cardiac system - nursinged.com · disorders of the cardiac system angina pectoris ... this includes...
TRANSCRIPT

CardiacSystem
243
d. Primaryfunctionoftheleftsideoftheheartis toreceiveoxygenatedbloodfromthelungs andtopumpthebloodthroughtheaortaintothe systemiccirculation. 2. Bothatriaarethereceivingchambers;both ventriclesaretheejectingchambers. 3. Theatrioventricularseptumseparatestherespective chambers. 4. Therightsideofthehearthasathinnermyocar- diumthantheleftsideandisalowerpressure system. 5. Theleftventricleiscomposedofthickermuscle,is ahigh-pressuresystem,andiscapableofgenerat- ingenoughforcetoejectbloodthroughtheaortic valveandthroughthesystemiccirculation. 6. Pericardium:afibroseroussacthatsurroundsthe heart.E. Cardiacvalves:maintainthedirectionalflowofblood throughtheheartchambers.F. Directionofbloodflowthroughtheheartstructure(see Figure12-1). 1. Fromthevenoussystem,thebloodenterstheright atriumviathesuperiorvenacavaandinferiorvena cava;itthenflowsthroughthetricuspidvalveinto therightventricle;bloodisejectedfromtheright ventriclethroughthepulmonaryvalveintothe pulmonaryartery;thenitgoestothelungsfor oxygenation. 2. Oxygenatedbloodreturnstotheleftatriumviathe pulmonaryveins;itflowsthroughthemitralvalve intotheleftventricle;bloodfromtheleftventricle isejectedthroughtheaorticvalveintotheaortic arch,whereitentersthesystemiccirculation. 3. Thepulmonaryarteryistheonlyarteryinthecir- culatorysystemtocarryunoxygenatedblood;the pulmonaryveinistheonlyveininthecirculatory systemtocarryoxygenatedblood.G. Cardiacfunction. 1. Onecompletecardiaccycleconsistsofcontraction ofthemyocardium(systole)andsubsequentre laxationofthemyocardium(diastole). 2. Theamountofbloodejectedfromtheventriclesis thestrokevolume. 3. Theheartpumpsapproximately5Lofbloodevery minute. 4. Theheartrateincreaseswithexercise;therefore cardiacoutputincreases.
PHYSIOLOGYOFTHECARDIACSYSTEMA. Theheartislocatedinthemediastinalspaceofthe thoraciccavity.B. Theapexoftheheartpointsdownwardandtotheleft; theapexcontactsthechestwallataboutthefifthto sixthintercostalspace;inthenormalindividual,the pointofmaximumimpulse(PMI)maybepalpated here;thisisalsotheareatoauscultateandevaluate theapicalheartrate.C. Myocardialwall. 1. Epicardium:theoutersurface. 2. Myocardium:themiddlelayerofcardiacmuscle. 3. Endocardium:theliningoftheinnersurfaceofthe cardiacchambers.D. Cardiacchambers(Figure12-1). 1. Fourchambersarelocatedwithintheheart;these chambersrepresenttwopumps. a. Right-sidepump:therightatriumandright ventricle,separatedbythetricuspidvalve. b. Primaryfunctionoftherightsideoftheheartis toreceivevenousbloodreturnfromthevascular systemandtopumpbloodthroughthelungs. c. Left-sidepump:leftatriumandleftventricle, separatedbythemitralvalve.
FIGURE 12-1 Heart structures and path of oxygenatedbloodthroughtheheart. (From deWit, S: Medical-surgical nursing: Concepts and practices, ed 7, St Louis, 2009, Saunders).

244 CHAPTER12 CardiacSystem
5. Thecardiacoutputwillvaryaccordingtothe amountofvenousreturn(preload).H. Myocardialbloodflow. 1. Coronaryarteriessupplytheheartmusclewithoxy genatedblood. 2. Collateralcirculation. a. Thereare3maincoronaryarteriesthatbranch fromtheaortaandsupplyoxygenatedbloodto thecardiacmuscle. b. Withagradualocclusionofthelargecoronary arteriesbyatheroscleroticheartdisease(ASHD), thesmallervesselsincreaseinsizeandbranch outtoprovidealternativesourcesofbloodflow (collateralcirculation). c. Becauseofthedevelopmentofthecollateral circulation,coronaryarterydisease(CAD)may bewell-advancedbeforetheclientexperiences symptoms.I. ConductionSystem(Appendix12-4)
System Data CollectionA. Healthhistory. 1. Identifypresenceofriskfactorsforthedevelopment ofarterioscleroticdisease(Box12-1). 2. Respiratorysystem. a. Historyofdifficultybreathing. b. Medicationstakenforrespiratoryproblems. c. Determinenormalactivitylevel. 3. Circulatorysystem. a. Historyofchestdiscomfort. b. Historyofedema,weightgain. c. Historyofsyncope. d. Medicationstakenfortheheartorforhighblood pressure.
TEST ALERT: Teach health promotion information. Know the risk factors for ASHD
and be able to teach the client how to effectively reduce risk factors.
B. Physicalassessment. 1. Whatistheoverallgeneralappearanceoftheclient? Isthereanyevidenceofdistress?Whatisthelevel oforientationandabilitytothinkclearly? 2. Evaluatebloodpressure. a. Pulsepressure:thedifferencebetweenthe systolicanddiastolicpressures. b. Assessforpostural(orthostatic)hypotension: decreaseinbloodpressurewhentheclient stands. 3. Evaluatecharacterofpulse. a. Rate,baserhythm. b. Regularity,presenceofirregularorectopic beats.
c. Pulsedeficit:thedifferenceintherateofthe pulseattheradiusandattheapex(orapical rate).Ifthereisapulsedifference,theradial pulseratewillbelessthantheapicalpulserate. d. Pulsequality:theamplitudeorqualityofthe pulse;pulsesshouldbeevaluatedbilaterally. (1) +1:thready,weak,rapidpulse. (2) +2:diminishedpulse;cannotbeobliterated. (3) +3:easytopalpate,full;cannotbeobliter- ated. (4) +4:strongboundingpulse;maybeabnormal. e. Palpitations:clientdescribesafeelingorsensa- tionofrapid,bounding,orirregularheartbeat. 4. Assessqualityandpatternofrespirationsandevi- denceofrespiratorydifficulty. 5. Apicalheartrate:listenfortheapicalpulseand counttheapicalrateatthefifthintercostalspace, mid-clavicularline. 6. Evaluateperipheralpulsesandobserveforpresence ofperipheraledema. 7. Weightgain:3ormorepoundsin24hoursrepre- sentsfluidgain. 8. Evaluateforpresenceofchestdiscomfort (Box12-2). a. Location. b. Intensityofpain. c. Precipitatingcauses. 9. Determineclient’sactivitylevel;increasingfatigue withmildexerciseoccurswithclientswithcardiac disease.
Modifi able Risk Factors• Elevatedserumcholesterollevels
• Highbloodpressure
• Cigarettesmoking
• Sedentarylifestyle
• Obesity
• TypeApersonality(high-pressurelifestyle,driving, competitive)
• Diabetesmellitus
nonmodifi able Risk Factors• Geneticpredisposition
• Positivefamilyhistoryofheartdisease
• Increasingage
• Gender:occursmoreofteninmen;increaseinwomen aftermenopause
BoX 12-1 RIsK FACtoRs In ARtERIosCLERotIC HEARt DIsEAsE

CHAPTER12 CardiacSystem 245
A. Pain(angina)occurswhentheoxygendemandsofthe heartmuscleexceedtheabilityofthecoronaryarteries todeliverit.B. Temporaryischemiadoesnotcausepermanentdamage tothemyocardium.Painfrequentlysubsideswhenthe precipitatingfactorisremoved.C. Typesofangina. 1. Chronicstableangina 2. Unstableangina(acutecoronarysyndrome). 3. Newonsetangina–firstsymptomsofanginathat mostfrequentlyoccurafterexertion.
Data CollectionA. Riskfactors/etiology. 1. Arterioscleroticheartdisease(seeChapter11) 2. Cardiacischemia. 3. Increasedcardiacdemands. a. Exercise. b. Emotionalstress. c. Heavymeals.B. Clinicalmanifestations—chronicstableangina. 1. Paininvaryinglevelsofseverity(seeBox12-2). a. Predictablewithlevelofstressorexertion;con- sistentlyrespondswelltonitroglycerine. b. Painrarelyoccursatrest. 2. Painmostoftenislocatedbehindorjusttotheleft ofthesternum. 3. Painmayradiatetoneck,jaw,andshoulders. 4. Clientmaydescribepainassqueezing,choking,or constrictingorasavaguefeelingofpressureand indigestion. 5. Clientwillfrequentlydenyseriousnessofthepain. 6. Mostclientscorrelatepainwithactivityandin- creasedcardiacdemands. 7. Painisofshortduration,generallylastingabout5 minutes. 8. Accompanyingsymptomsmayincludediaphoresis, increasedanxiety,pallor,anddyspnea.C. Nopermanentdamagetomyocardium.D. Diagnostics—chronicstableangina(seeAppendix12-1).
Treatment—Chronic Stable AnginaA. Primarygoaloftreatmentistorelievepainandprevent futureattacks.B. Medication–vasodilators,beta-adrengergiceblockers (Appendix12-2).C. Procedures/surgicalintervention. 1. Percutaneoustransluminalangioplasty(PTA),per- cutaneouscoronaryintervention(PCI):Aballoon ispassedthroughanarteryinthegroinintothe affectedcoronaryarterytotheareaofobstruction. Theballoonisinflatedinanattempttocompress theplaqueintheaffectedareaandre-establish bloodflowtothecardiacmuscle.
DISORDERSOFTHECARDIACSYSTEM
Angina Pectoris (Chronic Angina)
Coronaryarterydisease(CAD)occursasaresultoftheatheroscleroticprocess(seeChapter16)inthecoronaryarteries.Angina pectorisiscausedbymyocardialischemiaduetonarrowedorblockedcoronaryarteries.Thebuildupofplaqueorfattymaterialinthecoronaryarterycausesa narrowing of the lumen of the artery and precipitatesmyocardialischemiathatcauseschestpain.
✽
P:PrecipitatingFactors• Mayoccurwithoutobviouscause
• Physicalexertion
• Emotionalstress
• Eatingalargemeal
• Sexualactivity
Q:Quality• Pressure
• Squeezing
• Heaviness
• Smothering
• Burning
• Severepain
• Increaseswithmovement
R:RegionandRadiation• Substernalorretrosternal
• Spreadsacrossthechest
• Radiatestotheinsideofeitherorbotharms,theneck, jaw,back,upperabdomen
S:SymptomsandSigns(Associatedwith)• Diaphoresis;cold,clammyskin
• Nausea,vomiting
• Dyspnea
• Orthopnea
• Syncope
• Apprehension
• Dysrhythmias
• Palpitations
• Weakness
• Feelingofimpendingdoom
T:TimingandResponsetoTreatment• Suddenonset
• Constant
• Duration
• Responsetorestornitroglycerin
• Reliefwithnarcotics
BoX 12-2 AssEssIng CHEst PAIn-PQRst

