capacity building & change management - mhvic.org.au · aspects of building capacity and change...
TRANSCRIPT

Capacity Building & Change ManagementA guide for services implementing dual diagnosis processes
Victorian Alcohol and Other Drug Association

ACKNOWLEDGEMENTS
This manual has been developed by Positive Directions, Consultancy and Training under the aus-pice of VAADA (Victorian Alcohol and Drug Association). Funded by the Department of Health and Ageing under the Improved Services for People with Drug and Alcohol Problems and Mental Illness Initiative – Capacity Building Grants, 2008–2012.
This manual has been made possible by the input of many people who gave willingly of their time. In particular, thanks to the Advisory Group who gave their time, advice and content freely.
Advisory GroupMerissa van SettenLisa WalklateDebra HubyChris HynanBrandon JonesCaroline Lee-SmithJohn KatsourakisGary Croton
Authors Renee WilliamsGreg LoganLinda Rose
GraphicsAgeUbaldi Creative
Developed byPositive Directions, Consultancy and Trainingwww.positivedirections.net.au
Funded and supported by Department of Health and Ageing.www.health.gov.au
This manual and accompanying resources are available from www.comorbidity.org.au
Version 2, 2012
© Victorian Alcohol and Drug Association 2012211 Victoria Pde, Collingwood. VICTORIA. 3066 Ph: (03) 9412 5600 Fax: (03) 9416 2085

Capacity Building and Change Management i
FOREWORD
Up to 80 per cent of all alcohol and other drug consumers also have a mental illness. Approximately one in two mental health clients have a co-occurring alcohol and drug use issue. This is the reality that has led to increasing recognition that both the alcohol and other drug (AOD) and mental health (MH) sectors must be skilled and experienced in the ability to deal with both conditions. The days of treating one issue and not the other – or treating the two issues through entirely separate services – have passed.
The Victorian Alcohol and Drug Association (VAADA) warmly welcomed the Commonwealth Government’s decision to invest $127 million to address this issue. Between 2006 and 2011, the Department of Health and Ageing funded 122 AOD organisations across Australia (including 27 within Victoria) to build organisational capacity to better identify and treat people who experience co-morbid alcohol and other drug use and men-tal illness. The funding comes under the Improved Services Initiative (ISI) as part of the Council of Australian Governments’ National Action Plan on Mental Health 2006–2011. Under this plan, the Department of Health and Ageing has also funded VAADA to support ISI grant recipients and to coordinate a statewide approach to building capacity.
Through this support for the stakeholders, VAADA identified the need for a resource that addresses the change process undertaken by agencies moving toward dual diagnosis capability. The purpose of creating this resource has been to identify learnings of this initiative thus far and create a package that can be adapted by all agencies to achieve what will soon be the sector standard: dual diagnosis capable AOD and mental health agencies.
This manual offers a way forward in addressing the complexities of organisational change, in building stronger links with and between the AOD and mental health sectors, and in opening up agencies to the ‘no wrong door’ approach. It also assists uniform capacity across the sectors in this state and beyond.
VAADA would like to thank and acknowledge the Department of Health and Ageing for its support throughout the initiative and for the opportunity to produce this resource.
We would also like to thank the consultants, Positive Directions, and the resource development reference group for their energy and tireless work in bringing this manual together.
Sam Biondo Merissa van SettenExecutive Officer ISI State Coordinator
Victorian Alcohol and Other Drug Association

Capacity Building and Change Managementii
ABOUT THE AUTHORS
Renee WilliamsRenee is the Director of Positive Directions, Consultancy & Training – the consultants who authored this resource. Re-nee founded the company approximately 10 years ago and has 14 years’ experience in project consultancy and project management. As a change agent, her passion is service development, service integration and partnerships. Renee works with organisations and staff to improve service delivery, support change processes and implement specific projects.
Renee currently provides project consultancy and management to two ISI projects in Victoria.
As an accredited facilitator, Renee delivers tailored workshops for strategic planning, team building, partnership engage-ment and brainstorming.Renee has expertise and qualifications in education and training and can support organisations to further develop their capacity building by designing programs that reflect the educational needs of the organisation and staff.
As a supervisor and coach, Renee provides 1:1 and group supervision and leadership support for project managers, project teams and individual clinical staff.
Renee is also a Credentialed Mental Health Nurse and family therapist with a 26-year career path within mental health, alcohol and other drug, primary care and general practice settings. Renee is a peer credentialer for the Australian Col-lege of Mental Health Nurses.
Greg LoganGreg is a general and psychiatric nurse with 30 years’ experience in the mental health and alcohol and other drug sectors. He has degrees in education as well as 20 years’ experience in the development and delivery of educational programs. He lectured for 10 years at Monash University in Melbourne before being employed by Turning Point Alco-hol and Drug Centre. While at Turning Point, Greg was responsible for the development and management of their postgraduate course: the Graduate Diploma of Alcohol and Other Drug Studies. He was also responsible for the development of Turning Point’s capacity to develop and deliver online learning.
Recently he was the Manager of the Victorian Dual Diagnosis Initiative Education and Training Unit, based at St Vincent’s Hospital in Melbourne. In this role, Greg has been responsible for the development and delivery of dual diagnosis train-ing to all mental health and AOD workers across Victoria. He now has a consultancy business.
Greg has expertise in the development of both face-to-face and online learning and was awarded the title of e-Learning Champion by the Australian Flexible Framework in 2009. The course and subjects he has developed range over all areas of post-secondary education from Certificate IV to undergraduate and postgraduate.
His areas of expertise include mental health, alcohol and other drugs, and change management within the health sector. In addition, Greg is very familiar with the capabilities of Web 2.0 applications and has developed many interactive online resources.
Linda RoseLinda is a social worker with over 30 years’ experience working in the community sector. With a broad range of expe-rience, she has primarily focused on young people and/or families with multiple and complex needs. Linda was involved in establishing one of the first refuges for homeless young people and continued for many years working with young men exiting prison. She has also worked in a homeless shelter in London.
Linda taught at Swinburne University for five years in the Department of Family and Community Services and was then employed for a number of years as a grief and loss counsellor. Here she counselled adults and adolescents bereaved through sudden and traumatic death and also facilitated support groups. Linda has been involved in establishing many new programs in non-government organisations and has expertise in development and delivery of programs in this part of the sector. Linda is currently the Improved Services Initiative Project Officer with a Victorian Project. She has expertise in project management and supporting staff through change. An accredited trainer, she is also skilled at building dual diagnosis ca-pacity with staff through delivering relevant training. Linda also facilitates individual and group supervision for workers, including training for supervisors.

Capacity Building and Change Management iii

Capacity Building and Change Management 1
CONTENTS
PART A: Introduction 3Introduction to this manual / 3Definitions and jargon / 4Background / 6Dual diagnosis policy context / 7
PART B: Dual diagnosis capability and capacity building 11What is capacity building? / 11What does a dual diagnosis capable organisation look like? / 11The dual diagnosis capable worker / 13
PART C: Related practice knowledge and skills 17Consumers and significant others / 17Key partners / 20Policies and procedures / 23Supervision and mentoring / 25
PART D: Change management 29Tools for change / 31Assisting people during change / 32Resistance to change / 35Applying change management / 35
PART E: Stages to build capacity 37Stage 1: Communicate and engage / 37Stage 2: Develop a plan / 40Stage 3: Implement the plan / 44Stage 4: Evaluate / 44Stage 5: Share your knowledge and experience / 46
PART F: Appendices 47 Appendix 1: Stakeholder analysis / 49Appendix 2: Resistance assessment survey / 51Appendix 3: Information sheet / 53Appendix 4: Action plan / 55Appendix 5: Communication plan / 57Appendix 6: Plan template / 59Appendix 7: Plan – Do – Study – Act (PDSA) project / 61Appendix 8: Framework checklist for implementing change and/or projects / 65Appendix 9: Further reading / 69References / 71

Capacity Building and Change Management2

Capacity Building and Change Management 3
PART A: INTRODUCTION
INTRODUCTION TO THIS MANUAL
PurposeThe purpose of this manual is to provide a brief ‘How to’ guide for applying change management processes, specifically in relation to adopting dual diagnosis capability within service delivery organisations. The manual will outline the rationale for change and provide you with the knowledge and tools you need to successfully implement change within your organisation.
This manual does not attempt to replace or replicate the many resources that are available on change man-agement, dual diagnosis capability or any other aspect of care. It does, however, draw out key elements from texts and advice from experts in the field to show how they may be useful when applying a change process to your agency. It is recommended that you also consider follow-up reading. Some references are provided throughout the manual to help point the way.
The practical steps outlined in this manual are designed to ensure that change management is carried out in a positive and effective way in your agency. The goal is to ensure that processes and strategies are developed and applied to actively demonstrate and promote the incorporation of sustainable dual diagnosis practices in service system delivery.
Who should read this manualThis guide is written for all managers and staff who wish to move their agency towards becoming dual diagnosis capable. There are usually one or more people in the organisation that drive the change process. This guide is primarily for them. However, everyone in the organisation should be familiar with the contents and processes described in the manual.
This is important because everyone who is involved in your organisation’s service delivery has a part in developing dual diagnosis capacity. From the beginning, it is important to involve all those with whom your service has contact. Exactly who this includes will differ from one organisation to the next. At the very least, the following groups and individuals should be included:
• consumers and significant others• staff/workers• senior leaders• clinical leaders• champions/portfolio holders• other agencies• external experts and specialists. How to use this manualYou will notice that the manual is divided into six main parts. These are designed to give you an overview of the key areas involved in dual diagnosis capacity building. Parts A, B, C and D provide information on various aspects of building capacity and change management. It is a good idea to start there.
Part E is a ‘how to’ section that gives you a step-by-step guide to building dual diagnosis capacity. A range of tools and resources is provided in the Appendices.
Part A: Introduction This is the part you are currently reading. It provides important background information about the context of dual diagnosis capacity building and how to use this manual to support your work.
Part B: Dual diagnosis capability and capacity buildingThis part gives you an idea of what to expect from your organisation if it is to be successful in building capacity to assist consumers with a dual diagnosis. It also discusses what attitudes, skills and knowledge are required for workers to become dual diagnosis capable.

Capacity Building and Change Management4
Part C: Related practice knowledge and skills This part provides an important overview of the range of other information you will need at your disposal. It includes tips for involving consumers and significant others in all aspects of your capacity building. It also gives some insight into strategic partnership management, policy and procedure development and the im-portance of supervision and mentoring for building capacity.
Part D: Change managementThis part gives you an overview of change management: the process itself, how to support your organisation to transition through change and how to positively and creatively deal with resistance.
Part E: Stages to build capacityThis is the ‘how to’ part of the manual. It takes you step-by-step through the stages of change management and capacity building and offers tips, templates, resource materials and links to help you through each stage.
Part F: AppendicesThis part provides templates and other tools to help you build and sustain your organisation’s dual diagnosis capacity.
Help and resourcesPart E of this manual contains a number of resource lists. Some of these materials can be found in the Ap-pendices or are listed in the References list at the back of this manual. Others are available online and the URL is included.
Many workers and organisations are already on the path to building dual diagnosis capacity. A great deal of knowledge, insight and support is available to you from those organisations that have been down this path before you. You are encouraged to contact similar services and support each other.
DEFINITIONS AND JARGON
Dual diagnosis / co-occurring disorders / co-morbidity / mental health and substance useA range of terms are used in varying degrees to articulate or ‘name’ the co-existence of mental health and alcohol and other drug problems.
For the purposes of this manual, we will use the term ‘dual diagnosis’ to describe the co-existence of mental health and alcohol and other drug issues.
However, we recognise that ‘dual’ can suggest that there are only two problems. In fact, many people have multiple needs. These might include one or more medical problems, disability, and/or a range of social issues such as housing, income, employment and social isolation. In practice, people are usually only given a formal diagnosis of dual diagnosis if they have severe mental health problems (generally psychotic disorders) and severe alcohol and other drug problems that meet the criteria for specialist services. The issue then arises of how to access appropriate care for those people whose problems, while distressing, are not considered ‘serious’ enough to meet the threshold for specialist care.
ConsumersWithin the health and welfare sector, consumers are also referred to as patients, clients, service users and customers. For consistency within this resource, we will use the term ‘consumer’.
Significant OthersWithin this manual, ‘significant others’ represents any person/s in a consumer’s life they consider significant. It includes carers, family and friends who are involved in supporting the consumer.
No wrong doorThe ‘no wrong door’ (NWD) approach is based on the principle that every door in the health care system should be the ‘right’ door. People are welcomed and treated with a non-judgemental approach. Each provid-er within the system has a responsibility to address the range of consumer needs wherever and whenever

Capacity Building and Change Management 5
a consumer presents for care. This approach provides people with, or links them to, appropriate services regardless of where they enter the system. NWD acknowledges that it is the responsibility of the engaged health service to navigate and negotiate the web of health providers on behalf of the consumer and to ensure seamless service delivery between agencies. NWD supports enhanced dual diagnosis capability and integrated assessment and care.
Mental health and AOD services implement a ‘no wrong door’ approach for people who present with co-occurring conditions. All are eligible to receive coordinated service delivery using an integrated approach with triage (intake), assessment, care coordination and treatment. The presence of either a mental health or alcohol and other drug condition does not constitute criteria for service exclusion.
Service coordinationIn the Victorian state health context, service coordination stems from the Better Access to Services Policy and Opera-tional Framework (DHS, 2001). Service coordination is a statewide approach to align practices, processes, protocols and systems through functional integration. Achieving functional integration enables organisations to remain independent of each other as entities and still work in a cohesive and coordinated way so that consumers experience a seamless and integrated response.
Integrated careIntegrated care entails the coordination of interactions and relationships within and across services in order to secure the best possible service system response for a person with dual diagnosis. It does not imply the structural realignment of service systems. • At the service level – a core feature of integrated care is the provision of mental health and AOD serv-
ices in a single setting, wherever possible. If this is not possible, linkage with services should occur via agreed clinical pathways.
• At the systems level – integrated care entails a focus on the provision of holistic and coordinated care, liaison and advice and the development of clinical pathways between and across a range of agencies. This is a prerequisite for the delivery of effective treatment for people with dual diagnosis.
Integrated assessmentIdeally, integrated assessment refers to the provision of a comprehensive mental health and AOD assess-ment by a single clinician or treatment team wherever possible. The next best option is the provision of a comprehensive assessment by two clinicians working within a collaborative arrangement from a mental health and AOD service setting. In this instance, assessment must be delivered seamlessly and complimenta-rily for the person receiving the service.
Integrated treatmentIdeally, integrated treatment refers to the provision of treatment for both mental health and alcohol and other drug problems by a single clinician or treatment team wherever possible. The next best option is the provision of treatment by two or more clinicians working within a collaborative arrangement. In this in-stance, treatment delivery must appear seamless to the person receiving the service.
Dual diagnosis capability/capacityDeveloping dual diagnosis capable staff is fundamental to the success of establishing services that are rel-evant for people with dual diagnosis.
• Capacity building in this manual means the capacity of an organisation to provide the services appro-priate to consumers with dual diagnosis and their significant others.
• Capability is the individual worker’s ability to assist consumers with dual diagnosis and their signifi-cant others.
Supervision Supervision is a formal process of consultation between two or more professionals. The focus is to provide support for the supervisee(s) in order to promote self-awareness, development and growth within the con-text of their professional environment (Hancox & Lynch, 2002).

