c u s t o m e r d r i v e n. b u s i n e s s m i n d e d. 1 bureau of health systems joint provider...
TRANSCRIPT

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D. 1
Bureau of Health Systems
Joint Provider Surveyor Training
Mike Pemble, DirectorApril 10, 2012

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D. 2
Health Systems
License, certify and/or regulate facilities: 440 Nursing Homes equaling 46,890 licensed beds* 175 Hospitals equaling 26,397 licensed beds* 12 Psychiatric Hospitals / 48 Psychiatric Units within Hospitals* 26 Psychiatric Partial Hospitalization Programs* 9 Organ Transplant Facilities 662 Home Health Agencies 110 Hospice Programs and 21 Hospice Residences* 170 End Stage Renal Disease (Dialysis) 150 Rural Health Clinics 120 Freestanding Surgical Outpatient Facilities/Ambulatory Surgical Centers* 15 Comprehensive Outpatient Rehabilitation Facilities 11 Portable X-Ray Facilities 196 Outpatient Physical Therapy/Speech Pathology 7,659 Laboratories* (not licensed since 1992) 10,063 Radiation Machine Sites
*Licensed

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D. 3
LEGISLATIVE REPORT Michigan Legislature Requests Report: How will the Bureau of
Health Systems Become Self Sufficient?
Public Act 63 of 2011, Article XII, Section 731: (1) The Bureau of Health Systems shall prepare a report detailing the number of facilities,
locations, and beds for each type of health facility licensed, certified, inspected, or otherwise regulated by the bureau. The report shall also include the bureau’s cost to license, certify, inspect, or otherwise regulate each type of facility. The data required by this subsection shall be collected and reported on acute care hospitals, home health agencies, hospices, hospice residences, psychiatric units in general hospitals, psychiatric hospitals, partial hospitalization psychiatric programs, outpatient surgical facilities, laboratories, end stage renal disease facilities, rural health clinics, substance abuse programs, long-term care facilities including nursing homes, hospital long-term care units, county medical care facilities, and radiation machines.
(2) By February 1, the Bureau of Health Systems shall work with interested stakeholders to recommend to the governor and the legislature a schedule of fees to be charged by the bureau for regulating health facilities. The fee schedule proposed by the bureau shall bear a direct relationship to the cost of the service or act, including overhead expenses. The report shall also recommend the necessary statutory and administrative rule changes necessary to implement the recommended fee schedule.

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D. 4
Stakeholder Input Summary
• Electronic survey of stakeholders was sent to over 1,000 entities including affected licensed provider types and consumer groups
• Survey resulted in 302 responses; 282 licensed provider responses (93%), 12 non-licensed responders (4%), 8 responders did not self-identify
• 93% indicate importance of issuing a license within 90 days• 97% indicate importance of timely revisits after deficient practice is sited • 85% want timeliness and effectiveness of licensing process improved• 35% believe that care and treatment generally better when inspections are
performed• 92% believe BHS should respond timely to citizen complaints against providers• 49% believe fees should support cost of licensing activities• 37% would support reasonable license fee increase• 45% of responders would not actively oppose a license fee increase• 91% of responders indicate that any funding generated from a license fee increase
should be restricted to supporting only licensing functions
C U S T O M E R D R I V E N. B U S I N E S S M I N D E D. 5
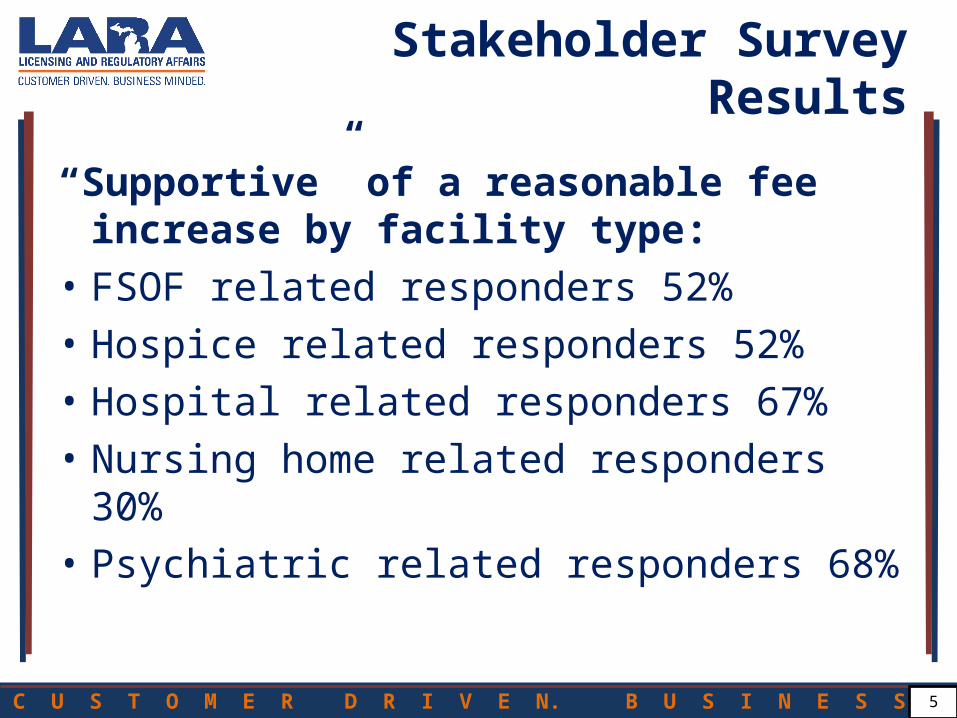
Stakeholder Survey Results
“Supportive” of a reasonable fee increase by facility type:
• FSOF related responders 52%• Hospice related responders 52%• Hospital related responders 67%• Nursing home related responders 30%• Psychiatric related responders 68%

