camelia registry slovakia and czech...
TRANSCRIPT

Indrák K.1, Faber E.1, Demečková E.2, Demitrovičová L.3, Voglová J.4, Jindra P. 5, Markuljak I.6, Chudej J.7, Cmunt E.8, Tóthová E.9, ŠtecováN.10, Palášthy S.11, Mužík J.12, Dušek L.12
CAMELIA REGISTRY Slovakia and Czech Republic
1. Dept. Hematooncology Olomouc, CR2. Dept. Hematology and Blood Transfusion, Bratislava, SR3. Dept . Internal Medicine, Division Hematol. and Blood Transfusion, NCI, Bratislava, SR4. 4th Dept. Internal Medicine - Hematology, Hradec Králové, CR5. Dept. Hematooncology, Plzeň, CR6. Dept. Hematology and Blood Transfusion, Martin, SR7. Dept. Hematology, Banská Bystrica, SR8. Dept. Internal Medicine, General University Hospital, Prague, CR9. Dept. Hematology and Hematooncology, Košice, SR10. HEMKO Ltd., Hematology and Onco-Hematology Outpatient Dept., Košice, SR11. J. A. Rieman Health Centre, Dept. Hematology, Prešov, SR12. Institute of Biostatistics and Analyses, Brno, CR
Institute of Biostatistics and AnalysesMasaryk University
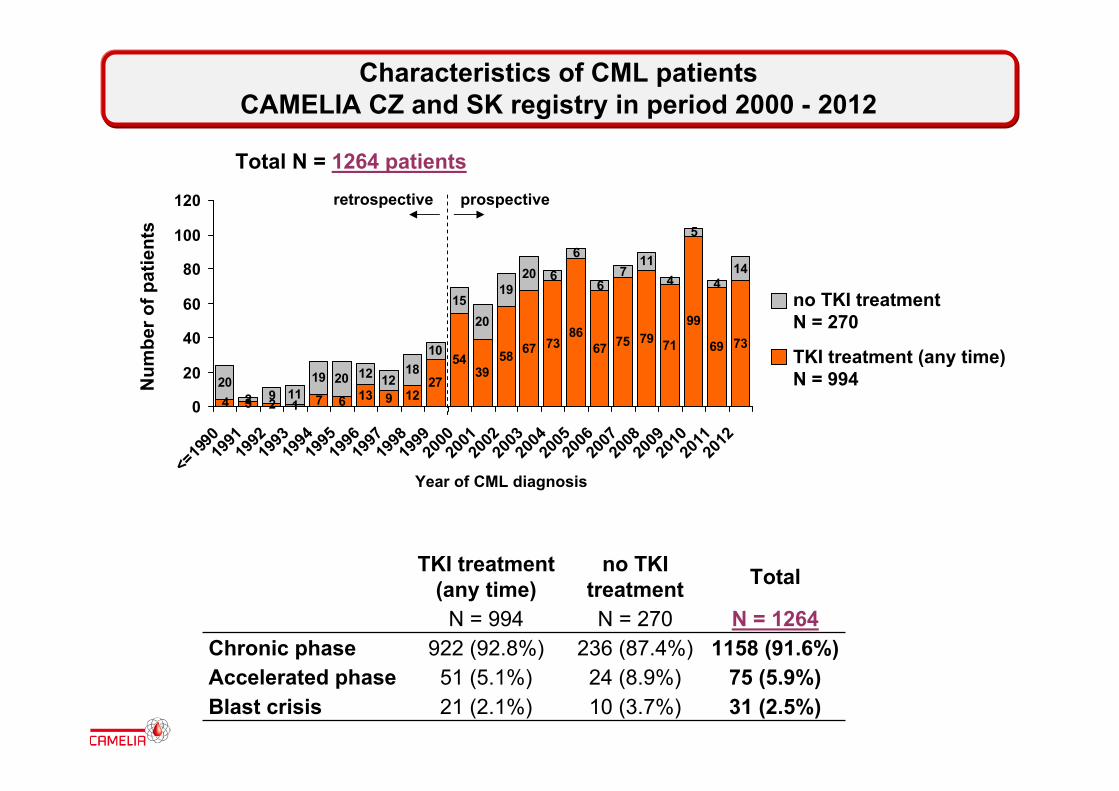
Characteristics of CML patients CAMELIA CZ and SK registry in period 2000 - 2012
4 3 2 1 7 6 13 9 1227
5439
58 67 7386
67 75 79 71
99
69 73
202 9 11
19 20 12 1218
10
1520
1920 6
6
67
