cardiostim 2016 late breaking clinical trial … · cardiostim 2016 late breaking clinical trial...
TRANSCRIPT
CARDIOSTIM 2016 LATE BREAKING CLINICAL TRIAL
FIRE AND ICE℠ AF Ablation Clinical Trial
Secondary Analyses: Reintervention, Rehospitalization, and Quality-of-Life Outcomes
INTRODUCTION
FIRE AND ICE is the largest randomized trial demonstrating non-inferiority of cryoballoon vs. radiofrequency ablation1
Current analysis examines secondary parameters important in a comprehensive clinically meaningful evaluation
Published studies have reported:
Nearly 40% hospitalization rates <1 year post-AF ablation2,3
AF-related readmission rates as high as 22%2,3
Approximately 10% of patients have a repeat ablation <1 year2,3,4
1. Kuck, et al. N Engl J Med 2016 [Epub ahead of print]. 2. Shah, et al. J AM Coll Cardiol. 2012; 59: 143-149. 3. Opolski, et al. Cardiol J. 2015: 22(6): 630-636. 4. Calkins, et al. Europace. 2012; 14:528-606.
FIREANDICE AF Ablation Clinical Trial

OBJECTIVES Evaluate clinical patient management after PVI by either:
Cryoablation (Arctic Front™ / Arctic Front Advance™ catheters) guided by fluoroscopy (or)
RFC ablation (THERMOCOOL® / THERMOCOOL® SF / THERMOCOOL
SMARTTOUCH® catheters) guided by fluoroscopy and CARTO® 3D mapping system
Secondary analyses:
Cardiovascular hospitalization* (including AF hospitalization†)
Repeat ablation*
Quality-of-life*
All-cause hospitalization
Direct current cardioversion (DCCV)
* Predefined secondary analyses † Not predefined but included in analyses
FIREANDICE AF Ablation Clinical Trial
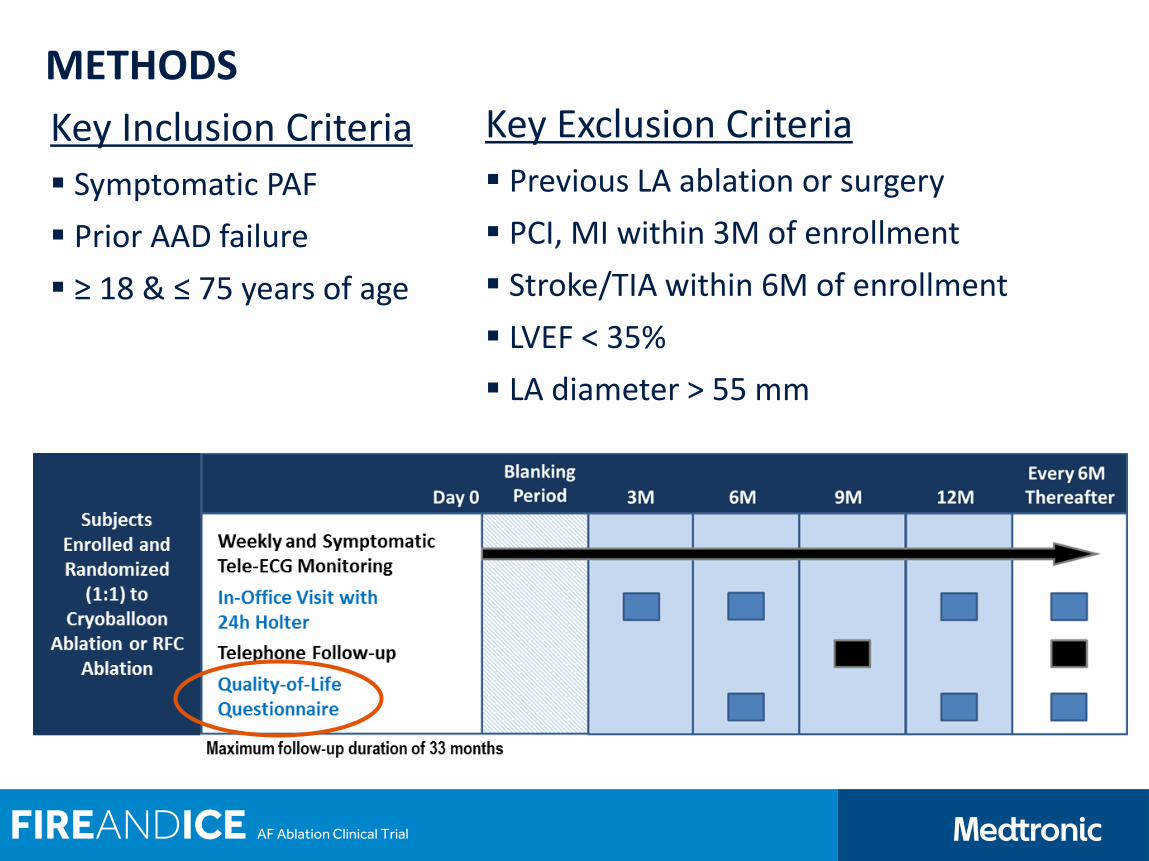
METHODS
Key Inclusion Criteria
Symptomatic PAF
Prior AAD failure
≥ 18 & ≤ 75 years of age
Key Exclusion Criteria
Previous LA ablation or surgery
PCI, MI within 3M of enrollment
Stroke/TIA within 6M of enrollment
LVEF < 35%
LA diameter > 55 mm
FIREANDICE AF Ablation Clinical Trial
METHODS
Investigators must have documented experience
≥ 50 cases with either technology
PVI-only approach
