cam for cancer in american samoa: formative research for a radio serial drama, sara krosch
DESCRIPTION
Complementary and Alternative Medicine for Cancer in American Samoa: Formative Research for the Development of a Radio Serial Drama, Sara Krosch, February, 2009TRANSCRIPT

THE AMERICAN SAMOA COMMUNITY CANCER COALITION
Complementary & Alternative Medicine for Cancer in American Samoa Pacific‐CEED Legacy Project
Formative Research for the Development of the Radio Serial Drama “Tasi le Ola”
Funded by REACH US Centers for Disease Control through the
Department of Family Medicine & Community Health, JABSOM, University of Hawaii
Sara Krosch & Vaioge Tuito’elau
4/1/2009
_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of isparities Legacy Project CDC US8DP000976‐02
D
| 2
Table of Contents List of Figures and Tables .................................................................................................................................................................. 3
Introduction ...................................................................................................................................................................................... 5
Part I‐ Literature Review ................................................................................................................................................................... 6
Cancer Care amongst Samoan Women ............................................................................................................................. 6
Complementary and Alternative Medicine ....................................................................................................................... 7
Traditional Healers .......................................................................................................................................................... 10
Samoan Culture and Cancer ............................................................................................................................................ 11
Radio Serial Dramas ........................................................................................................................................................ 13
Part II‐ Women’s Survey Results ..................................................................................................................................................... 15
Survey Methods .............................................................................................................................................................. 15
Respondent Demographics ............................................................................................................................................. 15
Survey Results: Analysis by Age and Education Groups .................................................................................................. 16
Evidence‐based Recommendations ................................................................................................................................ 25
Part III‐ Western Health Care Professionals Survey Results ............................................................................................................ 26
Survey Methods .............................................................................................................................................................. 26
Respondent Demographics ............................................................................................................................................. 26
Survey Results: Analysis by Gender, Age, Race/Ethnicity & Years in Health Care Profession ......................................... 28
Evidence‐based Recommendations ................................................................................................................................ 44
Part IV‐ Key Informant Interviews ................................................................................................................................................... 45
Evidence‐based Recommendations ................................................................................................................................ 46
Women’s Survey Results Summary ................................................................................................................................................ 49
Women’s Survey Form .................................................................................................................................................................... 51
Western Health Care Professional’s Survey Results Summary ....................................................................................................... 53
Western Health Care Professional’s Survey Form .......................................................................................................................... 56
Works Cited .................................................................................................................................................................................... 58

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 3
List of Figures and Tables
Figure 1: Women’s Survey Respondents’ Age Groups Page 15 Figure 2: Women’s Survey Respondents’ Educational Attainment 16 Figure 3: Age Groups‐ Smoking Status 17 Figure 4: Education Groups‐ Smoking Status 17
Figure 7: Age Groups‐ Mammogram Status 18
Figure 5: Age Groups‐ Any Cancer Screening Status 17Figure 6: Education Groups‐ Any Cancer Screening Status 18
Figure 8: Education Groups‐ Mammogram Status 19 Figure 9: Age Groups‐ Self‐Breast Exam Status 19 Figure 10: Education Groups‐ Self‐Breast Exam Status 20 Figure 11: Age Groups‐ Pap Test Status 20
Figure 14: Cancer Survivor Reported Treatments 22
Figure 12: Education Groups‐ Pap Test Status 21Figure 13: Survey Respondent Cancer Survivors 21
Figure 15: All Respondents‐ Proposed Advice to Family/Friend 22 Diagnosed with Breast or Cervical Cancer Figure 16: Age Groups‐ Proposed Advice to Family/Friend 23 Diagnosed with Breast or Cervical Cancer Figure 17: Education Groups‐ Proposed Advice to Family/Friend 23 Diagnosed with Breast or Cervical Cancer Figure 18: Age Groups‐ Personal Use of Traditional Samoan Healers 24 Figure 19: Education Groups‐ Personal Use of Traditional Samoan Healers 24 Figure 20: Health Care Professional Survey Respondents by Gender 26 Figure 21: Health Care Professional Survey Respondents by Age Group 26 Figure 22: Health Care Professional Survey Respondents by Race/Ethnicity 27 Figure 23: Health Care Professional Survey Respondents by Years in Health 27 Care Profession Figure 24: Health Care Professional Survey Respondents Current Position(s) 27 Figure 25: Number of Female Patients Age 40+ Seen Weekly 28 Figure 26: All Respondents (n=147)‐ Personal CAM Use & Recommendations 29 to Patients Figure 27: Females (n=17)‐ Personal CAM Use & Recommendations to 29 Patients Figure 28: Males (n=30)‐ Personal CAM Use & Recommendations to Patients 30 Figure 29: <40 Years Old (n=16)‐ Personal CAM Use & Recommendations to 30 Patients Figure 30: ≥40 Years Old (n=31)‐ Personal CAM Use & Recommendations to 31 Patients Figure 31: Samoans (n=22)‐ Personal CAM Use & Recommendations to 31 Patients Figure 32: Asians (n=10)‐ Personal CAM Use & Recommendations to 32 Patients Figure 33: Caucasians (n=12)‐ Personal CAM Use & Recommendations to 32 Patients Figure 34: ≤11 Years in Health Care Profession (n=23)‐ Personal CAM Use 33 & Recommendations to Patients Figure 35: >11 Years in Health Care Profession (n=23)‐ Personal CAM Use 33 & Recommendations to Patients Figure 36: All Respondents & Genders‐ Patient Consultations concerning 34 Samoan Healing Utilization Figure 37: Age Groups‐ Patient Consultations concerning Samoan Healing 34 Utilization Figure 38: Race/Ethnic Groups‐ Patient Consultations concerning Samoan 35 Healing Utilization Figure 39: Years in Health Care Profession‐ Patient Consultations concerning 35 Samoan Healing Utilization

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 4
Figure 40: All Respondents & Genders‐ Overall Impression of Samoan Page 36 Healing as CAM Figure 41: Age Groups‐ Overall Impression of Samoan Healing as CAM 36 Figure 42: Race/Ethnic Groups‐ Overall Impression of Samoan Healing as 37 CAM Figure 43: Years in Health Care Profession‐ Overall Impression of Samoan 37 Healing as CAM Figure 44: All Respondents & Genders‐ Awareness of Local Breast/Cervical 38 Cancer Patients Utilizing Samoan Healing as CAM Figure 45: Age Groups‐ Awareness of Local Breast/Cervical Cancer Patients 38 Utilizing Samoan Healing as CAM Figure 46: Race/Ethnic Groups‐ Awareness of Local Breast/Cervical Cancer 39 Patients Utilizing Samoan Healing as CAM Figure 47: Years in Health Care Profession‐ Awareness of Local Breast/ 39 Cervical Cancer Patients Utilizing Samoan Healing as CAM Figure 48: All Respondents & Genders‐ Perceptions of Samoan Healing 40 Impact on Health Figure 49: Age Groups‐ Perceptions of Samoan Healing Impact on Health 40 Figure 50: Race/Ethnic Groups‐ Perceptions of Samoan Healing Impact on 41 Health Figure 51: Years in Health Care Profession‐ Perceptions of Samoan Healing 41 Impact on Health Figure 52: All Respondents & Genders‐ Interest in Learning More about 42 Samoan Healing Methods Figure 53: Age Groups‐ Interest in Learning More about Samoan Healing 42 Methods Figure 54: Race/Ethnic Groups‐ Interest in Learning More about Samoan 42 Healing Methods Figure 55: Years in Health Care Profession‐ Interest in Learning More about 42 Samoan Healing Methods
Table 1: Cancer Incidence for Women Residing in Hawaii 1998‐2002 per 6 100,000 Table 2: Breast and Cervical Cancer Screening Variables for Samoan Women 7 Table 3: Predictors of CAM Use in United States Populations 9 Table 4: Reasons for Traditional Healer Utilization 24 Table 5: Types of Specialists and Other Professionals Surveyed 28 Table 6: Women’s Survey Results Summary 80 Table 7: Western Health Care Professional’s urvey Results Summary 84 S

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 5
Introduction
In January 2009, the American Samoa Community Cancer Coalition received Pacific‐CEED Legacy funding to explore the types of complementary and alternative medicines (CAM) used for cancer care in general and specifically amongst women age 40 and older at risk for breast or cervical cancer in the Territory. The project’s formative research methods consisted of surveys and interviews. Sara Krosch, Health Communication Consultant and Project Coordinator, developed the instruments. Face validity checks were done with partners at the American Samoa Community Cancer Network and Comprehensive Cancer Control of American Samoa. The women’s survey and interview questions for cancer survivors and traditional Samoan healers were translated by Vaioge Tuitoelau, Project Assistant, with input from the American Samoa Community College Institute for Samoan Studies. All instruments received Institutional Review Board approval on island.
Self‐administered surveys were completed by 179 women age 40 and older, the main target population for breast and cervical cancer screening. Research has shown that access to health professional is a strong predictor for breast and cervical cancer screening (Abraido‐Lanza, et al., 2004; Mandelblatt, et al., 1999) so 47 health care providers employed at the LBJ Tropical Medical Center (LBJ) and the American Samoa Department of Health’s Breast and Cervical Cancer Early Detection Program (BCCEDP) were surveyed. Interviews were done with 2 LBJ doctors, 2 BCCEDP staff, 4 cancer survivors (breast, cervical), and 2 family members of deceased cancer patients, and 3 traditional Samoan healers (Taulasea/Fofo) who have treated women with breast cancer. The purpose of the formative research was to arrive at a better understanding of the types of healing methods available to and accessed by women age 40 and older in American Samoa; the mainstream medical community’s perceptions of traditional Samoan healing and other CAM; and traditional Samoan healers perceptions of cancer and the care they can provide to cancer patients. The results of this research will inform the development of a 5‐part radio serial drama that will be aired in American Samoa in May‐June, 2009.
This document reports the results of a preliminary literature review, surveys and interviews. Recommendations are given to guide the scripting of a 5‐part radio serial drama in order to depict realistic characters and scenarios, and model quality of life‐centered recommendations within American Samoa’s current healthcare context.
The authors would like to thank all those who completed surveys, offered interviews and provided logistical and funding support to fulfill this formative research.
For more information on this project please contact:
Sara Krosch Vaioge Tuito’elau Health Communication Consultant ASCCN Pacific‐CEED Legacy Project Assistant ASCCN Pacific‐CEED Legacy Project Coordinator Email‐ [email protected]

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 6
Part I‐ Literature Review
A review of relevant literature was conducted by Sara Krosch December 2008‐January 2009 focusing on the following key terms: cancer (breast, cervical), women, complementary and alternative medicine/therapies, American Samoa, Samoans, traditional healers, and radio serial drama. The purpose of the literature review was to generally ground the local research in the larger field of CAM for cancer and to specifically inform the development of valid instruments to gather local data.
Cancer amongst Samoan Women
A study of Asian and Pacific Islanders diagnosed with cervical cancer in Hawaii revealed that 74% of Pacific Island women were diagnosed at an advanced stage and had significantly lower 5‐year survival rates compared to non‐Pacific Islanders, 32% versus 71% (Robinson, et al., 2002).
Statistical analysis conducted by Miller et al. (2007) showed that amid Asian Pacific Islander groups living in Hawaii overall cancer incidence and death rates were highest for Samoan women. Breast cancer is the leading site followed by cancers of the uterus and cervix with the disease often being diagnosed at advanced stages in younger women (APIAHF, 2006; Ishida, et al., 2001; Miller, et al., 2007). Samoan women’s cancer burden far outweighs that of other US Territorial women and cervical cancer rates exceed those of non‐Latina white women. 1
Table 1: Cancer Incidence for Women Residing in Hawaii 1998‐2002 per 100,000 (Source: Miller, et al., 2007)
Samoan Guamanian Non‐Latina White
All cancers 472 176 449
Breast cancer 103 45 145
Cervical cancer 18 NA 8 Among American Samoans, cancer is the second leading cause of mortality (APIAHF, 2006). Breast cancer is the most common cancer among American Samoan women—27% of the cases (Hubbell, et al., 2005). Cancer Screening
In the United States as a whole, Pacific islanders have the highest proportion of women not utilizing regular Pap smear services (Robinson, et al., 2002). Amongst Samoan women living in the United States, only 56% age 30 years or older have ever had a clinical breast exam and 33% age 40 and older have ever had a mammogram. Sixty‐four percent (64%) have ever had a pap smear, and less than half (46%) in the last 3 years (APIAHF, 2006; Hubbell, et al., 2005).
Researchers have found barriers outweigh facilitators of cancer screening for Samoan women. Despite regular education campaigns knowledge about cancer and screening services has not proven to be a strong indicator of uptake. The US National Cancer Institute recognizes both traditional healing 1 There are few local breast and cervical cancer statistics available in American Samoa so program planning is often reliant upon what is known about Samoans residing in Hawaii. This formative research aims to remedy this fact.

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 7
methods and prayer as complementary and alternative healing methods for cancer patients, however believing that cancer can be cured by Samoan Taulasea/Fofo or that a cancer diagnosis is God’s will leads some women to forego available western medical treatment. Fear works as both a motivator and a barrier to cancer screening.
Table 2: Breast and Cervical Cancer Screening Variables for Samoan Women (Sources: APIAHF, 2006; Hubbell, et al., 2005; Ishida, et al., 2001)
Barrier Variables Pain; Screening not prioritized; Fear; Concern over body being touched by self or
others; Belief that cancer can be cured by traditional healers; Belief that cancer is God’s will
Neutral Variables Knowledge about cancer; Knowledge about cancer screening services
Facilitator Variables Doctor Recommendation; Fear
Having a physician referral is the most common predictor of mammography use but minority women often face cultural, educational, and communication barriers in talking with their physicians about this screening which contributes to higher mortality rates compared to non‐Latina white women (Levy‐Storms and Wallace, 2003). The United States Department of Health and Human Services Preventative Services Task Force (USPSTF) recommends women age 40 and older have a mammogram with or without clinical breast exam every 1‐2 years while evidence is lacking to recommend for or against performing monthly self‐breast exams. The USPSTF recommends screening females age 18‐65 every 1 to 3 years for cervical cancer and older females if there is a history of abnormal pap test results (USDHHS‐USPSTF, 2007). Based on 2000 census population numbers, approximately 7,386 women would have been eligible for free breast and cervical cancer screening services in the Territory in 2003. Such services include pap tests, clinical breast exams, mammograms and biopsies paid for by the National Breast and Cervical Cancer Early Detection Program (BCCEDP) housed under the American Samoa Department of Health. The Territory’s BCCEDP reports that 2,236 (717 mammograms; 1,837 pap tests) women were served in a five year time span, 2003‐2007—30% of those eligible. The BCCEDP receives nearly all referrals for women age 40 and older. However, it is unknown how many of these women were repeat clients so it is likely the total number of women served by this program is lower (CDC NBCCEDP, 2007).
Complementary and Alternative Medicine
Complementary or Alternative Medicine (CAM) for cancer is any practice or product that is not thought of as standard medical care (chemotherapy, radiation, surgery) based on scientific evidence. Complementary medicines are used along with standard medical treatments whereas alternative therapies are scientifically unproven remedies and techniques used in place of standard medical treatments (Cassileth and Chapman, 1996; NCI, 2005; Swisher et al., 2002). Alternative therapies often

