cardiopulmonary arrest
DESCRIPTION
Kardiologi dan kedokteran vaskulerTRANSCRIPT
CARDIOPULMONARY ARREST
Background Every year in US, more than 250.000 person died suddenly
because of a cardiovascular disease Evaluation and effective treatment for patients at risk of cardiac
arrest requires an understanding of Pathomecanism of cardiac arrest so that the strategy in primary prevention as well as the techniques and modalities of treatment in secondary prevention can be prepared to obtain better results.
Cardiac arrest cases may rarely / not always available every day as a healthcare practitioner. But every member of a health practitioner must master and competent in performing basic life support for cardiac arrest which is a Life-Threatening case.
DefenitionCardiopulmonarry arrest is an Abrupt cessation of
cardiac mechanical function, which may be reversible with prompt intervention but will lead to death in its absence
Rare spontaneous reversions; the likelihood of successful intervention is related to the mechanism of arrest, clinical setting, and prompt return of circulation
Epidemiology In the US and Canada,approximately 350 000 people/year
(approximately half of them in-hospital) suffer a cardiac arrest and receive attempted resuscitation.
In the US and Canada, Cardiac arrest case is about 50 to 55/100 000 persons/year and approximately 25% of these present with pulseless ventricular arrhythmias.
The vast majority of cardiac arrest victims are adults, but thousands of infants and children suffer either an in-hospital or out-of-hospital cardiac arrest each year in the US and Canada
Anatomy and Physiology
The heart is a muscular organ located in the chest cavity, behind the sternum, in mediastinum, between the two lungs, and in front of the spine. Heart is located in this area such as the shape of an inverted triangle
Heart consist of 4 rooms that is Right and Left Atrium, also right and left ventricle.
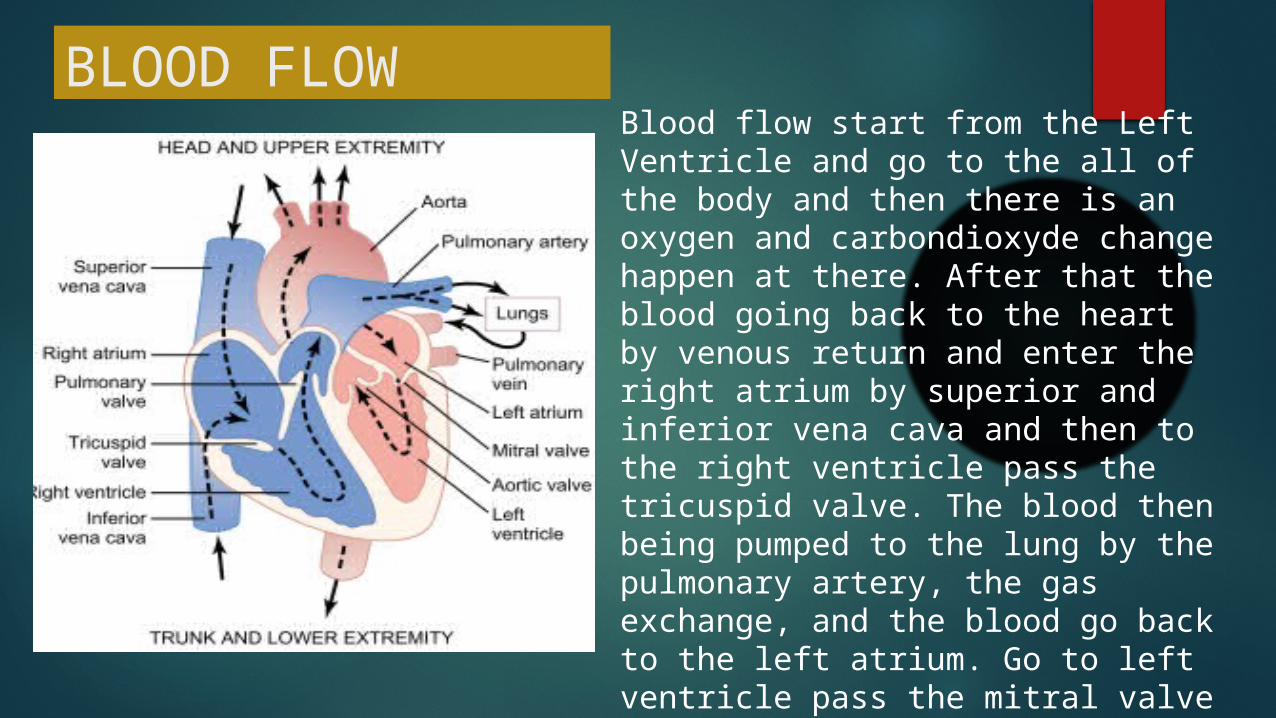
BLOOD FLOWBlood flow start from the Left Ventricle and go to the all of the body and then there is an oxygen and carbondioxyde change happen at there. After that the blood going back to the heart by venous return and enter the right atrium by superior and inferior vena cava and then to the right ventricle pass the tricuspid valve. The blood then being pumped to the lung by the pulmonary artery, the gas exchange, and the blood go back to the left atrium. Go to left ventricle pass the mitral valve and is pumped to all of the body again.
