caries vaccine
TRANSCRIPT

Dr Divya GaurDept of Pedodontics and Preventive Dentistry
CARIES VACCINE

• INTRODUCTION• ACQUISITION OF STREPTOCOCCUS MUTANS• BIOFILM• ROLE OF DENTAL PLAQUE• IMMUNOLOGY OF DENTAL CARIES IN HUMANS• TYPES OF IMMUNE RESPONSE• NEED FOR CARIES VACCINE• REQUIREMENTS OF DENTAL VACCINE• MOLECULAR PATHOGENESIS OF DENTAL CARIES• MOLECULAR TARGETS
• GLUCOSYLTRANFERASE• GLUCAN BINDING PROTEINS• ADHESINS

MECHANISM OF ACTION OF VACCINES TYPES OF VACCINES ROUTES OF IMMUNIZATION
LOCAL SYSTEMIC PASSIVE
ADJUVANTS AND DELIVERY SYSTEMS CLINICAL RESEARCH RISKS OF USING CARIES VACCINE PUBLIC HEALTH VIEW RECENT ADVANCES CONCLUSION

INTRODUCTION Dental caries is an infectious microbiologic disease of the
teeth that results in localized dissolution and destruction of the calcified tissue1.
Clifford MS. The art and science of Operative dentistry. 4th ed. MosbyPublications; 1995.
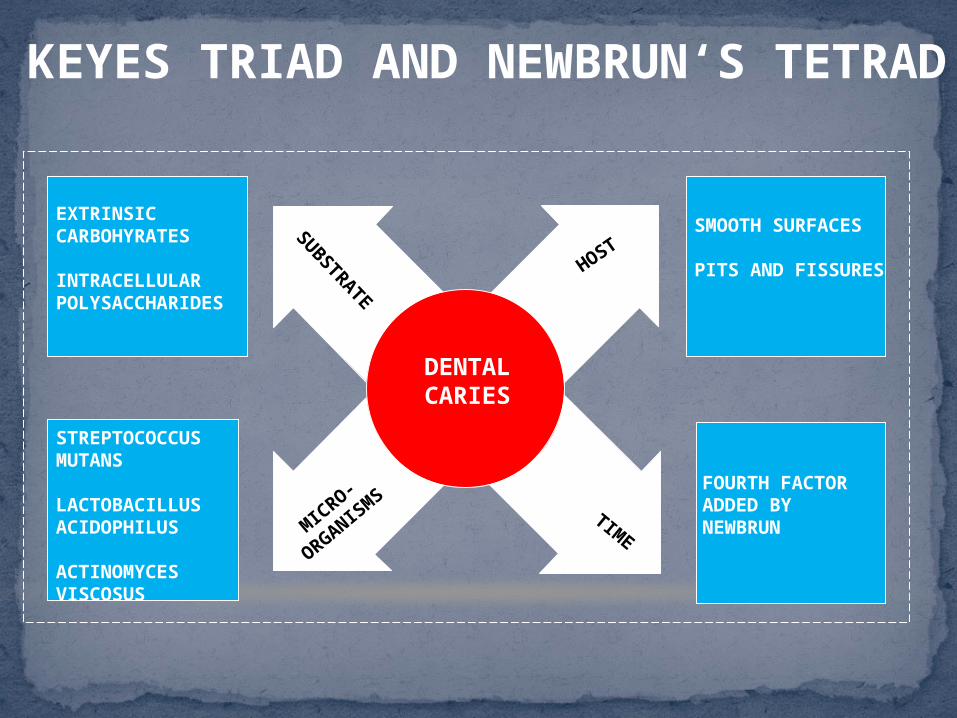
DENTAL CARIES
SUBSTRAT
E HOST
TIMEMICRO-
ORGANISMS
STREPTOCOCCUS MUTANS
LACTOBACILLUS ACIDOPHILUS
ACTINOMYCES VISCOSUS
EXTRINSIC CARBOHYRATES
INTRACELLULAR POLYSACCHARIDES
FOURTH FACTOR ADDED BY NEWBRUN
SMOOTH SURFACES
PITS AND FISSURES
KEYES TRIAD AND NEWBRUN‘S TETRAD