246 CHAPTER12 CardiacSystem
2. Atherectomy:acatheteristhreadedintothecoro- naryarteries,thereisarotatingshaveronthe tipthatcutsawaytheplaque. 3. Anintracoronarystentisanexpandablewiremesh thatcanbeinsertedduringanyoftheabovepro cedures.Astentservesasascaffoldtosupportthe coronaryarteryandincreasethebloodflowtothe cardiacmuscle. 4. Cardiacrevascularization:coronaryarterybypass graft(CABG)surgery,openheartsurgery.D. Restrictedactivity.E. Supplementaloxygen.F. Controlofthemodifiableriskfactors(seeBox12-1).
ComplicationsA. Dysrhythmias.B. Myocardialinfarction.
OLDER ADULT PRIORITY: In the older adult client, dyspnea, not angina, may be the presenting symptom of myocardial ischemia.
Nursing Interventions—see acute angina (coronary artery syndrome)
Unstable Angina PectorisUnstable Angina Pectoris (acute coronary syndrome)
Acute coronary syndrome (ACS) accordingtotheAmericanHeart Association, includes degrees of coronary arteryocclusionthatcandevelopwithcoronaryatherosclerosis.Thisincludesunstableanginathatoccurswhenathrombuspartially occludes a coronary artery causing prolongedsymptomsofischemiawhichcanoccuratrest.
AssessmentA. Riskfactors/etiology. 1. Familyhistoryofcoronaryarterydisease. 2. Hypertension,hypercholesterolemia. 3. Diabetes,smoking. 4. AverageageforfirstMI-menover64.5years, womenover70.5years. 5. Womenareatincreasedriskaftermenopause.B. Clinicalmanifestations. 1. Twoormoreepisodesofanginawithin24hours, painoccurswhenclientisatrest. 2. Chestpainlastinglongerthan20minutesandunre- lievedbynitroglycerine. 3. Presentingsymptomsinwomen:indigestion,pain betweentheshoulders,shortnessofbreath,and anxiety. 4. Hypotension,dysrhythmias.C. Diagnostics(Appendix12-1).D. Treatment(initial). 1. Bedrest. 2. Monitorvitalsigns,includingoxygensaturation level.
✔
✽
3.SupplementaloxygentomaintainO2satatorabove
90%. 4. Reducecoronaryreocclusionwithantiplateletmedi- cations.(Appendix12-2) 5. Reduceandcontrolischemicpain:vasodilators (nitroglycerin,narcotics(morphinesulfateIV—if painnotrelievedbythenitroglycerin).
ComplicationsA. Dysrhythmias(seeAppendix12-4).B. Myocardialinfarction(MI).
Nursing Interventions for Angina and Acute Coronary Syndromev Goal:Todecreasepainandincreasemyocardialoxy-genation.A. Maintainbedrest;positionclientinrecliningposition withheadelevated.B. BeginsupplementalO
2.
C. AssesscharacteristicsofpainD. Administermedications. 1. NitroglycerinsublingualIV,orspray(Box12-3; Appendix12-2),evaluateclient’sresponse;pain fromchronicanginaisusuallyrelieved;painfrom acuteanginamaynotberelieved.
1. Keepinatightlyclosed,darkglasscontainer. 2. Carrysupplyatalltimes—eithersublingual(SL)tablets ortranslingualspray;donotswallowsublingualtablets. 3. Freshtablets(sublingual)shouldcauseaslightburning/ tinglingunderthetongue. 4. Dateallopenedcontainersanddiscardallmedication thatis24monthsold. 5. Takenitroglycerinprophylacticallytoavoidpain— beforesexualintercourse,exercise,walking,etc. 6. Takenitroglycerinwhenpainbegins;stopallactivity. 7. Ifpainisnotrelievedin5minutes,call911andactivate EMS. 8. WhilewaitingforEMSresponse,ifchestpaincontinues, takeanotherSLpillor1meteredspray. 9. Remainlyingdown;orthostatichypotensioncanbea problem. 10. Long-actingpreparationsshouldnotbeabruptlydis- continued;thismayprecipitatevasospasm. 11. Todecreasedevelopmentoftoleranceinlong-acting preparations,schedulean8-hournitro-freeperiodeach day,preferableatnight. 12. Donottakeerectiledysfunctiondrugswithnitro- glycerine.
BoX 12-3 CLIEnt EDUCAtIon FoR nItRogLYCERIn ADMInIstRAtIon
TEST ALERT: Instruct clients about self-administration of medications.

CHAPTER12 CardiacSystem 247
2. Narcoticanalgesics(morphine),monitorresponseto smallincrementsofIVmorphineE. Immediatelyreportpresenceofchestpainandorany changesincharacteristicsofchestpain.F. Protectvenousaccess.G. Maintaincalm,reassuringatmosphere.H. Evaluatevitalsigns.I. Do not leave a client alone if they are experiencing chest pain.
TEST ALERT: Check client’s discomfort and pain levels. Evaluate client’s response to inter-
ventions.
v Goal:Toevaluatecharacteristicsofanginalpainandclient’soverallresponse(seeBox12-2).A. Doespainincreasewithbreathing?(Anginalpainis generallynotaffectedbybreathingorchangesin position.)B. Assessactivitytoleranceorprecipitatingfactor.C. Assesscharacteristicsofpain(Box12-2)D. Evaluateresponseofpaintotreatmentandorprogres- siontomoreseverelevel.E. Assessrespiratorystatusandresponsetopain;presence ofdyspnea,orwetbreathsoundsF. Assessforpresenceofirregularheartbeatandtolerance ofdysrhythmias.G. Assessadequacyofcardiacoutput–peripheralpulses, urinaryoutput,levelofconsciousnessH. ContinuousECGmonitoring-assessforpresenceof dysrhythmiaandimpactoncardiacoutput.I. Assessclient’spsychosocialresponse–denialiscom- mon;anger,fearanddepressionoccurinbothclientand family.v Goal:Toprovidecareaftercardiacinterventionaltherapies(e.g.,angioplasty,stentplacement).A. Monitorforchestpainandhypotension.B. Frequentreassessmentofstatusofcirculationdistalto areaofcatheterinsertion.C. Asheathmaybeleftinplace;monitorareaforbleed ing.Ifbleedingoccurs,putmanualpressureonthearea andnotify the RN.D. Preventflexionofaffectedextremityandmaintainbed restfor6to8hours.E. Immediatelyreportanybleeding at site and occurrence of chest pain or syncope.
TEST ALERT: Intervene in response to client’s unexpected response to therapy; document
response, promote recovery.
Home CareA. EducationregardingASHD. 1. Assistclienttoidentifypersonalriskfactorsand appropriatehealthpracticestodecreaseriskfactors.
2. Assistclienttoidentifyfactorsprecipitatingpain.B. Avoidactivitiesthatprecipitatepain(e.g.,largemeals, smoking,exercise,extremesinweather).C. Understandmedication(seeBox12-3andAppendix 12-2),activity,anddietregimen.D. Ifchestpainpersistsandisnotrelievedbymedication, clientshouldcallprimarycareprovider(PCP)orphysi- cianand/orgotoclosestemergencydepartment.E. Adviseclienttonottakeerectiledysfunctiondrugs (Appendix17-1)ifonnitratesforchestpain.
TEST ALERT: Review client/family understand-ing of health promotion behaviors/activities.
Myocardial InfarctionA myocardial infarction (MI, coronary occlusion,
heartattack)isatotalocclusionofaportionofacoronaryartery. Immediately following the occlusion, there ismyocardial ischemia. In the hours following an MI, thetissuebecomesnecrotic.A. Mostcommonsiteofinfarctionistheleftventricle.B. Theseverityoftheeventdependsontheareaofthe heartinvolved,aswellasthesizeoftheartery occluded.C. Thepresenceofpreestablishedcollateralcirculation willassistindecreasingthesizeofthenecroticarea.D. Thepresenceofpre-establishedcollateralcirculation willassistindecreasingthesizeofthenecroticarea.
Data CollectionA. Riskfactors/etiology–seeunstableangina.B. Clinicalmanifestations. 1. Typicalpainissevere,substernal,crushing,and unrelievedbynitroglycerin(seeBox12-2). 2. Frequentlyclientwilldenyseriousnessofthepain. 3. Painmayradiatedownthearmoruptothejaw. 4. Dyspnea,nausea,vomitingandindigestion. 5. Pale,duskyskin,syncope. 6. Onsetisusuallysudden. 7. Diaphoresis;extremeweakness. 8. Decreaseinbloodpressure,tachycardia,syncope. 9. Dysrhythmias:tachycardia,irregularrhythm.C. Diagnostics(Appendix12-1).
NURSING PRIORITY: Danger of death from an MI is greatest during the first 2 hours.
D. Complications 1. Dysrhythmias(seeAppendix12-4). 2. Cardiogenicshock. 3. Heartfailure,(congestiveheartfailure).
✽
✔

248 CHAPTER12 CardiacSystem
TreatmentA. Reperfusion(fibrinolytic)therapy:mosteffectiveif administeredimmediatelyorwithinthefirst3to6 hoursaftertheMI.B. Supplementaloxygen4L/minvianasalcannula(main- tainO
2satabove90%).
C. BedrestD. Maintainintravenous(IV)lineformedications.E. Paincontrol:mostoftenmorphine;painincreasescar- diacworkload.F. Medications(seeAppendix12-2).G. Dietaryrestrictions. 1. Progresstodietastolerated:lowsodiumandlow cholesterol. 2. Decreaseintakeofstimulants(e.g.,coffee,tea).H. Percutaneouscoronaryintervention(PCI).I. Openheartsurgeryformyocardialrevascularization.
Nursing Interventionsv Goal:Todecreasepainandincreasemyocardialoxy-genation(seepreviousrelatedgoalforanginapectoris).
NURSING PRIORITY: As long as a client is experiencing chest pain myocardial ischemia is present. If client experiences tachycardia, decrease activity whether client has chest pain or not.
v Goal:Toevaluatecharacteristicsofcardiacpainandclient’soverallresponse(seepreviousrelatedgoalforanginapectoris).v Goal:Tomaintainhomeostasisanddecreaseeffects ofMI.A. MaintainIVaccess;reportinfiltrationorphlebitisat site.B. Maintainbedrestinitially.C. Evaluateurinaryoutputandrenalresponsetochanges incirculation.D. Continuouscardiacmonitoring,assesscardiacrateand rhythm;dysrhythmiasaremajorcauseofdeathafter anMI.E. Assessrespiratorysystemforincreasingdyspneaand pulmonarycongestion.F. Evaluateperipheralcirculation;assessforpresenceof dependentedema.G. Frequentassessmentofvitalsigns;evaluateurinary outputinresponsetochangesinvitalsigns.H. Frequentassessmentforpresenceofchestpain.
TEST ALERT: Meet client’s pain management needs; provide medication for pain relief; moni-tor for effects of pain medication.
✔
I. MaintainNPOinitially;thenallowclearliquidsand progresstolightmealsthatarelowinsodiumandcho- lesterol.J. Promotenormalbowelpattern. 1. Stoolsofteners. 2. Bedsidecommode. 3. Cautionagainststrainingwhiledefecating(Valsalva maneuver). 4. IncreasefiberindietK. Decreaseanxiety. 1. Administerpainmedicationpromptly. 2. Keepclientinformedregardingprogressandimme- diateplanofcare. 3. Decreasesensoryoverload. 4. Encourageverbalizationofconcernsandfears. 5. Immediately report presence of chest pain.L. Monitorforchangesinneurologicalstatus(e.g.,confu- sion,disorientation).M. Monitorprogressiveactivity. 1. Earlyactivitiesshouldnotincreaseheartrate greaterthan25%ofrestingrate a. Walkinginhallway3-4timesadaywith gradualincreasingincrements. b. Decreasein20mmHginsystolicB/P,changes inheartrategreaterthan20bpm,shortnessof breathandorchestpainindicatepoor tolerancetoactivity. 2. Assessheartrhythm,fatigue,bloodpressure(BP) aftereachactivity. 3. Restingtachycardiaisacontraindicationtoactivity.
Home CareA. Participateinorganizedcardiacrehabilitationprogram. 1. Monitoredexercise. 2. Dietarymodifications. 3. ContinuededucationregardingASHDandmethods todecreasepersonalriskfactors.B. Understandmedicationregimen(seeBox12-3and Appendix12-2).C. Teachclienthowtocheckradialpulseforrateand regularity.D. Teachclienthowtoevaluateresponsetoincreased exercise,suchaschestpain,shortnessofbreathand tachycardia. 1. Whenbeginningwalkingprogram,remaincloseto home. 2. Alwayscarrynitroglycerinwhenwalkingor exercising. 3. Checkpulseratebefore,halfwaythroughandatthe endofactivity. 4. Stopactivityforpulseincreaseofmorethan 20bpm,shortnessofbreath,chestpain,ordizziness.