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 8
conflict with mainstream treatments and are potentially harmful, whereas complementary therapies are often sought for symptom control and pain management resulting in a better quality of life (Cassileth, 1999; Jump, et al, 1998). An alternative therapy can become conventional when its effectiveness is proven and a conventional therapy can become alternative when used for unproven indications (Cassileth and Chapman, 1996).
Types of CAM
The term CAM includes a wide range of therapies (Swisher et al., 2002). Common CAM for cancer include diet and nutrition; mind‐body techniques (prayer); traditional/folk remedies; massage; and herbal medicines among many other therapies (Cassileth and Chapman, 1996; Moa, et al, 2007; Swisher et al., 2002). In a sample of cancer survivors in the United States, Moa and associates found prayer to be the most popular CAM (62%). It is unknown how many American Samoan cancer survivors have used prayer as a CAM, but recent surveys have shown that 91%‐96% of the population ages 13‐85 site some church affiliation (Krosch, 2008). Twenty percent (20%) of US cancer patients use herbal remedies, 6% use massage, and only 1% use traditional medicine. Eighteen percent (18%) use multiple therapies (Moa, et al., 2007).
In American Samoa, CAM can involve a combination of herbal remedies, massage and spiritual healing—Christian prayer or incantations to drive off an offending spirit or aitu. Traditional Samoan herbal remedies have been documented by several sources but the medicinal value of most catalogued plants has not been scientifically proven. And the combinations of plant materials are subject to the patient’s condition and the individual healer (Whistler, 1995). Massage therapy in general is a largely unstudied CAM. The main documented physiological benefits attributed to massage include increases in immune function and pain reduction. Numerous psychological benefits have also been reported from massage including stress reduction, improved quality of life, and improved sleep patterns. The combination of these physical and psychological effects makes massage a promising therapy for cancer and other health conditions (Patterson, et al., 2008); however, traditional Samoan massage has not been studied as a CAM for cancer.
Reasons for CAM Use
Like mainstream therapies, CAM is used to increase physical, psychological, and emotional well‐being (Moa, et al., 2007; Swisher, et al., 2002). Patients often seek complementary or alternative therapies to manage symptoms and/or to find a healing method that is more compatible with their values and beliefs about the nature of health and illness (Astin, 1998; Cassileth and Chapman, 1996; Moa, et al, 2007). Cassileth and Chapman (1996) feel that CAM use has become widespread amongst cancer survivors due to fear and lack of understanding of the causes of the disease and adverse side‐effects of medical treatments like chemotherapy. Women often use CAM in hopes of preventing cancer recurrence with the most common perceived benefit of CAM use being increased hope or optimism (Moa, et al., 2007; Swisher et al., 2002).
Researchers have also found that CAM use is often rooted in distrust or dissatisfaction with mainstream, Western medical care and institutions (Cassileth and Chapman, 1996; Mao et al, 2007). Patients who

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 9
were dissatisfied with the cost of treatment, waiting time, and doctor‐patient interactions are more likely to use CAM (Lee, et al., 2004). According to a 2007 American Samoa Office of the Governor Situational Analysis2, a large percentage of American Samoans are dissatisfied with current Western health care services offered at the LBJ Tropical Medical Center: long wait times, no medication or treatment available, crowding, expensive fees, distance to health care facilities and poor of quality care. These grievances coupled with 61% of the population living below the US Federal Poverty Level (2000 census) (ASOG, 2007), facilitate CAM use via traditional Samoan healers.
When CAM is Used CAM use is most common after cancer diagnosis and decreases to as little as 25% two years after diagnosis (Lee, et al., 2004; Porter, et al., 2008). Swisher et al. (2002) found that increased CAM use amongst breast cancer patients correlated with increased psychosocial distress and decreased quality of life. The most common reasons for CAM discontinuation were feelings of ineffectiveness or harmfulness, and too much personal effort compared to other therapies (Porter, et al., 2008). Who Uses CAM Research conducted by Moa and colleagues (2007) estimates 83% of all cancer survivors in the US use CAM. Both recently and distantly (>10 years) diagnosed cancer survivors were more likely than the general US population to use CAM. Studies in the United States have uncovered several predictors of CAM use.
Table 3: Predictors of CAM Use in United States Populations
Predictors Sources
Women Moa et al., 2007; Pu, et al., 2008; Swisher et al., 2002
Breast or gynecological cancer site Moa et al., 2007; Pu, et al., 2008; Swisher et al., 2002
Younger (<50 years old) Lee, et al., 2004; Moa, et al., 2007; Pu, et al., 2008
Some college education Astin et al., 1998; Moa, et al., 2007
Traditional health beliefs Astin, 1998; Lee, et al., 2004
Poor health condition (chronic pain) Astin, 1998; Lee, et al., 2004
Perceived poor health status Lee, et al., 2004
From less‐developed, non‐Western country Pu, et al., 2008
Annual income higher than $30,000USD Swisher et al., 2002
Use of CAM prior to cancer diagnosis Swisher et al., 2002
Family use of CAM Lee, et al., 2004
Recommendation by close social contacts Lee, et al., 2004
Research conducted with Samoans in the United States and in American Samoa revealed that older age (>50 years); residing in American Samoa; belief that some illnesses only afflict Samoans (ma’i Samoa);
2 This report was commissioned as part of a study to determine the feasibility of offering universal health insurance to American Samoans. The territory’s population was deemed to be “uninsurable” largely due to a heavy burden of life style diseases such as diabetes and heart disease and large percent of smokers.

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 10
and past use of traditional Samoan healers were the greatest predictors of CAM use for any health ailment (Mishra, et al., 2003).
Doctors and CAM
Most patients use complementary therapies in conjunction with standard medical therapy, while a minority chooses alternative therapies to the exclusion of standard medical treatments (Swisher et al., 2002). Jump and colleagues (1998) found that physicians practicing for less than 10 years were more likely to regard most CAM therapies as legitimate. More than half of physicians surveyed ranked prayer, relaxation techniques, exercise, and self‐help groups as legitimate CAM, followed closely by massage, and diet modification. Less than one quarter of physicians felt that traditional/folk remedies and herbal medicine were legitimate complementary therapies. Nearly two‐thirds of the physicians (65%) surveyed had prescribed or referred for at least one complementary therapy with the most common conditions for CAM referral being pain management, anxiety/stress, depression, and insomnia. Other studies have found fewer than 25% of CAM users have received information about CAM from a physician or nurse (APIAHF, 2006; Swisher et al., 2002). More than one‐third of physicians (35%) had personally utilized at least one CAM and this experience resulted in a higher level of acceptance of CAM as legitimate medical therapy. The most common CAM prescribed are massage and exercise (14%, 11%), followed by prayer, diet, and self‐help groups (7% each), while only 4% of doctors had prescribed herbal remedies and 1% folk/traditional therapies. Despite doctors’ relatively positive attitudes toward some CAM therapies, most oncologists are not familiar with the CAM therapies their patients use (Cassileth and Chapman, 1996; Jump, et al., 1998). Unsupervised use of some therapies is potentially harmful and can be dangerous in combination with chemotherapy (Jump, et al., 1998; Swisher et al., 2002).
Traditional Healers Traditional healers are an integral part of culture and society worldwide. In Southern Africa they are the main provider of health care in most of rural areas. African traditional healers provide psychosocial support as well as herbal remedies in a familiar, village‐based setting. They are utilized by as many as 80% of HIV positive individuals in Southern Africa due to their accessibility, affordability and cultural familiarity. They have also proved to be a way to improve quality of life in resource‐poor areas when they partner with Western medicine health professionals. South Africans utilizing traditional healers are more likely to be unemployed and less likely to have an education beyond primary level. They are also more likely to report better self‐perceived quality of life3 one month after visiting a traditional healer) (Taylor, et al., 2008). Traditional Samoan Healers
3 Quality of life is defined as general health perceptions of physical and social function, pain, mental health and health distress (Taylor, et al., 2008).

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 11
In American Samoa, cancer treatment services are very limited. Most patients that can afford treatment are referred off‐island to Hawaii for services such as chemotherapy or radiation. Those who cannot afford to be sent off‐island remain in American Samoa. In both cases, patients may visit a traditional Samoan healer, a Fofo or Taulasea, for CAM.
Fofo is a generic term literally meaning “to doctor.” Fofo can be commonly divided into two groups, those who practice traditional Samoan massage (commonly referred to as fofo) and those who have some training (traditional apprenticeship) in diagnosis and treatment of illness of supernatural or natural origins (Taulasea). Traditional healers can be distinguished by levels of expertise and type of illness primarily treated. Fofo are more specialized and illness specific, often treating women and children (MacPhearson and MacPhearson, 19904). Taulasea sometimes treat certain or all illnesses. If a Fofo’s methods are unsuccessful, a person may be referred to a single or group of Taulasea (MacPhearson and MacPhearson, 1990). Samoan Taulasea are nearly all women who gained their knowledge and skills from their mothers or grandmothers. Because Samoans value their beliefs in CAM from Fofo or Taulasea, these traditional practices are used as both complementary and alternative therapies for many illnesses affecting women including cancer (Samoan Observer, July 20, 2003). An American Samoan cancer patient who can afford maintenance chemotherapy may also seek a Fofo for traditional massage therapy for pain management. A patient who cannot afford mainstream treatment may utilize a Taulasea using native plants to treat illnesses. There is a need to better understand Samoan traditional medicine and health‐seeking behaviors related to cancer and to explore whether indigenous Samoan healers can assist in the delivery of clinically proven and culturally sensitive disease management (Mishra, et al., 2003).
Tonga is a close Polynesian neighbor to Samoa sharing many cultural traits including wide‐spread use of traditional healers for illness and disease. Qualitative research conducted McMullin and colleagues (2008) found that Tongan culture is more focused on treating symptoms of illness than on prevention strategies for staying healthy. Tongans also feel that any health care is sought only when one cannot maintain and fulfill obligations and relationships with family, church and community. Antidotal evidence has shown that American Samoans sometimes seek out Tongan traditional healers on Tutuila Island when they have been recommended by family and friends.
Samoan Culture and Cancer
The Samoan way of life (fa’aSamoa) consists of a chief system responsible for the organization and leadership of family and villages, family‐based activities (including diet), churches and religious beliefs. Emphasis is placed on living one’s life to the benefit of the greater family. Fa’aSamoa is largely dictated by males, traditional leaders (matais) and church ministers age 50 and older. A qualitative study with this population, none of whom were cancer survivors, reported that disease prevention is not part of the fa’aSamoa. They stated that “fa’aSamoa is based on fear and respect” and it negatively influences the population by reinforcing and perpetuating shame/ embarrassment and a reluctance to discuss personal (bodily) issues. Samoans remain silent due to ignorance of the disease and out of “respect for
4 Confirmed in a personal interview with Noelle Potoa’e, January 19, 2009.
_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 12
the doctor.” They “refuse treatment out of pride” and seek it “only when they are near their death bed (Puaina, et al., 2008)”. And, preventative care is difficult to get because health providers are not oriented towards prevention in American Samoa (Hubbell, et al., 2005). Cancer Beliefs and Taulasea/Fofo Utilization
Studies have shown that American Samoans believe failure to follow the fa’aSamoa could lead to cancer and that a return to the fa’aSamoa could prevent cancer (Hubbell, et al., 2005; Puaina, et al., 2008). This complements the beliefs that cancer is not “part of Samoan culture” (there is no Samoan word for cancer) and that it is a relatively new disease brought by Westerners or brought on by adopting Western practices including diet (APIAHF, 2006; Hubbell, et al., 2005; Puaina, et al., 2008). Samoans reportedly believe that eating unhealthy foods (high‐fat, imported, canned, refrigerated), smoking cigarettes, drinking too much alcohol, breathing polluted air, and general neglect of one’s body can lead to cancer. Interestingly, smoking traditional Samoan cigarettes or drinking kava is not associated with cancer risk (Hubbell, et al., 2005). Cancer may also be God’s will. Some Samoan ministers explain cancer as an “act of God” explaining “people made it God’s will by participating in unhealthy or unwise behaviors” and God’s will should be accepted to avoid worry and anger. Few believe that spirits (aitu)—historically the cause of most Samoan illnesses—cause cancer (Hubbell, et al., 2005). Aitaoto et al (2007) report that Samoans differentiate between palagi (white person) illnesses—those that can be explained by trained health professionals and cured by Western medicine—and ma’i Samoa, illnesses that cannot be explained or treated with Western medicine and require the attention of traditional Samoan healers. According to Hubbell and associates (2005) Samoans use traditional remedies and traditional healers for all but the most serious illnesses. They offer the following quotation:
‘‘Let me explain a little bit. When you go to your plantation, you cut your finger, you don’t go to a doctor because right there is what we call fuafuasaina (an herbal cure) and then you put it on and then it heals it. There is no further need for any kind of medicine. If you get something else—what else for example, oloa (a slow‐healing ulcer), you go to a woman who can massage it, and it becomes normal. There is no need to go to a doctor. In my family, that is how we have been raised up.’’ ‐American Samoan woman
As high as 57% of American Samoan women report having visited a Fofo or Taulasea for health problems (35% only visited a Fofo), and 24% believe that traditional healers could cure cancer (Mishra, et al, 1997). “Samoans seek care from traditional Samoan healers prior to visiting Western medical providers (Mishra, et al, 1997).” These beliefs may account for Samoan women being more likely than other high risk populations (Native Hawaiians or non‐white Latinas) to receive a cancer diagnosis after metastasis has occurred (Mishra, et al, 2001). Most Samoan women age 40 an older with no personal history of cancer, despite having positive to neutral experiences with Western health care, reported they would use traditional Samoan medicine as a CAM if it was available (Ishida, et al., 2001).