114
5
414
0
20
40
60
80
100
120
<=19
9019
9119
9219
9319
9419
9519
9619
9719
9819
9920
0020
0120
0220
0320
0420
0520
0620
0720
0820
0920
1020
1120
12
Num
ber o
f pat
ient
s
Year of CML diagnosis
Total N = 1264 patients
TKI treatment (any time)
no TKI treatment Total
N = 994 N = 270 N = 1264Chronic phase 922 (92.8%) 236 (87.4%) 1158 (91.6%)Accelerated phase 51 (5.1%) 24 (8.9%) 75 (5.9%)Blast crisis 21 (2.1%) 10 (3.7%) 31 (2.5%)
TKI treatment (any time)N = 994
no TKI treatmentN = 270
prospectiveretrospective
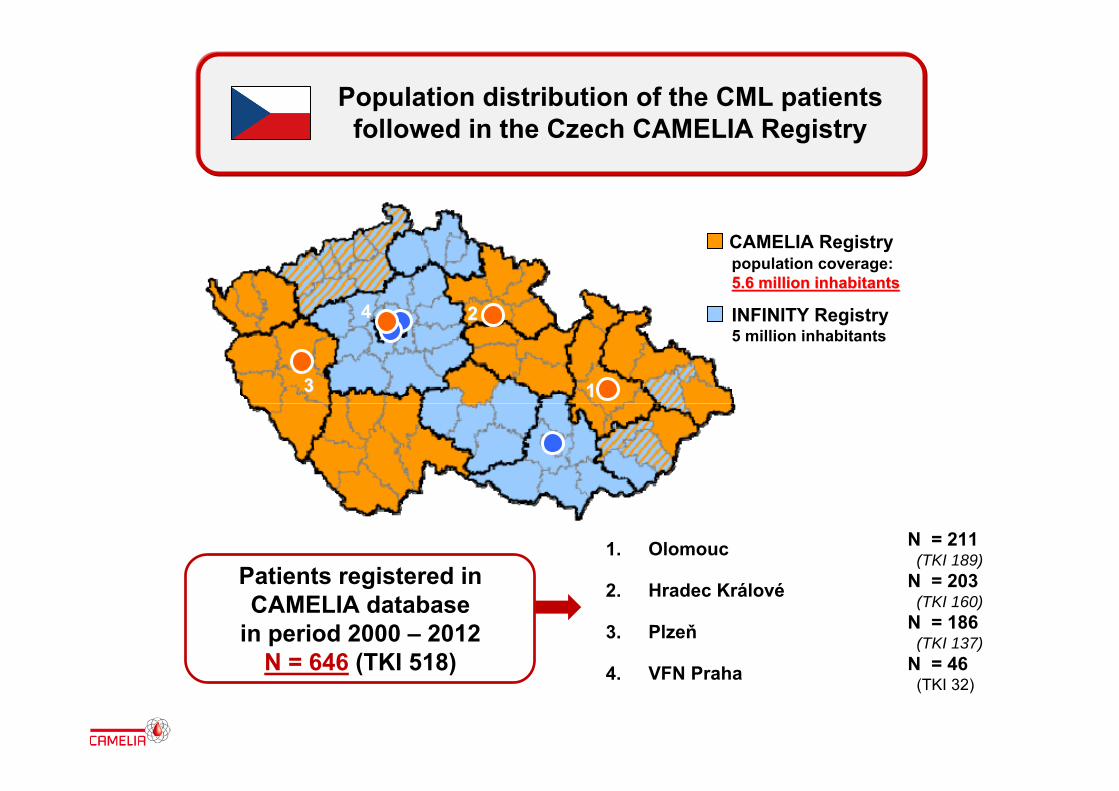
Patients registered in CAMELIA database
in period 2000 – 2012N = 646 (TKI 518)
11
22
33
44
CAMELIA Registry
INFINITY Registry5 million inhabitants
Population distribution of the CML patients followed in the Czech CAMELIA Registry
1. Olomouc N = 211(TKI 189)
2. Hradec Králové N = 203(TKI 160)
3. Plzeň N = 186(TKI 137)
4. VFN Praha N = 46(TKI 32)
population coverage:5.6 million inhabitants5.6 million inhabitants
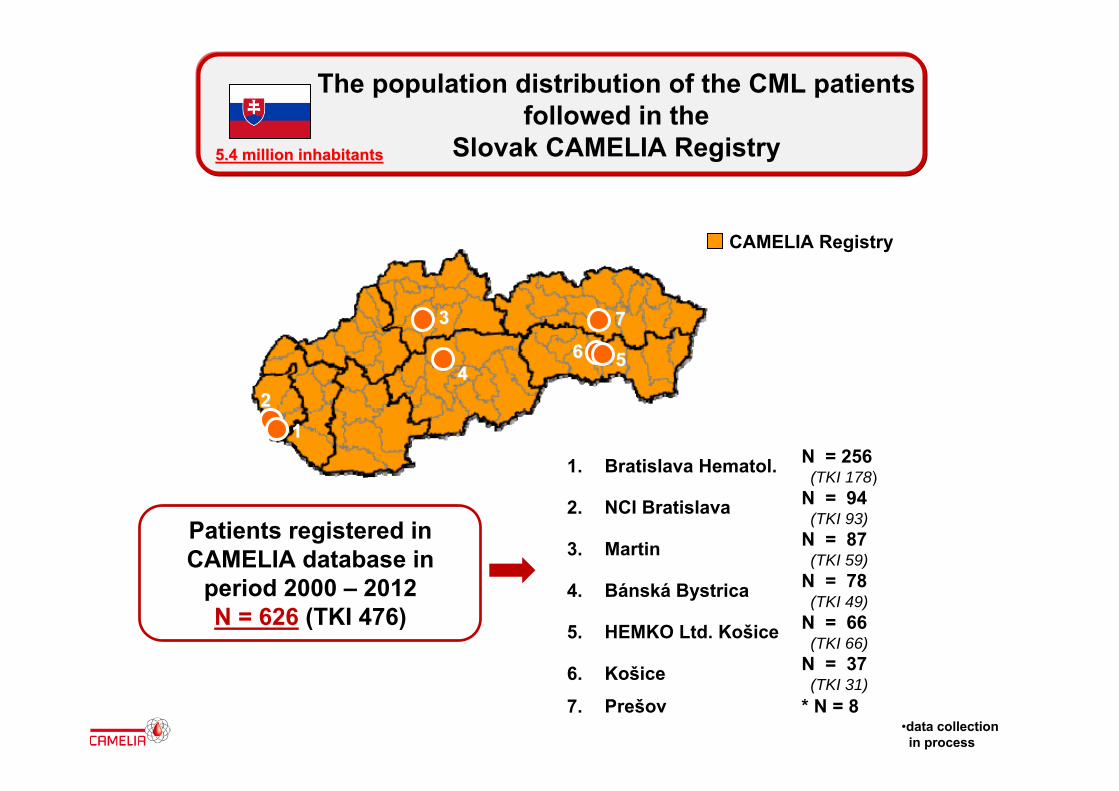
Patients registered in CAMELIA database in
period 2000 – 2012N = 626 (TKI 476)
5.4 million inhabitants5.4 million inhabitants
5544
11
33
CAMELIA Registry
The population distribution of the CML patients followed in the
Slovak CAMELIA Registry