CHAPTER12 CardiacSystem 249
OLDER ADULT PRIORITY: Older clients will require a longer warm-up session before exercise, as well as a longer period of low exercise and rest between activities. They may also have less tolerance of warm environment due to ineffective sweating.
E. Exerciseinclimate-controlledareas.F. Callthephysicianforpainnotcontrolledbynitro- glycerin,significantchangesinpulserate,decrease inactivitytolerance,syncope,orincreaseindyspnea.G. Sexualintercoursegenerallyisresumed4to6weeks followinganMI,orwhenclientcanclimbtwoflightsof stairs,orwalkoneblockwithoutexperiencingchest pain. 1. Donotdrinkalcoholoreatalargemealbefore sexualactivity. 2. Takenitroglycerinbeforesexualactivity. 3. Donottakeerectiledysfunctionmedications (Appendix17-1)iftakingnitrates.
H. Returntophysicianforregularcheckups.
Heart FailureHeart failure (cardiac insufficiency, ventricular
failure) is the inability of the heart to pump adequateamounts of blood into the systemic circulation to meettissuemetabolicdemands.
Physiology of Heart FailureA. Left-sidedfailure(congestiveheartfailure[CHF]) (Figure12-2). 1. Resultsfromfailureoftheleftventricletomaintain adequateoutput. 2. Bloodbacksupintotheleftatriumandintothepul- monaryveins. 3. Increasingpressureinthepulmonarycapillarybed causeslungstobecomecongested,resultingin respiratorydistress. 4. Increasingpulmonarypressureresultsinincreased pressureonrightsideofheart.B. Right-sidedfailure(corpulmonale). 1. Resultsfromfailureoftherightventricletomain- tainadequateoutput. 2. Bloodbacksupintothesystemiccirculationand causesperipheraledema. 3. Mostcommoncauseissecondarytoleft-sidedfail- ureandchronicpulmonarydisease.C. Eachsideoftheheartisdependentontheotherforad- equatefunction. 1. Left-sidedfailureresultsinpulmonarycongestion; thiscausesanincreaseinpulmonarypressure, whichputsincreasedworkloadontherightsideof theheartandprecipitatesright-sidedfailure. 2. Althoughtheoriginoftheproblemmaybegin solelyononeside,themajorityofclinicalsituations involvefailureonbothsides.
✔
✽
3. Left-sidedfailurerapidlycausesright-sidedfailure. However,right-sidedfailuremayoccuraloneforan extendedperiodoftime.Frequentlyassociatedwith chroniclungproblems.D. Theheartwillattempttomaintainthebodyrequire mentsforcardiacoutput(increasingcardiacrate, vasoconstriction)whenthesemechanismsbecomein- effective,cardiacdecompensationorfailurewilloccur.E. In children,HFoccursmostoftenastheresultofacon- genitaldefectoftheheart.F. Edemadevelopmentinheartfailure. 1. Decreasedcardiacoutputleadstodecreaseinrenal perfusion,thekidneysrespondbyincreasingthe retentionofsodiumandwater. 2. Dependentpittingedemaoccurswithanincreasein circulatingvolume(venouspressure).
TEST ALERT: If a test question states that a cli-ent is in heart failure, assume that both sides are
in failure unless indicated otherwise.
Data CollectionA. Riskfactors/etiology. 1. Diseaseofcardiacvalves,mostofteninvolvesthe mitralvalve. 2. Historyofmyocardialdisease. 3. Historyofcongenitalheartdisease. 4. Fluidoverload;excessiveIVfluids. 5. Chronicpulmonarydisease.B. Clinicalmanifestations. 1. Impairedcardiacfunction. a. Tachycardiaevaluatedaccordingtoagegroup (seeTable3-1). b. Enlargedheartfromdilatationandhypertrophy.
FIGURE 12-2 Left-Sided heart failure. (From Zerwekh J, Claborn J: Memory notebook of nursing, ed 3, vol 1, Ingram, Tex, 2004, Nursing Education Consultants.)

250 CHAPTER12 CardiacSystem
C. Maintainnormalbodytemperature;avoidchillingbe- causeitwillincreaseoxygenconsumption.D. Providesupplementaloxygen,especiallywhenneeded withincreasedactivity.E. Provideuninterruptedsleepwhenpossible.F. Monitorurinaryoutput:assessforanycorrelationof decreasedurineoutputwithdecreasedcardiacoutput.G. Minimizecryinginchildrenandinfants.H. Decreasestressandanxiety;encourageparentstore- mainwithchild.I. Carefullyassessvitalsignsandcomparewithother physicalassessmentdata.
NURSING PRIORITY: The goals for care of a client with CHF are to:
Improve cardiac output: digitalis and oxygen.Decrease cardiac workload (afterload): decrease
activity, administer vasodilator.Decrease venous return (preload): diuretics;
decrease sodium and fluid intake; place client in semi-Fowler’s position.
v Goal:Todecreasecirculatingvolume.A. Diuretics(seeAppendix11-5).B. Decreasedsodiumdietandfluidrestrictioninadults.C. Calculatefluidscarefully;clientfrequentlyonfluidre- striction.D. Evaluatefluidretentionbyobtainingaccuratedaily weights;teachclienttoweighdaily(1kgor2.2lb weightgain=1Loffluidlossorretention).E. Accurateintakeandoutputrecords;assessresponse to-diuretics;notify RN if client gains 2 to 4 pounds over 24-hours.v Goal:Toreducerespiratorydistressandpromotegasexchange.A. Positionclientcarefully. 1. Positionadultclientinsemi-Fowler’sorinanarm chair;donotelevateclient’slegsbecausethis increasesvenousreturn. 2. Infantsandsmallchildrenmaybreathebetterside- lyingwiththekneesdrawnuptothechest. 3. Infantsmaybeplacedinaninfantseat. 4. Makesurediapersarelooselypinnedandsafety restraintsdonothindermaximumexpansionofthe chest. 5. Holdinfantuprightovertheshoulderwithknees flexed(knee-chestposition).B. Administerhumidifiedoxygento keep saturation levels at or above 90%C. Decreaseexposuretoupperrespiratorytractinfections.D. Evaluatebreathsounds;checkfordistendedneckveins andperipheraledema.E. Promotegradualactivity.Determineclient’srespiratory responsetoincreasedactivity.F. Donotallowinfantstocryforextendperiods.
✔
••
•
c. Poorperfusion:coolextremities,weakpulses, poorcapillaryrefill. d. Ininfants,failuretothriveandgainadequate weight. 2. Pulmonarycongestion(left-sidedfailure). a. Dyspneaandcoughonexertion. b. Orthopnea,tachypnea. c. Paroxysmalnocturnaldyspnea(PND)occurs whileclientisasleep. d. Symptomsofrespiratorydistressandhypoxia (seeTable10-3). e. Hemoptysis. f. Congestedbreathsounds. g. Feedingdifficultiesininfantsduetodyspnea anddecreasedtoleranceofactivity. 3. Systemiccongestion(right-sidedfailure). a. Hepatomegaly(enlargedliver):maybeanearly signinchildren. b. Peripheraledemaandweightgain. c. Dependentedemaorgeneralizededemain infants;evaluatebyweightgain. d. Ascites. e. Increaseincentralvenouspressure(CVP). f. Jugularveindistention(JVD)withheadelevated 30degrees.C. Diagnostics–Appendix12-1
TEST ALERT: Determine changes in client’s cardiovascular status as related to the client’s CHF; interpret what data need to be reported immediately.
TreatmentA. Treatmentoftheunderlyingproblem.B. Prevention. 1. Earlytreatmentofhypertension. 2. Earlytreatmentofdysrhythmias.C. Oxygen.D. Bedrest:semi-Fowler’sorhigh-Fowler’sposition.E. Medications(seeAppendix12-2). 1. Angiotensin-convertingenzyme(ACE)inhibitors willdecreasesystemicvascularresistance;thiswill decreasecardiacworkload(seeAppendix11-4). 2. Cardiacglycoside(digitalis)willincreasecontrac- tilityofcardiacmuscleandincreasecardiacoutput. 3. Medicationstodecreaseplateletaggregationor clumping.F. Decreasesodiumindiet.G. Fluidrestriction:adultsandolderchildren.Infants seldomneedfluidrestrictionsduetofeedingdifficulty.
Nursing Interventionsv Goal:Todecreasecardiacdemandsandimprovecar-diacfunction.A. Earlyidentificationandtreatmentofdysrhythmias.B. Limitphysicalactivity.

