cardiac resynchronization therapy : atrial fibrillation
TRANSCRIPT
Cardiac Resynchronization Therapy:
Should Non-LBBB or Patients With
Atrial Fibrillation Receive CRT?
Michael R Gold, MD, PhD
Medical University of South Carolina
Charleston, SC
Disclosures: Consultant, Speaker Fees and Clinical Trials –
Boston Scientific, Medtronic, St Jude

Cardiac Resynchronization Therapy: Weight of Evidence
9,000 patients evaluated in randomized controlled trials of heart failure
Consistent improvement in quality of life, functional status, and exercise capacity
Strong evidence of changes in LV structure – ↓ LV volumes and dimensions
– LVEF
– ↓ Mitral regurgitation
Reduction in HF and all-cause morbidity and mortality
Pivotal RCTs of CRT
• NYHA II-IV
• LVEF < 35%
• QRS > 120-130 msec
• NRS (except RAFT)
• No study was restricted to LBBB or
even stratified randomization by BBB
or QRS duration

Subgroups Discouraged or
Prohibited from CRT by Updated
Guidelines
1. Non-LBBB
2. QRS < 150 msec
3. AF

RBBB in CRT Trials
Advanced HF
– MIRACLE
– CONTAK CD
– COMPANION
– CARE HF
Mild HF
– REVERSE
– MADIT-CRT
– RAFT
(28)
(33)
(162)
(35)
(82)
(228)
(161)
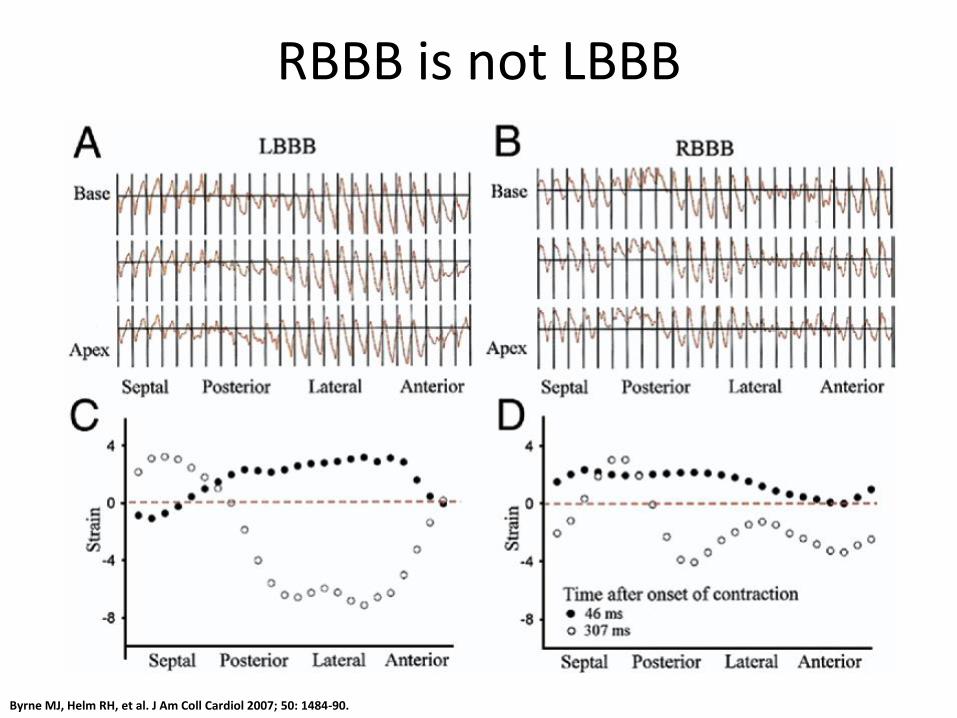
RBBB is not LBBB
Byrne MJ, Helm RH, et al. J Am Coll Cardiol 2007; 50: 1484-90.

Fantoni C, Kawabata M, Massaro R et al. J Cardiovasc Electrophysiol. 2005 Feb;16(2):112-9
Electrical Activation in RBBB and LBBB

Egoavil CA, Ho RT, Greenspon AJ, Pavri BB. Heart Rhythm. 2005 Jun;2(6):611-5.

COMPANION
Bristow, N Engl J Med. 2004;350:2140-50.

