case #1: difficult to control bp in an case studies in
TRANSCRIPT

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Case studies in Hypertension(pearls for achieving control) 2019
KARO L E . W A T S O N , MD , P H D , F A C C
P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y
D A V I D G E F F E N S C HOO L O F M ED I C I N E A T U C L A
CO ‐ D I R E C T O R , U C L A P R O G R AM I N P R E V E N T I V E C A R D I O L O G Y
Brachial blood pressure is a strong predictor of clinical outcomes in people with hypertension and it is assumed that brachial blood pressure accurately reflects pressures in the central aorta and thus left ventricular load
This assumption may not be valid in all circumstances
The gold standard for measuring central aortic pressure is invasive, however, noninvasive methods exist as well
Case #1: Difficult to control BP in an elderly patient
52-year-OldNormal Pressure Wave
81-year-Old Early Pulse Wave Reflection
Elderly Patients have Stiffer Blood VesselsAverage Blood Pressure Waveform
Notch Notch
Shoulder
Time (sec)Time (sec)
Average Blood Pressure Waveform
www.lejacq.com/Symposia_Info/UMH_DC-0504/Pickering.ppt
140
70
Radial
Transferfunction
Central Aortic
140
70

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Central blood pressure (CBP)
Diastolic and mean pressures are very similar at radial / brachial and central sites, but…
Systolic Central BP is not the same as brachial or radial systolic BP!
Case #1: Difficult to control BP in an elderly patient
Follow up: Central aortic BP 108/55
Follow up Medications: medications de‐escalated to Amlodipine 10 mg, Benazepril 20 mg, HCTZ 12.5 mg
Follow up Physical Exam: central aortic BP 128/55 mm Hg
Labs/studies: Unremarkable
Elderly patients are at risk for hypotension and falls after starting antihypertensive therapy
Butt DA et al. Arch Intern Med 2013
If your patient is dizzy when they stand up, it doesn’t matter what the guidelines say.

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Case #2: Patient with creatinine increase on ACE inhibitor
Chief complaint: 66 year old female referred by PCP for “renal injury” after starting ACE inhibitor. Patient is asymptomatic
PMH: HTN, fibromyalgia
Medications: Lisinopril 10 mg, Amlodipine 10 mg, HCTZ 12.5 mg, Atorvastatin 10 mg
Physical Exam: BP 128/82 mm Hg
Labs/studies: Creatinine 1.17 (baseline 0.9)
Serum Creatinine increase with ACE inhibitors and ARBs
Starting an ACE inhibitor or ARB can result in a small, non‐progressive increase in serum creatinine that reflects decreased glomerular filtration rate from the favorable hemodynamic effect of reducing intra‐glomerular pressure
A 30% increase in serum creatinine is generally acceptable
Creatinine will usually peak within a week, then stabilize
If > 30% increase in creatinine occurs, stop the drug
ACE/ARB dilate here
CapillaryAfferent arteriole Efferent arteriole
Intraglomerular pressure decreases
Filtration gradient decreases
Less creatinine is filteredSerum creatinine rises
Intraglomerular pressure decreases
Nephrons are sparedRenal function is
preservedOutcomes are improved
Changes in GFR with ACE‐I or ARB therapy
Aimun K. Ahmed et al. Nephrol. Dial. Transplant. 2010;25:3977-3982

