care beyond clinical: patient safety at the bedside
TRANSCRIPT

Oncology Nursing Society 43nd Annual CongressMay 17–20, 2018 • Washington, DC 1Clinical Practice
1. Sustaining Positive Outcomes With a Progressive Upright Mobility Program Protocol in Cancer PatientsVictoria Shemaria, BSN, RN, CCRNCancer Treatment Centers of AmericaPhiladelphia, PA
2. Child Visitation Guidelines: Development and Implementation on an Inpatient Cancer Center UnitStephanie Everitt, RN, BSN, OCNUniversity of Maryland Medical Center Baltimore, MD
3. Stop the Beeps! Decreasing Noise Level and Alarm Fatigue on an Oncology Intermediate Care UnitAshley Keppel, RN, MSN, OCN, PCCNRoswell Park Cancer InstituteBuffalo, NY
4. Can We Give You Some TIPS? Tailored Interventions for Patient Safety on a Hematopoietic Stem Cell Transplant (HSCT) UnitThanyanee McNinney, BSN, RN, OCNNew York Presbyterian: Weill-Cornell New York, NY
Care Beyond Clinical: Patient Safety at the BedsideSaturday, May 19 • 2:45–4 pm
Note one action you’ll take after attending this session: ____________________________________________________
________________________________________________________________________________

ONS 43rd Annual Congress
Clinical Practice (Shemaria) 1
Sustaining Positive Outcomes with a Progressive Upright
Mobility Protocol Program in Cancer Patients
Victoria Shemaria BSN RN CCRN, Anne Newbert BSN RN CCRN, Richard Wright BSN RN, Jason Brash BSN RN CPAN CCRN, Paul Gehringer BSNRN WCCN, Stephanie Ashton BSN RN CCRN, Joanne McGovern MSN RN CCRN, Jeffrey Hoag MD MS
Cancer Treatment Centers of America
Disclosures
I do not have a financial interest/arrangement or affiliation with one or more organizations that could be perceived as a
real or apparent conflict of interest in the context of the subject of this presentation.

ONS 43rd Annual Congress
Clinical Practice (Shemaria) 2
Introduction & Rationale
• Critical illness associated with immobility leads to significant morbidity including increased ICU and hospital lengths of stay (LOS) and prolonged deconditioning.
• Several prior studies have demonstrated improvements in LOS and ventilator days with early institution of mobility programs.
• Malignancy and short expected life span have been exclusions from all prior mobility studies.
• The purpose of this retrospective investigation was to examine the safety, effectiveness and sustainability of a Progressive Upright Mobility Program (PUM) in critically ill ventilated cancer patients.
• Measured variables include ventilator days, ICU/Hospital LOS, and severity of illness using the APACHE IV scoring system.
• Twelve months of baseline data collected:
Patient demographics
Ventilator days
ICU and hospital LOS
Severity of illness using APACHE IV scoring system
• Multidisciplinary team established (ICU RN’s, Intensivists, RT, PT/OT):
A stepwise PUM protocol was developed and followed in all mechanically ventilated patients admitted to a single subspecialty cancer hospital ICU.
Methods
Methods Advancement through the five step protocol:
Hemodynamic stability
Physical tolerance
RASS
Exclusion criteria included:
Hemodynamic instability
Neuromuscular blockade
ICP monitoring
Spinal cord injuries
Pelvic/lower extremity fractures
Richmond Agitation Sedation Score (RASS)

ONS 43rd Annual Congress
Clinical Practice (Shemaria) 3
Methods • Nurse driven protocol Core group of designated RN champions took the lead
• Resources: Provided education throughout departments on PUM protocol purpose and goals.
• Compliance: PUM initiated at onset of mechanical ventilation. Documentation tool utilized every shift. Added to charge nurse quality metric indicators checklist to ensure nurse accountability.
• Evaluated Complications: Addressed barriers to protocol advancement.
• Data from control period (Pre) was then compared to twelve month post-intervention (Post) data.
• Protocol sustainability was determined by collecting additional twelve months of data and comparing results to Pre and Post intervention groups.
PUM Protocol Level 1Breathe
PUM Protocol Level 2Tilt