Capacity Building and Change Management6
BACKGROUND
Why build capacity?Mental health (MH) and alcohol and other drug (AOD) services are working with increasing numbers of people who experience both mental health and drug and alcohol problems. The co-occurrence of these problems and disorders (dual diagnosis) adds complexity to service development and delivery.
Responding to consumers with complex needsIt is understood that dual diagnosis consumers are typically associated with poorer outcomes across a number of key life domains. Both the signs and symptoms of the disorders themselves and associated dis-abilities can have far-reaching and enduring consequences. Individuals experiencing co-occurring disorders have multiple and complex needs that require a high level of responsiveness across all service sectors and levels of care. Providing effective treatment and support requires an integrated approach to assessment, treatment planning and delivery, rehabilitation and recovery, and discharge.
The rationale for policy and practice changeTraditionally, the service sector has operated from a ‘specialist’ delivery model, designed to treat only one disorder or one disorder at a time. More recently, an increasing body of evidence has influenced a change in international, national and state perspectives and policy direction over the last 10 or so years.
This new approach creates dilemmas for traditional, single-treatment service agencies. It requires a philo-sophical change in the way the sector delivers its services. Policy now directs us to take an integrated ap-proach to service delivery.
Minkoff and Cline have observed that ‘dual diagnosis is the expectation, not the exception’ for the service sector (Minkoff & Cline, 2003).
People with dual diagnosis are the core business of both mental health and AOD services. The delivery of effective services, based on individual needs, relies on the provision of comprehensive, holistic, person (and their family) centred interventions (Queensland Government, 2008).
Barriers to integrated care The following factors highlight the need for agencies to become dual diagnosis capable.• Increasing numbers of people with dual diagnosis need and use services in each sector. Emergence of
dual diagnosis difficulties is occurring at an increasingly younger age.• Dual diagnosis is associated with poorer outcomes and increased risks to health and development over
time if not treated early and effectively.• Long-term benefits for individuals, their families and/or carers and communities can be achieved through
the early recognition and timely treatment of serious health problems such as dual diagnosis.• Services in each sector record significantly lower rates of dual diagnosis among those using their
services than would be expected from census and population surveys. This raises a number of concerns about recognition and response to dual problems in services as well as about the adequacy of routine data collection to inform service planning.
• Despite examples of good practice, mental health and AOD services typically continue to provide segre-gated services for dual diagnosis consumers, rather than integrated approaches to treatment and care.
• System barriers that impede integration of treatment, care and recovery (both centrally at a policy level and locally at a service level) need to be systematically addressed if outcomes for dual diagnosis con-sumers are to be improved.
(Department of Human Services, 2009)
What kind of change is needed?In response to this evidence-based policy direction, both the mental health and AOD sectors need to evolve to effectively respond to the needs of dual diagnosis consumers. All services and staff need to develop dual diagnosis capacity.
When considering the development of an able service system to meet the needs of consumers with co-occurring disorders, the evidence directs us to specific areas of focus:

Capacity Building and Change Management 7
Queensland Dual Diagnosis Principles
• development of effective collaborative partnerships • servicesystemplanninganddeliverytoreflectthatindividualswithdualdiagnosisare
the expectation, not the exception• an integrated care approach• a‘nowrongdoor’approach• development and maintenance of a therapeutic alliance• integrated service provision• a harm minimisation model• a recovery-based approach• bothpresentationsconsideredof‘primary’importance• acknowledgementofspecificconsiderationsfortheaged,youngpeople,Indigenous
people and people from culturally and linguistically diverse (CLD) backgrounds • activeparticipationoftheconsumer,carer,familyorsignificantother
• contribution of the community in recovery and support.
(Queensland Government, 2008)
• the attitudes and values of providers (dealing with stigma and resistance)• essential competencies for dual diagnosis able clinicians (basic, intermediate and advanced)• opportunities for continuing professional development towards an able workforce• service system development (a ‘no wrong door’ approach to concepts, policy and procedures)• partnerships with other services (meaningful and robust)• workforce development• supervision and mentorship.
Changes already madeIt must be stressed that many agencies and organisations across Australia have been working tirelessly to build dual diagnosis capacity over the years. There has been significant progress in some areas while, in oth-ers, the battle to ‘change’ the system continues to be an ongoing struggle.
Much of the information and many of the insights provided in this manual were gathered from the field. Some of those who contributed are battle-weary or battle-wary. Many have ‘walked the walk’ and continue to strive to ensure the messages are not lost on an ever-changing ‘health’ system. We hope that this manual will give you further assistance in helping those with a dual diagnosis.
DUAL DIAGNOSIS POLICY CONTEXT
Many states and territories in Australia now have dual diagnosis policies in place or are currently develop-ing them. In addition, national and international guidelines provide information on how services should care for people with a dual diagnosis. Below are some examples of policy in two states, Queensland and Victoria, as well as a summary of what is happening nationally and internationally. Other states and territories have or are in the process of developing dual diagnosis policy. For more information, contact your local state or territory health department.
STATE EXAMPLES
QueenslandQueensland Health has produced a policy document entitled Service delivery for people with dual diagnosis (co-occurring) mental health and alcohol and other drug problems (Queensland Government, 2008).It sets out the service requirements for dual diagnosis care within mental health and AOD agencies.
Twelve key principles are contained within the Queensland policy.

Capacity Building and Change Management8
VictoriaThe Victorian Department of Human Services (now Department of Health) policy is outlined in a document entitled Dual diagnosis: Key directions and priorities for service development. It lists five Service Develop-ment Outcomes (SDOs) that all mental health and AOD services must achieve.
Note: The Key Directions documents is, at time of print, under review and may be available under a new interation and a new name. More information should be available at: www.health.vic.gov.au
Victoria has a new Mental Health Plan: Because mental health matters, Victorian Mental Health Reform Strategy and Implementation Plan: 2009–2019. In this plan, the Victorian Government continues to articulate the need for an integrated service for people with mental health and alcohol and other drug issues. Dual diagnosis principles are articulated in the reform package via strengthening planning, governance and shared responsibility for service delivery within a number of key areas.
NATIONAL CONTEXT
Department of Health and Ageing: National Comorbidity Initiative
Australia’s National Comorbidity Initiative aims to improve service coordination and treatment outcomes for people with co-existing mental health and alcohol and other drug disorders. It focuses on the follow-ing priority areas:
Victorian Service Development Outcomes (SDOs)• Dualdiagnosisissystematicallyidentifiedandrespondedtoinatimely,evidence-
based manner as core business in both mental health and alcohol and other drug services.
• Staffinmentalhealthandalcoholandotherdrugservicesare‘dualdiagnosiscapable’;thatis,havetheknowledgeandskillsnecessarytoidentifyandrespondappropriatelyto dual diagnosis consumers. Advance practitioners are able to provide integrated assessment, treatment and recovery.
• Specialist mental health and alcohol and other drug services establish effective part-nerships and agreed mechanisms that support integrated assessment, treatment and recovery.
• Outcomes and service responsiveness for dual diagnosis consumers are monitored andregularlyreviewed.
• Consumers and carers are involved in the planning and evaluation of service re-sponses. (Department of Human Services, 2009)
Victorian Dual Diagnosis Principles
Reform Area 2: Early in life –improvedearlyidentificationandmentalhealthoutcomesforchildrenandyoungpeoplewithamentalillness
Reform Area 3: Pathways to care – righttime–rightplaceand‘nowrongdoor’servicedelivery
Reform Area 4: Specialist care – dual diagnosis capability Reform Area 6: Reducing inequality – dual diagnosis service provision Reform Area 7: Workforce and innovation – building system capacity and supporting innovative projects Reform Area 8: Partnerships and accountability – No Wrong Door principles (Department of Human Services, 2009)

Capacity Building and Change Management 9
• raising awareness of dual diagnosis among clinicians and health workers and promoting examples of good practice resources and models
• providing support to general practitioners (GPs) and other health workers to improve treatment out-comes
• facilitating and improving access to resources and information for consumers• improving data systems and collection methods within the mental health and AOD sectors to manage
dual diagnosis more effectively.
In 2009 the National Drug and Alcohol Research Centre (NDARC) published the Guidelines on the manage-ment of co-occurring alcohol and other drug and mental health conditions in alcohol and other drug treatment settings. These national guidelines were funded by the National Comorbidity Initiative and written to provide AOD workers with evidence-based information to assist with the management of co-occurring disorders. INTERNATIONAL CONTEXT
United KingdomThe UK Mental health policy implementation guide – dual diagnosis good practice guide clearly states that substance misuse is usual rather than exceptional among people with severe mental health problems and acknowledges that the relationship between the two is complex. Individuals with these dual problems deserve high-quality, consumer-focused and integrated care. This policy is referred to as ‘mainstreaming’. A key principle of this approach is that consumers should not be shunted between different sets of services or put at risk of dropping out of care completely. The guide points out that ‘mainstreaming’ will not reduce the specialist role of either AOD services or mental health services. Rather, it makes clear that unless people with a dual diagnosis are dealt with proactively in an integrated fashion, these services as a whole will fail to work effectively.
New ZealandSimilarly, the integration of mental health and AOD care has been a priority area in New Zealand for a number of years. This focus is reflected in a range of NZ health policies, including the most recent Te Kòkiri: The Mental Health and Addiction Action Plan 2006–2015 (Minister for Health, 2006). This plan identifies specific actions, key stakeholders and organisations responsible for coordinated care, outlines milestones and sets timeframes for achieving the 10 leading challenges identified in the Te Táhuhu (Improving Mental Health Strategy).
United StatesIn the US, the Substance Abuse and Mental Health Services Administration (SAMHSA) has been working in this area since 2002, when it submitted a report to Congress entitled The prevention and treatment of co-occurring substance abuse disorders and mental disorders.
This report, which included a ‘blueprint for action’, has lead the US towards best practice service delivery. SAMHSA’s mission is clear:
Since 2002 SAMHSA has developed a range of support documents and practice manuals to enable organi-sations to build their dual diagnosis capability. The most relevant of these is the Treatment Improvement Protocol Series (TIP 42) (Center for Substance Abuse Treatment, 2005).
The agency will enhance its leadership to create systems that put people first. It will provide incentives including training, technical assistance and discretion-ary funds to increase integrated substance misuse and mental health approach-es in both settings and encourage the appropriate integration of medication and psychosocial treatment approaches. These actions will support co-occur-ring capacity enhancement by developing performance measures based upon prevention, screening, assessment, treatment, training and evaluation.
(SAMHSA, 2002)

Capacity Building and Change Management10
• Language is important – but don’t get stuck on terminology/definitions. This is about holistic responses to meet identified needs of individuals, families and communities.
• Know the current state and federal policy that relates to dual diagnosis for your agency.
• Be familiar with the literature. Evidence clearly articulates the need for the sector to build its capacity to provide integrated screening, assessment and treatment in relation to mental health and alcohol and other drug issues.
• Understand consumer and significant other expectations. Consumer and significant others are adamant that they do not wish to be treated by discrete multiple services. They expect a team approach.
Helpful Tips

Capacity Building and Change Management 11
PART B: Dual diagnosis capability and capacity building
WHAT IS CAPACITY BUILDING?
Capacity building is a process that improves the ability of a person, group, organization, or system to meet objectives or to perform better.
LaFond and Brown (2003)
Resources are invested in different aspects of the health sector with the ultimate aim of enhancing health system performance and improving the health of populations. Translating these resources into sustained performance often requires new or improved capabilities in individuals and organisations operating within the health sector. Capacity represents the potential for using resources effectively and maintaining gains in performance with gradually reduced levels of external support.
Capacity and capabilityUsed alone, the term ‘capacity building’ is intangible and vague. What constitutes capacity building in practice can vary enormously and the concept continues to develop as field experience grows.
Initially many agencies equated capacity building with training. If there was a gap in performance, the solu-tion was often to hold a workshop to ‘retrain’ or ‘refocus’ the workers. We now know that individual skills are only one part of the complex mix of elements that constitute capacity to perform a certain function or groups of functions effectively and consistently over time.
In this manual, we use the following definitions:
• Capacity – the capacity of an organisation to provide the services appropriate to consumers with a dual diagnosis and their significant others.
• Capability – the individual worker’s ability to assist consumers with a dual diagnosis and their signifi-cant others.
Building capacityCapacity building and capability are obviously linked and cannot exist without each other. To effectively build capability and capacity, an organisation needs:• good quality educational programs for workers• quality supervision and mentoring• an internal infrastructure that supports the development of capacity and capability.
Specific areas of capacity and capability may differ in the various sectors (AOD, mental health and psycho-social rehabilitation). Within those sectors, there will also be subsets of ‘capability’. For example, in the AOD sector, the dual diagnosis capability of staff in the withdrawal unit will be different to the dual diagnosis capability of an intake worker.
WHAT DOES A DUAL DIAGNOSIS CAPABLE ORGANISATION LOOK LIKE?
Minkoff and Cline (2006) define dual diagnosis capability and organisational capacity in this way:
The evolving concept of dual diagnosis capability refers to the notion that every agency/program providing behaviouralhealthservicesmusthaveacorecapacity,definedthroughspecificcomponentsofprogram infrastructure like policies, procedures, clinical practice instructions and standards, and clinician competencies and scopes of practice, to provide appropriate services to the individuals and families with co-occurring men tal health and substance use issues who are already coming through its doors.
Dual diagnosis capable programs typically:• address dual diagnosis in their policies and procedures, assessment, treatment planning, program content
and discharge planning

Capacity Building and Change Management12
• have arrangements in place for coordination and collaboration between mental health and AOD services• can provide psychopharmacologic monitoring and psychological assessment and consultation, either
onsite or through coordinated consultation off-site• have staff that are able to address the interaction of the substance-related and mental disorders in as-
sessing the person’s readiness to change, relapse risk and recovery environment.
Six guiding principles have been identified for treating consumers with a dual diagnosis:
1. Employ a recovery perspective.2. Adopt a multi-problem viewpoint. 3. Develop a phased approach to treatment.4. Address specific real-life problems early in treatment.5. Plan for the consumer’s cognitive and functional impairments. 6. Use support systems to maintain and extend treatment effectiveness.(Centre for Substance Abuse Treatment, 2005)
Who is involved in capacity building?Capacity building inevitably involves a process of transition (or change) that may need careful management. Nickols (1990) describes change management as ‘the task of managing change in a planned and managed fashion’. Most literature describes the importance of all involved in the change process being involved in open and honest communication. The literature specific to the public health sector stresses the importance of involving a broad range of stakeholders. Part D of this manual looks in more detail at the processes of change management.
Everyone who is involved in your organisation’s service delivery has a part in developing dual diagnosis capacity. From the beginning, you will need to involve all those with whom your dual diagnosis service has contact. Exactly who this is will differ from one organisation to the next but, at the very least, Maher et al (2003) suggest the following groups and individuals should be included in all aspects of capacity building:• consumers and significant others• staff/workers• senior leaders• clinical leaders• champions/portfolio holders• other agencies• external experts and specialists.
How to engage these key players and what role they have in your capacity building process is discussed in more detail in Part C of this manual.
Importance of communicationEffective and open communication throughout the organisation is essential if there is to be a building of capacity. Communication needs to be two-way with all workers and management.
This may involve meetings or a range of other communication activities with staff and managers over a period of time to:• seek their ideas and support• inform them of the plans• update on the process• hear about any issues • brainstorm solutions.
The literature supports this need for communication and suggests that some common elements are re-quired for successful change management. These include: • a perceived need for change• strong, continuous and full-circle communication from and to all levels of the organisation