MANAGEMENT OF DENTAL CARIES: EVOLUTION
• ‘DRILL AND FILL’• EXTENSION FOR PREVENTION
CONVENTIONAL APPROACH

STREPTOCOCCUS MUTANS
•WHAT IS IT?• A gram + facultative anaerobe
characterized by 8 serotypes.
•PREVALENCE:• Most prevalent serotype: h
•HOW DOES IT CAUSE DENTAL CARIES?• BIOFILM formation• Aciduric and acidogenic.
S. mutansS.Sobrinus
S.RattiS.CricetiS.DowneiS.Ferus
S.macacae

ACQUISITION OF STREPTOCOCCUS MUTANS
CAUFIELD et al , « window of infectivity « : children become permanently colonized with mutans streptococci between the middle of second year and the end of the third year.
This window may open even earlier if maternal S. mutans infection levels are high, coupled with frequent exposures to dietary sucrose.
DNA probe technology have suggested that low levels of mutans streptococci may be found in the oral cavity during the first year of life.
Thus, data suggests that ‘window of vaccine opportunity’ could exist between 12 and 18 months for most populations.

BIOFILM
A COMMUNITY OF BACTERIA ATTACHED TO SALIVARY
COMPONENTS AND EMBEDDED IN A MATRIX OF GLUCAN OF
HIGH MOLECULAR WEIGHT, PRODUCED BY STRETOCOCCUS
MUTANS.

ROLE OF DENTAL PLAQUE Suggested by Williams in 1897.
GV BLACK (1899): ‘the gelatinous plaque of caries fungus is a thin, transparent film that
usually escapes observation and which is revealed only by careful search. It is not a thick mass of material alba frequently found upon the teeth, nor it is the whitish gummy material.’
Consists of salivary components (acquired pellicle- glycoproteins), desquamated epithelial cells and micro-organisms.
Blayney (1942) Acidogenic streptococci: 86% of plaque Lactobacilli: 57%

ORAL CAVITY DEFENSE CAN BE OF 2 TYPES:
NON- SPECIFIC: Lysozyme, lactoperoxidase and lactoferrin: active against many
species of bacteria.
SPECIFIC: Involves exposing the host to killed or attenuated forms of
organism to instruct the host’s immunological memory.
IMMUNOLOGY OF CARIES IN HUMANS

ANTIGEN – Any substance which stimulates production of antibody with which it reacts specifically and in an observable manner.
ANTIBODY – Substance which appears in serum/tissue fluids which react with the antigen specifically and in an observable manner.
IMMUNITY: It is defined as resistance offered by the host to the harmful pathogenic microbial infection.
ANTIGEN AND ANTIBODY
Specific Non-Specific Active Passive
Natural Artificial Natural Artificial
Innate Acquired

SECRETORY SALIVARY ANTIBODIES : IgA
SERUM ANTIBODIES : IgG, IgM AND IgA
ANTIBODIES IN THE MOUTH

THE PRIMARY RESPONSE: When an antigen is administered for the first time to an animal/ human.
Latent period of induction : 3-10 days.
Antibodies appear in the blood.
First antibody to be elicited: IgM type.
Antibody titre rises steadily during the next 2-3 days, reaches a peak level, and then declines almost as fast as it develops.
if antigenic stimulus was sufficient, IgG appears in a few days.
IgG reaches peak in 7-10 days and then gradually falls over a period of weeks or months.
TYPES OF IMMUNE RESPONSE
IMPORTANT OUTCOME OF PRIMARY RESPONSE: B and T lymphocytes produce “memory cells” or “ primed cells” that are responsible for immunological memory established after immunization.

THE SECONDARY (BOOSTER) RESPONSE: Also involves production of IgM and IgG antibodies .
Brief production of IgM and much larger and prolonged production of IgG antibody.
This accelerated response is attributed to immunological memory.
TYPES OF IMMUNE RESPONSE
Park K. Text book of preventive and social medicine. 17th ed. Bhanotidas Publication; 2004.Warren L, Ernest J. Medical microbiology and immunology. 6th ed. Lange Medical Publishing Division; 2000.