ONS 43rd Annual Congress
Clinical Practice (Shemaria) 4
PUM Protocol Level 3Sit
PUM Protocol Level 4Stand
PUM Protocol Level 5Move
ONS 43rd Annual Congress
Clinical Practice (Shemaria) 5
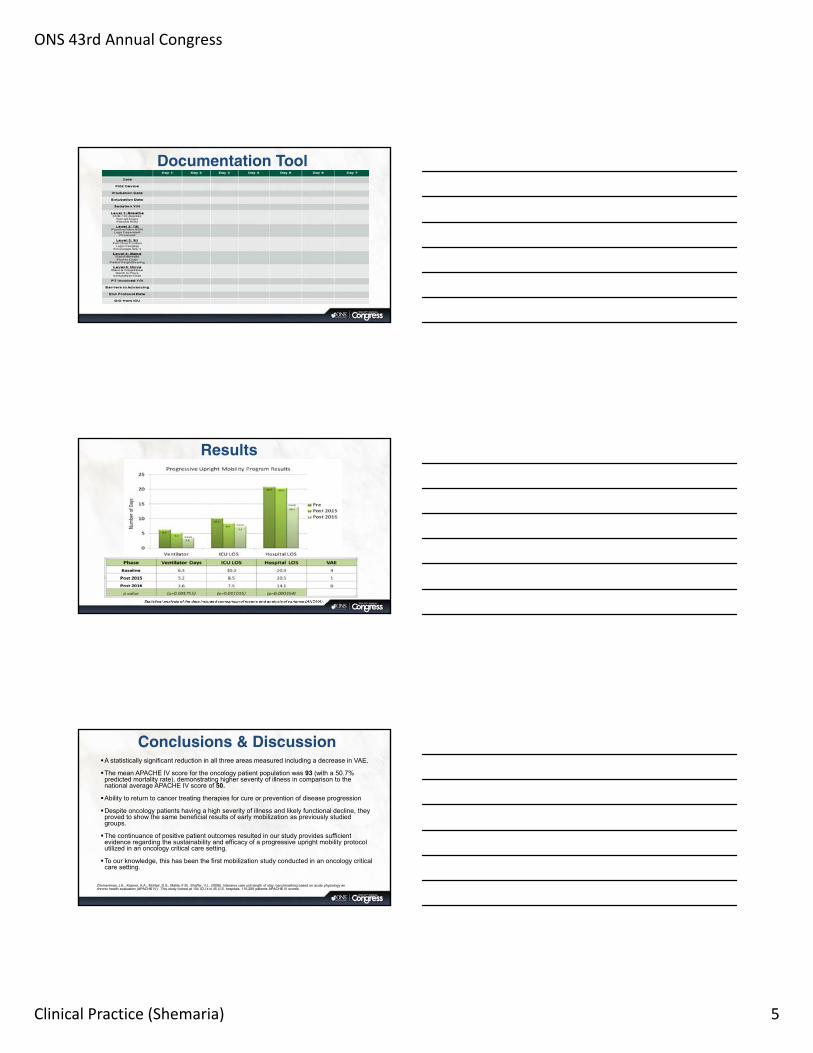
Documentation Tool
Results
Conclusions & DiscussionA statistically significant reduction in all three areas measured including a decrease in VAE.
The mean APACHE IV score for the oncology patient population was 93 (with a 50.7% predicted mortality rate), demonstrating higher severity of illness in comparison to the national average APACHE IV score of 50.
Ability to return to cancer treating therapies for cure or prevention of disease progression
Despite oncology patients having a high severity of illness and likely functional decline, they proved to show the same beneficial results of early mobilization as previously studied groups.
The continuance of positive patient outcomes resulted in our study provides sufficient evidence regarding the sustainability and efficacy of a progressive upright mobility protocol utilized in an oncology critical care setting.
To our knowledge, this has been the first mobilization study conducted in an oncology critical care setting.
Zimmerrman, J.E., Kramer, A.A., McNair, D.S., Malila, F.M., Shaffer, V.L. (2006). Intensive care unit length of stay: benchmarking based on acute physiology anchronic health evaluation (APACHE IV) This study looked at 104 ICU’s in 45 U.S. hospitals, 116,209 patients APACHE IV scores.