Capacity Building and Change Management 13
• building strong partnerships and coalitions to drive the change a coherent, adaptable and achievable plan• a commitment from all levels of the organisation to implement the plan.
Process for capacity building Minkoff and Cline (2006) suggest that typical starting places in most behavioural health agencies or pro-grams may include the following capacity-building activities:
1. Establish the baseline dual diagnosis capability (DDC) of each program in the agency (both routine and specialised programs) as the first step in initiating a quality improvement process.
2. Formally demonstrate commitment of the organisation to dual diagnosis capability as an agency-wide goal. 3. Develop a formal philosophy that welcomes consumers with complex needs.4. Establish a process (or role) within the agency which is responsible for the implementation of dual
diagnosis capacity building, including regular reviews of the agency’s dual diagnosis capability through continuous quality improvement.
5. Incorporate the consumer perspective in design, delivery and evaluation of dual recovery oriented services. 6. Identify and count the co-occurring disorder population and track individual service needs, including
populations that have poor outcomes and high costs that ‘fall through the cracks’.7. Clarify billing and documentation instructions for integrated services using existing funding streams. 8. Improve access to integrated assessments.9. Develop integrated treatment planning protocols that support interventions appropriate to a person’s
stage of change or stage of treatment and develop programmatic materials and structures (for example, groups) to organise the provision of those interventions more easily.
10. Develop procedures and protocols for interagency care coordination and collaboration. This will help facilitate the ability of each agency to assist the other to provide dual diagnosis capable treatment and to provide each clinician with clear instructions about how to coordinate care.
11. Develop core-integrated scopes of practice for singly trained mental health and AOD clinicians.12. Design and implement strategic training plans, where training is aligned with the development of sup-
portive infrastructure to implement new clinical practices.
THE DUAL DIAGNOSIS CAPABLE WORKERThere has been a great deal of discussion and literature about what dual diagnosis capability is and how we know if a worker has achieved it.
Capability of staff can be divided into three levels:• basic competence• intermediate competence• advanced competence.
At a basic level, the literature suggests that an ability to welcome and engage with the consumer is essential. All three levels can be measured through a range of other skills and knowledge that include:
ABILITY TO WELCOME AND ENGAGE WITH THE CONSUMER
Conceptual and theoretical issues (AOD/MH) Screening and assessment of dual diagnosisRisk assessment Knowledge of service system (AOD/MH)Relationships between AOD & MH disorders Symptoms and classifications of mental health dis-
ordersEffects of drugs and drug use Withdrawal/intoxication managementTreatment strategies (AOD/MH) Pharmacology (MH/AOD)Integrated treatment Partnerships between AOD/MH servicesReferral pathways Policy/LegislationSubjective & objective client outcome measures

Capacity Building and Change Management14
Essential areas of competenceRecently Graham and White (2011) described the ‘comorbidity competencies’ that they believe are essential to assist consumers with dual diagnosis. They described three overarching areas that must be addressed:
• Essential knowledge – important information and knowledge that anyone working with dual diagnosis consumers should possess. This includes a basic level of understanding and skills.
• Core practice skills – those skills that most productively assist practitioners to effectively work with dual diagnosis consumers.
• Specialist skills and leadership – attributes required for higher level work or management tasks in rela-tion to improving services for dual diagnosis consumers.
How to produce dual diagnosis capable workersThere are many paths to becoming dual diagnosis capable and these should be guided through a well-articu-lated workforce development process. This is a key part of your capability plan.
Workforce development is more than training. It includes a broad range of strategies targeted at systemic or structural issues, organisational issues and individual issues. These strategies include recruitment policies, remuneration, supportive management practices and policies, workplace learning opportunities and career pathways, training opportunities, supervision and mentoring, and staff exchanges. Local partnerships can also help foster these arrangements and open doors to staff exchanges and other joint strategies.
Even when there are few avenues to increase resources, workforce development can support improved service quality and staff retention by encouraging the professional development of staff. To achieve this, there needs to be a clear commitment by managers, governing bodies and staff. A more detailed definition of workforce development can be found on the National Centre for Education and Training on Addiction (NCETA) website at www.nceta.flinders.edu.au
As mentioned, there are a number of different pathways workers can take to become dual diagnosis capable. These may include:• educational programs• recognition of prior learning• self-assessment checklists• supervision and mentoring• observation and assessment of specific skills• a combination of any or all of these.
It is recommended that an audit of staff training needs be carried out across the organisation, using one of the dual diagnosis capability tools, and that individual development programs be developed to address specific needs.
These programs may include group training, but should also include mentoring and supervision to ensure skills and knowledge are transferred to the workplace.
Supervision and mentoringSupervision and mentoring are key professional skills that also provide useful strategies for developing dual diagnosis capable staff. Supervision aims to develop an improved service to consumers by ensuring effective performance among practitioners. Workers have the opportunity to stand apart from their work and reflect on what they do, the context in which they do it and the impact this has on the consumer and on themselves.
Mentoring is when a trusted and experienced staff member helps a colleague who has less experience. The goal is to help people reach their full potential, build confidence and provide guidance where necessary.These key areas of professional development are discussed in greater detail in Part C of this manual. The important thing to understand is that training alone will not create a dual diagnosis capable worker.
Workforce development is a multifaceted approach, which addresses the range of factors impacting on the ability of staff to function effectively.
(NCETA, 2001)

Capacity Building and Change Management 15
Effective transfer of knowledge into practiceNCETA in their three-part series on effective dissemination (Bywood et al 2008) examined 16 strategies of transferring knowledge into practice, which included:• Educational materials • Local consensus processes • Educational meetings (CME) • Educational outreach (academic detailing) • Local opinion leaders • Patient-mediated interventions • Prompts and reminders • Audit and feedback • Financial incentives• Electronic educational sources
The strategies that were found to be the most consistently effective were:
Educational meetings (interactive)This is where healthcare providers participate in conferences, lectures, workshops or traineeships It was found the Interactive Workshops were much more effective than didactic lectures and seminars
Education OutreachUse of a trained person who meets with providers in their practice setting to give information with the intent of changing the provider’s practice.
Prompts and reminders Patient- or encounter-specific information, provided verbally, on paper, or on electronically, which is de-signed to prompt a health professional to recall information. This usually occurs through general education, in medical records or by interactions with peers, reminding them to perform or avoid some action to aid individual patient care. Computer-aided decision support and drugs dosage are included.
Audit and feedbackAny summary of clinical performance of healthcare over a specified period. The summary may also include recommendations for clinical action. The information may be obtained from medical records, computerised databases or observations from patients.
Available from the VAADA Comorbidity Website: www.comorbidity.org.au• VDDI Dual Diagnosis Capability Discussion Paper• Graham H & White, R. (2011) Comorbidity competencies: Skills indicators.
University of Tasmania.• Minkoff, K., & Cline, C. Various articles.• Bywood, P.T., Lunnay, B. & Roche, A. M. (2008). Effective dissemination:
An examination of the costs of implementation strategies for the AOD field. National Centre for Education and Training on Addiction, Adelaide.
Support Materials
Helpful Tips
• From the beginning, involve all who may be stakeholders.• Effective and open communication is essential.• Establish a baseline. • Define essential knowledge, core practice skills and specialist skills and leader-
ship for your organisation.• Source supervision, mentoring and workforce development resources from
within or outside your organisation.• Utilise Educational meetings (interactive), Educational outreach, Prompts and re-
minders and Audit and feedback as your prefered method of knowledge transfer

Capacity Building and Change Management16

Capacity Building and Change Management 17
PART C: Related practice knowledge and skills
CONSUMERS AND SIGNIFICANT OTHERS
Within the health and welfare sector, consumers are also referred to as clients, service users, patients and customers. For consistency within this resource, we use the term ‘consumer’.
Consumer and significant others are willing, prepared and able to be part of the policy and decision mak-ing at all levels of the health process: from strategic planning through to service delivery. The participation of consumers and significant others in the mental health and AOD sectors is not just an idea, it is an active imperative. There is no longer a debate about validity of participation … it just is.
As you begin working towards building your agency’s dual diagnosis capability, now is the time to include consumers and significant others in all aspects of your capacity-building process.
Recommendations from those who knowConsumers and significant others can provide valuable feedback and information to enhance your work. It is im-portant to listen to their recommendations and consider how you can include them at all levels of your service.
Here are some of the things that Victorian consumers and significant others are saying.
Policy supports participationThe Victorian Department of Human Services policy statement, Dual Diagnosis: Key Directions and Priori-ties for Service Development (DHS, 2007), notes that the participation of consumers and their significant others in service development and design is recognised as good practice and a key to the success of pro-grams. It dedicates one of the five key priority areas in the Victorian Government platform to consumer and significant other engagement.
The National Action Plan on Mental Health (COAG, 2006) states: People with mental health problems and mental illness have the same rights as other Australians to full social, political and economic participation in their communities.
1. We know what works for us.2. We would like to be included in planning.3. Please look at us, the consumer, as a whole person.4. We only want to tell our story once.5. We do not want to be transferred from one place to another.6. We would like you to work together with all the other agencies that need to be
involved in our care.7. Please help us with our children and other family members, so that their needs are
met and they understand what is happening.8. Although you may not understand my culture, please be sensitive to my needs regardless.9. My journey to recovery may not fit your timeframes, but it does fit mine.10. I would like a service that fits in with my needs rather than me having to fit in with
the service’s needs.
Victorian, Hume Health Region: Consumer and Carer Representatives Forum, March 2011
Key Priority Area 5: Consumers and carers are involved in the planning and evaluation ofserviceresponses.Theinvolvementofclients,familiesandcarersintheplanning,review
and ongoing development of services is a requirement of quality service provision.

Capacity Building and Change Management18
The National Mental Health Statement of Rights and Responsibilities was adopted by the Australian Health Ministers in 1991 and articulates the need for: … participation in decision making regarding the development of mental health policy, provision of mental health care and representation of mental health consumer interests. (Department of Community Services and Health, 2000)
What is consumer and significant other participation?In their publication Straight from the source: a practical guide to consumer participation in the Victorian alcohol and other drug sector, Miriam Clarke and Regina Brindle define participation as the process of involving health consumers (and significant others) in decision making about AOD service planning, policy development, priority setting and quality in the delivery of health services.
Participation in the sector consists of including consumers and significant others in the decision-making processes around:• their own treatment• service planning, development, delivery and evaluation• policy and research• education and training of professionals.
This is reflected within the mental health sector through the Strengthening Consumer Participation in Victoria’s Public Mental Health Services: Action Plan (DHS, 2009). This action plan describes three levels for promotion of consumer participation.
Consumer Participation in Victoria’s Public Mental Health Services
1. Individual level – consumers are involved with the mental health service systems for direct treatment and support with their mental illness/psy-chiatric disability. Active consumer involvement is encouraged to ensure appropriate support and services are in place. This provides for an overall recovery-focused approach.
2. Local service level – through a number of mechanisms, consumers can participate in the planning, delivery and evaluation of local services. Par-ticipation at this level can be important for individual consumers’ health outcomes and also contributes to the improvement of local services as they are informed and shaped by consumers’ perspectives.
3. Systemic level – mental health services are an element of the broader mental health service system. At a systemic level, consumers importantly par-ticipate in the planning, development and evaluation of statewide initiatives and policies. (DHS, 2009)

Capacity Building and Change Management 19
Levels of participationDifferent modes of participation are sometimes represented as a continuum. Brager and Specht (1973) have developed one such continuum, known as the ‘Ladder of Participation’ (See Table 1 below). It ranges from ‘no participation’ through minimal levels (where consumers receive information but have little say in deci-sion making) through to joint planning and ultimately to consumer or community control.
Clarifying the ideas and assumptions that are guiding your practice of participation is an essential undertak-ing because participation can operate at different levels and may be motivated by contradictory intentions. Agendas are varied. Consumers can demand participation for a range of reasons that may or may not be similar to what your organisation has in mind.
This is why it is important to consult with consumers and significant others at an early stage to establish what capacity and level of participation the consumers can provide and how this compares with what your organisation is seeking.
Table 1: Ladder of participation
Adapted from: Brager & Specht (1973)
Participation in workforce developmentInclusion of consumers and significant others in the development and delivery of education and training for staff will assist in the ongoing development of a better understanding of the service system from their lived experience.
Consumer and significant other representatives (whether in an employed, voluntary or advisory role) also require capacity building and workforce development to enable them to be skilled and confident in achieving their roles and providing for their constituency.
Existing structure and mechanisms for consumer and significant other input into the planning and evaluation of services will need to be reviewed to ensure that they reflect these new directions.
Organisation presents a plan and invites questions. Prepared to modify plan only if absolutely necessary.
Degree Participants Action
Overview
Have Control
Organisation asks community to identify the problem and to make all the key decisions on goals and means. Willing to help community at each step to accomplish goals.
LOW
HIGH
None
Have delegated
Planjointly
Advise
Are Consulted
Organisation identifies and presents a problem to the community, defines the limits and asks community to make a series of decisions, which can be embodied in a plan it can accept.
Organisation presents tentative plan, subject to change and open to change from those affected. Expects to change plan at least slightly and perhaps more subsequently.
Organisation tries to promote a plan. Seeks to develop support to facilitate acceptance or give sufficient sanction to plan so administrative compliance can be expected.
Community not involved.

Capacity Building and Change Management20
Meaningful participationParticipation must be meaningful if it is to be at all useful. While engaging consumers in decision making aboutservices, policy, education and research may be a difficult task, it cannot be done if service providers and professionals are unwilling to change their current work practices.
Clark and Brindle (2010) suggest the following guidelines to ensure effective consumer participation:• Be clear about your organisation’s capacity to involve service users and to respond to service user
concerns.• Be careful not to promise what you can’t deliver.• Ensure that productive consumer participation is supported by management at all levels.• Be prepared as an organisation to listen to feedback, make decisions and accept any changes.• Understand and manage conflicts. Enhanced consumer participation can mean that tensions emerge
from time to time. This is okay and is likely to lead to better quality service and improved outcomes in the long term.
• Encourage dialogue and trust in your partnerships with service users. Trust is built by transparency and consistency.
• Engage service users early in the process – even in the process of deciding how your organisation will engage service users better.
KEY PARTNERS
Strategic partnerships can make or break the successful implementation of agency capacity building and dual diagnosis service delivery. It is important to identify your key partners and make sure they have a truly collaborative approach to implementation. The Victorian dual diagnosis policy (DHS, 2007) lists a key service development outcome as:
It is important to bring consumers and significant others ‘along for the ride’ when developing and imple-menting dual diagnosis capacity. Open and honest communication is critical. Those that are affected by change need an opportunity to hear the information, participate in the decisions, planning, implementation and review of the change itself. There is also the added benefit of maximising the ideas, potential strengths and skillsets of partners and key staff if they are informed and involved at the operational level.
Remember, leadership is not about managing things, but about developing your people. Do not assume that you know it all.
Who and whyLiterature specific to the public health sector stresses the importance of involving a broad range of key partners and stakeholders for successful dual diagnosis capacity building (Maher et al, 2003). Experience has shown that developing the plan in a consultative manner assists in achieving more effective implementation.
• Involve consumers from the start• Ascertain the level of participation consumers can provide and that the
organisation requires.
Support Materials
Helpful Tips
Available from the VAADA Comorbidity Website: www.comorbidity.org.au • Clarke, M. & Brindle, R. (2010) Straight from the source: a practical guide to
consumer participation in the Victorian alcohol and other drug sector
… specialist mental health and alcohol and other drug services establish effective partnerships and agreed mechanisms that support integrated assessment, treatment and care.