Immunobiological substance designed to produce specific protection against given disease.
It is a suspension of attenuated or killed microorganisms, administered for the prevention or treatment of infectious diseases.
They may be prepared from live modified organisms, inactivated or killed organisms, cellular fractions, toxoids or combinations of these.
DENTAL CARIES VACCINE: The evidence of a specific bacterial cause of dental caries and the function of salivary glands as an effector site of the mucosal immune system has provided a scientific basis for developing a vaccine against this highly prevalent oral disease.
VACCINE

EDWARD JENNER: pioneered in the field of immunology.
LOUIS PASTEUR: developed vaccines against rabies and
anthrax.
1930: Caries immunizaition experiments were performed on
lactobacillus.
1960: Streptococcus mutans became the target .
HISTORY OF VACCINES

Streptococcus mutans is a poor immunogen.
Entry of S.mutans through junctional epithelium of gingiva not sufficient to elicit an immune response.
T-cell response to S.mutans is of low order and needs boosting for sensitization.
NEED FOR CARIES VACCINE

REQUIREMENTS OF A DENTAL CARIES VACCINE
IDENTIFY THE TARGET.
IDENTIFY THE COMPONENT OF IMMUNE SYSTEM THAT SHOULD BE STIMULATED/ INDUCED.
SHOULD NOT HARM THE HOST

MOLECULAR PATHOGENESIS OF DENTAL CARIES
ACQUIRED PELLICLE FORMS ON THE TOOTH SURFACE
INTERACTION OF BACTERIAL PROTEINS (STREPTOCOCCAL ADHESINS) WITH DENTAL PELLICLE.
FURTHER ACCUMULATION OF ACIDOGENIC STREPTOCOCCI
ANTIGEN I/II or Pac
GLUCOSYLTRANSFERASES
GTF-B AND GTF-C
GTF provide scaffolding for aggregation of mutans and other oral streptococci through interaction with bacterial call- associated glucan binding proteins.

GLUCAN


MOLECULAR TARGETS

GLUCOSYLTRANSFERASE
Moro I, Lehner T. Symposium report: Sixth International congress of mucosal immunology; Dental caries vaccine. J Dent Res July 23rd 1990. p. 1863-4. Russell RR. The application of molecular genetics to the microbiology of dental caries. Caries Res 1994;28:69-82.

Function of Glucans: provide scaffolding for the aggregation of mutans and other oral streptoccocci through interaction with bacterial cell- associated glucan binding proteins.
Also, Glucans modify the porosity of the dental biofilm, thus increasing the availability of nutrients for continued bacterial metabolism.
GLUCOSYLTRANSFERASE
Moro I, Lehner T. Symposium report: Sixth International congress of mucosal immunology; Dental caries vaccine. J Dent Res July 23rd 1990. p. 1863-4. Russell RR. The application of molecular genetics to the microbiology of dental caries. Caries Res 1994;28:69-82.
Three forms of GTF: Water insoluble glucan synthesizing enzyme: GTF-I Water insoluble and water- soluble glucan synthesizing
enzymes: GTF-S-I Water- soluble glucan synthesizing enzymes: GTF-S

3 distinct proteins with glucan binding activity: GBP-A, GBP-B and GBP-C.
Only GBP-B has been shown to induce a protective immune response to experimental dental caries.
GLUCAN BINDING PROTEINS

First described by Russell and Lehner. Bind acidic, mucin like glycoproteins found in saliva. 2 principal human pathogens:
Antigens I/ II, Pac or P1 Streptococcus sobrinus: Spa-A or Pag.
Antigens I/II : found in the culture supernatant as well as in S. mutans cell surface. Contains alanine-rich tandem- repeating region in the N-terminal third
and a proline rich repeat region in the centre of the molecule. Antibody directed to the intact Ag I/II molecule or to its salivary
binding domain blocked adherence of S. mutans of saliva-coated hydroxyapatite.
CELL WALL ANTIGENS/ ADHESINS
Smith DJ. Dental caries vaccines: Prospects and concerns. Crit Rev Oral Biol Med 2002;13:335-49.

