carlson (7e) chapter 17: schizophrenia and the affective disorders
Post on 22-Dec-2015
217 views
TRANSCRIPT

Carlson (7e) Chapter 17: Schizophrenia and
the Affective Disorders
Schizophrenia
Schizophrenia represents a disorder of thought and emotion but not a “split-personality” Thought disorder (e.g., loose associations) Hallucinations (e.g., auditory) Delusions (e.g., paranoia) Bizarre behaviors
The incidence of schizophrenia is about 1-2% No clear gender differences in incidence
17.2

Symptoms of Schizophrenia
Positive symptoms include delusions, hallucinations and thought disorder Delusions are beliefs that are contrary to reality
Delusions can involve control, grandeur, or persecution
Hallucinations are perceptions that occur in the absence of stimuli (often auditory and/or olfactory)
Thought disorder: disorganized and irrational
Negative symptoms involve a loss of normal behaviors, such as Poverty of speech and low initiative Social withdrawal and diminished affect Anhedonia 17.3

Heritability of Schizophrenia
The heritability of schizophrenia is a strong indicator of a biological basis for schizophrenia Adoption studies
Adult schizophrenics that were adopted as children are likely to have schizophrenic biological relatives.
Twin studies Concordance rates for schizophrenia are higher for
identical than for fraternal twins: No single gene has been identified for schizophrenia
Genes may pass on a susceptibility to develop schizophrenia
17.4
The Dopamine Hypothesis of Schizophrenia
The “dopamine hypothesis” is that the positive symptoms of schizophrenia involve over activity of brain dopaminergic synapses Chlorpromazine (CPZ) was identified as an effective
antipsychotic (AP) agent CPZ was later found to block DA receptors (D2 receptors) D2 receptor blockade correlates with clinically effective dose
of typical antipsychotic medications
Stimulants such as amphetamine that release DA can produce the positive symptoms of schizophrenia in “normals” and relapse in schizophrenics 17.5
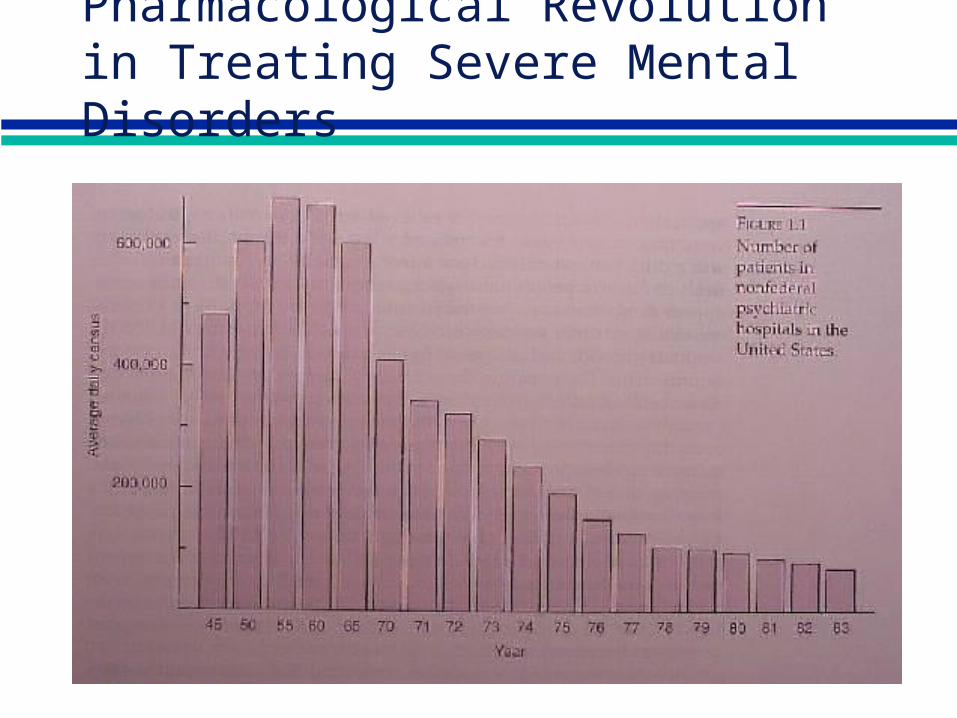
Pharmacological Revolution in Treating Severe Mental Disorders
DA Activity in Schizophrenia
PET studies indicate greater activity of dopamine in the striatum of schizophrenics to a test dose of amphetamine Amount of dopamine activity was related to the increase in positive
schizophrenia symptoms Studies of dopamine receptors in schizophrenic brain have
provided mixed results (but generally supportive) Postmortem studies suggest increased numbers of D2 receptors in
striatum (but may be due to exposure to antipsychotic drugs) The striatum is a motor control region: may be the wrong site Schizophrenia may be related to D4 or D3 receptors
Clozapine is an effective (atypical) antipsychotic drug that interacts with D4 and not D2 receptors
strong effect on mesolimbic/mesocortical dopamine system (A10) little effect on nigrostriatal dopamine system (A9)
17.7
Dopamine Augmentation & Schizophrenia
Psychomotor stimulants (e.g., amphetamine) ‘normals’ develop paranoid psychosis schizophrenics release -- subjectively indistinguishable for
worsening of endogenous illness (cf. LSD) L-DOPA (precursor loading)
little or no effect in ‘normals’ worsening of psychotic symptoms in schizophrenics schizophrenic symptoms in some Parkinson’s patients
Stress (increased dopaminergic activity) precipitate relapse & perhaps even initiate disorder