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 13
Acculturation also has an impact on cancer beliefs (Aitaoto, et al., 2007). Samoans residing in American Samoa were more likely than those residing in Hawaii or Los Angeles to say that cancer is caused by aitu (spirits) and Atua (God) and could be cured by traditional healers. Men were four times more likely to believe that cancer could be cured by traditional healers than women (58% and 11% respectively) and five times more likely to feel that it is better to go to a traditional Samoan healer than to a Western medical doctor if diagnosed with cancer (52%, 9%). This suggests that women already classify cancer as a palagi illness in need of Western medical care. However, Mishra, et al (2007) found that women with high culture‐specific beliefs—those who said they would seek treatment from a traditional healer if diagnosed with breast cancer—were less likely to have a mammogram even when they were aware of the test.
Radio Serial Dramas
Edu‐tainment—inserting educational messages into traditional entertainment channels—has been a popular international health communication strategy since the 1950s. Edu‐tainment strategies have been integrated into radio and television serials around the world on health issues such as domestic violence, HIV/AIDS prevention, and family planning (Hether, et al., 2008; Lovell, 2007‐8). And edu‐tainment radio serial dramas have been widely used throughout Sub‐Saharan Africa for health promotion (Pappas‐DeLuca KA, et al., 2008).
The only radio serial dramas known to be produced recently in the US‐Associated Pacific Islands were spearheaded by a US‐based conservation NGO called RARE. Characters and plotlines were generated after community stakeholder focus group discussions. Villagers generated lists of the main issues of importance which ranged from alcoholism, family planning and domestic violence to mangrove forest and coral reef preservation and sea turtle poaching. Between 2002 and 2004 the radio drama Changing Tides aired 160, 15 minute episodes heard by over 200,000 people in the Northern Marianas, Federated States of Micronesia, Marshall Islands and Palau. Listenership ranged from 53%‐84% with 83%‐91% of surveyed listeners claiming to have learned more about health issues from the program. A key aspect of the serial was characters modeling desired behaviors within familiar settings and circumstances to encourage community discussion and reduce stigmatization of once taboo subjects (Skirble, 2004).
Exposure
Uptake of a desired health behavior is more likely when radio serial drama listeners are exposed to a message consistently over time and via various channels (Pappas‐DeLuca KA, et al., 2008; Wray, at al, 2004). Studies evaluating long running (5+ years) dramas promoting HIV prevention showed that the more people were exposed to the program the lower their level of stigmatizing attitudes and stronger their intentions to have HIV testing and talk to their partners about testing (Pappas‐DeLuca KA, et al., 2008). An Australian study found a multi‐channel campaign (radio, television, print, and events) increased pap smears amongst both high and lower risk women, in rural and urban settings, with the greatest uptake occurring when doctors also communicated messages (Byles, et al., 1994). A study in South Africa comparing the effectiveness of a photo‐comic and a radio‐drama on increasing cervical screening uptake found that the print campaign resulted in only a 1% increase in screening whereas

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 14
exposure to the radio drama accounted for a 17% increase six months after the campaign launched (Risi, et al, 2004). Family planning and immunization programs in Bangladesh found that multi‐channel health promotion media campaigns are more effective compared to single channel approaches where uptake of services was the goal. Media activities alone showed to be more cost effective compared to events—$0.05 ‐ $0.36 versus $8.00 ‐ $32.00 per new user per behavior change (Hutchinson, et al, 2006).
Characters
Radio serial dramas typically have characters designed to be "negative," "positive," and "transitional" (moving from negative to positive behaviors) role models. The goal of the plot is to encourage audience members to think about and discuss the implications of specific behaviors by contrasting the different character types. Using more than one transitional character for each target behavior generally improves audience identification and reinforces personal behavior change (Lovell, 2007‐8; Sebert Kuhlmann, 2008). In Botswana, female listeners who could name a transitional character in a serial drama as their favorite character were nearly twice as likely to test for HIV during pregnancy—the target behavior—as those who did not (Sebert Kuhlmann, 2008).
Impact
Radio soap operas have also been found to promote progress through the Stages of Change Model, increasing self‐efficacy, and Diffusion of Innovations by stimulating involvement with characters and interpersonal communication to motivate modeling their actions (Rogers, et al. 1999; Vaughan and Rogers, 2000). Mohammed (2001) found that female listeners of an edu‐tainment radio soap opera in Tanzania most often discussed the serial’s themes of family planning and HIV prevention with their personal communication networks—those with similar tribal membership, religious affiliation and gender, and those who are equally or more highly educated than themselves—than non‐listeners.
Radio for Cancer Education in American Samoa
Research conducted by the American Samoa Community Cancer Network found that women ages 40‐60 report receiving the most messages about cancer from radio in the past, and they request future messages specifically about cancer survivors via the radio. The most popular radio station for women in this age group is KSBS (Krosch, 2009).

Part II‐ Women’s Survey Results
Survey Methods | 15 In February 2009, 179 women age 40 or older residing in American Samoa completed a 10 item survey (see page 82). Convenience sampling was done at locations where many Samoan women could be found. The majority of respondents (n=98) were surveyed at a BINGO hall in the centrally located, large village of Tafuna. These women were given a free pencil and a BINGO dabber for completing the survey. Thirty (n=30) women attending a church in Nuu’uli received a free pencil and a kitchen towel for completing the survey. 5 The remaining respondents (n=51) were sampled at the LBJ OB‐Gyn clinic and at local restaurants and received a free pencil or pen. An advertisement for free breast and cervical cancer screening clinics was attached to the BINGO dabbers and the kitchen towels (see photo below). A summery table of this survey’s results can be found on page 80.
Respondent Demographics
The survey was completed by 179 women age 40 and older currently residing in American Samoa (Figure 1). The majority of survey respondents were ages 40‐49. Only 8 women surveyed were 70 years or older so it is unknown if the results for this age group are representative. 6
5 Tafuna and Nuu’uli are the villages with the largest populations on Tutuila Island according to the 2000 census. 6 Little is known about the benefits of screening women age 70 and older for breast or cervical cancer. The US Department of Health and Human Services Preventative Services Task Force (2007) reports only 2 randomized control trials with women over age 69. Older women face a higher probability of developing and dying from breast cancer but also have a greater chance of dying from other causes. Women with co‐mormid conditions that limit life expectancy are unlikely to benefit from cancer screening. The USPSTF recommends against routinely screening women older than 65 for cervical cancer if they have a history of normal pap tests. _____________________________________________________________________________________________________________________
ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02

85, 47%
51, 29%
35, 20%
8, 4%
Figure 1: Women's Survey‐ Respondents' Age Groups
40‐49 50‐59 60‐69 70+
| 16
Most respondents had no more than a high school or 2 year college education. The highest educated women were in their 40’s (Figure 2).
0
20
40
60
80
100
120
140
160
180
All 40‐49 50‐59 60‐69 70+
3
63
64
29
146
Figure 2: Women's Survey‐ Respondents' Educational Attainment
no response
>4 yr college
4 yr college
2 yr college
secondary
elementary
# respon
dents
Survey Results: Analysis by Age Groups and Education Groups Women’s survey data was categorized by age group and education group. Age groups were defined in 10 year increments. Education groups were divided into three roughly equal categories: elementary or secondary diploma highest attainment (n=66); 2 year college degree attainment (n=64); and 4 year college degree attainment or beyond (n=43). Six (n=6) people (3%) did not provide their education level so these cases were excluded from analysis. Smoking increases breast cancer and cervical cancer risk (MayoClinic.com). Figure 3 shows over half of survey respondents have smoked sometime in their lives and a third are currently smokers. Most current smokers are age 50‐59. Women with an elementary or secondary education are the most likely to be current smokers while those with a 4 year college degree or more are the most likely to have quit smoking as shown in Figure 4. _____________________________________________________________________________________________________________________
ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
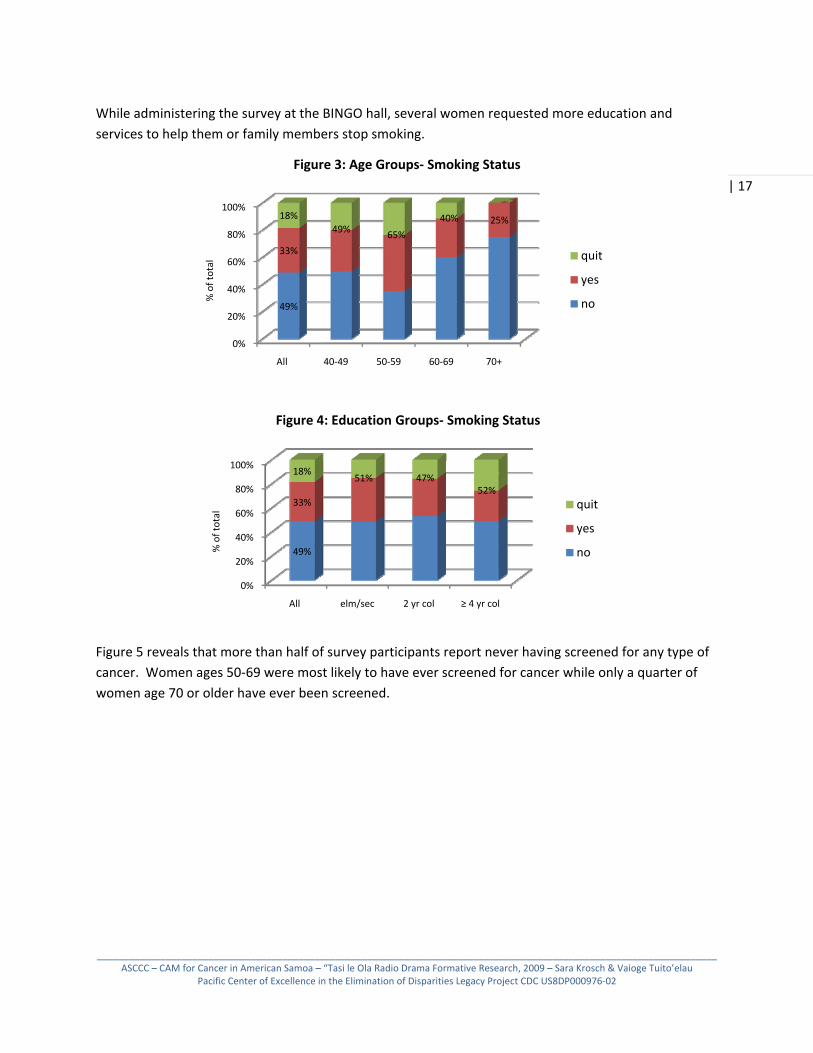
While administering the survey at the BINGO hall, several women requested more education and services to help them or family members stop smoking.
0%
20%
40%
60%
80%
100%
All 40‐49 50‐59 60‐69 70+
49%
33%
49% 65%
40% 25%18%
Figure 3: Age Groups‐ Smoking Status
quit
yes
no % of total
| 17
0%
20%
40%
60%
80%
100%
All elm/sec 2 yr col ≥ 4 yr col
49%
33%
51% 47%52%
18%
Figure 4: Education Groups‐ Smoking Status
quit
yes
no % of total
Figure 5 reveals that more than half of survey participants report never having screened for any type of cancer. Women ages 50‐69 were most likely to have ever screened for cancer while only a quarter of women age 70 or older have ever been screened.
_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02

0%
20%
40%
60%
80%
100%
All 40‐49 50‐59 60‐69 70+
55%
44%36%
55% 60%
25%
1%
Figure 5: Age Groups‐ Any Cancer Screening Status
no repsonse
yes
no% of total
| 18
Figure 6 illustrates that the likelihood of ever screening for any type of cancer increases with education attainment; women with a 4 year college degree or more were the most likely to have ever screened for cancer.
0%
20%
40%
60%
80%
100%
All elm/sec 2 yr col ≥ 4 yr col
55%
44% 41% 39%60%
1%
Figure 6: Education Group‐ Any Cancer Screening Status
no repsonse
yes
no% of total
American Samoa is fortunate to have a CDC‐funded Breast and Cervical Cancer Early Detection Program (BCCEDP) which offers free pap smears and mammograms to women age 40 and older. Some women appear to be accessing this program because 79 of the 179 women reported at least one cancer screen during their lives. Of these 79 women 44 (56%) have had a mammogram, 61 (77%) have performed a self‐breast exam, and 68 (86%) have had a pap test at least once during their lifetimes.
_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 19
0%
20%
40%
60%
80%
100%
All 40‐49 50‐59 60‐69 70+
38%
56%
32%
71%
66%
50%
6% 14%
50%
Figure 7: Age Groups‐Mammogram Status
no repsonse
yes
no% of total
Only 25% of the sample stated they had ever had a mammogram. As shown in Figure 5, 79 survey respondents reported screening for some type of cancer at least once. Fifty‐six percent (56%) of this group said they had at least one mammogram in their lives (Figure 7). This is much higher that then 33% of Samoan women living in the United States age 40 and older reporting ever having a mammogram (APIAHF, 2006; Hubbell, et al., 2005). The majority of these women are in their 50’s and 60’s. Only one women age 70 or older reported ever having a mammogram. Six percent (6%) of women who reported having been screened for cancer did not respond to the question of whether they had ever had a mammogram. It is possible the women surveyed are unfamiliar with the term mammogram. Figure 8 proves that education status alone does not ensure higher proportions of mammogram screening. Over half of women with elementary/secondary education and 2 year college degrees report having a mammogram, but this number drops to 38% of women with a 4 year college degree or beyond.
0%
20%
40%
60%
80%
100%
All elm/sec 2 yr col ≥ 4 yr col
53% 56% 68%
38%
6% 7% 4% 4%
Figure 8: Education Group‐Mammogram Status
no repsonse
yes
no% of total
About 34% of the sample said they had performed a self‐breast exam. Figure 9 illustrates that self‐breast exams (SBE) are common but their frequency is unknown. Sixty‐one (61) of the 79 women who have screened for cancer say they have done a self‐breast exam (SBE). Less than one fifth of women in their 50’s and 60’s have never performed a SBE but no women age 70 or older reported doing this self‐check. Several older respondents did not respond to this question.

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 20
0%
20%
40%
60%
80%
100%
All 40‐49 50‐59 60‐69 70+
20%
73%
65%
86%81%
7% 3%14%
50%
Figure 9: Age Groups‐ Self‐Breast Exam Status
no repsonse
yes
no% of total
Unlike mammogram status, Figure 10 exhibits the impact education level has on SBE performance. The percentage of women who have ever done a self exam increases with more years of formal education. Additionally, all women with a 4 year college degree or more responded to this question about SBE which could reveal a clearer understanding of the procedure. More than 10% of less educated women did not respond to this question possibly because they are not be familiar with SBEs.
0%
20%
40%
60%
80%
100%
All elm/sec 2 yr col ≥ 4 yr col
15%
77% 63%80%
81%
8% 11% 8%
Figure 10: Education Groups‐ Self‐Breast Exam Status
no repsonse
yes
no% of total
Robinson, et al. (2002) found that Pacific Islanders are the least likely racial/ethnic group to utilize regular pap test services in the United States. Yet, survey respondents were more likely to have had a pap test than a mammogram or SBE in their lifetimes. Sixty‐eight (68) of the 179 women surveyed (38%) report having had at least one pap test (Figure 11). This is lower than the 46% of Samoan women in American Samoa, Hawaii and Los Angeles reported by the Asian Pacifc Islander American Health Forum (2006) and Hubbell, et al. (2005).
As with other screening procedures women age 70 and older are the least likely to have ever had a pap test (Figure 11). Several women in their 50’s declined to answer this question for unknown reasons.

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 21
0%
20%
40%
60%
80%
100%
All 40‐49 50‐59 60‐69 70+
9%
50%
86% 84% 86%81%
50%
5% 14%
Figure 11: Age Groups‐ Pap Test Status
no repsonse
yes
no% of total
Compared to age, Figure 12 shows that education status is less of an indicator of women ever having a pap test. Over 80% of women from all education groups report having had a pap test in their lifetimes.
0%
20%
40%
60%
80%
100%
All elm/sec 2 yr col ≥ 4 yr col
9%
86% 88% 88% 81%
5% 4% 4%
Figure 12: Education Groups‐ Pap Test Status
no repsonse
yes
no
% of total
Nine (9) of the 179 survey respondents or 5% stated that had been diagnosed with cancer sometime during their lifetime (Figure 13). Of these 9 cancer survivors, most had breast cancer. This echoes previous research that found breast cancer is the most common amongst Pacific Islanders women living in Hawaii and American Samoa(APIAHF, 2006 ; Hubbell, et al., 2005; Ishida, et al., 2001; Miller, et al., 2007). More than twice as many breast cancer survivors than cervical cancer survivors were captured in the survey sample. All 5 breast cancer survivors were in their 60’s while the 3 other survivors (2 with cervical cancer and 1 with another site) were in their 40’s. It is unknown at what age all reported cancer survivors were first diagnosed.