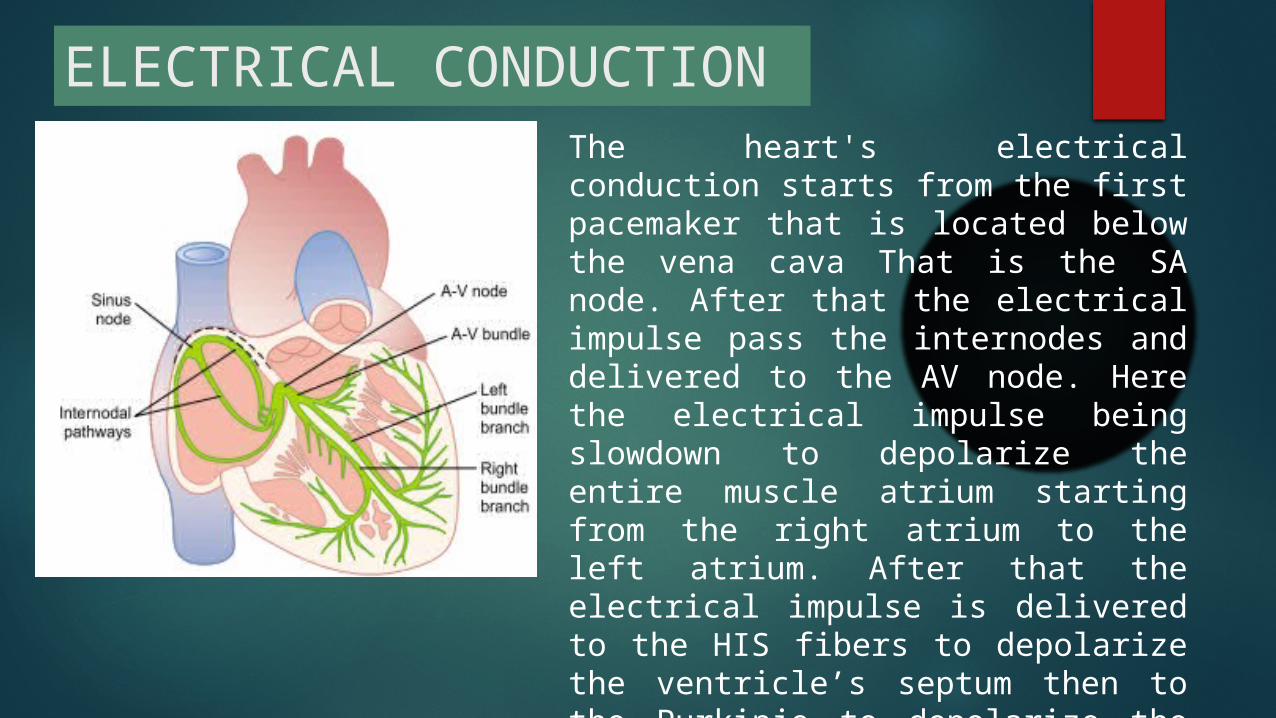
The heart's electrical conduction starts from the first pacemaker that is located below the vena cava That is the SA node. After that the electrical impulse pass the internodes and delivered to the AV node. Here the electrical impulse being slowdown to depolarize the entire muscle atrium starting from the right atrium to the left atrium. After that the electrical impulse is delivered to the HIS fibers to depolarize the ventricle’s septum then to the Purkinje to depolarize the entire wall of the left and right ventricle.