SALIVARY IMMUNOGLOBULIN may interact with BACTERIAL SURFACE RECEPTORS, and inhibit colonization . May inactivate surface glucosyltransferases, which would reduce
synthesis of extra cellular glucans resulting in reducing plaque formation.
SECRETORY IgA from salivary glands due to direct immunization of gut associated lymphoid tissue (GALT): May prevent MS from adhering to the enamel surface. May also prevent formation of dextran by inhibiting the activity of
glucosyltransferase (GTF).
GINGIVAL CREVICULAR mechanism : All humoral and cellular components of systemic immune system, that exert its function at tooth surface.
MECHANISM OF ACTION OF VACCINE
Lehner T. Immunology of dental caries. Immunology of oral diseases. 3rd ed. Blackwell scientific publications; 1992.
Wilton JM. Future control of dental disease by immunization: Vaccines and oral health. Int Dent J 1984;34:177-83.
Lehner T, Challacombe SJ, Caldwell J. Immuologic basis for vaccination against dental caries in Rhesus monkeys. J Dent Res 1976;55:C166-80.

Contains structural
elements of either adhesins or GTF or GBP.
Also called attenuated expression
vectors.Helpful in targeting vaccine to
appropriate lymphoid tissue
for mucosal response.
Chemical conjugation of
functionally associated
peptide components
with bacterial polyssacharides
.
TYPES OF VACCINESSUB UNIT VACCINE
RECOMBINANT VACCINE CONJUGATE VACCINE

ORAL/ MUCOSAL
SYSTEMIC (SUBCUTANEOUS)
ACTIVE GINGIVO- SALIVARY
PASSIVE DENTAL IMMUNIZATION
ROUTES OF IMMUNIZATION

ACTION OF LOCAL IMMUNITY
Administration of antigen in the vicinity of salivary glands
Induction of salivary IgA to S.mutans
Adverse reactions- Local inflammation Systemic serum antibody response

Mucosal application of dental caries vaccines is preferred for induction of secretory IgA antibodies in salivary compartment.
It has been shown that exposure of an antigen to a mucosally associated lymphoid tissue in the gut, nasal, bronchial, or rectal site can give rise to immune response not only in the region of induction but also in remote location.
Several mucosal routes used to induce protective immune responses to dental caries vaccine antigens: Oral Intra Nasal Tonsillar Minor salivary gland Rectal
COMMON MUCOSAL IMMUNE SYSTEM
Russell MW, Hajishengallis G, Childers NK, Michalek SM. Secretory Immunity in defense against cariogenic Mutans streptococci. Caries Res 1999;33:4-15.

Early studies relied on oral induction of immunity in GALT to elicit protective salivary IgA response.
Smith DJ (2002): applied antigen by oral feeding, gastric intubation, or in vaccine containing capsules or liposome.
ORAL
Smith DJ. Dental caries vaccines: Prospects and concerns. Crit Rev Oral Biol Med 2002;13:335-49.

Oral route failed to reduce caries significantly, as compared with subcutaneous immunization. The rise in secretory antibodies produced was small and of
short duration. Immunological memory in secretory IgA responses is rather
limited. Effect of stomach acidity on antigen, Inductive sites were relatively distant.
ORAL

Recent attempts have been made to induce protective immunity in mucosal inductive sites that are in close anatomical relationship to the oral cavity.
Intranasal installation of antigen targets the nasal associated lymphoid tissue (NALT) (Brandtzaeg & Haneberg,1997).
NALT is stimulated to produce antibodies against mutans streptococcal colonization and accumulation.
INTRANASAL ROUTE
Curtis R 3rd. 1984 Kreshover lecture: Genetic analysis of S. mutans virulence and prospects for an anticaries vaccine. J Dent Res 1986;65:1034-45.

