cahpo 2016. workshop 3: gill dawes and catherine ashworth
TRANSCRIPT

Service Redesign:Integration of Community Occupational Therapy and Physiotherapy

• Separate community Occupational Therapy & Physiotherapy teams
• Variation in therapy provision across community teams
• Services provided in professional silos
• Community therapy services not seen any progressive funding over several years
• Waiting lists – demand outstripping capacity
• Adversity promotes creative thinking & transformational change
Set The Scene

• 5 Year Plan
• Ageing Population
• Changes in the configuration & delivery of Intermediate Care across the health economy, specifically Reablement with Therapy
• Commissioners vision
Improving care for patients was at the heart of the change
Other Drivers For Service Redesign

Our VisionPrevention agenda
Reduce admissions
to hospital & care
Extend accessibility &
responsiveness
Support early
discharge
Playing a key role in
management of long term conditions
Reduce duplication
Locality based
workingFormalise
case management
approach
Ensure right care right time right place
Support whole system approach to
keep patient in environment of
choice
Remove professional barriers and put
patients needs at the centre
Equitable access with self referral Be able to
measure impact of intervention to
inform future commissioning
Integrated therapy roles

• To become a Community Integrated therapy service, demonstrating multidisciplinary working, across 5 localities
• To provide a detailed holistic assessment and deliver a personalised treatment plan based on patients needs and goals
• To work in partnership with family, carers and other professionals
• To help people stay independent and maximise their well-being
• Help to prevent unnecessary hospital admissions and support early, safe discharge
Aims of Service

• November 2011 Business Case for Reablement funding to facilitate the expansion in reablement services in social care
• Community therapies targeted as the services cut across all elements within the Intermediate Care Pathway
• Initial services considered for integration were Occupational Therapy and Physiotherapy with robust links to Speech & Language Therapy & Dietetics
• Workforce analysis identified the need to increase our baseline capacity, ability to work across professions and reduce duplication
• Intensive recruitment of qualified, non-qualified and administration staff to enable service redesign following the Occupational Therapy footprint of 5 localities
Methods & Approach

• Development of new roles within therapy services – Assistant Practitioner - Integrated Therapy Technicians
• Staff engagement• Estates• Systems
• Integrated referral• Integrated triage• Triage matrix• Joint documentation• Admin allocation to increase productivity
Methods & Approach

• Integrated skills training
• Caseload weighting
• Implementation of extended hours & 7 day working
• Evaluation
Methods & Approach
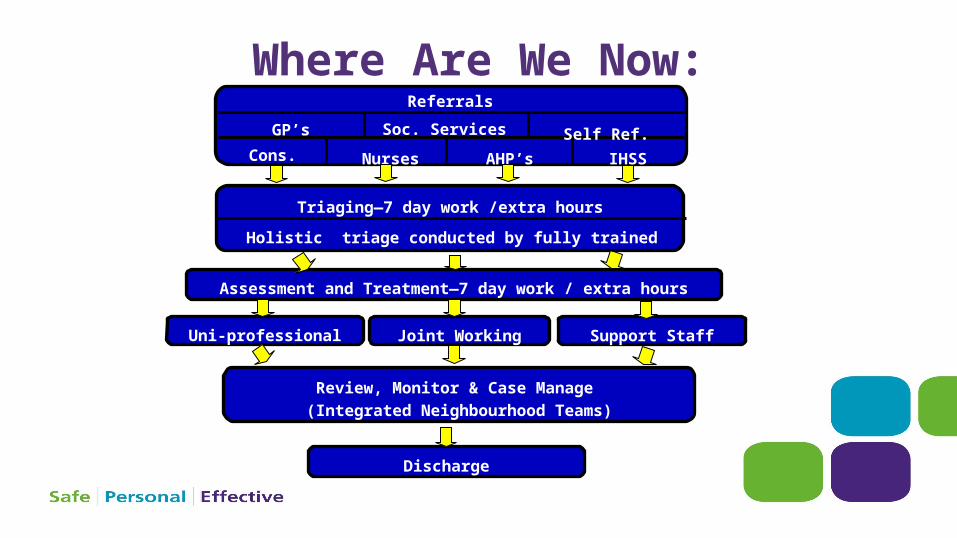
Where Are We Now: Referrals
GP’s Soc. Services Self Ref.Cons. Nurses AHP’s IHSS
Triaging—7 day work /extra hours
Holistic triage conducted by fully trained Physio’s or OT’s
Uni-professional Joint Working Support Staff
Assessment and Treatment—7 day work / extra hours
Review, Monitor & Case Manage (Integrated Neighbourhood Teams)
Discharge

