cáncer de páncreas -...
TRANSCRIPT

Diez años de avances
en el tratamiento de los tumores digestivos:
Cáncer de Páncreas
Fernando Rivera Herrero
Sv de Oncología Médica
Hospital Universitario Marqués de Valdecilla. Santander

Finantial disclosure
– Consultor: CELGENE
– Research fundings: AMGEN., MERCK-SERONO, ROCHE, SANOFI,
BAYER, LILLY, CELGENE
– Honoraria: AMGEN., MERCK-SERONO, ROCHE, SANOFI, BAYER,
LILLY, CELGENE, TECNOFARMA

Diez años de avances en el tto de los T. Digestivos: Cáncer de Páncreas
Summary
Introduction
Treatment of no metastatic PC Resectable and Borderline PC
Locally advanced PC
Treatment of metastatic PC Before 2010
FOLFIRINOX / Gem-Abx /Naliri-FuFol
New treatments
Conclusions

By the year 2020: Pancreatic cancer is expected to represent the second-leading cause of cancer-related mortality in US, trailing only lung cancer

PC is not an easy enemy …
… but we have to help our patients and avoid panic and pessimism

Adenoca de Páncreas Sv 5a 5% 1
INTRODUCCIÓN Cáncer de páncreas
Sv 5 a
1.- De Angelis R et al. EUROCARE-5. Lancet Oncol 2014; 15: 23–34
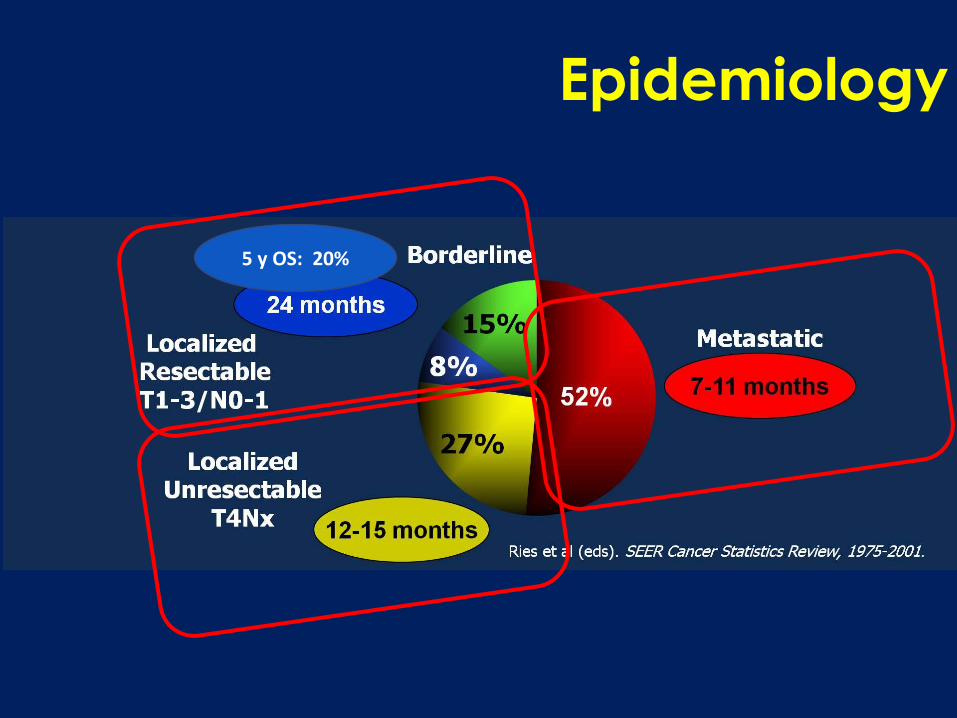
Epidemiology
5 y OS: 20%

