bundled payment primer - washington health care
TRANSCRIPT

Bundled Payment Primer
One Company’s Experience

Health Care Reform Brings New Focus on Post-Acute Care

2020 Goal: Minimum 50 Percent of Total Medicare PAC Provider Payments Bundled
$0
$5
$10
$15
$20
$25
$30
$35
2013 2015 2017 2018 2020
Bill
ion
s
All PAC providers
Pilot began Oct. 1
Reduce Spend by -2.85%
Add new participants
Jan. 1

Rapid Expansion of Bundling
38% 35%
27%
Fee-for-Service BundledPayments
Capitated orother paymentsw/insurance risk
Early Mid Late Unsure
Bundled Payment Implementation Progress2
What phase of bundled payment plan implementation is your health plan
currently in?
Bundled Payment Implementation Plans2 Average Percentage of Hospital Revenues by 20181
Health Systems Health Plans
1Source: Health Enterprise Partners, “Seizing Opportunity in the Wake of Reform-Executive Perspective Survey, 2012” 2Source: Avality, The Health Plan Readiness to Operationalize New Payment Models, April 2013. The study was administered by independent research firm Porter Research in the fourth quarter of 2012. Porter Research completed interviews with qualified participants of 39 health plans that represented more than 50% of total covered lives in the United States. Target participants included: quality management leadership, medical directors, and chief medical officers.
Currently Implemented
24%
Planning to Implement
34%
No Plans 42%
In the next 5 years, bundled payments will represent 35%
of U.S. health systems’ revenue
24% of health plans currently implementing bundled
payment contracts

Understanding Bundling and Why Post-Acute Care is Critical to Success

Bundled Payment for beginners
Acute
Care
HH
SNF
ILF
ALF
Traditional Medicare patients belonging to
target DRG enters network
2:
3: SNF or HH becomes episode initiator
1: Patient has acute care stay
90 Day Episode
4: “Bundler” manages PAC “charges” for 90 days SNF stay HH services All supplies MD visits OP service ED visits Hospital
readmissions
5:
Based on actual cost VS. target price, Medicare either risk OR
gain shares
Payor

7 Source: http://www.nejm.org/doi/full/10.1056/NEJMp1315607

Tremendous Variation in PAC Spending Provides Opportunity for Value Creation
Drugs, 9%
Procedures, 14%
Diagnostic Tests, 14%
Acute Care Only, 27%
PAC Only, 73%
8
Source: Variation in Health Care Spending, Institute of Medicine, October 2013
If regional variation in PAC spending did not
exist, Medicare spending variation would fall by 73%

Hospital Physician Post-Acute Care Readmissions Other
Significance of Post-acute Costs Vary by Clinical Condition
Stroke
Hip and Femur Proc.
Cardiac Bypass
Heart Failure
0% 20% 40% 60% 80% 100%
Source: MedPAC September 2012; MedPAC Analysis of 2004-2006 5% Medicare claims files