CHAPTER12 CardiacSystem 251
v Goal:Tomonitorfordevelopmentofhypoxia(seeChapter10).v Goal:Tomaintainnutrition.A. Duetodyspnea,eatingissometimesdifficult.B. Providesmall,frequentfeedings;allowclientadequate timetoeat.C. Infantsmayneedtobegavaged,duetoincreasedca- loricneedandincreasedworkofsucking.D. Infantsgenerallynotonfluidrestriction,duetode- creasedintakefromdyspnea.E. Donotpropthebottleandburptheinfantfrequently.
Home CareA. Clientshouldbeginwalkingshortdistances,250to 300feet,atleastthreetofourtimesperweek;distance canbeincreasedastolerated(noshortnessofbreath, dizziness,chestpain,ortachycardia).B. Teachclienthowtocounthisorherpulse.C. Clientshouldweighdaily,beforebreakfastandwith similarclotheson(nightgown,pajamas,etc.).D. Discussuseofandsafetyfactorsforhomeoxygen.E. Contacthealthcareproviderfor: 1. Weightgainof3-5poundsoveraweek,or1-2 poundsovernight. 2. Increaseindyspneaorangina,especiallywithde- creasedactivityoratrest. 3. Decreaseinactivitytolerancethatexceeds3or4 days. 4. Increasedurinationatnight,presenceorincreasein peripheraledema. 5. Coughorrespiratorycongestionthatlastslonger than3or4days.
F. Providewritteninstructionsformedications.
Rheumatic Heart DiseaseRheumatic heart disease occurs in about 40% of
clients with rheumatic fever; it primarily affects thecardiac valves. Myocardial involvement is characterizedby an inflammatory response, causing scarring of the cardiacvalves.Themitralvalveisthemostcommonareaaffected.A. UsuallyprecededbyagroupAbeta-hemolyticstrepto coccalinfection.B. Rheumaticcarditisistheonlysymptomthatproduces permanentdamage,mostofteninvolvesdamageto thetothemitralvalve.C. Rheumaticfeverusuallyoccursduringchildhood,but manifestationsofcardiacdamagemaynotbeevident foryears.
Data CollectionA. Clinicalmanifestationsofrheumaticfeversymptoms vary;nospecificsymptomorlabtestisdiagnosticof
✽
rheumaticfever.Criteriaforthediagnosisrequirea combinationofsymptomstobepresent. 1. Polyarthritis. 2. Carditisandfever. 3. Chorea:CNSinvolvementcharacterizedbyinvol- untarypurposelessmovement;noresidualdamage occurs. 4. Possiblerash. 5. Subcutaneousnodules.B. Clinicalmanifestationsofrheumaticcarditis. 1. Heartmurmur,tachycardia. 2. Pericarditis,pericardialfrictionrub,andchestpain.
NURSING PRIORITY: Prevention and adequate treatment of streptococcal infections prevent the devel-opment of rheumatic heart disease.
TreatmentA. Prevention:adequatetreatmentofstreptococcalinfec- tions.B. Restanddecreasedactivitytodecreasecardiacwork load.C. Salicylatestocontrolinflammatoryresponseand arthriticpain.D. Prophylactictreatment. 1. Initiatedafteracutetherapy. 2. Administrationofpenicillinoverextendedperiod oftime.Durationdependsonpresenceandlevelof cardiacinvolvement. 3. Beforeinvasivemedicalprocedures,clientwillneed additionalantibioticsduetoincreasedriskofbacte- rialendocarditis.
ComplicationsSeverevalvedamagesecondarytoinfectiveendocarditismayprecipitatethedevelopmentofcongestiveheartfailurewhichmayrequireopenheartsurgeryforreplacementofdiseasedvalve.
Nursing InterventionsChildisgenerallycaredforinthehomeenvironment.v Goal:Toassistparentsandfamilytoprovidehomeenvironmentconducivetohealingandrecovery.A. Decreaseactivity;maintainbedrestifpulserateis increasedoriffebrile.B. Encourageroutineactivitieswithinthehome.C. Friendsmayvisitforshortperiods;childisnotconta- gious.D. Arrangeforschoolworktobecontinuedathomeasap propriate.E. Maintainadequatenutritionandhydration.F. Administeranalgesicsforjointpain.v Goal:Toassistparentsandclienttounderstandneedforlong-termprophylacticantibiotictherapy.
✔

252 CHAPTER12 CardiacSystem
A. Discusstheimportanceofpreventingrecurring infections.B. Importanceofprophylactictherapybeforeinvasive medicalprocedures.C. Continuedmedicalfollow-upcareforthedevelopment ofvalveproblemsaschildgrows.D. Follow-uprequiredwithfemales;cardiacproblemsmay notbemanifesteduntilwomanispregnant.
Infective Endocarditis (Bacterial)Endocarditis isan infectionof thevalvesand inner
liningoftheheart.A. Organismmayenterfromanysiteoflocalizedinfec- tion.B. Organismgrowsontheendocardiumandproducesa characteristiclesionconsistingofvegetation,fibrin deposits,andcollagen;thelesionthenprogressesto damagedadjacentvalves.C. Lesionisfragileandparticlesmaybreakoffandform emboli.
Risk FactorsA. Congenitalheartdisease.B. Prostheticvalvereplacement.C. IVdrugabuse.D. Historyofrheumaticfeverwithcarditis.
Data CollectionA. Onsetisgradualwithnonspecificsymptoms. 1. Intermittentfever,highorlowgrade. 2. Anorexia,weightloss. 3. Jointpain. 4. Petechiae(common)inconjunctiva,lips,buccal mucosa,ontheankle,andintheantecubitaland poplitealareas. 5. Splinterhemorrhagesinnailbeds.B. Cardiacmurmur,symptomsassociatedwithheart failure.C. Symptomssecondarytoemboli. 1. Spleen:splenomegaly,upperleftquadrantpain. 2. Kidney:flankpain,hematuria. 3. Brain:hemiplegia,decreasedlevelofconscious- ness. 4. Pulmonary:dyspnea,chestpain,hemoptysis.
TreatmentA. Identificationofinfectiousorganismandappropriate antibiotictherapyfor4-6weeks(seeAppendix5-10).B. Bedrestifhighfeverorifevidenceofheartfailureis present.C. Prophylacticantibioticsfor3to5years,especiallyin childrenwithhistoryofrheumaticcarditisorcongenital abnormalities.
✽
D. Prophylacticantibioticsbeforedentalwork,invasive diagnosticprocedures,orsurgery.
Nursing Interventionsv Goal:Toassistparents/clienttounderstandneedforlong-termprophylactictherapyinhigh-riskcandidates(seerelatedgoalforrheumaticheartdisease).v Goal:Tomaintainhomeostasisandpreventcomplica-tionsoverlong-termhospitalization.A. Maintainpatternofdecreasedactivity;assessactivity tolerance.B. Evaluateforcomplicationsofemboliandcongestive heartfailure.
Home CareA. Explainthepurposeoflong-termantibiotictherapy.B. Goodoralhygiene 1. Dailycareandregulardentalvisits. 2. InformdentistsandPCPsbeforeanyinvasive procedure(e.g.,toothextraction,cystoscopy).Anti- bioticswillbeorderedprophylactically.C. Monitortemperature;reportfever,chills,malaise, increasingfatigue,weightlosstoPCP.D. Followaprogressiveactivityscheduleuntilbackto previouslevelofactivity;avoidexcessivefatigue;plan restperiodsandactivity.E. Adviseallhealthcareprovidersofhistoryofendo- carditis.
PericarditisPericarditis is an inflammation of the pericardium.
Thepericardialspaceisacavitybetweentheinnerandtheouterlayersofthepericardium.
Data CollectionA. Acuteformmayoccur2to3daysafteramyocardial infarction.B. Chronicpericarditis(Dressler’ssyndrome)mayoccur1 to4weeksafteranMI.C. Chestpainaggravatedbybreathing,swallowing,lying supine.D. Painincreaseswithdeepinspirationandlyingsupine; sittingmayrelievepain;painmayradiate,makingit difficulttodifferentiatefromangina.E. Pericardialfrictionrubcausedbymyocardiumrubbing againstinflamedpericardium.F. Fever,dyspnea,tachypnea.G. Restlessness,irritability,anxiousness.
TreatmentA. Acute. 1. Treatunderlyingproblem. 2. Restrictedactivity. 3. Antiinflammatorymedications.
✽