Diez años de avances en el tto de los T. Digestivos: Cáncer de Páncreas
Summary
Introduction
Treatment of no metastatic PC Resectable and Borderline PC
Locally advanced PC
Treatment of metastatic PC Before 2010
FOLFIRINOX / Gem-Abx /Naliri-FuFol
New treatments
Conclusions
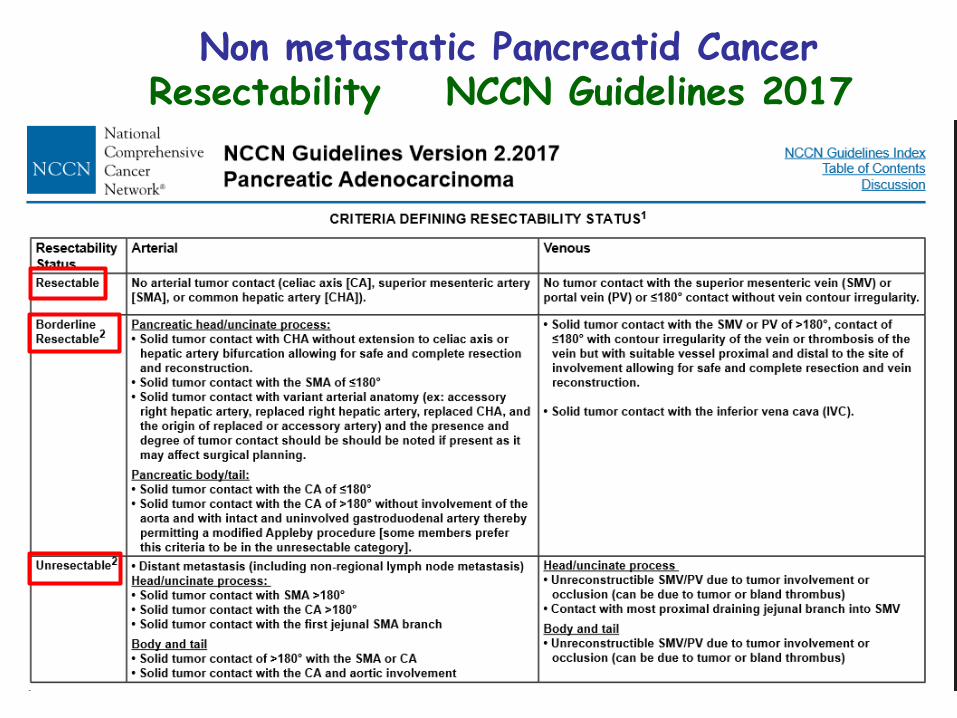
Non metastatic Pancreatid Cancer Resectability NCCN Guidelines 2017

Epidemiology
5 y OS: 20%

Resectable PC: Adjuvant CT improves DFS and OS
CT (5-FU) 5y OS: 25%
No CT 10%
ESPAC-1 1
1.- Neoptolemos et al. NEJM. 2004 2.- Oettle et al, JAMA 2007 3.- Nptolemos et al. JAMA 2010
OS HR 0.71 p 0.009
OS p 0.005
CT (Gem) 5y OS: 21 %
No CT 9 %
CONKO-3 2
CT (Gem) 5y OS: 21 %
CT (5-FU-Fol) 21 %
OS HR 0.94 p 0.39
ESPAC-3 3

Resectable PC: Adjuvant CT improves DFS and OS
CT (S1) 5y OS: 44 %
CT (Gem) 24 %
JASPAC-1 1
1.- Uesaka K, et al. Lancet 2017 3.- Nptolemos JP et al. Lancet 2017
OS HR 0.57 p < 0.001
ESPAC-4 2 CT (Gem-Cap) 5y OS: 32 %
CT (Gem) 18 %
OS HR 0.82 p 0.03

Postoperative Chemotherapy Ongoing Phase III trials
PRODIGE-24
490 PTS
R0-1 Resected Panc.Adenoca
Postop.mFOLFIRINOX
(6 months)
Postop. Gem
(6 months) Primary endpoint: DFS
F III APACT 800 PTS
R0-1 Resected Panc.Adenoca
Postop.Gem-nabPaclitaxel (6 months)
Postop. Gem
(6 months) Primary endpoint: DFS
Italy, GIP-2
490 PTS
R0-1 Resected Panc.Adenoca
Postop.FOLFOXIRI (6 months)
Postop. Gem
(6 months) Primary endpoint: DFS

Resectable PC: Doubts about the role of RT
CT/RT (5-FU) 5y OS: 12%
NoCT/RT 20 %
ESPAC-1 1
1.- Neoptolemos et al. NEJM. 2004 ; 2.- Smeenk et al, Ann Surg 2007 ; 3.- Safran et al, ASCO 2017
OS HR 1,28 p 0.05
CT/RT (5-FU) 5y OS: 25%
NoCT/RT 22 %
EORTC-40891 2
OS HR0,91 p 0.5
R0-1
Resected Panc.Adenoc. Observation Postop RT/Fu or Cape
RTOG (2nd Rand) 3 Postop. CT
(6 months)

