cancer pain: neuropathic pain and btcp sebastiano mercadante, md director anesthesia and intensive...
TRANSCRIPT

Cancer pain:Neuropathic pain and BTcP
Sebastiano Mercadante, MDDirector
Anesthesia and Intensive Care UnitAnesthesia and Intensive Care UnitPain Relief and Palliative Care UnitPain Relief and Palliative Care Unit
La Maddalena Cancer Center La Maddalena Cancer Center Palermo – ItalyPalermo – Italy
Professor of palliative medicineProfessor of palliative medicineUniversity of PalermoUniversity of Palermo

• Cancer pain is a mixed mechanism pain, rarely presenting as a pure neuropathic, visceral or somatic pain syndrome.
• Rather, it may involve inflammatory, neuropathic, ischemic, and compressive mechanisms at multiple sites
Cancer pain is complex



Neuropathic Pain Syndromes in Cancer Patients
Tumor relatedBrachial plexopathyLumbosacral plexopathyEpidural spinal cord compressionCompressive neuropathiesSciatic neuropathy, others

Non malignant Post-Mastectomy Pain
• Occurs in 5-20% of women
• More common with axillary dissection
• Can be quite severe and disabling
• Incidence probably declining
• Treatment
• Physical therapy
• Pain medications

Neuropathy induced by CH
Vinka-alkaloids (vincristine)Taxanes (paclitaxel, docetaxel)Platinum (cis, carbo, oxali-platinum) Thalidomide
Co-treatment, high cumulative dosesPrevalence:10-100%Onset & severity depend on concomitant conditions: diabetes, alcholism, paraneoplastic

Paraneoplastic neuropathy
Autoimmune response to an antigen on a nerve cell:
- SCLC (1-30%)
- Ovarian
- Breast
Dysesthesia, pain, initially distal, asymmetric
Sensory neuropathy
May preceed
Anti-Hu (blood, nerve)
Inflammation, gliosis

Assessment- Common scales, non specific to NP, sensitive to change
♠ McGill Pain Questionnaire
♠ Brief Pain Inventory
- Specific scales, sensitive to changes♠ Leeds Assessment of NP♠ NP symptom inventory♠ NP scale




Neuropathic painIt is considered a negative prognostic factor, but not absolutely
Non responsive (Arner,1988) Poor prognostic factor (Bruera,1989)Opioid resistant (Portenoy,1989, Mercadante,1992, Jadad,1992)More likely associated to cognitive failure, probably because associated with higher doses (Mercadante,1997).Higher doses of opioids (Mercadante, 2009)
•Friends against pain & suffering
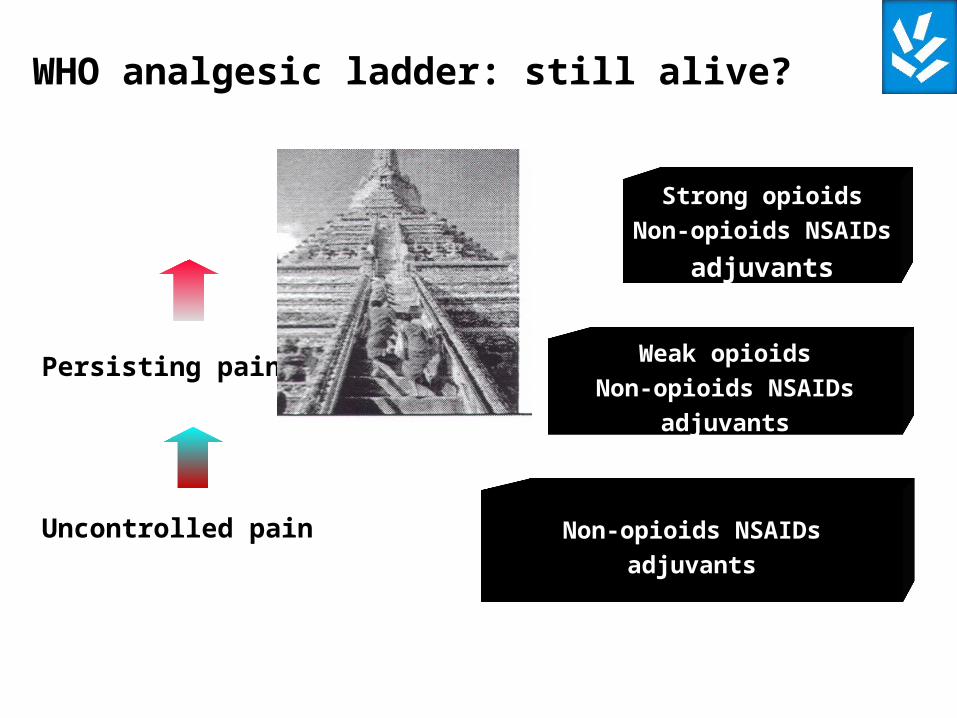
Non-opioids NSAIDs
adjuvants
Weak opioids
Non-opioids NSAIDs
adjuvants
Strong opioids
Non-opioids NSAIDs
adjuvants
Uncontrolled pain
Persisting pain
WHO analgesic ladder: still alive?