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• We know licensees want:– Quick report – the clock on fines starts ticking the
day we exit from an inspection.– Quick review – a timely response with quality
feedback from qualified BHS staff.– Quick revisit – all stakeholders want the facility to
be in compliance ASAP to protect residents, avoid penalties and accept new admissions.
Better Customer Service
6

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D. 7
Health Systems
The Role of Effective Regulation in Job Creation The number one concern for new providers interested in building new health
facilities in Michigan is whether they will receive a timely initial licensing and certification survey once construction is complete.
A new facility creates construction jobs and ongoing jobs to run the facility. BHS licensing and certification inspections verify compliance with licensing
requirements and Medicare and Medicaid conditions of participation to secure funding that reimburses the facility for the delivery of care.
Initial Medicare/Medicaid Certification Surveys are completed by BHS in accordance with the priorities set by the federal Department of Health and Human Services, Centers for Medicare/Medicaid Services, the authority having jurisdiction.
Adequate State funding can assure completion of all State and federal survey activity to make Michigan an attractive location to establish new facilities.
Inadequate State funding results in failure to complete required inspections. In turn, CMS may deny or delay certification of new providers in the State.

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
We are facing a perfect storm:•Nursing Home complaints increasing•Increased reporting requirements•No additional staff•30 years: No license fee increases•Past 10 years: General funding cuts, unpaid furlough days, hiring freezes, early retirement incentives•The overall cost and number of staff necessary to regulate nursing homes has increased annually (insurance, travel, retirement, office space, etc.)
Bureau of Health Systems
8

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D. 9
Health SystemsGetting the most from its resources:
Eliminated long standing backlog of nursing home complaint investigations
Innovative nurse recruitment techniques assist in filling health care surveyor vacancies
Improved coordination and efficiencies in the inspection process
Improved communication with provider community
Biannual joint training for providers and surveyors huge success
BHS meeting all LARA departmental dashboard performance requirements
91% Survey Reports issued within 10 days in FY12 (up from 85%)
Significant progress made on program to allow electronic submissions of Plans of Correction
C U S T O M E R D R I V E N. B U S I N E S S M I N D E D. 10
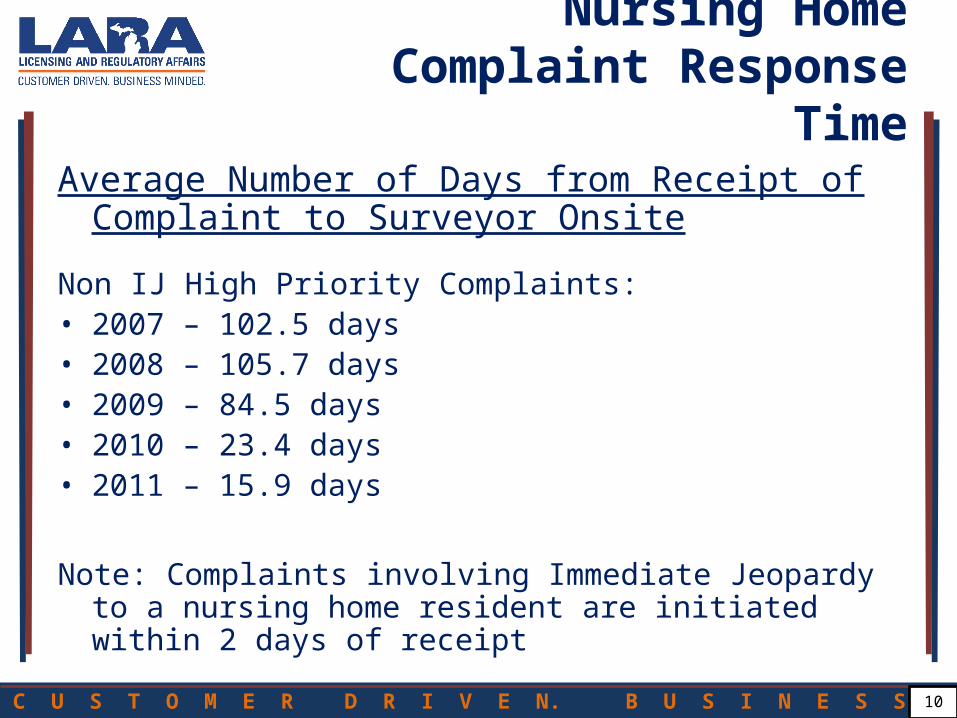
Nursing HomeComplaint Response Time
Average Number of Days from Receipt of Complaint to Surveyor Onsite
Non IJ High Priority Complaints:• 2007 – 102.5 days• 2008 – 105.7 days• 2009 – 84.5 days• 2010 – 23.4 days• 2011 – 15.9 days
Note: Complaints involving Immediate Jeopardy to a nursing home resident are initiated within 2 days of receipt