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Case #2: Patient with creatinine increase on ACE inhibitor
Follow up: 0.9 to 1.17 is a 30% increase in creatinine
Follow up Medications: No change
Follow up Physical Exam: BP 125/80 mm Hg
Labs/studies: Creatinine stable at 1.12
A 30% increase in serum Creatinine after addition of an ACE inhibitor or ARB is acceptable.
Case #3: 33 year old patient with new onset hypertension
Chief complaint: 33 year old male referred by PCP for new onset hypertension. Has been following this patient for over 10 years but for the last 3 visits his BP has suddenly jumped up. Patient’s only complaint is back pain from an occupational injury
PMH: back strain, current smoker
Medications: Amlodipine 10 mg, Ibuprofen prn
Physical Exam: BP 148/92 mm Hg
Labs/studies: Unremarkable
Renin‐Angiotensin‐Aldosterone Regulation of Blood Pressure
http://vasoactivetherapy.com/files/CORLOPAM.PPT
Blood Pressure
Vasoconstriction
Angiotensin IRenin Substrate
Angiotensin IIRenin
Sodium & Water Reabsorption
Aldosterone
The role of aldosterone is to retain sodium in the face of deficiency
Adrenal Cortex
Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
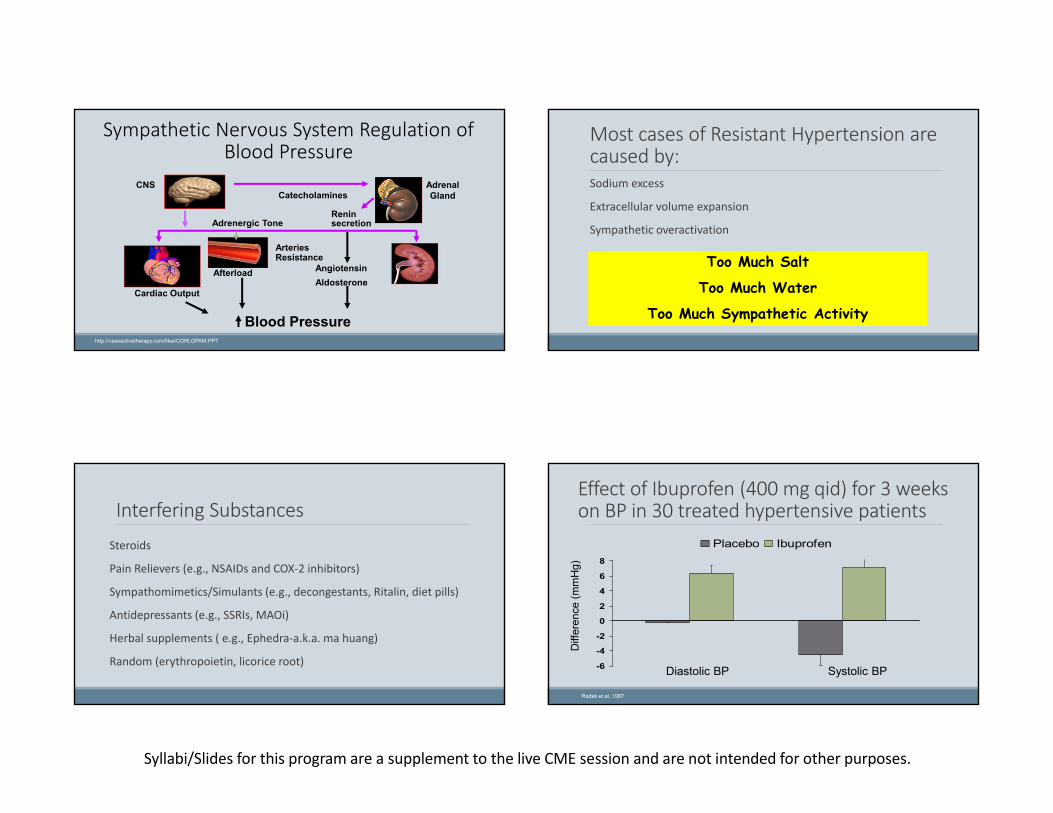
Sympathetic Nervous System Regulation of Blood Pressure
http://vasoactivetherapy.com/files/CORLOPAM.PPT
Adrenergic Tone
Angiotensin
Cardiac Output
CatecholaminesAdrenal Gland
CNS
ArteriesResistance
Afterload
Blood Pressure
Reninsecretion
Aldosterone
Most cases of Resistant Hypertension are caused by:Sodium excess
Extracellular volume expansion
Sympathetic overactivation
Too Much Salt
Too Much Water
Too Much Sympathetic Activity
Interfering SubstancesSteroids
Pain Relievers (e.g., NSAIDs and COX‐2 inhibitors)
Sympathomimetics/Simulants (e.g., decongestants, Ritalin, diet pills)
Antidepressants (e.g., SSRIs, MAOi)
Herbal supplements ( e.g., Ephedra‐a.k.a. ma huang)
Random (erythropoietin, licorice root)
Effect of Ibuprofen (400 mg qid) for 3 weeks on BP in 30 treated hypertensive patients
-6
-4
-2
0
2
4
6
8
Placebo Ibuprofen
Diff
eren
ce (m
mH
g)
Diastolic BP Systolic BP
Radak et al, 1987