Resectable PC: Doubts about the role of RT

RESECTABLE PC: Preoperative CT/RT or CT
Retrospective studies - SEER: 3008 pts Preoperative RT
Postoperative RT
No RT
Rand P.II : Interdisciplinary Cancer Group of Gastrointestinal Tumours (AIO, ARO, CAO)
Cis-Gem/RT Surg Gem
Surg Gem
P.III NEOPAC 1º endpoint PFS
GemOx Surg Gem
Surg Gem
310 resectable p
166 PTS
Periop.Gem-Abx
(x2 Cir x4)
Postop. Gem-Abx
(x 6)
Primary endpoint: DFS
F II Rand NEONAX
Ongoing Rand trials

Borderline PC

Epidemiology
5 y OS: 20%

Locally Advanced PC: FOLFIRINOX
Suker M, et al. Lancet Oncol. 2016;17(6):801-810.
FOLFIRINOX for Locally Advanced Pancreatic Cancer:A Systematic Review and Patient-Level Meta-Analysis
Background: 35% of patients with pancreatic cancer have unresectable locally advanced disease at diagnosis
Suker M, et al. Lancet Oncol. 2016;17(6):801-810.
FOLFIRINOX for Locally Advanced Pancreatic Cancer:A Systematic Review and Patient-Level Meta-Analysis
Background: 35% of patients with pancreatic cancer have unresectable locally advanced disease at diagnosis
• Applicability of results from trials on stage IV to stage III may be tricky
• Stage-specific trials are mandatory and patients should be offered them
GAP (Gemcitabine Abraxane Pancreas) TrialPhase III PRODIGE 29-NEOPAN Trial in LAPC:
FOLFIRINOX vs Gemcitabine
National Institutes of Health. http://clinicaltrials.gov/ct2/show/NCT02539537 and
http://clinicaltrials.gov/ct2/show/NCT02043730. Accessed: 21 September 2017.
Suker M et al. Lancet Oncol 2016
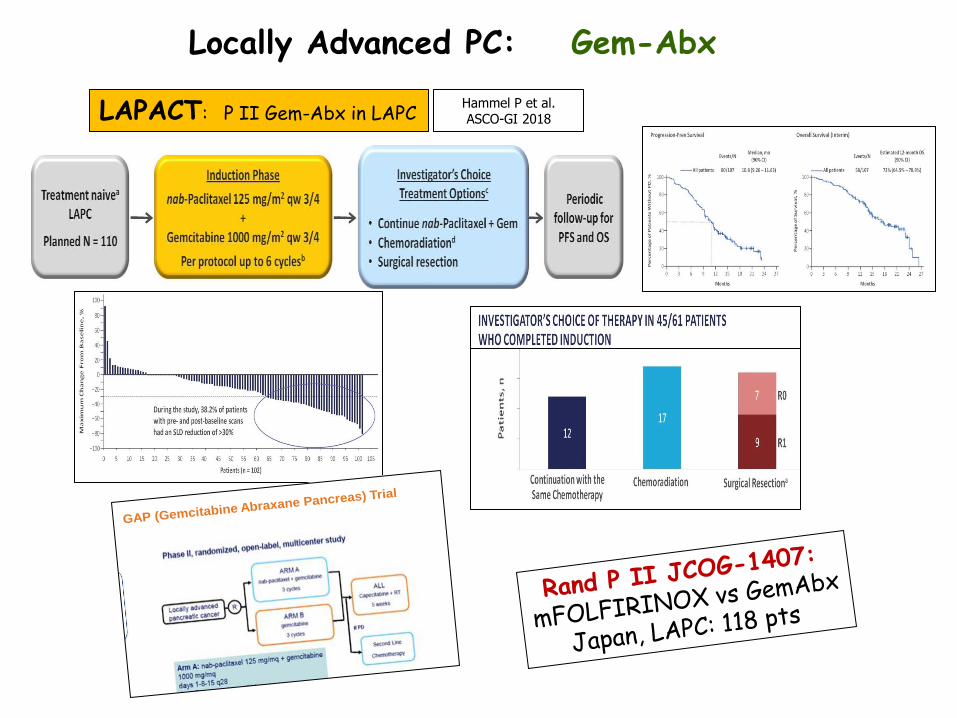
Locally Advanced PC: Gem-Abx
Hammel P et al. ASCO-GI 2018 LAPACT: P II Gem-Abx in LAPC
• Applicability of results from trials on stage IV to
stage III may be tricky
• Stage-specific trials are mandatory and patients
should be offered them
GAP (Gemcitabine Abraxane Pancreas) Trial
Phase III PRODIGE 29-NEOPAN Trial in LAPC:
FOLFIRINOX vs Gemcitabine
National Institutes of Health. http://clinicaltrials.gov/ct2/show/NCT02539537 and
http://clinicaltrials.gov/ct2/show/NCT02043730. Accessed: 21 September 2017.