CHAPTER12 CardiacSystem 253
Nursing Interventionsv Goal:Tomaintainhomeostasisandpromotecomfort.A. Assesscharacteristicsofpain;administerappropriate analgesics.B. Positionclientupright;clientleaningforwardfrequent- lyrelievespain.C. Decreaseanxietyasclientoftenassociatesproblem withanMI;assistclienttodistinguishthedifference. 1. Paindoesnotincreasewithactivity. 2. Painisnotrelievedbyrest. 3. Painisrelievedbysittingupandleaningforward.D. Inaclientwithchronicpericarditis,evaluatefor symptomsofCHFandinitiateappropriatenursing intervention.
Cardiovascular Disease in PregnancyRheumaticheartdiseaseandcongenitalheartdefects
account for the greatest incidence of cardiac disease inpregnancy.Ofthese,mitralvalvestenosisisbyfarthemostcommonproblem.
A. Normalphysiologicalalterationsofpregnancythatin- creasecardiovascularstress. 1. Increaseinoxygenrequirements. 2. Increaseincardiacoutput. 3. Weightgain. 4. Hemodynamicchangesduringdelivery.B. Asnormalpregnancyadvances,cardiovascularsystem isunabletomaintainadequateoutputtomeetincreas- ingdemands.
Data CollectionClinicalmanifestationsindicativeofcardiacdecompensationarethoseofimpendingcardiacfailure.A. Frequentcough.B. Progressivegeneraledema(face,feet,hands);excessive weightgain.C. Progressivedyspnea.D. Excessivefatigueforlevelofactivity.E. Dysrhythmias:tachycardiagreaterthan100beats/min.F. Congestedbreathsounds.G. Cardiacdecompensationincreaseswithlengthofgesta- tion;increasedincidenceofheartfailureat28-to 32-weeksgestation.
TreatmentA. Managementofthepregnantclient. 1. Balancednutritionalintake;adequatecaloriesto maintainweight(avoidattemptstoloseweight). 2. Restrictedactivity,frequentrestperiods. 3. Ifsevere,maybehospitalizedandplacedonbed restat28to32weeks,duetoimpendingcardiac failure.4. Prophylacticpenicillintopreventinfection:especially importantinwomenwithmitralvalvediseasefrom rheumaticfever.
✽
B. Managementoftheclientduringlaboranddelivery. 1. Continuousmonitoringoffetusandmother. 2. Supplementaloxygen.C. Managementoftheclientduringpostpartum. 1. Becauseofdramaticchangesinthehemodynamic systemofthemother,thefirst24hourspostpartum isaperiodofincreasedrisk. 2. Clientistreatedsymptomaticallyaccordingtosta- tusofcardiovascularsystem;thefirst24-48hours postpartumisperiodofhighestriskforHFinthe mother.
Nursing Interventionsv Goal:Toassistclienttomaintainhomeostasisduringpregnancy.A. Providewritteninformationregardingnutritional needs.B. Assessforearlysymptomsofcardiacfailure.C. Encouragefrequentrestperiods;stopanyactivitythat increasesshortnessofbreath.v Goal:Tomaintainhomeostasisinpostpartumperiod.A. Assesspulmonaryandcardiacadaptationtochangesin hemodynamics.B. Increasedbloodflowduetodecreasedabdominalpres- suremaycausearefluxbradycardiaC. Maintainsemi-Fowler’spositionorleftlateralposition withtheheadelevated.D. Promotegradualprogressionofactivitiesdependingon cardiacstatusasindicatedby: 1. Normalpulserate. 2. Goodrespiratorystatus. 3. Activitytolerance.E. Encourageprogressiveambulationassoonaspossible topreventvenousstasisanddevelopmentofDVT.F. Assistmotherandfamilytopreparefordischarge.
TEST ALERT: Provide care for client experiencing complications of pregnancy.
Congenital Heart DiseaseA. Clinicalmanifestationsdependontheseverityofthe defectandtheadequacyofpulmonarybloodflow.B. Normalpressureintherightsideoftheheartislower thanpressureintheleftside;thereisanincreasedblood flowfromanareaofhighpressuretoanareaoflow pressure. 1. Whenthereisanopeningbetweentherightandleft sideoftheheart,oxygenatedbloodwillshuntfrom theleftsideofthehearttotherightside(right- to-leftshunt). 2. Whenthepressuresontherightsideoftheheart exceedthepressureontheleftsideoftheheart, unoxygenatedbloodfromtherightsidewillflow intotheleftsideandunoxygenatedbloodwillflow intothesystemiccirculation(left-to-rightshunt).C. Physicalconsequencesofcongenitalheartdefects.
254 CHAPTER12 CardiacSystem
1. Delayedphysicaldevelopment. a.Failuretogainweight,causedbyinabilityto maintainadequatecaloricintaketomeet increasedmetabolicdemands. b.Tachycardiaandtachypneaprecipitateincrease incaloricrequirements. 2. Excessivefatigue,especiallyduringfeedings. 3. Frequentupperrespiratorytractinfections. 4. Dyspnea,tachycardia,tachypnea. 5. Hypercyanoticspells(called“blue”spellsor“tet” spells):infantsuddenlybecomesacutelycyanotic andhyperpneic;occurmostofteninchildren2 monthsto1yearofage.D. Diagnostics(seeAppendix12-1).
Nursing Interventionsv Goal:Toevaluateinfant’sresponsetocardiacdefect.A. Determineinfant’sApgarscoreatbirth.B. Evaluateadequacyofweightgain.C. Assessforfeedingproblems. 1. Poorsuckingreflex. 2. Poorcoordinationofsucking,swallowing, breathing. 3. Fatigueseasilyduringfeeding;mayresultininad equateintake.D. Frequencyofupperrespiratorytractinfections.
E. Determineifcyanosisoccursatrestorisprecipitated byactivity.F. Presenceandqualityofpulsesinextremities.G. Allfeversshouldbereported,bacterialendocarditisis aprimaryconcernbeforeandaftercorrectionof congenitaldefect.
PEDIATRIC PRIORITY: Cyanosis that decreases with crying is associated with respiratory function; cyanosis that increases with crying is associated with cardiac function.
v Goal:Toassistparentsinadjustingtodiagnosis.A. Allowfamilytogrieveoverlossofperfectinfant.B. Evaluateparents’levelofunderstandingoftheinfant’s problem.C. Fosterearlyparent-infantattachment;encourage touching,holding,andgeneralphysicalcontact.D. Assistthefamilytodeveloparelationshipwhichfosters optimalgrowthanddevelopmentofallfamilymem bers.(SeeChapter3forpsychosocialaspectofchroni- callyillchildren.)v Goal:Todetect,prevent,andtreatHF–seeearlierdiscussionofheartfailure.v Goal:Toprovideappropriatenursinginterventionsfortheclientundergoingopenheartsurgeryforrepairofadefect.
✔
StudyQuestions:CardiacSystem
1. Thenurseispreparingaclientforacardiaccatheteriza- tion.Whatisimportantforthenursetoexplainto theclientregardinghiscareafterthetest? 1 Itwillbeimportantforyoutolieflatforseveral hours. 2 Itwillbenecessaryforyoutoambulatesoonafter thetest. 3 Youwillbeverysleepy;letthenurseknowifyou arehurting. 4 Therewillbeacatheterinyourbladderbecauseyou cannotgetup.2. Acardiaccatheterizationisscheduledforaclient.In consideringallergicreactionstothedyeusedinthe procedure,anallergicreactiontowhatfoodwould causethenursethemostconcern? 1 Eggs. 2 Milkproducts. 3 Shellfish. 4 Penicillin.3. Cardiacisoenzymesareorderedforaclientwhois admittedwithadiagnosisof“ruleoutmyocardial infarction.”Whatinformationwillthistestprovide? 1 Identifiesmyocardialtissuedamage. 2 Determinestheareaofmyocardialinvolvement. 3 Evaluatestheabilityofheartmuscletocontract. 4 Identifiespresenceofendocarditis.4. Thenurseisassessingtheapicalheartrateonaclient.
Whereonthechestwallshouldthenurseplacethe stethoscope? 1 Midlineandtotheleftofthemediastinum. 2 Mid-clavicularline,fifthintercostalspaceonthe left. 3 Fifthintercostalspace,leftmid-axillaryline. 4 Rightofmediastinum,anteriortotheaxillaryarea.5. Aclientwithbacterialendocarditisisbeingdischarged. Whatwillbeimportantforthenursetoreviewwiththe client? 1 Beginexerciseregimeninabout2weeks. 2 Increaseyourfluidintakeoffruitjuices. 3 Keeptakingyourantibiotic. 4 Returnweeklyforanelectrocardiogram.6. Whatistherationaleforalow-sodiumdietintheclient withcongestiveheartfailure? 1 Fluidretentionwilldecrease,andthiswillimprove cardiacoutput. 2 Fluidswillberetainedtomaintaincardiacoutput. 3 Adecreaseinsodiumlevelwillcauseadecreasein potassiumlevels. 4 Myocardialcontractilitydependsonnormalserum sodiumlevels.7. Thenurseisadministeringnitroglycerintoaclientwho saysheisexperiencingmidsternumchestpain.What wouldthenurseidentifyasacommonsideeffectofthis medication?

CHAPTER12 CardiacSystem 255
1 Pulserateof120beatsperminute. 2 Increaseinsystolicbloodpressure. 3 Onsetofnauseaandvomiting. 4 Clientsayshisheadishurting.8. Aclienthasadiagnosisofleft-sidedheartfailure,and heistellsthenurseheishavingdifficultybreathing. Thenursedeterminestheclient’spulseratetobe120 beatsperminute;respirationsare32breathsperminute. Whatistheimmediatenursingaction? 1 Determinewhenhelasthadhismedications. 2 Evaluatetheadequacyofurinaryoutput. 3 Puthiminsupinepositionwithfeetelevated. 4 Placehiminhigh-Fowler’spositionwithfeet dependent.9. Aclientwithadiagnosisofchronicanginaisbeingdis- charged.Whatisimportantforthenursetoteach theclientregardinghowtotakethesublingual nitroglycerintablets? 1 Takethemedicationwithafullglassofwater. 2 Keepthemedicationinaclearcontainer. 3 Themedicationhasarapidonsetofactionof2to5 minutes. 4 Takethemedicationatthefirstonsetofchestpain.10. Digitalishasbeenorderedforaclientincongestive heartfailure.Whatwouldthenurseexpecttofindwhen evaluatingtheclientforthetherapeuticeffectivenessof thedrug? 1 Improvedrespiratorystatusandincreasedurinary output. 2 Increasedheartrateandbloodpressure. 3 Diaphoresiswithdecreasedurinaryoutput. 4 Increasedheartratewithincreasedrespirations.11. Whenshouldthenursedeterminetheclient’spulserate bycheckingtheapicalheartrate?Selectallthatapply:____ 1 Determiningpulseratebeforetheadministrationof____ digitalis.____ 2 Checkingthevitalsignsonahypertensiveclient.____ 3 Determiningtheheartrateinaclientwithan ____ irregularpulse.____ 4 Evaluatingvitalsignswithinthefirst24hoursafter____ amyocardialinfarction.____ 5 Evaluatingaclientwithorthostatichypotension.____ 6 Determiningvitalsignsonaninfant.12. Asedemadecreasesinaclientwithheartfailure,what physiologicalresponsewouldthenurseexpecttofind? 1 Increaseinbodyweight. 2 Ralesacrossalllungfields. 3 Respiratoryrategreaterthan24breathsperminute. 4 Increaseintheurinaryoutput.13. Thenurseiscaringforaclientwithachronicpulmo- naryconditionwhohasdevelopedacomplication ofright-sidedheartfailure.Whichnursingobservation isassociatedwiththiscomplication? 1 Decreasingurinaryoutput. 2 Anirregularpulserate. 3 Jugularveindistention. 4 Increasingpulmonarycongestion.
14. Thenurseisassessingaclient2daysafterhewas diagnosedwithamyocardialinfarction.Whatfinding wouldcausethemostimmediateconcern? 1 Urinaryoutputof40mlperhour. 2 Jugularveindistentioninthesupineposition. 3 Shootingpainintheleftupperthigh. 4 Irregularpulserateof120beatsperminute.15. Anolderadultclientisadmittedincongestiveheart failure.Whatobservationbythenurseindicatesthatthe client’sconditionisgettingworse? 1 1+edemainlowerextremities. 2 Bloodpressureof160/98mmHg. 3 Urinaryoutputof60ml/hr. 4 Increasingirritabilityandconfusion.16. Aclientwithahistoryofcardiacproblemstellsthe nurseheisbeginningtohavechestpainwhilehe issittinginabedsidechair.Whatwouldbethefirst nursingaction? 1 Assessthecharacteristicsofthechestpain. 2 Returntheclienttobedandbeginoxygen. 3 Advisethephysicianregardingtheclient’sstatus. 4 Determinewhentheclientlastateanyfood.17. Whatisconsideredamodifiableriskfactorforcoronary arterydisease? 1 Age. 2 Race. 3 Diet. 4 Heredity.18. Aclientisadmittedtothehospitalduetomalfunction ofhispermanentpacemaker.Whatwouldbeimportant toincludeinthenursingcareofthisclient? 1 Encourageincreasedfluidintake. 2 Maintainfallprecautions. 3 Encouragedailyambulationinthehall. 4 Assessfordevelopmentofhypoxia.19. Aclientreturnstotheroomafterplacementofaper- manentpacemakerviatherightsubclavianvein.What isanimportantnursingactiontopreventcomplications? 1 Ambulatetheclientandencouragedeepbreathing. 2 Checktheradialpulseratetoevaluatethepace- makerfunction. 3 Limitmovementandabductionoftherightarm. 4 Assessthestatusofincisionandexternalpace- makerwire.20. WhyistheclientplacedonafirmsurfacewhenCPRis performed? 1 Theheartiscompressedbetweenthesternumand thespine. 2 Itiseasiertoestablishandmaintainanopenairway. 3 Itpromotesvenousreturnbacktotheheart. 4 Itdecreasesthepotentialfordamagetothexiphoid process.
Answers and rationales to these questions are in the section at the end of the book titled Chapter Study Questions: Answers and Rationales.