Sites reported all hospitalizations / reinterventions
Cardiovascular-related, repeat ablations, and DCCVs
Defined as prolonged stay ≥2 nights post-index procedure or in-patient stay not concurrent with index procedure ≥1 calendar day
Quality-of-life assessed every 6 months using SF-12 and EQ-5D-3L
FIREANDICE AF Ablation Clinical Trial

COMMITTEES
Steering Committee Prof. Dr. Karl-Heinz Kuck – PI Hamburg, DE
Prof. Dr. Josep Brugada Barcelona, ES
Dr. Alexander Fürnkranz Frankfurt, DE
Dr. Jean-Paul Albenque Toulouse, FR
Prof. Dr. Claudio Tondo Milan, IT
Prof. Dr. Stuart Pocock London, UK
PD Dr. Kurt Bestehorn Munich, DE
Independent Endpoint Review Committee
Prof. Dr. Thorsten Lewalter – Chairman Munich, DE
Dr. Malte Kuniss Bad Nauheim, DE
Prof. Dr. Lars Lickfett Moenchengladbach, DE
Independent Data & Safety Monitoring Board
Prof. Dr. Hein J. J. Wellens – Chairman Maastricht, NL
Dr. Ricardo Cappato Milano, IT
Dr. David Wyn Davies London, UK
Dr. Jan Tijssen – Statistician Amsterdam, NL
