cancer and heart attack: a capecitabine story · cancer and heart attack: a . capecitabine story....
TRANSCRIPT
CentralBringing Excellence in Open Access
Journal of Cardiology & Clinical Research
Cite this article: Maruri Sánchez RF, Díez-Villanueva P, Revuelta JR, Alfonso F (2017) Cancer and Heart Attack: A Capecitabine Story. J Cardiol Clin Res 5(6): 1117.
*Corresponding author
Pablo Díez-Villanueva, Department of cardiology, Hospital Universitario La Princesa, Madrid, Spain; Email:
Submitted: 17 July 2017
Accepted: 18 August 2017
Published: 19 August 2017
Copyright© 2017 Díez-Villanueva et al.
OPEN ACCESS
Keywords•Capecitabine•Cardiotoxicity•Myocardial infarction
Case Report
Cancer and Heart Attack: A Capecitabine StoryRamón F. Maruri Sánchez1, Pablo Díez-Villanueva1*, Jacobo Rogado Revuelta2, and Fernando Alfonso1
1Department of Cardiology, La Princesa University Hospital, Spain 2Department of Oncology, La Princesa University Hospital, Spain
Abstract
A 55-year-old female, smoker, with no previous family or personal history of heart disease, treated with capecitabine due to metastatic breast cancer, was admitted to our hospital due to typical chest pain, with electrocardiographic changes and slight elevation of markers of myocardial damage. Diagnosis of non ST elevation myocardial infarction was achieved. Coronary angiography revealed no significant coronary lesions, and coronary vasospasm test was negative. Cardiac MRI showed normal ventricular ejection fraction, and no macroscopic myocardial fibrosis was observed. The event was attributed to capecitabine, although the mechanism by which it occurred remains unknown.
CASE PRESENTATIONA 55-year-old woman with previous history of smoking and
no any family or personal history of heart disease was admitted to our hospital because of typical chest pain.
In 2009 she was diagnosed of breast cancer, undergoing surgery, radiotherapy, chemotherapy and hormone therapy. She had a recurrence of the disease with bone metastases. Despite various antitumor drugs and because of the progression of bone involvement, capecitabine was initiated.
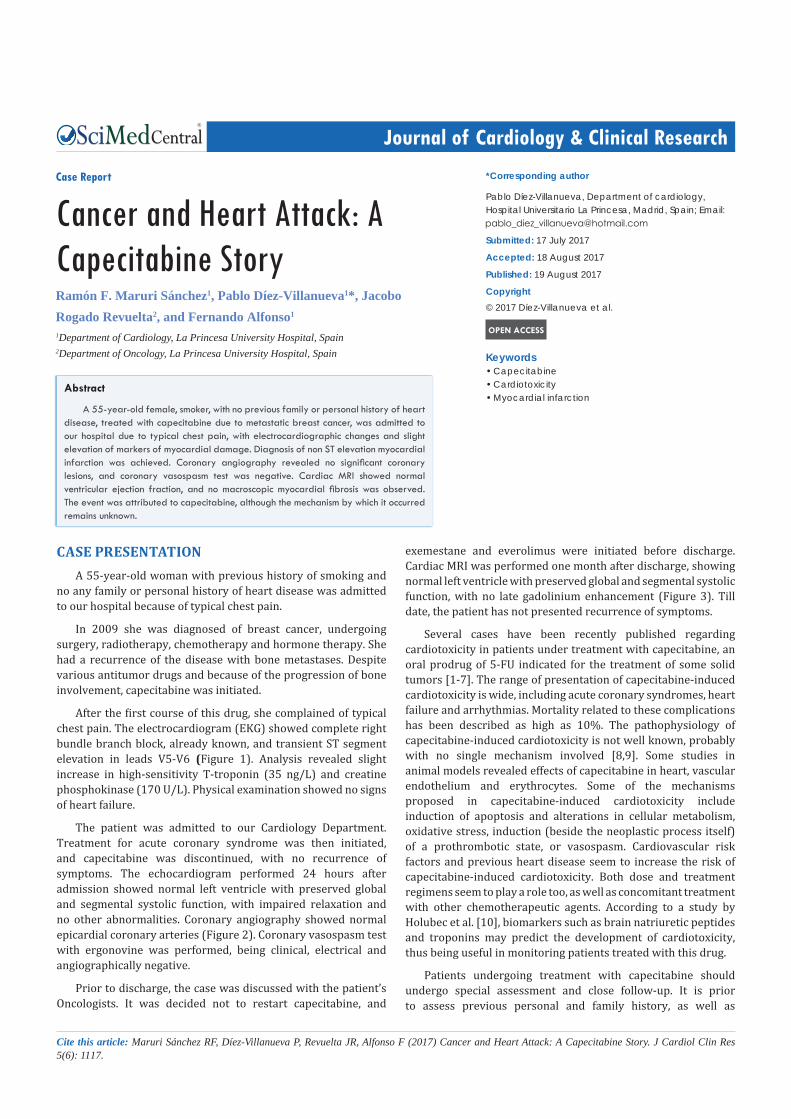
After the first course of this drug, she complained of typical chest pain. The electrocardiogram (EKG) showed complete right bundle branch block, already known, and transient ST segment elevation in leads V5-V6 (Figure 1). Analysis revealed slight increase in high-sensitivity T-troponin (35 ng/L) and creatine phosphokinase (170 U/L). Physical examination showed no signs of heart failure.