Amitriptyline in neuropatic cancer pain in patients on morphine therapy: a R-C study
Mercadante et al, Tumori 2002
Analgesic effects
No significant differences in pain intensity were found in a cross-over study, unless for “worst pain”
Adverse effects Drowsiness, confusion and dry mouth, significantly increased

Farmaci adiuvanti antiepilettici
Caraceni et al, 2000
Gabapentin dose titration in 3-7 days up to 800-1200mg, 22 pts
Decrease in global pain, burning pain, and shooting pain, as weel as allodynia...
No changes in adverse effects, decrease in myoclonus...

Gabapentin is effective in the treatmnt of cancer-related neuropathic pain: a prospective, open-label
study. Ross et al, J Palliat Med 2005
62 pts 300 to 1800 mg/day
25 Treatment - related
37 Tumor – related
Attrition rate at day 15: n = 21
Mean dose: 1200 mg/day
No differences in etiology (treatment v cancer)
Tumor-related group 97 mg/day of morphine orally (no changes)
Females more responsive?

Effectiveness of antiepileptic or antidepressant drugsWhen added to opioids for cancer pain: systematic review.
Bennett M, Palliat Med 2010
465 pts5 RCT studies (2 gabapentin, 1 amitryptiline, phenytoin, imipramine)3 observational studies (2 gabapentin, 1 valproate)
Gabapentin 1004-1395 mgAmitryptiline 50 mgOpioids kept stable or varied

Main conclusions
Opioids alone can be effective in NP Best evidence for gabapentin Reduction on >1 point, but more AEBenefit within 1 week Effect size less than that in non cancer NP (NNT and NNH different) Combination of lower dose opioid and adjuvants resultedin better outcome
Questions
Adjuvants may improve pain outomes but requires skilful prescribingLow doses combinations of adjuvants?How was NP defined ?

Pregabalin• Similar to gabapentin• More potent• Titration more feasible
•May low doses of pregabalin produce analgesia, independently from a neuropathic pain mechanism, reducing opioid escalation?
Morphine and pregabalin Morphine alone
4 weeks
CRITERIA FOR SELECTING ANALGESICS CRITERIA FOR SELECTING ANALGESICS FOR CANCER PAIN: DRIVERS IN DECISIONFOR CANCER PAIN: DRIVERS IN DECISION
Overall EfficacyOverall AE profile Individual clinical situationPretreatmentPain intensityPain mechanismOnsetComorbidity InteractionsAbuse potentialCostCultural influenceGuidelines

Breakthrough painBreakthrough pain
“..the term is typically Am-English and does not have any correspondent in other languages in Europe..”.
“..a broader and less burdened term could be
episodic or transient pain”
Mercadante & Expert Working Group of the EAPC
Cancer 2002
“The term breakthrough pain is expanding nowand more easily recognizable”

Optimisation of the opioid regimenMercadante S et al. Cancer 2002
Mercadante S, et al. J Pain Symptom Manage 2004.
• Is breakthrough pain a function of inadequate pharmacological therapy?1
– 'end-of-dose failure'
• Does breakthrough pain occur only if baseline pain is well-controlled?
– Patients suffering with frequent daily episodes often require re-assessment of the background opioid regimen2
Mostly same location as baseline pain
Higher basal pain intensity: more episodes
Resistant pain related to the onset: spontaneous recovery

pain peaks
Well controlled pain
pain peaks
Uncontrolled pain
a: typical BP pattern, requiring rescue doses. b: uncontrolled basal pain requiring both optimization of basal analgesia and rescue doses during titration. c: changes in pain intensity of both basal analgesia and BP, obtainable after optimization of therapy
a
b
c

Ideal Breakthrough Pain Medication
• Rapid onset
• Short duration of effect
• Minimal side effects
• Noninvasive, easy-to-use
• Cost-effective
Portenoy RK, Hagen NA. Pain. 1990;41:273-281.

