cardiac catheterization
TRANSCRIPT

What’s new?
C With improvement in technology and miniaturization of equip-
ment, radial access is increasingly being used for routine cardiac
catheterization.
C Catheters have been designed that enable engagement of both
INVESTIGATIONS
Cardiac catheterizationDeepak Goyal
Karim Ratib
Rajay Narain
Jim Nolan
left and right coronary ostia with the same catheter, limiting theneed for catheter exchanges.
C Vascular closure devices have been developed to aid in
managing femoral arterial punctures.
C The requirement for cardiac catheterization has been reduced
by comprehensive non-invasive imaging, but it remains the
gold standard for quantifying disease severity and planning
therapy for many patients with severe cardiac disease.
AbstractCardiac catheterization involves insertion of fine-bore tubes (catheters)
into the heart through cannulae inserted into a peripheral artery or
vein. Procedures are commonly performed via the femoral vessels.
However, the radial artery approach has the best safety record and is
becoming increasingly popular. Brachial access is now rarely used
because of its complexity and potentially higher complication rates.1
Left heart catheterization is used to diagnose or evaluate coronary artery
disease and valvular heart disease. Left ventriculography, selective coro-
nary angiography and measurement of pressure in the left ventricle (LV)
are routinely performed. Aortography is performed in patients with aortic
regurgitation or aortic root dilatation. Left ventriculography allows visual
assessment of LV size/function as well as measurement of LV pressure
and systolic pressure gradients across diseased aortic valves. Coronary
angiography provides information on coronary anatomy. Right heart cath-
eterization allows measurement of haemodynamic data and oxygen satu-
rations from the right heart chambers and pulmonary circulation. It
provides information on right ventricular function, pulmonary artery pres-
sure, right-sided and left-sided filling pressures, cardiac output and left-
to-right shunts. Combined right and left catheterization is used in the
comprehensive evaluation of patients with complex cardiac conditions,
particularly those with valvular heart disease, intra-cardiac shunts or
heart failure.2
Keywords aortography; cardiac catheterization; coronary angiography;
right heart catheterization; ventriculography
Introduction
Cardiac catheterization involves insertion of fine-bore tubes
(catheters) into the heart through a cannula in a peripheral artery
Deepak Goyal MD MRCP is Specialist Registrar in Cardiology in the West
Midlands Deanery, UK. Competing interests: none.
Karim Ratib MRCP is Cardiology Research Fellow at the University
Hospital of North Staffordshire, Stoke-on-Trent, UK. Competing
interests: none.
Rajay Narain MRCP is Specialist Registrar in Cardiology in the West
Midlands Deanery, UK. Competing interests: none.
Jim Nolan MD FRCP is Consultant Cardiologist in the Cardiothoracic
Centre at the University Hospital of North Staffordshire, Stoke-on-Trent,
UK. Competing interests: none.
MEDICINE 38:7 390
or vein under fluoroscopic guidance. The first human heart
catheterization was performed in 1929, when Werner Forssman
inserted a catheter into his own heart via a cut-down of his left
antecubital vein. Modern invasive and interventional cardiology
began when Mason Sones obtained the first selective coronary
angiogram in 1958, using a brachial artery cut-down technique.3
The introduction of the Seldinger technique and development of
pre-shaped catheters in the late 1960s established the femoral
approach as the preferred method. The radial artery approach,
which has better procedure-related vascular complication rates,
was introduced in 1989 by Campeau and has been rapidly
adopted by many cardiologists as their access site of choice.4
Left heart catheterization involves injection of contrast into
the left ventricle (ventriculography) and selective coronary
angiography. Pressures in the left ventricle and aorta are also
measured. Right heart catheterization involves passing a catheter
through the right heart chambers into the pulmonary circulation,
and provides additional haemodynamic data. Some of the hae-
modynamic data obtained rely on several assumptions, and so
must be interpreted together with information from other sources
and assessment of the patient’s clinical condition.