ONS 43rd Annual Congress
Clinical Practice (Shemaria) 6
References• Davis, J., Crawford, K., Wierman, H., Osgood, W., Cavanaugh, J., Smith, K. A., . . . Orff, S. (2013). Mobilization of
Ventilated Older Adults. Journal of Geriatric Physical Therapy, 36(4), 162-168. doi:10.1519/jpt.0b013e31828836e7
• Demmayer, J., Baldwin, N., Packard, D., Harrington, S., Cristofferson, B., Christopher, J., . . . Iwashyna, J. (2013). Mobilizing Outcomes Implementation of a Nurse-Lead Multidisciplinary Mobility Program. Critical Care Nursing Quarterly, 36(1), 109-119. doi:10.1097/CNQ.0b013e31827535db
• Engel, H. J., Needham, D. M., Morris, P. E., & Gropper, M. A. (2013). ICU Early Mobilization. Critical Care Medicine, 41. doi:10.1097/ccm.0b013e3182a240d5
• Hopkins, R. O., & Spuhler, V. J. (2009). Strategies for Promoting Early Activity in Critically Ill Mechanically Ventilated Patients. AACN Advanced Critical Care, 20(3), 277-289. doi:10.4037/15597768-2009-3009
• Kasotakis, G., Schmidt, U., Perry, D., Grosse- Sundrup, M., Benjamin, J., Ryan, C., . . . Eikermann, M. (2012). The surgical intensive care unit optimal mobility score predicts mortality and length of stay*. Critical Care Medicine, 40(4), 1122-1128. doi:10.1097/ccm.0b013e3182376e6d
• Schweickert, W. D., Pohlman, M. C., Pohlman, A. S., Nigos, C., Pawlik, A. J., Esbrook, C. L., . . . Kress, J. P. (2009). Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. The Lancet, 373, 1874-1882. doi:10.1016/S0140-6736(09)60658-9
• Winkelman, C., Johnson, K. D., Hejal, R., Gordon, N. H., Rowbottom, J., Daly, J., . . . Levine, A. D. (2012). Examining the positive effects of exercise in intubated adults in ICU: A prospective repeated measures clinical study. Intensive and Critical Care Nursing, 28(6), 307-318. doi:10.1016/j.iccn.2012.02.007
• Zimmerman, J.E., Kramer, A.A., McNair, D.S., Malila, F.M., Shaffer, V.L. (2006). Intensive care unit length of stay: benchmarking based on acute physiology and chronic health evaluation (APACHE IV

ONS 43rd Annual Congress
Clinical Practice (Everitt) 1
Care Beyond Clinical: Patient Safety at the Bedside
Child Visitation Guidelines: Development and Implementation on an
Inpatient Cancer Center UnitStephanie Everitt, BSN, RN, OCN®
Senior Clinical Nurse IKaren Snow Kaiser, PhD, RN
Clinical Practice Coordinator University of Maryland Medical Center
Greenebaum Comprehensive Cancer Center
Disclosures• The authors have no disclosures to report.

ONS 43rd Annual Congress
Clinical Practice (Everitt) 2
Significance• Child visitation restrictions have been common practice in oncology
inpatient settings for infection prevention reasons• Age-based visitor restriction is not:
– evidence-based– recommended by any professional oncology organization
• Age-based visitor restriction conflicts with the gold standard, patient-centered care
• Family presence in the hospital has been linked to:– an increased sense of well-being – a decrease in patient and family member stress levels
Purpose• To develop and evaluate a
standardized oncology nursing unit visitation process that:– supports patient-centered
care – maintains patient safety
(Photo consent obtained)
Background: Initial Visit Practices• Hospital policy
– Child under the age of 12 may visit at the discretion of the patient’s nurse or clinical area
• Informal unit practice– Allow adults– Restrict visitation in patient’s room if child under the age 12– Allow child under the age 12 in the visitor lounge with patient (if patient
physically and mentally able)

