by dr. rania samir associate professor of cardiology ain …epsegypt.com/upload/21032013/atrial...
TRANSCRIPT

BY
Dr. Rania samir
Associate Professor of Cardiology
Ain Shams University

Atrial flutter occurs when the atria are stimulated to contract at 200-350 bpm usually because electrical impulses are traveling in a circular fashion around and around the atria.
Often the impulses are traveling around an obstacle like the mitral valve, tricuspid valve or the openings of the superior or inferior vena cavae.

The re-entry circuits often occupy large areas of the atrium & are referred to as “macro-reentrant”
characterized by a regular rate, a uniform flutter wave morphology with characteristic saw-toothed electrocardiographic appearance.

Atrial flutter represents the most important & most
common atrial tachyarrhythmia after AF The overall incidence of atrial flutter in a recent
population study was 0.88%,
0.05% in patients < 50 years old
5.87% among individuals > 80 years of age.
2.5 times more common in males Risk increases 3.5 times in presence of CHF Risk increases 1.9 times in presence of COPD
(Granada et al, 2000)

In 1905, William Ritchie first recorded atrial flutter with an ink-polygraph recorder
In 1913, Sir Thomas Lewis made the first clear-cut ECG description of atrial flutter
In 1921, Lewis considered that atrial flutter was the result of a circus movement
In 1970, Puech et al identified 2 types of atrial flutter: common type and rare type

Many different forms of atrial flutter exist & since it
was first described in 1911, many terms have been