Four Models of Bundled Payment
Types of Services Included in Bundle Model 1
Acute Hospital
Stay Only
Model 2
Acute Hospital
+
Post-Acute
Model 3
Post-Acute
Care Only
Model 4
Acute Hospital
Stay +
Readmissions
Inpatient hospital and physician services Related post-acute care services Post-acute care services Related readmissions Other services defined in the bundle (Part A & Part B) Awardees 21 148 152 22
Episode-Initiating Hospital
Admission
PAC Services Physician Services
Readmissions Other Services*
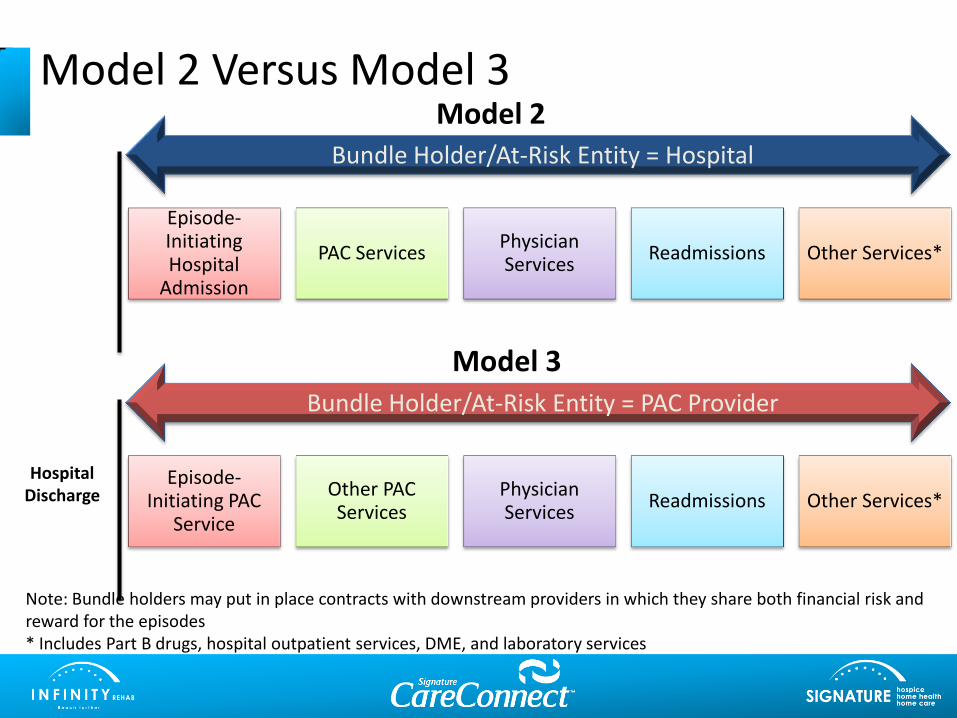
Model 2 Versus Model 3
Episode-Initiating PAC
Service
Other PAC Services
Physician Services
Readmissions Other Services*
Bundle Holder/At-Risk Entity = Hospital
Model 2
Bundle Holder/At-Risk Entity = PAC Provider
Hospital Discharge
Model 3
Note: Bundle holders may put in place contracts with downstream providers in which they share both financial risk and reward for the episodes * Includes Part B drugs, hospital outpatient services, DME, and laboratory services

Potential Roles for Post-Acute Providers
Model 2
• Episode Integrated Provider to Model 2 Awardee Convener (preferably with gainsharing to share risk)
• Vendor to Model 2 Awardee Convener (accept referrals according to predetermined criteria)
• Partner to Model 2 Convener (create and control bundling structure)
Model 3
• Model 3 Awardee or Awardee Convener (accept risk, control gains)
• Model 3 Facilitator Convener (might be applicable for large post-acute and LTC systems that are loosely affiliated)
• Vendor or Episode Integrated Provider to Model 3 Awardee
12