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Case #3: 33 year old patient with new onset hypertension
Follow up: Ibuprofen discontinued; Amlodipine discontinued
Follow up Medications: None
Follow up Physical Exam: BP 120/78 mm Hg
Labs/studies: Unremarkable
Case #4: 58 year old with hypertension, worried about cancer scare
Chief complaint: 58 year old male referred by PCP for worry about cancer scare
PMH: hypertension, well controlled
Medications: Amlodipine 10 mg, Irbesartan 300 mg daily
Physical Exam: BP 128/82 mm Hg
Labs/studies: Unremarkable
•Several pharmaceutical companies have announced recalls of generic versions of valsartan, irbesartan and losartan.
•This is due to the contaminants NDMA and NDEA being found in certain lots
•The Food and Drug Administration has traced the contaminated products to a large factory in China and later a second factory in India. Both used a similar manufacturing process to make and supply generic drug companies worldwide.
•Only generic versions are affected. Not all makers of genetic versions are affected.
•Check FDA website for most up‐to‐date information on recalls
Case #4: 58 year old with hypertension, worried about cancer scare
Follow up: Patient called his pharmacy and checked the FDA website. There is no recall of his medication lot. He is reassured
Follow up Medications: No change
Follow up Physical Exam: BP 120/78 mm Hg
Labs/studies: Unremarkable
Case #4: 58 year old with hypertension, worried about cancer scare

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Case #5: 68 year old with difficult to control hypertension
Chief complaint: 68 year old male referred by PCP for resistant hypertension. Blood pressure has been slowly increasing over the past several years and now has become resistant to prescribed therapies.
PMH: hypertension, migraines
Medications: Amlodipine 10 mg, valsartan 320 mg daily, Chlorthalidone 50 mg daily
Physical Exam: BP 147/86 mm Hg, BMI 33
Labs/studies: Unremarkable
What Is Resistant Hypertension?
BP not on target
Three drugs used
At appropriate doses
One is a diuretic
You have a patient who is adherent to medications and lifestyle measures, BUT…
Resistant hypertension is primarily a systolic and age related problem
Diastolic BP goal achieved ≥ 90% in the major trials
Systolic BP goal achieved 60‐65% in the major trials
True resistance occurs in about 15%
Resistant Hypertension is more common in the elderly
Resistant HypertensionCause of resistance found in 94% of cases
Garg JP, et al. Am J Hypertens 2003;16:925-930
Drug-relatedcauses
58%
Nonadherence16%
Unknown6%
Officeresistance
6%Psychologicalcauses
9%
SecondaryHTN5%
Interferingsubstances
1%

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Secondary Cause of HTN
When to evaluate for secondary cause?
1.Unusual presentation of hypertension‐ Severe‐ Sudden‐ Very young or very old‐ Resistant
2.Clinical clues suggesting a particular form of secondary hypertension
Calhoun DA, et al. Circulation. 2008;117(25):e510‐e526.
Coarctation of aortaSleep ApneaIllicit drugsPheochromacytoma
Renal Artery StenosisRenal failureHypervolemiaPreeclampsia
HyperaldosteronismSalt overconsumptionNSAID useAcromegaly (anti-natriuretic action of GH)Hyperparathyroidism
Causes of Secondary HypertensionCauses of Secondary HypertensionTOO MUCH SYMPATHETIC ACTIVITY
TOO MUCH WATER
TOO MUCH SODIUM
Secondary Causes of Hypertension
COMMON RARESleep Apnea (Very Common) Pheochromocytoma (<0.5%)
Renal Disease (1‐8%) Coarctation of Aorta (<1%)
Hyperaldosteronism (1.5‐15%) Cushing’s Syndrome (0.5%)
Renal Artery Stenosis (3‐4%) Acromegaly
Obstructive Sleep Apnea
Obstructive Apnea◦ Apnea/Hypopnea ◦ Hypoxia◦ Hypercapnia
Resumption of breathing◦ Labile blood pressure
• Fragmented sleep• Increased sympathetic activity