FIREANDICE AF Ablation Clinical Trial
RESULTS

SUBJECT FLOW CHART
FIREANDICE AF Ablation Clinical Trial

DEMOGRAPHICS
Demographics RFC (N=376) Cryoballoon (N=374) P-Value*
Gender (male,%) 236 (63%) 221 (59%) 0.30
Age (years) 60.1 ± 9.2 59.9 ± 9.8 0.83
BMI (kg/m2) 27.8 ± 4.5 28.0 ± 4.7 0.66
CHA2DS2-VASc score (N, %) 0.19**
0 58 (15.5%) 67 (17.8%)
1 108 (28.9%) 109 (29.0%)
2 95 (25.4%) 97 (25.8%)
3 60 (16.0%) 62 (16.5%)
4 40 (10.7%) 33 (8.8%)
5 10 (2.7%) 7 (1.9%)
6 3 (0.8%) 1 (0.3%)
First PAF diagnosis (years) 4.7 ± 5.3 4.6 ± 5.1 0.97
Left atrial dimension (mm) 40.6 ± 5.8 40.8 ± 6.5 0.58
Previous DC cardioversion (N,%) 88 (23.4%) 86 (23.0%) 0.89
Systolic blood pressure (mm Hg) 134.8 ± 18.9 133.6 ± 18.0 0.40
Diastolic blood pressure (mm Hg) 78.9 ± 10.6 78.8 ± 11.5 0.83
* t-test for continuous variables, Fisher ’s exact test for dichotomous ** Cochran-Mantel-Haenszel statistics
FIREANDICE AF Ablation Clinical Trial
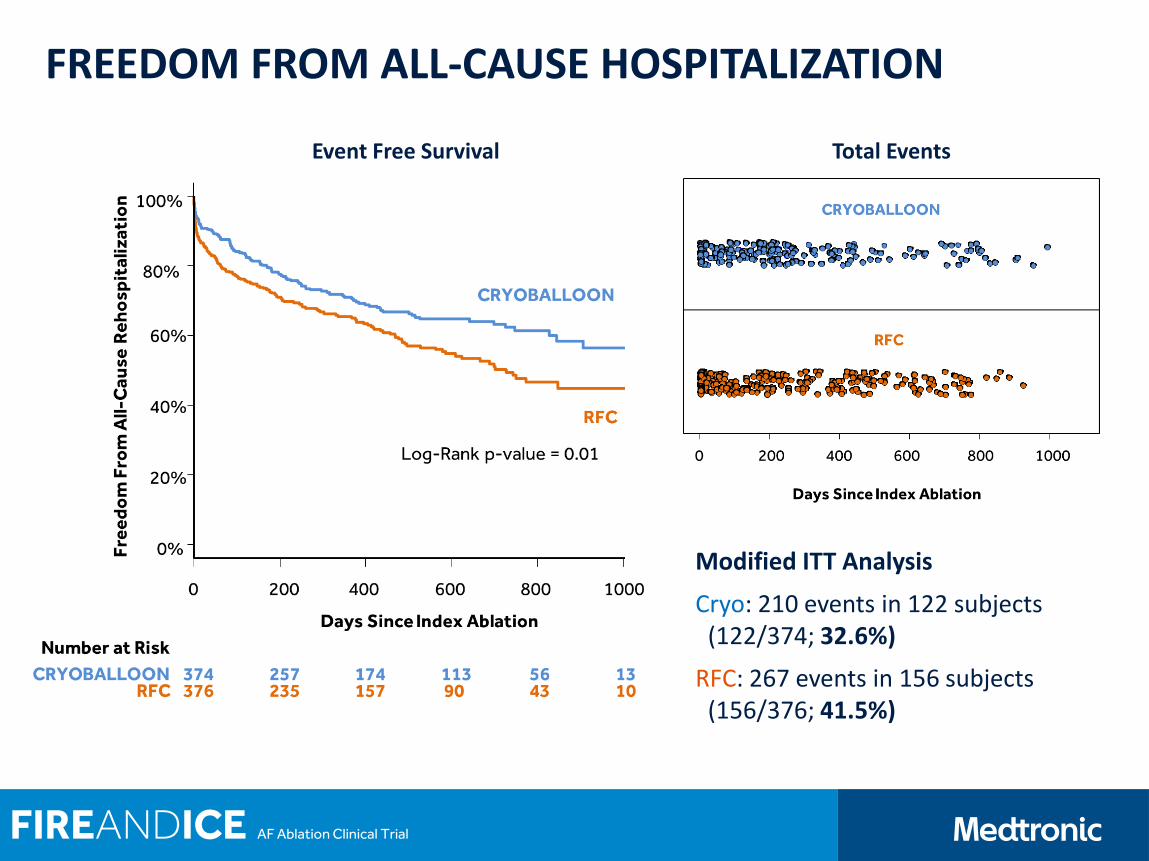