9, 100%
5, 56%
2, 22%1, 11% 1, 11%
Figure 13: Survey Respondent Cancer Survivors
All
breast
cervix
other
no response
#respon
dents
| 22
All cancer survivors surveyed reported seeking some sort of treatment. Figure 14 illustrates that the majority (78%) were treated at a hospital. But nearly 1/4 (22%) said they utilized a traditional Samoan healer (Taulasea/Fofo) to treat their cancer. This is a significantly higher percentage than the 1% of US cancer patients Moa and colleagues (2007) report using traditional medicine.7
9, 100%
7, 78%
2, 22%
Figure 14: Cancer Suvivor Reported Treatments
All
hopsital
Taulasea/Fofo#respon
dents
Research in the United States (Lee, et al.,2004 ) and in American Samoa (Hubbell, et al.,2005) has shown that family recommendations can be strong indicators of cancer patient treatment choices. Survey participants were asked what they would advise a female friend or relative to do if she was diagnosed with breast cancer or cervical cancer. Figure 15 illustrates that most women from all age groups would encourage their peers to seek hospital treatment after a cancer diagnosis. The second most popular advice is prayer, often concurrently, as a complementary therapy, with hospital treatment. More women chose not to respond to this question (13%) than to advise seeking a Taulasea/Fofo (5%) for cancer treatment. Previous focus group research conducted by the American Samoa Community Cancer Network (ASCCN) with males age 40 and older in American Samoa found several were reluctant to offer advice to other men about their health—stating it was not their place (Krosch, 2008). This appears to be true for a significant percentage of women as well. However other ASCCN research has shown that 46% of females ages 40 and older have learned about cancer in the past from cancer survivors and 65% of this population want to learn more about cancer from cancer survivors (Krosch, 2009).
7 A larger sample of female cancer survivors in American Samoa is needed to confirm this finding. _____________________________________________________________________________________________________________________
ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02

“Other” responses included: do nothing (n=3); see a specialist (n=2); eat the right food (n=1); make my own Samoan medicine from plants (n=1); get a second opinion (n=1), wait (n=1); and, any other treatment possible (n=1).
_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 23
0
20
40
60
80
100
120
140
160
84%
5%22%
8% 13%
Figure 15: All Respondents‐ Proposed Advice to Family/Friend Diagnosed with Breast or Cervical Cancer
hospital
Taulasea/Fofo
prayer
other
no response
% of total respondents
# respon
dents
Figure 16 illustrates the difference age makes in the type of advice women would give their peers. Older women are slightly less likely to recommend hospital treatment for breast or cervical cancer than are their younger counterparts. This group may also be the most likely to give no advice given 38% did not answer this question. Nearly 1/4 of women in their 60’s would recommend prayer, and this group is the most likely to advise others to seek a Taulasea or Fofo.
0
10
20
30
40
50
60
70
80
90
40‐49 50‐59 60‐69 70+
Figure 16: Age Groups‐ Proposed Advice to Family/Friend Diagnosed with Breast or Cervical Cacner
hospital
Taulasea/Fofo
prayer
other
no response
% respo
nden
ts
Education level makes little difference in proposed cancer treatment advice with the exception of women with only an elementary/secondary education being two to three times more likely to encourage traditional healing methods (Figure 17).

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 24
0102030405060708090100
elm/sec 2 yr col ≥ 4 yr col
Figure 17: Education Groups‐ Proposed Advice to Family/Friend Diagnosed with Breast or Cervical Cancer
hospital
Taulasea/Fofo
prayer
other
no response
% respo
nden
ts
Swisher et al. (2002) found that personal use of CAM prior to a cancer diagnosis is a strong indicator of utilization for cancer treatment. Some traditional Samoan treatments are commonly known and can be prepared and administered without the direction of a Taulasea or Fofo while others require visiting these specialists (MacPherson and MacPherson, 1990; Whistler, 1995). The final women’s survey questions asked if respondents had ever visited a traditional Samoan healer for any reason. Over 2/3 of respondents (77%) said no—the predominate answer for all age groups and education groups (Figures 18‐19). Likelihood of Traditional Samoan healer utilization increased with age and decreased with higher educational attainment.
0%
20%
40%
60%
80%
100%
All 40‐49 50‐59 60‐69 70+
77%
22% 18% 24% 31%10%1%
Figure 18: Age Groups‐Personal Use of Tradtional Samoan Healers
no response
yes
no
% of total

____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
_
| 25
Table 4 lists the reasons respondents gave for ever having visited a Taulasea/Fofo.
Table 4: Reasons for Traditional Healer Utilization
Illness/Reason # RespondentsStomachache 8 Headache 6 Back pain 3 Cancer 2
8Toala/Infertility 2 Massage 1 Legs 1 Cold 1 Flu 1
Hyperthyroid 1 Breast 1
Evidence‐based Recommendations from Women’s Survey for Radio Serial Drama Development
• Main characters should be representative of the sample: between 40‐60 years old, with a secondary school diploma or 2 year college degree.
• Smoking is common amongst women so smoking risks should be addressed in a secondary plot line
• Half of women age 40‐60 have never screened for any type of cancer so the screening process and benefits should be communicated and modeled.
• Women with less education are less likely to screen for cancer. This scenario should be depicted in a transitional character: a woman with a secondary or 2 year college degree overcoming barriers to cancer screening.
8 Toala: A Samoan illness/concept often associated with infertility, thought to be a floating organ that needs to be realigned or placed properly via massage to ensure fertility or other wellbeing (MacPherson and MacPherson, 1990; Whistler, 1995).
0%
20%
40%
60%
80%
100%
All elm/sec 2 yr col ≥ 4 yr col
77%
22% 27% 23% 14%1%
Figure 19: Education Groups‐Personal Use of Tradtional Samoan Healers
no response
yes
no% of total

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 26
• Fewer than half of the women surveyed report ever screening for breast or cervical cancer: 25% had a mammogram; 34% had performed a SBE; and 38% had ever had a pap test. All three screening procedures should be modeled by characters.
• Women were least likely to have screened with a mammogram so this process in particular and its benefits should be communicated and modeled. A character in her 40’s should get regular mammograms to model consistent screening at an earlier age. Women with higher education levels need encouragement to have regular mammograms
• Self‐breast exams were common but it is unknown how frequently women do this check. The process and benefits of SBEs should be communicated and modeled especially by an older female character with less education.
• Age or education level had little impact in predicting who is likely to have a pap test. However, 14% of women in their 50’s declined to answer the question about pap tests. A transitional character in this age group should model overcoming barriers to regular pap tests.
• Survivors were most likely to have been diagnosed with breast cancer and to be to seek hospital treatment. A character should be diagnosed with breast cancer and model seeking Western medical treatment.
• A quarter of cancer survivors reported seeing a Taulasea/Fofo for their cancer. The pros and cons of using traditional healing methods as complementary and an alternative medicine should be communicated.
• The most common advice women would give to a friend or family member diagnosed with breast or cervical cancer is to seek hospital treatment and to pray. Older women and those with an elementary or secondary education are more likely to encourage traditional healing. These scenarios should be depicted.
Part III‐ Western Health Care Professionals Survey Results
Survey Methods
In February 2009, 43 health care professionals employed at LBJ Hospital and 4 staff members from the American Samoa Department of Health Breast and Cervical Cancer Early Detection Program (BCCEDP) were surveyed. Hospital staff members were given the 15‐item self‐administered survey (see page 87) at a weekly in‐service training held at the hospital conference room and earned a pen and a $2 hospital cafeteria coupon for completing it. BCCEDP staff members were surveyed at their office and were given pencils. The survey questions were mainly inspired by Jump and colleagues’ 1998 United States‐based

research entitled Physicians’ Attitudes toward Complementary and Alternative Medicine. A summary table of this survey’s results can be found on page 84.
Respondent Demographics
Four main characteristics were sought for data analysis: gender, age group, race/ethnicity, and number of years in the medical profession. There were almost twice as many males as females surveyed (Figure 20). Most respondents were in their 30’s and 40’s (Figure 21) and the majority was Samoan (Figure 22). Figure 23 shows the sample could be evenly divided into two groups: those who had been in the medical profession 11 years or less or longer than 11 years.
| 27
47
17
30
Figure 20: Respondents by Gender
All
Females
Males
# repondents
0
10
20
30
40
50
All Females Males
14
15
Figure 21: Respondents by Age Group
60+
50‐59
40‐49
30‐39
20‐29
# repo
nden
ts
0
10
20
30
40
50
All Females Males
22
310
12
Figure 22: Respondents by Race/Ethnicity
Caucasian
Asian
Other Pac Is
Samoan# repo
nden
ts
_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 28
0
10
20
30
40
50
All Females Males
23
23
1
Figure 23: Respondents by Years in Health Care Profession
no response
> 11 yrs
≤ 11 yrs# repo
nden
ts
Additionally, health care professionals were asked their current position and the number of females age 40 and older, the main target group for breast and cerival cancer screening, they see on a weekly basis. Figure 24 reveals that most respondents were doctors and/or specialists. Females were likely to fall into the “other” category. Regardless of a respondent’s position, it was assumed that members of the community at large would see any hospital or public health employee as a representative of the Western medical sector and consider her/his advice reflective of mainstream medical beliefs and practices.
0
5
10
15
20
25
All Females Males
Figure 24: Respondents' Current Position(s)
doctor
medical officer
nurse
specialist
other
no response
# repo
nden
ts
Table 5: Types of Specialists and Other Professionals Surveyed
Types of Specialists Other Professionals Ob/Gyn=6 Surgeon=3 Emergency=2 Ophthalmologist=2 Anesthesiologist=2 Pathologist=1 Pediatrician=1
Dentist/Dental Officer=4Physician Assistant=4 Medical Social Worker=1 CEO=1 Midwife=1 Health Educator=1 Clerk=1 Program Coordinator=1

As shown in Figure 25, most respondents see 10‐29 women age 40 and older each week. Male medical professionals are more likely to see 50 or more women weekly. Seeing more women in this target population may make males more influential.
_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 29
0
10
20
30
40
50
All Females Males
Figure 25: Number Female Patients Age 40+ Seen Weekly
no response
50+
30‐49
10‐29
< 10
# repo
nden
ts
Survey Analysis by Gender, Age, Race/Ethnicity & Years in Health Care Profession
Jump et al. found that doctors in the United States were more likely to recommend CAM to their patients if they were CAM users themselves and they were most likely to recommend the specific types of CAM they had personally used. The categories of CAM provided in our survey are among the most popular reported in Jump’s study with the addition of “Samoan healer.” Traditional Samoan healing methods are have been practiced in American Samoa and independent Samoa since before European contact and today parallel medical systems—traditional and Western/scientific—coexist (MacPearson and MacPhearson, 1990).
Figure 26 shows us that exercise and diet are the top two CAM personally used and recommended by the professionals surveyed followed by prayer and massage. Professionals have turned to prayer and herbal remedies significantly more often than they have recommended these CAM. Conversely, they recommend support groups more than they have participated in these. Massage and herbal remedies are the main types of CAM practiced by Samoan healers but the survey data does not confirm if these types of CAM are administered by Taulasea/Fofo.

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 30
0
5
10
15
20
25
30
35
40
Figure 26: All Respondents‐ Personal CAM Use & Recommendations to Patients
All used
All recm.
# repo
nden
ts
Females and males have personally used the same 4 CAM most often: diet, exercise, prayer and massage (Figures 27 and 28). However, genders differ in terms of recommendations to patients. Women are less likely to recommend prayer, massage, relaxation techniques and Samoan healers than are men. In general, women tend to use more CAMs than they recommend to others. This may be influenced by the facts that most female respondents are younger, have been in the medical profession fewer years, and see fewer women per week than male respondents. Both females and males have used and recommended massage over herbal remedies or explicitly seeing a Samoan healer. With the exception of a few massage therapists on the island, massage is largely practiced by Samoan Fofo. Therefore, if a medical professional recommends a patient be massaged they could be indirectly encouraging Samoan healer use as a CAM.
0
2
4
6
8
10
12
14
Figure 27: Females (n=17)‐ Personal CAM Use & Recommendations to Patients
Females used
Females recm.# repo
nden
ts

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 31
0
5
10
15
20
25
Figure 28: Males (n=30)‐ Personal CAM Use & Recommendations to Patients
Males used
Males recm.# repo
nden
ts
Jump and colleagues found that younger doctors were more likely to have used and recommended any type of CAM. Almost twice as many survey respondents were age 40 or older. Exercise, diet, prayer and massage were the top CAM used and recommended by respondents regardless of age (Figures 29 and 30). Those 40 and older were more likely to use and recommend herbal remedies and Samoan healers.
0
2
4
6
8
10
12
14
16
Figure 29: <40 Years Old (n=16)‐Personal CAM Use & Recommendations to Patients
< 40 yrs used
< 40 yrs recm.# repo
nden
ts

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 32
0
5
10
15
20
25
30
Figure 30: ≥40 Years Old (n=31)‐Personal CAM Use & Recommendations to Patients
≥ 40 yrs used
≥ 40 yrs recm.# repo
nden
ts
Respondents fell into 4 categories of race/ethnicity9: Samoan, Other Pacific Islander, Asian or Caucasian. Only 3 surveyed were Other Pacific Islanders so these cases were excluded from analysis. Figures 31‐33 exhibit the similarities and differences between the different race/ethnic groups. All three groups have used and recommend diet and exercise as CAM most often. Samoans and Asians have turned to prayer, while Caucasians have used massage and relaxation techniques as the third most popular CAM. All Asian respondents have used at least some type of CAM and nearly all Asians and all Caucasians recommend exercise and diet changes. Samoans and Caucasians recommend massage equally. Samoans are the mostly likely to have used and recommended herbal remedies and Samoan healers.
0
4
8
12
16
20
Figure 31: Samoans (n=22)‐ Personal CAM Use & Recommendations to Patients
Samoan used
Samoan recm.
# repo
nden
ts
9 These categories are adapted from those used by the United States National Institutes of Health (NIH): 2 ethnic categories (Hispanic/Latino and Non‐Hispanic/Latino) and 5 racial categories (American Indian/Alaska Native, Asian, Black/African American, Native Hawaiian/Other Pacific Islander, and White). Racial and ethnic classifications were self‐identified by survey respondents. Racial categories are social‐political constructs and should not be interpreted as being anthropological or biological in nature. These distinctions are sought in order to uncover and monitor trends and potential health disparities between groups.

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 33
0
2
4
6
8
10
Figure 32: Asians (n=10)‐ Personal CAM Use & Recommendations to Patients
Asian used
Asia recm
# repo
nden
ts
0
2
4
6
8
10
12
Figure 33: Caucasians (n=12)‐ Personal CAM Use & Recommendations to Patients
Caucasian used
Caucasian recm.
# repo
nden
ts
US doctors newer to the medical profession were more likely to have used and recommended CAM (Jump, et al, 1998). This was also true of the sample in American Samoa. Diet, exercise, prayer and massage remained the top picks despite number of years in the medical profession. However, respondents who had been professionals up to 11 years were more likely to have used and recommended diet, exercise, support groups and relaxation techniques as CAM. Their senior counterparts were more likely to have used and recommended prayer and massage as CAM.