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D. 11
Complaints:
Protecting Our Most Vulnerable Citizens
90% of the complaints the Bureau of Health Systems receives are
related to nursing homes

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D. 12
1092
274
1139
1031
1104
5135
1260
3646
1285
5644
1257
5063
1295
4443
1441
4571
629
2658
1510
6379
0
1000
2000
3000
4000
5000
6000
7000
FY 2004 FY 2005 FY 2006 FY 2007 FY 2008 FY 2009 FY 2010 FY 2011 FY2012 1st 5-
months
FY2012
Projected
Complaints
FRIs
Nursing Home Citizen Complaints and Facility Reported Incidents (FRIs)
• Facility Reported Incidents (FRI’s) of alleged abuse, neglect, misappropriation of resident property, and injuries of an unknown (suspicious) origin are projected to increase 40% based on 1st 5-months FY12 actual data.
• FY12 Citizen Complaints are projected to increase another 5% based on 1st 5-months actual data.• Citizen Complaints increased 11% in FY11.
C U S T O M E R D R I V E N. B U S I N E S S M I N D E D. 13
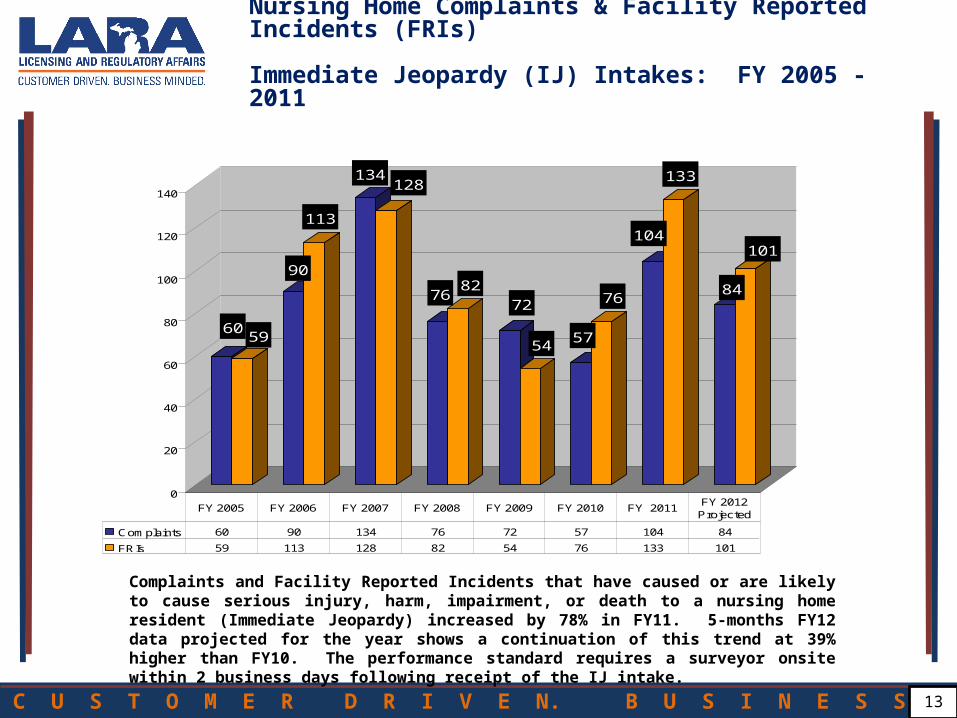
Nursing Home Complaints & Facility Reported Incidents (FRIs) Immediate Jeopardy (IJ) Intakes: FY 2005 - 2011
6059
90
113
134128
7682
72
5457
76
104
133
84
101
0
20
40
60
80
100
120
140
Complaints 60 90 134 76 72 57 104 84
FRIs 59 113 128 82 54 76 133 101
FY 2005 FY 2006 FY 2007 FY 2008 FY 2009 FY 2010 FY 2011FY 2012 Projected
Complaints and Facility Reported Incidents that have caused or are likely to cause serious injury, harm, impairment, or death to a nursing home resident (Immediate Jeopardy) increased by 78% in FY11. 5-months FY12 data projected for the year shows a continuation of this trend at 39% higher than FY10. The performance standard requires a surveyor onsite within 2 business days following receipt of the IJ intake.