used to characterize atrial flutter, particularly
recently, to the point that atrial flutter terminology
has become quite confusing
This has led to multiple classification schemes.


Based mainly on ECG criteria, the first simple
classification in 1970:
2 subclasses
Typical atrial flutter (common)
Atypical atrial flutter (rare or uncommon)

Typical atrial flutter:
Dominant -ve sawtooth
flutter waves with terminal low amplitude +Ve component in ECG leads II, III and aVF
+ve flutter waves in V1,
transition to –Ve in V6
Lead I is low amplitude
–Ve/isoelectric, aVL is
upright
Ain Shams University EP lab

Atypical atrial flutter:
+Ve , broad based, notched
flutter waves in II, III, aVF
- Ve, broad flutter waves in V1 ususally notched transitioning to +Ve across the pericordium to +Ve flutter waves in V6
lead I is upright, aVL is low amplitude –Ve & notched
Ain Shams University EP lab
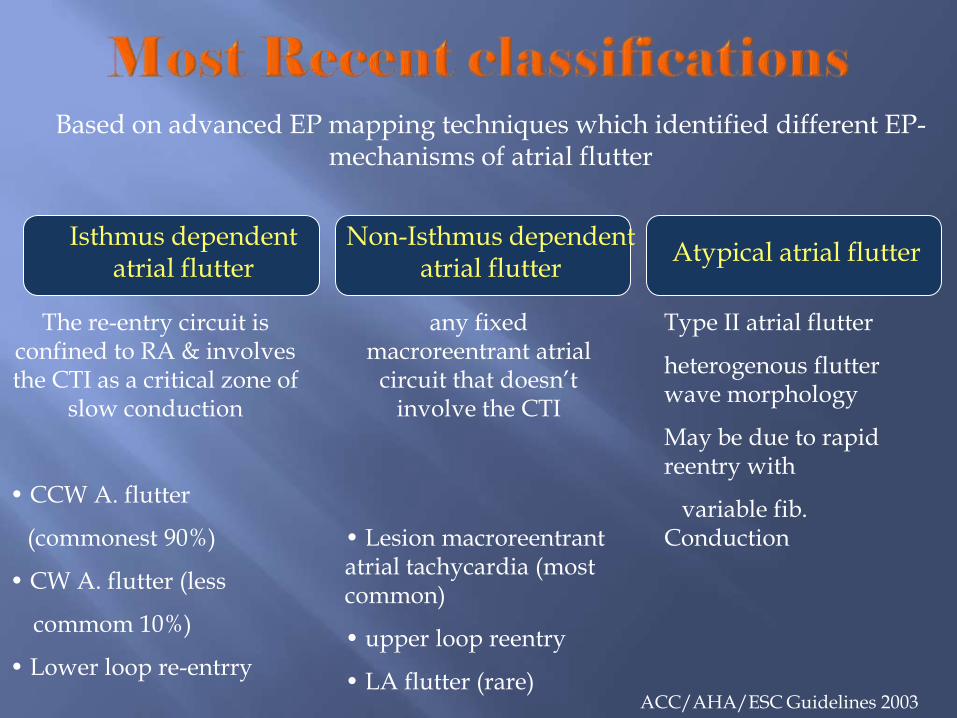
Based on advanced EP mapping techniques which identified different EP- mechanisms of atrial flutter
Isthmus dependent atrial flutter
Non-Isthmus dependent atrial flutter
Atypical atrial flutter
The re-entry circuit is confined to RA & involves the CTI as a critical zone of
slow conduction
• CCW A. flutter
(commonest 90%)
• CW A. flutter (less
commom 10%)
• Lower loop re-entrry
any fixed macroreentrant atrial
circuit that doesn’t involve the CTI
• Lesion macroreentrant atrial tachycardia (most common)
• upper loop reentry
• LA flutter (rare)
Type II atrial flutter
heterogenous flutter wave morphology
May be due to rapid reentry with
variable fib. Conduction
ACC/AHA/ESC Guidelines 2003