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 34
0
5
10
15
20
25
Figure 34: ≤11 Years in Health Care Profession (n=23)‐Personal CAM Use & Recommendations to Patients
≤ 11 yrs used
≤ 11 yrs recm.
# repo
nden
ts
0
5
10
15
20
25
Figure 35: >11 Years in Health Care Profession (n=23)‐Personal CAM Use & Recommendations to Patients
> 11 yrs used
> 11 yrs recm.
# repo
nden
ts
Health provider‐patient consultations present a pivotal opportunity to recommend treatments. Professionals were asked if they have ever asked a patient if they were using Samoan healing methods; if they had ever been told by a patient they were using Samoan healing methods (whether they had asked or not); and if they had asked a patient to stop using Samoan healing methods, presumably because they were believed to be ineffective or interfering with mainstream treatment.
Figure 36 shows the majority of females and male respondents recall asking patients if they were using Samoan healing methods and recall being told by patients they are using this CAM. Respondents are less likely to ask a patient about using Samoan healing methods than to have been told which leads one to believe that some patients offer this information to health providers unprompted. Likelihood drops significantly for female and male providers to tell a patient to stop using Samoan healing methods. Over
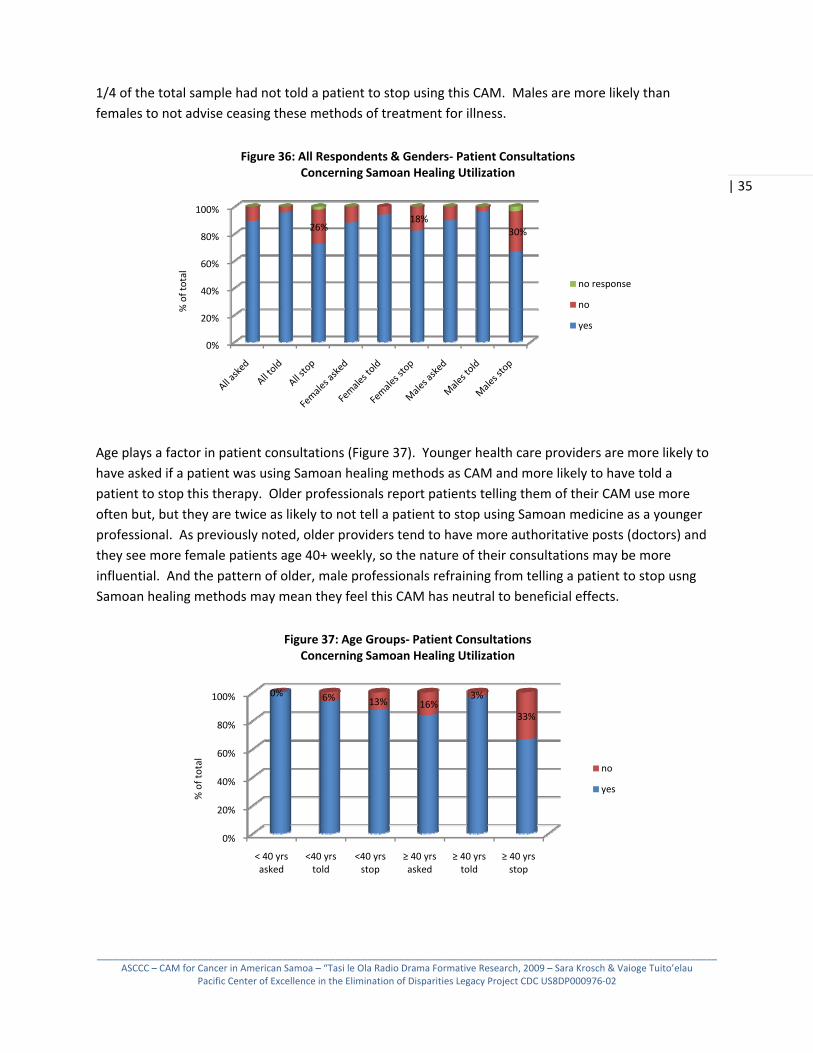
1/4 of the total sample had not told a patient to stop using this CAM. Males are more likely than females to not advise ceasing these methods of treatment for illness.
_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 35
0%
20%
40%
60%
80%
100%
26%18%
30%
Figure 36: All Respondents & Genders‐ Patient Consultations Concerning Samoan Healing Utilization
no response
no
yes
%of to
tal
Age plays a factor in patient consultations (Figure 37). Younger health care providers are more likely to have asked if a patient was using Samoan healing methods as CAM and more likely to have told a patient to stop this therapy. Older professionals report patients telling them of their CAM use more often but, but they are twice as likely to not tell a patient to stop using Samoan medicine as a younger professional. As previously noted, older providers tend to have more authoritative posts (doctors) and they see more female patients age 40+ weekly, so the nature of their consultations may be more influential. And the pattern of older, male professionals refraining from telling a patient to stop usng Samoan healing methods may mean they feel this CAM has neutral to beneficial effects.
0%
20%
40%
60%
80%
100%
< 40 yrs asked
<40 yrs told
<40 yrs stop
≥ 40 yrs asked
≥ 40 yrs told
≥ 40 yrs stop
0% 6% 13% 16%3%
33%
Figure 37: Age Groups‐ Patient Consultations Concerning Samoan Healing Utilization
no
yes
%of to
tal

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 36
0%
20%
40%
60%
80%
100%9% 30% 42%
Figure 38: Race/Ethnic Groups‐ Patient Consultations Concerning Samoan Healing Utilization
no response
no
yes
%of to
tal
The racial/ethnic group of the professional results in different patient consultations (Figure 38). Samoan providers, the largest group employed at LBJ, are the most likely to ask a patient if they are using Samoan healing methods and they are the least likely to tell a patient to stop using this CAM. All Caucasian providers recall patients divulging their use of Samoan healing compared to 90% of Samoans and Asians. The biggest differences can be seen in advice to stop using Samoan healing; 30% of Asian and 42% of Caucasian providers have not told a patient to stop utilizing Samoan healing methods compared to 9% of Samoans. This could reflect lack of knowledge of the effectiveness of Samoan healing methods compared to mainstream care and therefore a reluctance to advise a patient to stop and/or an acceptance of the potential Samoan healing methods have for complementary therapy.
0%
20%
40%
60%
80%
100%
≤ 11 yrs asked
≤ 11 yrs told
≤ 11 yrs stop
> 11 yrs asked
> 11 yrs told
> 11 yrs stop
17%30%
Figure 39: Years in Health Care Profession‐ Patient Consultations Concerning Samoan Healing Utilization
no response
no
yes%of to
tal
Figure 39 shows us that more senior providers were almost twice as likely to tell patient to stop using Samoan healing methods.

Samoan healing methods could be used a complementary care, at the same time as mainstream treatment, or in lieu of Western medicine as alternative care. Health care providers were asked if they felt most American Samoan patients used Samoan healing methods as complementary or alternative therapy, or both. The majority off females and males felt patients predominantly access Western medical treatment and use Samoan medicine to complement this care (Figure 40). Slightly more females than males felt that patients forego mainstream care and rely on Samoan healing as an alternative treatment. About 10% of the sample felt Samoan healing methods are used as both complementary and alternative medicine in the general population.
| 37
0%
20%
40%
60%
80%
100%
All Females Males
Figure 40: All Respondents & Genders‐Overall Impression of Samoan Healing as CAM
Both
Alternative
Complementary
%of to
tal
Figure 41 reveals that older respondents had more varied opinions about the nature of Samoan healing as a CAM with fewer seeing it as strictly a complementary or alternative therapy. Perhaps older professionals have a deeper understanding of the many applications of Samoan healing such that some methods are effective as a complementary course of action and others are used as an alternative to hospital care.
0%
20%
40%
60%
80%
100%
<40 yrs ≥40 yrs
81%68%
18%16%
16%
Figure 41: Age Groups‐Overall Impression of Samoan Healing as CAM
Both
Alternative
Complementary%of to
tal
_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 38
0%
20%
40%
60%
80%
100%
Samoan Asian Caucasian
73% 70% 66%
18%10% 26%
9% 20%8%
Figure 42: Race/Ethnic Groups‐Overall Impression of Samoan Healing as CAM
Both
Alternative
Complementary%of to
tal
Figure 42 illustrates Caucasian respondents are the most likely to feel that Samoan healing methods are used instead of mainstream Western methods. More than twice as many Asian professionals believe Samoan healing is used as both a complementary or alternative therapy. It is unknown if respondents endorse Samoan methods as an alternative therapy for any illness or any stage of illness.
Providers with less professional experience were almost two times as likely to think Samoan healing methods are used primarily as an alternative to mainstream care (Figure 43).
0%
20%
40%
60%
80%
100%
≤ 11 yrs > 11 yrs
22% 13%
Figure 43: Years in Health Care Profession‐Overall Impression of Samoan Healing as CAM
Both
Alternative
Complementary
Health care professionals were specifically asked if they were aware of local breast or cervical cancer survivors who had used or were using Samoan healing methods as complementary medicine or alternative medicine. Figure 45 shows that 60% of all respondents said they were aware of breast or cervical cancer survivors using Samoan healing with equal proportions of complementary and alternative use. Males were more likely to be aware of these local cases of CAM for women’s cancer. Slightly fewer females are aware of women using Samoan healing as an alternative rather than a complementary therapy for cancer care.

0%
20%
40%
60%
80%
100%
All Comp.
All Altn.
Females Comp.
Females Altn.
Males Comp.
Males Altn.
Figure 44: All Respondents & Genders‐Awareness of Local Breast/Cervical Cancer Patients
Utilizing Samoan Healing as CAM
yes
no
%of to
tal
| 39
One third more of older respondents were aware of women using Samoan healing as complementary and alternative therapy for breast or cervical cancer (Figure 46).
0%
20%
40%
60%
80%
100%
<40 yrs Comp. < 40 yrs Altn. ≥40 yrs Comp. ≥ 40 yrs Altn.
Figure 45: Age Groups‐Awareness of Local Breast/Cervical Cancer Patient
Utilization of Samoan Healing as CAM
yes
no
%of to
tal
Figure 47 shows Asian providers are the most aware of breast and cervical cancer patients using Samoan healing as CAM followed by Samoans and Caucasians. Both Samoans and Caucasians are aware of more cases of Samoan healing methods being used as an alternative to mainstream care than as a complement to hospital treatment.
_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 40
0%
20%
40%
60%
80%
100%
Samoan Comp.
Samoan Altn.
Asian Comp.
Asian Altn.
Caucasian Comp.
Caucasian Altn.
Figure 46: Race/Ethinc Groups‐Awareness of Local Breast/Cervical Cancer Patients
Utilization of Samoan Healing as CAM
yes
no
%of to
tal
And similar to age groups, the longer a provider had been in the medical profession the more likely she or he was to be aware of breast and cervical cancer patients using Samoan healing as a CAM. Professionals with 11 or less years of experience are aware of slightly more cases of alternative use of Samoan healing methods (Figure 48).
0%
20%
40%
60%
80%
100%
≤ 11 yrs Comp ≤ 11 yrs Altn > 11 yrs Comp > 11 yrs Altn
Figure 47: Years in Health Care Profession‐Awareness of Local Breast/Cervical Cancer Patient
Utilization of Samoan Healing as CAM
yes
no
%of to
tal
Whether a health care professional endorses a CAM or advises a patient to discontinue use of a CAM is most likely to correspond to their perceptions of its overall impact on the health of the patient; does the CAM result in a helpful, neutral or harmful outcome.10 Survey respondents were divided on the impact Samoan healing methods in general have on patients. In Figure 49 we see that more health care professionals feel Samoan healing methods have a harmful effect on patient health than a helpful effect. More females felt traditional healing methods were harmful, while males were evenly divided between harmful and helpful verdicts.
10 Patient health/health outcome was not strictly defined in the survey so it is unknown if respondents interpreted the question to mean only physical health outcomes or if they took “health” to mean overall quality of life.

Given the variety of traditional healing methods—incantations and prayers, topical and oral herbal remedies, and massage—it is no wonder that some created their own categories to respond to this question resulting in “harmful‐neutral” and “harmful & helpful” choices. If a percentage of these two responses were added to the “harmful” response we see even more of the sample feel traditional healing methods tend to be more harmful than helpful to patient health.
| 41
0%
20%
40%
60%
80%
100%
All Females Males
36% 44% 32%
29% 25% 32%
Figure 48: All Respondents & GendersPerceptions of Samoan Healing Impact on Health
no response
harmful & helpful
helpful
neutral
harmful ‐ neutral
harmful
%of to
tal
There was little difference between age groups except older professionals feel Samoan healing methods are less purely neutral and more harmful to neutral in their effects (Figure 50).
0%
20%
40%
60%
80%
100%
< 40 yrs ≥40 yrs
Figure 49: Age Groups‐Perceptions of Samoan Healing Impact on Health
no response
harmful & helpful
helpful
neutral
harmful ‐ neutral
harmful
One third of Asian and Caucasian providers surveyed felt that Samoan healing methods had a helpful impact on patient health compared to 22% of Samoans (Figure 51). Asians were the most likely to think that traditional healing would have a neutral effect on health, more than twice as much as Samoans and four times more than Caucasians. A significant percentage of Samoan and Caucasian providers did not respond to this question. Caucasians most likely did not respond due to lack of knowledge about Samoan healing methods and experience with patents utilizing this CAM as previously shown. It is unknown why 9% of Samoans, the group most senior in age and experience at LBJ, seeing the most patients per week, thus presumably in the best place to comment on the impact Samoan healing methods have on patient health outcome, declined to answer this question.
_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 42
0%
20%
40%
60%
80%
100%
Samoan Asian Caucasian
14% 33%
8%
22%
30%
33%
9%16%
Figure 50: Race/Ethnic Groups‐Perceptions of Samoan Healing Impact on Health
no response
harmful & helpful
helpful
neutral
harmful ‐ neutral
harmful
Finally, Figure 52 shows professionals working more than 11 years were more likely to feel Samoan healing methods were helpful to patients. More than half (64%) of junior professionals felt traditional medicine had a harmful or neutral effect. Again, professionals with more experience were more likely to not respond to this question for unknown reasons.
0%
20%
40%
60%
80%
100%
≤ 11 yrs > 11 yrs
43%30%
22%39%
Figure 51: Years in Health Care Profession‐Perceptions of Samoan Healing Impact on Health
no response
harmful & helpful
helpful
neutral
harmful ‐ neutral
harmful
Lastly, health care professionals were asked if they were interested in learning more about traditional Samoan healing methods. Figure 52 shows that 70% said yes, with females more eager to learn than males. Younger providers and those in the medical profession less than 11 years wanted information more than older providers (Figures 53 and 55). All Caucasian respondents want to learn more about traditional medicine compared to 2/3 of Samoan and Asian providers (Figure 54). This probably reflects the fact that many Caucasian professionals are contract workers at LBJ, with stays as short as a few months to 2 years, compared to long‐term Samoan and Asian residents who have had a longer time to gain knowledge of Samoan healing methods. It could also point to Jump et al.’s findings that junior professionals have received more education about CAM and see these methods as more legitimate care options than do senior professionals.

0%
50%
100%
All Females Males
70% 76% 66%
Figure 52: All Respondents & Genders‐Interest in Learning More about Samoan Healing Methods
yes
no
| 43
0%
50%
100%
< 40 yrs ≥40 yrs
81% 65%
Figure 53: Age Groups‐ Interest in Learning More about Samoan Healthing Methods
yes
no
0%
50%
100%
Samoan Asian Caucasian
Figure 54: Race/Ethnic Groups‐Interest in Learning More about Samoan Healing
Methods
yes
no
0%
50%
100%
≤ 11 yrs > 11 yrs
83% 61%
Figure 55: Years in Health Care Profession‐Interest in Learning More about Samoan Healing
Methods
yes
no
_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02

Evidence‐based Recommendations from Health Care Professional’s Survey for Radio Serial Drama Development
• Male, Samoan Doctor/Specialists with more than 11 years of experience typically see the most women age 40 and older so a character should be created to fit this description.
_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 44 • The most widely accepted CAM are diet modifications, increased exercise, prayer and massage. Health care professional characters should model these CAM recommendations.
• Health care providers are in favor of support groups but may be unaware of them on the island. Cancer‐related support groups should be featured in the plot.
• Massage is a more acceptable CAM than herbal remedies or specifically recommending seeing a Taulasea/Fofo. The health benefits and potential hazards of massage as a complementary therapy should be communicated.
• Prayer is a widely used and recommended CAM. It should be modeled as a complementary medicine and not an alternative to mainstream care.
• Older males, especially Asians and Caucasians, are less likely to tell a patient to stop using Samoan healing methods as a CAM despite perceptions of negative health consequences. They may be a secondary target audience with a relatable character modeling a patient consultation.
• Health care professionals who are female, under 40 years old and with, 11 years experience feel Samoan healing methods are used more often as alternative care rather than complementary. A character fitting this description likely comes in contact with women in informal settings and could encourage using some Samoan healing methods as complementary care to mainstream treatments.
• The majority of health providers were aware of breast or cervical cancer patients using Samoan healing methods as both complementary and alternative treatments. A provider character should encourage a patient character to disclose all methods of treatment they are using and document and monitor patient progress so as to encourage effective complementary care and not a loss to alternative methods.
• The majority of health care providers feel that Samoan healing methods in general have a harmful to neutral effect on patient health. And most providers want to know more about Samoan healing methods. Therefore, health care providers should be a secondary target audience so they can be more informed and feel confident in recognizing positive or negative effects from Traditional healing.