FREEDOM FROM ALL-CAUSE HOSPITALIZATION
Modified ITT Analysis
Cryo: 210 events in 122 subjects (122/374; 32.6%)
RFC: 267 events in 156 subjects (156/376; 41.5%)
Event Free Survival Total Events
FIREANDICE AF Ablation Clinical Trial

FREEDOM FROM CARDIOVASCULAR HOSPITALIZATION
Modified ITT Analysis
Cryo:139 events in 89 subjects (89/374; 23.8%)
RFC:203 events in 135 subjects (135/376; 35.9%)
Event Free Survival Total Events
FIREANDICE AF Ablation Clinical Trial
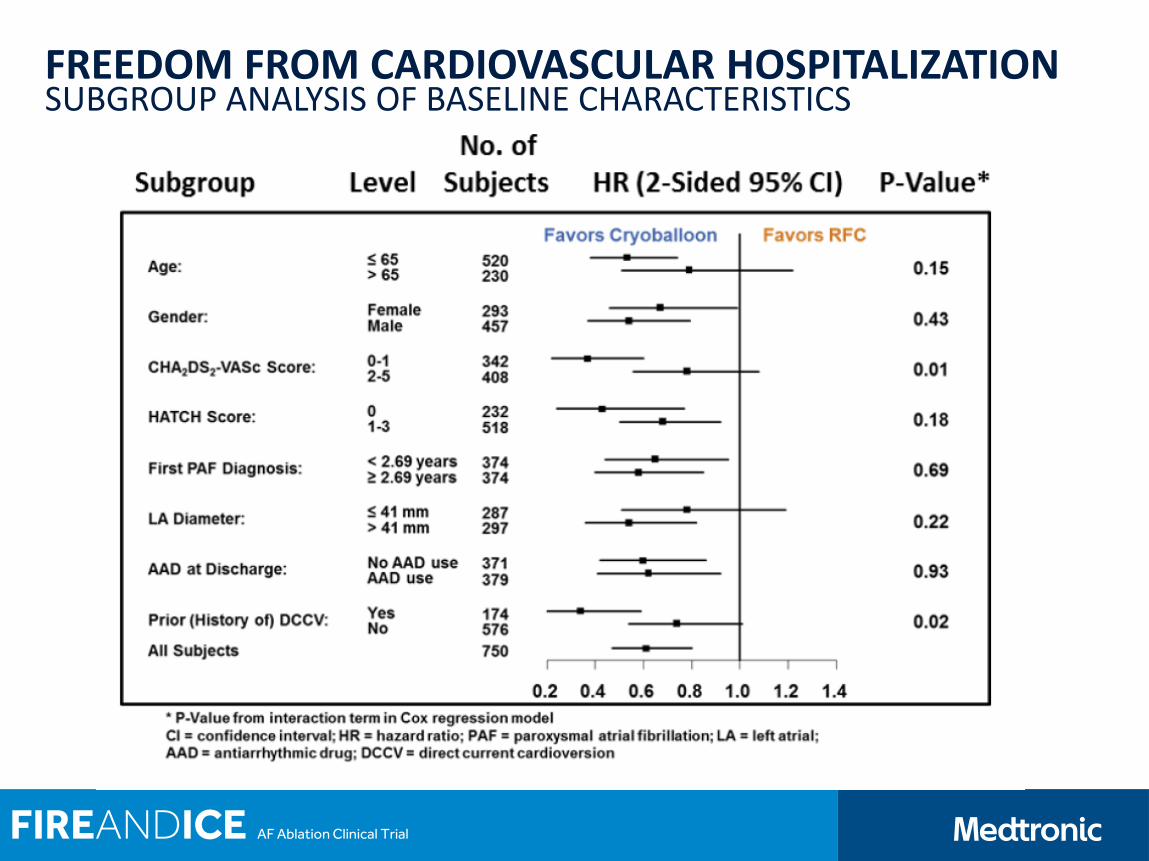
FREEDOM FROM CARDIOVASCULAR HOSPITALIZATION SUBGROUP ANALYSIS OF BASELINE CHARACTERISTICS
FIREANDICE AF Ablation Clinical Trial
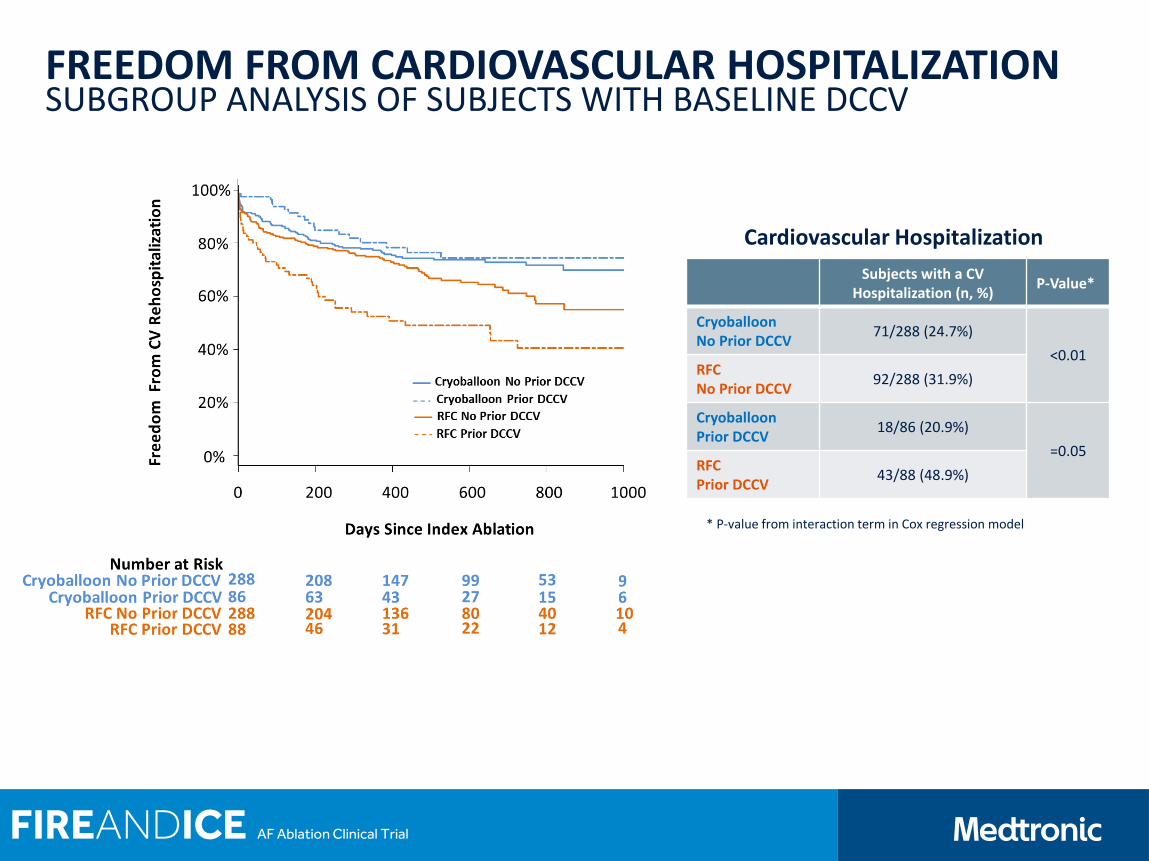
FREEDOM FROM CARDIOVASCULAR HOSPITALIZATION SUBGROUP ANALYSIS OF SUBJECTS WITH BASELINE DCCV
Subjects with a CV Hospitalization (n, %)
P-Value*
Cryoballoon No Prior DCCV
71/288 (24.7%)
<0.01 RFC No Prior DCCV
92/288 (31.9%)
Cryoballoon Prior DCCV
18/86 (20.9%)
=0.05 RFC Prior DCCV
43/88 (48.9%)
Cardiovascular Hospitalization
