caring for the critical and ventilated covid-19 patient in ... · information contained in this...
TRANSCRIPT
Caring for the Critical and Ventilated COVID-19 Patient
in the EDWebinar Presentation
Tuesday 30th March 2020Repeated Wednesday 1st April 2020
Presented byDavid CorkillEmergency Nurse EducatorMEmergN, MAdvPrac (Hth Prof Edu), BN, Dip App Sc
Disclaimer The information around COVID-19 is rapidly changing. This information was developed using the most up to date resources available. However as new information emerges, this may rapidly change the recommendations provided and become obsolete.
The practice of clinical care is a complex interaction of experience, common sense and good judgement. Information contained in this material is no substitute for clinical expertise, thoughtful contemplation and technical experience.
Every patient problem is unique, and so should be the approach to delivering acute emergency care. Use this information carefully, thoughtfully, and at your own risk.

Intubation and Ventilation For ED Nurses
An online webinar workshop
Topics:
- Equipment of Intubation - Airway Management - Drugs of Intubation - Rapid Sequence Induction - Difficult Airways - Post Intubation Care - Modes of Ventilation - Ventilation Strategies
Dates :
- Course Date: 14th-18th April 2020 - Time: 1030hrs-1230hrs (AEST) - Location: Your table/couch/Your house - CPD Points: 8 Points All live sessions recorded and available to watch at a
later date, Includes certificate and USB with all talks
and further reading
www.thinkasklearn.com.au
Registrations :
- Don’t miss out on this fantastic workshop
- Book in via website or via form
PO Box 458 Chirn Park, QLD, 4215
Web: www.thinkasklearn.com.au Email: [email protected]
ABN: 78 119 360 846
Intubation and Ventilation for ED Nurses An online webinar workshop - 14th-18th April
Registration Form 2020 Please complete and return via mail or email to [email protected]
Mailing address required to post Certificate and USB with talks and further readings
Registration Refund Policy: Cancellation fourteen (14) or more days before workshop – 100% refund minus $50 administration fee. No refunds for cancellations within fourteen (14) days of the workshop.
Online Webinar Workshop Registration - $155
Payment Options
Paid via Website
Payment by EFT
BSB 638 060 Account No 13277308 Name Think Ask Learn Pty ltd
Credit Card Visa Mastercard Amount _$__________
Name on Card ____________________________________________
Card Number ____________________________________________
Expiration Date _________________ CCV____________
Signature _______________________________________
Credit card payments via this form attracts 3.6%+ $.30 merchant fee surcharge
Please keep me informed via email of future events Yes No
Registration Details
Title:
First Name:
Last Name:
Postal Address
Suburb Postcode
Course Date/Location
Mobile Phone:
Email:
Employed At:
Unit and Position:
www.thinkasklearn.com.au
ThinkAskLearn
www.thinkasklearn.com.au 1
www.thinkasklearn.com.au
CaringfortheCriticalandVentilatedCOVID-19PatientintheED
DavidCorkillEmergencyNurseEducatorMEmergN,MAdvPrac(HthProfEdu),BN,DipAppSc
IntubationandVentilation
ForNursesWorkshop
2020DatesOnlineWebinarWorkshop-14th-18thApril
Brisbane5thJuneMelbourne14thAugGoldCoast27thNov
ThinkAskLearn www.thinkasklearn.com.

ThinkAskLearn
www.thinkasklearn.com.au 2
2020 Dates* 4th June Brisbane
13th Aug Melbourne 26th Nov Gold Coast
ThinkAskLearn www.thinkasklearn.com.
AdvancedCardiacLifeSupportCourse
GoldCoast26th/27thMarch 10th/11thSept
ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn
www.thinkasklearn.com.au 3
CareoftheCrashingED
PatientWorkshop
Onecourseonly!Brisbane28thAug2020
ThinkAskLearn www.thinkasklearn.com.
Paediatric Emergency Nursing
Workshop Online May 12th-15th Adel – 30th Oct 2020
ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn
www.thinkasklearn.com.au 4
AcuteComplexCareCourse
6DayIntensiveCourseCreditforPostGradStudy/PD
ACLScourseincludedDifferentAssessmentModes
June&Oct2020ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn
www.thinkasklearn.com.au 5
ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn
www.thinkasklearn.com.au 6
ThinkAskLearn www.thinkasklearn.com.
Ifyouarehavingtroublehearingmeorseeingmethenjumpoutofthewebinarroomandjumpbackin
ProblemswithWebinar
ThinkAskLearn
www.thinkasklearn.com.au 7
www.thinkasklearn.com.au
CaringfortheCriticalandVentilatedCOVID-19PatientintheED
DavidCorkillEmergencyNurseEducatorMEmergN,MAdvPrac(HthProfEdu),BN,DipAppSc
• OwnerandDirectorThinkAskLearn–HealthProfessionalEducationCompany
• Receivesnomoniesorinkindsupportfromanypharmaceuticalorequipmentcompanies
Disclaimer
ThinkAskLearn
www.thinkasklearn.com.au 8
ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn www.thinkasklearn.com.

ThinkAskLearn
www.thinkasklearn.com.au 9
• DonningandRemovingPPE• TestingofsuspectedCOVID-19patients• EfficacyofTestkits• ManagingnoncriticalCOVID-19patients• VentilatorTriageDecisions• PresumedAsymptomaticCarrierTransmissionofCOVID-19
• NursingHomesArePotentialGroundZeroforCOVID-19Pandemic
Notontoday’swebinar
• WhatPPEtousewhen(briefIpromise)• 3slides– 1scary,1hopeful,1Idon’tknow
• InformationfromtheUK• IntubationofCOVID-19patient• SetupforVentilation• Otherstrategiesrequired
Wewillcover
ThinkAskLearn
www.thinkasklearn.com.au 10
ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn
www.thinkasklearn.com.au 11
FaceMaskinClinicalAreaNonCovidPt
ThinkAskLearn www.thinkasklearn.com.
AustGov30thMarch2020ThinkAskLearn www.thinkasklearn.com.

ThinkAskLearn
www.thinkasklearn.com.au 12
ThinkAskLearn www.thinkasklearn.com.
https://www.brisbanetimes.com.au/national/queensland/queensland-hospitals-very-low-on-gloves-masks-gowns-and-told-to-re-use-20200317-p54azh.htmlThinkAskLearn www.thinkasklearn.com.

ThinkAskLearn
www.thinkasklearn.com.au 13
ForCloseorProlongedContactOnlyofwellCOVID-19pt
ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn
www.thinkasklearn.com.au 14
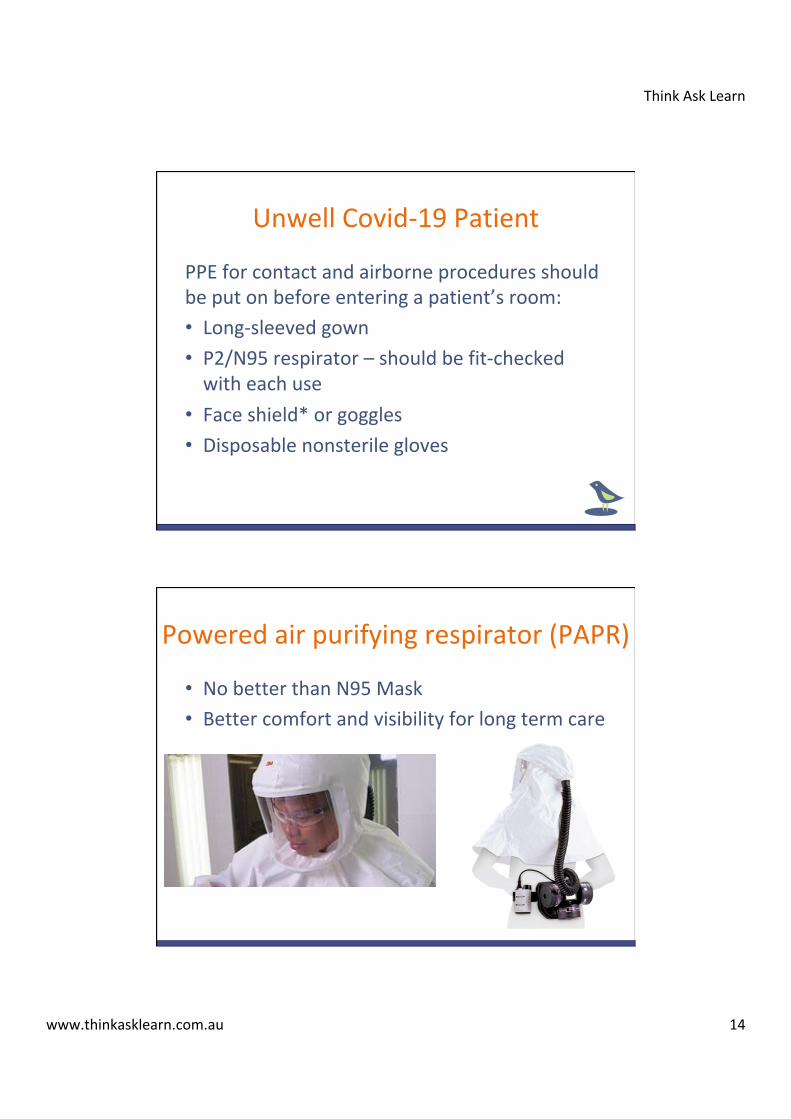
UnwellCovid-19Patient
PPEforcontactandairborneproceduresshouldbeputonbeforeenteringapatient’sroom:• Long-sleevedgown• P2/N95respirator–shouldbefit-checkedwitheachuse
• Faceshield*orgoggles• Disposablenonsterilegloves
• NobetterthanN95Mask• Bettercomfortandvisibilityforlongtermcare
Poweredairpurifyingrespirator(PAPR)
ThinkAskLearn
www.thinkasklearn.com.au 15
PresumethatanycriticallyillpatientisCOVIDpositiveuntilprovenotherwise First10EMThinkAskLearn www.thinkasklearn.com.