The patient was admitted to our Cardiology Department. Treatment for acute coronary syndrome was then initiated, and capecitabine was discontinued, with no recurrence of symptoms. The echocardiogram performed 24 hours after admission showed normal left ventricle with preserved global and segmental systolic function, with impaired relaxation and no other abnormalities. Coronary angiography showed normal epicardial coronary arteries (Figure 2). Coronary vasospasm test with ergonovine was performed, being clinical, electrical and angiographically negative.
Prior to discharge, the case was discussed with the patient’s Oncologists. It was decided not to restart capecitabine, and
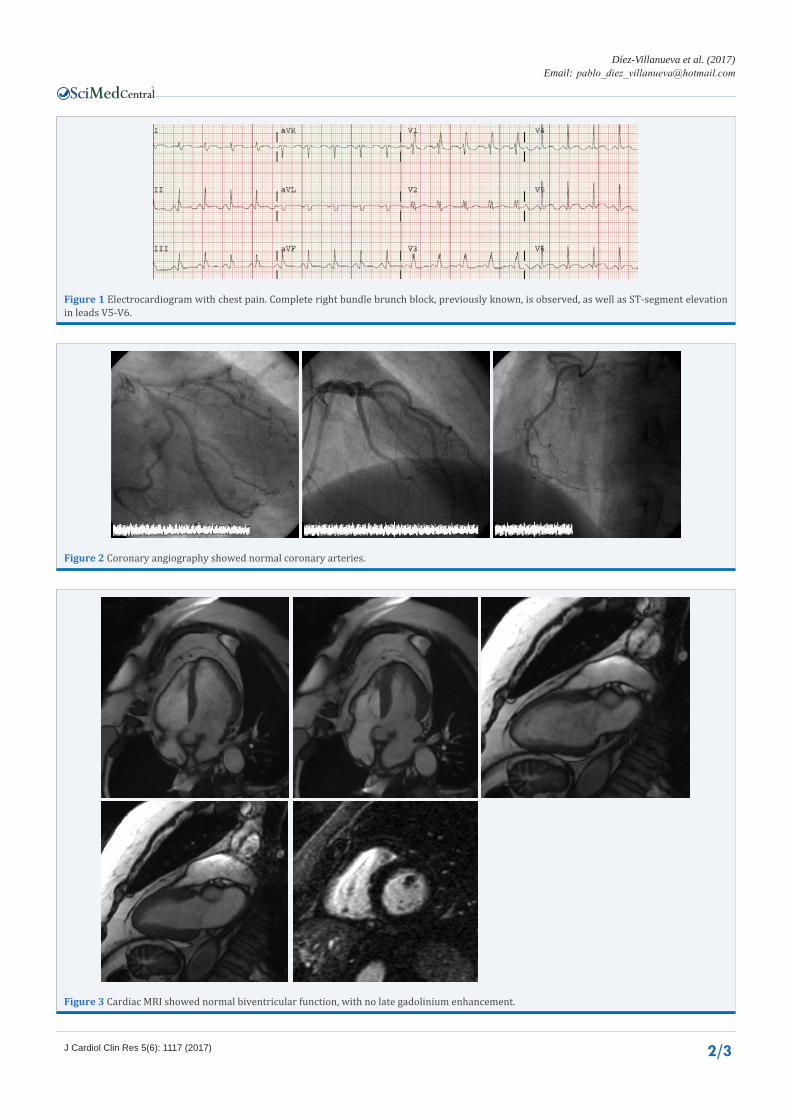
exemestane and everolimus were initiated before discharge. Cardiac MRI was performed one month after discharge, showing normal left ventricle with preserved global and segmental systolic function, with no late gadolinium enhancement (Figure 3). Till date, the patient has not presented recurrence of symptoms.