Indications
Patients with known or suspected coronary artery disease or
aortic valve disease usually undergo left heart catheterization to
clarify the diagnosis and to help in planning an optimal treatment
strategy. Left ventricular catheterization allows visual assess-
ment of left ventricular (LV) function and size, measurement of
LV end-diastolic pressure (LVEDP) and the systolic pressure
gradient across the aortic valve. Coronary angiography provides
information on coronary anatomy. Aortography is also per-
formed in those with aortic regurgitation, aortic root dilatation or
during assessment for aortic valve interventions.
Patients with mitral, tricuspid or pulmonary valve disease,
heart failure, pericardial constriction or suspected intra-cardiac
shunts, and those being assessed for cardiac transplantation
usually undergo both right and left cardiac catheterization. Right
heart catheterization provides haemodynamic information on
pulmonary and tricuspid valve gradients, right ventricular func-
tion, pulmonary artery pressure, right-sided and left-sided filling
� 2010 Published by Elsevier Ltd.

Figure 1 Angiogram demonstrating the left coronary artery anatomy in the
left anterior oblique view. The left coronary artery arises from the proximal
ascending aorta as the left main stem (LMS). This bifurcates into the
circumflex artery (Cx) and the left anterior descending artery (LAD).
Branches of the LAD are the septal arteries which supply the septum and
INVESTIGATIONS
pressures, cardiac output and left-to-right shunts. Simultaneous
left heart catheterization allows assessment of LV and mitral
valve function and associated coronary disease.
Pre-catheterization evaluation
This should include a full medical history, with particular
emphasis on co-morbidities such as diabetes, kidney disease and
anticoagulation status. Any previous allergies to contrast medium
or latex should be recorded. Full procedural details relating to
previous cardiac or peripheral arterial interventions or cardiac
surgery should also be obtained along with a physical examina-
tion and ECG. Routine laboratory tests should include a full blood
count including platelet count, serum electrolytes and creatinine,
plasma glucose and an international normalized ratio. Patients
with diabetes taking metformin should omit this drug on the
morning of the procedure and for 2 days after it. Patients with
a history of contrast medium allergy should be given prophylaxis
with corticosteroids and antihistamines. Patients with chronic
renal impairment are susceptible to contrast nephropathy, and
require pre-treatment with fluid loading and acetylcysteine, and
use of low-nephrotoxicity contrast agents.5
Procedures
the diagonal arteries (Dx). Branches of the circumflex artery (Cx) are called
Left heart catheterization obtusemarginals (OM). The circumflex artery (Cx) is dominant. This artery isfree from disease.
Left heart catheterization is commonly performed via a sheathpositioned in the right femoral artery. The sheath is inserted
using a Seldinger technique, and a side-hole catheter (usually
a pigtail catheter) is passed over a J-tipped guide-wire to the
aortic root and across the aortic valve into the left ventricle. A
straight guide-wire is used to cross the valve in patients with
aortic stenosis. If good echocardiographic data are available, it is
often unnecessary to cross a severely stenosed aortic valve, as
the non-invasive test will provide sufficient information on
stenosis severity and left ventricular function.6
With the catheter in the left ventricle, pressure is recorded and
the end-diastolic pressure measured. Ventriculography is per-
formed using a mechanical power injector. Pressure is then
recorded as the catheter is withdrawn across the aortic valve;
a decrease in pressure indicates the presence of aortic stenosis.
The catheter may also be placed above the aortic valve and
a further power injection performed to image the ascending aorta
and assess aortic regurgitation (aortography).
Selective coronary angiography is then performed. In about
90% of transfemoral diagnostic studies, Judkin’s catheters are
used. These are pre-shaped end-hole catheters that are designed
to engage the coronary ostia with minimal manipulation. In the
other 10% of cases, catheters of various shapes are used,
depending on the size and orientation of the aortic root and the
relative positions of the coronary ostia. The left and right coro-
nary arteries (Figure 1) are imaged in several different projec-
tions, using 5e10 mL of contrast for each view. Typically, six to
eight views of the left coronary artery and three of the right
coronary artery are obtained. These angiographic images are
used to detect and quantify the presence of stenotic coronary
lesions. When the procedure is completed, the catheters and
sheath are removed and manual pressure applied to the femoral
puncture sites to obtain haemostasis. As an alternative, vascular
closure devices can be used to close the vascular puncture
rapidly and reduce the need for bed rest.