ONS 43rd Annual Congress
Clinical Practice (Everitt) 3
Background• Performed literature search
• Found one evidence-based process case study described revisions to child visitation policy1
‒ Assessed national guidelines/position statements‒ No literature supported child visitor restrictions‒ Stressed environmental precautions
‒ Surveyed local facilities• 71% of large facilities allowed child visitors (17 large hospitals)• 53% of smaller facilities allowed child visitors (17 smaller hospitals,
including clinics)
1Falk, J., Wongsa, S., Dang, J., Comer, L. & LoBiondo-Wood, G. (2012). Using an evidence-based practice process to change child visitation guidelines. Clinical Journal of Oncology Nursing, 16(1), 21-23.
Background (con’t)• Performed literature search (con’t)
‒ We assessed updated and additional national guidelines/position statements than case study article‒ Centers for Disease Control and Prevention, American Cancer Society,
Infectious Disease Society of America‒ Findings similar to case study
‒ use proper hand hygiene‒ avoid crowds‒ avoid sick contacts
Intervention• Developed visitation guidelines and screening criteria
– Worked with Infection Control and Infectious Disease personnel– Created a form to screen child visitors <12 years of age
• Deployed a staff survey about screening practices and barriers – Nine-item survey (six, 5-point Likert items and 3 open-ended response items)– Thirty-five oncology staff (nurses, nursing assistants, unit secretaries) completed;
39% response rate• Used survey responses to guide staff education and clinical
implementation – Unit-based governance council educated staff via a continuing education module
(69% completion rate) and in-services

ONS 43rd Annual Congress
Clinical Practice (Everitt) 4
Intervention• Assembled and deployed a staff resource
binder including talking points• Placed guidelines on back of screening
form and posted in each patient room• Screened all visitors to detect signs and
symptoms of infection
New General Visitor GuidelinesProcess• Visitors receive a copy of the
guidelines• Staff are expected to:
– review guidelines with family/patient
– educate family/patient on avoiding sick contacts (protect immune-compromised patients)
– take responsibility in ensuring visitors are healthy and not showing signs of illness
Visitor Guidelines• Should not visit if they had or were in contact
with anyone who had:– signs of illness within the past seven days (e.g.,
respiratory symptoms, GI symptoms, fever, rash) – a contagious illness within the past month (e.g.,
tuberculosis, chicken pox or measles)
• Must wash hands with soap/water or hand sanitizer before entering and when leaving a patient room
• May spend night in patient’s room (1 adult) – Permission granted by the nurse
New Child Visitor GuidelinesProcess• Screening form
– Complete each time child visits– Encourage initiation before the planned visit
day
• Child– Receives a sticker (located in the treasure
box at the nurses station) if passes screening – Can visit in lobby waiting area outside the
unit if does not pass screening
• Specific concerns– Contact Infection Prevention as needed
Guideline (< age 12)• Must have up-to-date vaccinations (per the
American Academy of Pediatrics)• Must have a non-patient caregiver in charge
of the child during visit • May visit 10am-10pm (facilitates patient care
and sleep)• May not visit patients with airborne isolation,
droplet isolation or active Clostridium Difficile• May be asked to leave per nurse’s discretion

ONS 43rd Annual Congress
Clinical Practice (Everitt) 5
Child Visitor Screening Form
Evaluation• Same nine-item survey deployed three months post-implementation
– Mann-Whitney U to compare pre- and post-implementation responses– Content analysis for open-ended items (2 reviewers, consensus agreement)
• Convenience sample consisted of 36 staff (47% response rate)
Evaluation • Staff were significantly more likely to agree post implementation that there is a
unit specific visitation guideline