442 pts Locally Advanced PC
Gem-erlotinib x 4 Gem x 4
P III LAP 07 (GERCOR)
Cap-RT Gem / Gem-erlo x 2
1º endpoint OS
269 pts (61%)
Hammel P et al. JAMA 2016
Hammel P, et al. JAMA. 2016;315(17):1844-1853.
Effect of Chemoradiotherapy vs Chemotherapyon Survival in Patients With Locally Advanced
Pancreatic Cancer Controlled After Four Monthsof Gemcitabine With or Without Erlotinib
The LAPO7 Randomized Clinical Trial
Locally Advanced PC: Radiotherapy??


Strobel O, et al. Surgery. 2012;152(3 Suppl 1):S33-S42.
Overall Post-Operative Survival
Resection After Neoadjuvant Therapy for Locally Advanced, “Unresectable” Pancreatic Cancer
P<.004
P = .19
Locally Advanced PC: Salvage suergery

Diez años de avances en el tto de los T. Digestivos: Cáncer de Páncreas
Summary
Introduction
Treatment of no metastatic PC Resectable and Borderline PC
Locally advanced PC
Treatment of metastatic PC Before 2010
FOLFIRINOX / Gem-Abx /Naliri-FuFol
New treatments
Conclusions

Hidalgo M et al. CTO 2016
% of pts ??
30% ? 35% ? 35% ?

It is important to avoid delays in the treatment of mPC
Suzuki R et al. ASCO-GI 2015
Sv
Short: <10 days

Diez años de avances en el tto de los T. Digestivos: Cáncer de Páncreas
Summary
Introduction
Treatment of no metastatic PC Resectable and Borderline PC
Locally advanced PC
Treatment of metastatic PC Before 2010
FOLFIRINOX / Gem-Abx / Naliri-FuFol
New treatments
Conclusions


RR, PFS and OS in mPC
- Gem (30 min) 5-12% 3,5m 5,5m 18% - GEMOX / GEMCAP 25% 5 m 7m 25% - Gem-Erlotinib 8,6% 3,8m 6,3m 24%
Treatment RR PFS OS 1y OS

Diez años de avances en el tto de los T. Digestivos: Cáncer de Páncreas
Summary
Introduction
Treatment of no metastatic PC Resectable and Borderline PC
Locally advanced PC
Treatment of metastatic PC Before 2010
FOLFIRINOX / Gem-Abx / Naliri-FuFol
New treatments
Conclusions

342 PTS (2005-09, 48 centers)
Rand PII: 88 pts RR 31,8 vs 11,3%P.III
Criteria <76 y (28% > 65 y)
M1
PS ECOG 0-1
Bilirrubine < 1,5 x UNL
Normal renal,hema.function No cardiocirc. disease...
FOLFIRINOX
P. II-III Prodige 4- ACCORD 11 FOLFIRINOX vs Gemcitabine
Gem (30 min)
6 m (stop and go)
1ºendpoint:OS OS (median) 11,1 m HR 0,57 p<0,0001 6,8 m
1 year 48,4% 20,6%
PFS 6,4 m HR 0,47 p<0,0001 3,3 m
RR: 31,6% p<0,0001 9,4%
Dis Control: 70,2% p<0,0001 50,9%
Conroy T et al. N Engl J Med 2011;364:1817-25.