MEDICINE 38:7 391
Right heart catheterization
The femoral vein is the most commonly used access site for right
heart catheterization. A sheath is placed in the vein using
a percutaneous Seldinger technique and a pre-shaped end-hole
catheter is passed into the right atrium, the right ventricle and the
pulmonary artery using standard manipulations under fluoro-
scopic control. Pulmonary artery pressure is recorded, and the
catheter is advanced until it plugs a branch of one of the pulmonary
arteries and the waveform changes to a pulmonary capillary
wedge (PCW) tracing closely matched to the left atrial pressure.
When mitral valve disease is suspected, simultaneous left
heart catheterization is performed and the LV and PCW pressures
are recorded simultaneously. Any difference between these
measures in end-diastole indicates mitral stenosis.
The pulmonary artery catheter is then withdrawn and pres-
sures in the pulmonary arteries, the right ventricle and the right
atrium are measured sequentially (Figure 2). Left-to-right intra-
cardiac shunts are assessed using a ‘saturation run’, in which
blood samples withdrawn from the pulmonary artery, the right
ventricle, the right atrium and the caval veins are analyzed and
their oxygen saturations compared. In patients who have
a significant left-to-right shunt, oxygenated blood enters the right
heart via a defect (such as an ASD, PDA or VSD) and produces an
abnormal increase in oxygen saturation (the magnitude of this
increase is proportional to the size of the shunt and this allows
quantification of the lesion).7
Flexible, balloon-tipped catheters may also be used to
measure right heart pressures and cardiac output in ICUs and
coronary care units (e.g. the SwaneGanz catheter). They are
commonly inserted via the subclavian, femoral or jugular vein,
and are floated across the tricuspid and pulmonary valves; in
many cases fluoroscopic guidance is not needed. With the
� 2010 Published by Elsevier Ltd.
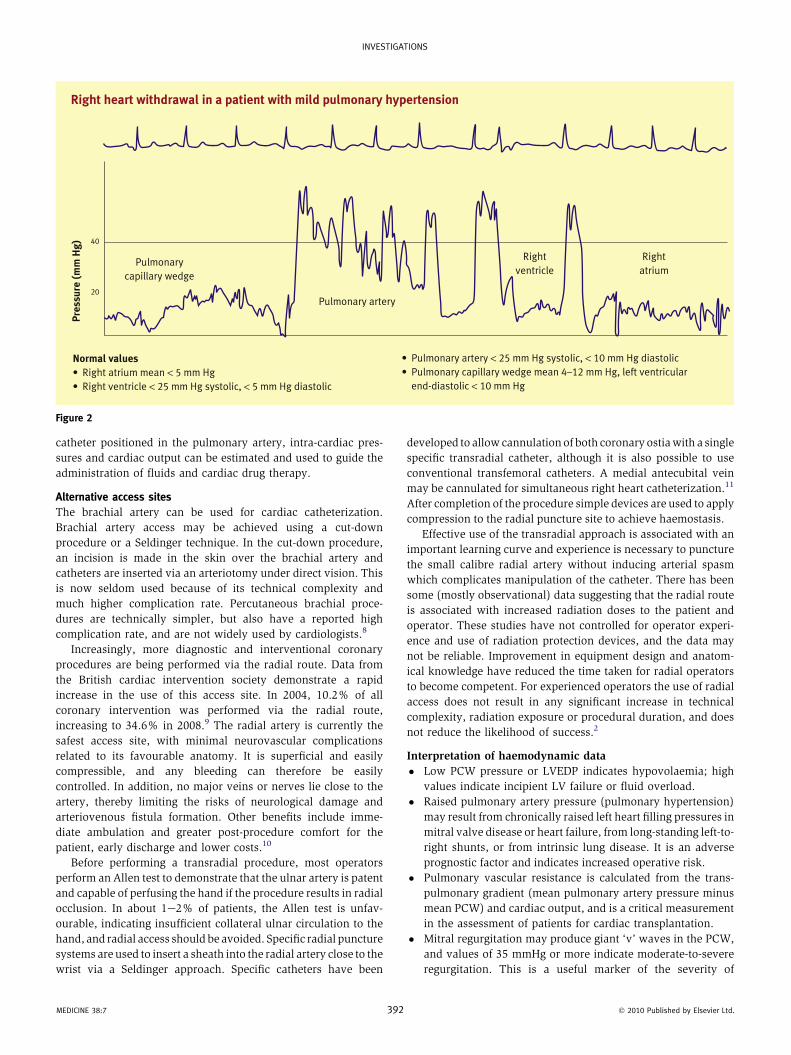
Right heart withdrawal in a patient with mild pulmonary hypertension
Normal values
• Right atrium mean < 5 mm Hg
• Right ventricle < 25 mm Hg systolic, < 5 mm Hg diastolic
• Pulmonary artery < 25 mm Hg systolic, < 10 mm Hg diastolic
• Pulmonary capillary wedge mean 4–12 mm Hg, left ventricular
end-diastolic < 10 mm Hg
Pre
ssu
re (
mm
Hg
) 40
20
Pulmonary
capillary wedge
Pulmonary artery
Right
ventricle
Right
atrium
Figure 2
INVESTIGATIONS
catheter positioned in the pulmonary artery, intra-cardiac pres-