Oral Morphine Profile
BTP Profile Overmedication
Pain relief gap
Time (minutes)5 30 60
Pai
n In
tens
ityBTP Profile

Treating Cancer Pain–Ideal
Ideal Breakthrough MedicationAround-the-Clock
Medication
Persistent PainPersistent Pain
Time
Over MedicationOver Medication
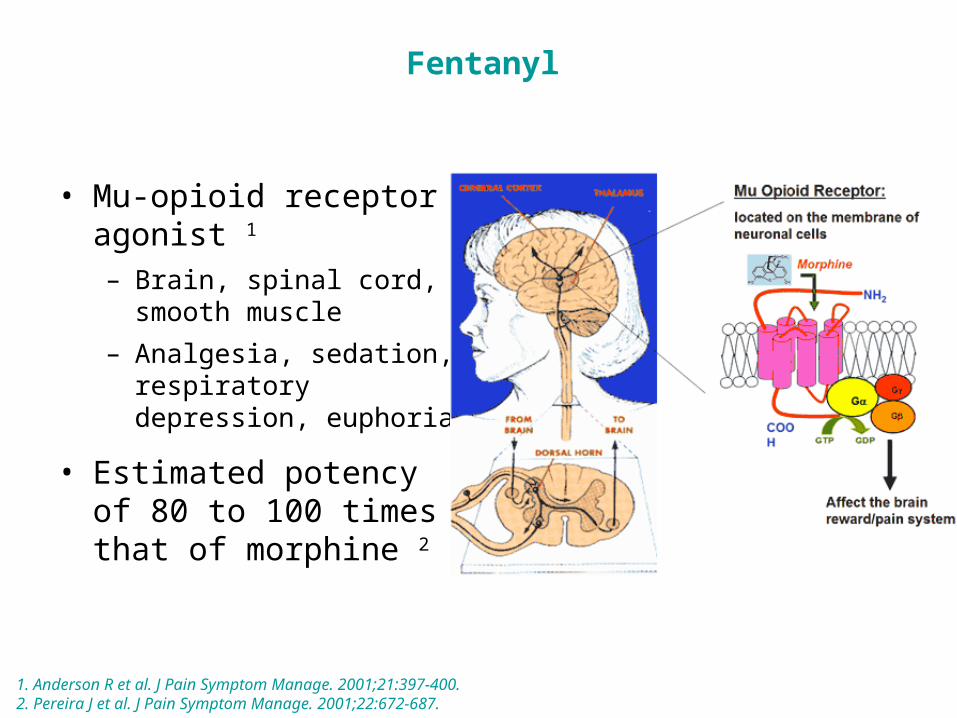
• Mu-opioid receptor agonist 1
– Brain, spinal cord, smooth muscle
– Analgesia, sedation, respiratory depression, euphoria
• Estimated potency of 80 to 100 times that of morphine 2
1. Anderson R et al. J Pain Symptom Manage. 2001;21:397-400.2. Pereira J et al. J Pain Symptom Manage. 2001;22:672-687.
Fentanyl

BTcP Therapies: Target Product Profile
• Concentration–time profile that closely mirror the pain intensity–time profile of the BTcP episode
• Delivery systems with potential to:
– Enhance dissolution
– Enhance absorption
– Minimize the first-pass effect

BTcP Therapies: Delivery Systems
1998
2006/2008
2009
2008
Oral trans-mucosal fentanyl citrateOTFC
FENTORA®(US)/ EFFENTORA™(EU)
ONSOLIS™(US) FBSF
Rapinyl™/Abstral
(EU) SLF
2009
Instanyl™(EU) INFS
2009
Nasalfent ® (EU) FPNS
Effervescent BuccalTablet
Fentanyl Buccal Soluble Film
OralTransmucosal
Lozenge
Intranasal Fentanyl Spray
SublingualFentanyl
Fentayl Pectin Nasal Spray

• Buccal/Sublingual
– Actiq
– Effentora™
– Onsolis™
– Rapinyl™/Abstral
• Intranasal
– Instanyl™
– NasalFent®
BTcP Therapies: Delivery Systems Cont.