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 45
Part IV‐ Key Informant Interviews
January‐March 2009 the authors gathered data from 13 interviews conducted in American Samoa. The purpose of the interviews was to gain a deeper understanding of Samoan healing methods as CAM in general and specifically for breast and cervical cancer treatment locally. Information from the interviews will be used to develop realistic characters and scenarios for a 5‐part radio serial drama.
Five groups of people were sought for interviews: 1) medical doctors diagnosing breast or cervical cancer at LBJ hospital; 2) BCCEDP staff; 3) breast cancer and cervical cancer survivors; 4) traditional Samoan healers (Taulasea/Fofo) who have treated cancer patients in American Samoa; 5) Others with knowledge and experience of cancer treatment including surviving family members of cancer patients and Samoans who use traditional medicine.
The authors conducted formal, taped interviews lasting 30‐60 minutes with 1 medical doctor seeing breast cancer patients at LBJ, 2 Department of Health BCCEDP staff, 3 breast cancer survivors, 1 cervical cancer survivor, 2 surviving family members of deceased cancer patients, and 2 Taulasea/Fofo who have treated women diagnosed with breast cancer.
Thirty minute informal interviews, untapped with written notes taken, were conducted with 1 medical doctor seeing cervical cancer patients at LBJ and 1 Taulasea who has treated cancer patients. In appreciation for their participation in the project, each interviewee was given a case of canned Wahoo fish or a $10 restaurant gift certificate.
A written informed consent was obtained from all interviewees. Five (5) interviews were conducted in Samoan and 8 were done in English suiting the interviewee. Transcripts were written for all taped interviews. If the interview was conducted in Samoan it was first transcribed in Samoan and then translated to English by Ms. Tuitoelau. Full written transcripts and summarized notes form all interviews were analyzed to arrive at the following Evidence‐based Recommendations.
_____________________________________________________________________________________

Evidence‐based Recommendations from Interviews for Radio Serial Drama Development
• Women face several cancer prevention and treatment barriers that should be addressed in scripts‐
o Older women, age 50+, feel screening services are for younger women of childbearing years. They seem to associate breast and cervical health with being sexually active and do not see the need to prioritize cancer screening if they are no longer “having relations” with their husbands. Older women need targeted messages that convince them that breast and cervical cancer screening services are primarily for them.
_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 46
o Screening or other proactive health measures are not a priority for women. Other “plan ahead” behaviors women engage in should be compared to screening for cancer.
o Some women lack the finances for off‐island cancer treatment. The plot should feature this dilemma and illustrate how a female character copes in this situation.
o Fear presents many barriers. For many, cancer only means death. Several women reported being “trained” to perform SBEs or that they had attended educational meetings where they became aware of the symptoms of breast or cervical cancer. But when they experienced symptoms (felt a lump or pain) their knowledge was not enough to empower them to seek treatment for some time. Women need to be encouraged to act on their knowledge and take responsibility for their health as soon as they notice something is wrong. It is also common to fear invasive screening and treatment procedures that involve needles or cutting (fine needle aspiration, biopsy, and surgery). The steps and benefits of these procedures need to be thoroughly explained to dissipate fears.
o Misunderstandings about the nature of cancer and how it can be treated are common. Basic facts about what cancer is, the symptoms and treatment options should be covered.
o Lack of trust in mainstream care contrasted with the ease and comfort of seeing a traditional healer lead many women to stop hospital treatment despite the best attempts at follow‐up. More faith is placed in a Taulasea who always has a diagnosis and a treatment and many women have had success with traditional healing methods for other conditions in
the past. The benefits and limitations of care options should be weighed by characters.
• Family members often discourage hospital treatment and encourage women diagnosed with cancer to seek Samoan healers at all stages of the disease. Family members, especially female relatives and husbands should be a secondary target audience.
• Prayer and religious belief is seen as both a help and a hindrance to cancer screening and treatment. Some doctors feel prayer complements their treatments and that they are seen as “an arm of the Lord.” But, some women may rely only on the power of prayer, especially when they cannot seek off island treatment, when fear overwhelms them, or at advanced stages of cancer. A fatalistic view of cancer being untreatable seems to encourage a heavier reliance on prayer and traditional healing over mainstream care. This view should be replaced by one of empowerment and optimism based on the stories of cancer survivors.

• Women may be most influenced by other cancer survivors, female relatives and husbands. These groups should be represented by different characters who also undergo a thought/behavior change in secondary plot lines.
• Traditional healers lack basic understanding about the stages of cancer. They report seeing most women with “open wounds” on their breasts and they feel that if they treat the wound then cancer will not develop. Healers need to be educated on the stages of cancer, at which stages the disease can be cured, and by what means.
_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 47
• Cancer is considered an oloa a chronic, hard to treat illness. This category includes a wide range of health problems including infected cuts or scratches. This reflects the late stage at which Taulasea see many cancer patients, after they have been experiencing symptoms for months or years, they are overcome with pain and are exhibiting open wounds, and they or their family members are desperate to find help. There seems to be much confusion about if a person is actually suffering from cancer or mainly from other co‐morbid symptoms that could also be considered oloa (diabetes, boils, etc.) At least one Taulasea considers herself a specialized “breast healer” and uses a standard oloa topical treatment for wounds.
• Some cancer patients will go to several Samoan healers after a diagnosis (sometimes experiencing adverse effects from their medicine) and may not return to the hospital unless they are near death. This seems to be primarily because they are afraid of hospital treatments (which some feel can cause or spread cancer) or they are diagnosed at a late stage when little can be done for them at a hospital. Most reported each healer being unsuccessful but a continued desire to seek out healers who have a reputation for curing cancer most often in Apia. This scenario should be depicted in scripts.
• Some Samoan healers feel their medicine will not work if a patient has received mainstream treatment (incisions), while others encourage patients to go to the doctor first, especially if they have co‐morbidities like diabetes, claiming their medicine will be ineffective if the person is sick for other reasons besides oloa/cancer. Traditional healers should be encouraged to tell patients to seek hospital care along with their treatments so patients can be formally monitored.
• Women report using Samoan healing methods to complement mainstream pre‐natal care and as an alternative medicine if diagnosed with cancer. This shift in treatment faith should be explored in the scripts.
• Many believe that cancer is a “new” incurable illness but cancer manifest in the symptoms of an oloa can be cured. Breast cancer is called a mumu (swelling) illness by some patients and Taulasea. Taulasea use noni leaves, breadfruit leaves to treat oloa/breast cancer when manifest as late stage open wounds, tea leaves and coconut or baby oil are used to massage breast lumps; and mamala leaves are used in a drink to prevent and treat cancer.

• Women frequently site the importance of their children as a reason for utilizing both Western medical treatment and Samoan healing for cancer. Some women seek treatment so they can be there for their children. Others do not want to know if they have cancer because they will only worry and not enjoy their remaining days with their children. At least one woman reported not accessing the free screening clinics because “there is no cure…when the time comes that I will die, I will die.” Empowering messages linked to family values should be developed.
_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 48
• Cancer survivors and other women are frustrated with not receiving their test results. This should be depicted with a character being proactive about receiving results and then making informed decisions about her health.
• Tailored messages should be developed for working women and “home women.”
• Women are more comfortable discussing breast health and being screened for breast cancer than they are discussing or having pap smears. Regular cervical cancer screening should be a key message conveyed in a way that is sensitive to women’s reluctance to discuss reproductive body parts.
• Interviewees offer the following messages to be communicated to women at risk for breast or cervical cancer‐
o Don’t let fear keep you from acting. o Ask the doctor questions so you will understand your options. o Faith without works is dead. Have faith but you must act to fulfill those prayers. o Knowledge is not enough. You must act on your knowledge and overcome your
fears. o It is your body and your life. Only you can decide what you will do about your
health. o Don’t give up because the hospital is busy. o Educate yourself and ask questions about your body so you can make informed
decisions. o Don’t be afraid. You are important to your family, your church, your community so
you must take care of yourself. No one will do it for you. o You have to listen to your body. Only you know when something is wrong. o Fear is not the solution. o If you are sick no one will be there to fulfill your obligations so you have to put your
health first. o Get screened early and often. If cancer is discovered early it can be treated and
cured. o Take advantage of all of the education programs and services available to you.

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 49
Table 6: Women’s Survey Results Summary Note‐ percentages are of total and are rounded up Question Age 40‐49
(n=85) Age 50‐59(n=51)
Age 60‐69(n=35)
Age 70+ (n=8)
Have you ever smoked cigarettes?
No=42, 49% Yes, currently=26, 30% Yes, I quit= 17, 19% NR=0, 0%
No=18, 35%Yes, currently=21, 41% Yes, quit=12, 24% NR=0, 0%
No=21, 60%Yes, currently=10, 29% Yes, quit=4, 11% NR=0, 0%
No=6, 75% Yes, currently=2, 25% Yes, quit=0, 0% NR=0, 0%
Have you ever been screened (tested) for cancer?
No=52, 61% Yes= 31, 36% NR= 2, 2%
No=23, 45%Yes=28, 55% NR=0, 0%
No=14, 40%Yes=21, 60% NR=0, 0%
No=6, 75% Yes=2, 25% NR=0, 0%
a. Have you ever had a mammogram?
No=21, 68% Yes= 10, 32% NR=0, 0%
No=8, 29%Yes=20, 71% NR=0, 0%
No=4, 19%Yes=14, 66% NR=3, 14%
No=1, 50% Yes=0, 0% NR=1, 50%
b. Have you ever done a self‐breast exam?
No‐11, 35% Yes=20, 65% NR=0, 0%
No=3, 11%Yes=24, 86% NR=1, 3%
No=1, 4%Yes=17, 81% NR=3, 14%
No=1, 50% Yes=0, 0% NR=1, 50%
c. Have you ever had a pap smear?
No=5, 16% Yes=26, 84% NR=0, 0%
No=4, 14%Yes=24, 86% NR=0, 0%
No=1, 4%Yes=17, 81% NR=3, 14%
No=1, 50% Yes=1, 50% NR=0, 0%
Have you ever been told you have cancer?
No=78, 92% Yes=3, 3% NR=4, 5%
No=49, 96%Yes=0, 0% NR=2, 4%
No=26, 74%Yes=6, 17% NR=3, 9%
No=6, 75% Yes=0, 0% NR=2, 25%
a. What type of cancer were you diagnosed with?
Breast=0, 0% Cervical=2, 67% Other=1, 33% NR=0, 0%
Breast=0, 0%Cervical=0, 0% Other=0, 0% NR=0, 0%
Breast=5, 83%Cervical=0, 0% Other=0, 0% NR=1, 17%
Breast=0, 0% Cervical=0, 0% Other=0, 0% NR=0, 0%
b. Were you treated at a hospital for your cancer?
No=0, 0% Yes=3, 92% NR=0, 0%
No=0, 0%Yes=0, 0% NR=0, 0%
No=0, 0%Yes=4, 67% NR=2, 33%
No=0, 0% Yes=0, 0% NR=0, 0%
c. Did you visit a Samoan healer (Taulasea/Fofo) for your cancer?
No=1, 33% Yes=2, 67% NR=0, 0%
No=0, 0%Yes=0, 0% NR=0, 0%
No=4, 67%Yes=0, 0% NR=2, 33%
No=0, 0% Yes=0, 0% NR=0, 0%
If a friend or family member was told she had breast cancer or cervical cancer what would you advise her to do?
Hospital=71, 84% Samoan Heal=4, 5% Pray=19, 22% Other=7, 8% NR=8, 9%
Hospital=41, 80%Samoan Heal=1, 2% Pray=7, 14% Other=3, 6% NR=8, 17%
Hospital=28, 80%Samoan Heal=3, 9% Pray=12, 34% Other=2, 6% NR=4, 11%
Hospital=4, 50% Samoan Heal=0, 0% Pray=0, 0% Other=1, 13% NR=3, 38%
Have you ever visited a traditional Samoan healer (Taulasea/Fofo) for any personal illness?
No=68, 80% Yes=15, 18% NR=2, 2%
No=39, 76%Yes=12, 24% NR=0, 0%
No=24, 69%Yes=11, 31% NR=0, 0%
No=7, 90% Yes=1, 10% NR=0, 0%
a. What illness did the Taulasea/Fofo treat?
Headache=2, 13% Stomachache=2, 13% *Toala=1, 6% Massage=1, 6% Cancer=1, 6% Flu=1, 6% Cold=1, 6% Hyperthyroid=1, 6% NR=5, 33%
Headache=3, 25%Stomachache=2, 17% Legs=1, 8% Back pain=1, 8% Infertility=1, 8% NR=4, 33%
Headache=1, 9%Stomachache=4, 36% Back pain=2, 18% Cancer=1, 9% Breast=1, 9% NR=2, 18%
NR=1, 100%

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 50
Table 6: Women’s Survey Results Summary continued
Question Ele/Sec Ed (n=66)
2 Yr College(n=64)
≥4 Yr College(n=43)
Have you ever smoked cigarettes?
No=32, 48% Yes, currently=24, 36% Yes, quit=10, 15% NR=0, 0%
No=34, 52%Yes, currently=20, 31% Yes, quit=10, 16% NR=0, 0%
No=21, 49%Yes, currently=11, 26% Yes, quit=11, 26% NR=0, 0%
Have you ever been screened (tested) for cancer?
No=39, 59% Yes=27, 41% NR=0, 0%
No=38, 59%Yes=25, 39% NR=1, 2%
No=17, 40%Yes=26, 60% NR=0, 0%
a. Have you ever had a mammogram?
No=10, 37% Yes=15, 56% NR=2, 7%
No=7, 28%Yes=17, 68% NR=1, 4%
No=15, 58%Yes=10, 38% NR=1, 4%
b. Have you ever done a self‐breast exam?
No=7, 26% Yes=17, 63% NR=3, 11%
No=3, 12%Yes=20, 80% NR=2, 8%
No=5, 19%Yes=21, 81% NR=0, 0%
c. Have you ever had a pap smear?
No=3, 11% Yes=24, 88% NR=0, 0%
No=2, 8%Yes=22, 88% NR=1, 4%
No=4, 15%Yes=21, 81% NR=1, 4%
Have you ever been told you have cancer?
No=60, 91% Yes=1, 2% NR=5, 7%
No=57, 89%Yes=3, 5% NR=4, 6%
No=39, 90%Yes=2, 5% NR=2, 5%
a. What type of cancer were you diagnosed with?
Breast=1, 100% Cervical=0, 0% Other=0, 0% NR=0, 0%
Breast=2, 67%Cervical=1, 33% Other=0, 0% NR=0, 0%
Breast=1, 50%Cervical=0, 0% Other=1, 50% NR=0, 0%
b. Were you treated at a hospital for your cancer?
No=0, 0% Yes=1, 100% NR=0, 0%
No=0, 0%Yes=2, 67% NR=1, 33%
No=0, 0%Yes=2, 100% NR=0, 05
c. Did you visit a Samoan healer (Taulasea/Fofo) for your cancer?
No=1, 100% Yes=0, 0% NR=0, 0%
No=1, 33%Yes=1, 33% NR=1, 33%
No=1, 50%Yes=1, 50% NR=0, 0%
If a friend or family member was told she had breast cancer or cervical cancer what would you advise her to do?
Hospital=52, 79% Samoan Heal=5, 8% Pray=15, 23% Other=4, 6% NR=11, 17%
Hospital=48, 75%Samoan Heal=2, 3% Pray=11, 17% Other=3, 5% NR=9, 14%
Hospital=39, 91%Samoan Heal=1, 2% Pray=11, 26% Other=5, 12% NR=3, 7%
Have you ever visited a traditional Samoan healer (Taulasea/Fofo) for any personal illness?
No=48, 73% Yes=18, 27% NR=0, 0%
No=48, 75%Yes=15, 23% NR=1, 2%
No=36, 84%Yes=6, 14% NR=1, 2%