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D. 14
Nursing Home Complaints & Facility Reported Incidents (FRIs) Harm Level Non-IJ High Intakes FY 2005 - 2011
843
665
829761
949
720
10511206
1063
841
1174
1092
1274
1928
1275
2885
0
500
1000
1500
2000
2500
3000
Complaints 843 829 949 1051 1063 1174 1274 1275
FRIs 665 761 720 1206 841 1092 1928 2885
FY 2005 FY 2006 FY 2007 FY 2008 FY 2009 FY 2010 FY 2011FY 2012 Projected
Complaints and Facility Reported Incidents that have alleged harm to a nursing home resident, but no Immediate Jeopardy, increased by 41% in FY11. Based on 5-months FY12 data, these Priority 2 intakes are projected to increase by another 30% in FY12. Also, 5-month data from FY10 and FY11 annualized produce projections that are about 17% below the actual number of FRI’s received for each year. The performance standard is to be onsite to investigate within 10 business days of receipt.

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D. 15
0
500
1000
1500
2000
2500
3000
FY 2007 2846 1584 555 411 2226 896
FY 2008 2742 1450 616 503 2452 858
FY 2009 2826 1443 721 516 2052 913
FY 2010 2430 1434 1503 511 2058 798
FY 2011 1755 1356 1578 216 1743 799
IL (788)* IN (503)* MI (429)* MN (386)* OH (955)* WI (390)*
Long Term Care - Total Number of Complaint Health Surveys Conducted
*(Total Number of Nursing Homes)
Michigan is the only state within Region V reflecting a consistent pattern of increasing complaint investigations. MI is on a trend to have its nursing home complaints exceed those in states with nearly double the number of nursing homes.

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D. 16
Nursing Homes cont’d
BHS current staff dedicated to nursing home regulation: 162.85 FTE’s • Health Care Surveyors: 110 • Non-Surveyor Professionals: 30.85• Clerical: 22
Relevant factors:• 17% increase in nursing home complaints since FY10• 44% increase in facility reported abuse/neglect since FY10• 90% of all BHS complaints involve nursing homes • 85% of all BHS inspection time is spent on nursing homes• 14 new nursing homes licensed in FY12• $1.6 million cost accounting increase in staff retirement/healthcare for FY12• Investigations are accumulating a backlog (currently >300 intakes pending)• Reports are not always issued timely• Revisits are not always timely
C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
Nursing Home licensees currently pay: •$2.20/bed x 46,890 beds = $103,000 •Total Costs: $23 million to regulate MI nursing homes•BHS receives federal and state funding, mostly federal funds since most nursing homes are Medicare/Medicaid certified.
State obligation: •$7,210,221 / 48,245 beds = $150 per bed
Report recommendation: •$1,500 annual license fee along with a $136 annual per bed fee to more fairly balance the costs between very small and very large nursing home operators.
Bureau of Health Systems
17

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D. 18
Analysis of Disputed Citations FY09 - FY11
FY 09 FY 10 FY11
Total Health Citations 4,538 4,267 4,359
Standard Survey Citations 3,889 3,365 3,335 (8.4 per survey ave) (7.3 per survey ave) (7.4 per survey ave)
Complaint Survey Citations 649 902 1,024 (0.9 per survey ave) (0.6 per survey ave) (0.6 per survey ave)
Citations Appealed 305 299 360Through IDR process (7% of total) (7% of total) (8% of total)
Source: BHS IDR Log PDQ federal data base

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D. 19
Out of 278 Percentage
BHSTotal Tags Reviewed 278 77%
Supported 172 62%
Amended 43 15%
Deleted 63 23%
Out of 82 Percentage
MPRO Total Tags Reviewed 82 23%
Supported 67 82%
Amended 4 5%
Deleted 11 13%
BHS and MPRO IDR Results: 360 Total
Overall, <2% of all FY 11 citations were deleted through informal appeal. Only 8% of all FY 11 citations were appealed through IDR.
Source: IDR Log

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D. 20
Keynote Address:
Dr. Charlotte Eliopoulos, RN, PhD
“Challenges of Caring for Clinically Complex Residents”