• Impact Recording
• Patient Stories
• Clinical Outcome measures
• Staff evaluation
• Extended hours & weekend working review
Evaluation

Benefits to Integration
Time management
Increases baseline capacity and
patient facing time Integrated student training
Integrated competencies,
training, enhanced learning, skill sharing
AP role development
More responsive
service
Increased productivity
Improved patient
experience
Driven integration across the
organisation

• Strong leadership at all levels
• Foster a positive attitude to change
• Empower & engage the whole staff group to make changes
• Co-location is fundamental to success
• Continually acknowledge with staff successes
• Allow time to embed service developments
Key Learning Points

Timeline of Integration2011 2015201420132012 2016
• Business Case Reablement Funding
• Recruitment• Integrated Triage• Joint waiting list
validation• Created 5 community
Physio teams, in line with OT structure
• Inaugural Integrated Therapies Away Day (3 monthly)
• Recruitment of OT’s, Physios, Assistant Practitioners & Admin
• Estates process commenced
• Consultation re locality base
• Co-location of 9 existing teams into 5 locality base teams
• Impact recording commenced
• Hyndburn co-located (Oct)
• Ribble Valley co-located (Oct)
• Pendle co-located (Dec)
• Impact Recording continues
• Burnley co-located (June)
• Joint Documentation Working Party
• Rossendale co-located (Dec)
• Consultation for 7 day work & extended hours (Jan)
• Commenced 7 day work & extended hours (April)
• Pilot Caseload weighting (April)
• Pilot risk matrix for ITT referrals
• Development of Integrated Neighbourhood Teams (June)
• Establishment of Intensive Home Support Service (Nov)
• Integrated Long Term Condition Reviews
• Review of weekend working & extended hours
• EMIS• Role out Caseload
weighting• Role out of risk
matrix for ITT referrals
• Evaluation of new roles & services

• Embed the case management approach within the Integrated Neighbourhood Teams
• Continue to evaluate newly established roles; Integrated Neighbourhood Team co-ordinators, Assistant Practitioners & Integrated Therapy Technicians
• Marketing community therapy services
• Identify & implement appropriate evaluation tools to look at productivity, staff, patient & stakeholder evaluation
• Continue to respond flexibly to service needs and outcome of evaluation
The Future

What our patients say
· “Thank you for a speedy, caring and efficient service”
· “Had visit on Sunday & several visits on Monday including in the evening, to provide equipment and ensure the patient was safe with transfers & toileting. Highly commended the staff for the marvellous service they received”
• “Having recently needed help from physio I am very satisfied with all the help I received and also from the OT lady, these 2 people have worked together to make my physical needs much easier. Thank you for the service. First class!”

· “Joint working has increased productivity and improved practice by removing barriers to communication and co-operation”
· “Support staff have a wide range of skills, allowing them to deliver multiple interventions in a single visit.”
· “Joint OT and PT sessions reduce duplication and encourage clinical reasoning discussions”
What our Staff say

Catherine AshworthClinical Co-ordinator for Pendle Integrated Neighbourhood TeamAdvanced occupational [email protected] 01282 804998
Gill DawesAdvanced Physiotherapist / Team LeaderRibble Valley Community Integrated Therapy [email protected] 01200 449037
Contact Details