ILCOR–DraftStatement
• “Wesuggestitmaybereasonableforhealthcareproviderstoconsiderdefibrillationbeforedonningaerosolgeneratingpersonalprotectiveequipmentinsituationswheretheproviderassessesthebenefitsmayexceedtherisks(goodpracticestatement)”
ILCOR31stMarch2020
ThinkAskLearn
www.thinkasklearn.com.au 16
www.thinkasklearn.com.au
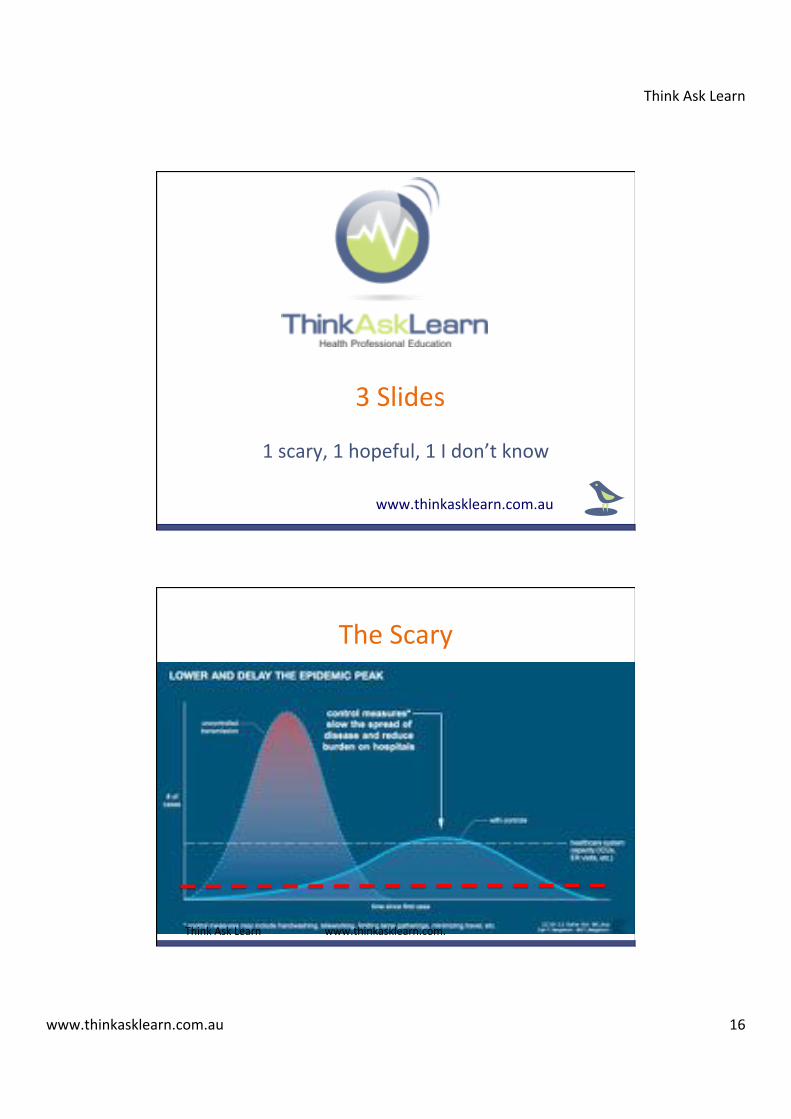
3Slides
1scary,1hopeful,1Idon’tknow
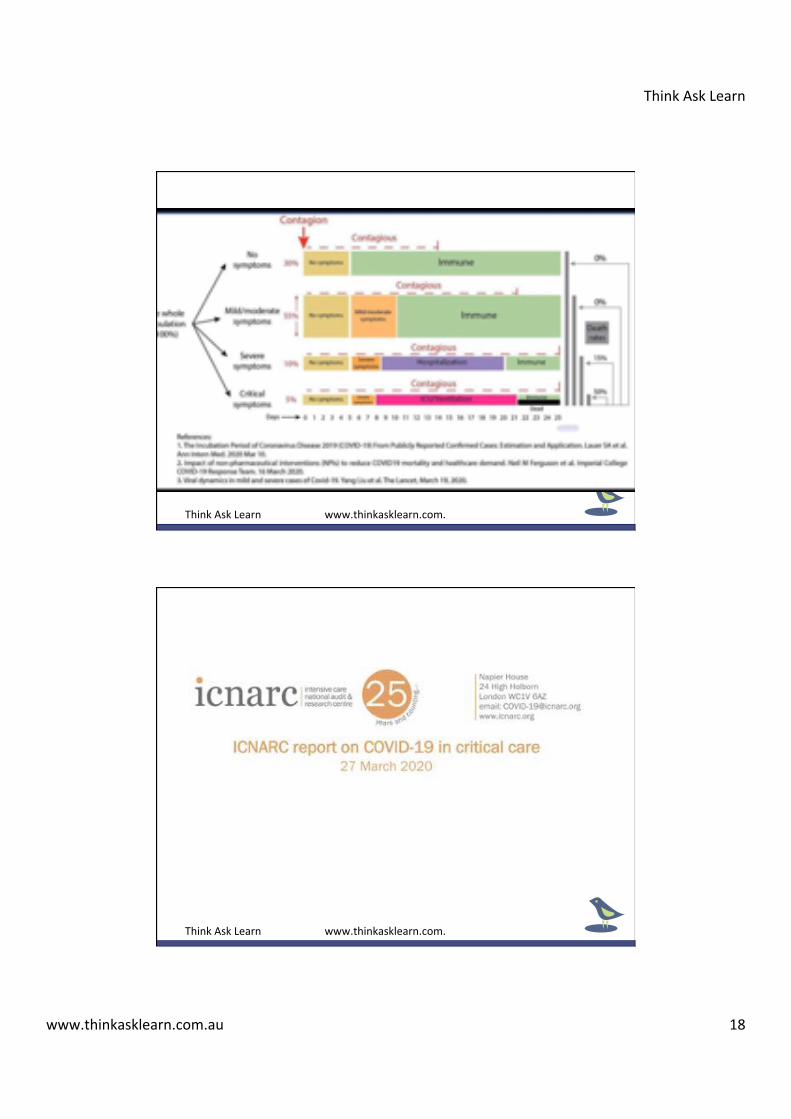
TheScary
ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn
www.thinkasklearn.com.au 17
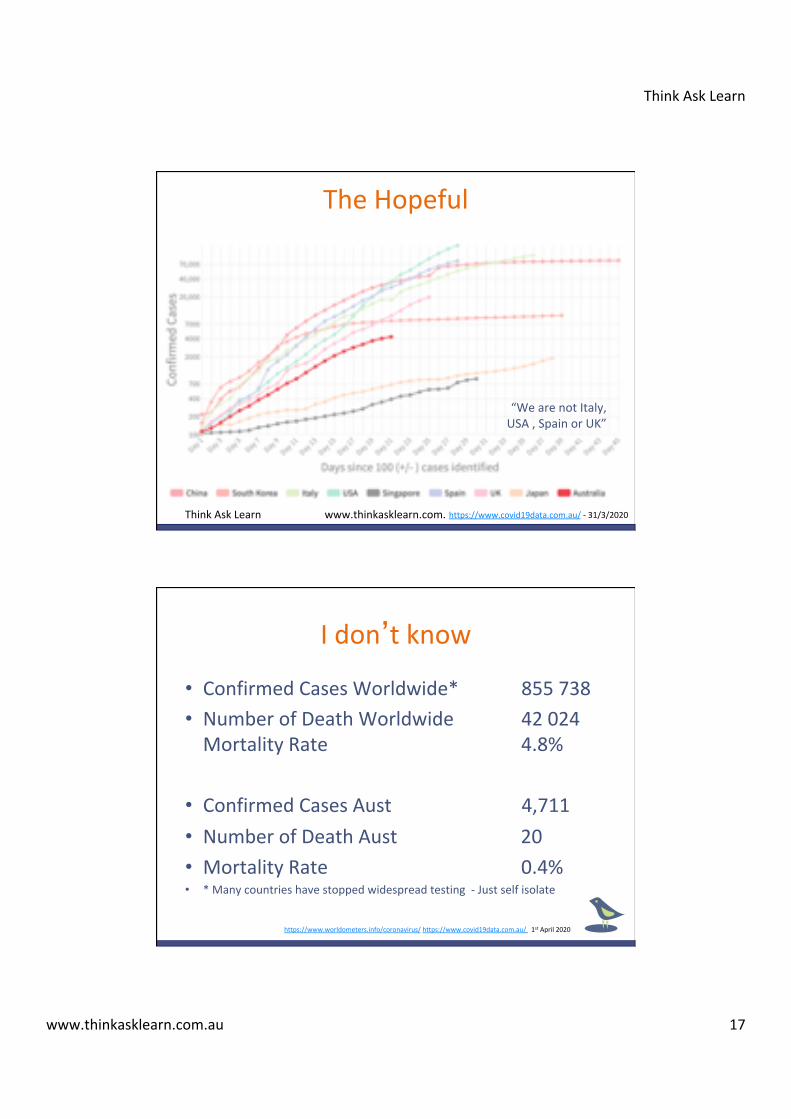
TheHopeful
“WearenotItaly,USA,SpainorUK”
https://www.covid19data.com.au/-31/3/2020ThinkAskLearn www.thinkasklearn.com.
• ConfirmedCasesWorldwide*855738• NumberofDeathWorldwide42024MortalityRate4.8%
• ConfirmedCasesAust4,711• NumberofDeathAust20• MortalityRate0.4%• *Manycountrieshavestoppedwidespreadtesting-Justselfisolate
Idon’tknow
https://www.worldometers.info/coronavirus/https://www.covid19data.com.au/1stApril2020
ThinkAskLearn
www.thinkasklearn.com.au 18
ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn www.thinkasklearn.com.
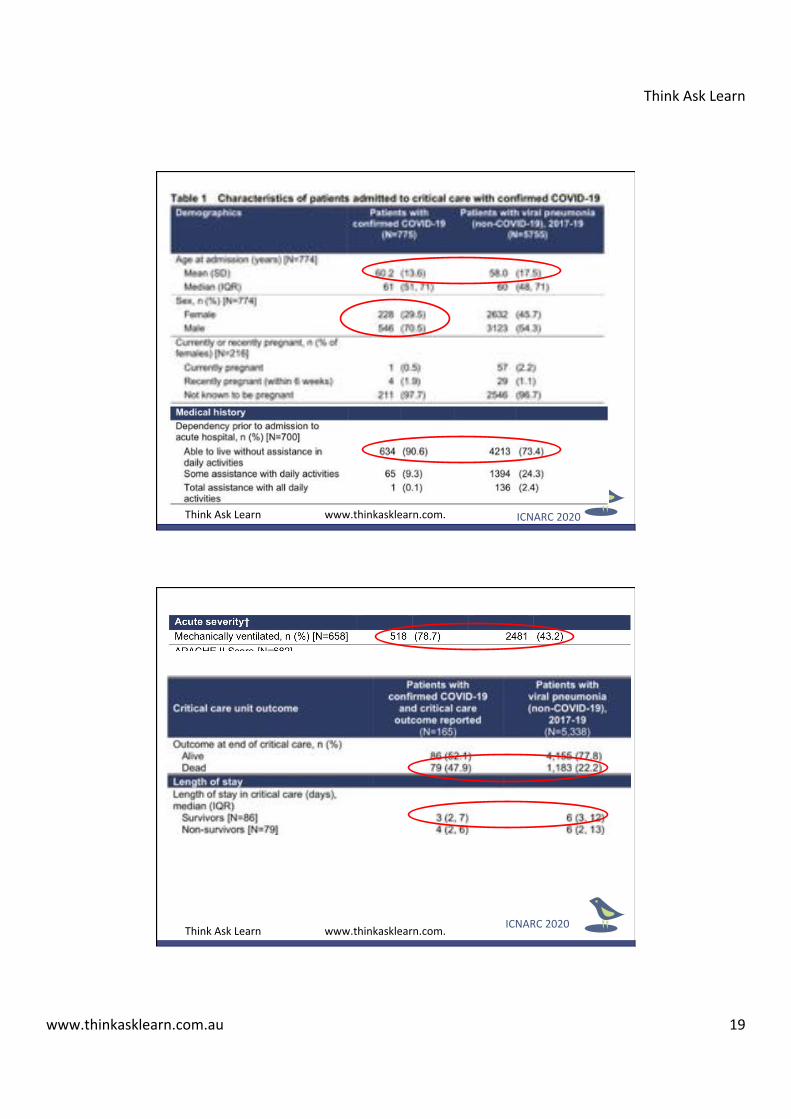
ThinkAskLearn
www.thinkasklearn.com.au 19
ICNARC2020ThinkAskLearn www.thinkasklearn.com.