Several cases have been recently published regarding cardiotoxicity in patients under treatment with capecitabine, an oral prodrug of 5-FU indicated for the treatment of some solid tumors [1-7]. The range of presentation of capecitabine-induced cardiotoxicity is wide, including acute coronary syndromes, heart failure and arrhythmias. Mortality related to these complications has been described as high as 10%. The pathophysiology of capecitabine-induced cardiotoxicity is not well known, probably with no single mechanism involved [8,9]. Some studies in animal models revealed effects of capecitabine in heart, vascular endothelium and erythrocytes. Some of the mechanisms proposed in capecitabine-induced cardiotoxicity include induction of apoptosis and alterations in cellular metabolism, oxidative stress, induction (beside the neoplastic process itself) of a prothrombotic state, or vasospasm. Cardiovascular risk factors and previous heart disease seem to increase the risk of capecitabine-induced cardiotoxicity. Both dose and treatment regimens seem to play a role too, as well as concomitant treatment with other chemotherapeutic agents. According to a study by Holubec et al. [10], biomarkers such as brain natriuretic peptides and troponins may predict the development of cardiotoxicity, thus being useful in monitoring patients treated with this drug.
Patients undergoing treatment with capecitabine should undergo special assessment and close follow-up. It is prior to assess previous personal and family history, as well as
CentralBringing Excellence in Open Access
Díez-Villanueva et al. (2017)Email:
2/3J Cardiol Clin Res 5(6): 1117 (2017)
Figure 1 Electrocardiogram with chest pain. Complete right bundle brunch block, previously known, is observed, as well as ST-segment elevation in leads V5-V6.
Figure 2 Coronary angiography showed normal coronary arteries.
Figure 3 Cardiac MRI showed normal biventricular function, with no late gadolinium enhancement.

CentralBringing Excellence in Open Access
Díez-Villanueva et al. (2017)Email:
3/3J Cardiol Clin Res 5(6): 1117 (2017)
Maruri Sánchez RF, Díez-Villanueva P, Revuelta JR, Alfonso F (2017) Cancer and Heart Attack: A Capecitabine Story. J Cardiol Clin Res 5(6): 1117.
Cite this article
cardiovascular risk factors. ECG and echocardiography should be early performed in order to anticipate possible complications. Other treatments instead of capecitabine should also be taken into account. Moreover, patients ought to be warned about adverse effects and ask for medical attention in case of specific signs or symptoms. In case of cardiovascular complications, discontinuation of capecitabine must be considered. In our opinion, more studies are necessary to well identify the mechanisms involved in capecitabine-induced cardiotoxicity, as well as specific markers that may help to early recognize development of cardiotoxicity.
REFERENCES1. Ang C, Kornbluth M, Thirlwell MP, Rajan RD. Capecitabine-
induced cardiotoxicity: case report and review of the literature. Curr Oncol. 2010; 17: 59-63.
2. Camaro C, Danse PW, Bosker HA. Acute chest pain in a patient treated with capecitabine. Neth Heart J. 2009; 17: 288-291.
3. Díez Martínez AM, Navarro Martínez A, Sáez Méndez L, Valladolid Walsh A. Acute coronary syndrome in a patient previously treated with capecitabine and 5-fluorouracil. Farm Hosp. 2005; 29: 295-296.
4. Güvenç TS, Celiker E, Ozcan KS, Ilhan E, Eren M. Acute
myocardial infarction after capecitabine treatment: not always vasospasm is responsible. Chin Med J (Engl). 2012; 125: 3349-3351.
5. Scott PA, Ferchow L, Hobson A, Curzen NP. Coronary spasm induced by capecitabine mimicks ST elevation myocardial infarction. Emerg Med J. 2008; 25: 699-700.
6. Sentürk T, Kanat O, Evrensel T, Aydinlar A. Capecitabine-induced cardiotoxicity mimicking myocardial infarction. Neth Heart J. 2009; 17: 277-280.
7. Y-Hassan S, Tornvall P, Törnerud M, Henareh L. Capecitab-ine caused cardiogenic shock through induction of global Takotsubo syndrome. Cardiovasc Revasc Med. 2013; 14: 57-61.
8. Polk A, Vaage-Nilsen M, Vistisen K, Nielsen DL. Cardiotoxicity in can-cer patients treated with 5-fluorouracil or capecitabine: a systematic review of incidence, manifestations and predisposing factors. Can-cer Treat Rev. 2013; 39: 974-984.
9. Polk A, Vistisen K, Vaage-Nilsen M, Nielsen DL. A systematic review of the pathophysiology of 5-fluorouracil-induced cardiotoxicity. BMC Pharmacol Toxicol. 2014; 15: 47.
10. Holubec L Jr, Topolcan O, Finek J, Salvet J, Svoboda T, Svobodova S, Mrazkova P, Ludvikova M. Dynamic monitoring of cardio-specific markers and markers of thyroid gland function in cancer patients--a pilotstudy. Anticancer Res. 2007; 27: 1883-1886.