care coordination project: 2007-2011 overview and results grant mitchell, md commissioner...
TRANSCRIPT

Care Coordination Project:2007-2011 Overview and Results
Grant Mitchell, MD Commissioner
Westchester County Department of Community Mental Health
1

Westchester’s Care Coordination Program
To improve health outcomes and reduce costs, Westchester County implemented a more self-directed, recovery-focused, care coordination program for individuals with historically poor outcomes and high costs.
Goals:– Individuals to have greater control of and responsibility for
their own care– Expand the “menu” of services beyond those reimbursed by
Medicaid by providing self-directed funds.– Improve health outcomes and reduce costs– Ensure access to needed services– Coordinate services to address fragmentation 2

Westchester’s Care Coordination Program
Eligibility:– Voluntary– Serious mental illness– High service utilization/costs– History of criminal justice involvement and/or
homelessness (not required)
3

Westchester’s Care Coordination Program
4
Service-Resistant Clients?
OR
Client-Resistant Services?

Traditional Approaches
A Traditional Sequenceof Delivering Services
PERSON DREAM SUPPORT RESOURCES
5

An Alternative to Traditional Approaches
PERSON DREAM SUPPORT RESOURCES
6

Goals of the Care Coordination Program
Culture change to emphasize person-centered planning and
recovery. Empower individuals through service planning that promotes choice
and is shared across the service system . Coordinate services delivered by multiple providers. Implement evidence-based and best practices where available. Allocate resources based on individual need. Utilize information systems that provide timely, useful information. Determine performance by measuring outcomes.
7

Care Coordinators
Each Care Coordinator partners with 12 enrollees Individual creates an Individual Service Plan (ISP) that is
shared across services (Web-based) and includes use of self-determination funds for non-traditional services and supports (like the Peer Mentor Program.)
Arrange admission into desired or needed standard health services
Coordinate mental health, chemical dependence, medical, legal, housing and needed support services
Collect and report outcomes data
8

Self-Directed Funds
$1500 per individual/year Individual control over how dollars are spent
related to goals as established in the ISP Expand the array of services/supports beyond
those covered by Medicaid
9
Self-Directed Funds
Examples:– Housing: Furnishings, household items,
maintenance, temporary housing– Education: Courses, computers, – Medical care: Dental, medication– Employment: Resume, clothing for interviews– Other: gym membership, exercise equipment,
yoga, music, books, personal care
10

Peer Mentoring Program
Option to select a recovery mentor Mentors participate in engagement & ISP
development Serve as role models, partners with enrollee and
the care coordinator Crisis prevention and intervention Not case managers
Employment/Training
48 slots/3 years 1 week intensive program Assistance in locating employment
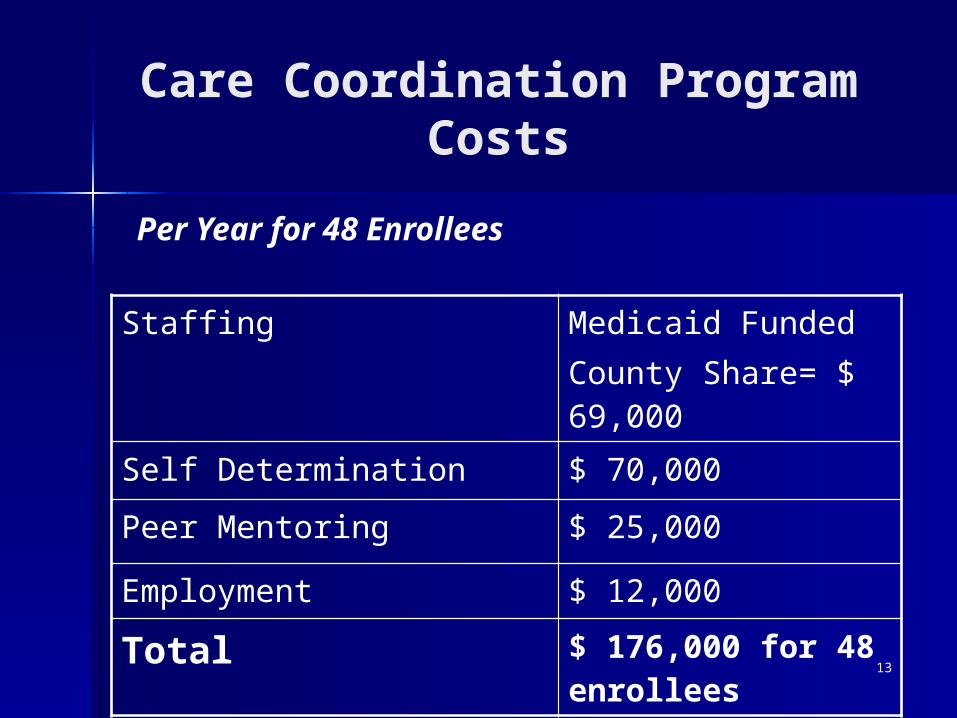
Care Coordination Program Costs
Staffing Medicaid Funded County Share= $ 69,000
Self Determination $ 70,000
Peer Mentoring $ 25,000
Employment $ 12,000
Total $ 176,000 for 48 enrollees
Per Year for 48 Enrollees
13