ICNARC2020ThinkAskLearn www.thinkasklearn.com.
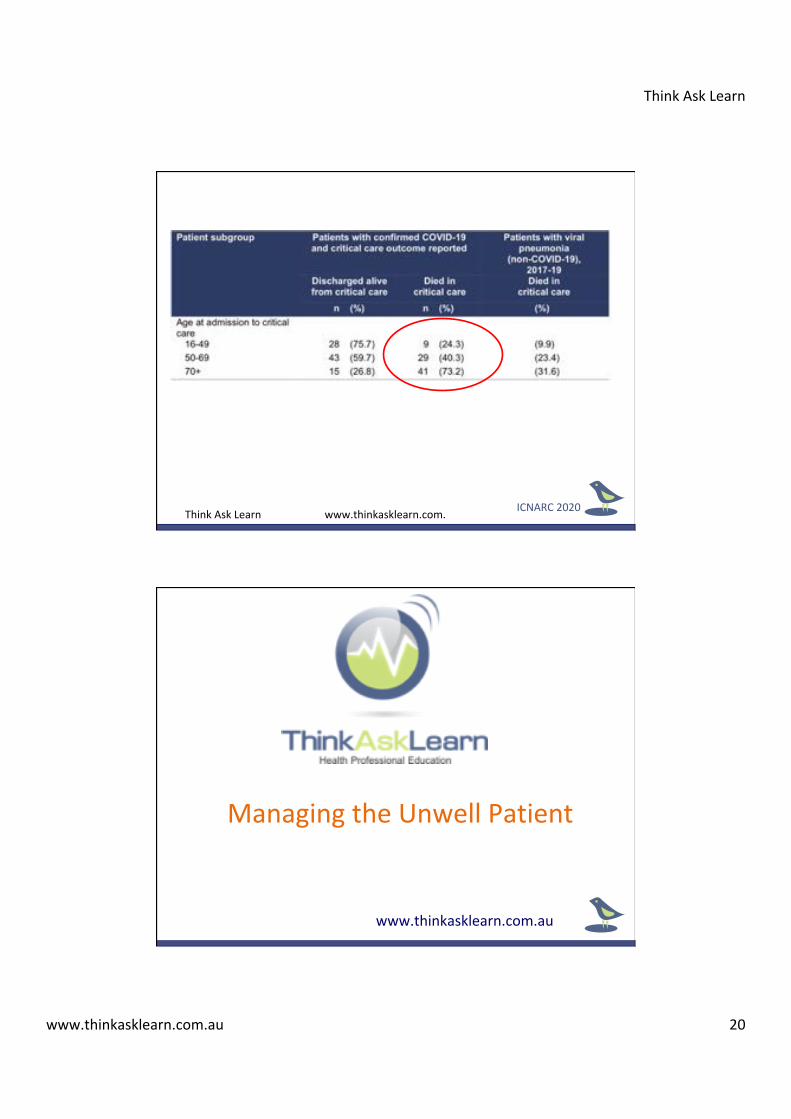
ThinkAskLearn
www.thinkasklearn.com.au 20
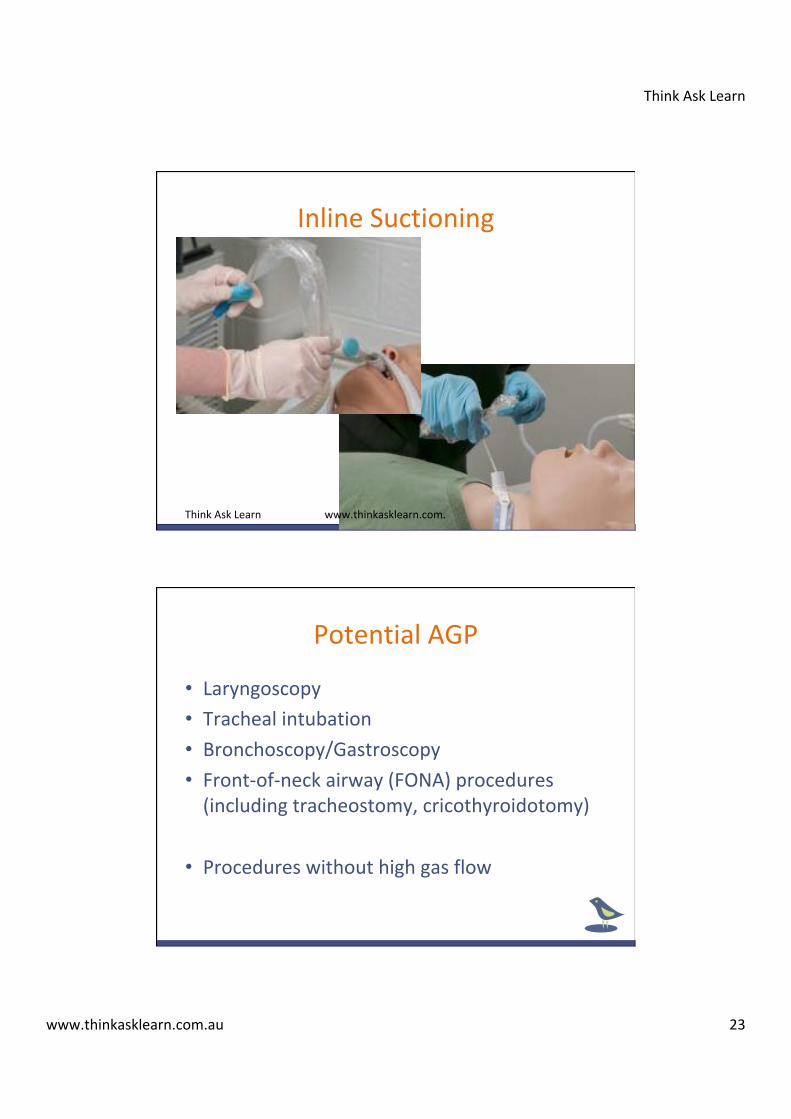
ICNARC2020ThinkAskLearn www.thinkasklearn.com.
www.thinkasklearn.com.au
ManagingtheUnwellPatient

ThinkAskLearn
www.thinkasklearn.com.au 21
ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn www.thinkasklearn.com.

ThinkAskLearn
www.thinkasklearn.com.au 22
Aerosol-generatingprocedures
ThinkAskLearn www.thinkasklearn.com.
Aerosol-generatingprocedures(AGPs)
• NIVorpositivepressureventilationwithinadequateseal*
• Highflownasaloxygen(HFNO)• Deliveryofnebulised/atomisedmedicationsviasimplefacemask
• Cardiopulmonaryresuscitation(priortointubation)
• Trachealsuction(withoutaclosedsystem)• Trachealextubation• Disconnectionofventilatortubing
ThinkAskLearn
www.thinkasklearn.com.au 23
InlineSuctioning
ThinkAskLearn www.thinkasklearn.com.
• Laryngoscopy• Trachealintubation• Bronchoscopy/Gastroscopy• Front-of-neckairway(FONA)procedures(includingtracheostomy,cricothyroidotomy)
• Procedureswithouthighgasflow
PotentialAGP
ThinkAskLearn
www.thinkasklearn.com.au 24
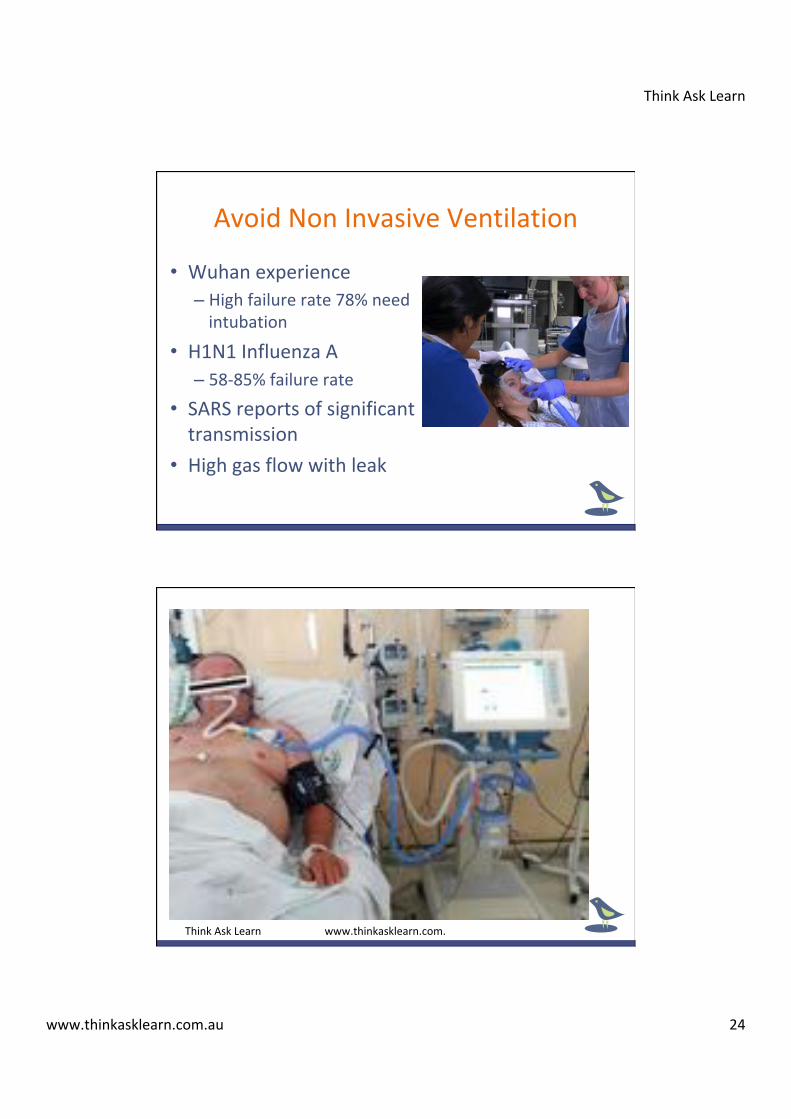
• Wuhanexperience– Highfailurerate78%needintubation
• H1N1InfluenzaA– 58-85%failurerate
• SARSreportsofsignificanttransmission
• Highgasflowwithleak
AvoidNonInvasiveVentilation
ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn
www.thinkasklearn.com.au 25
• Nothelpfulincriticalunwellpatient• Evidenceisunclearasto‘normaluseinED’• SomereportsbeingusedtoassistCOVID-19– Likelymilderdisease
• Riskofaerosolislikelylow(wethink)– Lowerthancoughing
• RiskvsBenefit–Donotuse– Revisitthiswhenventilatorsbecomescarce– ICUconsideringuse,-vepressureroom,airbornePPE
HighFlowNasalOxygen
NoNebulizer,Everyagain?
ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn
www.thinkasklearn.com.au 26
ThinkAskLearn www.thinkasklearn.com.
The10P’sofIntubation
• Prepare– Checklist
• Personnel• Prepare– Equipment
• Pumpset– IVfluids
• Positioning– Patient
• Pre-oxygenate• Pre-medicate• Paralyse• Perform– Intubation
• Placement– Confirm
• Phew!
ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn
www.thinkasklearn.com.au 27
• Variationstonormalworkflow• Unfamiliarworkingenvironments• Unfamiliarmultidisciplinaryteams• Potentialresourcedepletion• Criticallyillpatientswithlimitedphysiologicalreserves
• Clinicianstressandfatigue
ChallengestoStaffinIntubation
Quote
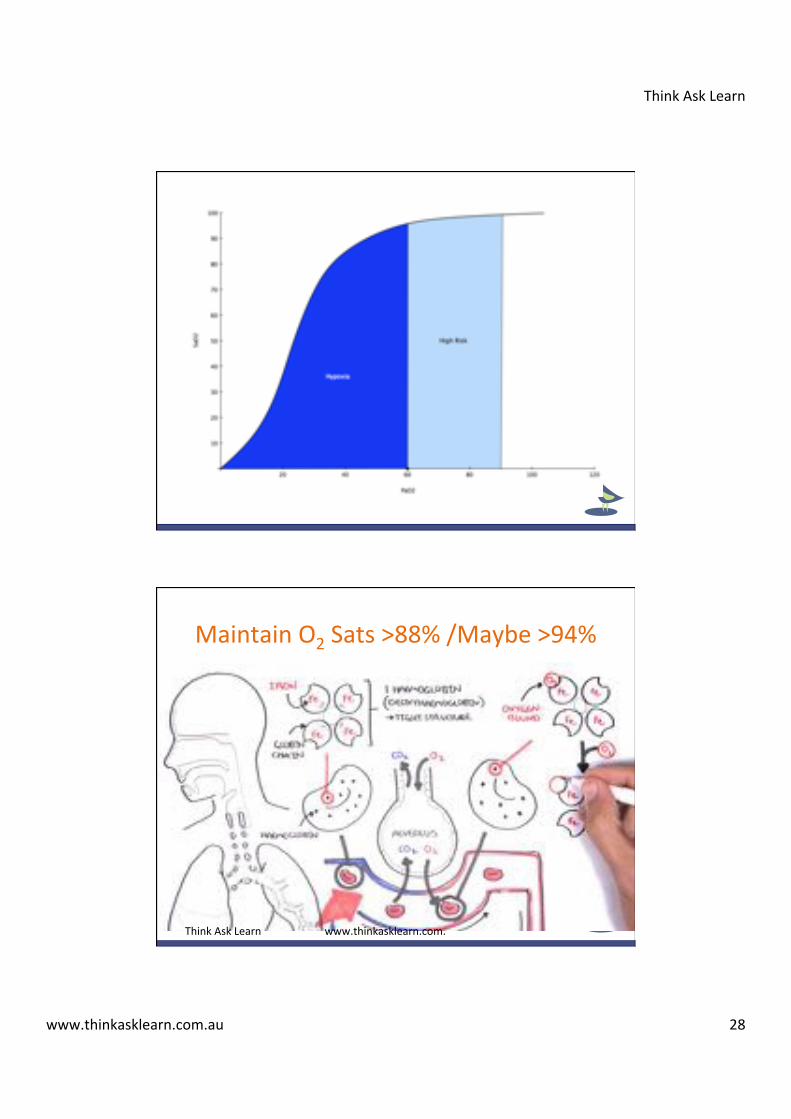
�Careandtimetakenduringthispreparationandassessmentphaseofintubationpaysgreatsdividendswhenthesequenceisinitiated.�
RonWalls(2020)EmergencyAirwayManagement5thEd
ThinkAskLearn
www.thinkasklearn.com.au 28
MaintainO2Sats>88%/Maybe>94%
ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn
www.thinkasklearn.com.au 29
• ConsiderO2>6l/minasaerosolising• PatientwithNPO2shouldhavesurgicalmask• PatientswithO2>6-8l/minorFiO2>50%havehighfailurerate– Considerintubatingearly
• NormalIntubationprocedureformost• Minimisenumberofpeopleinroom– Outsiderunners
Donotdelayintubation
ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn
www.thinkasklearn.com.au 30
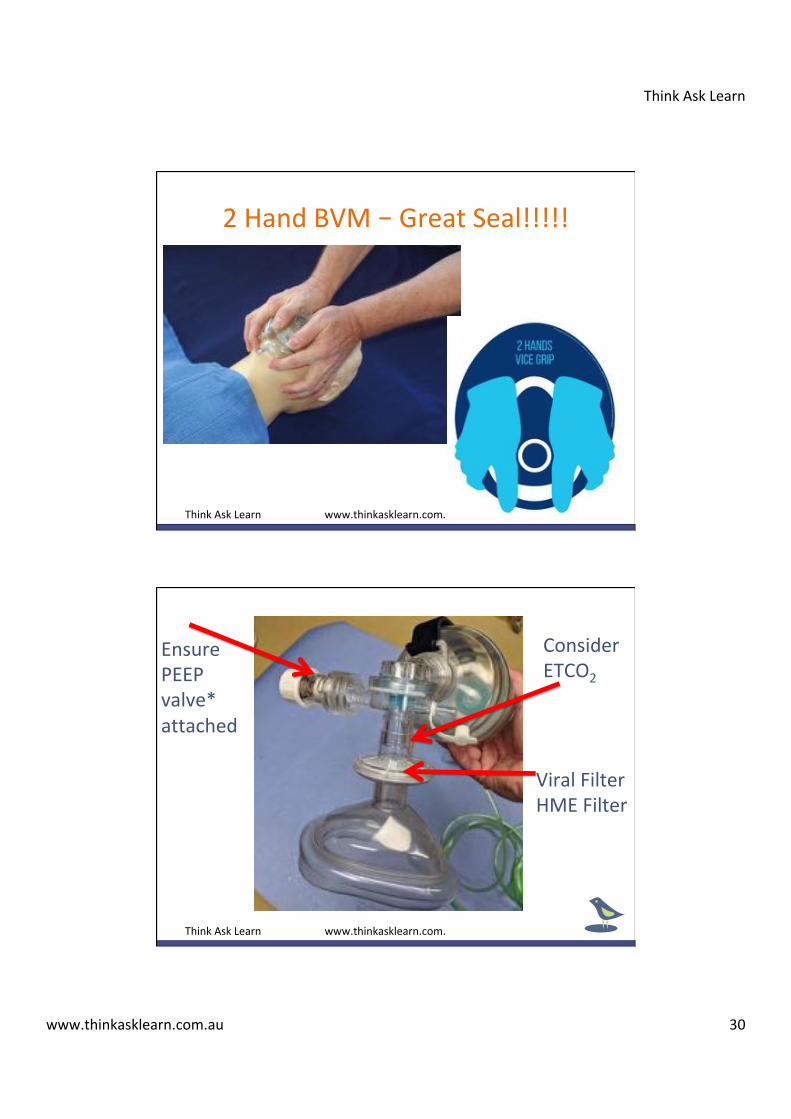
2HandBVM–GreatSeal!!!!!
ThinkAskLearn www.thinkasklearn.com.
EnsurePEEPvalve*attached
ViralFilterHMEFilter
ConsiderETCO2
ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn
www.thinkasklearn.com.au 31
• DonotuseApnoeicDiffusion/NP– AlsonoBIPAP/CPAP,HFNP
• BVMinspontaneousbreathingwithGREATseal– NOSqueezingofBag
• SitPatientupat45degreesforPreOxygenation• Duringapnoeaavoidventilationifpossible– IFdesat,-minimalchestrise,6bpm
• Aimfor5minsofpreoxygenation
IntubationPreoxygenation
• Rapiddosingofdrugs– Notitration
• Generousdosingofdrugs– Roc>1.5mg/kgIBW)ORSux1.5mg/kgTBW– Goodparalysis=NOcough
• Watchthetime– Goodparalysisbutminimisetheapnoeaperiod
RapidSequenceIntubation

ThinkAskLearn
www.thinkasklearn.com.au 32
ThinkAskLearn www.thinkasklearn.com.
VideolaryngoscopeRecommended
ThinkAskLearn
www.thinkasklearn.com.au 33
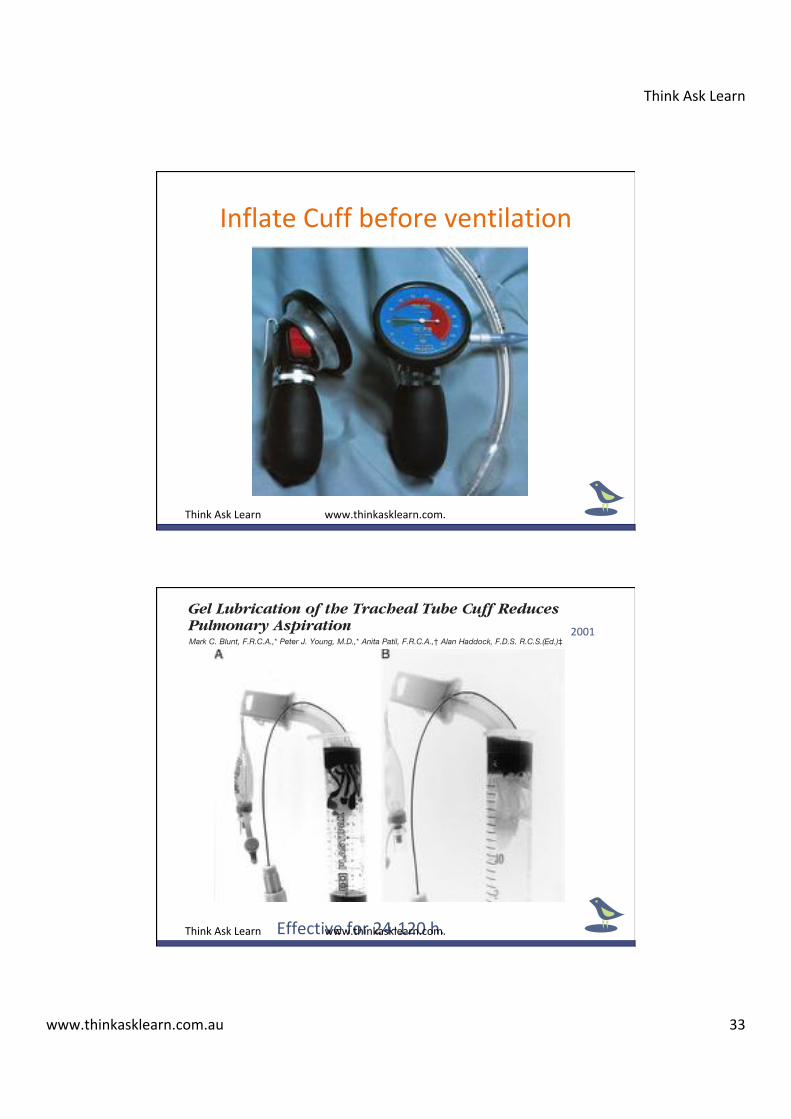
InflateCuffbeforeventilation
ThinkAskLearn www.thinkasklearn.com.