Usually paroxysmal, occasionally persistent
Occurs commonly after open heart surgery
Associated with COPD, MVD or TVD, PE, thyrotoxicosis, and atrial enlargement.
Frequent association with AF.
In the presence of WPW syndrome, it may lead to 1:1 AV conduction and dire consequences.
A. Flutter is one of atrial tachyarrythmias occurring with SSS.

Most common ECG presentation HR 150 bpm, 2:1 AV conduction

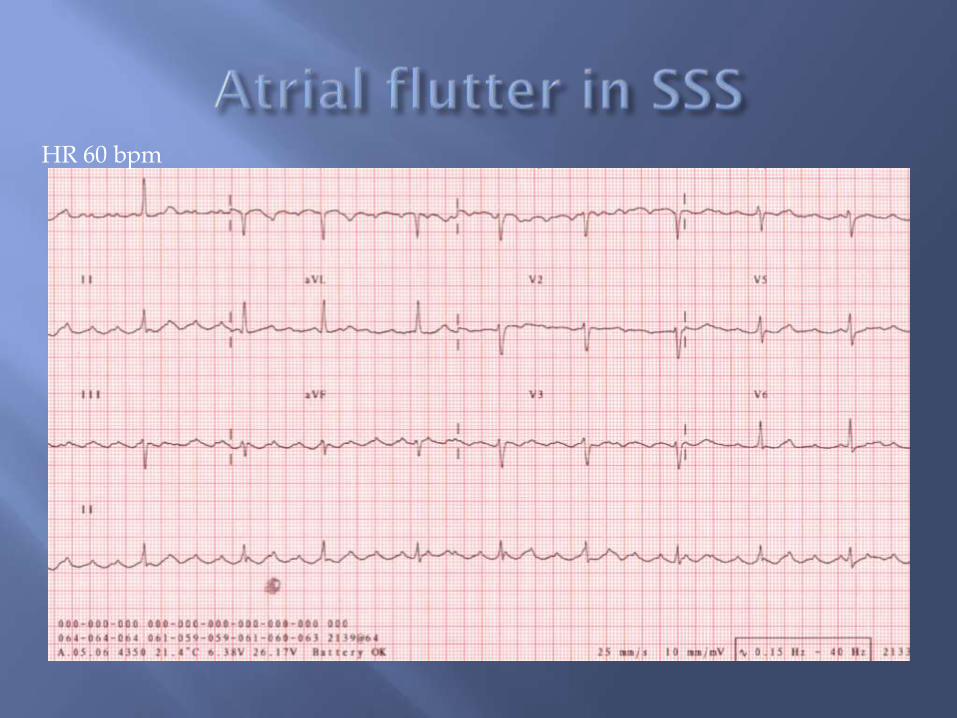
HR 60 bpm
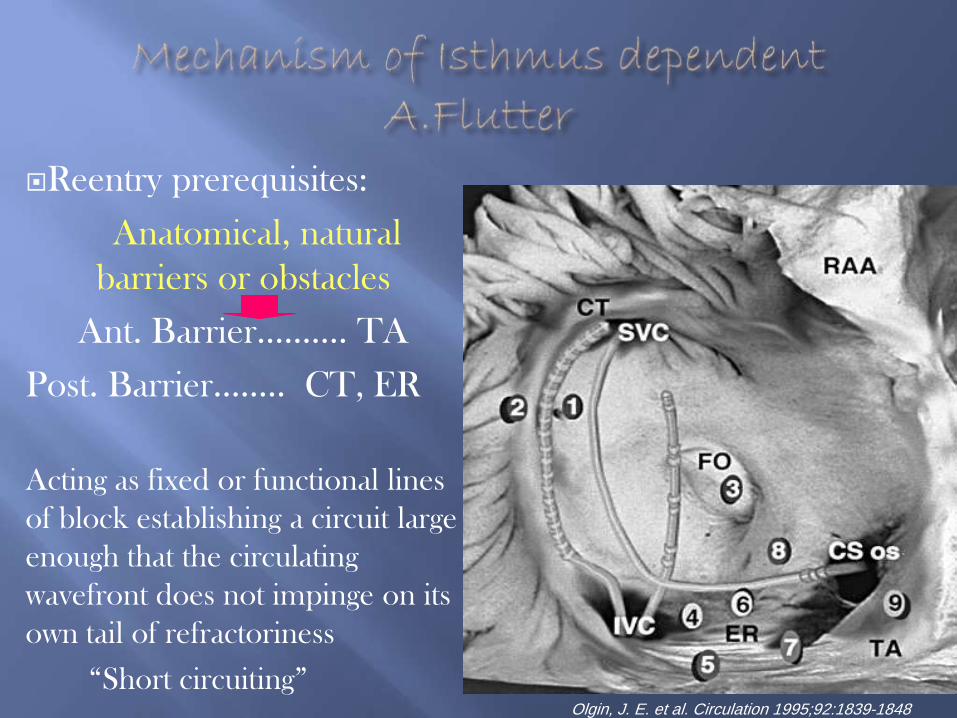
Reentry prerequisites:
Anatomical, natural
barriers or obstacles
Ant. Barrier………. TA
Post. Barrier…….. CT, ER
Acting as fixed or functional lines
of block establishing a circuit large
enough that the circulating
wavefront does not impinge on its
own tail of refractoriness
“Short circuiting”
Olgin, J. E. et al. Circulation 1995;92:1839-1848