1. Bratislava Hematol. N = 256(TKI 178)
2. NCI Bratislava N = 94(TKI 93)
3. Martin N = 87(TKI 59)
4. Bánská Bystrica N = 78(TKI 49)
5. HEMKO Ltd. Košice N = 66(TKI 66)
6. Košice N = 37(TKI 31)
7. Prešov * N = 8
22
•data collection in process
77
66
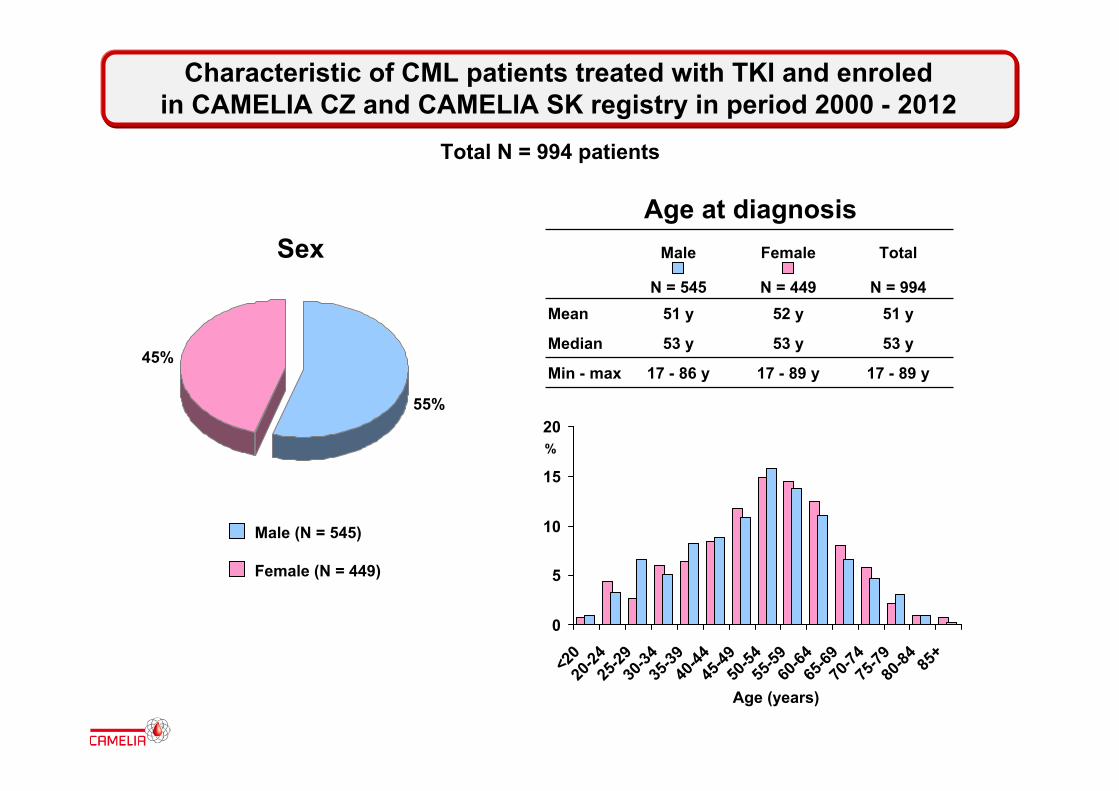
Male Female Total
N = 545 N = 449 N = 994Mean 51 y 52 y 51 y
Median 53 y 53 y 53 y
Min - max 17 - 86 y 17 - 89 y 17 - 89 y45%
55%
SexAge at diagnosis
0
5
10
15
20
<20
20-24
25-29
30-34
35-39
40-44
45-49
50-54
55-59
60-64
65-69
70-74
75-79
80-84 85
+
%
Age (years)
Male (N = 545)
Female (N = 449)
Characteristic of CML patients treated with TKI and enroled in CAMELIA CZ and CAMELIA SK registry in period 2000 - 2012
Total N = 994 patients
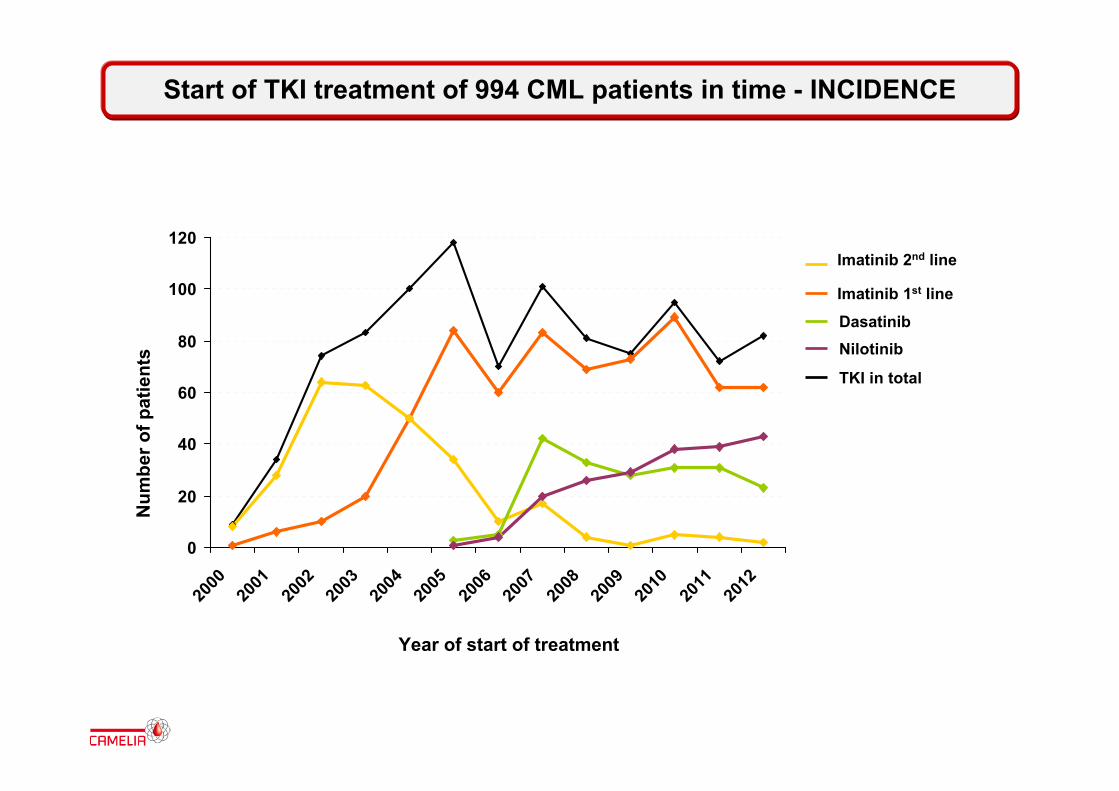
Start of TKI treatment of 994 CML patients in time - INCIDENCE
TKI in total
Imatinib 2nd line
Imatinib 1st line
DasatinibNilotinib
0
20
40
60
80
100
120
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
Num
ber o
f pat
ient
s
Year of start of treatment

TKI treatment of 994 CML patients in time - PREVALENCE
TKI in total
Imatinib 2nd line
Imatinib 1st line
DasatinibNilotinib
0
100
200
300
400
500
600
700
800
900
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