INTRANASAL ROUTEBy nasal spray : Vaccine is introduced into the mucosal immune system by nasal
spray. Thus causing increased production of immunoglobulin IgA which fights tooth decay by interrupting the colonization of the bacterium S.mutans.
Advantage: lower doses of ag needed easy adm induces both systemic & mucosal immunity

Has both IgA and IgG response: IgG is more dominant.
Palatine tonsils and nasopharyngeal tonsils contribute precursor cells to mucosal effector sites: such as salivary gland.
Experiments have shown that formalin- killed Streptococcus sobrinus cells in rabbit can induce a salivary immune response, which can significantly decrease the consequences of infection with cariogenic Streptococcus sobrinus.
Repeated tonsillar application of a particulate antigen can induce the appearance of IgA antibodies in both major and minor salivary glands of rabbit. Smith DJ 2002.
TONSILLAR ROUTE
Smith DJ. Dental caries vaccines: Prospects and concerns. Crit Rev Oral Biol Med 2002;13:335-49.

Populate the lips, cheeks, and soft palate.
Their short, broad secretory ducts facilitate retrograde access of bacteria and their products: potential routes for mucosal induction of salivary immune responses.
Experiments with topical application of Streptococcus sobrinus GTF on lower lips of young adults : lower proportion of indigenous S. mutans/ total Streptoccal flora in their whole saliva during a 6 week period following a dental prophylaxis, compared with a placebo group. Smith and Taubman, 1990
Used in children with respiratory ailments where intranasal application is not possible.
MINOR SALIVARY GLAND ROUTE
Smith DJ. Dental caries vaccines: Prospects and concerns. Crit Rev Oral Biol Med 2002;13:335-49.

Colorectal region as an inductive location for mucosal immune responses in humans: it has the highest concentration of lymphoid follicles in the lower intestinal tract.
Preliminary studies have indicated that this route could also be used to induce salivary IgA responses to mutans streptococcal antigens such as GTF.
RECTAL
Smith DJ. Dental caries vaccines: Prospects and concerns. Crit Rev Oral Biol Med 2002;13:335-49.

Subcutaneous administration of S. mutans : elicited IgG, IgM and IgA antibodies.
Antibodies reach oral cavity via gingival crevicular fluid.
Whole cells, cell walls and the 185 KD streptococcal antigen have been administered on 2-4 occasions.
IgG antibodies are well maintained at high titre, IgM progressively fall and IgA antibodies increase slowly in titre.
IgG develop within months of immunization , reaching a titre of upto 1:1280.
SYSTEMIC ROUTE OF IMMUNIZATION
Lehner T. Immunology of dental caries. Immunology of oral diseases. 3rd ed. Blackwell scientific publications; 1992.

To limit potential side effects of other routes and to localize the immune response.
Associated with increased IgG and IgA.
Various modalities: Injecting lysozyme into rabbit gingiva: elicited local antibodies Brushing live S. mutans onto the gingiva of Rhesus monkeys, which
failed to induce antibody formation. Using smaller molecular weight S. antigen, which resulted in better
performance probably due to better penetration.
ACTIVE GINGIVO-SALIVARY ROUTE
Tandon S. Textbook of Pedodontics. 1st ed. Paras Publishing; 2001

External supplementation of antibodies.
Approaches tried: Monoclonal antibodies: to surface antigen I/ II Bovine milk and whey: systemic immunization of cows with a vaccine
using whole S. mutans led to bovine milk and whey containing polyclonal IgG antibodies.
Egg- yolk antibodies: Hamada introduced using hen egg-yolk antibodies against cell- associated GTF of S. mutans.
Transgenic plants: caries vaccine developed from a genetically modified (GM) tobacco plant. Vaccine is colourless and tasteless and can be painted onto the teeth rather than injected and is the first plant derived vaccine.
PASSIVE IMMUNIZATION
Tandon S. Textbook of Pedodontics. 1st ed. Paras Publishing; 2001.News. Genes .n. Greens: The future of oral medicine? Br Dent J2002;192:674.