Program Outcomes
Medicaid Costs Days in State Hospital Days Incarcerated Visits to ER Homelessness Quality of Life Indicators Satisfaction with Program (staff/enrollee) Person-centeredness
14
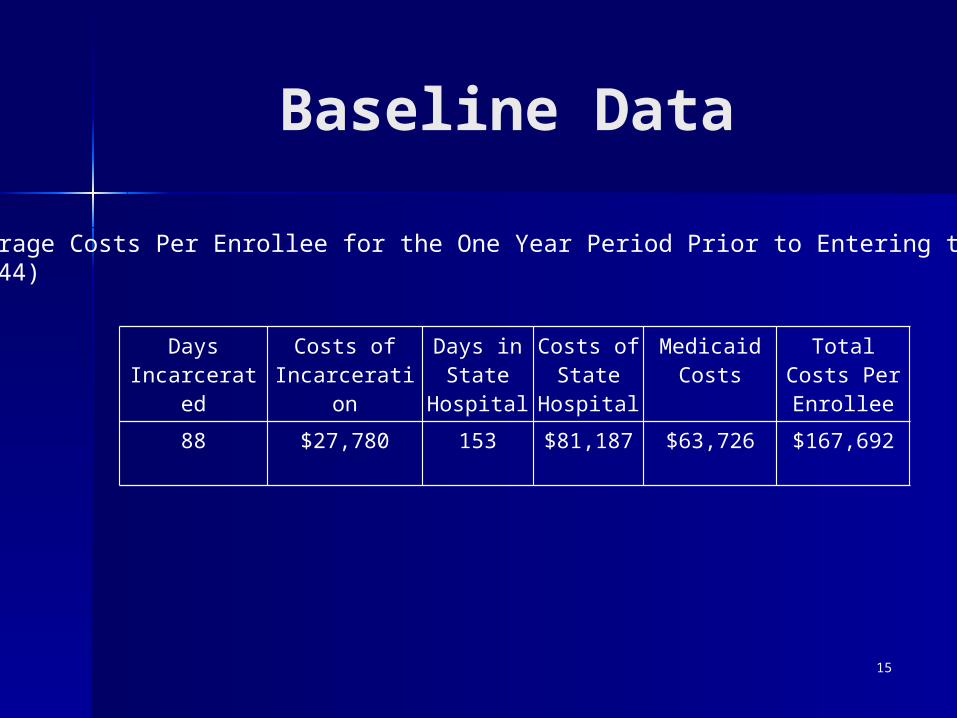
Baseline Data
Days Incarcerated
Costs of Incarceration
Days in State
Hospital
Costs of State
Hospital
Medicaid Costs
Total Costs Per Enrollee
88 $27,780 153 $81,187 $63,726 $167,692
Average Costs Per Enrollee for the One Year Period Prior to Entering the Program (N=44)
15

Results: Pre & Post-Enrollment Cost Data(N= 31)
$822,119
$535,634
$870,260
$410,860
$592,150
$129,850
0
100000
200000
300000
400000
500000
600000
700000
800000
900000
Medicaid Jail State Hospital
pre-enrollment
post-enrollment
16