ELECTRICAL CONDUCTION
EtiologyThe loss of function of the heart in cardiac arrest can be caused by conditions such as :1. Coronary Artery Abnormalities2. Ventricular Hypertrophy and Hypertrophic
Cardiomyopathy3. Nonischemic Cardiomyopathy4. Acute Heart Failure5. Electrophysiology abnormality (Short and Long QT
Syndrome, Brugada Syndrome)6. Other Cardiac disease (Valvular Heart Disease, And
Congenital Heart disease)
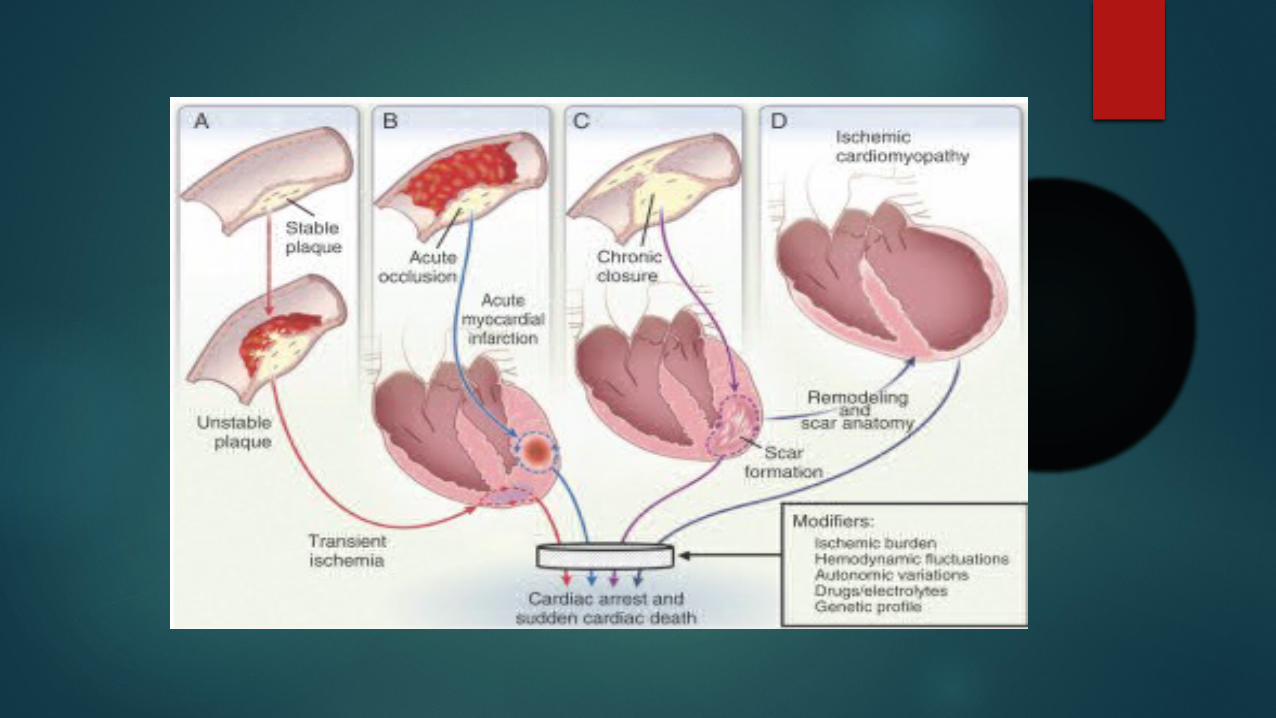
Coronary Artery AbnormalitiesIs the most cause (80%) of the cardiac arrest and
can be happened because of :- Atherosclerotic Coronary Artery Disease
Myocardial Infarc or ischaemic can make a ventricle Fibrilation.- Nonatherosclerotic Coronary Artery Abnormalities
Such as Embolism to the Coronary Arteries, Coronary Arteritis, and Coronary artery spasm.