G-CSF 42% 5%
F. III Prodige 4- ACCORD 11 Toxicity: G 3-4
No colangitis and no more toxicity in patients with biliar stent

861 PTS (151 sites, 11 contries) M1
KPS ≥ 70
Bilirrubine < UNL
nabPaclitaxel-Gem nabP; 125 mg/m2 iv Gem: 1000 mg/m2 iv weekly 3/4 w
P. III MPACT 1 nabPaclitaxel-Gem vs Gemcitabine
Gem (30 min)
Gem 1000 mg/m2 iv weekly 7/8 w followed by 3/4 w
1ºendpoint:OS
1.- Von Hoff DD et al. N Engl J Med 2013; 2.- (OS updated results) Goldstein D et al. ASCO-GI 2014
OS 2 (mediana) 8.7 m HR 0,72 p<0,0001 6,6 m
1 y 35% 22%
2 y 10% 4%
PFS 5.5 m HR 0,69 p<0,001 3,7 m
RR (central rev): 23% p<0,001 7%
Dis Control: 48% p<0,001 33%
PFS

CA19-9, carbohydrate antigen 19-9; Gem, gemcitabine; KPS, Karnofsky performance status; nab-P, nab-paclitaxel; ULN, upper
limit of normal. Von Hoff DD, Ervin T, Arena FP, et al. Randomized Phase III Study of Weekly nab-Paclitaxel plus Gemcitabine vs Gemcitabine Alone in Patients with
Metastatic Adenocarcinoma of the Pancreas (MPACT) [abstract LBA148]. Oral presentation at: The Gastrointestinal Cancers Symposium 2013;
January 24-26; San Francisco, CA.
OS - Prespecified Subgroups
3
4
>65: 42%
KPS 70-80: 40%

Preferred Term nab-P + Gem
n = 421
Gem
n = 402
Patients with at least 1 AE leading to death, % 4 4
Grade ≥ 3 hematologic AEs,a %
Neutropenia
Leukopenia
Thrombocytopenia
Anemia
38
31
13
13
27
16
9
12
Patients who received growth factors, % 26 15
Febrile neutropenia,b % 3 1
Grade ≥ 3 nonhematologic AEsb in > 5% of patients, %
Fatigue
Peripheral neuropathyc
Diarrhea
17
17
6
7
< 1
1
Grade ≥ 3 neuropathy
Time to onset in days, median
Time to improvement to grade ≤ 1 in days, median
Patients who resumed nab-P, %
140
29
44
113
--
--
Safety

Abraxane in mPC
Abraxane was approved by FDA (2013) and EMA (2014) for first line treatment of metastatic pancreatic adenocarcinoma

Primary Endpoint OS
Conroy T. N Engl J Med 2011;364:1817-
25
mOS 11.1m FOLFIRINOX VS. 6.8 m G
mOS 8.7 m NP-G vs. 6.6 m G
Von Hoff DD, N Engl J Med. 2013;369:1691-1703

Características de las poblaciones
Estudio PRODIGE/ACCORD FOLFIRINOX
MPACT GZT+NBP
Edad (mediana y rango) 61 años (25-76) 63 años (27-86)
Pacientes ancianos >76 años No Si
Pacientes PS0 37% 16%
Pacientes PS2 1% 7%
Mediana de localizaciones metastásicas
2 3
Ca19.9 >59 LAN
(medida indirecta carga tumoral)
++ 42%
+++ 52%
MPACT
• Población con características clínicas más desfavorables en cáncer de páncreas: más jóvenes y más “sanos”

Tabernero et al. Beaujon Conference 2014
Pacientes ECOG 0-1 MPACT
Mediana de SG con Gem-Abx: 9,7 meses
Tabernero J et al, The Oncologist 2015;20:1–8

FRAGANCE: Gem-Abx in mPC with ECOG 2
MPACT (GA): 8.5 m MPACT (GA): 5.5 m
Hidalgo M et al, ESMO 2017

FRAGANCE
Hidalgo M et al, ESMO 2017

Braiteh, ASCO-GI. 2016. Abst 433
Retrospective Study Gem/Abx and FOLFIRINOX in mPC
U.S. community oncology Database (Jun 2013->Jun 2014)
Gem-Abx 122 pts FOLFIRINOX 80 pts Age (mean) 67 y 61.4 y