Capacity Building and Change Management 21
It is recommended that the following key partners are included as an integral part of the process. These are not listed as options but are all, as a collective group, key to successful capacity building.
CONSUMERS AND SIGNIFICANT OTHERS Better outcomes for consumers are often the motivation for changing work practice. However, it is important to realise that consumers and significant others are also great allies to the or-ganisation in maintaining sustained change. Consumers and significant others need to be kept informed about the imminent and ongoing changes and enlisted to support the change process. Consumers and significant others more often know about what changes need to take place.
CLINICAL LEADERS
The engagement of clinicians in the redesign and improvement of services is an important factor in ca-pacity building. A clinical leader is a person with a clearly defined role to activate, stimulate, nurture and sustain service improvement. Successful clinical leaders have legitimacy among their clinical colleagues and are opinion leaders.
CHAMPIONS/ PORTFOLIO HOLDERSThere will always be a need for someone to take the lead on capacity building and managing change within the organisation. This ‘champion’ will be the one who is committed to not only the process, but also to communicating effectively with all stakeholders, identifying any issues and eliciting strategies to overcome those issues.
EXTERNAL SPECIALISTS Many agencies have been working slowly towards dual diagnosis over the last 10 years or more. Within this context, change management is a process that all agencies have to tackle.
There are many experts or specialists who have ‘walked in your shoes’ and can provide mentorship and support. Their lived experience and learnings are extremely valuable to an agency seeking to embrace a new dual diagnosis vision. A number of services have engaged in developments aimed at more systemic dual diagnosis capacity building, which can also provide valuable learning for others about to embark on this task.
Staff education and training is a core tool in building capacity. It is essential that there is involvement and consultation with relevant training organisations, providers and institutions about how best to deliver the education and training your staff need.
STAFF/ WORKERS
Staff need not only to be aware of the change process, but be actively engaged in it. They need to play an active part in the innovation, design and implementation of the process. It is important to include regular meetings and other communication forums through which staff are able to express their con-cerns, accomplishments and ideas. While achieving better outcomes for service users is often good motivation for change, staff need to be made aware that there will be benefits for them as well. This may include a reduction in duplication of work, improved efficiency or better working conditions
SENIOR LEADERS/ MANAGERSSenior leaders must be involved in capacity building for dual diagnosis. This may include managers all the way up to the CEO or Director. Their engagement, support and promotion of the process is invaluable and helps to ensure that staff will continue the process of change.

Capacity Building and Change Management22
OTHER AGENCIES Dual diagnosis, by its very definition, means the co-occurrence of mental health and alcohol and other drug problems. Service response and working relationships need to address this co-occurrence. Agencies that may be key players in your capacity-building process could include:• public and private mental health services• alcohol and other drug services• psychiatric disability and rehabilitation services• community health services• general practice• police and forensic services• housing and homelessness services• specific culturally appropriate services related to your agencies catchment area• age-specific services (youth, adult or older persons services).
How to engage key partnersOne of the key elements of successful dual diagnosis capability building is effective partnerships with key part-ners. The engagement of these key partners at the earliest opportunity and at a meaningful level is important.
Deciding on the partnershipDeciding who to partner with is particularly important. Carefully consider your answers to the following questions:• Who would you need to engage for successful dual diagnosis capacity building? • What is their vested interest in this? What is their stake/impact/needs in the change outcomes?• Have you included consumer and significant others? • Who would be your supporters?• Who will be your barriers? What would it take to get their support and have them working actively
with you?• Do you require support from fund holders or policy developers?• Do you require a dual diagnosis or change management consultant to help you get started? • Do you need to conduct some activities to align or join the partnership?• How often does this group or partnership need to meet? What are the Terms of Reference for this
group?• How will the partners define success? Ovens and King Community Health Service 2010
Communication processQueensland Health has published a ‘how to guide’ of change management. In this guide, they describe the importance of an effective and ongoing communication process. They suggested a range of strategies for ensure effective communication is achieved.
STRATEGIES FOR EFFECTIVE COMMUNICATION
• Consider what will need to be communicated and by whom?• Establish a formal consultative process that involves representatives of all stakeholder groups. Deter-
mine what is negotiable and what is not and why this is the case.• Keep people informed of ongoing changes as often and using as many channels as possible – when,
why, how? Work collaboratively with opinion leaders, sponsors and funders, stakeholders and staff when developing the communication process. It is important to allow all those involved to determine what this should look like.
• Emphasise messages by using credible, respected spokespersons that are trusted and liked.• Top down, bottom up communication should be the same. Everyone gets the same message.• Consider what you would want to know (usually staff would like to know what is in it for them and
how can they contribute).

Capacity Building and Change Management 23
• Build in a means by which those that are affected by the change have a forum or opportunity to raise concerns early. This ensures their fears are heard and addressed before they have a chance to grow.
• Build in a ‘no secrets/no surprises’ rule wherever and whenever possible.• If you don’t know something, say that you don’t know.• If you don’t act on people’s suggestions, make sure you explain the reasons why.• Allow yourself to be human and make mistakes. Deal with the mistake, acknowledge it, apologise and
make amends.• Celebrate and promote success. Take opportunities along the way to celebrate small achievements as
well as the major milestones.• Acknowledge all stakeholders and their input in key documents, presentations, reports and communication
POLICIES AND PROCEDURES
Effective policies are the foundation for consistent quality practice in service delivery. Comprehensive policies ensure that:• all stakeholders have the same understanding and expectations about what happens in the agency• staff have a reference point where agency expectations are articulated to guide practice • there is a record of accountability for certain decisions made by staff, significant others and management.
How does a policy help?Policies and procedures are the strategic link between an agency’s vision and its day-to-day operations. Well-written policies and procedures allow employees to understand their roles and responsibilities within predefined limits and allow management to guide operations without constant management intervention.
Difference between policy and procedureA ‘policy’ is a predetermined course of action established to provide a guide toward accepted agency strate-gies and objectives. Policies identify the key activities of the organisation and provide a general strategy for staff on how to handle issues as they arise.
A ‘procedure’, on the other hand, aims to provide the reader with a clear and easily understood plan of action for what is required to carry out or implement a policy. A well-written procedure will also help eliminate common misunderstandings by identifying job responsibilities and establishing boundaries for the employees in specific roles.
POLICY PROCEDURESIs general in nature Identifies specific actionsIdentifies company rules Explains when to take actionsExplains why they exist Describes alternativesTells when the rule applies Shows emergency proceduresDescribes who it covers Includes warning and cautions
• Include all key partners from the beginning.• Get to know your partners. Understand their work context, their environment
and their culture. For example, it is important that the mental health sector understand the working context of their AOD sector cousins (and vice versa).
• Ensure both top-down and bottom-up involvement.• Ensure you consider the needs, strengths and limitations of all your key partners.• Remember, relationships take time to build but it is a worthwhile investment.• Recruit an external facilitator to help build and expand the partnership.• Formalise the partnership through written agreements (for example, MoUs, ToR
and so on).• Ensure you set regular meetings and regular review points.
Helpful Tips

Capacity Building and Change Management24
Shows how the rule is enforced Gives examplesDescribes the consequences Shows how to complete formsIs normally described using simple sentences and paragraphs
Is normally written using an outline format
In relation to capacity building for dual diagnosis, each core change embedded into an agency will need to be reflected in agency policy and procedures.
It is important to note that a policy and procedure manual may be designed as either:• a combined document• two separate documents.
Policy to build capacity Most capacity-building strategies and activities will have an impact on current policy and require the revision of your organisation’s policy and procedures. Policy adaptation and review should be considered right at the beginning, when you are first developing your implementation plan.
There are many policy examples and templates available for you to use as a guide in developing policies that are relevant to your specific needs and context. A number of peak bodies maintain a variety of policy exam-ples and templates for the AOD sector to download. An example of this is the NADA Policy Toolkit (NADA, 2010). This resource is designed to guide non-government AOD services to develop and review operational policy documents and support their formal quality improvement program. The resource provides practical policy development templates related to governance and leadership, administration and support, and service delivery.
Clinical policy areasCommon areas of clinical policy that will need to be reviewed, updated or developed include:• overall philosophy of the agency (‘no wrong door‘, welcoming to all)• intake• screening and assessment• case formulation• shared care/integrated treatment and care• clinical review• crisis• secondary consultation• discharge.
Process policy areasCommon areas of process policy that will need to be reviewed, updated or developed include:• ‘no wrong door’ (protocols and pathways)• minimum standard and capability for recruitment of staff• clear role delineation and definition for specialist staff (for example, portfolio holders)• tools (shared and common tools)• supervision (individual and group, managerial and clinical)• peer networks (portfolio holders groups)• workforce development.
Communicate policy changesOnce your policies have been updated, all staff and stakeholders will need to be informed of changes and supported to implement them correctly. This may be done through normal meeting and communication processes or through more formal means such as staff in-service activities.
• Your current agency policy and procedure manual Available from the VAADA Comorbidity Website: www.comorbidity.org.au
• NADA Policy Toolkit (also at www.nada.org.au)• No Wrong Door Protocol (also at www.nowrongdoor.org.au)
Support Materials

Capacity Building and Change Management 25
SUPERVISION AND MENTORING
Supervision and mentoring are essential skill and role development strategies for health professionals. They are also useful strategies to employ when developing dual diagnosis capable staff and supporting staff through a change process.
For many agencies, dual diagnosis portfolio holders are those who provide supervision and mentorship to the sector as well as lead agency innovation and change management.
Supporting your staff
Supervision Ultimately, the primary aim of supervision is to develop an improved service to consumers by ensuring ef-fective performance among practitioners. This is done, in part, by providing the opportunity for workers to stand apart from their work and to reflect on what they do, the context in which they do it and the impact that this has on the consumer and on themselves – as people and as professionals.
Supervision has been a core practice for many years in a variety of settings. The following list are the key components of supervision:• skills development• education and training• support• theory development and practice integrations• role development• modelling• quality assurance.
It is well documented that staff in clinical positions require regular supervision from experienced and trained supervisors. It is common practice for mental health, psychiatric disability and rehabilitation support, and AOD services to engage their staff in supervision processes that are supported by organisational poli-cies and procedures. This ensures a shared understanding among all staff of the professional and organisa-tional expectation for supervision, as well as the function, process and structure it will provide.
MentoringMentoring is when a trusted staff member, with experience and expertise, helps a colleague who has lesser experience. The goal is to help people to reach their full potential and to build confidence and provide guid-ance where necessary.
The mentor may be a supervisor, experienced co-worker or portfolio holder.
Mentoring involves observing and monitoring the performance of the skill or task and giving feedback. This feedback cycle can be performed multiple times. An example is when a mentor observes the implementa-tion of a screening and assessment tool by a mentee and then provides feedback and suggestions for skill building.
• Understand the policy and process challenges you face. Consider which policy and procedures you may need to adapt and review as part of your implementa-tion plan.
• Aim to develop practical, clear tools that are relevant to your specific needs and context. You may find it helpful to use support materials (such as the NADA Policy Toolkit) to help you think about all areas of your activities.
• Don’t reinvent the wheel … use policy examples and templates from other organisations or capacity building experts to guide your own.
• Inform all staff of changes to policy and procedures and support them to imple-ment the changes correctly.
Helpful Tips

Capacity Building and Change Management26
Benefits of supervisionWhen done well, supervision reduces levels of staff burnout, increases job satisfaction and promotes quality practice. Coleman (2002) suggests that supportive supervision is concerned with increasing job perform-ance by decreasing job-related stress that interferes with work performance. The supervisor increases the worker’s motivation and develops a work environment that enhances work performance.
Munson (2002) also noted that workers identified good, supportive supervisors as the main source of help in dealing with stress. Experienced supervisors with an understanding of stress (its causes and cures) avoid the temptation to offer instant advice with simplistic solutions that do not work and often increase the worker’s distress.
Barriers to supervisionJohn Challis (2011) names a number of barriers to supervision, including:• lack of management support, where supervision is not a priority for management and so staff are subtly
or overtly discouraged from taking the time required • lack of skills among supervisors (untrained or unexperienced)• time limitations available for supervision• staff not understanding or seeing the benefits of supervision• lack of outcome-based supervision – untrained supervisors may not be able to assist practitioners to
develop new skills and solve problems.
Supervision should be targeted to the needs of the supervisee and to the skillsets that will help them to improve their work practice. This could include discussions of theoretical frameworks that help to inform practice, an exploration of feelings and work experiences, role playing, appropriate interventions and coun-selling techniques, discussion of work scenarios, motivational interviewing and developing ways of providing an integrated response to consumers with dual diagnosis.
Different roles or aspects of supervision
1. Administrative/management supervisionA manager who is responsible for the overall performance of a team or program provides this. Administra-tive matters relating to service planning, development and delivery are addressed by ensuring that program activities are carried out in a manner that is consistent with funding and legislative requirements, job de-scriptions, work plans, external policy directions and internal policies and procedures.
2. Clinical supervision (individual or group)Clinical supervision can be provided within a group context or through a one-to-one relationship. The focus is on the delivery of clinical practice and the challenges and learnings that the clinician experiences. Supervi-sion is a formal process of consultation between two or more professionals. The focus is to provide support for the supervisee(s) in order to promote self-awareness, development and growth within the context of their professional environment (Hancox & Lynch, 2002).
Group supervision provides an opportunity for supervisees to experience mutual support, share common experiences, solve complex tasks, learn new behaviours, participate in skills training, increase interpersonal competencies and increase insight. The essence of group supervision is the interaction of the supervisees (MacKenzie, 1990).
Collegial supervision allows for a further development in the way supervision is provided. It can focus on a specific professional body, a specific skillset or specific training content. Collegial supervision is where col-leagues work together and offer one another feedback on their practice. An example of this is a group of clinicians meeting to consolidate their newly acquired skills in motivational interviewing or a project man-agement group meeting regularly to discuss the implementation of their funded projects.
3. Project management supervision, mentoring and supportProject management support is useful in addressing short-term skill gaps, while building long-term capability

Capacity Building and Change Management 27
• Identify supervisors and mentors from within your organisation or from outside sources.
• Be open to all levels of staff and management receiving supervision and mentoring.• Ensure administrative (managerial) supervision is separated from individual
supervision.
• Available from the VAADA Comorbidity Website: www.comorbidity.org.au• NCETA 2005, Clinical supervision: A practical Guide for the Alcohol and
Other Drugs field• Queensland Health 2009, Cclinical supervision guidelines for mental health services
Helpful Tips
Support Materials
in your organisation. If your intent is to develop internal staff to be effective project managers, mentoring and supervision is essential.
Mentoring will allow for skill transition in a supportive, ‘on the job’ setting. It can be used to help inexpe-rienced project managers or change agents to get up to speed quickly, while providing them the necessary support. In relation to dual diagnosis capacity building and change management, staff and agencies who have ‘walked in your shoes’ before may be relevant mentors (for example, the Victorian Dual Diagnosis Leader-ship Group, dual diagnosis portfolio holders and Improved Services Initiative project managers).
Supervision is a more formal arrangement with, commonly, an external experienced project manager or change agent providing specific support to your organisation’s context.
Other means of project support may be provided by an established governance structure or steering committee. It is important to match experience and knowledge of the members of such a structure to the needs of the project or change process. As with clinical or administrative supervision and mentorship, the following values underpin the support you may need:
• Expertise – access to project management/change management skills.• Experience – access to practical project management/change management experience.• Neutrality – advice offered on an impartial basis.• Partnership – collaboration with other project management/change management professionals.• Empowerment and confidence – involvement and skills transfer.

Capacity Building and Change Management28

Capacity Building and Change Management 29
PART D: Change management
PREPARING ORGANISATIONS FOR CHANGE
The only constant is changeHeraclitus (535–475BC)
RationaleThe development of a service system’s dual diagnosis capability is an evolutionary process, as with any major philosophical shift in service delivery. It involves a combination of ‘inner’ shifts in people’s values, aspirations and behaviours with ‘outer’ shifts in processes, strategies, practices and systems.
Most change initiatives fail or have a poor track record in sustaining the change. This is because many change initiatives focus only on the ‘outer’ shifts (Senge, 1999).
To enable agencies to successfully work towards being dual diagnosis capable, a clear understanding and ap-plication of the core principles behind change management is required.
Preparation for changeIt is important to consider your workplace carefully before articulating or suggesting a need for change. As a change agent, it is imperative that you consider and understand the workplace culture, values, people and behaviours, especially in relation to previous responses to change strategies.
Change management vs Project management Project management is ‘the application of knowledge, skills, tools and techniques to project activities to meet project requirements’ (Project Management Institute, 2010).
Project management is accomplished through the application and integration of a series of well-defined processes: initiating, planning, executing, monitoring and controlling, and closing. The project manager is the person responsible for accomplishing the project objectives.
By comparison, change management is a structured and strategic approach to initiating and managing a change process within an organisation or other specific context. Change management may be an essential strategy in addressing one aspect of the activities within a project. If the change is significant enough, it may also be redefined into a project itself.
It will be up to your agency and key stakeholders to decide whether this implementation is viewed as a change management strategy or defined as a specifically targeted project. In either case, it is recommended that an experienced change agent or a project manager be appointed (or recruited) to support the process.
For the purposes of this manual, ‘project management’ refers to the implementation of a change manage-ment practice within a dual diagnosis context.
CONSIDER THE FOLLOWING:
• How has change happened in your workplace previously?• What change strategies have been successful and not successful and why?• Do you have to start from scratch again or can you build on previous change processes?• How do staff normally respond to a new idea or process?• Is change traditionally perceived as a threat or an exciting opportunity?• How does management support and view change?• How do you see change?