Nonischemic CardiomyopathyIs 10% of the most cause of the cardiac arrest. This disease can cause an arrhythmia of the heart like monomorphic or polymorphic tachycardia ventricle which can make an cardiac arrest and sudden death
PathophysiologyAll of the etiology will make an abnormal electrical conduction, that is :1. Ventricle Fibrillation2. Pulseless ventricular tachycardia3. Pulseless electrical activity (PEA)4. Asystole
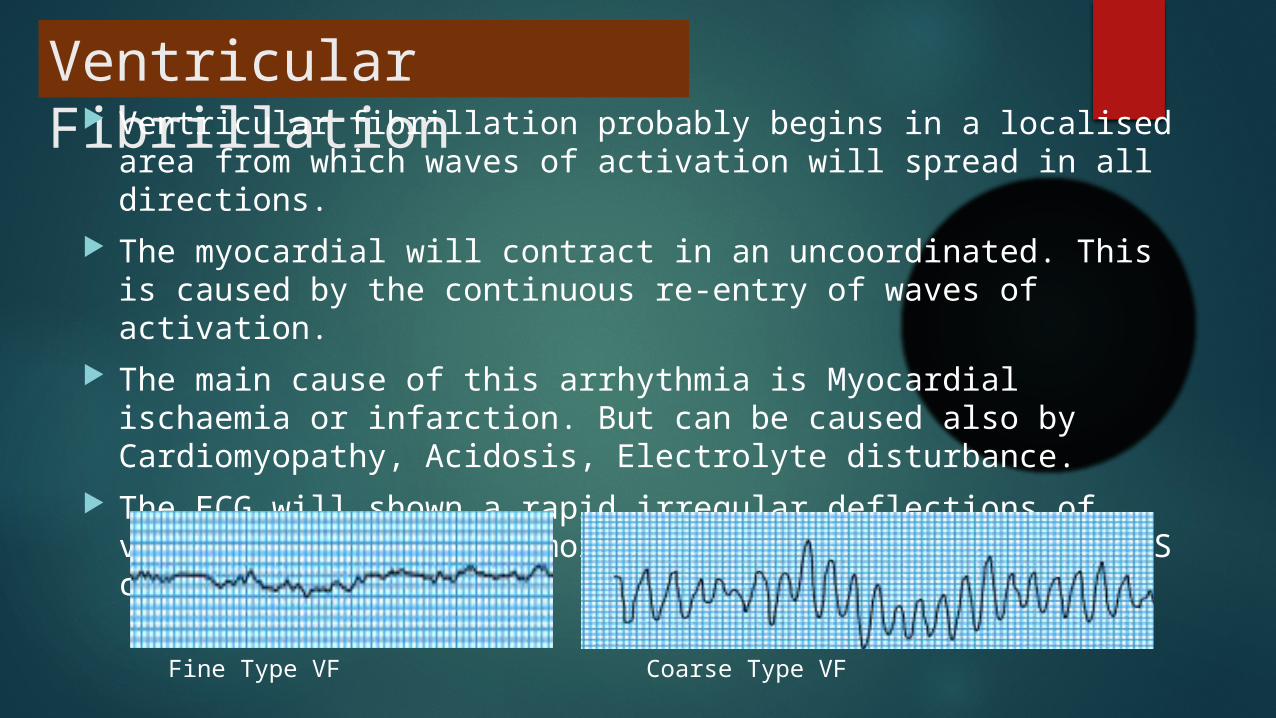
Ventricular Fibrillation Ventricular fibrillation probably begins in a localised area from
which waves of activation will spread in all directions. The myocardial will contract in an uncoordinated. This is caused
by the continuous re-entry of waves of activation. The main cause of this arrhythmia is Myocardial ischaemia or
infarction. But can be caused also by Cardiomyopathy, Acidosis, Electrolyte disturbance.
The ECG will shown a rapid irregular deflections of varying amplitude and morphology and no discernible QRS complexes
Fine Type VF Coarse Type VF
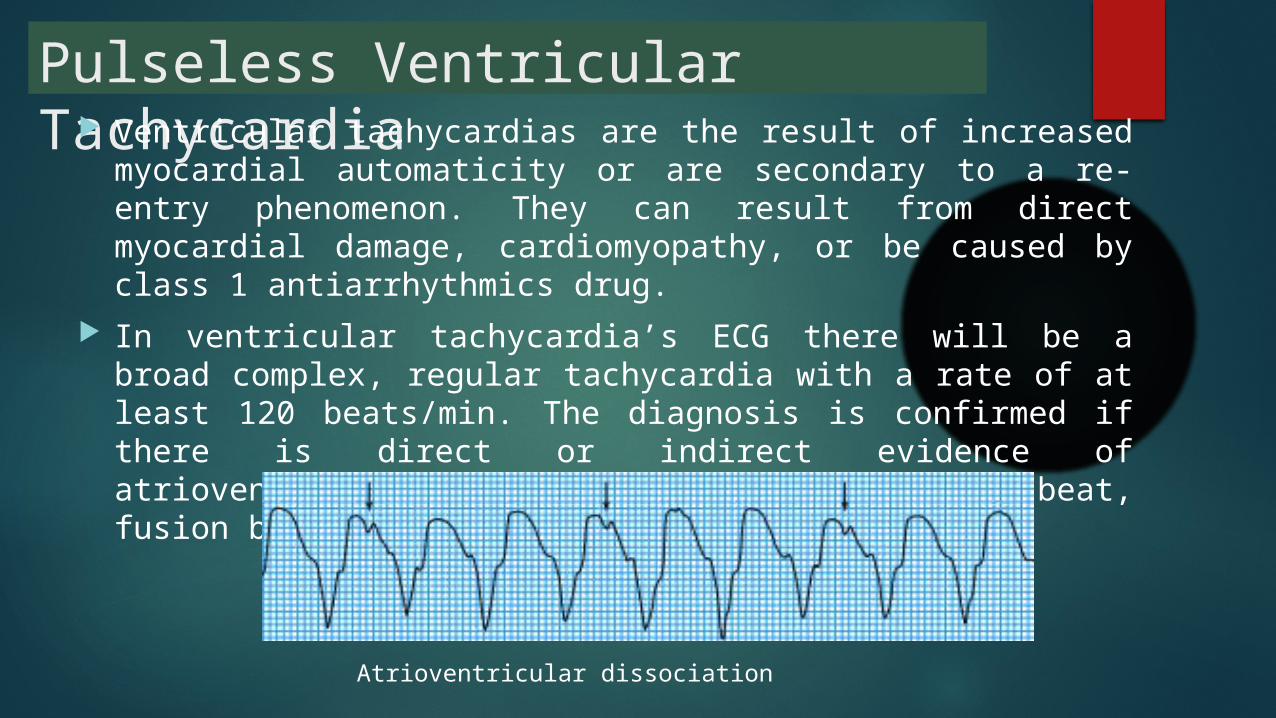
Pulseless Ventricular Tachycardia Ventricular tachycardias are the result of increased myocardial
automaticity or are secondary to a re-entry phenomenon. They can result from direct myocardial damage, cardiomyopathy, or be caused by class 1 antiarrhythmics drug.