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Somers et al. J Clin Invest. 1995;96:1897.
Sympathetic Activity in Sleep Apnea Blood Pressure in OSA
Effect of CPAP on Blood Pressure
Becker et al, 2003
15
10
5
0
-5
-10
-15
-20
-25
MAP systolic diastolic
mm
Hg
* * *
Active CPAP Control CPAP
OSA is a common cause of resistant HTN. Effective treatment can decrease mean BP by 10mmHg.

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Follow up: Patient underwent sleep study and found to have severe obstructive sleep apnea (apnea: hypopnea index of 32). CPAP begun
Follow up Medications: No change
Follow up Physical Exam: BP 129/80 mm Hg
Labs/studies: Unremarkable
Case #5: 68 year old with difficult to control hypertension
Case #6: 58 year old who complains about amlodipine
Chief complaint: 58 year old female referred by PCP for complaints about amlodipine. PCP has tried multiple antihypertensive regimens and the only time she was able to gain control was when amlodipine was added. Patient complains of lower extremity edema
PMH: hypertension, metabolic syndrome
Medications: Amlodipine 10 mg, HCTZ 12.5 mg daily
Physical Exam: BP 118/78 mm Hg, 1‐2+ ankle edema
Labs/studies: Unremarkable
Calcium Channel Blockers and Edema
CCBs dilate here
ACE/ARB dilate here
CapillaryAfferent arteriole Efferent arteriole

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Adding an ACE inhibitor or an ARB to a CCB can decrease edema
Follow up: Amlodipine dose lowered; An ARB was added to the regimen
Follow up Medications: Amlodipine 5 mg, Benazepril 20 mg, HCTZ 12.5 mg daily
Follow up Physical Exam: BP 125/65 mm Hg, NO ankle edema
Labs/studies: Unremarkable
Case #6: 58 year old who complains about amlodipine
Case #7: Young man referred by PCP for elevated BPChief complaint: 21 year old male track star referred by PCP for elevated BP. Secondary causes have been ruled out. Patient states “I won’t take medications”
PMH: Elevated BP
FH: Severe hypertension (early onset) in multiple family members. Father died at age 44 of MI, mother suffered TIA last year
Medications: None
Physical Exam: BP 128/88 mm Hg
Labs/studies: Unremarkable
Categories of BP in Adults
BP Category SBP DBP
Normal <120 mm Hg and <80mm Hg
Elevated 120–129 mm Hg and <80 mm Hg
Hypertension
Stage 1 130–139 mm Hg or 80–89 mm Hg
Stage 2 ≥140 mm Hg or ≥90 mm Hg
J Am Coll Cardiol. 2017 Nov
130 is the new 140