Date of preparation March 2016 INT-ABR160015
151611844624 14 3 1 11
OFF vs FF as 2nd-line therapy for APC*
(CONKO-003)
OFF†
FF
Stratification: Presence of metastases, duration of 1st-line gemcitabine therapy (3, 3–6, or >6 months),
KPS (70–80% or 90–100%)
Primary endpoint: OS
Secondary endpoints: TTP, tolerability
• PD following gemcitabine 1st-line therapy
• KPS ≥70
• Measureable
disease
100
80
60
20
0
40
Time (months)
86 0 3 12 15 24 27 38 33 6 9 18 21 30
0 76 34 6 5 1 1 0 1 14 7 5 3 1 1 84 20 3 3 2 2 1 2 9 7 2 2 2 FF
OFF No at risk
100
80
60
20
0
40
Time (months) No at risk
48 18 9 12 0 3 6 36 24 30 42 86 54
FF OFF 2 10 22 15 76 59 37 4 6 5 3 0 1
Overa
ll s
urv
ival (%
) P
rogre
ssio
n-f
ree s
urv
iva
l (%
)
OFF median 2.9 months (95% CI 2.4–3.2)
FF median 2.0 months (95% CI 1.6–2.3)
HR 0.68 (95% CI 0.50–0.94) p=0.019
OFF median 5.9 months (95% CI 4.1–7.4)
FF median 3.3 months (95% CI 2.7–4.0)
HR 0.66 (95% CI 0.48–0.91) p=0.010
R 1:1
Oettle et al. JCO 2014;32:2423-9
*>88% of patients had metastatic disease †OFF differs from FOLFOX (folinic acid, fluorouracil, and oxaliplatin)
with respect to the frequency of treatment administration: fluorouracil
is administered weekly for the first 4 weeks, and oxaliplatin is
administered on Days 8 and 22 of a 6-week cycle
2nd line in mPC
Naliri: NAPOLI-1
Oxali: CONKO-003
Oxali: PANCREOX

Sequence of treatment in mPCP

2017: A Classical Case of mPDAC
Nab-paclitaxel +
gemcitabine
2018

Diez años de avances en el tto de los T. Digestivos: Cáncer de Páncreas
Summary
Introduction
Treatment of no metastatic PC Resectable and Borderline PC
Locally advanced PC
Treatment of metastatic PC Before 2010
FOLFIRINOX / Gem-Abx / Naliri-FuFol
New treatments
Conclusions



Veliparib (Inhibidor de PARP)
F IB : Cis-Gem-Veliparib 1 9 pts con mut BRCA 1,2: 5 RP y 4 EE
1.- O´Reilly EM, et al. ASCO 2014, #4023
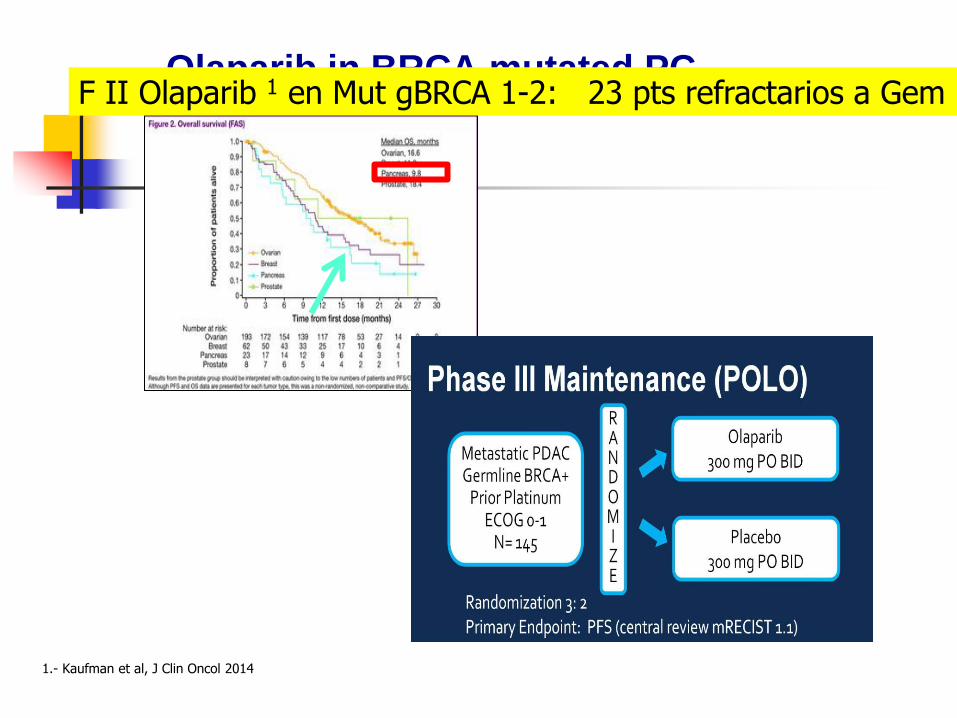
Olaparib in BRCA mutated PC
1.- Kaufman et al, J Clin Oncol 2014
F II Olaparib 1 en Mut gBRCA 1-2: 23 pts refractarios a Gem