Study Design. This was a prospective open observa-tional study. Nine critically ill patients who required atracheostomy were recruited. All the study patients weregiven an 8-mm-ID Portex Profile cuffed tracheostomytube at percutaneous tracheostomy by the Griggs tech-nique. The cuff was lubricated with KY jelly, inflated to30 cm H2O (2.9 kPa) and maintained at this pressure byintermittent checks before dye instillation and every 8 husing a cuff inflator (SIMS Portex Ltd.). Half a milliliterE122 blue food dye followed by 3 ml saline was instilleddaily through the catheter into the subglottic space. Thenurse responsible for the patient was instructed to re-port dye obtained from tracheal aspirates (performedafter instillation and at least every 4 h thereafter). Tra-cheobronchial aspiration was deemed to have occurredif dye was retrieved from the trachea.
Statistical AnalysisPower Analysis for Anesthetized Patient Study. In
a previous study of intensive care unit patients withPortex Profile cuffs Young et al.3 showed an 87% aspi-ration rate, and in anesthetized patients with nonlubri-cated cuffs Seegobin and Van Hasselt2 showed an aspi-ration rate of 100% of subglottic dye detected bybronchoscopy. We expected that the aspiration rate wewould detect with tracheal aspirates might be approxi-mately 85%. We thought a clinically important reductionwould be a reduction of 50%. With an ! value of 0.05and a " value of 0.2, 18 patients would be required ineach group.
Statistical Analysis. For the benchtop study, a 2 ! 2table was constructed and the data were analyzed usingthe Fisher exact test. For anesthetized patients, a 2 ! 2table was constructed and the data were analyzed usingthe Fisher exact test. For critically ill patients, because
this part of the study was purely observational, no sta-tistical test was applied.
Results
Benchtop StudiesIn the rigid cylinder, the nonlubricated cuff permitted
leakage but the lubricated cuff did not (figs. 2A and B).All five of the nonlubricated cuffs leaked, and none ofthe lubricated cuffs leaked in the pig tracheal model(0 vs. 100%, P " 0.01).
Anesthetized Patient StudyThere were 18 patients in each group. Eleven percent
of the lubricated cuffs leaked, and 83% of the nonlubri-cated cuffs leaked (P " 0.0001).
Critically Ill Patients with TracheostomiesThe lubricated tracheostomy tube cuffs leaked after a
median period of 48 h (range, 24–120 h).
Discussion
The prevention of aspiration in tracheally intubatedanesthetized patients is important to prevent rare, clini-cally apparent aspirations4 and more commonly unrec-ognized aspiration.6 The exact incidence and morbidityof silent or unrecognized aspiration during anesthesia isunknown. Clinically apparent aspiration past adequatelyinflated HVLP endotracheal tube cuffs was reportedas early as 1975.4 Seegobin and Van Hasselt2 studied30 anesthetized patients and bronchoscopically soughtfor leakage of dye from the subglottic space past thenonlubricated cuff to the tracheobronchial tree. Fifteen
Fig. 2. (A) Nonlubricated tracheostomytube high-volume, low-pressure cuff in-flated to 30 cm H2O in a rigid cylinder.Leakage occurs along channels in the cuffwall. (B) Lubricated tracheostomy tubehigh-volume, low-pressure cuff inflatedto 30 cm H2O in a rigid cylinder. Thefigure shows prevention of leakage be-cause channels in the cuff wall areblocked by the gel.
379PREVENTION OF LEAKAGE USING CUFF LUBRICATION
Anesthesiology, V 95, No 2, Aug 2001
Effectivefor24-120h.
Anesthesiology 2001; 95:377–81 © 2001 American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc.
Gel Lubrication of the Tracheal Tube Cuff ReducesPulmonary AspirationMark C. Blunt, F.R.C.A.,* Peter J. Young, M.D.,* Anita Patil, F.R.C.A.,† Alan Haddock, F.D.S. R.C.S.(Ed.)‡
Background: Leakage of fluid occurs along the longitudinalfolds within the wall of an inflated high-volume, low-pressurecuff. Theoretically, lubrication of the cuff with a water-solublegel might prevent aspiration by plugging the channels in thecuff wall. Pulmonary aspiration during anesthesia has beenlinked with postoperative pneumonia and during critical illnesscauses ventilator-associated pneumonia.
Methods: Lubricated cuffs were compared with nonlubricatedcuffs for leakage of dye placed in the subglottic space to thetracheobronchial tree in a benchtop model (n ! 5) and in aprospective double-blinded randomized controlled trial ofanesthetized patients (n ! 36). The duration of the efficacy ofthe lubricant was determined in a prospective open observa-tional study of critically ill patients with tracheostomies (n ! 9).Dye was detected clinically by dye coloration of secretions dur-ing tracheal suctioning.
Results: In the benchtop model the incidence of leakage was0% in the lubrication group and 100% in the nonlubricationgroup (P < 0.01). Dye leakage in anesthetized patients was 11%in the lubrication group and 83% in the nonlubrication group(P < 0.0001). In the critically ill patients with lubricated cuffedtracheostomy tubes, leakage first occurred after a median pe-riod of 48 h (range, 24–120 h).
Conclusions: Cuff lubrication with a water-soluble gel reducespulmonary aspiration in anesthetized patients. In the criticallyill patient with a tracheostomy the protective effect is lost after24–120 h.
REGURGITATION and pulmonary aspiration are infre-quently recognized during anesthesia.1 The exact inci-dence of aspiration during anesthesia is unknown, but itis clear that high-volume, low-pressure (HVLP) endotra-cheal tube cuffs do not reliably prevent subglottic fluidfrom passing to the tracheobronchial tree.2–4 Postoper-ative pneumonia has been linked to microaspiration ofpathogens originating in the gastrointestinal tract.5 Inpediatric intensive care patients with pH probes locatedin the esophagus and the trachea, esophageal reflux wasnoted in 40% and tracheal aspiration in 20%. The tra-cheal aspiration occurred whether the tube was cuffedor uncuffed.6 Leakage of contaminated oropharyngealsecretions occurs past endotracheal tube cuffs in criti-cally ill, mechanically ventilated patients. This is theleading cause of tracheobronchial colonization and ven-
tilator-associated pneumonia.7 This leakage occurs downlongitudinal channels caused by folds in the cuff wallmaterial.2,4 These folds always occur in an HVLP cuffinflated within a trachea because the diameter of the cuffmust be greater than that of the trachea for the intracuffpressure to be equal to the tracheal wall pressure.
Seegobin et al.2 suggested that cuff lubrication with agel may reduce aspiration by filling and effectively dam-ming the channels within the cuff wall. The currentstudy compares lubricated cuffs (using a water-solublegel) with nonlubricated cuffs in a benchtop model inanesthetized patients and in critically ill patients withtracheostomies.
Materials and Methods
Benchtop ModelRigid Cylinder Model. A 2-cm-diameter rigid cylin-
der (20-ml syringe barrel, Plastipak; Becton DickinsonSA, Madrid, Spain) was intubated with lubricated andnonlubricated Portex Profile (SIMS Portex Ltd., Hythe,United Kingdom) tracheostomy tubes (8-mm ID), andthe cuff was inflated to 30 cm H2O. Dye was placedabove the cuff and photographed to demonstrate themechanism of leakage.
Static Pig Trachea Model. Nine-centimeter lengths offive pig tracheas within 24 h of slaughter were chosen tospan the range for the human as calculated from a post-mortem study (1.4–2.7 cm).8 The tracheas were sus-pended vertically and sequentially intubated by one ofthe investigators so that the cuff center was 4 cm belowthe upper tracheal edge. Each trachea received a lubri-cated and a nonlubricated cuffed tracheal tube (8-mmID, Portex Profile) in a random order (closed-envelopetechnique). The cuff pressure was set at 30 cm H2O witha commercial cuff inflator (SIMS Portex Ltd.). This hadpreviously been checked against a mercury column toconfirm accuracy. The observer was blinded as towhether or not the cuff was lubricated. Blue dyed water(3.5 ml) was placed above the cuff. If, after 15 min, dyehad leaked to the trachea, this was recorded as leak; ifnot, this was recorded as no leak.
Tracheal Sizes. The range of mean tracheal diameterswas 1.4–2.5 cm.
Cuff Leakage with Anesthetized PatientsEthical Considerations. After local ethical commit-
tee approval (King’s Lynn and Wisbech National HealthService Trust Ethics Committee, Queen Elizabeth Hospi-tal, King’s Lynn, Norfolk, United Kingdom), informed
* Consultant Anaesthetist, † Anaesthetic Registrar, ‡ Oral Surgeon.
Received from the Department of Anaesthesia, Queen Elizabeth Hospital,Kings Lynn, United Kingdom. Submitted for publication November 6, 2000.Accepted for publication March 1, 2001. Supported by an Oxford and AngliaNational Health Service Research and Development Grant, Oxford, United Kingdom.Presented in part at the State of the Art meeting of the Intensive Care Society,London, United Kingdom, December 9, 1999, and at the meeting of the AmericanSociety of Anesthesiologists, San Francisco, California, October 18, 2000.
Address correspondence to Dr. Blunt: Department of Anaesthesia, QueenElizabeth Hospital, Kings Lynn, PE30 4ET, United Kingdom. Address electronicmail to: [email protected]. Reprints will not be available from the authors.Individual article reprints may be purchased through the Journal Web site,www.anesthesiology.org.
Anesthesiology, V 95, No 2, Aug 2001 377
2001
ThinkAskLearn www.thinkasklearn.com.

ThinkAskLearn
www.thinkasklearn.com.au 34
ThinkAskLearn www.thinkasklearn.com.