Num
ber o
f pat
ient
s
Year of treatment

0 12 24 36 48 60 72 84 96 108 120 1320.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0Pr
opor
tion
of p
atie
nts
on tr
eatm
ent
Time from start of TKI treatment (months)
Time on TKI treatment of 994 CML patients in period 2000 - 2012
TKI in total (N = 994)
TKI in 1st line (N = 710)
TKI in 2nd line (N = 284)
Log-rank test p = 0.019

0 12 24 36 48 60 72 84 96 108 120 1320.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0Pr
opor
tion
of s
urvi
ving
pat
ient
s
Time from start of TKI treatment (months)
OS of 994 CML patients on TKI treatment in period 2000 – 2012
TKI in total (N = 994)
TKI in 1st line (N = 710)
TKI in 2nd line (N = 284)
Log-rank test p < 0.001
0 12 24 36 48 60 72 84 96 108 120 1320.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 12 24 36 48 60 72 84 96 108 120 1320.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 12 24 36 48 60 72 84 96 108 120 1320.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
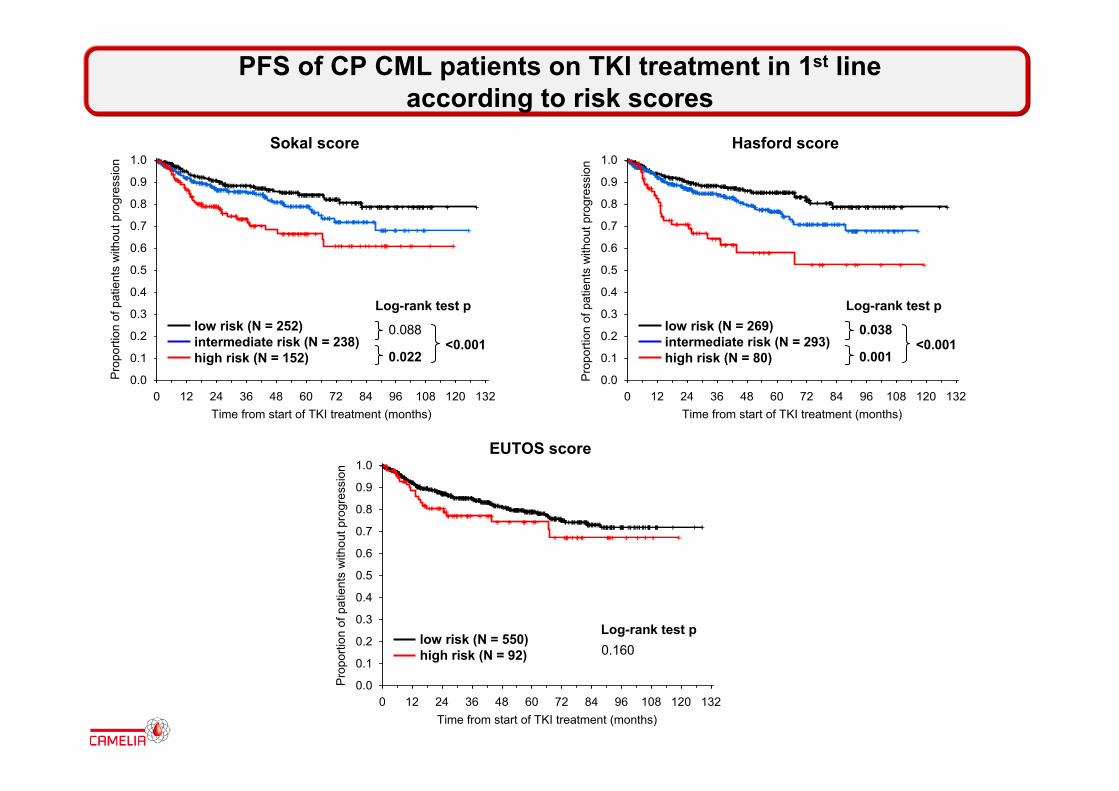
PFS of CP CML patients on TKI treatment in 1st line according to risk scores
low risk (N = 252)intermediate risk (N = 238)high risk (N = 152)
Sokal score
Time from start of TKI treatment (months)
