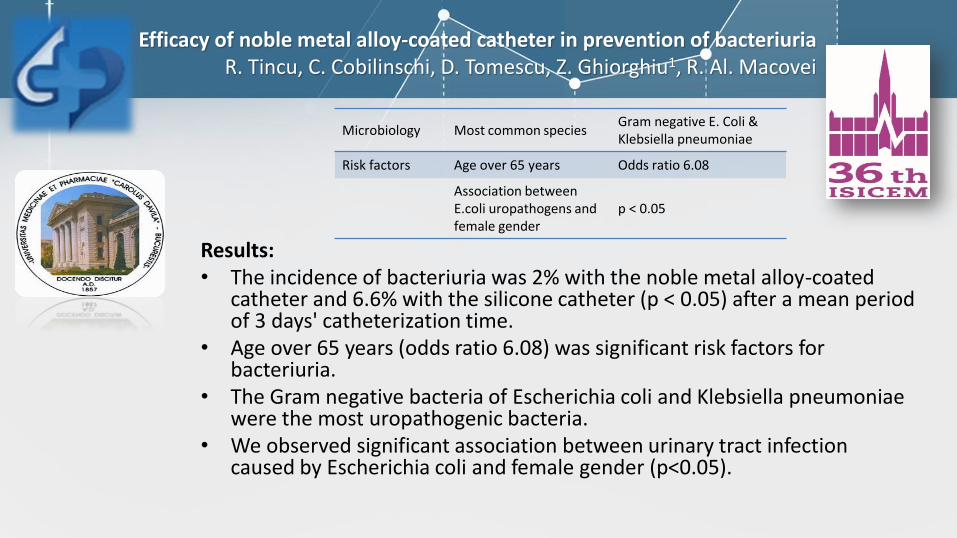
Efficacy of noble metal alloy-coated catheter in prevention of bacteriuriaR. Tincu, C. Cobilinschi, D. Tomescu, Z. Ghiorghiu1, R. Al. Macovei
Results: • The incidence of bacteriuria was 2% with the noble metal alloy-coated
catheter and 6.6% with the silicone catheter (p < 0.05) after a mean period of 3 days' catheterization time.
• Age over 65 years (odds ratio 6.08) was significant risk factors for bacteriuria.
• The Gram negative bacteria of Escherichia coli and Klebsiella pneumoniae were the most uropathogenic bacteria.
• We observed significant association between urinary tract infection caused by Escherichia coli and female gender (p<0.05).
Microbiology Most common speciesGram negative E. Coli & Klebsiella pneumoniae
Risk factors Age over 65 years Odds ratio 6.08
Association between E.coli uropathogens and female gender
p < 0.05

Efficacy of noble metal alloy-coated catheter in prevention of bacteriuriaR. Tincu, C. Cobilinschi, D. Tomescu, Z. Ghiorghiu1, R. Al. Macovei
Conclusions:
1. Noble metal alloy-coated catheters may decrease the incidence of urinary tract infections compared with silicon ones and in the meantime may lower the need for antibiotics.
2. Also, we noticed that the incidence of bacteriuria increased with age in both groups, but remained lower in noble metal alloy-coated catheter group.

FINAL Conclusions
1. CA-UTI is an important device-associated health care acquired infection, accounting for more
than 30% of acute care hospital infections.
2. 13,000 deaths are associated with UTIs each year (NHSN report).
3. There are estimated to be 449,334 CAUTI events per year.
4. Each CAUTI is associated with the medical cost of $758.
5. Over $340 million spent in health care is attributable to the incident of CAUTI in the U.S. each
year.
6. Noble metal alloy-coated Bactiguard catheters may decrease the incidence of urinary tract
infections compared with silicon ones and in the meantime may lower the need for antibiotics.
Thank you!

Call for action…
Fight Against Nosocomial Infections Symposium 45
more info at table with
case 3