• ETCO2immediately• NGTimmediatelyafter• EarlyIDCwithhourlybag• InvasiveTempProbeforall• Arterialline/CVL• DecreaseFi02levelstolowtomaintainsats• Bloodgastoconfirmventilationstatus• DelayCXR– Aftercentrallineinsertion
Postintubationcareaspernormal
ThinkAskLearn
www.thinkasklearn.com.au 35
PostIntubation
VentilatorSettings
ThinkAskLearn
www.thinkasklearn.com.au 36
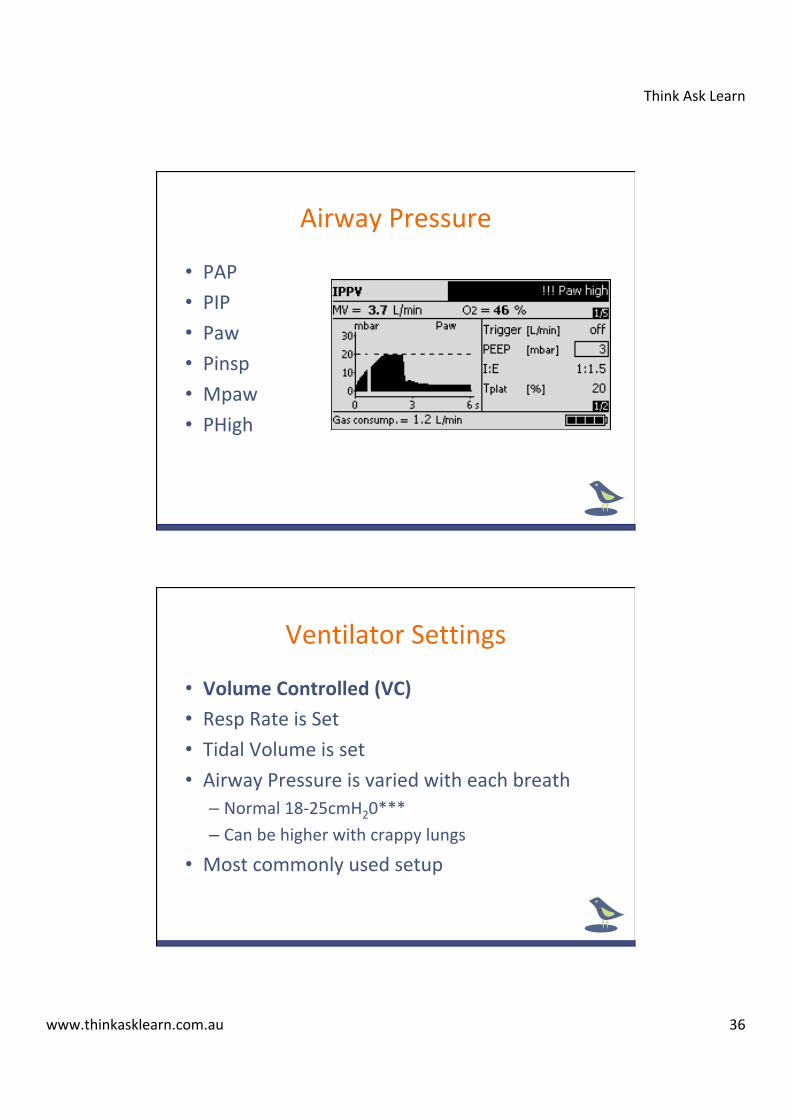
• PAP• PIP• Paw• Pinsp• Mpaw• PHigh
AirwayPressure
• VolumeControlled(VC)• RespRateisSet• TidalVolumeisset• AirwayPressureisvariedwitheachbreath– Normal18-25cmH20***– Canbehigherwithcrappylungs
• Mostcommonlyusedsetup
VentilatorSettings
ThinkAskLearn
www.thinkasklearn.com.au 37
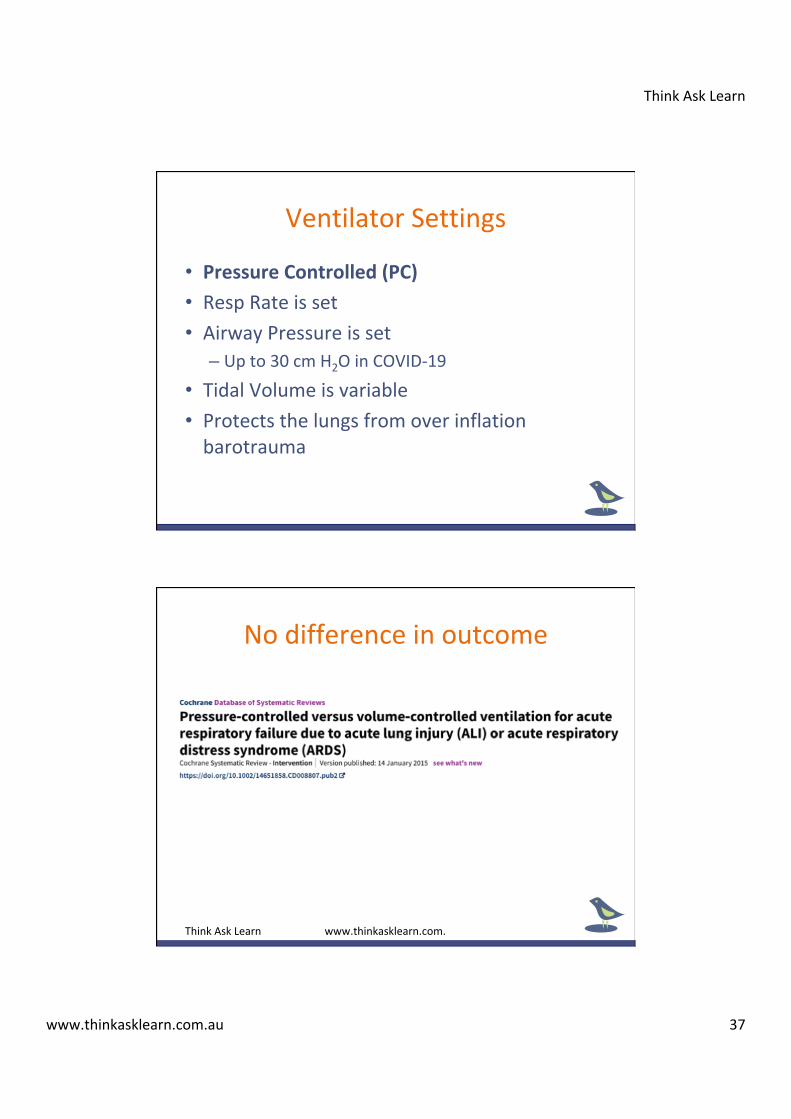
• PressureControlled(PC)• RespRateisset• AirwayPressureisset– Upto30cmH2OinCOVID-19
• TidalVolumeisvariable• Protectsthelungsfromoverinflationbarotrauma
VentilatorSettings
Nodifferenceinoutcome
ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn
www.thinkasklearn.com.au 38
ModesofVentilation
CMVvsSIMV
ThinkAskLearn www.thinkasklearn.com.
ContinuousMechanicalVentilation
• CMV• Thepatientreceivesapresetnumberofbreathsperminuteofapredeterminedvolume
• Patientisabletobreathforthemselvesthroughtriggerssettings

ThinkAskLearn
www.thinkasklearn.com.au 39
SynchronisedIntermittentMandatoryVentilationSIMV
• Ptreceivesapresetnumberofbreaths• Theptmayalsoinitiatespontaneousbreaths• Mayusepressuresupport(highorlowlevels)ifWOBnoteffective
• Triggersensitivitycanbevaried• Goodforlongterm,lightlysedatedorthepatientthatneedstobeweaned.
• Avoidcoughing,fightingtheventilator• “Deepsedationmayberequiredtocontrolrespiratorydriveandachievetidalvolumetargets”WHO2020
• Paralysismayberequiredifworseninghypoxia• Intubate–Paralysis–Paralysis1-2hrsthenreviewwithICU
DeepSedation

ThinkAskLearn
www.thinkasklearn.com.au 40
SIMVThinkAskLearn www.thinkasklearn.com.
WHOrecommends
ThinkAskLearn
www.thinkasklearn.com.au 41
• 6-8mlkg(7ml/kg)ratherthan10mls/kg
– COVIDPtrecommendstartingat6mls/kgWHO2020
• Lessdamage
• Noincreaseuseofsedationorvasopressors
• NothigherPEEPorFiO2
• LesslikelytodevelopARDSfromthestart
LowTidalVolumes
ThinkAskLearn
www.thinkasklearn.com.au 42
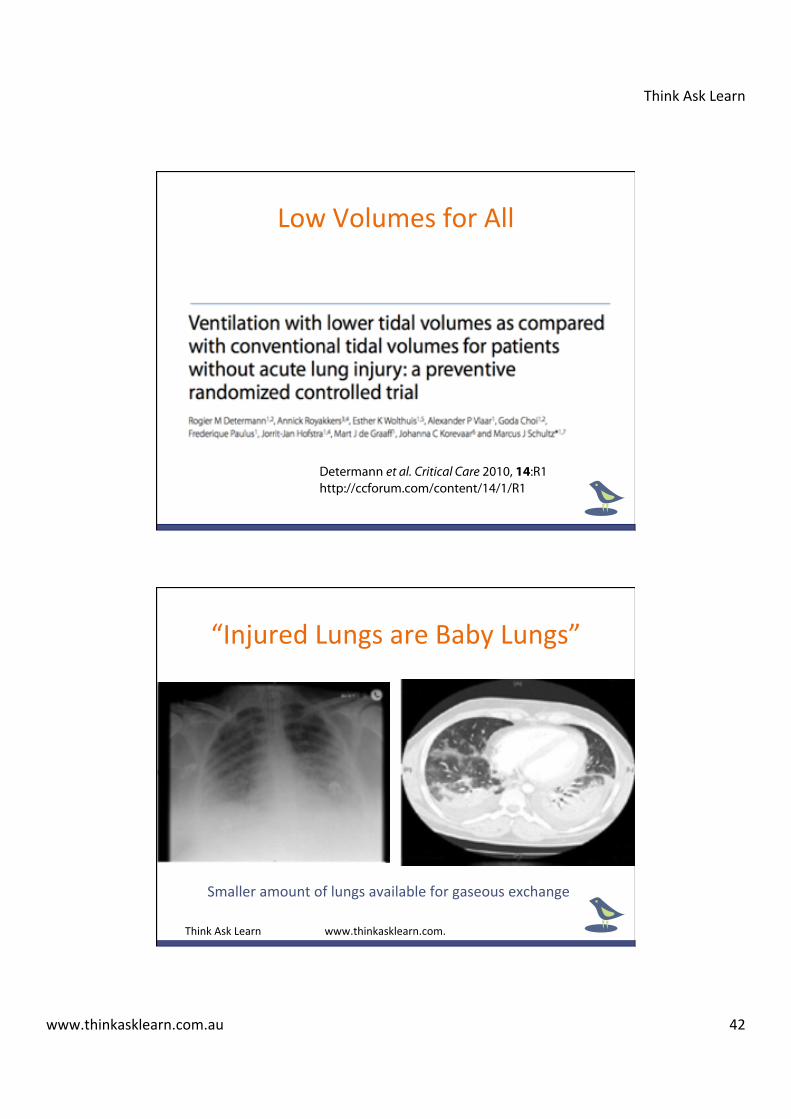
LowVolumesforAll
Determann et al. Critical Care 2010, 14:R1http://ccforum.com/content/14/1/R1
Page 2 of 14
lator-associated lung injury in patients with acute lunginjury (ALI) or its more-severe form, acute respiratorydistress syndrome (ARDS), by showing reduced morbid-ity and mortality in the lower tidal-volume arm [3-6]. Asa result of these studies, current guidelines now clearlysupport the use of lower tidal volume in patients withALI/ARDS [7]. In contrast, little evidence supports theuse of lower tidal volume in critically ill patients withoutALI/ARDS, partly because of a lack of randomized con-trolled trial evidence on the best ventilator strategies inthese patients [8].