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
JAMA Cardiol. 2018;3(5):427-431. doi:10.1001/jamacardio.2018.0250
Trajectories of BP elevation preceding diagnosis of HTN: Framingham
Whelton PK et al. JAMA. 1997;277:1624-1632.
Nonpharmacologic Interventionsand BP Reduction
BP
Dec
reas
e(m
m H
g)
SBP DBP
ExerciseLow-Salt
DietAlcohol
ReductionPotassiumRepletion
5
4
3
2
1
0
6
7
Weight Loss(19.4 lb)
The Role of Potassium in Hypertension
Potassium deficit is critical in hypertension
Recent evidence as well as classic studies point to the interaction of sodium and potassium, as compared with an isolated abnormality of either alone, as a dominant factor in hypertension
Processed foods are high in sodium and low in potassium; Conversely, fruits and vegetables are sodium‐poor and potassium‐rich
The Institute of Medicine (IOM) recommendations: 4.7 grams K+ per day (4 ½ cups, 9‐10 servings)
‐Whelton PK. Potassium and blood pressure. In: Izzo JL Jr, Black HR, eds. Hypertension primer. 3rd ed. Dallas: American Heart Association/Council on HighBlood Pressure Research, 2003:280‐.;He FJ, MacGregor GA. Beneficial effects of potassium. BMJ 2001;323:497‐501; Dietary reference intakes for water,potassium, sodium, chloride, and sulfate. National Academies Press, 2005.
Salt Sensitivity related to potassium intake
J Am Coll Nutr June 2006 vol. 25 no. suppl 3 262S‐270S
• Black and White men were maintained on diets of varying Potassium levels.
• Then given 7‐days of salt loading and salt sensitivity measured
• On the low K+ diet, 80% of Black and 35% of White men were salt sensitive
• As potassium intake INCREASED, salt sensitivity DECREASED.
• On the high K+ diet, only 20% of the Black men, and none of the White men remained salt sensitive
African American White

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
DASH diet is rich in potassium
DASH = Dietary Approaches to Stop Hypertension
The diet is rich in fruits, vegetables (high K+), low fat dairy foods, and low in fat, total fat, cholesterol and salt
Appel, et al. Circulation, 102:852, 2000
Follow up: Dietary history reviewed. Patient admits to eating out most nights (high salt) and rarely, if ever, eating fruits and vegetables. Dietary counseling given and patient adopted recommendations
Follow up Medications: No medications
Follow up Physical Exam: BP 118/70 mm Hg
Labs/studies: Unremarkable
Case #7: Young man referred by PCP for elevated BP
Chief complaint: 68 year old female referred by PCP for resistant HTN. Secondary causes have been ruled out.
PMH: Severe hypertension, rheumatoid arthritis, CKD
Medications: Amlodipine 10 mg, Chlorthalidone 50 mg, Olmesartan 40 mg, rosuvastatin 10 mg
Physical Exam: BP 158/92 mm Hg, BMI 34
Labs/studies: Cr – 1.2, K+ ‐ 3.9
Case #8: Middle aged woman with resistant hypertension
Aldosterone Levels are Increased in Obesity
Krug A W , and Ehrhart-Bornstein M Hypertension. 2008;51:1252-1258

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Hyperaldosteronism is much more common today – in part due to the obesity epidemic
Spironolactone
• ASCOT Trial: 1,411 patients failing a 3‐drug regimen
• Spironolactone 25 mg once daily added
• Results: With addition of spironolactone, mean BP fell by 21.9/9.5 mm Hg (P<0.001).
Chapman N, et al. Hypertension. 2007;49:839-845.
Spironolactone can be effective in patients with resistant hypertension
• Adverse events: Gynecomastia (6%); biochemical abnormalities (2%) (mainly hyperkalemia)
Nishizaka MK, et al. Am J Hypertens 2003;16;925-930
Spironolactone (Aldosterone antagonist)
-21
-10
-23
-10
-25
-12
-30-25-20-15-10
-50
BP
resp
onse
(mm
Hg) 6wk 3mo 6mo
Systolic BP Diastolic BP
Patients with resistant hypertension who were documented to have normalaldosterone levels. Treated with a diuretic and ACE inhibitor or ARB In patients with resistant hypertension, it
is reasonable to give a trial of Spironolactone
But watch K+ carefully