ONS 43rd Annual Congress
Clinical Practice (Everitt) 6
Evaluation • Staff were significantly more likely to agree post-implementation that they felt
comfortable explaining current visitation practice reasons
Evaluation • Staff were significantly more likely to agree post-implementation that they
screen all patients
Evaluation Screening Barriers Pre Post
N % of responses % of cases N % of responses % of cases
Time consuming 16 15.7% 45.7% 21 25.6% 61.8%
No screening standard 28 27.5% 90.0% 7 8.5% 20.6%
No reminder 9 8.8% 25.7% 5 6.1% 14.7%
Intrusive 13 12.7% 37.1% 11 13.4% 32.4%
Unaware of New Visitor 32 31.4% 91.4% 31 37.8% 91.2%
Responsible for my patients 4 3.9% 11.4% 7 8.5% 20.6%
Total 102 100% 291.4% 82 100% 241.2%

ONS 43rd Annual Congress
Clinical Practice (Everitt) 7
Evaluation • Content analysis
‒ Compared to pre-implementation, when screening for illness post implementation staff:‒ observed for more specific signs and symptoms of infection‒ asked more specific questions of families about signs and symptoms of infection ‒ provided more information about visitation rationale and rules
Discussion• Increased staffs’ reported comfort level with explaining visitation
rationale and screening process• Increased staffs’ self-report of:
– signs and symptoms of infection – screening criteria – rationale and rules of visitation
• Provided patient- and family-centered care– 180 screenings completed in a 6-month period
• Identified barriers to screening:– awareness of visitors on the unit– time commitment
Next Steps• Evaluate guideline using a quality improvement perspective for its
impact on:– patients– families– Infection rates
• Assess visitors’ knowledge of visitation best practices

ONS 43rd Annual Congress
Clinical Practice (Everitt) 8
References• Center for Disease Control and Prevention. (2017). What you need
know neutropenia and risk for infection. Retrieved from https://www.cdc.gov/cancer/preventinfections/pdf/neutropenia.pdf
• Falk, J., Wongsa, S., Dang, J., Comer, L. & LoBiondo-Wood, G. (2012). Using an evidence-based practice process to change child visitation guidelines. Clinical Journal of Oncology Nursing, 16(1), 21-23.
• Thom, K.A., Kleinberg, M., & Roghmann, M. (2013). Infection prevention in the cancer center. Clinical Infectious Diseases, 57(4), 579–585. https://doi.org/10.1093/cid/cit290

ONS 43rd Annual Congress
Clinical Practice (Keppel) 1
Stop the Beeps!Decreasing Noise Level and Alarm Fatigue
on an Oncology Intermediate Care Unit
Ashley Keppel, MSN, RN, OCN, PCCNClinical Nurse Manager
Erin Hughes, BSN, RNBMT Administrative Charge Nurse
Disclosures
There are no financial interests or relationships to disclose

ONS 43rd Annual Congress
Clinical Practice (Keppel) 2
Introduction
Who are we? • Roswell Park Comprehensive Cancer Center
– NCI designated– Free-standing comprehensive cancer center in Buffalo, NY– Ranked among the nation's top cancer hospitals by U.S. News & World Report 2017-2018– 133 bed hospital
• Intermediate Care Unit (IMCU)– 17 beds– Caring for post-surgical patients or patients requiring higher level care
• Unit Based Council (UBC)– Consisting of staff members in all positions
Significance National Patient Safety Goal 2015 Reduce the harm associated with clinical alarm systems.NPSG.06.01.01: Use Alarms Safely- Multifaceted problem- Unique and customized solutions necessary
Problem Noise level of an oncology intermediate care unit increased in the year 2015 as evidenced by HCAHPS scores
Staff concern for alarm fatigue related to unnecessary alarms, potentially compromising patient safety

ONS 43rd Annual Congress
Clinical Practice (Keppel) 3
Problem
• UBC developed survey and distributed to all staff with a 73% response rate
• Staff believed the Drager® Monitor was safer but unnecessary alarms were causing delay in response
• 77% of nurses said alarms were being ignored due to excessive alarms
Problem• Two monitors being utilized at the same time for one critical care patient
• Standard parameter settings for both systems
• Lack of knowledge regarding how to adjust alarm settings and systems
• Equipment not readily available (not enough cords for all monitors)
Action• Interventions were initiated in three areas of concern:
– Inappropriate default settings • Peer-to-peer education provided to all staff • Nurse-to-nurse report included checking alarms• MD Orders placed for monitor limits, to adjust settings as indicated by provider
– Multiple systems monitoring one patient• Obtained approval from key stakeholders • Staff ordered necessary equipment to support using one primary system for all patients, and secondary
system only in designated situations
– Staff fatigue• Highlighted importance of alarm safety• Encouraged staff feedback regarding alarms and impact on patient