sures and cardiac output can be estimated and used to guide the
administration of fluids and cardiac drug therapy.
Alternative access sites
The brachial artery can be used for cardiac catheterization.
Brachial artery access may be achieved using a cut-down
procedure or a Seldinger technique. In the cut-down procedure,
an incision is made in the skin over the brachial artery and
catheters are inserted via an arteriotomy under direct vision. This
is now seldom used because of its technical complexity and
much higher complication rate. Percutaneous brachial proce-
dures are technically simpler, but also have a reported high
complication rate, and are not widely used by cardiologists.8
Increasingly, more diagnostic and interventional coronary
procedures are being performed via the radial route. Data from
the British cardiac intervention society demonstrate a rapid
increase in the use of this access site. In 2004, 10.2% of all
coronary intervention was performed via the radial route,
increasing to 34.6% in 2008.9 The radial artery is currently the
safest access site, with minimal neurovascular complications
related to its favourable anatomy. It is superficial and easily
compressible, and any bleeding can therefore be easily
controlled. In addition, no major veins or nerves lie close to the
artery, thereby limiting the risks of neurological damage and
arteriovenous fistula formation. Other benefits include imme-
diate ambulation and greater post-procedure comfort for the
patient, early discharge and lower costs.10
Before performing a transradial procedure, most operators
perform an Allen test to demonstrate that the ulnar artery is patent
and capable of perfusing the hand if the procedure results in radial
occlusion. In about 1e2% of patients, the Allen test is unfav-
ourable, indicating insufficient collateral ulnar circulation to the
hand, and radial access should be avoided. Specific radial puncture
systems are used to insert a sheath into the radial artery close to the
wrist via a Seldinger approach. Specific catheters have been
MEDICINE 38:7 392
developed to allow cannulation of both coronary ostiawith a single
specific transradial catheter, although it is also possible to use
conventional transfemoral catheters. A medial antecubital vein
may be cannulated for simultaneous right heart catheterization.11
After completion of the procedure simple devices are used to apply
compression to the radial puncture site to achieve haemostasis.