Cubillo A et al. ESMO 2017
O´Reilly E et al. ASCO-GI 2017
mPC: Targeting the Notch pathway



279 pts HA hight 84 pts (30%)
420 PTS
Placebo-Gem-Abx PEGPH20-Gem-Abx Primary endpoints: PFS / OS
P III HALO 301
mPC; HA hight




Possibilities of combination with Immune checkpoint inhibitors
Philip AP. ASCO-GI 2017



Protegido del sistema inmune
IDO inh
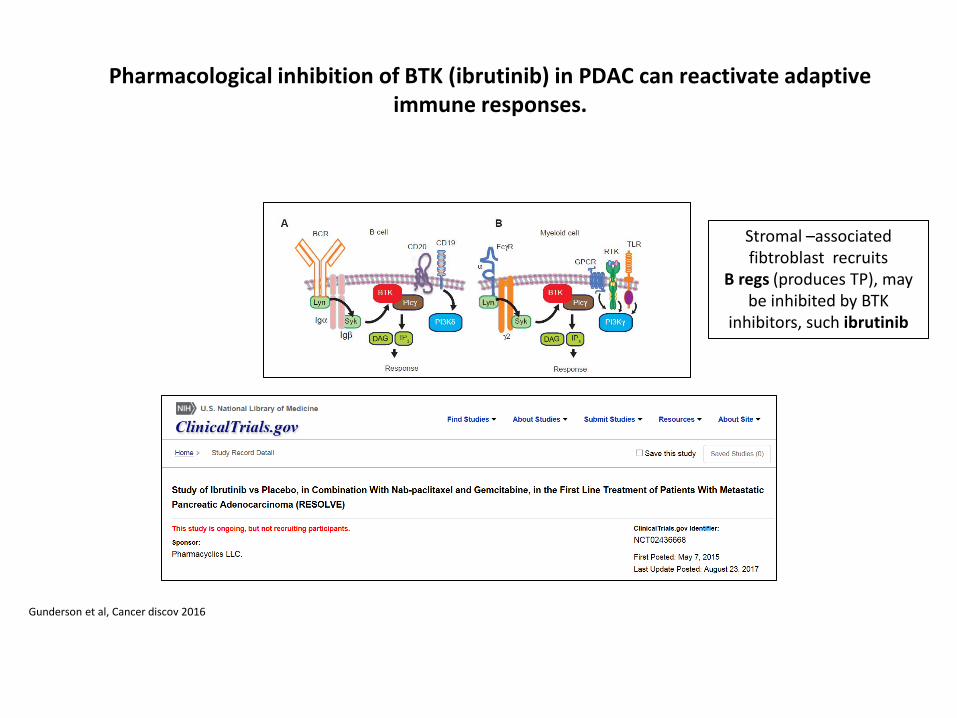
Pharmacological inhibition of BTK (ibrutinib) in PDAC can reactivate adaptive immune responses.
Gunderson et al, Cancer discov 2016
Stromal –associated fibtroblast recruits
B regs (produces TP), may be inhibited by BTK
inhibitors, such ibrutinib

Diez años de avances en el tto de los T. Digestivos: Cáncer de Páncreas
Summary
Introduction
Treatment of no metastatic PC Resectable and Borderline PC
Locally advanced PC
Treatment of metastatic PC Before 2010
FOLFIRINOX / Gem-Abx / Naliri-FuFol
New treatments
Conclusions

Conclusions

Conclusions .- Resectable PC
Adj CT: Gem-Cap (waiting for FOLFIRINOX and Gem-Abx)
Borderline PC Preoperative CT (+/-RT)
.- Locally Advanced PC
CT: FOLFIRINOX or Gem-Abx
No stablish role for RT
Salvage Sx if feasible
.- Metastatic PC
In 2010: P III FOLFIRINOX: Active (but toxic)
P III MPACT: Gem-Abx is active and less toxic.
FRAGANCE: Gem-Abx in ECOG-2
New targeted drugs: some negative trials but a lot of ongoing trials

Gracias Thank you