ONS 43rd Annual Congress
Clinical Practice (Keppel) 4
Action• An educational flyer was provided
to staff as well as sent in email for all staff to reference
• Education set expectations for all staff members
• Staff signed off on education
• Utilized “Champions” as needed for questions
Results
5.5
17.1
10.8
0
5
10
15
20
HCAHPS Results: Patients reporting the area around their room was “always” quiet at night
Q1, 2016
Q2, 2016
Q3, 2016
% of increase in HCAHPS
result post‐intervention
And the survey says:
90.9% of staff surveyed were checking and adjusting settings on their monitor
71% of staff felt that alarm fatigue had been reduced post‐interventions
100% of staff felt the single monitor was safer for patients

ONS 43rd Annual Congress
Clinical Practice (Keppel) 5
Results
Patient satisfaction
Nurse responsiveness Single monitoring systemImproved Patient Safety
Nursing Implications• Frontline staff can initiate practice change to decrease
alarm fatigue
• Collaboration between key stakeholders and shared governance councils can lead to improved patient safety
• Education on alarms and monitoring systems should be ongoing and unique to staff input
References• Best Hospitals for Cancer 2017-2018. (n.d.) U.S. News and World Report. Retrieved from
https://health.usnews.com/best-hospitals/rankings/cancer
• HCAHPS Fact Sheet. (2017). Centers for Medicare & Medicaid Services. Retrieved from http://www.hcahpsonline.org/en
• The Joint Commission. (n.d.). National Patient Safety Goals Effective January 1, 2015. Retrieved from https://www.jointcommission.org/assets/1/6/2015_NPSG_HAP.pdf

ONS 43rd Annual Congress
Clinical Practice (Keppel) 6
Questions• Contact information:

ONS 43rd Annual Congress
Clinical Practice (McNinney) 1
Thanyanee McNinney, BSN, RN, OCN®
Senior Staff Nurse
New York Presbyterian: Weill-Cornell Medical Center
Can We Give You Some TIPS?Tailored Interventions for Patient Safety on a
Hematopoietic Stem Cell Transplant (HSCT) Unit
Disclosures
I have no personal or financial interests to declare. I have no financial support from an industry source at the current presentation.