Franciscan Alliance ACO Focused on Post-acute Care…and Made Gains
• Number of SNFs in the ACO network fell from 30 to 9
• Significant reductions in LOS of network providers: dropping from 42 days to less than 28 days
• Corollary reductions in readmission also led to cost savings and reduced risk for the hospital, system, or ACO
– For one network SNF, the acute care hospital readmission rate fell from 18% to less than 2% in 12 months
• Family and patient satisfaction with discharge management is also improved, given hospital/SNF effort to better coordinate care along the continuum
13
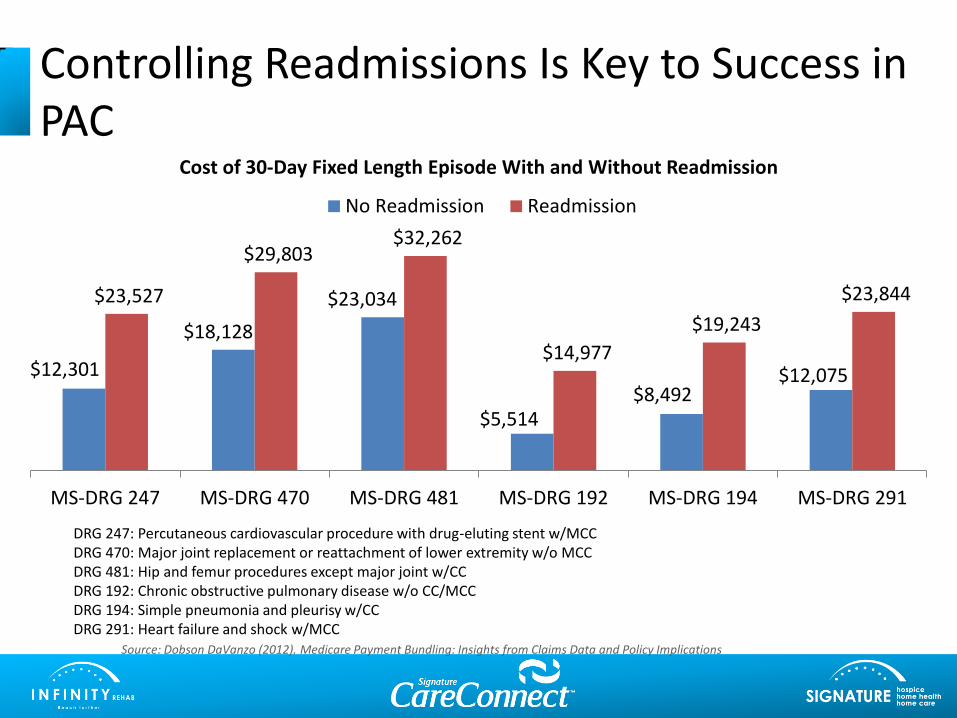
Controlling Readmissions Is Key to Success in PAC
$12,301
$18,128
$23,034
$5,514 $8,492
$12,075
$23,527
$29,803 $32,262
$14,977
$19,243
$23,844
MS-DRG 247 MS-DRG 470 MS-DRG 481 MS-DRG 192 MS-DRG 194 MS-DRG 291
Cost of 30-Day Fixed Length Episode With and Without Readmission
No Readmission Readmission
Source: Dobson DaVanzo (2012). Medicare Payment Bundling: Insights from Claims Data and Policy Implications
DRG 247: Percutaneous cardiovascular procedure with drug-eluting stent w/MCC DRG 470: Major joint replacement or reattachment of lower extremity w/o MCC DRG 481: Hip and femur procedures except major joint w/CC DRG 192: Chronic obstructive pulmonary disease w/o CC/MCC DRG 194: Simple pneumonia and pleurisy w/CC DRG 291: Heart failure and shock w/MCC
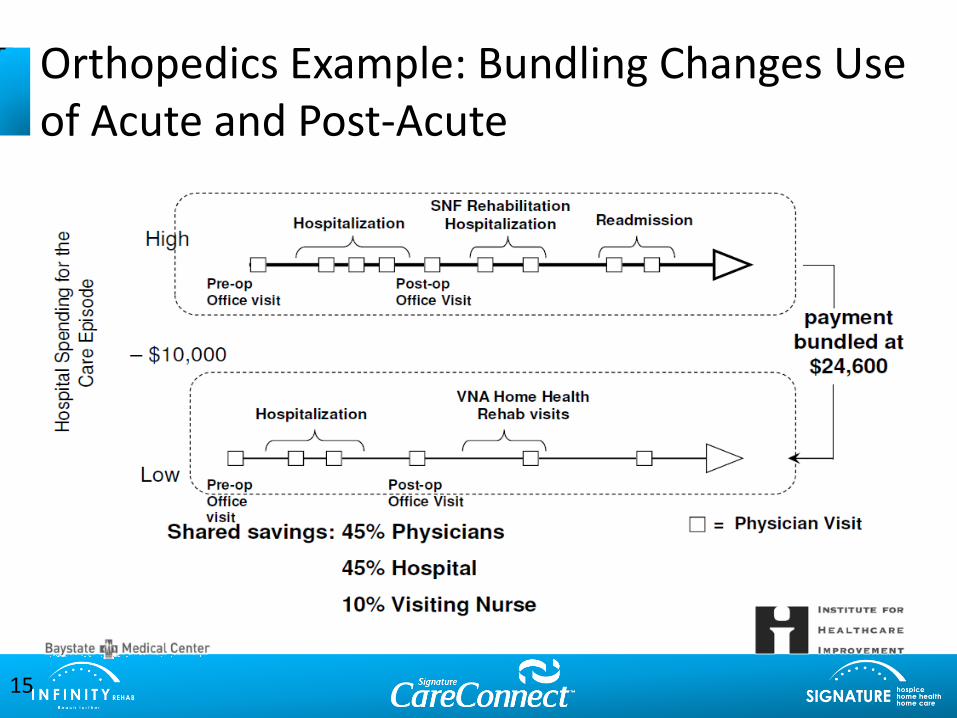
Orthopedics Example: Bundling Changes Use of Acute and Post-Acute
15
A Closer Look at Model 3