Effective use of the transradial approach is associated with an
important learning curve and experience is necessary to puncture
the small calibre radial artery without inducing arterial spasm
which complicates manipulation of the catheter. There has been
some (mostly observational) data suggesting that the radial route
is associated with increased radiation doses to the patient and
operator. These studies have not controlled for operator experi-
ence and use of radiation protection devices, and the data may
not be reliable. Improvement in equipment design and anatom-
ical knowledge have reduced the time taken for radial operators
to become competent. For experienced operators the use of radial
access does not result in any significant increase in technical
complexity, radiation exposure or procedural duration, and does
not reduce the likelihood of success.2
Interpretation of haemodynamic data
� Low PCW pressure or LVEDP indicates hypovolaemia; high
values indicate incipient LV failure or fluid overload.
� Raised pulmonary artery pressure (pulmonary hypertension)
may result from chronically raised left heart filling pressures in
mitral valve disease or heart failure, from long-standing left-to-
right shunts, or from intrinsic lung disease. It is an adverse
prognostic factor and indicates increased operative risk.
� Pulmonary vascular resistance is calculated from the trans-
pulmonary gradient (mean pulmonary artery pressure minus
mean PCW) and cardiac output, and is a critical measurement
in the assessment of patients for cardiac transplantation.
� Mitral regurgitation may produce giant ‘v’ waves in the PCW,
and values of 35 mmHg or more indicate moderate-to-severe
regurgitation. This is a useful marker of the severity of
� 2010 Published by Elsevier Ltd.

Formulae used for haemodynamic data
C Left-to-right shuntPulmonary flow
Systemic flow¼ SaO2 �MVO2
98� PaO2SaO2, aortic oxygen saturation; PaO2, pulmonary artery saturation
MVO2 ¼ (3 � superior vena cava saturation þ inferior vena cava
saturation)/4
C Aortic valve area (cm2)
(Gorlin formula)
Cardiac output (L/min)
(Opening time/beat) � heart rate � Omean gradient (mmHg) � 44$3C Mitral valve area (cm2)
(Gorlin formula)
Cardiac output (L/min)
Opening time/beat � heart rate � Omean gradient (mmHg) � 37$7
C Cardiac output (L/min)
(Fick principle)
Oxygen consumption (mL/min)
1.36 (SaO2 � PaO2) � haemoglobin concentration (g/L)
Table 1
INVESTIGATIONS
regurgitation, but the size of the ‘v’ wave is considerably
affected by left atrial compliance.
� The transmitral gradient (PCW � LVEDP) is a measure of the
severity of mitral stenosis. End-diastolic gradients of more
than 5 mmHg are significant, and gradients of 12e16 mmHg
are typically seen in severe stenosis. However, the size of the
gradient depends on heart rate and cardiac output, and this
technique has been superseded by echocardiographic criteria.
Mitral valve area derived from the Gorlin formula (Table 1) is
more reliable, but requires estimation of cardiac output.
� The pull-back aortic gradient (Figure 3) is an important
measure of the severity of aortic stenosis; a gradient of 50
mmHg or more prompts consideration of valve replacement.
Echocardiography measures instantaneous gradients, which
are typically 10 mmHg or more greater than pull-back gradi-
ents, and this may lead to significant overestimation of the
severity of aortic stenosis. However, if LV function is poor,
the pull-back gradient is reduced, and estimation of valve
area using echocardiography or the Gorlin formula is a more
accurate guide to severity.
Pressure during pull-back across the aortic valve50 mm Hg
Pre
ssu
re (
mm
Hg
)
100
50
Figure 3
MEDICINE 38:7 393
� Left-to-right intra-cardiac shunts are assessed by comparing
oxygen saturations in the superior vena cava, the inferior
vena cava, the high, mid and low right atrium, the right
ventricle and the pulmonary artery. An increase in saturation
of more than 7% suggests a left-to-right shunt. Small shunts
may not be detected. The magnitude of the shunt is measured
in terms of the relative blood flows in the systemic and
pulmonary circulations.
� Cardiac output is measured using a thermodilution method or
by the Fick principle. The Fick principle calculates cardiac
output from oxygen consumption (measured using ametabolic
hood or a Douglas bag) and the arteriovenous difference in
oxygen content (measured from blood samples taken in the
pulmonary artery and aorta). Alternatively, oxygen consump-
tion can be estimated as 3ml O2/kg bodyweight, but this is less
accurate.