Pro
porti
on o
f pat
ient
s w
ithou
t pro
gres
sion
0.088
0.022<0.001
Log-rank test plow risk (N = 269)intermediate risk (N = 293)high risk (N = 80)
Hasford score
Time from start of TKI treatment (months)
0.038
0.001<0.001
Log-rank test p
low risk (N = 550)high risk (N = 92)
EUTOS score
Time from start of TKI treatment (months)
0.160Log-rank test p
Pro
porti
on o
f pat
ient
s w
ithou
t pro
gres
sion
Pro
porti
on o
f pat
ient
s w
ithou
t pro
gres
sion

0 12 24 36 48 60 72 84 96 108 120 1320.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 12 24 36 48 60 72 84 96 108 120 1320.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 12 24 36 48 60 72 84 96 108 120 1320.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
low risk (N = 252)intermediate risk (N = 238)high risk (N = 152)
Sokal score
Time from start of TKI treatment (months)
Pro
porti
on o
f sur
vivi
ng p
atie
nts
0.070
0.2950.007
Log-rank test plow risk (N = 269)intermediate risk (N = 293)high risk (N = 80)
Hasford score
Time from start of TKI treatment (months)
Pro
porti
on o
f sur
vivi
ng p
atie
nts
0.001
0.090<0.001
Log-rank test p
low risk (N = 550)high risk (N = 92)
EUTOS score
Time from start of TKI treatment (months)
Pro
porti
on o
f sur
vivi
ng p