Capacity Building and Change Management30
What works for project management?MacLean et al (2010) studied more than 1,000 projects that were funded in the Australian AOD sector. They found the three key elements of success project management were:• effective partnerships with other agencies and communities• project leadership• effective planning and design.
They went on to describe specific enabler and barrier mechanisms in the projects they studied. These are described in Table 2.
Table 2: Enabler and barrier mechanisms in project management
ENABLING MECHANISMS BARRIER MECHANISMSProject planning and design:Evidence-based model, good fit to needs, flexible design, appropriate scoping, rules, holistic approach, advice on implementation
Project planning and design:Poor fit, inadequate scoping, poor timing, IT problems
Research, evaluation and data collection:Well-documented, effective data collection, in-formed by ongoing research
Research, evaluation and data collection:Poor data collection systems, low response to evaluation, datasets missing
Funding and resourcing:Well-funded, used existing resources, gained addi-tional funding, partner agency contributed resources
Funding and resourcing:Submissions for ongoing funding unsuccessful, other funding problems at organisation
Staffing and leadership:Employed suitable staff or contractors, staff or man-agement provided leadership, staff training activities undertaken
Staffing and leadership:Delay in staff recruitment, staff or management turnover, staff lacked required skills
Organisational governance and capacity:Organisation already experienced in project work, good policies and procedures and suitable systems, effective reference group
Organisational governance and capacity:Lack of management involvement, project staff overloaded, reference group unrepresentative or ineffective
Workplace integration:Staff engaged and enthusiastic about project, inclu-sion of consultation mechanisms
Workplace integration:Staff roles unclear, staff conflict, staff didn’t prioritise involvement, placed additional stress on staff
Engaging communities and partners:Strong support from partner agencies or key par-ticipating communities, utilised existing networks
Engaging communities and partners:Lack of partner agency or community interest in or commitment to project, reluctance to address AOD/MH issues
Sensitivity to service users and settings:Model culturally appropriate, intensive support, employed culturally/gender appropriate staff
Sensitivity to service users and settings:Resources or approach not culturally appropriate, failed to engage specific demographics
Participatory approach to service delivery: Target group involved in development, used role models or peer approaches, activity based approach
Participatory approach to service delivery:Participation poor; difficulties in service users lives interfered with attendance, challenging behaviours
Wider service system challenges:Lack other services, inter-professional problems, philosophical differences in addressing AOD/MH
Adapted from: MacLean et al (2010)

Capacity Building and Change Management 31
TOOLS FOR CHANGE
The PDSA toolPDSA stands for Plan – Do – Study – Act (or C for ‘Check’ if you prefer to call it a PDCA cycle).
The PDSA is a proven project or change management tool that you can use to address just about any proc-ess that needs to be implemented or changed. While it appears deceptively simple, it is actually very power-ful. The more you use it, the more you improve.
The PDSA cycle was developed by W. Edwards Deming, a statistician and manufacturing consultant in the mid 20 century.
The PDSA cycle 1. PlanPlan what you want to happen or to achieve. First set the objectives – decide on the end results you want. Then plan the tasks or activities required to get there.
2. DoImplement the plan. Do what you have set out to do.
3. StudyOnce you have implemented the plan (or a component of it), you then study the outcome. Look at what happened. • Did you get the results you planned for, expected or wanted? • Did you get a different result? Was the result you got unwanted or unexpected? • If it didn’t go as planned, why not? • Are things better now or worse? • If better, can they be improved? If worse, why and what should you do next? • Do you need to do something different, continue for longer or change some aspects?
Some methods you might use in this phase include observation, monitoring, measuring, studying the data you collect, analysing, discussing, holding ‘management reviews’ and looking at results of audits.
Note: This phase is also known as ‘Check’ or sometimes ‘Review’. It was originally called ‘Check’, but Deming renamed it ‘Study’ later on. He was reportedly concerned that it may be seen to be merely a matter of inspec-tion, whereas it should be far more than that. In this manual, we use ‘Study’ to give a more accurate clue to the activities that are (or should be) involved.
4. ActThis is where you take action, based on the results and the lessons learnt. • If the change was a good one, build it into your system. • If it didn’t work out well or needs further work, you might refine it or start again from the beginning,
planning some different action.
Which takes you back to the next stage: Step 1 (Plan) again, but this time with new information and knowledge.
PDSA and quality assuranceThe PDSA cycle is designed to be used as part of a continuous quality improvement system. Each time you complete it, you learn new information and knowledge that can be used to improve your change manage-ment process.
Thus, you repeat Step 2 (Do) again, with new information and knowledge. And you repeat another cycle of Plan – Do – Study - Act … followed by another ... and another ... and so on. With each cycle, you cannot help but improve your quality system. Figure 1 shows this cycle.

Capacity Building and Change Management32
Figure 1: Plan - Do - Study - Act Cycle
Where failures occurMany organisations tend to do only part of this cycle, most often the ‘Plan – Do’ phase. The majority of organi-sations are most comfortable in the ‘Do’ phase. There’s a lot of activity, all of which is seen as ‘the real work’.
‘Plan’ is also usually at least acknowledged or paid lip service to. The organisation may do some planning, to a greater or lesser degree. They know that it’s important and try to do it … or mean to … when they ‘get around’ to it ... when they ‘find the time’.
Where most organisations fall short is in the other half of the cycle: ‘Study (Check) – Act’. An organisation may Plan and then Do, but they often don’t make the time to Study what happened and then to Act depend-ing on the results.
Some organisations may even produce a plan but then rarely use it or apply it. They don’t make time at intervals to review (study) their plan and compare where they are now with where they planned to be. It’s only when an organisation learns to place its attention on all of the stages of the PDSA cycle that it will start to experience major improvement. Highly successful organisations put equal attention on all four aspects of the cycle and practice them all, without emphasising any one to the exclusion of others. They understand that this apparently simple tool is incredibly powerful if used correctly.
ASSISTING PEOPLE DURING CHANGE
The difference between change and transition Society confuses change and transition constantly. We imagine that transition is just another word for change, but it isn’t.
• Change is situational – for example, moving to a new city or shifting to a new job. • Transition is psychological – it is the inner reorientation and self-redefinition that you have to go
through in order to incorporate changes in your life.
Without a transition, a change is just a rearrangement of the furniture. Unless transition happens, the change won’t work because it doesn’t ‘take’. This process is described by William Bridges in more detail in his book, Managing transitions: making the most of change.
Phases of transitionBridges (2009) states that people will experience a range of emotions as they come to transition through change. Three transition phases have been identified:
1. The ending 2. The neutral zone3. The new beginning.

Capacity Building and Change Management 33
Figure 2: Transition process
Source:Bridges(2009)–Reproducedwithpermission
Supporting people through transitionUnderstanding the transition phases and how people respond to change is crucial to recognising the needs of staff and other stakeholders as they move through transition.
Figure 3: Understanding the phases of transition
Source:Bridges(2009)-Reproducedwithpermission
Bridges describes the tasks that managers need to perform to assist staff and other stakeholders through transition at each stage. These are decribed in Table 3.

Capacity Building and Change Management34
Table 3: Transition phases and managers’ tasks
Transition phase Description Managers’ tasksEnding (losing, letting go) Tangible and intangible losses can
lead to emotions such as denial, shock, frustration and anger.
Support people to deal with their tangible and intangible losses and mentally prepare to move on.
The neutral zone The person will find themselves in a ‘neutral zone’ for a period of time where they may feel some ambivalence or scepticism, but they are beginning to let go of the old and move on to the new. Crit-ical psychological realignments and re-patterning takes place.
Support people to get through it and capitalise on all the confu-sion by encouraging them to be innovators.
The new beginning This last phase of the transition will take the person through scepticism, acceptance, hope and enthusiasm until they embrace the ‘new beginning’.
Support people to develop their new identity, experience new en-ergy and discover the new sense of purpose that will enable the change to begin to work.
Adaptedwithpermissionfrom:Bridges(2009) ‘Transition able’ organisationsTransition ‘able’ organisations have in place policies, roles, culture, leadership, structure, resources and histo-ries that provide a supportive environment for successful transitions.
Bridges suggests some strategies organisations can use to help people through the transition phases:• Work less with the change management and more with the transition management.• Remember that change is perceived personally, yet we try to deal with it organisationally. The more
included people are early in the development of an idea, the easier and quicker they can begin their transition.
• Be mindful that each person transitions at their own pace.• Attempts to ‘sell’ the new beginning zone to staff will not move them towards leaving the ending zone.• Movement occurs when you show that you understand the individual’s transition.
Change is a slow process. Timelines need to be realistic and variable depending on the type of change ar-ticulated in each step of your change management plan. All change agents must be able to analyse the system or agency in which they operate and understand what is required to bring about change. It is important to be aware that changes in any part of a system will have an impact on every other part of the system.
• Set realistic timelines for change that reflect the type of change you want to see. • Think about how change might affect your organisation. Make sure you are clear about
what kind of change you are planning and understand the impacts of that change on all parts of your organisation.
• Remember the three key elements of successful project management are: - effective partnerships with other agencies and communities - project leadership - effective planning and design.
• Improved Services Initiative project managers• For Victorian context: the Victorian Dual Diagnosis Leadership Group• Change management literature• Change management consultants• Appendix 7: PDSA project template • Appendix 8: Framework checklist for implementing change and/or projectsAvailable from the VAADA Comorbidity Website: www.comorbidity.org.au• Bridges, W (2009), Managing Transitions: Making the Most of Change. Lifelong Books,
San Francisco
Helpful Tips
Support Materials

Capacity Building and Change Management 35
RESISTANCE TO CHANGE
In any change process there will be resistance. Resistance shouldn’t be seen as a negative or undermining response that needs to be ‘managed’. Often it reflects a genuine concern that, if recognised, can provide greater clarity and focus to the changes required. Open communication and willingness to address these concerns is essential.
Much of the literature on resistance to change quotes Rick Maurer (2009) and the three levels of resistance he describes in “Introduction to Change without Migraines”. These are:• Level 1 – I don’t get it• Level 2 – I don’t like it• Level 3 – I don’t like you.
Level 1 – I don’t get itLevel 1 involves information: facts, figures and ideas. It is the world of thinking and rational action, presenta-tions, diagrams and logical arguments.
Level 1 resistance may come from:• lack of information • disagreement over interpretation of the data • lack of exposure to critical information • confusion over what it all means.
Giving people information is the most common way organisations try to deal with resistance. Many make the mistake of treating all resistance as if it were Level 1.
Level 2 – I don’t like itLevel 2 is an emotional reaction to the change. People may be afraid that this change will affect how they do their job or the quality of the services they offer. They may also be afraid that change will cause them to lose face, status or control – maybe even their jobs.
When Level 2 is active, it makes communicating change very difficult. People stop listening.
Level 3 – I don’t like youLevel 3 is a major reason why resistance flourishes and changes fail. Maybe they do like you, but they don’t trust or have confidence in your leadership.
In Level 3 resistance, people are not resisting the idea. In fact, they may love the idea you are presenting. They are resisting you. Maybe their history with you makes them wary. Perhaps they are afraid that this will be ‘a flavour of the month’, like so many other changes, or that you won’t have the courage to make the hard decisions that will see this change through.
It may not be you. Perhaps people have had a bad experience with change and leaders before. Or they may be resistant to those that you represent. The moment that some people hear someone from management is present and wanting to help, they become sceptical. If you happen to be that person from management, you’re going to have a hard time getting those people to listen.
APPLYING CHANGE MANAGEMENT
The critical steps to successThe key elements discussed in this chapter are described in further detail in Part E of this manual. These steps are critical to successful change. You may choose to use these steps as a checklist and apply those areas that are relevant to your agency. Remember that you may not need to use every component at all or in detail, but being mindful of these components will ensure you are not neglecting any core steps. Appendix 8 provides a ready-to-use copy of this checklist.

Capacity Building and Change Management36
Steps to successful change management include:• Define your purpose.• Carry out a pre-agency audit.• Gain agency endorsement.• Create a vision.• Identify the leaders.• Develop a plan.• Establish consultation and communication process.• Ensure consumer and carer/family/ significant other involvement.• Carry out a post-agency audit.
It is important to recognise that, even with the best of intentions, managers and project leaders can sometimes overlook elements of the change process or move too quickly through the steps before others have had a chance to ‘catch up’.
Barriers to implementation The barriers to effectively implementing dual diagnosis capacity building are well documented. It is important to be aware of the core issues and address obstacles early. Some common barriers are found in many agencies. • Many agencies are currently orientated, trained and structured to respond to single disorders only.• Despite national and state dual diagnosis policy, some agencies continue to have service exclusion criteria
based on the presence of a co-occurring mental health and substance use disorder.• In agencies that have undergone significant restructure or alteration, staff may be ‘change-weary’ and
‘change-wary’.• There may be a lack of understanding (and expectations) of the other treatment system’s strengths, con-
straints and philosophies.• The agency may fail to recognise the presence of co-occurring disorders and lack the expertise and/or
confidence in deploying integrated treatment.• There may be a perception that this will add to already burdened workload.
• Find a mentor for your project. Several dual diagnosis projects have been deliv-ered over the last 10 years and there are many leaders in the field who may be available to mentor your agency if you do not have any identifiable leaders.
• Engage an outside facilitator. It may be worth considering contracting a strategic facilitator to lead this component and support the discussions towards a tangi-ble outcome.
• Find examples to spark discussion and thinking: Many dual diagnosis capac-ity building plans have been written. It may be useful to source examples from other agencies or colleagues to use as a framework your own and your agency’s discussions and considerations.
• Address obstacles early. The barriers to effectively implementing dual diagnosis capacity building are well documented. Make sure you are aware of the core is-sues to be mindful of and take action to address them.
Helpful Tips

Capacity Building and Change Management 37
Part E: Stages to build capacity
There are five stages that are essential to building capacity within organisations:Stage 1: Communicate and engage.Stage 2: Develop a plan.Stage 3: Implement the plan.Stage 4: Evaluate.Stage 5: Share your knowledge and experience.
STAGE 1: COMMUNICATE AND ENGAGE
Before you do anything, communicate! Then take a baseline to understand where you are coming from and develop a vision for where you are headed to guide your planning. At all stages, communication is the key.Part D of this manual provides a checklist of possible actions for successful change management. Some or all of these may be applied by agencies wishing to build dual diagnosis capacity. At Stage 1 of the capacity build-ing process, some first critical steps are listed below.
Identify your stakeholdersWho will be involved?Any change will require all stakeholders to be involved in the process from the beginning. You will need to decide who your key partners are. Remember that everyone who is involved in your organisation’s service delivery has a part in developing dual diagnosis capacity, including:• consumers and significant others• staff/workers• senior leaders• clinical leaders• champions/portfolio holders• other agencies• external experts and specialists.
A description of each of these stakeholder groups is included in Part C of this manual.
Who will lead?In relation to specific leadership roles, change management leaders need to be clearly identified. These roles require meaningful tasks and responsibilities endorsed by management with clear pathways of reporting and authorisation. Change management leadership roles need to be clearly defined and communicated to all managers and staff.
Typically the role of a change management leader is to:• publicly support and sustain momentum for the change process or project• legitimise their role by talking about the process, report against the outcomes, consult with the staff and
managers and monitor key performance• provide coaching and feedback to staff and managers• develop the plan and coordinate the project implementation• ensure communication of project progress to all staff• ensure milestones of progress are celebrated• ensure the project is adequately resourced.
What support is required from your partners and from you?Support is a two-way street. Once you have identified who will be involved, you need to ascertain the level and type of support you will need to provide your stakeholders, as well as the type and level of support they can offer you.Conduct a stakeholder analysis to work out who will be involved and how they might assist the process. You can use the Stakeholder analysis template provided in the Appendices of this manual to help you do this.
• Appendix 1: Stakeholder analysis templateSupport Materials