ONS 43rd Annual Congress
Clinical Practice (McNinney) 2
New York Presbyterian: Well-Cornell Medical Center
• Founded in 1771
• Located on the Upper East Side of Manhattan
• Large urban academic medical center associated with Ivy League Medical College, Weill Cornell Medical College
• 862 Inpatient beds
• US News & World Report #1 Hospital in the NYC metropolitan area for the past 8 years
New York Presbyterian: Weill-Cornell OncologyINPATIENT & OUTPATIENT UNITS
• Radiation Oncology
• Outpatient Infusion Centers
• 83 inpatient beds
10 WEST: HEMATOPOETIC STEM CELL TRANSPLANT UNIT
• FACT Accredited• 16 beds, all private rooms• 200 transplants/year• 36 registered nurses• 40% certified nurses (OCN®,
BMTCN®)
10 West HSCT
16 beds
10 NorthOnc/HSCT
19 beds
10 SouthHeme/Onc
20 beds
10 CentralHeme/Onc
28 beds
Inpatient Oncology
Background• According to Morse (2009), 92% of falls are preventable
Accidental falls = 14%
Anticipated physical falls = 78%
• According to Center for Medicare and Medicaid Services (CMS), falls are
Hospital-Acquired condition (HAC) and are reasonably preventable using
evidence-based guidelines.
• The Joint Commission (TJC) requires accredited hospitals to conduct
assessments on all hospitalized patients to identify risk for falls.
ONS 43rd Annual Congress
Clinical Practice (McNinney) 3
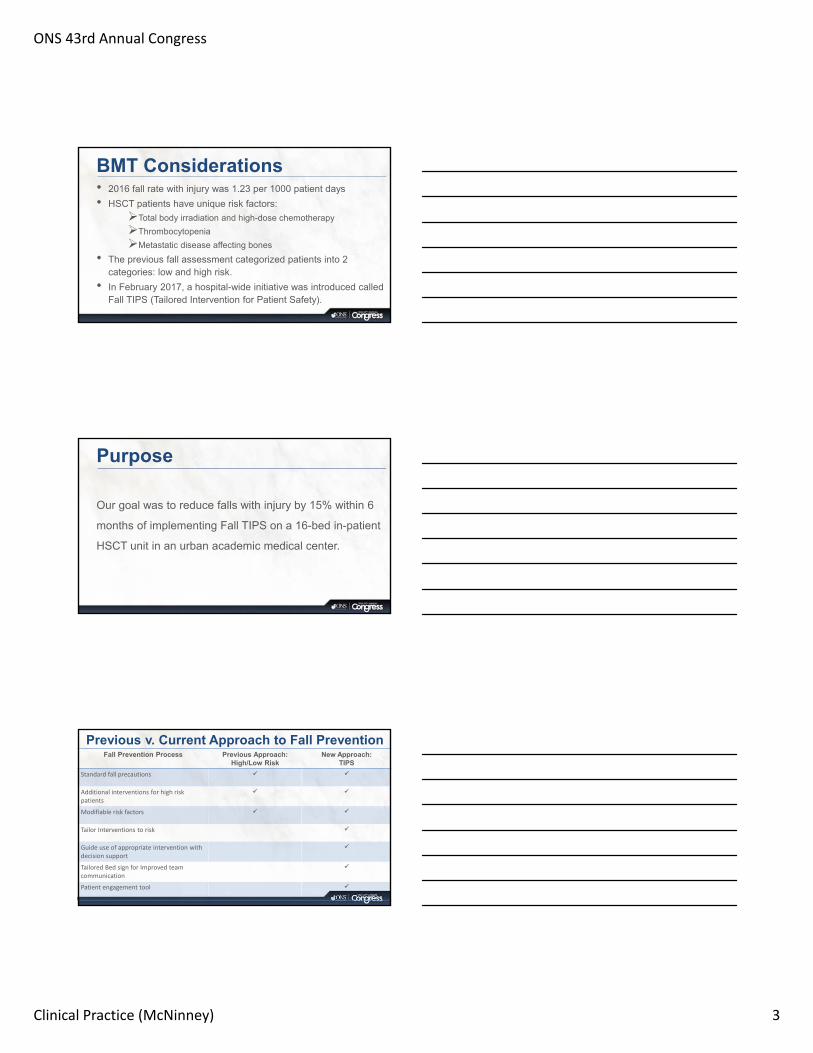
BMT Considerations• 2016 fall rate with injury was 1.23 per 1000 patient days
• HSCT patients have unique risk factors:
Total body irradiation and high-dose chemotherapy
Thrombocytopenia
Metastatic disease affecting bones
• The previous fall assessment categorized patients into 2 categories: low and high risk.
• In February 2017, a hospital-wide initiative was introduced called Fall TIPS (Tailored Intervention for Patient Safety).
Purpose
Our goal was to reduce falls with injury by 15% within 6
months of implementing Fall TIPS on a 16-bed in-patient
HSCT unit in an urban academic medical center.
Previous v. Current Approach to Fall PreventionFall Prevention Process Previous Approach:
High/Low RiskNew Approach:
TIPS
Standard fall precautions
Additional interventions for high risk patients
Modifiable risk factors
Tailor Interventions to risk
Guide use of appropriate intervention with decision support
Tailored Bed sign for Improved team communication
Patient engagement tool