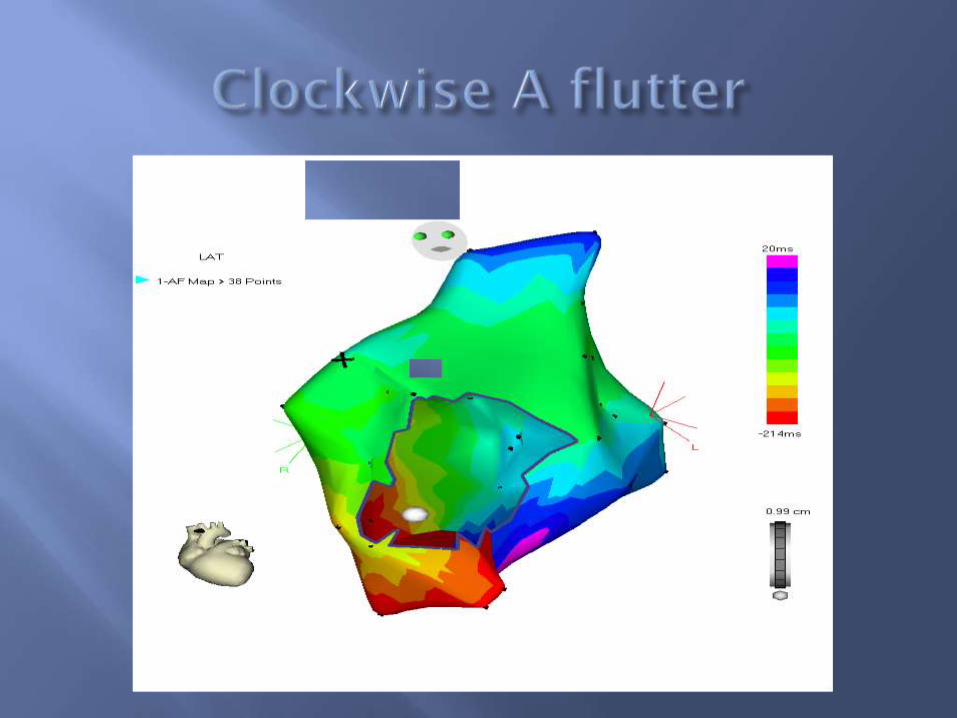
isthmus dependent atrial
flutter was determined to be
due to a macroreentrant
circuit rotating in either a
counterclockwise
(common) or clockwise
(uncommon) direction in
the right atrium, with an
area of relatively slow
conduction in the low
posterior right atrium
IAS
CT
IVC ER
CS
TA
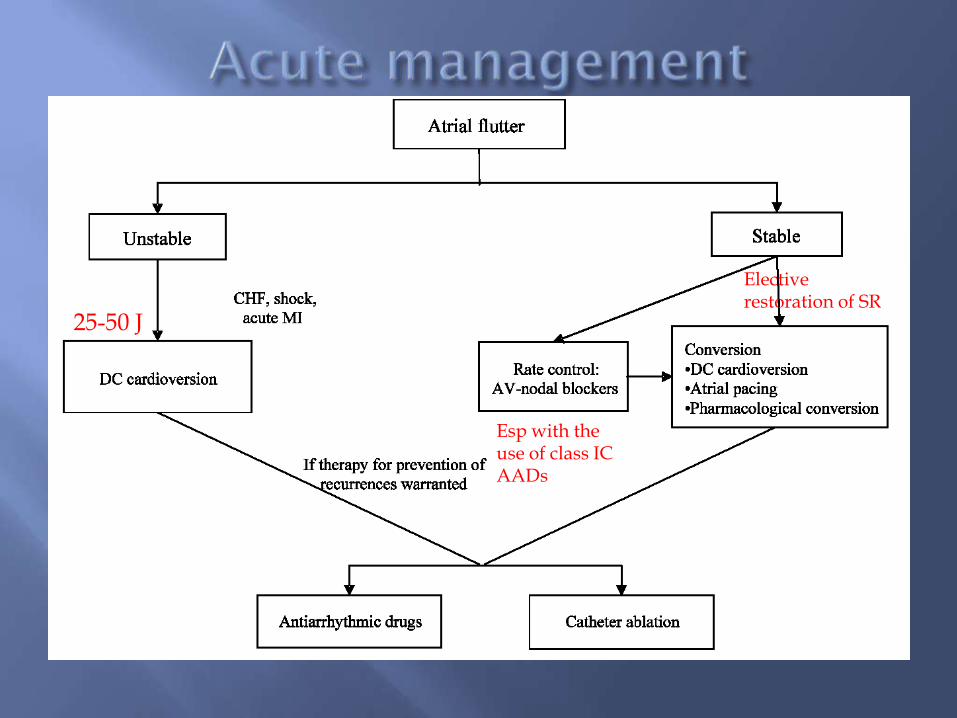
Esp with the use of class IC AADs
25-50 J
Elective restoration of SR

38-79%
20-40%

Atrial flutter is most often a nuisance arrhythmia & its clinical significance lies largely in its frequent association with AF or rapid ventricular response which is principally responsible for many of the associated symptoms So, maintenance of SR after CV is mandatory in cases of recurrent A. flutter
Based on the available long term data, drug treatment offered a limited ability to maintain SR without occasional to frequent recurrences of A.flutter, even when multiple agents are used.