256 CHAPTER12 CardiacSystem
Continued
Appendix 12-1 CARDIAC DIAgnostICs
SERUMLABORATORYSTUDIES Cardiac EnzymesEnzymesaredrawntoevaluatemyocardialmuscleanddetermineiftherehasbeendamagetothemuscle.1. Creatininekinase(CK-MB).Increasesoccurwithin4to6hoursafteranMI,peakin12to24hours,andreturntonormalin24-36 hours.Increasesgreaterthan5%oftotalcreatinekinasearestronglysupportiveofanhighlyindicativeofMI2.2.CardiactroponinTandcardiactroponinI:normallevelsarelessthan0.2ng/ml(forT)andlessthan0.03ng/dl(forI);levelsare elevatedwithin3to6hoursafteranMIandpeakwithin10to24hours.Anyelevationissignificantbecauseitisnotfoundinhealthy clients.
Nursing Implications1. Enzymesmustbedrawnonadmissionandobtainedatregularintervals.Thereisacharacteristicpatterntotheincreasesanddecreasesof enzymelevelsinaclientwithanMI.2. Thelargertheinfarction,thelargertheenzymeresponse.3. Increasedlevelsoftroponinarethemostsignificantanddiagnosticofmyocardialdamage.4. Cardiac-specifictroponinhelpsdiscriminatefromothertissueinjury.
C-Reactive Protein (CRP), Highly sensitive C-Reactive Protein (hs-CRP)HighlysensitiveCRP(hs-CRP)maybeusedtoidentifyriskfordevelopinganMI.Theresponsetothetestassistsinevaluatingtheseverityandcourseofinflammatoryconditions.Normal:Lessthan1mg/Lor8mg/dL;increasinglevelissignificantandmayindicatesomedegreeofinflammatoryresponsecausedbyplaqueformation.
B-type natriuretic Peptide (BnP)Firstwholebloodmarkerforidentifyingandtreatingheartfailure.SerialBNPvaluesmaybeusedtoevaluateleftventricularfunction;assiststoidentifyheartfailureversusrespiratoryfailureascauseofdyspnea.Normalislessthan100pg/mL.
NONINVASIVE Electrocardiogram (ECg)Agraphicrepresentationoftheelectricalactivityoftheheart,generallyconductedusinga12-leadformat.Testtoidentifyconductioninrhythmdisordersaswellasspecificelectricalchangesthatcorrelatewithcardiacischemiaandinjury.
Holter MonitorClientisconnectedtoasmallportableECGunitwitharecorderthatrecordstheclient’sheartactivityforapproximately24hours.Theclientisdirectedtokeepalogofactivity,pain,orpalpitations.Theclientshouldnotshowerorbathewhilethemonitorisinplace.Therecordingisthenanalyzed,comparingtheheartrateandrhythmtotheclient’sactivitylog.
Event MonitorClientisconnectedtoanECGportableunitwitharecorder.Theclientcanactivatetherecorderatanytimehefeelsanydizzinessorpalpitations.Monitormaybewornforextendedperiodsoftime.Monitorleadsandbatteryunitmayberemovedforshowering,butshouldbereconnectedimmediatelyafterbathing.Recordingsaretransmittedoverthephone.
Exercise stress testThistestinvolvestheclientexercising.Thismaybedoneonatreadmillorastationarybicyclethatincreasesinspeedanddegreeofinclinetoincreasetheheartrateandbloodpressure.ECGleadsareattachedtotheclient,andtheresponseofthehearttoexerciseisevaluated.
Nursing Implications1. Appropriatepretestclienteducation;establishbaselinevitalsignsandcardiacrhythm.2. Clientshould: a. Avoidsmoking,ordrinkingalcoholimmediatelybeforetest,alightmealmaybegive2hourspriortothetest. b. Avoidstimulants(caffeine),andextremetemperaturechangesimmediatelyaftertest.3. Cardiacrhythmandvitalsignsaremonitoredconstantlyduringtest.4. Reasonsforterminatinganexercisestresstest:predeterminedheartrateisreached,chestpain,excessivefatigue,dyspnea,vertigo, hypotensionorventriculardysrhythmiasoccur;ECGchangesofsignificantSTsegmentdepressionorT-waveinversionoccurs.5. Ifanyoftheabovechangesoccurandthetestisterminated,itissaidtobeapositivestresstest.
thallium 201 testAsmalldoseofthalliumisadministered,andacamerarecordstheuptakeofthalliumthroughtheheart.Normaltissuehasarapiduptakeofthallium;areasofscarringordamagehaveslowerornouptakeofthallium.Clientsshouldnotingestcaffeineorsmokebeforethistest.
EchocardiogramAnultrasoundproceduretoevaluatevalvularfunction,cardiacchambersize,ventricularmuscle,andseptalmotion.Theultrasoundwavesaredisplayedonagraphandinterpreted.ProvidesmorespecificinformationthatanECG.Thethroatisanesthetized,andaflexibleendoscopeispassedintotheesophagustotheleveloftheheart.Sedationisusedduringtheprocedure.

CHAPTER12 CardiacSystem 257
Appendix 12-1 CARDIAC DIAgnostICs—cont’d.
transesophageal EchocardiographyThistestisanendoscopyultrasoundandprovidesahigherqualitypicturethanaregularechocardiogram.Thethroatisanesthetized,andaflexibleendoscopeispassedintotheesophagustotheleveloftheheartandanechocardiogramisconductedfromtheesophagealview.Sedationisusedduringtheprocedure.
Nursing Implications1. NPOfor4to6hoursbeforetest.2. Afterthetest,checkforgagreflexbeforeresumingPOfluids.
Magnetic Resonance ImagingThisisanoninvasivediagnosticscan.Amagneticfieldandradiowavesareusedtodetectanddefinethedifferencesbetweenhealthytissueanddiseasedtissue.Providesimagesinthreedimensions.
Nursing Implications1. Theclientcannothaveanymetalonhis/herbody;removealljewelry,hairclips,etc.2. Clientswithpermanentmetalimplantedinthebody(pacemakers,implantedclipsandwires,insulinpumps)arenotcandidatesforMRI.3. Clientmustbecooperativeandremainverystillduringtheprocedure.4. Nospecificcarerequiredaftertheprocedure.
Positron Emission tomography (PEt)Verysensitiveinidentifyingviableandnonviablecardiactissue.Theproceduretakesabout2to3hours,andaradioactivedyeisinjectedintravenously,followedbyglucose.Aclient’sglucosemustbebetween60-140mg/dLpriortothetest.
INVASIVEDIAGNOSTICSCardiac CatheterizationAninvasiveprocedureinwhichacatheterispassedthroughanarteryorveinintotheheart.Cardiaccatheterizationwillprovidedataregardingstatusofthecoronaryarteries,aswellascardiacmusclefunction,valvularfunction,andleftventricularfunction(ejectionfraction).Right-side catheterization:Providesinformationregardingthefunctionandstructureoftherightatrium,rightventricle,pulmonicvalve, andtricuspidvalve.Left-side catheterization:Providesinformationregardingthefunctionandstructureoftheleftatrium,leftventricle,aorticvalve,and mitralvalve.Thecatheterismanipulatedthroughtheaortaanddyeisinjectedintothecoronaryarteries(coronaryangiogram).
Nursing Implications1. Pretestpreparation. a. NPO4to8hoursbeforetest. b. Recordqualityofdistalpulsesforcomparisonpost-test. c. Checkfordyeallergy,especiallyiodineandcontrastmedia. d. Determinewhetheranymedicationsneedtobewithheld. e. Clienteducation:reportanychestpainordiscomfortordifficultybreathing.Clientwillneedtoliestillonhardtable;aflushedfeeling mayoccurwhendyeisinjected. f. Clientisawakeduringprocedure;sedativemaybegiven.
2. Post-test. a. Evaluatecatheterizationentrysite(mostoftenfemoral)forhematomaformation.Notifyphysicianimmediatelyforexcessivebleeding atthesite,andforsignificantchangesinbloodpressure. b. Evaluatepulsesdistaltocatheterizationsite,color,sensationoftheextremity.Notifyphysicianimmediatelyforadecreasein peripheralcirculationorneurovascularchangesinaffectedextremity. c. Assessfordysrhythmias. d. Maintainbedrestfor4to8hours;avoidflexion,keeptheextremitystraight. e. Keepheadofbedelevatedat30degreesorless. f. Fluidswillbeencouragedtoflushthedyeoutofthebody.
TEST ALERT: Monitor peripheral pulses; identify and intervene to prevent circulatory complications.

258 CHAPTER12 CardiacSystem
Appendix 12-2 CARDIAC MEDICAtIons
NITRATES:Increasebloodsupplytotheheartbydilatingthecoronaryarteries;cardiacworkloadisreducedduetodecreaseinvenous returnbecauseofperipheralvasodilation.
Medications side Effects nursing Implications
Nitroglycerin(NTG,Nitrostat):sublingualNitroglycerin(Nitro-BID,Nitrol):topical(patch)Nitroglycerinointment(Nitropaste):topical,bytheinchNitroglycerintranslingualspray
Headaches(willdiminishwiththerapy),posturalhypotension,syncope,blurredvision,drymouth,reflextachycardia
1. Adviseclientthatalcoholwillpotentiateposturalhypotension.2. Educateclientregardingself-medication(seeBox12-3).3. Donottakewitherectiledysfunctiondrugs.4. Topicalortransdermalapplicationisusedforsustainedprotectionagainstanginalattacks.5. Avoidskincontactwithtopicalform;removeallpreviousapplicationsonclient’sskin.6. Sublingualtabletsandtranslingualspraygivenforanimmediateresponse.
CalciumChannelBlockers:Blockadeofcalciumchannelreceptorsintheheartcausesdecreasedcontractilityanddliationofarteriesfortreatmentofhypertensionandangina;somemedicationshavecardiacspecificproperties.
Medications side Effects nursing Implications
Diltiazem(Cardizem):PO,IVNifedipine(Procardia):POVerapamil(Calan,Isoptin):IV,PO
Constipation,exacerbationofCHF,hypotension,bradycardia,peripheraledema
1. Nifedipineislesslikelytoexacerbatepreexistingcardiacconditions;isnoteffectiveintreatingdysrhythmias.2. Intensifiescardiosuppressanteffectsofbeta-blockermedications.3. Assessforbradycardia.
Beta-AdrenergicBlockingAgents(adrenergicantagonists):Blockadeofbetareceptorsintheheartcausesdecreased heartrate,anddecreasedrateofAVconduction.Usedtotreathypertensionaswellasangina.Betablockersshouldbeadministeredtoall clientsexperiencingunstableanginaorhavinganMIunlesscontraindicated.
Medications side Effects nursing Implications
Labetalol(Trandate):PO,IVMetoprolol(Lopressor,ToprolXL):PO,IVPropranolol(Inderal):PO,IVAtenolol(Tenormin):PO,IVCarvedilol(Coreg):PONote:Carvedilol,bisoprolol,andmetoprololsustainedreleaseareusedtotreatHF
Bradycardia,hypotension,depression,lethargyandfatigue
1. Closelymonitorcardiacclient—mayprecipitateheartfailure, butisalsousedtotreatheartfailure.2. Teachclienthowtodecreaseeffectsofposturalhypotension.3. Teachclienttocontinuemedicationregardlessoffeeling better.4. Checkpulseforbradycardiabeforeadministering.5. Ifclienthasdiabetes,bloodglucosecontrolmaybeimpaired.6. Givewithcautiontoclientswithhistoryofbronchospasm.
AntidysrhythmicMedications:Decreasecardiacexcitability;delaycardiacconductionineithertheatriumorventricle. Atropineiscardiacstimulantforbradycardia.
GeneralNursingImplications— Assess client for changes in cardiac rhythm and impact on cardiac output.— Evaluate effect of medication on dysrhythmia and resulting effects on cardiac output.— Have atropine available for cardiac depression resulting in symptomatic bradycardia.— All cardiac depressant medications are contraindicated in clients with sinus node or AV node blocks.— Digitalis will enhance cardiac depressant effects.— Closely monitor for dysrhythmias that are precipitated by the treatment.— All of these medications can make existing dysrhythmias worse and also create new ones.— RN or physician will administer IV medications; LPN may assist in monitoring the client.
Continued