American Samoa Community Cancer Coalition ‐ Pacific CEED Legacy Project
Survey‐ Women 40 Years and Older The American Samoa Community Cancer Coalition would like you to complete this short survey. Your answers will be used to plan an educational radio program. Please answer all questions. Thank you for your time!
| 51 1) What is your age? 40‐49 50‐59 60‐69 70+ 2) What is your highest level of education? elementary secondary 2 year college 4 year college more than 4 year college
3) Have you ever smoked cigarettes? No, I have never smoked. Yes, I currently smoke. Yes, but I quit smoking.
4) Have you ever been screened (tested) for cancer? No Yes If Yes:
a. Have you ever had a mammogram? No Yes
b. Have you ever done a self‐breast exam? No Yes
c. Have you ever had a pap smear? No Yes
5) Have you ever been told you have cancer? No Yes If Yes:
a. What type of cancer? breast cancer cervical cancer other:________________
Were you treated in a hospital? No Yes
b. Did you visit a Samoan healer (Taulasea/Fofo)? No Yes
6) If a friend or family member was told she had breast cancer or cervical cancer what would advise them to do? get treatment at a hospital get treatment from a Samoan healer pray for better health Other: (please describe)_________________________________________________
7) Have you ever visited a traditional Samoan healer (Taulasea/Fofo) for any personal illness? No Yes If Yes:
a. What illness was treated?______________________________
_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
Amerika Samoa Community Cancer Coalition‐Pacifi CEED Legacy Project
Sailiga‐Tina & Tama’ita’i 40‐70+ Tausaga
O lo’o mana’omia nei e le ofisa o le Amerika Samoa Community Cancer Coalition, ni tagata e auai i le fa’atumuina o le sailigi o lo’o faia nei. Fa’amoemoe o lenei sailigi e fa’amausali ai se polokalama letio mo ni a’oa’oga ta’ua. Fa’amolemole, ia tali uma fesili. Fa’afetai lava, mo lou taimi fa’aavanoaina!
| 52
1. Pe fia tausaga o lou soifua? 40‐49 50‐59 60‐69 70+
2. Po’o le a le maualuga o lau a’oa’oga?
A’oga Tulaga I A’oga Tulaga II Kolisi (2 Tausaga) Kolisi (4 Tausaga) Kolisi 4+
3. Sa e taumafa/ulaula tapa’a mumua? Leai Ioe Ioe, ae ua ou le toe ulaula
4. Na su’esu’eina muamua oe i le fa’ama’i o le kanesa?
Leai Ioe Afai e Ioe:
a. Na fai muamua sau su’ega/fa’aata
o lou susu? Leai Ioe
e. Na fai sau lava su’ega mo lou susu?
Leai Ioe
i. Na fai muamua sau su’ega o le
totoga fanau? Leai Ioe
5. Afai e te silafia o maua sau uõ po’o se isi o lou aiga i le fa’ama’i le kanesa o le susu, o le a sau fautuaga mo ia? saili togafiti i le falema’i saili togafiti i se Taulasea/Fofo Tatalo ina ia manuia O se isi tali ese: (fa’amatala) _________________________________________
6. Sa e saili togafiti muamua i se Taulasea po’o se Fofo samoa? Leai Ioe
Afai e Ioe:
a. O le a le ituaiga gasegase na e saili togafiti e fia maua?
______________________________
_____________________________________________________________________________________________________________________
ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02

Table 7: Western Health Care Professional’s Survey Results Summary Note‐percentages are of the total and are rounded up
Question Females (n=17)
Males (n=30)
Age <20‐39 (n=16)
Age 40‐60+ (n=31)
CAM personally used Diet=14, 80% Prayer=8, 47% Herbal Rem=3, 18% Exercise=14, 82% Massage=9, 53% Support Grp=5, 29% Relax Tech=5, 29% Samoan Heal=3, 18% Other=1, 6% None=1, 6% NR=0, 0%
Diet=24, 80%Prayer=13, 43% Herbal Rem=5, 17% Exercise=25, 83% Massage=9, 30% Support Grp=5, 17% Relax Tech=5, 17% Samoan Heal=6, 20% Other=0, 0% None=3, 10% NR=0, 0%
Diet=15, 94%Prayer=7, 44% Herbal Rem=1, 6% Exercise=14, 88% Massage=5, 31% Support Grp=4, 25% Relax Tech=5, 31% Samoan Heal=3, 19% Other=0, 0% None=1, 6% NR=0, 0%
Diet=23, 74%Prayer=14, 45% Herbal Rem=7, 23% Exercise=25, 81% Massage=13, 42% Support Grp=6, 19% Relax Tech=5, 16% Samoan Heal=6, 19% Other=1, 3% None=3, 10% NR=0, 0%
CAM recommended to patients/others
Diet=14, 82% Prayer=5, 29% Herbal Rem=1, 6% Exercise=13, 77% Massage=6, 35% Support Grp=6, 35% Relax Tech=2, 12% Samoan Heal=2, 12% Other=0, 0% None=1, 6% NR=0, 0%
Diet=24, 80%Prayer=12, 40% Herbal Rem=3, 13% Exercise=25, 83% Massage=11, 37% Support Grp=6, 20% Relax Tech=7, 23% Samoan Heal=6, 20% Other=1, 3% None=1, 3% NR=1, 3%
Diet=14, 88%Prayer=5, 31% Herbal Rem=1, 6% Exercise=13, 81% Massage=7, 44% Support Grp=4, 25% Relax Tech=4, 25% Samoan Heal=2, 13% Other=0, 0% None=1, 6% NR=1
Diet=24, 77%Prayer=12, 39% Herbal Rem=4, 13% Exercise=25, 81% Massage=10, 32% Support Grp=8, 26% Relax Tech=5, 16% Samoan Heal=6, 19% Other=0, 0% None=2, 6% NR=0, 0%
Asked patient if using Samoan healing
No=2, 12% Yes=15, 88% NR=0, 0%
No=3, 10%Yes=27, 90% NR=0, 0%
No=0, 0%Yes=16, 100% NR=0, 0%
No=5, 16% Yes=26, 84% NR=0, 0%
Told by patient was using Samoan healing
No=1, 6% Yes=16, 94% NR=0, 0%
No=1, 3%Yes=29, 97% NR=0, 0%
No=1, 6%Yes=15, 94% NR=0, 0%
No=1, 3% Yes=30, 97% NR=0, 0%
Advised patient to stop using Samoan healing
No=3, 18% Yes=14, 82% NR=0, 0%
No=9, 30%Yes=20, 67% NR=1, 3%
No=2, 12%Yes=14, 88% NR=0, 0%
No=10, 32% Yes=20, 65% NR=1, 3%
Aware of BCC patient using Samoan healing methods as complementary medicine
No=10, 59% Yes=7, 41% NR=0, 0%
No=11, 37%Yes=19, 63% NR=0, 0%
No=11, 69%Yes=5, 31% NR=0, 0%
No=10, 32% Yes=21, 68% NR=0, 0%
Aware of BCC patient using Samoan healing methods as alternative medicine
No=11, 65% Yes=6, 35% NR=0, 0%
No=10, 33%Yes=20, 66% NR=0, 0%
No=11, 69%Yes=5, 31% NR=0, 0%
No=10, 32% Yes=21, 68% NR=0, 0%
Most AS patients’ usual use of Samoan healing methods
Comp=12, 70% Altn=3, 18% Both=2, 12% NR=0, 0%
Comp=22, 73%Altn=5, 17% Both=3, 10% NR=0, 0%
Comp=13, 81%Altn=3, 19% Both=0, 0% NR=0, 0%
Comp=21, 68%Altn=5, 16% Both=5, 16% NR=0, 0%
Health outcome of Samoan healing
Harm=7, 41% Harm‐No Effect=1, 6% No Effect=2, 12% Help=4, 24% Harm & Help=2, 12% NR=1, 6%
Harm=10, 33%Harm‐No Effect=1, 3% No Effect=5, 17% Help=10, 33% Harm & Help=1, 3% NR=3, 10%
Harm=6, 38%Harm‐No Effect=0, 0% No Effect=3, 19% Help=5, 31% Harm & Help=1, 6% NR=1, 6%
Harm=11, 36%Harm‐No Effect=2, 7% No Effect=4, 13% Help=9, 29% Harm & Help=2, 7% NR=3, 10%
Interested in learning more about Samoan healing methods
No=4, 24% Yes=13, 76% NR=0, 0%
No=10, 33%Yes=20, 66% NR=0, 0%
No=3, 19%Yes=13, 81% NR=0, 0%
No=11, 36% Yes=20, 64% NR=0, 0%
_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 53

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 54
Table 7: Western Health Care Professional’s Survey Results Summary continued
Question Samoan (n=22)
Asian (n=10)
Caucasian (n=12)
CAM personally used Diet=16, 73%Prayer=12, 55% Herbal Rem=6, 27% Exercise=17, 77% Massage=9, 41% Support Grp=4, 18% Relax Tech=3, 14% Samoan Heal=6, 27% Other=0, 0% None=2, 9% NR=0, 0%
Diet=9, 90%Prayer=4, 40% Herbal Rem=1, 10% Exercise=10, 100% Massage=2, 20% Support Grp=2, 20% Relax Tech=1, 10% Samoan Heal=0, 0% Other=0, 0% None=0, 0% NR=1, 10%
Diet=11, 92% Prayer=3, 25% Herbal Rem=1, 8% Exercise=10, 83% Massage=5, 42% Support Grp=4, 33% Relax Tech=5, 42% Samoan Heal=2, 17% Other=1, 8% None=1, 8% NR=0, 0%
CAM recommended to patients/others Diet=15, 68%Prayer=9, 41% Herbal Rem=4, 18% Exercise=14, 64% Massage=7,32% Support Grp=4, 18% Relax Tech=3, 14% Samoan Heal=7, 32% Other=0, 0% None=2, 9% NR=1, 5%
Diet=9, 90%Prayer=3, 30% Herbal Rem=1, 10% Exercise=9, 90% Massage=3, 30% Support Grp.=4, 40% Relax Tech=2, 20% Samoan Heal=0, 0% Other=0, 0% None=0, 0% NR=0, 0%
Diet=11, 92% Prayer=5, 42% Herbal Rem=0, 0% Exercise=12, 100% Massage=6, 50% Support Grp=3, 25% Relax Tech=3, 25% Samoan Heal=1, 8% Other=0, 0% None=0, 0% NR=0, 0%
Asked patient if using Samoan healing No=1, 4%Yes=21, 96% NR=0, 0%
No=1, 10%Yes=9, 90% NR=0, 0%
No=1, 85 Yes=11, 92% NR=0, 0%
Told by patient was using Samoan healing
No=1, 4%Yes=21, 96% NR=0, 0%
No=1, 10%Yes=9, 90% NR=0, 0%
No=12, 100% Yes=0, 0% NR=0, 0%
Advised patient to stop using Samoan healing
No=2, 9%Yes=19, 86% NR=1, 5%
No=3, 30%Yes=7, 70% NR=0, 0%
No=5, 42% Yes=7, 58% NR=0, 0%
Aware of BCC patient using Samoan healing methods as complementary medicine
No=8, 36%Yes=14, 64% NR=0, 0%
No=3, 30%Yes=7, 70% NR=0, 0%
No=9, 75% Yes=3, 25% NR=0, 0%
Aware of BCC patient using Samoan healing methods as alternative medicine
No=10, 45%Yes=12, 55% NR=0, 0%
No=3, 30%Yes=7, 70% NR=0, 0%
No=7, 58% Yes=5, 42% NR=0, 0%
Most AS patients’ usual use of Samoan healing methods
Comp=16, 73%Altn=4, 18% Both=2, 9% NR=0, 0%
Comp= 7, 70%Altn=1, 10% Both=2, 20% NR=0, 0%
Comp=8, 67% Altn=3, 25% Both=1, 8% NR=0, 0%
Health outcome of Samoan healing Harm=8, 36%Harm‐No Effect=2, 9% No Effect=3, 14% Help=5, 23% Harm & Help=2, 9% NR=2, 9%
Harm=4, 40%Harm‐No Effect=0, 0% No Effect=3, 30% Help=3, 30% Harm & Help=0, 0% NR=0, 0%
Harm=4, 33% Harm‐No Effect=0,0% No Effect=1, 8% Help=4, 33% Harm & Help=1, 8% NR=2, 17%
Interested in learning more about Samoan healing methods
No=8, 36%Yes=14, 64% NR=0, 05
No=4, 40%Yes=6, 60% NR=0, 0%
No=0, 0% Yes=12, 100% NR=0, 0%
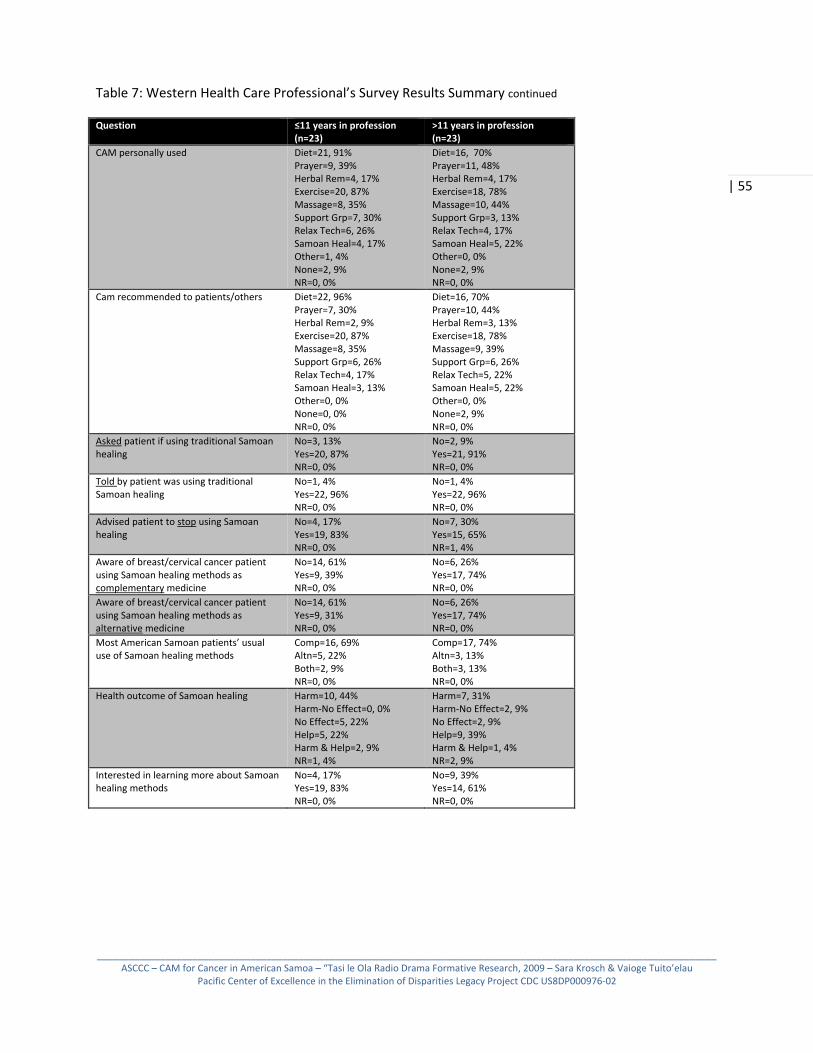
_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 55
Table 7: Western Health Care Professional’s Survey Results Summary continued
Question ≤11 years in profession (n=23)
>11 years in profession (n=23)
CAM personally used Diet=21, 91%Prayer=9, 39% Herbal Rem=4, 17% Exercise=20, 87% Massage=8, 35% Support Grp=7, 30% Relax Tech=6, 26% Samoan Heal=4, 17% Other=1, 4% None=2, 9% NR=0, 0%
Diet=16, 70%Prayer=11, 48% Herbal Rem=4, 17% Exercise=18, 78% Massage=10, 44% Support Grp=3, 13% Relax Tech=4, 17% Samoan Heal=5, 22% Other=0, 0% None=2, 9% NR=0, 0%
Cam recommended to patients/others Diet=22, 96%Prayer=7, 30% Herbal Rem=2, 9% Exercise=20, 87% Massage=8, 35% Support Grp=6, 26% Relax Tech=4, 17% Samoan Heal=3, 13% Other=0, 0% None=0, 0% NR=0, 0%
Diet=16, 70%Prayer=10, 44% Herbal Rem=3, 13% Exercise=18, 78% Massage=9, 39% Support Grp=6, 26% Relax Tech=5, 22% Samoan Heal=5, 22% Other=0, 0% None=2, 9% NR=0, 0%
Asked patient if using traditional Samoan healing
No=3, 13%Yes=20, 87% NR=0, 0%
No=2, 9%Yes=21, 91% NR=0, 0%
Told by patient was using traditional Samoan healing
No=1, 4%Yes=22, 96% NR=0, 0%
No=1, 4%Yes=22, 96% NR=0, 0%
Advised patient to stop using Samoan healing
No=4, 17%Yes=19, 83% NR=0, 0%
No=7, 30%Yes=15, 65% NR=1, 4%
Aware of breast/cervical cancer patient using Samoan healing methods as complementary medicine
No=14, 61%Yes=9, 39% NR=0, 0%
No=6, 26%Yes=17, 74% NR=0, 0%
Aware of breast/cervical cancer patient using Samoan healing methods as alternative medicine
No=14, 61%Yes=9, 31% NR=0, 0%
No=6, 26%Yes=17, 74% NR=0, 0%
Most American Samoan patients’ usual use of Samoan healing methods
Comp=16, 69%Altn=5, 22% Both=2, 9% NR=0, 0%
Comp=17, 74%Altn=3, 13% Both=3, 13% NR=0, 0%
Health outcome of Samoan healing Harm=10, 44%Harm‐No Effect=0, 0% No Effect=5, 22% Help=5, 22% Harm & Help=2, 9% NR=1, 4%
Harm=7, 31%Harm‐No Effect=2, 9% No Effect=2, 9% Help=9, 39% Harm & Help=1, 4% NR=2, 9%
Interested in learning more about Samoan healing methods
No=4, 17%Yes=19, 83% NR=0, 0%
No=9, 39%Yes=14, 61% NR=0, 0%