Dopamine Attenuation & Schizophrenia
DA synthesis inhibitors (e.g., AMPT) abate schizophrenia
DA storage depleters (e.g., reserpine) abate schizophrenia
D2 receptor blockers (e.g., typical antipsychotics) abate schizophrenia
Even atypical antipsychotics (which do not effectively block D2 receptors) influence mesolimbic DA activity

Antipsychotic Medications
Antipsychotic medications diminish the thought disorder & disruptive behavior evident in schizophrenia
Side effects of antipsychotic medications include Major
Extrapyramidal (Parkinsonism-like) side effects due to blockade of DA receptors
Tardive dyskinesia: facial tics and gestures due to an over stimulation of DA receptors (may be related to CNS sensitization and relapse)
Minor Autonomic problems (dry mouth) Skin-eye pigmentation Breast development (increased prolactin release after blockade of dopamine
neurons)
17.10
Brain Damage and Schizophrenia
The negative symptoms of schizophrenia may be related to brain damage The neurological signs evident in schizophrenia include
Eye tracking problems Catatonia Problems with blinking, eye focusing, and visual pursuit
Schizophrenics exhibit enlarged brain ventricles, which suggests loss of brain cells
Regions of schizophrenic brain that are abnormal include Prefrontal cortex Medial temporal lobes Medial diencephalon
17.11
Causes of Brain Damage in Schizophrenia
The neurological symptoms of schizophrenia may be caused by Birth trauma (obstetrical issues) Viral infections that impair neural development during the
second trimester Seasonality effects (schizophrenia is more likely for winter births)
Nutritional issues (Hunger Winter: female offspring were more likely to exhibit schizophrenia than male offspring)
Maternal stress may compromise the immune system of the mother and lead to a greater chance of contracting a viral infection
17.12
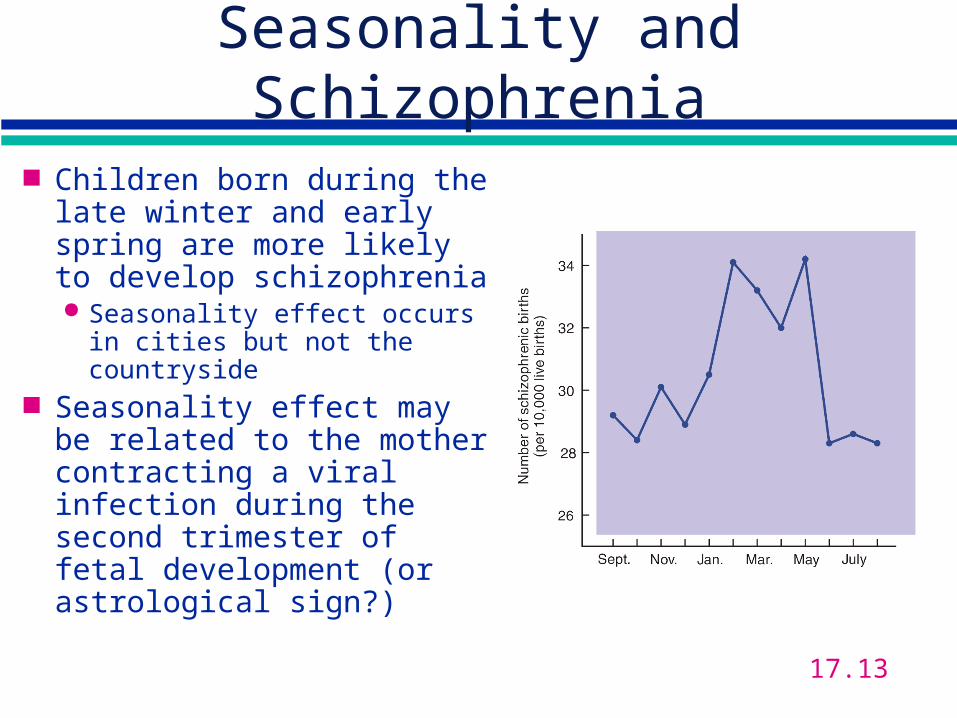
Seasonality and Schizophrenia
Children born during the late winter and early spring are more likely to develop schizophrenia Seasonality effect occurs in
cities but not the countryside Seasonality effect may be
related to the mother contracting a viral infection during the second trimester of fetal development (or astrological sign?)
17.13