In ventricular tachycardia’s ECG there will be a broad complex, regular tachycardia with a rate of at least 120 beats/min. The diagnosis is confirmed if there is direct or indirect evidence of atrioventricular dissociation, such as capture beat, fusion beat, or independent P wave activity.
Atrioventricular dissociation
Pulseless electrical activity In pulseless electrical activity the heart continues to
work electrically but fails to provide a cardiac output sufficient to produce a palpable pulse.
The other cause of PEA are Hypovolaemia, Cardiac tamponade.
The appearance of the electrocardiogram varies, but several common patterns exist.
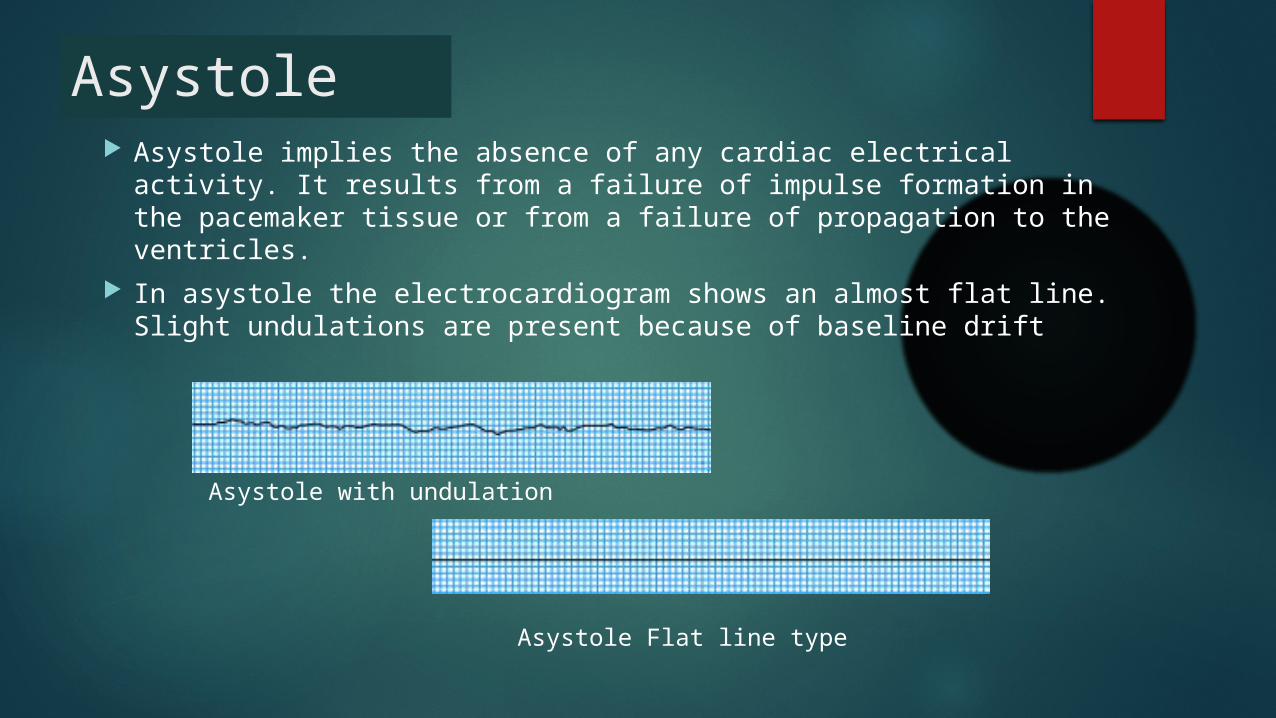
Asystole Asystole implies the absence of any cardiac electrical activity.