• Antigen derived from animals/ humans has potential for hypersentivity.
• Give antibodies in GCF and saliva.
Synthetic peptides
• CT is a powerful mucosal immuno adjuvant.
• Mucosal appl of soluble protein or peptide antigen alone: not effective.
• Addition of CT or E.coli heat labile LT: enhances immune response.
Coupling with Cholera Toxin subunits.
• Avirulent strains of salmonella act as effective vaccine vector: fusion using recombinant techniques
Fusing with salmonella• Microcapsules and
microparticles of polylactide-co-glycolide (PLGA) used as local delivery systems.
• Advantages: ability to control the rate of release, evade preexistent antibody clearance mechanisms and degrade slowly without eliciting an inflammatory response
Microcapsules and microparticles
• Liposomes are bilayered phospholipids membrane vesicles manufactured to contain and deliver drugs and antigens.
• Are thought to improve mucosal immune responses by facilitating M cell uptake and delivery of antigen to lymphoid elements of inductive tissue.
Liposomes
ADJUVANTS AND DELIVERY SYSTEMS
News. Genes .n. Greens: The future of oral medicine? Br Dent J 2002;192:674.

CLINICAL RESEARCH IN THE FIELD OF CARIES VACCINE

CLINICAL RESEARCH IN THE FIELD OF CARIES VACCINE


All vaccines have risks.
Immunologically cross reactive with human heart tissue and rabbit skeletal muscle myosin are found in cell membranes of S. mutans.
Heart cross reactive Ab do not develop in Rhesus monkey or rabbits immunized with purified Ag I/II from S. mutans.
Due to potential of S.mutans whole cells to induce heart – reactive Ab, the development of subunit vaccine for caries has been focused of intense research interest.
RISK OF USING CARIES VACCINE

Although the prevalence of dental caries has declined according to a national epidemiological survey by US national institute of dental research, this oral disease is still a significant health problem that affects approximately 50% of 5-17 year old children.
Developing countries without a water fluoridation system and where access to dental health education and treatment may not be available to everyone are in great need of a vaccine.
PUBLIC HEALTH ASPECTS

Caries reduction could be attained if colonization of S. mutans could be prevented or reduced at the time of eruption of both primary and permanent teeth.
Caries vaccine can be a successful adjunct to other caries-preventive measures.
PUBLIC HEALTH ASPECTS

Identify virulence agents Design means to induce protective response Animal model Human tests
Caries vaccines response requirements:o -interfere with early colonizationo -not necessarily bactericidalo -non-inflamatory responseo -persistent responseo -site directed response (oral cavity)
PRODUCTION OF DENTAL CARIES VACCINE

Trangenic plants: - Hyatt • Passive immunization with tobacco plants.• Genetic materials can easily be exchanged• Possible to manipulate the antibody structure while preserving its
specifity• Can avoid cross reactivity• Large scale production possible• cheap
RECENT ADVANCES
Wuhan Institute of Virology, China: developed a new DNA vaccine : pGJA-P/VAX
pGJA-P/VAX: Encoding two antigenic domains , Pac and GLU of S mutans
Induced accelerated and increased specific antibody response in serum and saliva compared with non fusion DNA vaccine in rabbits.
Limitation: Weak protective effect against S sobrinus.
NEW FUSION ANTI- CARIES DNA VACCINE

Etiologic agent part of indigenous flora Vaccination should be done on periodic basis Development of tolerance or immune exclusion Caries occurs on non living surface
WHY IS CARIES VACCINE NOT MUCH IN PRACTICE??

Both passive and active immunization approaches have demonstrated succes in animal models and human clinical trials.
The efficacy of active immunization with subunit vaccines from S.mutans has been proved to prevent dental caries in animal models.
However, there are few studies on efficacy in humans. The primary target of such a vaccine would be young children, who
are at high risk at this disease. Risk-free and more effective approach to prevent human dental
caries should be developed. Recent advances in research on mucosal vaccines will lead to a
safe and effective vaccine
CONCLUSION