Complications
Major complications (e.g. major haemorrhage, myocardial infarc-
tion, stroke, major arrhythmia, death) occur in 0.25% of patients,
, showing a peak-to-peak gradient of
50 mm Hg
� 2010 Published by Elsevier Ltd.

INVESTIGATIONS
and are more common in those with advanced cardiac disease.
Minor complications (e.g. vasovagal reactions, urticaria) occur in
about 5% of patients. Predictors of significant complications
include advanced New York Heart Association functional class,
hypotension, shock, aortic valve disease and renal insufficiency.
Access site-related neurovascular complications are common with
thebrachial artery approach andoccur in about 1e2%of caseswith
the femoral approach. With the radial approach, the risk of access
site complications is significantly lower.
Conclusions
Although non-invasive imaging (in the form of echocardiography,
cardiac CT and magnetic resonance scanning) is useful in many
patients, cardiac catheterization remains the gold standardmethod
of evaluating serious cardiac disease, and is mandatory in many
patients before percutaneous or surgical treatment. Advances in
equipment design and catheterization techniques, particularly the
use of the radial access site, have improved the tolerability and
safety of cardiac catheterization procedures. Cardiac catheteriza-
tionwill continue to play an important role in the investigation and
management of cardiac patients for the foreseeable future. A
REFERENCES
1 Davis C, VanRiper S, Longstreet J, Moscucci M. Vascular complications
of coronary interventions. Heart Lung 1997; 26: 118e27.
2 Butler R, Gunning M, Nolan J. Essential cardiac catheterization.
London: Hodder Arnold, 2008.
3 Forssmann W. Uber die Wirkung der Leberfutterung auf das rote
Blutbild and den Cholesterinspiegel im Serum des gesunden
MEDICINE 38:7 394
Menschen Friedrich-Wilhelms Universitat, Inaugural-Dissertation,
Berlin, February 1929 (The report of first human heart catheterization
e a self experiment by Werner Forssman).
4 Agostoni P, Biondi-Zoccai GG, de Benedictis ML, et al. Radial versus
femoral approach for percutaneous coronary diagnostic and
interventional procedures; systematic overview and meta-analysis of
randomized trials. J Am Coll Cardiol 2004; 44: 349e56.
5 Scanlon PJ, Faxon DP, Audet AM, et al. ACC/AHA guidelines for
coronary angiography. A report of the American College of Car-
diology/American Heart Association Task Force on practice guidelines
(Committee on Coronary Angiography). Developed in collaboration
with the Society for Cardiac Angiography and Interventions. J Am Coll
Cardiol 1999 May; 33: 1756e824.
6 Omran H, Schmidt H, Hackenbroch M, et al. Silent and apparent
cerebral embolism after retrograde catheterisation of the aortic
valve in valvular stenosis: a prospective, randomised study. Lancet
2003 Apr 12; 361: 1241e6.
7 Gorlin R, Gorlin S. Hydraulic formula for calculations of stenotic mitral
valve, other cardiac valves, and central circulatory shunts. Am Heart J
1951; 41: 1e29.
8 Kiemeneij F, Laarman GJ, Odekerken D, Slagboom T, van der Wieken R.
A randomized comparison of percutaneous transluminal coronary
angioplasty by the radial, brachial and femoral approaches: the access
study. J Am Coll Cardiol 1997; 29: 1269e75.
9 Ludman P. BCIS dataset 2007, 2008, 2009.
10 Freestone B, Nolan J. Transradial cardiac procedures e the state of
the art. Heart, in press.
11 Lo TS, Buch AN, Hall IR, Hildick-Smith DJ, Nolan J. Percutaneous left
and right heart catheterization in fully anticoagulated patients
utilizing the radial artery and forearm vein: a two-center experience.
J Interv Cardiol 2006; 19: 258e63.
� 2010 Published by Elsevier Ltd.