Hypofrontality and Schizophrenia
Hypofrontality refers to the decreased activity of the dorsolateral prefrontal cortex Damage to the prefrontal cortex
impairs behavioral flexibility (card sorting task) may disinhibit mesolimbic dopamine system
Schizophrenics show decreased activity in the prefrontal cortex
Abuse of PCP produces positive and negative symptoms of schizophrenia Positive: related to indirect actions of PCP on accumbens DA Negative: related to decreased DA utilization in prefrontal cortex
following PCP treatment Data are less compelling that dopamine-agonist effect
17.14

Major Affective Disorders
Affect refers to emotions, moods, and feelings Our affect is usually a reflection of our experiences In the major affective disorders, our emotional
reactions are at the extremes and may not be related to our actual experiences
The major affective disorders include Bipolar disorder - alternating cycles of
Mania: euphoria, delusions Depression: profound sadness, guilt, suicide risk
Unipolar depression: continuous, episodic
17.15
Biological Bases of Affective Disorder
Heritability of affective disorder (AD) has been established in twin studies and family studies Bipolar disorder may be related to a single gene
Depression is amenable to physical treatments including Pharmacological treatments
MAO inhibitors (e.g. iproniazid) Noradrenergic reuptake inhibitors (desmethylimipramine) Serotonin reuptake inhibitors (e.g. Prozac)
Electroconvulsive shock therapy (ECS) Sleep deprivation 17.16
Monoamine Hypothesis of Depression
Depression results from reduced activity of brain monoamines Reserpine depletes monoamines--> depression Suicidal depression is related to a low level of
5-HIAA Antidepressant medications increase either NE or
5-HT Usually via blockade of monoamine reuptake
Tryptophan deletion procedure: Reduces brain 5-HT levels Reinstates depression in former depressed patients
17.17