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Follow up: Spironolactone added to regimen
Follow up Medications: Amlodipine 10 mg, Chlorthalidone 50 mg, Olmesartan 40 mg, rosuvastatin 10 mg, Spironolactone 25 mg daily
Follow up Physical Exam: BP 128/70 mm Hg
Labs/studies: Cr – 1.2, K+ ‐ 4.6
Case #8: Middle aged woman with resistant hypertension
Chief complaint: 59 year old male with hypertension. Self‐referred with Chief complaint: “I take too many darn pills!”
PMH: Hypertension, BPH, GERD
Medications: Amlodipine 5 mg, HCTZ 12.5 mg, olmesartan 20 mg
Physical Exam: BP 128/82 mm Hg, BMI 30
Labs/studies: Cr – 0.9
Case #9: Patient with hypertension complains “I take too many darn pills!”
Shallow dose‐response for antihypertensives
mm Hg BP
drop
010
20
Fraction of pill
CCBACE‐i
¼ ½ 1 2 4 8 ¼ ½ 1 2 4
Thiazides
¼ ½ 1 2 4
BMJ volume 326 28 June 2003 bmj.com
BP lowering effect of “doubling dose” of 1 agent or “combination” of lower doses of 2 agents
-104 -100-116
-89
-19 -23 -20
-37
-140
-120
-100
-80
-60
-40
-20
0Thiazide β-blocker ACE-I CCB
% a
dditi
onal
SB
P re
duct
ion
Wald et al. Combination Versus Monotherapy for Blood Pressure Reduction, The American Journal of Medicine, Vol 122, No 3, March 2009
Combination
Doubling dose

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Combining lower doses of antihypertensive agents improves BP control and limits side effects
Case #9: Patient with hypertension complains “I take too many darn pills!”
Follow up: Patient switched to the generic form of Tribenzor which contains olmesartan medoxomil 20 mg, amlodipine 5 mg, hydrochlorothiazide 12.5 mg
Follow up Medications: generic Tribenzor 1 tablet daily
Follow up Physical Exam: BP 128/70 mm Hg
Labs/studies: Cr – 0.9
Chief complaint: 89 year old woman with hypertension. Referred by PCP for very elevated HTN
PMH: Hypertension, hearing loss, HFpEF
Medications: Amlodipine 10 mg, Chlorthalidone 25 mg, valsartan 320 mg
Physical Exam: BP 188/82 mm Hg, BMI 22
Labs/studies: Cr – 1.5, GFR 35
Case #10: Very elderly woman with hypertension
Inclusion Criteria:Aged 80 or moreSystolic BP 160-199 mm Hg Informed consent
Target blood pressure150/80 mm Hg
3,845 elderly patients with STANDING SBP > 150 mm Hg randomized to Indapamide (thiazide‐like diuretic) + perindopril (ACE‐inhibitor)
Primary Endpoint:All strokes (fatal and non-fatal)
Exclusion Criteria:Standing SBP < 140 mm HgStroke in last 6 monthsDementiaNeed daily nursing care
N Engl J med 2008;358/ACC 2008

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Blood pressure results
70
80
90
100
110
120
130
140
150
160
170
180
0 1 2 3 4 5Follow-up (years)
Blo
od P
ress
ure
(mm
Hg)
Placebo
Indapamide SR +/-perindoprilIMedian follow-up 1.8 years
15 mm Hg
6 mm Hg
N Engl J med 2008;358/ACC 2008
P=0.055
Stroke results (30% reduction)
N Engl J med 2008;358/ACC 2008
P=0.019
N Engl J med 2008;358/ACC 2008
Total mortality (21% reduction)
P=0.046
N Engl J med 2008;358/ACC 2008
Fatal stroke (39% reduction)

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
P<0.0001
N Engl J med 2008;358/ACC 2008
Heart failure (64% reduction)
35%-40%
20%-25%
>50%
Average reduction
in events (%)
–60
–50
–40
–30
–20
–10
0Stroke Myocardial infarction Heart failure
Blood Pressure Lowering Treatment Trialists’ Collaboration. Lancet. 2000;355:1955-1964.
Long‐Term Antihypertensive Therapy Significantly Reduces CV Events
Follow up: Central aortic pressure was 145 mm Hg; Standing central aortic pressure was 140 mm Hg; No change in her medications was made
Follow up Medications: Amlodipine 10 mg, Chlorthalidone 25 mg, valsartan 320 mg
Follow up Physical Exam: BP 140/70 mm Hg
Labs/studies: Cr – 1.5
Case #10: Very elderly woman with hypertension