Pneumonia, aspiration, sepsis, trauma, shock, and mul-tiple blood transfusions are well-described risk factors forALI/ARDS [9]. Animal studies demonstrate that mechan-ical ventilation with conventional tidal volume not onlymay aggravate, but also may initiate lung injury [1,2]. Therole of tidal-volume size as a contributor to the develop-ment of lung injury in humans is, however, less clear. Onestudy on reduced tidal volume and pressure settings didnot show a reduction in mortality but suggested moreside effects of lower tidal-volume ventilation in patientsat high risk for ALI/ARDS [10]. Conversely, pulmonaryprocoagulant changes and increased systemic cytokineproduction were observed in patients without preexistinglung injury receiving conventional-tidal-volume mechan-ical ventilation during surgery [11,12].
Other studies have challenged these findings [13,14].Results from cohort studies suggest that mechanical ven-tilation with conventional tidal volumes may cause orcontribute to development of lung injury in critically illpatients who did not have ALI/ARDS at the onset ofmechanical ventilation [15,16]. The inconclusive resultsfrom the studies in surgical patients may arise from thefact that these patients were ventilated for only a shortperiod, whereas the patients of the larger cohort studieswere critically ill patients who had been ventilated for alonger period.
As ALI/ARDS is characterized by a profound produc-tion of inflammatory mediators, it might be expected thatif conventional tidal volumes contribute to developmentof lung injury, the injury also may be associated withincreased production of cytokines. We therefore con-ducted a trial to determine whether mechanical ventila-tion with conventional or lower tidal volume would beassociated with different cytokine patterns in the lungsand the plasma of critically ill patients without ALI atonset of mechanical ventilation. Secondary end pointswere development of lung injury, duration of mechanicalventilation, and mortality.
Materials and methods
ParticipantsFrom January 2005 until December 2007 patients wererecruited in the intensive care departments of one aca-demic and one regional teaching hospital in the Nether-lands. The academic ICU is a 28-bed "closed format"department where medical/surgical patients (includingneurosurgery/neurology, cardiothoracic surgery, and car-diology patients) were under the direct care of the ICUteam. The ICU team comprised 10 full-time ICU physi-cians, eight subspecialty fellows, 12 residents, and occa-sionally one intern. The regional teaching ICU is an eight-bed "open format" department with medical/surgicalpatients (not including neurosurgery and cardiothoracicsurgery patients). The ICU team comprised three full-time ICU physicians, five physicians who participate inevening and night shifts, and one resident. The two ICUshad similar standards of practice in terms of mechanical-ventilation and sedation protocols.
Patients were eligible for the study if they did not meetthe consensus criteria for ALI/ARDS [17] and neededmechanical ventilation for an anticipated duration ofmore than 72 hours. Patients had to be randomized lessthan 36 hours after the onset of mechanical ventilation.Exclusion criteria were age younger than 18 years, partic-ipation in other clinical trials, pregnancy, increaseduncontrollable intracranial pressure, chronic obstructivepulmonary disease (defined as a forced expiratory volumein 1 second to a forced vital capacity ratio less than 0.64and daily medication), restrictive pulmonary disease (evi-dence of chronic interstitial infiltration on chest radio-graph), use of immunosuppressive agents (100 mghydrocortisone per day was allowed), pulmonary throm-boembolism, previous pneumectomy or lobectomy, andprevious randomization in this study. Randomization wasperformed by using sealed opaque envelopes in blocks of50 patients. Each study center had its own randomizationblock. The protocol was approved by the medical ethicscommittees of both hospitals, and written informed con-sent was obtained from the patient or closest relativesbefore entry in the study. All procedures were done incompliance with the Helsinki declaration.
InterventionsThe volume-controlled mode was used for mechanicalventilation. To calculate tidal volume, predicted bodyweight was used, as described [3]. The target tidal volumein the conventional group was 10 ml/kg of predicted bodyweight, which was routine practice at the time of the con-duct of the study. Patients from the intervention groupwere ventilated at tidal volumes of 6 ml/kg of predictedbody weight. In case patients were randomized to 6 ml/kg, the attending physician was allowed to increase tidal-
“InjuredLungsareBabyLungs”
Smalleramountoflungsavailableforgaseousexchange
ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn
www.thinkasklearn.com.au 43
Vt=Protection
VentilatorRelatedPneumothorax
• Plateaupressure–Alveoliaresafefrombarotrauma• Peakpressuremeansnothing
ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn
www.thinkasklearn.com.au 44
• Plateaupressurekeepat30cmH20
• Measureevery20minsorso
• Over30cmH20alveoliatrisk
• Atrisk-Notprotected–TurnDownTidalVolume
– TalktoICU,mayrecommenddroppingto4/5mls/kg
PlateauPressure
Vt=Protection
ThinkAskLearn
www.thinkasklearn.com.au 45
60ml/kg/minIntubation
120ml/kg/minDeadSpace
70kg x 120ml = 8400ml/min 8400/500ml(7ml/kg) = 17 bpm
Adjust from Blood Gas
RespiratoryRate
RR=Ventilation
ThinkAskLearn
www.thinkasklearn.com.au 46
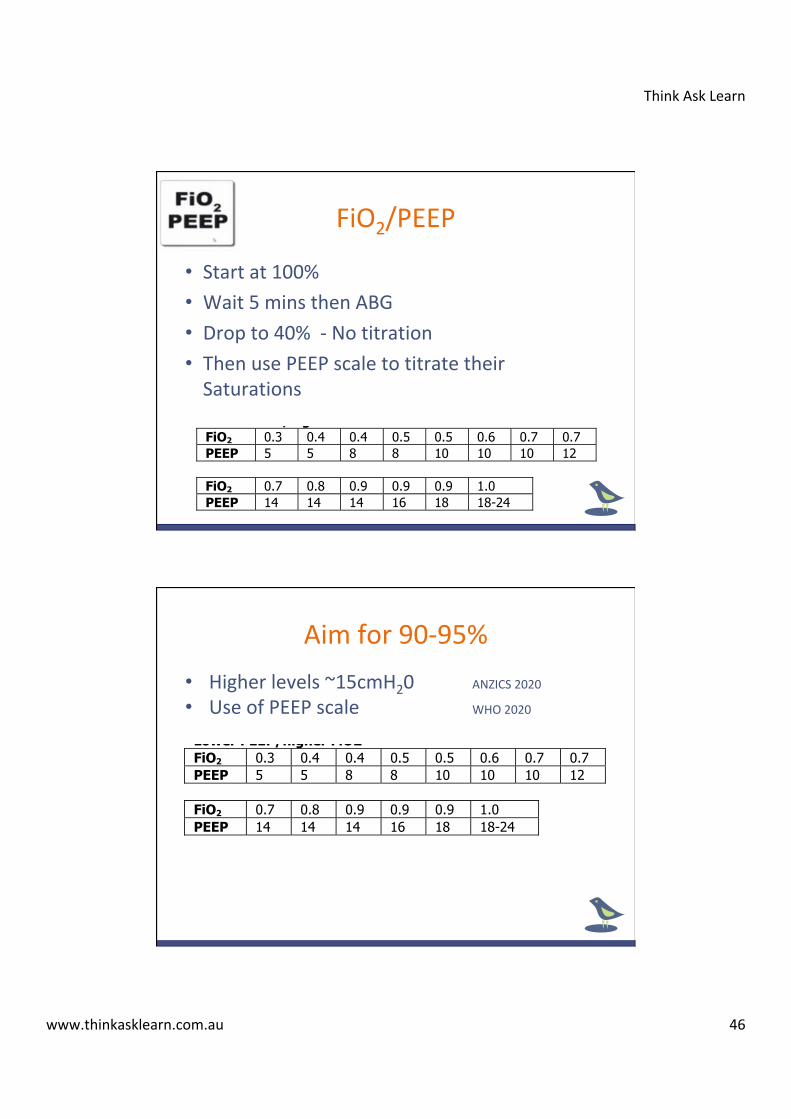
• Startat100%• Wait5minsthenABG• Dropto40%-Notitration• ThenusePEEPscaletotitratetheirSaturations
FiO2/PEEP
INCLUSION CRITERIA: Acute onset of 1. PaO2/FiO2 d 300 (corrected for altitude) 2. Bilateral (patchy, diffuse, or homogeneous) infiltrates consistent with
pulmonary edema 3. No clinical evidence of left atrial hypertension PART I: VENTILATOR SETUP AND ADJUSTMENT 1. Calculate predicted body weight (PBW)
Males = 50 + 2.3 [height (inches) - 60] Females = 45.5 + 2.3 [height (inches) -60]
2. Select any ventilator mode 3. Set ventilator settings to achieve initial VT = 8 ml/kg PBW 4. Reduce VT by 1 ml/kg at intervals d 2 hours until VT = 6ml/kg PBW. 5. Set initial rate to approximate baseline minute ventilation (not > 35
bpm). 6. Adjust VT and RR to achieve pH and plateau pressure goals below.
AARRDDSSnnee tt OXYGENATION GOAL: PaO2 55-80 mmHg or SpO2 88-95% Use a minimum PEEP of 5 cm H2O. Consider use of incremental FiO2/PEEP combinations such as shown below (not required) to achieve goal. Lower PEEP/higher FiO2
FiO2 0.3 0.4 0.4 0.5 0.5 0.6 0.7 0.7 PEEP 5 5 8 8 10 10 10 12
NIH NHLBI ARDS Clinical Network FiO2 0.7 0.8 0.9 0.9 0.9 1.0 PEEP 14 14 14 16 18 18-24 Mechanical Ventilation Protocol Summary Higher PEEP/lower FiO2 FiO2 0.3 0.3 0.3 0.3 0.3 0.4 0.4 0.5 PEEP 5 8 10 12 14 14 16 16 FiO2 0.5 0.5-0.8 0.8 0.9 1.0 1.0 PEEP 18 20 22 22 22 24 __________________________________________________________ PLATEAU PRESSURE GOAL: d 30 cm H2O Check Pplat (0.5 second inspiratory pause), at least q 4h and after each change in PEEP or VT. If Pplat > 30 cm H2O: decrease VT by 1ml/kg steps (minimum = 4 ml/kg). If Pplat < 25 cm H2O and VT< 6 ml/kg, increase VT by 1 ml/kg until Pplat > 25 cm H2O or VT = 6 ml/kg. If Pplat < 30 and breath stacking or dys-synchrony occurs: may increase VT in 1ml/kg increments to 7 or 8 ml/kg if Pplat remains < 30 cm H2O.
Aimfor90-95% INCLUSION CRITERIA: Acute onset of 1. PaO2/FiO2 d 300 (corrected for altitude) 2. Bilateral (patchy, diffuse, or homogeneous) infiltrates consistent with
pulmonary edema 3. No clinical evidence of left atrial hypertension PART I: VENTILATOR SETUP AND ADJUSTMENT 1. Calculate predicted body weight (PBW)
Males = 50 + 2.3 [height (inches) - 60] Females = 45.5 + 2.3 [height (inches) -60]
2. Select any ventilator mode 3. Set ventilator settings to achieve initial VT = 8 ml/kg PBW 4. Reduce VT by 1 ml/kg at intervals d 2 hours until VT = 6ml/kg PBW. 5. Set initial rate to approximate baseline minute ventilation (not > 35
bpm). 6. Adjust VT and RR to achieve pH and plateau pressure goals below.