Antidepressant Medication and 5-HT
17.18

REM Sleep and Depression
Sleep pattern is disrupted in depressed persons Reduced REM latency, reduced stages 3 and 4 sleep
REM deprivation improves mood Antidepressant drugs suppress REM sleep, and
increase slow-wave sleep Persons who have short REM sleep latency are
more likely to develop depression REM sleep deprivation is more effective than is
total sleep deprivation (effects last longer)
17.19
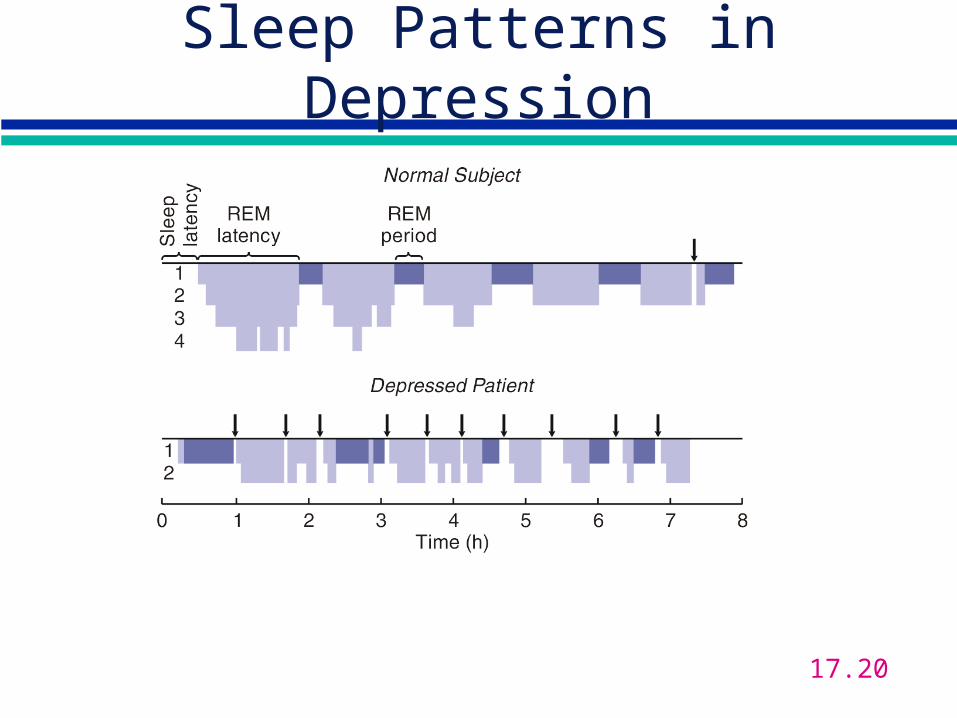
Sleep Patterns in Depression
17.20
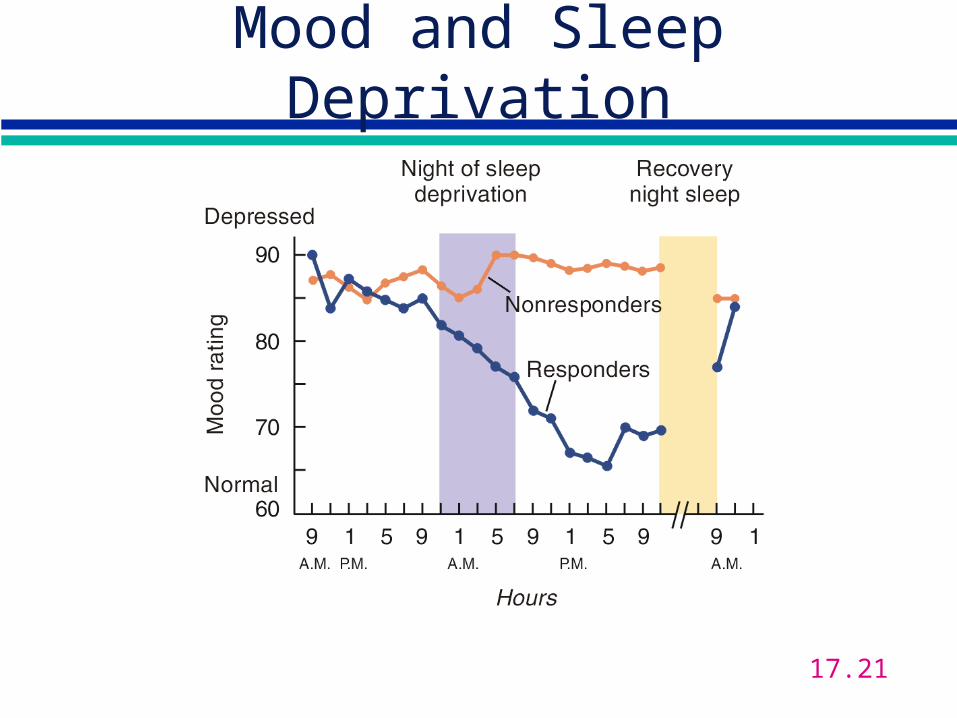
Mood and Sleep Deprivation
17.21

Seasonal Affective Disorder
SAD is a form of depression evident in winter months (short days/long nights)
SAD involves Mood and sleep disturbances Carbohydrate cravings and weight gain
Phototherapy for SAD: increased exposure to light improves mood in SAD (and also for unipolar depression)
17.22