* P-value from interaction term in Cox regression model
FIREANDICE AF Ablation Clinical Trial
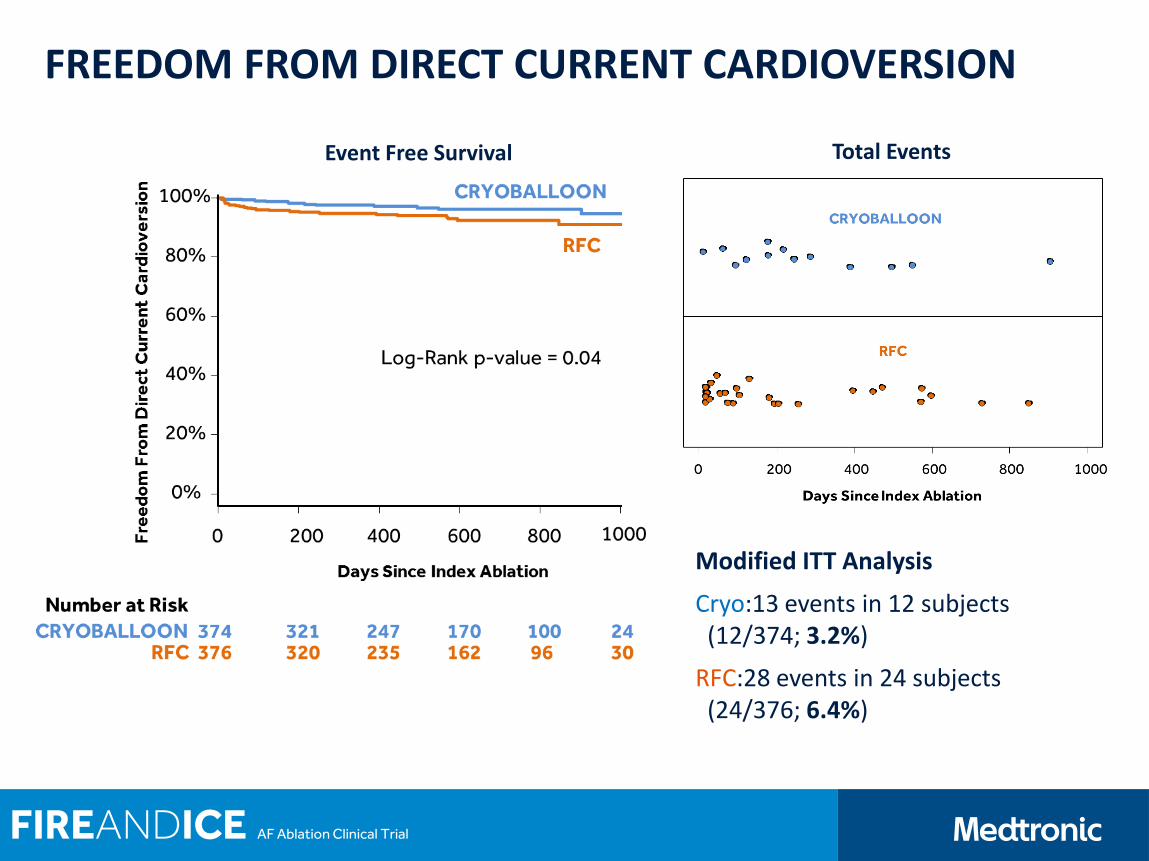
FREEDOM FROM DIRECT CURRENT CARDIOVERSION
Modified ITT Analysis
Cryo:13 events in 12 subjects (12/374; 3.2%)
RFC:28 events in 24 subjects (24/376; 6.4%)
Event Free Survival Total Events
FIREANDICE AF Ablation Clinical Trial
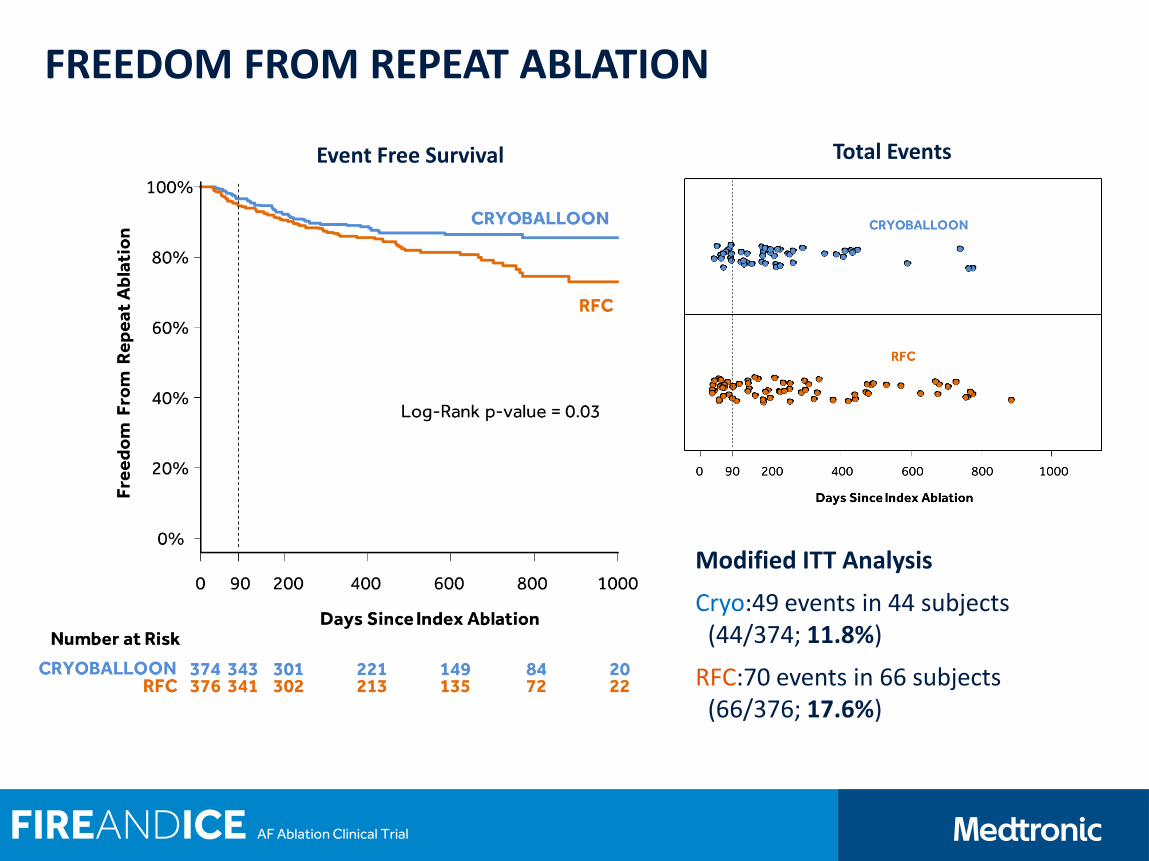
FREEDOM FROM REPEAT ABLATION
Modified ITT Analysis
Cryo:49 events in 44 subjects (44/374; 11.8%)
RFC:70 events in 66 subjects (66/376; 17.6%)
Event Free Survival Total Events
FIREANDICE AF Ablation Clinical Trial
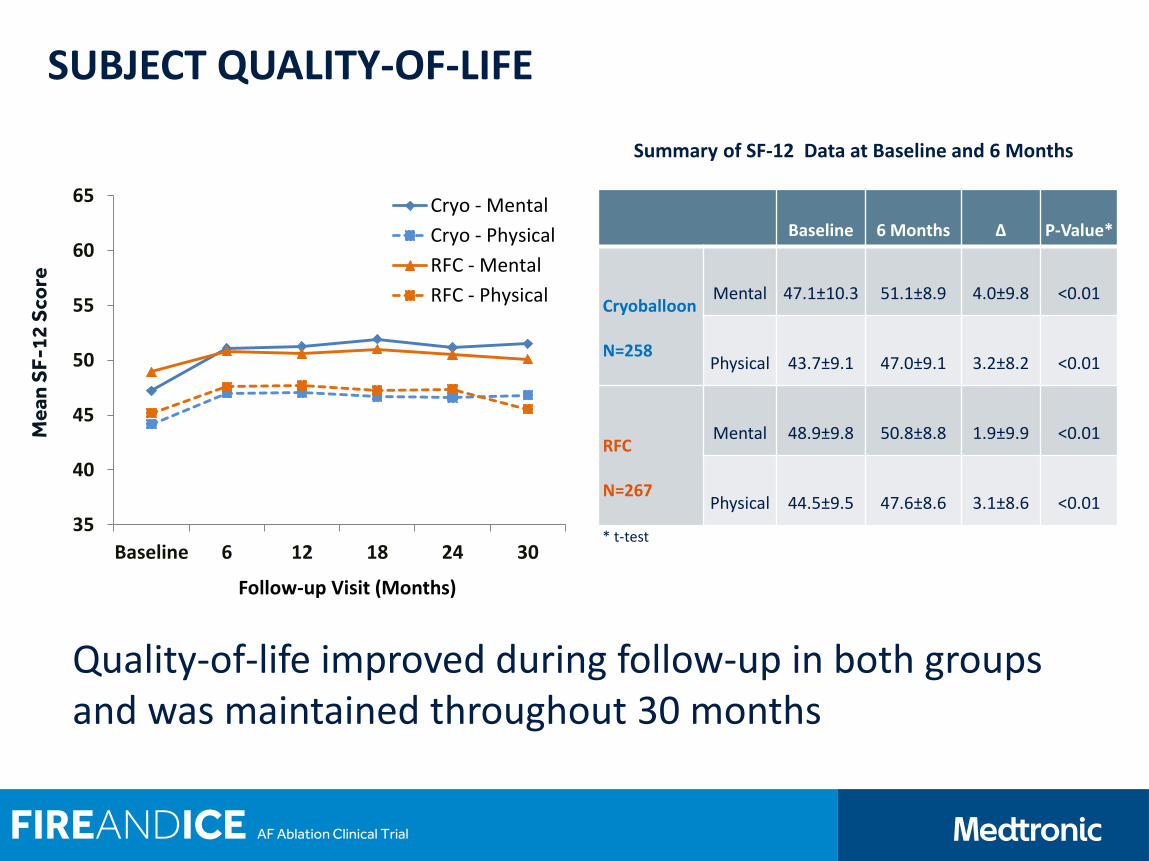
SUBJECT QUALITY-OF-LIFE
Summary of SF-12 Data at Baseline and 6 Months
Quality-of-life improved during follow-up in both groups and was maintained throughout 30 months
Baseline 6 Months ∆ P-Value*
Cryoballoon
N=258
Mental 47.1±10.3 51.1±8.9 4.0±9.8 <0.01
Physical 43.7±9.1 47.0±9.1 3.2±8.2 <0.01
RFC
N=267
Mental 48.9±9.8 50.8±8.8 1.9±9.9 <0.01