It results from a failure of impulse formation in the pacemaker tissue or from a failure of propagation to the ventricles.
In asystole the electrocardiogram shows an almost flat line. Slight undulations are present because of baseline drift
Asystole Flat line type
Asystole with undulation
TreatmentThe Principal of cardiac arrest treatment is doing a CHAIN OF SURVIVAL which is consist by :1. Early recognition and activation actually an cardiac arrest patient is
unresponsive, no breathing or no normal breating (only gasp), and no pulse.
2. Early CPR3. Early defibrillation if there an AED, better we use it than doing CPR (in
Hospital cardiac arrest case) but just For VF and Pulseless VT, not for asystole or PEA
4. Effective advanced life support5. Integration of post-cardiac arrest care
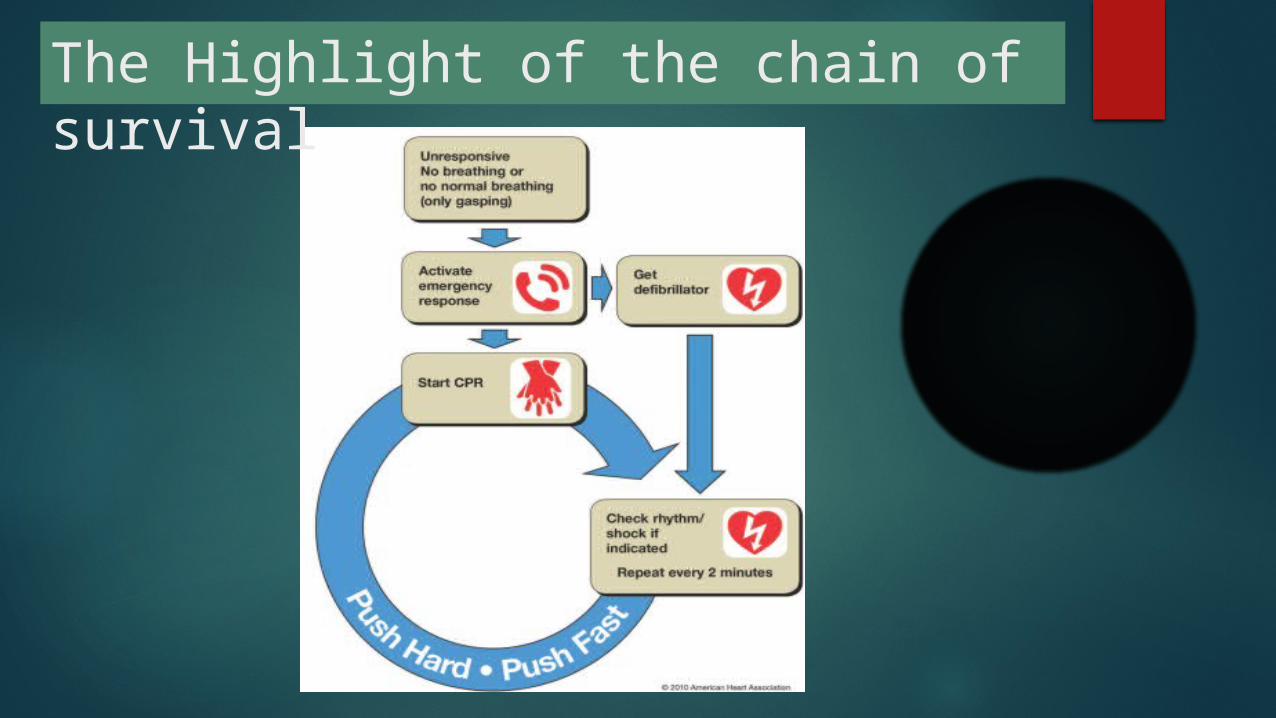
The Highlight of the chain of survival
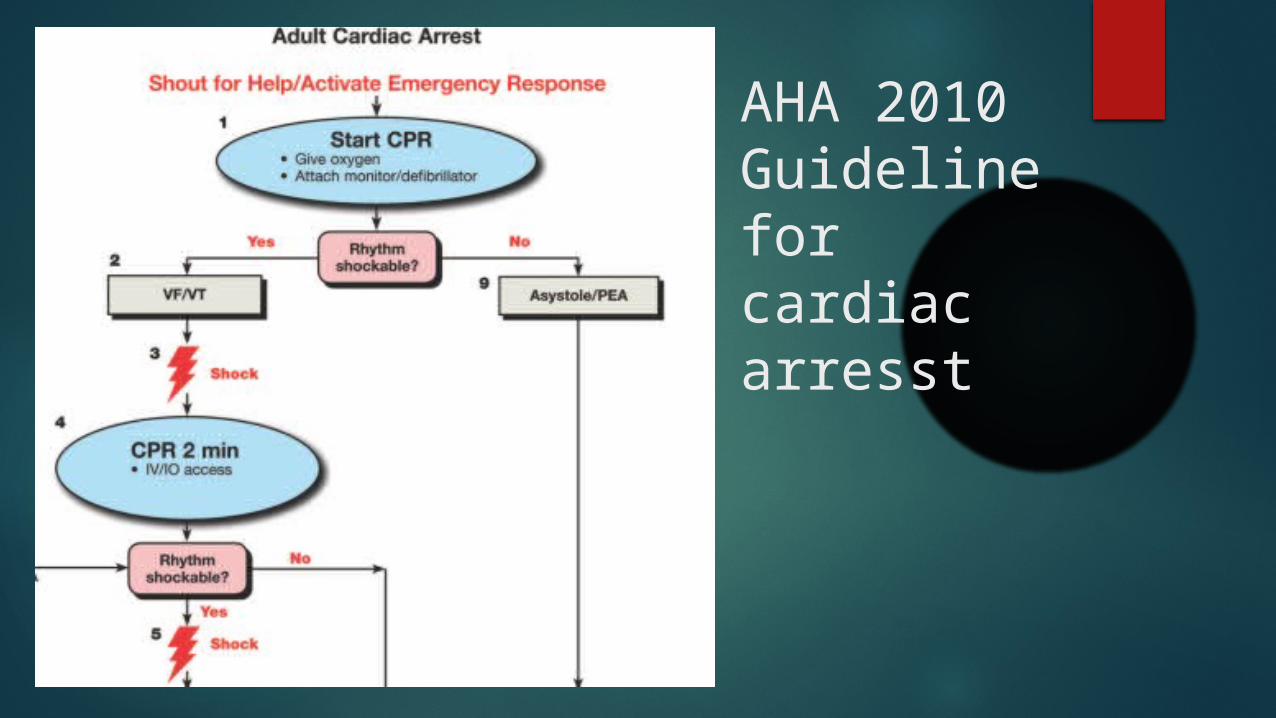
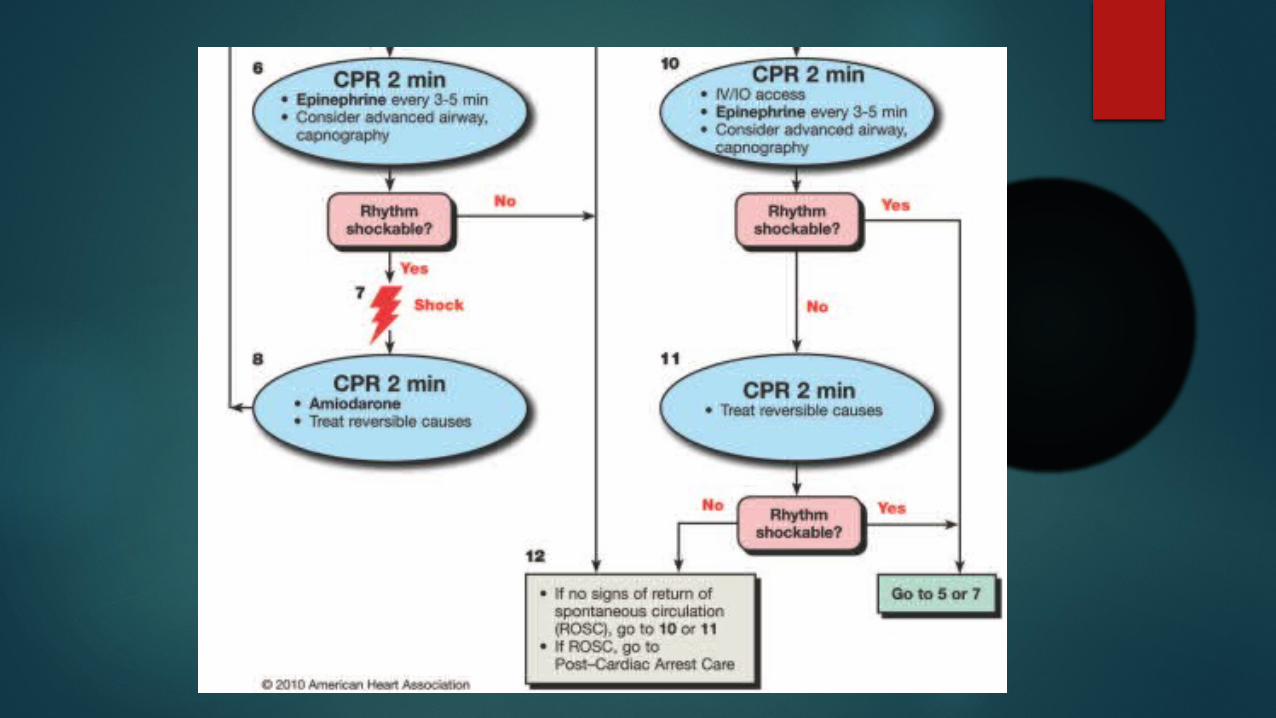
AHA 2010 Guideline for cardiac arresst
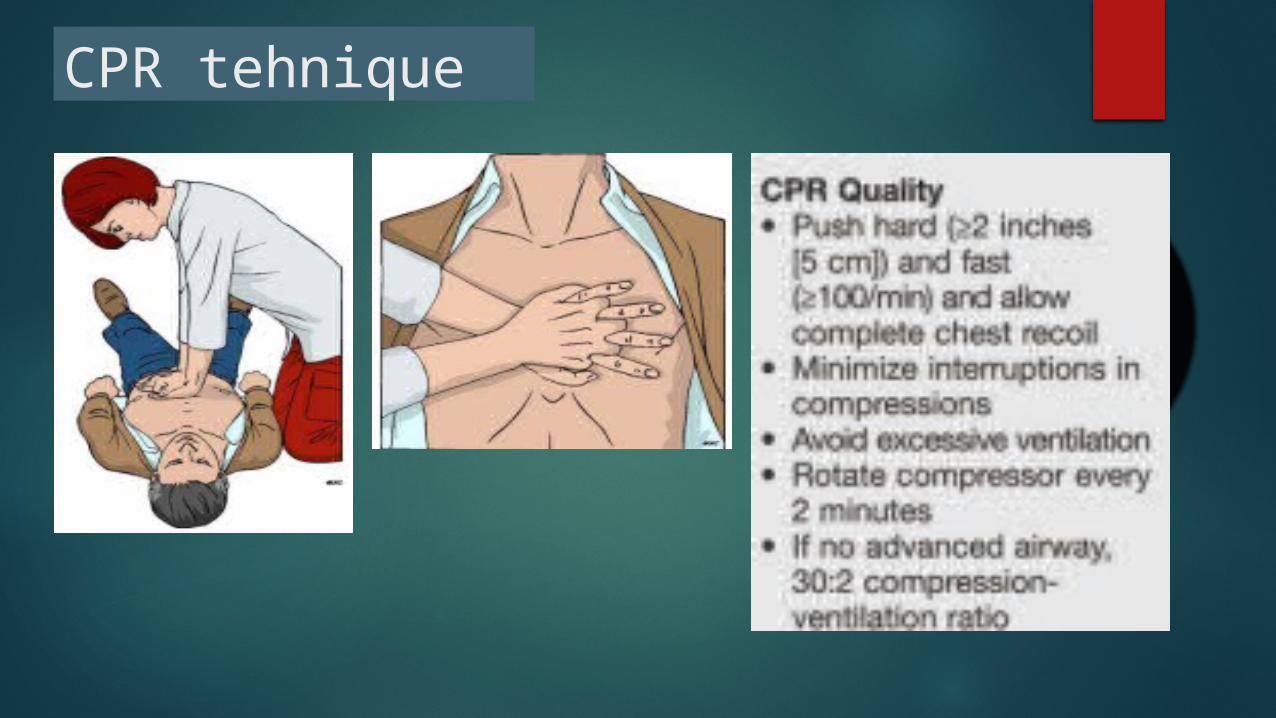
CPR tehnique
Prognosis The Result is based from how fast we recognize and how fast
we do CPR. This is because of 3 phase that happen in Cardiac arrest (example VF)
1. Phase 1 (electric phase) start from VF appear until 5 minutes after the cardiac arrest. This is the best phase we do Defibrilation
2. Phase 2 (Circulating and Haemodynamic phase) 5 – 15 minutes after cardiac arrest. CPR is the best method than the defibrillation
3. Phase 3 (metabolic Phase) more than 15 minutes the effectiveness of CPR and defibrillation is decreased.