Reported long term success rates ranging from 50% for
class I to 73% for class III (oral dofetilide) Also, long-term rate control alone usually requires large
doses of AV nodal blocking agents
Singh et al, Circulation 2000

Approaches to endocardial mapping of A flutter
include standard multielectrode catheters, Expanding
electrode arrays or 3D mapping techniques but still
Standard multielectrode catheter-based mapping still
remains the main tool for the study of A flutter
The recent advances in this therapeutic approach were associated with high success rates, low recurrence rates and minimal complications.

IAS
Isthm
IAS
Isthm IVC
LAO LAO

Large randomized trials, RF- ablation creating linear lesions across the critical zone of slow conduction (CTI) till achievement of CBIB as an endpoint of ablation
High success rates 90-100%
Low recurrence rate 6-9%
over a period of 9-17 mo
(Tai et al., 1998) (Wu et al.,2002)

RAO LAO
Ain Shams University EP lab

ACC/AHA/ESC guidelines,2003
Comparing the published success rates of AADs in maintaining SR to significantly high long term success rates of RF-ablation Favors RF ablation as an acceptable therapeutic approach of A . flutter

Although the success rates of RF-ablation using conventional & 3D mapping techniques are similar
Shorter fluoroscopy time (3.9±15 vs 22 ±6.3 min)
(Kottkamp et al, 2000)
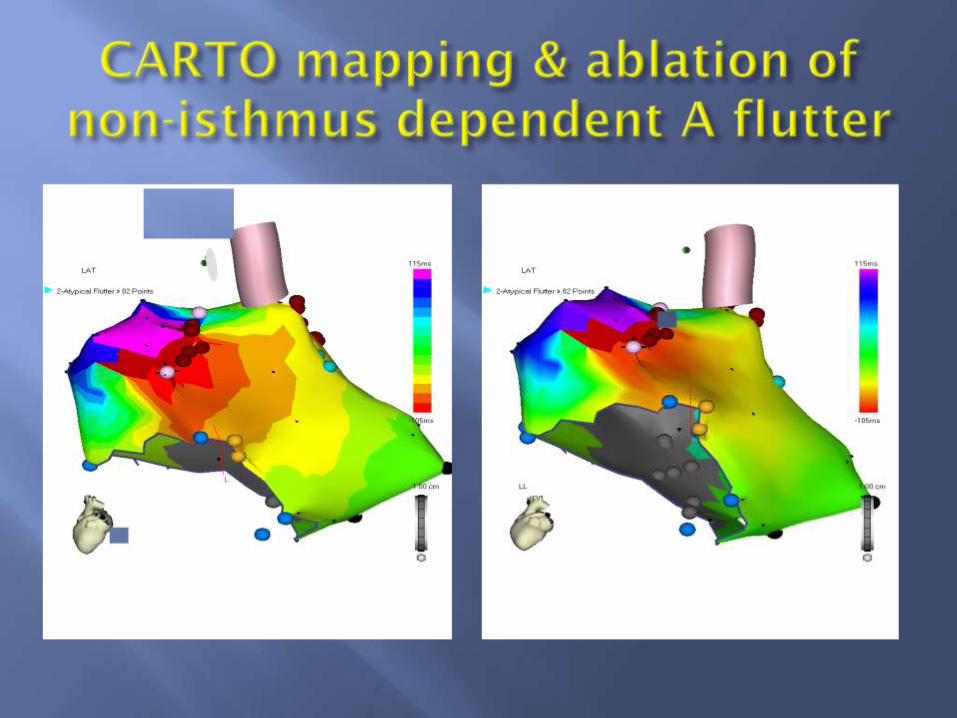
Precise identification of discrete gaps within non-contiguous lesion lines the ability to renavigate to previously mapped & ablated sites
Extremely important for mapping & ablation of non-isthmus dependent A flutter.

Isthmus ablation in patients with atrial flutter has proved positive impact on QOL.
Catheter ablation is curative in many patients obviating the need for life-long AADs, and may be more cost effective on the long term than AAD therapy.
Substantial fluoroscopy exposure, which is necessary for conventional isthmus ablation, is significantly reduced with 3D mapping for isthmus ablation which have an impact on the long-term safety of this invasive treatment strategy.