AARRDDSSnnee tt OXYGENATION GOAL: PaO2 55-80 mmHg or SpO2 88-95% Use a minimum PEEP of 5 cm H2O. Consider use of incremental FiO2/PEEP combinations such as shown below (not required) to achieve goal. Lower PEEP/higher FiO2
FiO2 0.3 0.4 0.4 0.5 0.5 0.6 0.7 0.7 PEEP 5 5 8 8 10 10 10 12
NIH NHLBI ARDS Clinical Network FiO2 0.7 0.8 0.9 0.9 0.9 1.0 PEEP 14 14 14 16 18 18-24 Mechanical Ventilation Protocol Summary Higher PEEP/lower FiO2 FiO2 0.3 0.3 0.3 0.3 0.3 0.4 0.4 0.5 PEEP 5 8 10 12 14 14 16 16 FiO2 0.5 0.5-0.8 0.8 0.9 1.0 1.0 PEEP 18 20 22 22 22 24 __________________________________________________________ PLATEAU PRESSURE GOAL: d 30 cm H2O Check Pplat (0.5 second inspiratory pause), at least q 4h and after each change in PEEP or VT. If Pplat > 30 cm H2O: decrease VT by 1ml/kg steps (minimum = 4 ml/kg). If Pplat < 25 cm H2O and VT< 6 ml/kg, increase VT by 1 ml/kg until Pplat > 25 cm H2O or VT = 6 ml/kg. If Pplat < 30 and breath stacking or dys-synchrony occurs: may increase VT in 1ml/kg increments to 7 or 8 ml/kg if Pplat remains < 30 cm H2O.
• Higherlevels~15cmH20 ANZICS2020• UseofPEEPscale WHO2020
ThinkAskLearn
www.thinkasklearn.com.au 47
PEEP/FiO2=Oxygenation
ThinkAskLearn
www.thinkasklearn.com.au 48
• GiveempiricantibioticstotreatsuspectedCAP/sepsis/secondarypneumonia– preferwithin1hour/?
• Giverestrictivefluidmanagement– Maintenanceonly– Earlyadoptionofinotropicsupport–CENSER2019
• Steroids/Antiviralsnotrecommend• Enrollintotrial!
Othertreatment
ThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn
www.thinkasklearn.com.au 49
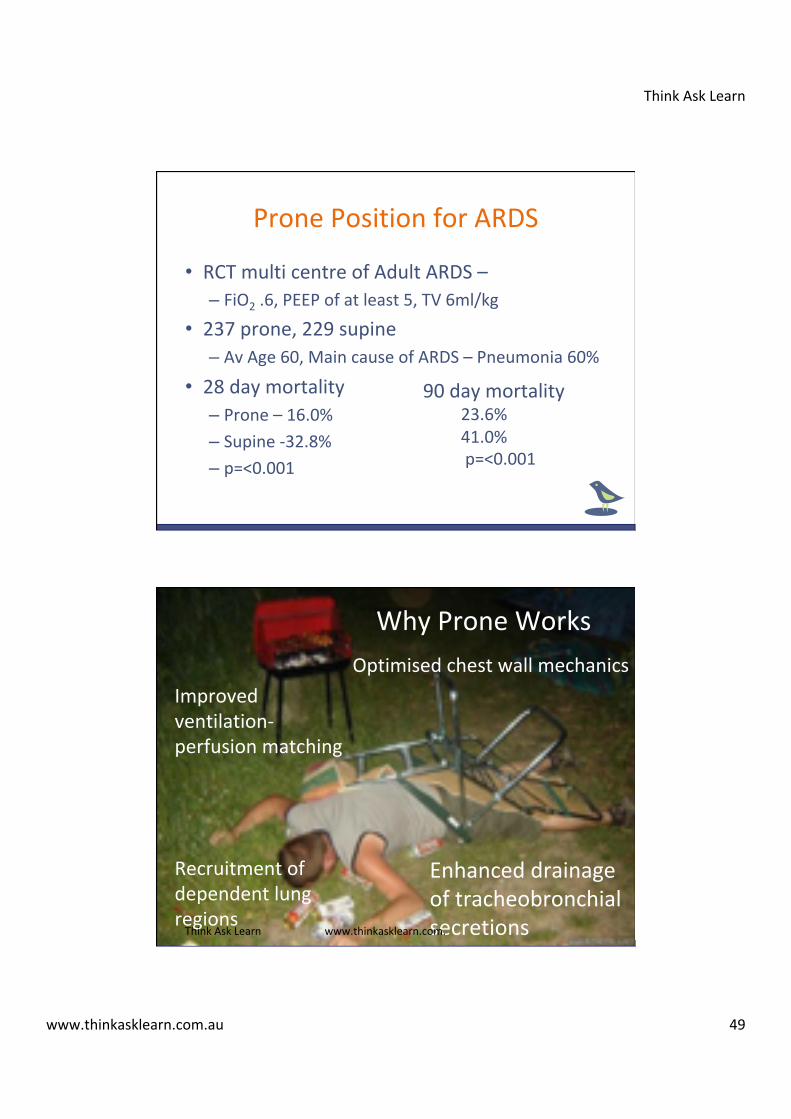
PronePositionforARDS
• RCTmulticentreofAdultARDS–– FiO2.6,PEEPofatleast5,TV6ml/kg
• 237prone,229supine– AvAge60,MaincauseofARDS–Pneumonia60%
• 28daymortality – Prone–16.0% – Supine-32.8% – p=<0.001
90daymortality23.6%41.0%p=<0.001
WhyProneWorks
Improvedventilation-perfusionmatching
Recruitmentofdependentlungregions
Optimisedchestwallmechanics
EnhanceddrainageoftracheobronchialsecretionsThinkAskLearn www.thinkasklearn.com.
ThinkAskLearn
www.thinkasklearn.com.au 50
NEJM–YouTubepronepositionventilation
ThinkAskLearn www.thinkasklearn.com.
ProneintheED?
Proneventilationfor12–16hoursperdayisrecommended. WHO2020
ThinkAskLearn www.thinkasklearn.com.

ThinkAskLearn
www.thinkasklearn.com.au 51
ThinkAskLearn www.thinkasklearn.com.
• UsePPEwisely,getabuddysystem• Intubateaspernormal,somechanges– NoBIPAP,HFNO,ApnoeicDiffusion
• VentilateforARDS– Lowvolume,HighPEEP,
• ProneVentilationworks• FluidRestrict
TakeHomeMessage
Reference List for COVID-19 Webinar
Real time data of COVID-19
Data on World Case of COVID-19 https://www.worldometers.info/coronavirus//
Date on Australian COVID-19 cases - https://www.covid19data.com.au/
Australian Government Response
Australian Government COVID-19 Response
https://www.health.gov.au/news/health-alerts/novel-coronavirus-2019-ncov-health-alert/
coronavirus-covid-19-advice-for-the-health-and-aged-care-sector
Australian Government Interim PPE Guidelines
https://www.health.gov.au/news/health-alerts/novel-coronavirus-2019-ncov-health-alert/
coronavirus-covid-19-advice-for-the-health-and-aged-care-sector#using-personal-protective-
equipment-ppe
Guidelines of Management
World Health Organisation (2020) Clinical management of severe acute respiratory infection when
COVID-19 is suspected https://www.who.int/publications-detail/clinical-management-of-severe-
acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected
Brewster, D. J., Chrimes, N. C., Do, T. B., Fraser, K., Groombridge, C. J., Higgs, A., ... & Nickson,
C. P. (2020). Consensus statement: Safe Airway Society principles of airway management and
tracheal intubation specific to the COVID-19 adult patient group. The Medical Journal of
Australia, 212(10), 1.https://www.mja.com.au/journal/2020/consensus-statement-safe-airway-
society-principles-airway-management-and-tracheal
www.thinkasklearn.com.au [email protected]
The Australian and New Zealand Intensive Care Society (ANZICS) COVID-19 Guidelines https://
www.anzics.com.au/wp-content/uploads/2020/03/ANZICS-COVID-19-Guidelines-Version-1.pdf
Anaesthesia and caring for patients during the COVID-19 outbreak ASA (2020). https://
www.asa.org.au/wordpress/wp-content/uploads/News/eNews/covid-19/
ASA_airway_management.pdf
UK/Italy Data from ICU
Intensive Care National Audit & Research Centre (UK) ICU COVID-19 data
https://www.icnarc.org/About/Latest-News/2020/03/27/Report-On-775-Patients-Critically-Ill-
With-Covid-19
Characteristics of COVID-19 patients dying in Italy Report based on available data on March 20th,
2020 Italian ICU data https://www.epicentro.iss.it/coronavirus/bollettino/Report-
COVID-2019_20_marzo_eng.pdf
Some evidence mentioned in Webinar
COCHRANE Review of Evidence in critical care - Overview of topics in critical care - Not COVID
evidence https://www.cochranelibrary.com/collections/doi/SC000039/full
Cochrane review of evidence Pressure Controlled vs Volume Controlled Ventilation https://
www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD008807.pub2/full
ARDS NET Protocol of ventilation http://www.ardsnet.org/tools.shtml
Guérin, C., Reignier, J., Richard, J. C., Beuret, P., Gacouin, A., Boulain, T., ... & Clavel, M. (2013).
Prone positioning in severe acute respiratory distress syndrome. New England Journal of
Medicine, 368(23), 2159-2168 https://www.nejm.org/doi/full/10.1056/NEJMoa1214103
www.thinkasklearn.com.au [email protected]
Video of Proning
NEJM Video -Youtube - https://www.youtube.com/watch?v=E_6jT9R7WJs&t=4s
Multiple Patients on One Ventilator
Joint Statement on Multiple Patients Per Ventilator
https://www.sccm.org/Disaster/Joint-Statement-on-Multiple-Patients-Per-Ventilato
Farkas, J, (2020). Splitting ventilators to provide titrated support to a large group of patients.
PulmCrit(EMCrit) https://emcrit.org/pulmcrit/split-ventilators/
Farkas, J, (2020). Why the SCCM/AARC/ASA/APSF/AACN/CHEST joint statement on split
ventilators is wrong. PulmCrit(EMCrit) https://emcrit.org/pulmcrit/pulmcrit-wee-why-the-sccm-
aarc-asa-apsf-aacn-chest-joint-statement-on-split-ventilators-is-wrong/
Iwashyna, J. (2020). Should we put multiple COVID-19 patients on a single ventilator? Life in the
Fast Lane https://litfl.com/should-we-put-multiple-covid-19-patients-on-a-single-ventilator/
Columbia University College of Physicians & Surgeons New York-Presbyterian Hospital (2020).
Ventilator Sharing Protocol: Dual-Patient Ventilation with a Single Mechanical Ventilator for Use
during Critical Ventilator Shortages https://www.gnyha.org/wp-content/uploads/2020/03/
Ventilator-Sharing-Protocol-Dual-Patient-Ventilation-with-a-Single-Mechanical-Ventilator-for-Use-
during-Critical-Ventilator-Shortages.pdf
www.thinkasklearn.com.au [email protected]