CHAPTER12 CardiacSystem 259
Appendix 12-2 CARDIAC MEDICAtIons—cont’d.
Medications side Effects nursing Implications
Quinidinesulfate(QuinidineSulfate,Quinidex):PO
Atropine:subQ,IV
Amiodaronehydrochloride(Cordarone):PO,IV
Lidocainehydrochloride(Xylocaine):IV
Procainamide(Pronestyl):PO,IV
Propranololhydrochloride(Inderal):PO,IV
HypotensionDiarrhea,nausea,vomiting
TachycardiaDrymouth,blurredvision,dilatedpupils
AVheartblock,hypotensionToxicity—lungandvisualproblems
Drowsiness,confusion,seizures,severedepressionofcardiacconduction
Abdominalpain,cramping,hypoten-sion,prolongedQTintervalBlooddyscrasias
Seepreviousdiscussionofbeta-adren-ergicblockers
1. Administerwithfood.2. MonitorforECGchangesfortoxicity—widenedQRSand prolongedQT.3. Uses: supraventriculartachycardiaandventricular dysrhythmias.
1. Use:symptomaticbradycardia.2. Assessclient’scardiacoutputinresponsetothebradycardic episode.
1. Use:life-threateningventriculararrhythmias,atrial fibrillation.2. Monitorforseverebradycardia.3. Monitorforindicationsofpulmonarytoxicity–dyspnea andcough.4. AHighAlertMedication-cautionwithadministrationandmaintaincloseclientobservation.
1. Use:ventriculardysrhythmias.2. MustuseIVpreparatioinofLidocaineforIVinfusion.3. Monitorforseizuresandbradycardia.4.HighAlertMedication-useonlycardiacpreparationforIV.
1. Use:short-andlong-termcontrolofventricularand supraventriculardysrhythmias.2. Closelymonitorforbradycardiaandhypotension.3. DonottakeOTCcoldpreparations.4. Maydevelopautoimmuneproblems–systemiclupus erythematosus.
1. Use:long-andshort-termtreatmentandpreventionof tachycardia.2.HighAlertMedication-givewithcautionandcloselymonitorclientresponse.
Fibrinolytic(thrombolytic)medications:Initiatefibrinolysisofaclot.Medicationswillbreakupaclotanywhereinthebody–inasurgicalincisionaswellasintheheart.
Nursing Implications— Therapy should begin as soon as the MI is diagnosed or when there is a history of prolonged angina—for best results, from admission in the ED until medication is administered is 30 min (door-to-needle), or within 60 min of onset of symptoms.— Used to treat: acute coronary thrombosis (MI), deep vein thrombosis (DVT), and massive pulmonary emboli.— Medication should be administered by an RN or physician; LPN may monitor client after infusion.— Bleeding precautions (see Table 9-1).
Medications side Effects nursing Implications
Alteplase(tPA,Activase):IVReteplase(Retavase):IVStreptokinase(Streptase,Kabikinase):IV
Bleedingandhypotension 1. Obtainbasevitalsigns,monitorforhypotension.2. Monitorforallergicreactionswithstreptokinase.3. Monitorforbleeding.4. Avoidvenipuncturesduringandafterinfusion.5.HighAlertMedication-monitorclientclosely.6. Use:MI,PE,DVT;brainaccident,contraindicatedinclients withactivebleeding.
Continued
HIGH
ALERT

260 CHAPTER12 CardiacSystem
Appendix 12-2 CARDIAC MEDICAtIons—cont’d.
OLDER ADULT PRIORITY: Older adults are more sensitive to digitalis and are more likely to experience toxicity.✔
BloodViscosityReducingAgent:
Pentoxifylline(Trental):PO Nausea,vomiting,dizziness,headache,diarrhea,
1. Primaryuseisforreliefofintermittentclaudication fromPVD.2. Therapeuticeffectmaynotbenotedfor2-4weeks.3. Donotchew,crushorbreaktablets.
GI,Gastrointestinal;MI,myocardialinfarction;PO,bymouth(orally);TIA,transientischemicattack;PVD,peripheralvasculardisease.
CardiacGlycosides(e.g.,digitalis):Increasemyocardialcontractilityandcardiacoutput.Decreaseheartratebyslowing conductionofimpulsesthroughtheAVnode.
GeneralNursingImplications— Take the apical pulse for a full minute; if the rate is below 60 beats/min in an adult or below 90-110 beats/min in infants and young children, or below 70 in a child, hold the medication and notify the physician.— Evaluate for tachycardia, bradycardia, and irregular pulse. If there is significant change in rate and rhythm, hold the medication and notify the charge nurse or primary care provider. — Evaluate serum potassium levels and response to diuretics; hypokalemia potentiates action of digitalis.— Gastrointestinal symptoms are frequently the first indication of digitalis toxicity.— Teach client not to increase or double a dose in the case of a missed dose; if client vomits, do not give an additional dose.— To achieve maximum results rapidly, an initial loading dose is administered; then dose is reduced to a maintenance dose.
Medications side Effects nursing Implications
Digoxin(Lanoxin):PO,IV Mostcommon:anorexia,nausea,vomiting.Mostserious:drug-induceddysrhyth-miasVisualdisturbances,fatigueChildren/infants:frequentvomiting,poorfeeding,orslowheartratemayindicatetoxicity
1. Therapeuticplasmalevelsofdigoxinare0.5-2.0ng/mL.2. FirstsignoftoxicityisusuallyGIsymptoms.3. Uses:supraventriculartachycardia,CHF.4. Monitorserumpotassiumlevels–lowpotassiumpotentiates actionofdigitalis.5.HighAlertMedication-monitorclientcloselyforsideeffectsandtoxicity.
ANTIPLATELETS(PLATELETAGGREGATIONINHIBITORS):Inhibittheaggregationandclumpingofplateletswhichreducesthe riskofstroke,orMIorperipheralvascularocclusioninclientswithperipheralvascular.
Medications side Effects nursing Implications
Aspirin:PO
Clopidogrel(Plavix)PO
Ticlopidine(Ticlid):PO
Cilostazol(Pletal):PO
GIbleeding,dyspepsiaHemorrhagicstroke
GIdisturbances,skinreactions,blooddyscrasias
Headache,dizziness,
1. Aspirinisgiveninsmalldoses(e.g.,81mgdaily).2. TakeaspirinandTiclidwithfoodtodecreasegastric irritation.3. ProphylactictherapyforpreventionofMIandischemicstroke (thrombotic)inclientswithTIAs.4. Monitorcoagulationstudiesthroughouttherapy.
1. PrimaryuseisforreliefofintermittentclaudicationinPVD.2. Grapefruitjuiceinhibitsmetabolism.3. Administeronanemptystomach.
HIGH
ALERT
GI,Gastrointestinal;MI,myocardialinfarction;PO,bymouth(orally);TIA,transientischemicattack;PVD,peripheralvasculardisease.

CHAPTER12 CardiacSystem 261
Appendix 12-3 CARDIoPULMonARY REsUsCItAtIon (CPR) FoR HEALtH CARE PRoVIDERsTheAmericanHeartAssociation(AHA)hasestablishedstandardsforcardiopulmonaryresuscitationforthehealthcareprovider.Forfurtherdelineationoftheprocedure,consulttheAmericanHeartAssociationCardiopulmonaryResuscitationGuidelines.Forhealthcareproviders,theAmericanHeartAssociationusestheterminfanttorefertoindividualsbetweenbirthand1yearofage;childisusedtorefertothosewhoarebetween1yearofageandtheonsetofpuberty.
1.AIRWAY.1. Identifythatthevictimisunconscious.2. Activatetheemergencymedicalservices(EMS)system.3. Obtainautomatedexternaldefibrillator(AED).UseAEDassoonasitisavailableforalladultsandchildrenforsudden,witnessed collapseandforin-hospitalclients.4. Placeclientinpositiontoopenairway.5. Opentheairway:head-tilt/chin-liftmaneuver.6. Checkforadequatebreathing(look,listen,andfeelforbreaths).7. Ifvictimisbreathing,placeinrecoveryposition.8. Ifvictimisnotbreathing,give2rescuebreathsusingmouthtomouth,orapocketmaskorbagmask.
2.Breathing.1. Maintaintheopenairway.2. Pinchnostrilsclosed.3. Givetwobreathsthatmakethechestrise,at1secperbreath,usingmouth-to-mouthtechnique(mouth–to–noseandmouthtechniquemay beusedforsmallchildrenandinfants).4. Donotgive“extra”breaths;donotgivelarge,forcefulbreaths.5. Whenanadvancedairwayispresent,ventilateattherateof8-10/min;donotpauseforcompressions.
3.Checkthepulsefornomorethan10sec.1. Adultandchild:Checkthecarotidpulse.2. Infant:Checkthebrachialorfemoralpulse.3. Ifthepulseisabsent,beginchestcompressions—cyclesof30compressionsand2breathsuntilACLSorPALSstandardsareinitiated.4. Ifthepulseispresent,continuerescuebreathing,andrecheckpulseevery2min.If,despiteadequateventilation,theheartrateofan infantorchildremainsunder60bpm,chestcompressionsshouldbestarted.5. Adult:1breathevery5-6sec,10-12permin.6. Childandinfant:1breathevery3-5sec,12-20breathspermin.7. Advancedairwaypresent(laryngealmaskairway,endotrachealtube):1breathevery6-8secwithouttryingtosynchronizebreathswith compressions.
4.Externalcardiaccompression.1. Placethevictimonafirmsurface.Iftheclientisinabed,putacardiacboardbehindhimorher.DONOTattempttoremovetheclient fromthebed.2. Locatethelowerhalfofthesternumintheadult.Fortheadult,placeonehandoverthelowersternum;placetheotherhandontopofthe previoushand.Forachild(age1yeartopuberty),usetheheelofonehand,ortwohandsbasedonthesizeofthechild,andpressonthe centerofthechestatthenippleline.Foraninfant,locatethenippleline;theareaforcompressionisonefinger’swidthbelowtheline.3. Depressthesternum11⁄2to2inchesintheadult;inchildrenandinfantsdepressapproximatelyone-thirdtoone-halfofdepthofchest.4. Pushhardandfast;allowthechesttorecoilcompletelybetweencompressionsandasfewinterruptionsaspossible.Adult and child:Onerescuerandtworescuers:30compressions(rateof100permin)to2ventilations.Infant:Onerescuer:30compressions(rateof100permin)to2ventilations.Tworescuers:15compressionsto2ventilations.
PEDIATRIC PRIORITY: Be careful not to hyperextend the infant’s head; this may block the airway. Don’t pinch the infant’s nose shut—cover the nose with your mouth instead. Breathe slowly, just enough to make the chest rise.
✔
Continued