Physical 44.5±9.5 47.6±8.6 3.1±8.6 <0.01 35
40
45
50
55
60
65
Baseline 6 12 18 24 30
Follow-up Visit (Months)
Cryo - Mental
Cryo - Physical
RFC - Mental
RFC - Physical
Me
an
SF
-12
Sco
re
* t-test
FIREANDICE AF Ablation Clinical Trial

FIREANDICE AF Ablation Clinical Trial
CONCLUSIONS
Subjects treated with cryoballoon compared to RFC had significantly fewer:
Cardiovascular hospitalizations*
Includes AF hospitalizations† (218/342, 63.7%)
Repeat ablations*
All-cause hospitalizations
Direct current cardioversions
Both patient groups demonstrated improved quality-of-life scores after an AF ablation*
The secondary analyses favor cryoballoon over RFC, with important implications on daily clinical practice
* Predefined secondary analyses † Not predefined but included in analyses
BACK UP

PARTICIPATING SITES Investigator Center Country
Prof. Dr. Karl-Heinz Kuck Asklepios Klinik St. Georg, Hamburg Germany
Dr. Julian Chun Cardioangiologisches Centrum Bethanien CCB, Frankfurt Germany
Dr. Arif Elvan Isala Klinieken, Zwolle The Netherlands
Prof. Dr. Thomas Arentz Krozingen University Heart Center Freiburg, Bad Krozingen Germany
PD Dr. Michael Kühne Universitätsspital, Basel Switzerland
Dr. Laszlo Gellér Semmelweis Egyetem, Budapest Hungary
Dr. Matthias Busch Universitaetsmedizin, Greifswald Germany
Dr. Lluis Mont Hospital Clinic de Barcelona, Barcelona Spain
Dr. Alberto Barrera Hospital Clínico Universitario “Virgen de la Victoria”, Malaga Spain
PD Dr. Thomas Deneke Herz-und Gefaess-Klinik, Bad Neustadt Germany
Dr. Jean-Paul Albenque Clinique Pasteur, Toulouse France
Prof. Dr. Volker Kühlkamp Herz-Zentrum Bodensee, Konstanz Germany
Prof. Dr. Claudio Tondo Centro Cardiologico Monzino University of Milan, Milan Italy
Dr. Ricardo Ruiz-Granell Hospital Clinico Universitario, Valencia Spain
Prof. Petr Neuzil Na Homolce Hospital, Prague Czech Republic
Dr. Nicasio Pérez-Castellano Hospital Clinico San Carlos, Madrid Spain
FIREANDICE AF Ablation Clinical Trial