Cost Outcomes (N= 31)
Medicaid (other than state
hospital)
Incarceration State Hospital Total
2007- 2008Pre-Enroll
$ 822,119 $ 870,260 $ 592,150 $ 2,284,529
2008-20091 year after
$ 535,634 $ 410,860 $ 129,850 $ 1,076,344
Savings $ $ 286,485 $ 459,400 $ 462,300 $ 1,208,185
Savings % 35% 53% 78% 53%
17
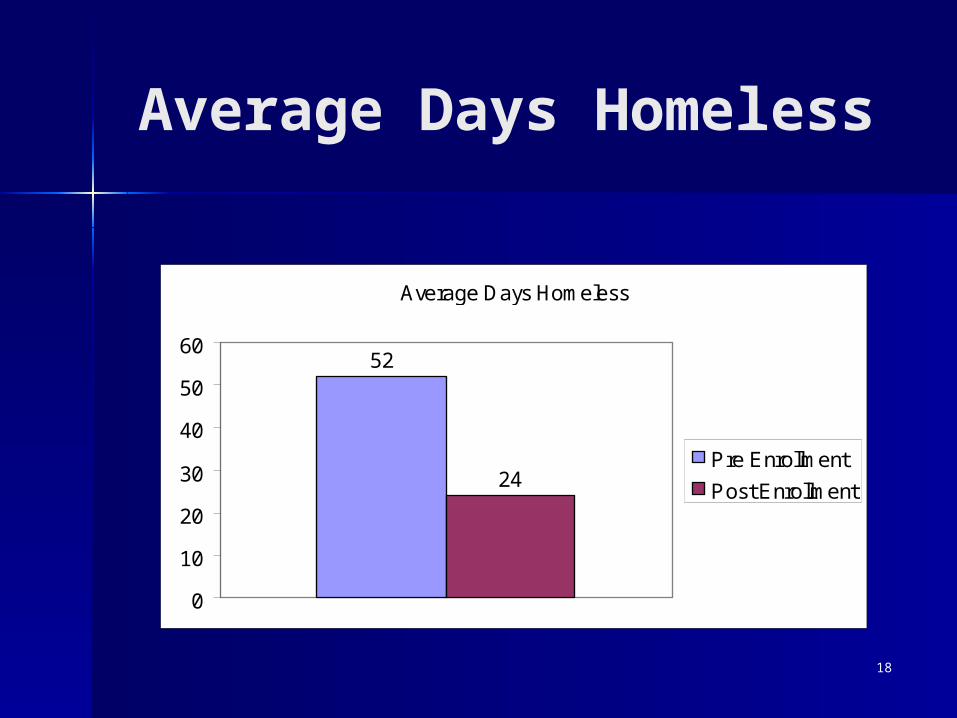
Average Days Homeless
Average Days Homeless
52
24
0
10
20
30
40
50
60
Pre Enrollment
Post Enrollment
18
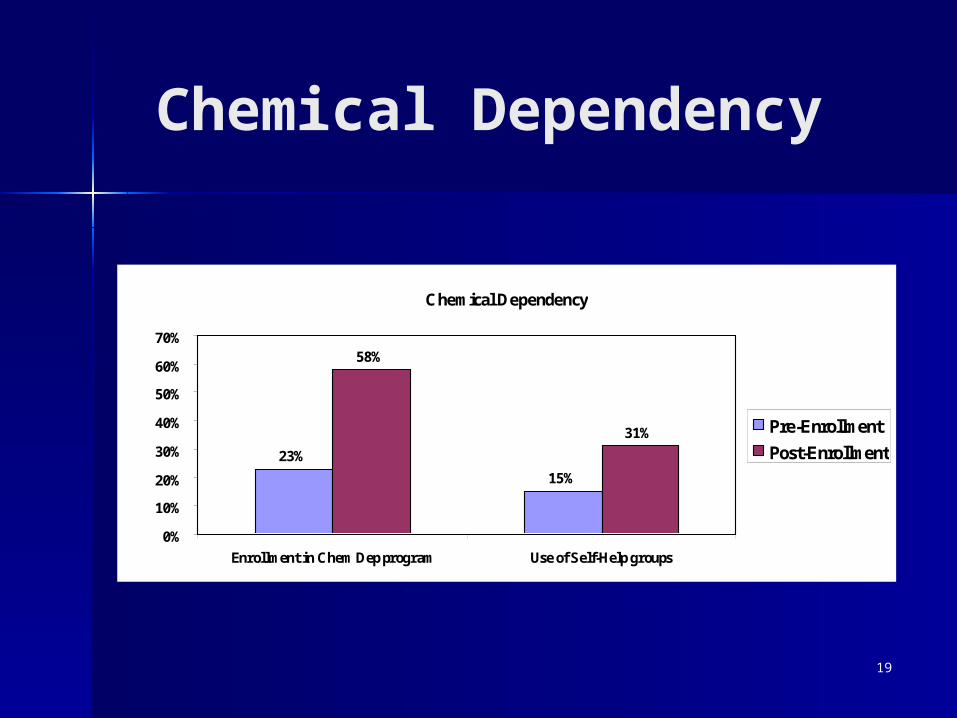
Chemical Dependency
Chemical Dependency
23%
15%
58%
31%
0%
10%
20%
30%
40%
50%
60%
70%
Enrollment in Chem Dep program Use of Self-Help groups
Pre-Enrollment
Post-Enrollment
19