Capacity Building and Change Management38
Discuss and communicateThe importance of open and two-way conversations with all stakeholders cannot be underestimated. The format and style of the communication may differ depending upon the needs of the stakeholder.
For example, staff will need to be informed of the change and the process, but equally important they will need the opportunity to voice concerns and take part in the development and staging of the plan. Senior leaders will initially need to be fully briefed, but may only need brief updates as the changes take place.
Define your purposeThe processes are intertwined and will be the basis for your plan. Through effective two-way communica-tion with consumers and staff, they will be able to identify changes that need to occur and help define the purpose of the change, which will involve providing a better service for people with a dual diagnosis.
Carry out a pre-agency (baseline) auditBefore any changes can occur, you need to know where your organisation and staff are in regard to dual diagnosis capacity and capability. One way is to do a pre-agency or ‘baseline’ audit. There are several tools available for your audit.
COMPASS™ (Comorbidity Program Audit and Self-Survey for Behavioral Health Services) is a tool that can be used by services to assess program competencies in multiple areas that reflect standards for Dual Diagnosis Capable mental health and AOD services. This tool was developed to assist in the implementation of the Comprehensive Continuous Integrated Systems of Care (CCISC) Model for systems change (Minkoff, 2001)
DDCAT (Dual Diagnosis Capability in Addiction Treatment ) Index, is an instrument that can be used for measuring capacity of an AOD service to provide dual diagnosis services. The DDCAT evaluates 35 (33 in the Australian context) program elements that are subdivided into 6 dimensions:• Program Structure• Program Milieu• Clinical Process dimensions (Assessment and Treatment)• Continuity of Care• Staffing• Training
The Agency Dual Diagnosis Capability Checklist, developed in Australia by Gary Croton is one of a suite of checklists available through the Dual Diagnosis Australia and New Zealand website. This checklist covers several domains of an organisation’s ability to provide services to clients with a dual diagnosis.
A baseline audit is a quality activity that will provide you with:• evidence and an argument for the need to build capacity• pre-capability measures providing a base for growth as you implement your plan• identified strengths and weaknesses that will help define the priority areas to focus on within the plan.
It is essential that the audit process is open and that the results of the audit are com-municated to all stakeholders.
Available from the VAADA Comorbidity Website: www.comorbidity.org.au• DDACT• COMPASS• Agency Dual Diagnosis Capability Checklist
Support Materials

Capacity Building and Change Management 39
Gain agency endorsementIt is important that change should be delivered from both the top down and bottom up. You will create a firm foundation to build upon if you include all layers of the agency in the endorsement of the need for change and then the development of a vision.
Create a visionOften the vision has been developed during the early stages of the change management process, but should be made public and used in conjunction with the evidence from the audit to gain agency and stakeholder endorsement.
A vision statement is a vivid description of a desired outcome that inspires, energises and helps you create a mental picture of how the system will look, feel and function when providing an effective response to the needs of persons with a dual diagnosis.
Remember that the audience for the vision is the staff, management and other stakeholders in the organisa-tion so it should resonate with them. You should seek the assistance of others in the organisation to help with developing the vision. These people should include those who:• have the best interests of the organisation at heart• will challenge your thinking and that of your organisation• bring a different perspective.
Again this vision needs to be communicated to all stakeholders and you will need to seek an endorsement of the vision from all stakeholders and a commitment to working to improve dual diagnosis capability.
The vision for your dual diagnosis capable programs will typically include key components outlined by Minkoff and Cline (2006) and a range of other elements described in Part B of this manual.
Dealing with resistanceAs described in the change management section, there are three levels of resistance:• Level 1 – I don’t get it.• Level 2 – I don’t like it.• Level 3 – I don’t like you.
Identifying resistanceIt is important that you identify resistance early and reassess as you move through the change process. The three types of resistance can occur at any stage. A Resistance Assessment Survey is provided in the Appendices section of this manual for your use.
Managing resistanceThere are a number of ways that you can deal with this resistance, all of which involve open, honest and two-way communication.
Level 1: Make your case• Make sure that people know why a change is needed. Before you talk about how you want to do things,
explain why something must be done.• Present the change using understandable language. • Find multiple ways to make your case. People take in information in different ways. Some like to hear
the data, while others prefer visual sources like pictures or text. Some people learn best by interacting in a group or through conversation. The more variety in the communication channels, the greater the chance that people will comprehend what you have to say.
• Appendix 6: Plan templateSupport Materials

Capacity Building and Change Management40
Level 2: Reduce fear and increase excitement• Remove as much of fear as you can and increase staff’s excitement about what’s positive about the change.• Emphasise what’s in it for them. Staff need to understand that these changes will benefit them as well
as the consumers. For example, you could explain that work will be easier, relationships will improve, career opportunities will open up or job security will increase.
• Engage people in the process. People tend to support things that they have a hand in building.• Be honest. If a change will hurt them, tell them the truth. It’s the right thing to do and it stops the ru-
mor mill from inventing stories about what might happen. Also, honesty bolsters their trust in you (a Level 3 issue).
Level 3: Rebuild damaged or neglected relationships • Take responsibility for things that may have led to the current tense relations.• Keep commitments. Demonstrate that you are trustworthy.• Find ways to spend time together so they get to know you and your team. This is especially helpful if
the resistance comes from people’s attitude towards those whom you represent and not just from your personal history together.
• Allow yourself to be influenced by the people who resist you. This doesn’t mean that you give in to every demand, but rather that you can admit that you may have been wrong and that they may have ideas worth considering.
STAGE 2: DEVELOP A PLAN
Having engaged your stakeholders, you are now ready to develop a plan to scope the change process. Good planning in the beginning can save you a lot of time and trouble as the project progresses. Consultation and communication are the key activities in the plan’s development. All key stakeholders, partners and leaders should be involved in the plan.
The plan will include general principles that will guide the implementation as well as the specific activities to be completed and (as appropriate) timeline and persons(s) responsible. It will also include some detail of ongoing and continuous assessment and evaluation of the plan’s progress.
As a guide to the general principles, take a look at the information sheet, Overarching principles to address the needs of persons with dual diagnosis, in the Appendices section of this manual.
• Seek out consumer and significant other representatives and involve them as key partners from the beginning.
• Identify and engage key consumer and significant other groups who may be able to provide representation from other sectors.
• Check your communication process to make sure it involves all consumers and significant others of your agency and not just those in co-opted positions.
• Make sure your communication process also involves feeding back to consumer and significant other groups of other agencies.
• Network with the peak agencies.
• Appendix 2: Resistance Assessment Survey
Helpful Tips
Support Materials
• Appendix 3: Information sheet: Overarching principles to address the needs of persons with dual diagnosis
Support Materials

Capacity Building and Change Management 41
The PDSA cycleThe PDSA cycle can be used in all aspects of the dual diagnosis capability plan. Several sub-plans will need to be developed and using the PDSA cycle can assist in ensuring quality control. A full description of the PDSA cycle is provided in Part D of this manual.
PDSA stands for Plan – Do – Study – Act.
Working with the PDSA cycle Use the PDSA Project Template in the Appendices section of this manual to work your way through the PDSA cycle. • Plan.• Do.• Study.• Act.Then repeat step 2 (Do) again, with new information and knowledge.
Thus you repeat another cycle of Plan – Do – Study – Act … followed by another ... and another ... and so on. With each cycle, you cannot help but improve your quality system.
Who is involved in developing the plan?In designing your approach to the development of dual diagnosis capability, you will be able to:• identify the stakeholders and their roles• identify barriers of resistance• identify a change management team with their roles and responsibilities.
StakeholdersIdentifying the levels of participation of stakeholders in the change process allows you to make sure that a wide variety of interests are taken into account. Using the Stakeholder Analysis Tool, you will be able to identify who needs to be involved as well as answer the following questions.• What are the specific target groups/audiences that will be impacted by this change?• Who might be able to help you the most? • Who might present the most resistance?• Who will be the change drivers?
ResistanceResistance is a natural and unavoidable part of any change process. It is a survival mechanism within organi-sations. There are a number of reasons why staff resist change, so it is important to identify the root causes in order to plan some of your strategies for implementation.
When you understand what lies behind people’s concerns, you can begin to reduce them, using a range of strategies including open communication. Use the Resistance Assessment Survey tool provided in the Appendices section of this manual to help you identify the sources of resistance in your organisation.
• Appendix 7: PDSA Project templateSupport Materials
• Appendix 1: Stakeholder Analysis Tool
• Appendix 2: Resistance Assessment Survey
Support Materials
Support Materials

Capacity Building and Change Management42
Change management teamIn the development of your change strategies, you may want to consider developing a change management team who can help drive the implementation of the change. The change management team is there to sup-port and offer guidance.
• Team members should represent a variety of functions, departments and levels in the organisation, while also representing a cross-section from your stakeholder groups.
• They need to have excellent communication skills, have business influence, be committed to the change, know the business and be a team player. Some change management experience would be an asset.
• The team does not have to be working on your project full time but must be able to commit some time to the project.
• The team may require some team development to provide a common understanding of the business issues that motivated the change and the vision for the future state for the organisation.
• The team need to identify roles and responsibilities in the implementation of the change plan.
Action planThe Action Plan is your master plan and lists the activities, responsibilities and timeframes for the project to be rolled out.
ACTIVITY RESPONSIBILITY TIMEFRAMEEg. Communication Activities
The following plans are listed in summary in the Action Plan.
Communication planWhen developing a communication plan, it is important to create reporting protocols specifically for devel-oping dual diagnosis capability and identify who will be the responsible member from the project team to have overall responsibility for the rolling out of communication. Make sure you include all stakeholders (for example, other project teams, staff or key stakeholders).
• Appendix 4: Action PlanSupport Materials
Throughout the process of developing the plan, ensure that all stakeholders are aware of the progress and that there are mechanisms for them to clarify any areas and have input into the development of the plan.
• Appendix 5: Communication PlanSupport Materials

Capacity Building and Change Management 43
Training planKeep in mind that all staff will be at differing levels of dual diagnosis capability (for more details about dual diagnosis capacity building, see Part B of this manual). It is known that to effectively build capability and capacity, you will need:
• good quality educational programs for workers• quality supervision and mentoring• an infrastructure within your organisation that supports the development of capacity and capability.
Any training plan must also include supervision and mentoring.
Ideally, training should be tailored to the needs of the individual. Individual capability checklists can be valu-able for staff to identify their training needs and inform the training plan.
Business systems and policy planIt is vital to ensure that your organisation has an infrastructure that will support and sustain the change you envisage. This will include having enough financial human resources to implement the contents of your plan. Equally important are the changes to policies and procedures.
Your business systems and policy plan will need to outline steps you will take to ensure your organisation has adequate resources and infrastructure to achieve your goals.
This may include planning to:• include the new process in staff orientation packages • embed dual diagnosis capability in staff appraisal checklist as a review mechanism• ensure the project is listed on key meeting agendas• embed changes into all relevant policy and procedures• institute an annual system to update training for all staff• identify and remunerate or resource dual diagnosis leaders• update staff job descriptions with any changes in core competencies• monitor and update quality assurance mechanisms (for example, pre- & post-capability audits,
policy review and updates)• change policy and procedure
Your business systems and policy plan will also include:• costs and timelines• a list of possible resources that are available or required• agreements with other agencies (for example, partnership agreements or MoUs)• an evaluation strategy.
Plan to monitor and reviewBefore you implement the plan, make sure you know how, when and who will be monitoring various aspects of the change process. This is important as you will need to celebrate the successes as well as be aware of any areas that are not going to plan.
Monitoring activities may include the use of training reports and evaluations, staff and consumer satisfaction surveys, change management reports and any other tools that you may find useful to review your progress.
• Appendix 8: Framework checklist for implementing change and/or projectsSupport Materials

Capacity Building and Change Management44
STAGE 3: IMPLEMENT THE PLAN
Now it is time to put the plans into action. The various aspects of the plans will start at differing times and there will be differing timelines. It is important to monitor the implementation as the plans proceed.
Once the plan is implemented, it is important to ensure that the momentum of change continues. This will require regular two-way communication with all stakeholders.
Importance of senior and clinical leadersOf particular importance are your senior and clinical leaders. They may need to occasionally meet with or send messages to the rest of the staff to help them maintain their confidence in the process of change and encourage them to maintain their commitment to the process.
Monitor and reviewAs stated earlier, the monitoring of the process is vital. If there are any problems arising, you will need to iden-tify them early and intervene before the problem escalates. The Change Management Team is there to support and offer guidance.
Equally important are the successes, which need to be communicated and celebrated.
The regular use of the various auditing tools will give an idea of how the organisation and individuals are go-ing in building dual diagnosis capability.
Inclusion of an implementation committee or project management committee will also work as useful strat-egies for monitoring implementation of a plan.
STAGE 4: EVALUATE
It can be said that change never ends and is therefore difficult to evaluate. However, in the planned proc-ess that you have been involved in, it is important to go back to the beginning and see if the organisation has achieved the goals you originally set.
Your PDSA cycle will give you information of what has been achieved and the issues that arose. You should use this to build the ongoing evaluation of the process. Some questions you might ask include:
• Has the vision been achieved or is it closer to being achieved?• Is there a positive change in the results of the audits?• Are staff and consumer satisfaction surveys reflecting a positive change?
Compare your progress against your baseline. Re-instigate the audit tool you selected at the beginning of this process.
Remember that the audit is a quality activity that will provide you with the following comparative data from your baseline:
• evidence and an argument for the need to apply capacity building in an ongoing manner• pre- and post-capability measures showing growth as you implement a plan• identified achievements, hiccups and barriers – this information will influence priority areas to focus
on for future planning purposes. As with the pre-audit, it is essential that the post- or review audit process is open and that the results of the audits are communicated to all stakeholders. Make sure you use the same audit tool you selected in the beginning of this process.
When interpreting your audit results, there are a couple of things you need to be aware of.• It is important to remember that many agencies find their initial audit is often scored quite ‘gener-
ously’. Then, when a follow-up audit is conducted, the scores may not appear to have moved greatly.