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 56
American Samoa Community Cancer Coalition ‐ Pacific CEED Legacy Project Survey‐ Western Health Care Professionals
The American Samoa Community Cancer Coalition (ASCCC) received funding from The Pacific Center of Excellence in the Elimination of Disparities (Pacific‐CEED) for a two‐part project: 1) to explore the use of alternative and complementary medicines used by patients in American Samoa, and 2) to communicate research findings via a radio serial drama targeting women ages 40 and older at risk for breast and cervical cancer. As part of our research, the ASCCC would like you to complete this short survey. Your insights are important to us so please answer all questions. Thank you for your time!
1) What is your gender? female male
2) What is your age? under 20 20‐29 30‐39 40‐49 50‐59 60+
2) What is your ethnicity? (Check all that apply) Samoan Other Pacific Islander Asian White/Caucasian Other: (please specify)____________________________________________
3) How long have you been working in the Western medical field? __________years 4) What is your current position/job? medical doctor specialist: (please specify)____________________________ medical officer other: (please specify)_______________________________ nurse
5) How many female patients age 40 or older do you come in contact with per week? less than 10 10‐29 30‐49 50 or more
6) Aside from mainstream Western medical treatments, which of the following complementary methods have you personally used to treat an illness or alleviate symptoms? (Check all that apply) diet modification exercise relaxation techniques (meditation, yoga) prayer massage traditional healing (Samoan Taulasea/ Fofo) herbal remedies (plants) support groups None of the above other: (describe)______________________________________________________________

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 57
7) Which of the following complementary methods have you recommended to a patient to treat an illness or alleviate symptoms? (Check all that apply) diet modification exercise relaxation techniques (meditation, yoga) prayer massage traditional healing (Samoan Taulasea/Fofo) herbal remedies (plants) support groups None of the above other: (describe) ______________________________________________________________
8) Have you ever asked a patient if she/he is using traditional Samoan healing methods to treat an illness or symptoms? Yes No
9) Has a patient ever told you she/he is using traditional Samoan healing methods to treat an illness or symptoms? Yes No
10) Have you ever advised a patient to stop using traditional Samoan healing methods? Yes No
11) Are you aware of any breast cancer or cervical cancer patients who have used traditional Samoan healing methods along with (at the same time as) Western medical treatment? Yes No
12) Are you aware of any breast cancer or cervical cancer patients who have used traditional Samoan healing methods in place of (instead of) Western medical treatment? Yes No
13) In my opinion, patients in American Samoa most often use traditional Samoan healing practices along with Western medical treatment (complementary medicine). in place of Western medical treatment (alternative medicine).
14) In my opinion, traditional Samoan healing practices usually have a harmful effect on a patient’s quality of life. no effect on a patient’s quality of life. a helpful effect on a patient’s quality of life.
15) Are you interested in learning more about traditional Samoan healing methods? Yes No

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 58
Works Cited
Abraido‐Lanza, Ana et al. (2004) Breast and Cervical Cancer Screening Among Latinas and Non‐Latina Whites. American Journal of Public Health. 94(8):1393‐1398.
Aitaoto, Nia, et al. (2007) Cultural Considerations in Developing Church‐based Programs to Reduce Cancer Health Disparities Among Samoans. Ethnicity and Health. 12(4):381‐400.
American Samoa Office of the Governor (ASOG). (2007) Territory of American Samoa Coverage for All American Samoa: Policy Leadership Group Recommendations to Fono.
Asian and Pacific Islander American Health Forum (APIAHF). (2006) Health Brief: Samoans in the United States.
Astin, John, A. (1998) Why Patients Use Alternative Medicine: Results of a National Study. Journal of the American Medical Association. 279(19):1548‐1553.
Byles JE , et al. (1994) Effectiveness of three community based strategies to promote screening for cervical cancer. Journal of Medical Screening. 1(3):150‐8.
Cassileth, Barrie. 1999. ‘Complementary’ or ‘alternative’? It makes a difference in cancer care. Complementary Therapies in Medicine. 7:35‐37.
Cassileth, Barrie and Christopher C. Chapman. (1996). Alternative and Complementary Cancer Therapies. Cancer. 4: 1026‐1034.
Census Data 2000 for American Samoa. (2001) United States Census Bureau.
www.census.gov/census2000/Americansamoa.html
Hether, Heather, et al. (2008) Entertainment‐Education in a media‐saturated Environment: Examining the Impact of Single and Multiple Exposures to Breast Cancer Storylines on Two Popular Medical Dramas. Journal of Health Communication. 13:808‐823.
Hubbell, FA, et al. (2005). Exploring beliefs about cancer among American Samoans: focus group findings. Cancer Detection and Prevention. 29:109‐115.
Hutchinson P, et al. (2006) Measuring the cost‐effectiveness of a national health communication program in rural Bangladesh. Journal of Health Communication. 11 (Supplement 2):91‐121.
Ishida, Dianne, et al. (2001) Beliefs and Attitudes of Samoan Women toward Early Detection of Breast cancer and Mammography Utilization. Cancer. 91(1):262‐6
Jump, et al. (1998) Physicians’ Attitudes toward Complementary and Alternative Medicine. Integrative Medicine. 1(4):149‐153.

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 59
Krosch, Sara. (2008) Cancer Prevention Billboard Evaluation Report – December 2008. American Samoa Community Cancer Network.
Krosch, Sara. (2008) Prostate Cancer Screening Clinic Program Impact Evaluation. American Samoa Community Cancer Network.
Krosch, Sara. (2009) Target Audience Analysis: Media Habits and Preferences. American Samoa Community Cancer Network.
Lee, GBW, et al. (2004) Complementary and alternative medicine use in patients with chronic diseases in primary care is associated with perceived quality of care and cultural beliefs. Family Practice. 21(6): 554‐560.
Levy‐Storms, Lene and Steven P. Wallace. (2003) Use of mammography screening among older Samoan women in Los Angeles County: a diffusion network approach. Social Science & Medicine. 57: 987‐1000.
Lovell CC, et al. (2007‐08) "One Day I Might Find Myself HIV‐Positive Like Her": Audience Involvement and Identification with Role Models in an Entertainment‐Education Radio Drama in Botswana. International Quarterly of Community Health Education. 28(3):181‐200.
MacPherson, Cluny and La’avasa MacPherson. (1990) Samoan Medical Belief and Practice. Auckland University Press.
Mandelblatt JS, et al. (1999) Breast and cervix cancer screening among multiethnic women: role of age, health, and source of care. Preventative Medicine. 28:418–425. Mao, J J, et al. (2007). Use of Complementary and alternative medicine and prayer among a national sample of cancer survivors compared to other populations without cancer. Complementary Therapies in Medicine. 15:21‐29.
Mayo Clinic (MayoClinic.com). (2008) Breast Cancer. Accessed on August 14, 2008. www.mayoclinic.com/health/breast‐cancer/DS00328
Mayo Clinic (MayoClinic.com). (2008) Cervical Cancer. Accessed on August 14, 2008. www.mayoclinic.com/health/cervical‐cancer/DS00167
McMullin, J M et al. 2008. Tongan Perceptions of Cancer. Cancer Detection and Prevention. 32S:S29‐S36.
Miller, Barry A, et al. (2007) Cancer incidence and mortality patterns among specific Asian and Pacific Islander populations in the US. Cancer Causes Control. Springer online.
Mishra, SI, et al. (1997). Cancer Control Needs Among Native American Samoans: Results from American Samoa, Hawaii and Los Angeles. Irvine California: University of California‐Irvine.
Mishra, SI, et al. (2001). Breast Cancer Screening among American Samoan Women. Prevention Medicine. 33:9‐17.

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 60
Mishra, SI et al. (2003) Predictors of Indigenous healer use among Samoans. Alternative Therapies in Health and Medicine. 9(6):64‐69.
Mishra, SI, et al. (2007) Results of a randomized Trial to Increase Mammogram Usage among Samoan Women. Cancer Epidemiological Biomarkers Prevention. 16(12):2594‐ 2604.
Mohammed S. (2001) Personal communication networks and the effects of an entertainment‐ education radio soap opera in Tanzania. Journal of Health Communication. 6(2):137‐54.
National Breast and Cervical Cancer Early Detection Screening Program Summaries—American Samoa (CDC‐NBCCEDP). 2007. Centers for Disease Control (CDC). www.cdc.gov
National Cancer institute (NCI). (2005) Thinking About Complementary and Alternative Medicine. (brochure)
Pappas‐DeLuca KA, et al. (2008) Entertainment‐education radio serial drama and outcomes related to HIV testing in Botswana. AIDS Education and Prevention. 20(6):486‐503.
Patterson, Michael, et al. (2008) A novel clinical‐trial design for the study of massage therapy. Complementary Therapies in Medicine. 16:169‐176.
Porter, Matthew, et al. (2008) Changing patterns of CAM use among prostate cancer patients two years after diagnosis: Reasons for maintenance or discontinuation. Complementary Therapies in Medicine. (In Press)
Pu, CY, et al., (2008) The determinants of traditional Chinese medicine and acupuncture utilization for cancer patients with simultaneous conventional treatment. European Journal of Cancer Care. 17(4): 340‐349.
Puaina, Seumaninoa, et al. (2008) Impact of traditional Samoan lifestyle (fa’aSamoa) on cancer screening practices. Cancer Detection and Prevention. 32S:S23‐S28.
Risi, l, et al. (2004) Media interventions to increase cervical screening uptake in South Africa: an evaluation study of effectiveness. Health Education Resources. 19(4):457‐68.
Robinson, Steven, et al. (2002) Ethnic Differences in Survival among Pacific Island Patients Diagnosed with Cervical Cancer. Gynecologic Oncology. 84:303‐308.
Rogers EM, et al. (1999) Effects of an entertainment‐education radio soap opera on family planning behavior in Tanzania. Studies in Family Planning. 30(3):193‐211.
Samoan Observer. (2003) Apia, Samoa. July, 20.
Sebert Kuhlmann, AK. (2008) Radio role models for the prevention of mother‐to‐child transmission of HIV and HIV testing among pregnant women in Botswana. Health Promotion International. 23(3):260‐8.

_____________________________________________________________________________________________________________________ASCCC – CAM for Cancer in American Samoa – “Tasi le Ola Radio Drama Formative Research, 2009 – Sara Krosch & Vaioge Tuito’elau
Pacific Center of Excellence in the Elimination of Disparities Legacy Project CDC US8DP000976‐02
| 61
Skirble, Rosanne. (2004) Radio Drama Makes Waves in Pacific. Voice of America News. December 14.
Swisher, Elizabeth, et al. (2002) Use of Complementary and Alternative Medicine among Women with Gynecological Cancers. Gynecologic Oncology. 84:363‐367.
Taylor, T.N. et al. (2008) HIV/AIDS‐specific quality of life change in Zimbabwean patients. Journal of Acquired Immune Deficiency Syndrome. 49: 552‐53. United States Department of health and Human Services Preventative Services Task Force (USDHHS‐USPSTF). (2007) The Guide to Clinical Preventative Services 2007: Recommendations of the US Preventative Services Task Force.
Vaughan PW and EM Rogers. (2000) A staged model of communication effects: evidence from an entertainment‐education radio soap opera in Tanzania. Journal of Health Communication. 5(3):203‐27.
Whistler, Arthur. (1995) Samoan Herbal Medicine – O La’au ma Vai Fofo o Samoa. Swedish Nature Society. Samoa.
Wray RJ, et al. (2004) Preventing domestic violence in the African American community: assessing the impact of a dramatic radio serial. Journal of Health Communication. 9(1):31‐52.