First simple classification based on ECG patterns, in 1970
-Typical atrial flutter (Counter-clockwise)
- Atypical atrial flutter (Clockwise)

CT
IAS
IVC ER

During PCS pacing
Before ablation After ablation
Complete CW block
Ain Shams University EP lab

LRA pacing
Before ablation After ablation
Complete CCW block
Ain Shams University EP lab

Variation in the isthmus width
Wide isthmus (49 mm) making sharp angle with IVC 79°
Craniocaudally elongated RA with short isthmus (17 mm)
Isthmus width 17-54 mm
Isthmus width > 39 mm or Cath-IVC angle <81° assoc with difficuilty of reaching TA
Heidbüchel et al Circulation 2000
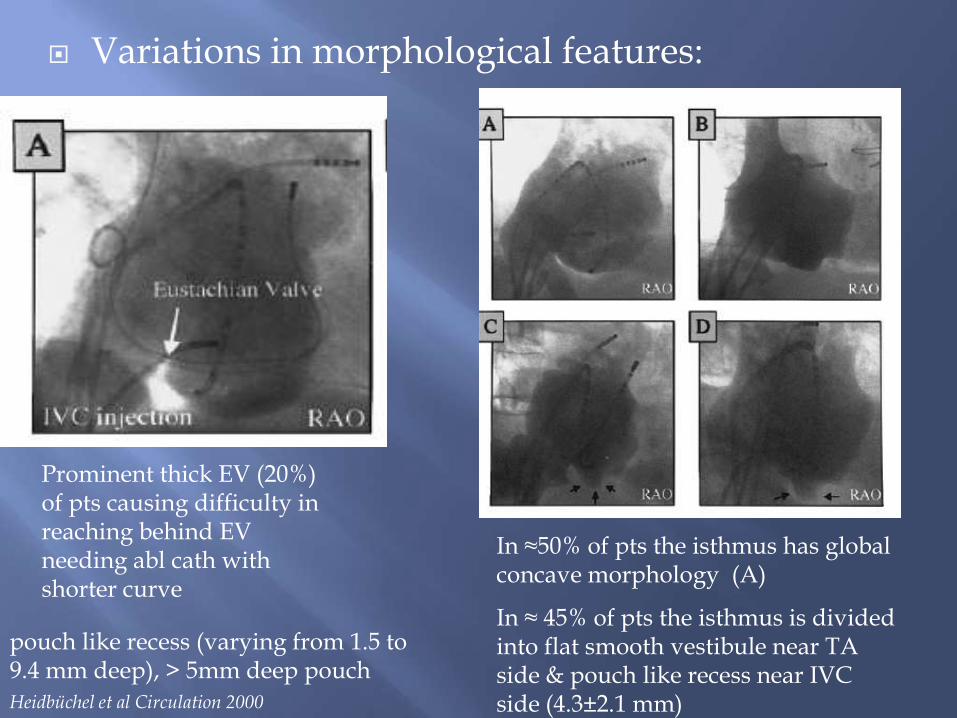
Variations in morphological features:
In ≈50% of pts the isthmus has global concave morphology (A)
In ≈ 45% of pts the isthmus is divided into flat smooth vestibule near TA side & pouch like recess near IVC side (4.3±2.1 mm)
Prominent thick EV (20%) of pts causing difficulty in reaching behind EV needing abl cath with shorter curve
Heidbüchel et al Circulation 2000
pouch like recess (varying from 1.5 to 9.4 mm deep), > 5mm deep pouch
Need for prompt restoration of sinus rhythm
DC cardioversion (25-50 J)
Elective restoration of sinus rhythm
Antiarrhythmic drug (ibutilide or class IC agent)
Rapid atrial pacing
Ventricular rate control: often required (β-blocker or calcium channel blocker), especially with use of class IC antiarrhythmic agent

TCL 240 ms
Ain Shams University EP lab

CS pacing before ablation CS pacing after ablation showing CW isthmus block
Ain Shams University EP lab

Before ablation After ablation
Ain Shams University EP lab