BTcP Therapies: Early Absorption parameters
Actiq Effentora
Onsolis
Abstral
Instanyl
Nasalfent
Dose(mcg)
400100-1600
400100-800
400100-1200
400100-800
40050-200
400100-800
Dwell Time(min)
15 15-20 N/A N/A
Cmax(ng/mL)
0.6 0.9 0.7 0.7 2.5 1.5
Tmax(min)
120(30–240)
45(20–240)
60-
-(23–240)
15(6-90)
20(5-90)

Oral morphine oxycodone hydromorphone
OTFC
Effervescent fentanyl
Oral methadone
IV fentanylIntranasal fentanyl
T0 T15 T30 T45
Intravenous morphine
Sublingual fentanyl
The rush….
.. to meaningfulpain relief
A question of minutes…
Mean duration of a BP event
peak
peak

Pts should be assessed for the presence of BtcP – DPts with BtcP should have this pain specifically assessed – DThe management of BtcP should be individualized – DConsideration should be given to treatmetn of the underlying cause of pain – DConsideration should be given to avoidance of the precipitating factors – DConsideration shoulc be given to modification of the background analgesia - DOpioids are the rescue medication pf choice – DThe dose should be determined by individual titration – BNon pharmacological methods may be useful – DNon-opioid analgesics may be useful – DInterventional techniques may be useful – DPts should have BtcP re-assessed - D


Portenoy RK, et al. Pain. 1999;79:303-312. Christie JM, et al. J Clin Oncol. 1998;16:3238-3245. Farrar JT, et al. J Natl Cancer Inst. 1998;90:611-616. Coluzzi PH, et al. Pain. 2001;91:123-130.

Main concerns about OTFC studiesin breakthrough pain
BP type ? Incident ? Activity test? 66% of the episodes with placebo did not require additional dose
medication (short-lived episodes? Placebo response?) In less 42% of episodes OTFC produced a >33% change of PI
(morphine 31.8%...). Is it an effective dose? Basal pain controlled (4 episodes/day)? BP not severe enough: Mean basal PI 4.7 (with extremes 1-9) Mean breakthrough PI: 6.8 (with extremes 2-10) Many patients failed titration and dropped out without being
considered Pts on high doses do not find a successful dose...

0 100 200 300 400 500 600 700 800
120
100
100
80
60
40
20
0
Hagen et al. J Palliat Med 2007
Dose of breakthrough oral opioid versus ATC dose from the four
studies of OTFCSignificant relationship (p<0.001)
High variability
INTRAVENOUS MORPHINE FOR BREAKTHROUGH PAIN IN AN ACUTE PALLIATIVE CARE UNIT: A CONFIRMATORY STUDY.
Mercadante, et al JPSM 2008
Even given in older pts or relatively large doses, IV-MO did not result in life-threatening AE in a large number of episodes (945 events) while being effective by patients in most cases. The mean dose of IV-M was 12 mg (95% CI 9-14 mg).In 8 episodes no changes in pain intensity were observed and a further dose of IV-M was given. The remaining pts did not require further interventions. No clinical events requiring medical intervention were recorded.
The role of nurses is of paramount importance in monitoring and collecting data to gather information for audit purposes in the unit.

N° patients 25 Age 59 (55-63)
Gender (M/F) 12/13 Basal morphine dose 120 mg (96-144)
Doses (OTFC / IV-MO) events / patients 200 / 4 9 / 6
400 / 8 5 / 3 600 / 12 14 / 5 800 / 16 6 / 1 1200 / 24 13 / 8 1600 / 32 6 / 2
OTFC VERSUS IV-MORPHINE FOR BREAKTHROUGH PAIN
S. Mercadante et al, Br J Cancer 2007


Zeppetella J. Opioids for cancer breakthrough pain: a pilot study reporting patient assessment of time to meaningful
pain relief. JPSM 2008
• 50 pts
• 250 episodes
• The dose of the oral rescue dose was on average 18% of the ATC dose
• For OTFC, the rescue dose was approximately 36% of the ATC dose

Opioid titration 100 200 400 800
Proportional doses
FBT for BTcP: dose titration versus doses proportional to opioids given for background analgesia
Outcomes: - number of successful episodes- tolerability
Conclusion
- Titration may be reduce patients' complicance
- Titration has not been “scientifically” demonstrated to be superior
- Doses proportional to the opioid basal regimen has been proven to be effective and safe with different ROO, facilitating prescription for BtcP in ambulatory and home care patients

Conclusion
BP should be separately evaluatedCharacteristics stressedOptimization of opioid therapyDouble prescription: specific as neededChoice according to timing and patient’s preferenceSelected cases require more expertiseMore data needed on new technologies