262 CHAPTER12 CardiacSystem
Appendix 12-3 CARDIoPULMonARY REsUsCItAtIon (CPR) FoR HEALtH CARE PRoVIDERs—cont’d.Defibrillation:Useautomaticelectronicdefibrillator(AED)assoonasavailableforsuddencollapseandforin-hospitalclients.Stepsforusinganautomatedexternaldefibrillator(AED):1. ProvideCPRuntiltheAEDarrives.2. Onarrival,openthecaseandturnthepoweron.3. Selectthecorrectpadsforthesizeandageofthevictim(onlyusethechildpads/systemforchildrenlessthan8yearsold).4. Attachtheadhesiveelectrodes—oneontheupper-rightsideofthechestdirectlybelowtheclavicle,theotherbelowtheleftnipplebelow
theleftarmpit.5. AttachtheconnectingcabletotheAED.6. Compressionswillneedtobediscontinuedwhiletherhythmisanalyzed.7. Ifshockisindicated,loudlystate“Clear!”andvisuallychecktoensurethatnooneistouchingtheclient.8. PresstheSHOCKbutton.9. ResumeCPRimmediatelywithcyclesof30compressionsto2breaths.
10. After2min,theAEDwillpromptyoutorepeatsteps6through9.
5.TerminationofCPR.A rescuer who is not a physician should continue resuscitation efforts until one of the following occurs:1. Spontaneouscirculationandventilationhavebeenrestored.2. Resuscitationeffortsaretransferredtoanotherequallyresponsiblepersonwhocontinuestheresuscitationprocedure.3. Aphysicianorphysician-directedpersonassumesresponsibilityforresuscitationprocedure.4. Thevictimistransferredtoanemergencymedicalservice(e.g.,paramedicsandambulance).5. Therescuerisexhaustedandunabletocontinueresuscitation.
TEST ALERT: Identify and intervene in life-threatening client situations. Notify primary health care provider about unexpected response/emergency situation of client.
CHAPTER12 CardiacSystem 263
LifeThreateningDysrhythmiasVentriculartachycardia
Ventricularfibrillation
Wide,bizarre,erraticorregularORScomplexesoccurringataveryrapidrateof125to200beats/min
Veryrapid,erraticconductionwithundeterminedrate;cannotidentifyQRScomplexes;
Severedecreaseincardiacoutput;potentiallylife-threateningsituation.Mayhaveapulseorbepulseless.IfunconsciousandpulselessinitiateCPR.Treatment:lidocaine,amiodarone,procainamide,cardioversion.
Clientisunresponsive,withnopulse;initiateacodeandbeginCPR.Treatment:defibrillation,lidocaine.
Appendix 12-4 CARDIAC ConDUCtIon AnD DYsRHYtHMIAs
CHARACTERISTICSOFNORMALSINUSRHYTHMPulseCharacteristics:Rate:60to100beats/minRhythm:regular
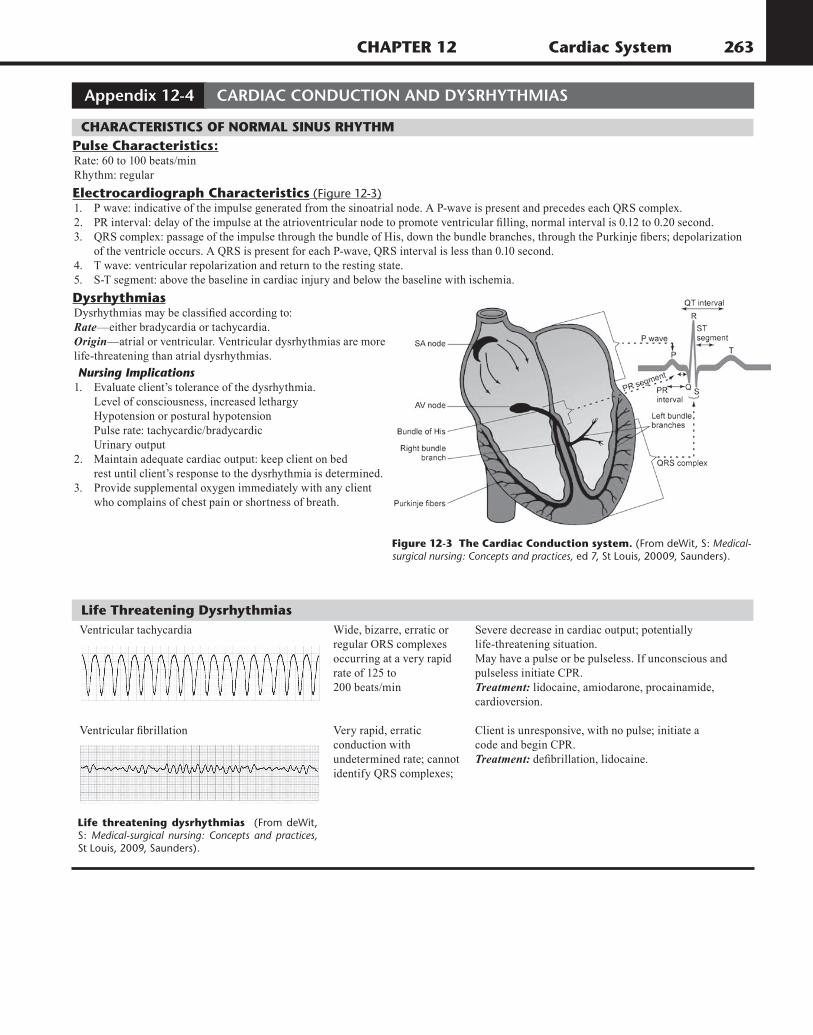
ElectrocardiographCharacteristics (Figure 12-3)1. Pwave:indicativeoftheimpulsegeneratedfromthesinoatrialnode.AP-waveispresentandprecedeseachQRScomplex.2. PRinterval:delayoftheimpulseattheatrioventricularnodetopromoteventricularfilling,normalintervalis0.12to0.20second.3. QRScomplex:passageoftheimpulsethroughthebundleofHis,downthebundlebranches,throughthePurkinjefibers;depolarization oftheventricleoccurs.AQRSispresentforeachP-wave,QRSintervalislessthan0.10second.4. Twave:ventricularrepolarizationandreturntotherestingstate.5. S-Tsegment:abovethebaselineincardiacinjuryandbelowthebaselinewithischemia.
DysrhythmiasDysrhythmiasmaybeclassifiedaccordingto:Rate—eitherbradycardiaortachycardia.Origin—atrialorventricular.Ventriculardysrhythmiasaremorelife-threateningthanatrialdysrhythmias.
Nursing Implications1. Evaluateclient’stoleranceofthedysrhythmia. Levelofconsciousness,increasedlethargy Hypotensionorposturalhypotension Pulserate:tachycardic/bradycardic Urinaryoutput2. Maintainadequatecardiacoutput:keepclientonbed restuntilclient’sresponsetothedysrhythmiaisdetermined.3. Providesupplementaloxygenimmediatelywithanyclient whocomplainsofchestpainorshortnessofbreath.
Figure12-3TheCardiacConductionsystem.(From deWit, S: Medical-surgical nursing: Concepts and practices, ed 7, St Louis, 20009, Saunders).
Lifethreateningdysrhythmias (From deWit, S: Medical-surgical nursing: Concepts and practices, St Louis, 2009, Saunders).

264 CHAPTER12 CardiacSystem
Appendix 12-5 PACEMAKERs
PERMANENTAninternalgeneratorisinsertedintosofttissueofupperchestorabdomen,andelectrodesarepositionedintheheartaccordingtothepacingmode;procedureplannedandconductedunderhighlycontrolledenvironment.Mostoftendoneinsame-daysurgery(Figure12-5).
DemandPacingModeTheheartisstimulatedtobeatwhentheclient’spulseratefallsbelowasetvalueorrate.Themajorityofpacemakershaveasetratebetween60and72beatsperminute;ifclient’spulseratefallsbelowthesetvalue,thepacemakerwillbeinitiated.Thepacemaker“senses”theinitiationofabeatandthefollowingconduction.Ifanormalcardiacimpulseorbeatisinitiatedandconducted,thepacemakerdoesnotinitiateanimpulse.
Nursing Implications1. Assessinsertionsiteforsignsofbleedingorhematomaformation.2. Ifpulseratefallsbelowpresetlevel,keepclientinbedandreportitimmediately.3. Assessclient’stoleranceofactivity:syncopeororthostatichypotensionshouldnotoccur.4. Afterinitialinsertion,avoidmovingaffectedarmabovethehead.
ClientEducation1. Wearamedicalalertidentification,andadviseallhealthcareprofessionalsregardingthepacemaker.2. Avoidirritatingortightclothingthatputspressureonorirritatesthesite;reportanysignsofinfectionoversite.3. Safeenvironment:avoidclosecontactwithareasofhighvoltage,magneticforcefields,largerunningmotors;microwavesarenota problem.4. AvoidactivitythatrequiresvigorousmovementofarmsandshouldersoranydirectblowstoPMsite.5. Advisetheclientofthesetrateofpacemaker;teachclienthowtocounttheirradialpulse.Notifythecardiaccenterorprimarycare providerimmediatelyifthepulserateislowerthanthesetrate.6. Adviseclienttoimmediatelyreportepisodesofsyncope.7. Follow-upcareandmonitoringofthepacemakerareveryimportant.Follow-upisusuallydoneonamonthlybasisviaatrans-telephonic device;itdoesnotrequireclienttocomeintooffice.8. Clientmaytravelwithoutrestrictions.
NURSING PRIORITY: Pacemaker failure - An ECG must be available to validate pacemaker failure. If a client with a pacemaker experiences syncope or a bradycardia below the rate set on the pacemaker, it needs to be investigated immediately.
✔
Figure12-5PermanentPacemakerPlacement.(From Phipps W et al: Medical-
surgical nursing: Health and illness perspectives, ed 7, St. Louis, 2003, Mosby)
TEST ALERT: Determine pacemaker malfunction.