ONS 43rd Annual Congress
Clinical Practice (McNinney) 4
Previous Fall Assessment & Intervention
FALL RISK INTERVENTION BUNDLE HALLWAY SIGN
LOW RISK 0-6
NONE
HIGH RISK 7-22
Fall TIPS
Fall TIPS
Step 1:
Morse Fall Risk
Assessment
• Modifiable risk
factors
Step 2:
Tailored fall
prevention
strategy
• Nursing
Judgement
Step 3:
Consistent
Implementation
• Tailored
Interventions
• Standard fall
precautions

ONS 43rd Annual Congress
Clinical Practice (McNinney) 5
• Mr. S is a 43 year-old male with Multiple Myeloma s/p AutoSCT day +8
• Unsteady gait with generalized weakness; ambulates with cane
• Currently with AMS, neutropenic fevers, and hypoxia
• @0500 RN drew morning labs
• @0530 RN found patient on the floor in a pool of blood
• @0700 Patient head CT shows subdural hematoma and transferred to ICU
Case Study
Step 1: Morse Falls Scale 1. History of Falls in the past 3 months No (0)
Yes (25)
2. Secondary Diagnosis No (0)Yes (15)
3. Ambulatory Aide None/Bed Rest/ Nurse Assist (0)Crutch/Cane/Walker (15)Holds onto furniture (30)
4. IV present No (0)Yes (25)
5. Gait Normal/Bedrest (0)Weak (10)Impaired (20)
6. Mental Status Normal/knows own limitsOverestimates/forgets limits
Step 2: Tailored InterventionsSAFETY
DOCUMENTATIONTOILETING
ASSISTANCEBEDSIDE
ASSISTANCEAMBULATION ASSISTANCE

ONS 43rd Annual Congress
Clinical Practice (McNinney) 6
Putting it all together for the bedside sign…
Patient Education
Results
0
1
2
3
4
5
6
7
8
9
Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17
Fal
ls p
er 1
000
pat
ien
t d
ays
Month and Year
2016-2017 Falls on 10 West
Fall Total
Falls WithInjury

ONS 43rd Annual Congress
Clinical Practice (McNinney) 7
TIPS for Our Success• Fall champions performed TIPS compliance audits
Hospital-wide goal of 10 audits/month per unit
HSCT unit completed, on average, 16 audits per month
•Patient and caregiver interviews
•Reinforced nurse teaching
•Ensured patients requiring assistance/bed rest have a yellow bracelet on
•Root-cause analysis and fall trends
•Post-fall huddles
Challenges & Next Steps •Fall TIPS reduced falls with injury and improve patient safety by focusing on modifiable risk
factors, tailored inventions, and communication tools for patients and staff.
•Challenges
Improve staff compliance
High fall rate
•Next Steps
More language options
Improved staff compliance with posting and updating bed signage
Decrease overall number of falls by implementing purposeful hourly rounding
•All members of the multidisciplinary team play a role in fall prevention!
Acknowledgements
• German Rodriguez, NYP Weill-Cornell Director of
Oncology
• Lara Scrimenti, Patient Care Director
• Catherine Barrie, Clinical Manager
• Cosme Taipe, Nursing Project Manager
• Dianna Assalone, Senior Staff Nurse and Fall
Champion
Thank you to ONS for allowing us to present our work to our nursing colleagues!

ONS 43rd Annual Congress
Clinical Practice (McNinney) 8
ReferencesChristy, R. (2017). Preventing falls in hospitalized older adults. Nursing, 47(7), 1-3.
Dykes, P. C., Carroll, D. L., Hurley, A., Lipsitz, S., Benoit, A., Chang, F., ... & Middleton, B.
(2010). Fall prevention in acute care hospitals: a randomized trial. Jama, 304(17), 1912-
1918.
France, D., Slayton, J., Moore, S., Domenico, H., Matthews, J., Steaban, R. L., & Choma, N.
(2017). A Multicomponent Fall Prevention Strategy Reduces Falls at an Academic
Medical Center. Joint Commission Journal On Quality & Patient Safety, 43(9), 460-470.
Morse, J (2009). Preventing Patient Falls: Establishing a Fall Intervention Program, 2nd
Edition. New York: Springer.
Pond, M. (2017). Fall prevention safety bundle: Collaboration leads to fewer falls. American
Nurse Today, 12(7), 25-26