atie
nts
0.373Log-rank test p
OS of CP CML patients on TKI treatment in 1st line according to risk scores
1. FABER E., INDRÁK K. ET AL. Chronická myeloidní leukemie. Galén 2010
2. E. FABER, D. FRIEDECKÝ, K. MIČOVÁ ET AL. Imatinib dose escalation in two patients with chronic myeloid leukemia, with low trough imatinib plasma levels measured at various intervals from the beginning of therapy and with suboptimal treatment response, leads to the achievement of higher plas. IJH, 2010, 91(5): 897-902.
3. P. ROHOŇ, Š. ROŽMANOVÁ, J. ZAPLETALOVÁ ET AL. Výsledky liečby pacientov v chronickém fáze chronickej myelocytovej leukémie na HOK v Olomouci v rokoch 2000-2009: prognostický význam Sokalovho indexu a ELN kritérií. Transfuze a hematologie dnes, 2010, 16(4): 202-209.
4. P. ROHON, M. DIVOKA, L. CALABKOVA et al. Identification of e6a2 bcr-abl fusion in Philadephia –positive CML with marked basofilia: implication for treatment strategy. Biomed Pap 2011,155: 187-90.
5. E. FABER, J. MUŽÍK, V. KOZA ET AL. Treatment of consecutive patients with chronic myeloid leukemia in the cooperating centres form the Czech Republic and the whole of Slovakia after 2000 – a report from the population-based CAMELIA Registry. EJH 2011, 87(2):157-168.