Capacity Building and Change Management 45
It is common that the second and third audits are more true to context and the first is more generously scored.• As a result, it is often worthwhile recruiting an external auditor to limit the chances of this anomaly
occurring. If you are using the COMPASS an external auditor is mandatory.
STAGE 5: SHARE YOUR KNOWLEDGE AND EXPERIENCE
You have been involved in a major process of implementing change. You now have a responsibility to share your knowledge and experience with others. Become a mentor. You can assist others and other organisations to become dual diagnosis capable.
Available from the VAADA Comorbidity Website: www.comorbidity.org.au
• DDCAT• COMPASS• Agency Dual Diagnosis Capability Checklist
Support Materials

Capacity Building and Change Management46

Capacity Building and Change Management 47
Part F: Appendices
Appendix 1: Stakeholder analysis
Appendix 2: Resistance assessment survey
Appendix 3: Information sheet
Appendix 4: Action plan
Appendix 5: Communication plan
Appendix 6: Plan template
Appendix 7: Plan – Do – Study – Act (PDSA) project
Appendix 8: Framework checklist for implementing change and/or projects
Appendix 9: Further reading

Capacity Building and Change Management48

Capacity Building and Change Management 49
APPENDIX 1: STAKEHOLDER ANALYSIS
NAME OF INDIVIDUAL OR GROUP
NEED FOR SUPPORT LIKELIHOOD OF SUPPORT
• In the first column, list all the major individuals and groups that need to go along with this idea.
• In the second column, rate the level of support you need from each individual or group on a scale of 1 to 5.
5 = They must take an active part in the development and be vocal champions for the change. 4 = They must take part in the development. 3 = They need to go along with whatever is decided. 2 = It’s OK if they have some objections. 1 = It’s OK if they resist strongly.
• In the third column, list the level of support you can expect from them today. 5 = They will fully support and champion the change. 4 = They’ll help some. 3 = They’ll go along with whatever is decided. 2 = They are likely to complain. 1 = They are likely to resist this change openly and strongly.
• Examine the scores. For effective change, you need matching scores such as 5/5, 4/4 and 3/3. These scores indicate that the support you need matches the support you are likely to receive. Mismatches are dangerous, especially 5/1, 5/2, 4/1, 4/2. All of these indicate that you need strong support but you are likely to get resistance. This tells you that these relationships need work.
Adaptedfrom:QueenslandGovernment(2008);ChangeManagementPlan:WorkbookandTemplate

Capacity Building and Change Management50

AP
PE
ND
IX 2
: RE
SIS
TA
NC
E A
SS
ES
SM
EN
T S
UR
VE
Y
Belo
w is
a li
st o
f pot
entia
l are
as fo
r re
sist
ance
tha
t yo
u m
ay b
e ex
peri
enci
ng in
the
impl
emen
tatio
n of
the
pro
ject
. Fo
r ea
ch a
rea
indi
cate
the
deg
ree
to w
hich
you
agr
ee o
r di
sagr
ee b
y pl
acin
g yo
ur r
espo
nse
in t
he R
atin
g co
lum
n fr
om t
he fo
llow
ing
scal
e.
1.S
tro
ngl
y D
isag
ree
2.D
isag
ree
3
. Ne
ith
er
ag
ree
or
dis
ag
ree
4. A
gre
e5
. Str
on
gly A
gre
e
Ass
ess
the
scor
es in
divi
dual
ly a
nd h
ighl
ight
any
sco
res
that
are
gre
ater
tha
n 3.
T
his
area
sho
uld
then
bec
ome
your
pri
mar
y fo
cus
for
addr
essi
ng t
he g
reat
est
resi
stan
ce t
o yo
ur p
roje
ct.
Are
as o
f R
esi
stan
ceD
esc
rip
tio
nR
atin
g
Lac
k o
f u
nd
ers
tan
din
g o
f th
e p
urp
ose
an
d
dri
vers
of
the
ch
an
ges
The
re m
ay b
e a
lack
of u
nder
stan
ding
of t
he p
urpo
se o
f the
pro
ject
.T
here
may
be
a la
ck o
f aw
aren
ess
of t
he n
eed
for
the
chan
ge t
o oc
cur.
Fe
eli
ng
of
losi
ng
con
tro
lPe
ople
sup
port
wha
t th
ey h
ave
help
ed t
o cr
eate
. If t
hey
feel
the
y ha
ve n
ot h
ad s
uffic
ient
inpu
t, re
sist
ance
us
ually
incr
ease
s.
Lac
k o
f su
pp
ort
fro
m v
ari
ou
s le
vels
in
th
e
org
an
isat
ion
If pe
ople
per
ceiv
e th
at k
ey in
divi
dual
s or
gro
ups
in t
heir
are
a ar
e no
t ge
nuin
ely
supp
ortiv
e of
the
pro
ject
, th
eir
acce
ptan
ce is
diffi
cult
to s
ecur
e.
Fe
eli
ng
that
th
ere
is
a re
al t
hre
at t
o e
x-
isti
ng
po
we
r, j
ob
se
curi
ty o
r p
ers
on
al a
nd
ca
ree
r go
als
Res
ista
nce
is in
crea
sed
if pe
ople
bel
ieve
the
cha
nge
will
res
ult
in g
reat
er e
mot
iona
l or
care
er c
osts
rel
ativ
e to
wha
t th
ey m
ay g
ain.
Co
nce
rns
ab
ou
t a
lack
of
skil
ls a
nd
kn
ow
l-e
dge
Peop
le m
ay r
esis
t ch
ange
if t
hey
belie
ve t
hey
do n
ot p
osse
ss t
he s
kills
or
the
abili
ty fo
r op
timal
per
form
ance
du
ring
and
aft
er t
he c
hang
e.
Hig
h leve
l o
f im
pac
t o
n d
aily
wo
rk p
atte
rns
Failu
re t
o ac
know
ledg
e an
d, if
pos
sibl
e, m
inim
ise
the
impa
ct o
f pro
ject
tea
m a
ctiv
ities
and
cha
nges
on
peo-
ple’
s w
ork
patt
erns
ten
ds t
o pr
omot
e di
stru
st a
nd a
liena
tion.
Lac
k o
f ti
me
to
ab
sorb
th
e c
han
ges
The
abi
lity
of s
taff
to a
ssim
ilate
the
cha
nge
and
all i
ts c
onse
quen
ces
mus
t be
ass
esse
d.
Hig
h l
eve
l o
f
un
cert
ain
tySo
met
imes
just
the
unc
erta
inty
of t
he s
ituat
ion
can
mak
e pe
ople
rea
ct n
egat
ivel
y.
Ad
vers
e c
han
ges
to k
ey w
ork
ing
re
lati
on
ship
sPe
ople
may
be
resi
stan
t if
they
feel
the
cha
nges
may
adv
erse
ly a
ffect
the
way
the
y re
late
to
othe
rs o
r w
ho
they
wor
k w
ith o
r re
port
to.
Hig
h l
eve
l o
f p
ast
rese
ntm
en
ts a
nd
dis
lik
es
Peop
le m
ay d
istr
ust
or d
islik
e sp
onso
rs o
r ch
ange
age
nts
or h
ave
had
nega
tive
expe
rien
ces
arou
nd c
hang
e –
if th
is is
the
cas
e, a
lack
of a
ccep
tanc
e an
d en
thus
iasm
for
the
chan
ge w
ill q
uick
ly m
ater
ialis
e.
Lac
k o
f in
cen
tive
s an
d r
ew
ard
sC
hang
e in
volv
es le
arni
ng a
nd le
arni
ng u
sual
ly in
volv
es e
rror
s. W
hen
peop
le a
re n
ot g
iven
the
free
dom
to
mak
e m
ista
kes
whi
le le
arni
ng, t
hey
beco
me
afra
id.
Peop
le n
eed
to b
e re
war
ded
for
acco
mpl
ishi
ng t
he c
hang
e in
the
form
of s
omet
hing
the
y tr
uly
valu
e.
Adaptedfrom:QueenslandGovernment(2008);ChangeManagementPlan:WorkbookandTemplate

Capacity Building and Change Management52

Capacity Building and Change Management 53
APPENDIX 3: INFORMATION SHEET
OVERARCHING PRINCIPLES TO ADDRESS THE NEEDS OF PEOPLE WITH DUAL DIAGNOSIS
Principle 1Co-occurring disorders are to be expected in all behavioural health settings. System planning must address the need to serve people with dual diagnosis in all policies, regulations, funding mechanisms and programming.
Principle 2An integrated system of mental health and addiction services that emphasises continuity and quality is in the best interest of consumers, providers, programs, funders and systems.
Principle 3The integrated system of care must be accessible from multiple points of entry (there is no wrong door) and be perceived as caring and accepting by the consumer.
Principle 4The system of care for dual diagnosis should not be limited to a single ‘correct’ model or approach.
Principle 5The system of care must reflect the importance of the partnership between science and service. It must support both the application of evidence- and consensus-based practices for people with dual diagnosis and evaluation of the efforts of existing programs and services.
Principle 6Behavioural health systems must collaborate with professionals in primary care, human services, housing, crimi-nal justice, education and related fields in order to meet the complex needs of people with dual diagnosis.
Principle 7Co-occurring disorders must be expected when evaluating any person and clinical services should incorpo-rate this assumption into all screening, assessment and treatment planning.
Principle 8Within the treatment context, both co-occurring disorders are considered primary.
Principle 9Empathy, respect and belief in the individual’s capacity for recovery are fundamental provider attitudes.
Principle 10Treatment should be individualised to accommodate the specific needs, personal goals and cultural perspec-tives of unique individuals in different stages of change.
Principle 11The special needs of children and adolescents must be explicitly recognised and addressed in all phases of assessment, treatment planning and service delivery.
Principle 12The contribution of the community to the course of recovery for consumers with dual diagnosis and the contribution of consumers with dual diagnosis to the community must be explicitly recognised in program policy, treatment planning and consumer advocacy.
Adapted from: CenterforSubstanceAbuseTreatment(2007)Overarchingprinciplestoaddresstheneedsofpersonswithco-occurringdisorders,
Substance Abuse and Mental Health Services Administration, US Department of Health and Human Services.

Capacity Building and Change Management54

Capacity Building and Change Management 55
AP
PE
ND
IX 4
: AC
TIO
N P
LA
NA
ctio
nsR
espo
nsib
le P
erso
nT
imef
ram
e
Stak
ehol
der
activ
ities
Proj
ect
man
agem
ent
te
am a
ctiv
ities
Com
mun
icat
ion
activ
ities
Trai
ning
act
iviti
es
Aud
it ac
tiviti
es
Adaptedfrom:QueenslandGovernment(2008);ChangeManagementPlan:WorkbookandTemplate

Capacity Building and Change Management56

Capacity Building and Change Management 57
AP
PE
ND
IX 5
: CO
MM
UN
ICA
TIO
N P
LA
N
Nam
e of
con
tact
per
son
for
all p
roje
ct c
omm
unic
atio
n: _
____
____
____
____
____
___
Au
die
nce
Se
nd
er
Ke
y m
ess
age
sD
eli
very
me
tho
dD
ate
Le
ngt
h o
f se
s-si
on
(i
f ap
pli
cab
le)
Lo
cati
on
Exam
ple:
Team
lead
ers
Seni
or m
anag
ers
Exam
ple:
Pro
ject
man
ager
Exam
ple:
St
aff u
sers
Exam
ple:
Sup
ervi
sor
Adaptedfrom:QueenslandGovernment(2008);ChangeManagementPlan:WorkbookandTemplate

Capacity Building and Change Management58

Capacity Building and Change Management 59
AP
PE
ND
IX 6
: PL
AN
TE
MP
LA
TE
PR
IOR
ITY
ON
E:
GO
AL
STR
ATEG
YR
ESPO
NSI
BILI
TY
TIM
ELIN
E
1.1
1.2
1.3
ReproducedwithpermissionfromPositiveDirections,consultancyandtraining,2009.

Capacity Building and Change Management60

Capacity Building and Change Management 61
APPENDIX 7: PLAN – DO – STUDY – ACT (PDSA) PROJECT
CYCLE: What are the dates of your project?
PROJECT: What are you testing?
TEAM: Who is conducting the test?
BACKGROUND: Who are you testing the change on? What do you predict will happen?
STEP 1: PLANPlan the test
What is the objective of this improvement cycle?
What is the goal? (include a numeric goal to achieve)
What is your plan to achieve the goal?
What data sources are needed for the test?
What measures are used to analyse if you are achieving the goal?
How often will you monitor this project?

Capacity Building and Change Management62
Step 2DO:Try out the test on a small scale.
Implement the plan. Document problems and unexpected observations.
Step 3STUDY:Set aside time to analyse the data and study the results.
Analyse the results and compare the results with your goal.
Step 4ACT:Determine if the test was successful or the plan needs to be revised.
If the test was successful, how will you implement the plan on a wider scale?
If it was not successful, what needs to be changed (based on what you have learned)? Should you continue to search for other root causes?

Capacity Building and Change Management 63
Guidelines for using the PDSA process to create change
PROCESS Answer these questions
Generate ideas Gain consensus What to do be-fore proceeding to the next step
PLAN: Identify an opportunity and plan for change.
How can we get to where we want to be? What do we do first?
What’s the best way to do it?
May include ideas on:• how to solve the
problem• how to implement
solutions • how to monitor
and evaluate the trial improvement.
Agree on a design and implementa-tion plan for a trial improvement
Agree on criteria for evaluating trial.
Brainstorm possible improve-ments; analyse strengths and weaknesses; establish criteria for selection; establish timelines and a plan for monitor-ing and evaluating the trial.
DO:Implement the change on a small scale.
Document problems and unexpected observations.
STUDY:Use data to analyse the results of the change and determine whether it made a difference.
Have we implemented the trial improvement correctly?
Have we followed the monitoring plan?
Are we improving?
What are we learning?
Agree on effective-ness of trial.
Evaluate improve-ment trial using established criteria; compare results with desired state; check for new problems; decide to implement change system-wide or return to root cause analysis to search for other sources of variation.
ACTIf the change was successful, implement the plan and continuously monitor results.
If the change did not work, start the process again.
Should we imple-ment system-wide change?
Does manage-ment support the change?
If not, should we continue to search for other root causes?
Develop ideas for planning system-wide change.(Implement action based on what you learned in the study step. If the change did not work, go through the process again with a different plan, using what you have learned in the study step.)
Agree to a new plan for system-wide change.
Agree to return to root cause analysis and start the proc-ess again.
Prepare to report results of the project; com-municate results throughout the organisation; con-tinue to monitor.
Adapted from: Bendigo Community Health