Other Outcomes
Enrollees report feeling more in control of life. “Authority”
Care Coordinators report job satisfaction levels are up vs. working in traditional ICM role (“This is why I went into the field.” “In many ways, my job is now significantly easier).”
Trumpet; birthdays
21
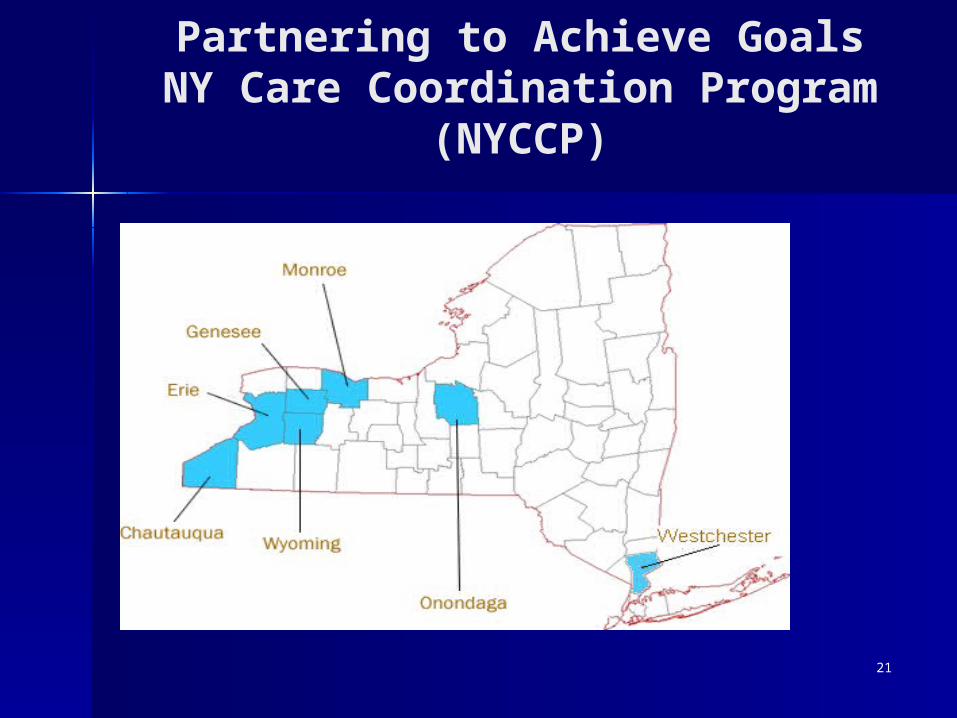
Partnering to Achieve GoalsNY Care Coordination Program (NYCCP)

22
NY Care Coordination Program (NYCCP)
– Care Coordination– Person-centered planning– Managed care as a vehicle to achieve flexibility– System transformation– Existing working relationships with Beacon Health
Strategies– Pay for Performance

Next Steps—Westchester’s Care Coordination Program Western New York—Care Coordination Program
– 7 County Consortium– Years of Experience– Better Outcomes and Reduced Costs
System reform– Align funding and structures to improve
outcomes and reduce health care costs– Expand the “menu” of services—flexible
spending– Prepare for Health Care Reform- Regional
BHO’s and Health Homes23