Heart Failure (HF) Event or Death by QRS Pattern in MADIT-
CRT Patients
LBBB Non-LBBB

RAFT
Tang. N Engl J Med. 2010 363:2385-2395.
12
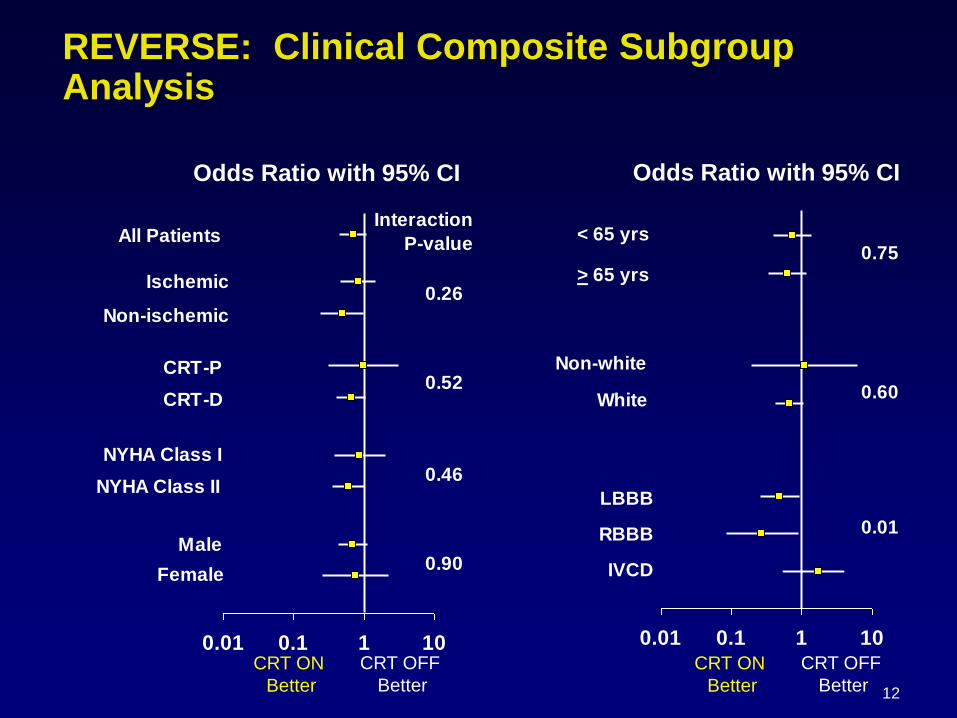
REVERSE: Clinical Composite Subgroup Analysis
0.01 0.1 1 10
All Patients
Ischemic
Non-ischemic
CRT-P
CRT-D
NYHA Class I
NYHA Class II
Male
Female
0.26
0.90
0.46
0.52
Interaction
P-value
0.01 0.1 1 10
LBBB
RBBB
IVCD
Non-white
White
> 65 yrs
< 65 yrs0.75
0.60
0.01
Odds Ratio with 95% CI Odds Ratio with 95% CI
CRT ON
Better
CRT OFF
Better
CRT ON
Better
CRT OFF
Better

What is the QRS Morphology Hiding?
Can we identify patients or pacing sites with late mechanical or
electrical LV activation?

Hara H, et al. Eur Heart Journal. 2012.

Must be More Than Just RBBB
Hara H, et al. Eur Heart Journal. 2012.

Physiologic Guided Lead Positioning:
QLV Interval Measurement

Q-LV Interval to Predict Acute Response
R = 0.74
-5
0
5
10
15
20
25
30
35
40
0 50 100 150 200
Q-LV (ms)
%L
V+
dP
/dT
max
R
NR

Results: CRT Response By QLV Quartiles

Impact of QRS Duration
Cleland et al
Eur Heart J
2013

LVESV Response by Subgroup
Univariate Logistic Regression Results

RAFT: Primary Outcome

Mean F.U. :
25.2 + 18 months
673 pts 162 Permanent AF
114 pts
AF-abl
48 pts
Drugs + VRR
BVP % at 2 months
> 85% 85%
1. AVJ ablation and reverse remodelling
J Am Coll Cardiol 2006; 48 (4): 734-743

1) Significant EF increase both in SR and AF-abl No change for AF drugs
3) Similar LVESV reductions in SR and AF-abl
2) Functional capacity score increase both in SR and AF-abl

Meta Analysis of AVJ ablation for CRT.

1812 pts
Inadequate % BIV pacing
AF pts
AF pts
50% mortality if BIV pacing< 92%
25% pts BIV < 92%

Summary
CRT response rates are best in the presence
of sinus rhythm, LBBB and QRS > 150 msec
However, RCT included or studied other
groups of patients who show benefit, albeit
more variable
Late electrical mechanical activation helps
identify subjects with non-LBBB who respond
AV node ablation improves CRT response in
AFib