6. VOGLOVÁ J, MUŽÍK J, FABER E, ET AL. Incidence of second malignancies during treatment of chronic myeloid leukemia with tyrosine kinase inhibitors in the Czech Republic and Slovakia. Neoplasma. 2011; 58 (3): 256-262.
CAMELIA publications 2010-2011
1. E. Faber, D. Friedecky, K. Micova, et al.: Imatinib trough plasma levels do not correlate with the response to therapy in patients with chronic myeloid leukemia in routine clinical setting.An Hematol. 01/2012; DOI:10.1007/s00277-011-1394-
2. E. Faber, A. Kuba, J. Zapletalova, et al. on Behalf of Cooperating Group: Operational Cures After Interferon-Alpha in Patients with Chronic Myeloid Leukemia in Central and Northern Moravia. JOURNAL OF INTERFERON & CYTOKINE RESEARCH, 32, 5, 2012 Ş Mary Ann Liebert,
3. Š. Rožmanová, P. Rohoň, M. Divoká, et al.: Hodnocení časné molekulární odpovědi po 3 měsících léčby imatinibem může u nemocných s chronickou myeloidní leukemií přispět k upřesnění odhadu prognózy – zkušenosti jednoho centra. Transf. Hematol. dnes 18, 2012, 66-71
4. E. Faber, D. Friedecky, K. Micova, et al.: Imatinib dose escalation in two patients with chronic myeloid leukemia, with low trough imatinib plasma levels measured at various intervals from the beginning of therapy and with suboptimal treatment response, leads to the achievement of higher plasma levels and major molecular response. IJH 04/2012; 91(5):897-902.
5. E. Faber, A. Kuba, J. Zapletalova, et al.: Interferon-alpha in chronic myeloid leukemia revisited: A long-term retrospective study in Central and Northern Moravia. Biomed Pap 2012;
CAMELIA publications 2012-2013
1. H. Klamova, E. Faber, D. Zackova et al.: Dasatinib in imatinib-resistant or intolerant CML patients: data from the clinical practise of 6 hematological centers in the Czech Republic. Neoplasma 57 (4) 355 – 359, 2010
2. A. Kreutzman, P. Rohon, E. Faber, K. Indrak et al.: Chronic myeloid leukemia patients in prolonged remission following interferon-α monotherapy have distinct cytokine and oligoclonal lymphocyte profile. PLoS ONE 01/2011; 6(8):e23022. DOI:10.1371/journal.pone.0023022
3. H. Klamová1, K. Machová Poláková1, J. Mužík2, et al.: Evaluation of 5-year imatinib treatment of 458 patients with CP-CML in routine clinical practice and prognostic impact of different BCR-ABL cutoff levels. Cancer Medicine 2, 2, 216-225, 4, 2013
4. T. Pavlik, E. Janousova, J. Mayer, K. Indrak, et al: Current survival measures reliably reflect modern sequential treatment in CML: correlation with prognostic stratifications. AJH. 2013 doi: 10.1002/ajh.23508, 6/2013
CAMELIA joint publications 2010 - 2013
1. EUTOS for CML out-study patients – accepted 240 patients
2. EUTOS for CML population-based registry – reported in total 312 patients from region of 11 mil population diagnosed in between 7/2009 - 12/2012, it means incidence of 0.81/100,000 per year
3. EURO-SKI – individual participation of the Czech republic CAMELIA centre (Olomouc, Hradec Kralove and Pilzen) through Infinity Registry
4. Pregnancy study – interest in participation of CAMELIA SR (Responsible Z. Sninska, MD, PhD.) and CR (Responsible K. Steinerova, MD, PhD.)
The proposed CAMELIA projects:
5. The prognostic significance of anemia for CML (Prof. E. Faber, MD, PhD.)
6. The validation of prognostic risk score in CML patients in real clinical practice (Z. Sninska, MD, PhD.)
7. The impact of cytogenetic abnormalities on treatment results of CML patients (Prof. M. Jarosova, MA, PhD., T. Pavlik, MA, PhD.)
8. The analyses of nilotinib treatment in clinical practice (Prof. E. Tóthová, MD, PhD.)
CAMELIA participation on ELN WP4 clinical projects and the proposed projects

Camelia group participants
Brno 4/2009
Thank you for your attention!
Olomouc 4.5.2011