Capacity Building and Change Management64
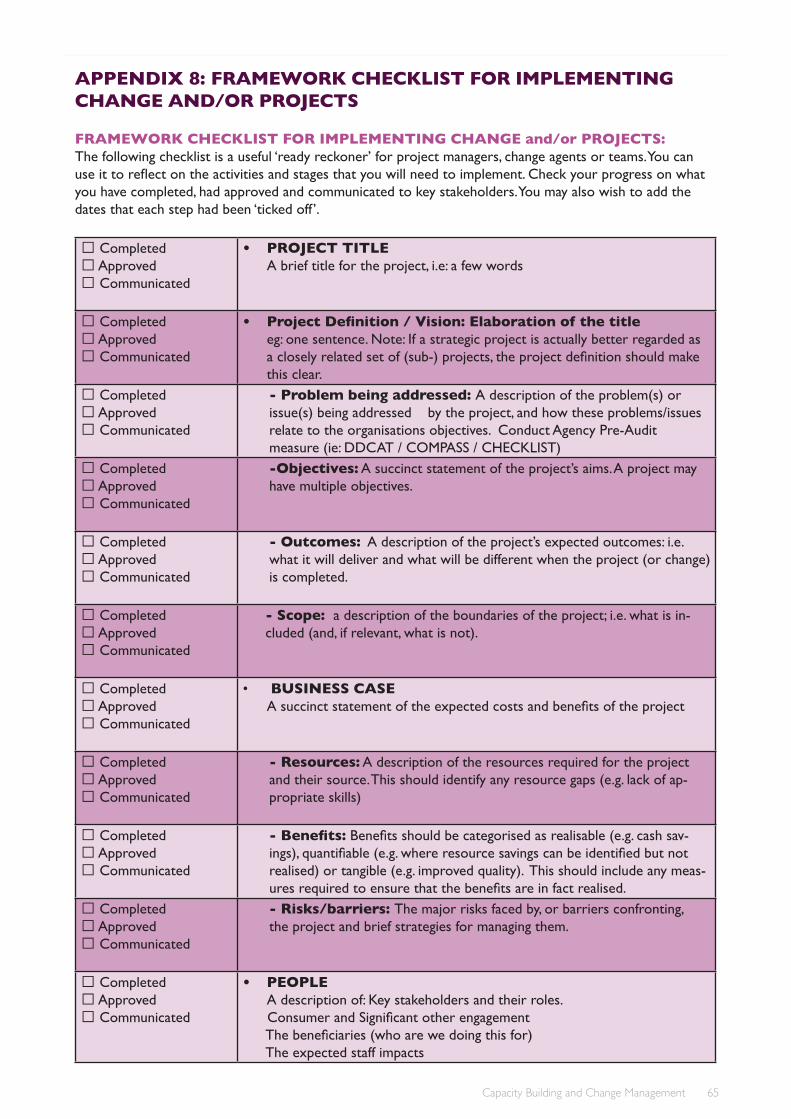
Capacity Building and Change Management 65
APPENDIX 8: FRAMEWORK CHECKLIST FOR IMPLEMENTING CHANGE AND/OR PROJECTS
FRAMEWORK CHECKLIST FOR IMPLEMENTING CHANGE and/or PROJECTS:The following checklist is a useful ‘ready reckoner’ for project managers, change agents or teams. You can use it to reflect on the activities and stages that you will need to implement. Check your progress on what you have completed, had approved and communicated to key stakeholders. You may also wish to add the dates that each step had been ‘ticked off ’.
Completed Approved Communicated
• PROJECT TITLE A brief title for the project, i.e: a few words
Completed Approved Communicated
• Project Definition / Vision: Elaboration of the title eg: one sentence. Note: If a strategic project is actually better regarded as a closely related set of (sub-) projects, the project definition should make this clear.
Completed Approved Communicated
- Problem being addressed: A description of the problem(s) or issue(s) being addressed by the project, and how these problems/issues relate to the organisations objectives. Conduct Agency Pre-Audit measure (ie: DDCAT / COMPASS / CHECKLIST)
Completed Approved Communicated
-Objectives: A succinct statement of the project’s aims. A project may have multiple objectives.
Completed Approved Communicated
- Outcomes: A description of the project’s expected outcomes: i.e. what it will deliver and what will be different when the project (or change) is completed.
Completed Approved Communicated
- Scope: a description of the boundaries of the project; i.e. what is in-cluded (and, if relevant, what is not).
Completed Approved Communicated
• BUSINESS CASE A succinct statement of the expected costs and benefits of the project
Completed Approved Communicated
- Resources: A description of the resources required for the project and their source. This should identify any resource gaps (e.g. lack of ap-propriate skills)
Completed Approved Communicated
- Benefits: Benefits should be categorised as realisable (e.g. cash sav-ings), quantifiable (e.g. where resource savings can be identified but not realised) or tangible (e.g. improved quality). This should include any meas-ures required to ensure that the benefits are in fact realised.
Completed Approved Communicated
- Risks/barriers: The major risks faced by, or barriers confronting, the project and brief strategies for managing them.
Completed Approved Communicated
• PEOPLEA description of: Key stakeholders and their roles.
Consumer and Significant other engagement The beneficiaries (who are we doing this for) The expected staff impacts

Capacity Building and Change Management66
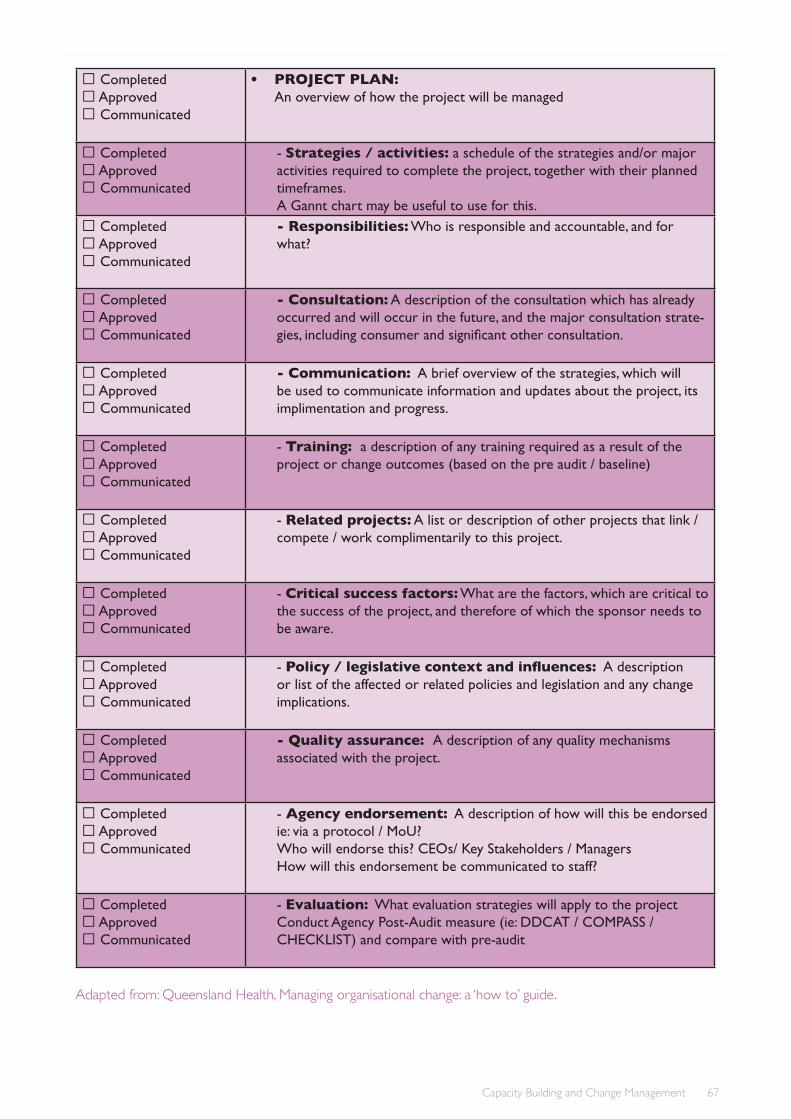
Capacity Building and Change Management 67
Completed Approved Communicated
• PROJECT PLAN: An overview of how the project will be managed
Completed Approved Communicated
- Strategies / activities: a schedule of the strategies and/or major activities required to complete the project, together with their planned timeframes. A Gannt chart may be useful to use for this.
Completed Approved Communicated
- Responsibilities: Who is responsible and accountable, and for what?
Completed Approved Communicated
- Consultation: A description of the consultation which has already occurred and will occur in the future, and the major consultation strate-gies, including consumer and significant other consultation.
Completed Approved Communicated
- Communication: A brief overview of the strategies, which will be used to communicate information and updates about the project, its implimentation and progress.
Completed Approved Communicated
- Training: a description of any training required as a result of the project or change outcomes (based on the pre audit / baseline)
Completed Approved Communicated
- Related projects: A list or description of other projects that link / compete / work complimentarily to this project.
Completed Approved Communicated
- Critical success factors: What are the factors, which are critical to the success of the project, and therefore of which the sponsor needs to be aware.
Completed Approved Communicated
- Policy / legislative context and influences: A description or list of the affected or related policies and legislation and any change implications.
Completed Approved Communicated
- Quality assurance: A description of any quality mechanisms associated with the project.
Completed Approved Communicated
- Agency endorsement: A description of how will this be endorsed ie: via a protocol / MoU? Who will endorse this? CEOs/ Key Stakeholders / Managers How will this endorsement be communicated to staff?
Completed Approved Communicated
- Evaluation: What evaluation strategies will apply to the projectConduct Agency Post-Audit measure (ie: DDCAT / COMPASS / CHECKLIST) and compare with pre-audit
Adaptedfrom:QueenslandHealth,Managingorganisationalchange:a‘howto’guide.

Capacity Building and Change Management68

Capacity Building and Change Management 69
APPENDIX 9: FURTHER READING
Screening and assessment• A review of screening, assessment and outcome measures for Drug and Alcohol Settings, NADA 2009
http://www.nada.org.au• Screening for and assessment of co-occurring substances use and mental health disorders for Alcohol
and Other drug and Mental Health Services, Victorian Dual Diagnosis Initiative, G. Croton, 2007
Change management• Managing Organisational Change: A ‘How to’ Guide, Queensland Health, 1999• Supporting employees through organisational change – ‘How to’ Guide, Queensland Health, 1999• Tools and processes for implementing organisational change – ‘How to’ Guide, Queensland Health, 1999• Bridges, W (2009), Managing Transitions: Making the Most of Change. Lifelong Books, San Francisco• Project Implementation in the alcohol and other drug field: enablers, barriers and sustainability. Turning-
Point Alcohol & Drug centre. 2010.
Policy and procedures• NADA Policy toolkit, 2010: A resource designed to support non government drug and alcohol services
to develop and review their own policy documents. This resource provides practical policy development templates related to governance & leadership, administration &support, and service delivery. http://www.nada.org.au/index.php?option=com_content&task=view&id=236&Itemid=44
• No Wrong Door 2, 2010: Ovens and King Community Health Service. http://www.nowrongdoor.org.au• Co-morbidity/dual diagnosis competencies• Comorbidity Competencies, Improving services to support recovery from comorobidity in Tasmania.
2011. Graham & White.• National Cultural Competency Tool (NCCFT) for Mental Health Services.
Multicultural Mental Health Australia. 2010.


Capacity Building and Change Management 71
REFERENCES
Ask, A., & Roche, A.M. (2005). Clinical Supervision: A Practical Guide for the Alcohol and Other Drugs Field. Adelaide: National Centre for Education and Training on Addiction, Flinders University, Adelaide, Australia
Brager & Specht (1973), ‘Community Organising’, in Consumer Focus Collaboration (2000), Improving health services through consumer participation: a resource guide for organisations, Columbia University Press, New York.
Bridges, W. (2009), Managing transitions: making the most of change, Lifelong Books, San Francisco.
Bywood, P.T., Lunnay, B. & Roche, A. M. (2008). Effective dissemination: An examination of the costs of imple mentation strategies for the AOD field. National Centre for Education and Training on Addiction, Adelaide.
Center for Substance Abuse Treatment (2005), Substance abuse treatment for persons with co-occurring disor - ders, Substance Abuse and Mental Health Services Administration, Rockville, MD. Treatment Improve ment Protocol (TIP) Series 42. DHHS Publication No. (SMA) 05-3992.
Center for Substance Abuse Treatment (2007), Overarching principles to address the needs of persons with co-occurring disorders, Substance Abuse and Mental Health Services Administration, Rockville, MD. COCE Overview Paper 3. DHHS Publication No. (SMA) 07-4165.
Challis, J. (2011). Building co-occurring capability: An incremental approach. Presentation at VAADA Conference 2011. Melbourne
Clarke, M. & Brindle, R. (2010), Straight from the source: a practical guide to consumer participation in the Victorian alcohol and other drug sector, Association of Participating Service Users (APSU).
Coleman, M. (2003, June), ‘Supervision and the clinical social worker’, Clinical Social Work: Practice Update, vol. 3, no. 4. Retrieved on May 8 2011 at http://www.socialworkers.org/practice/clinical/csw0703b.pdf
Council of Australian Governments (COAG) (2006). National Action Plan on Mental Health 2006 – 2011, Commonwealth of Australia.
Department of Community Services and Health (2000), Mental health: statement of rights and responsibilities, Commonwealth of Australia.
Department of Health UK (2002), Mental health policy implementation guide – dual diagnosis good practice guide, Department of Health Publishing, UK.
Department of Human Services (2001), Better Access to Services Policy and Operational Framework, Victorian Government, Melbourne.
Department of Human Services (2007), Dual diagnosis: key directions and priorities for service development, Victorian Government, Melbourne.
Department of Human Services (2009), Because mental health matters: Victorian Mental Health Reform Strategy and Implementation Plan: 2009–2019, Victorian Government, Melbourne.
Department of Human Services (2009), Strengthening consumer participation in Victoria’s Public Mental Health Services Action Plan, Victorian Government, Melbourne.
Department of Public Health, Flinders University and the South Australian Community Health Research Unit (2000), Improving health services through consumer participation: a resource guide for organisations, A Consumer Focus Collaboration publication, Commonwealth Department of Health and Aged Care, Canberra.


Capacity Building and Change Management 73
Graham, H. & White, R. (2011), Comorbidity competencies: skills indicators, University of Tasmania.
Hancox, K., Lynch, L., Happell, B. & Biondo, S. (2004), ‘An evaluation of an educational program for clinical supervision’, International Journal of Mental Health Nursing, vol. 13, no. 3, pp. 198–203.
LaFond, A. & Brown, L. (2003), Guide to monitoring and evaluation of capacity-building interventions in the health sector in developing countries, MEASURE Evaluation Manual Series, No. 7, Carolina Population Center, University of North Carolina at Chapel Hill.
MacKenzie, K. R. (1990), Introduction to time-limited group therapy, American Psychiatric Press, Washington, DC.
MacLean, S., Berends, L., Hunter, B., Mugavin, J. & Roberts, B. (2010), Project implementation in the alcohol and otherdrugfield:enablers,barriersandsustainability,Turning Point Alcohol and Drug Centre, Melbourne.
Maher, Gustafson & Evans (2003), The NHS Sustainability Model, NHS Institute for Innovation and Improvement, London.
Maurer, R. (2009). Introduction to Change without Migraines. Maurer and Associates http://www.rickmaurer.com/wp/wp-content/uploads/2010/12/Intro-CWOM-tm-final.pdf [11 April 2011]
Minister of Health (2006), Te Kòkiri: The Mental Health and Addiction Action Plan 2006–2015, Ministry of Health, Wellington, New Zealand.
Minkoff, K. & Cline, C. (2003), ‘Scope of practice guidelines for addiction counselors treating the dually diagnosed counselor’, The Magazine for Addiction Professionals, October 2003, vol. 4, no. 5, pp. 24–27.
Munson, C. (2002), Social work supervision: classic statement and critical issues, Simon and Schuster.
National Centre for Education and Training on Addiction (2005), Clinical supervision: a practical guide for the alcoholandotherdrugsfield, NCETA, South Australia.
National Drug and Alcohol Research Centre (2009), Guidelines on the management of co-occurring alcohol and other drug and mental health conditions in alcohol and other drug treatment settings, NDARC, Sydney. National Resource Centre for Consumer Participation in Health (2002), Primary care self assessment tool for community and consumer participation, V1.0, May 2002.
Network of Alcohol and Other Drug Agencies (2010), NADA Policy Toolkit, Online: http://www.nada.org.au/index.php?option=com_content&task=view&id=236&Itemid=44. [Retrieved May 2011] NADA, New South Wales.
Nickols, F. (2008), Change management 101: a primer, Distance Consulting, USA. Online: http://www.nickols.us/change.htm [Retrieved March 2011]
Ovens and King Community Health Service (2010), No Wrong Door Integrated Dual Diagnosis Protocol 2010: consultation learnings from multi-agency partnership development, Online: http://www.nowrongdoor.org.au/ [Retrieved March 2011]
Project Management Institute (2010), A guide to the Project Management Body of Knowledge (PMBOK® Guide), 4th edition, Project Management Institute, USA.
Queensland Government Chief Information Office (2008) Change Management Plan: Workbook and Template Online: http://www.qgcio.qld.gov.au/qgcio/Pages/searchresults.aspx?k=Change%20Management%20 Plan%20Workbook%20and%20Template [May 2011]
Queensland Health (1999), Managing organisation change: a ‘how to’ guide, Queensland Government, Brisbane.


Capacity Building and Change Management 75
Queensland Health (2008), Service delivery for people with dual diagnosis (co-occurring) mental health and alcohol and other drug problems, Queensland Government, Brisbane.
Queensland Health (2009), Clinical supervision guidelines for mental health services, Queensland Government, Brisbane.Roche, A.M. & McDonald, J. (2001), Workforce development and capacity building: new directions for the alcohol and other drugs field, National Centre for Education and Training on Addiction (NCETA), Adelaide.
Senge, P., Kleiner, A., Roberts, C., Ross, R., Roth, G. & Smith, B. (1999), The dance of change: the challenges to sustaining momentum in learning organizations, Doubleday, USA.
Substance Abuse and Mental Health Services Administration (2002), The prevention and treatment of co-occurring substance abuse disorders and mental disorders, SAMHSA, US Department of Health and Human Services.