Criteria for Beneficiary Inclusion in Episode in Model 3
• Beneficiary is: – Eligible for Part A and enrolled in Part B
– Admitted to or initiates services with an episode initiator within 30 days after the beneficiary has been discharged from an acute care hospital for an MS-DRG included in a clinical episode associated with the episode initiator
• Beneficiary must: – Not have end-stage renal disease
– Not be enrolled in any managed care plan, e.g., Medicare Advantage, health care prepayment plans, cost-based health maintenance organizations)
Entities That Can Initiate Episodes in Model 3
Skilled nursing facilities (SNF)
Inpatient rehabilitation facilities (IRF)
Long-term care hospitals
(LTCH)
Home health agencies (HHA)
Physician group
practices (PGP)

Bundled Payment Components
Defined population
Defined period of
time
Quality of care
Fixed price

Defined Population
Defined population
Defined period of
time
Quality of care
Fixed price

Bundled Payment: 7 Diagnostic Groups
48 Diagnostic Families: Orthopedics
Orthopedics
•Major joint replacement of the lower extremity
•Hip & femur procedures except major joint
•Spinal fusion (non-cervical)
•Revision of the hip or knee
•Lower extremity & humerus procedure except hip, foot, femur
•Double joint replacement of the lower extremity
•Fractures femur and hip/pelvis
•Amputation for MSK/CT or endocrine/nutrition or circ disorder
•Back & neck except spinal fusion
•Cervical spinal fusion
•Major joint upper extremity
•Combined anterior posterior spinal fusion
•Complex non-cervical spinal fusion w/spinal curv/malig/infxn/9+fusion
•Removal of devices (both hip/femur and other)
•Knee procedures w/ and w/o infection
•Medical non-infectious orthopedic problems (sprains, strains, back pain)

48 Diagnostic Families: Cardiology and Cardiothoracic Surgery
Cardiology
• CHF
• Percutaneous coronary intervention
• Cardiac arrhythmia
• AMI discharged alive
• Pacemaker
• Cardiac defibrillator
• Chest pain
• Transient ischemia
• Pacemaker device replacement or revision
• AICD generator or lead
Cardiothoracic Surgery
• Cardiac valve
• CABG
• Major cardiovascular procedure

48 Diagnostic Families: Internal, Pulmonary Medicine, Neurology, Other
Internal Medicine
• UTI
• Nutritional & misc metabolic disorders
• Peripheral vascular disorders (medical)
• Atherosclerosis
Neurology
• Stroke w/ and w/o T-PA
• Syncope & collapse
Pulmonary Medicine
• Simple pneumonia/Respiratory infections
• COPD, bronchitis/asthma
• Other respiratory
Other
• Sepis
• Major bowel
• Cellulitis
• GI hemorrhage
• GI obstruction
• Renal failure
• Esophagitis, gastroenteritis & misc digestive
• Other vascular
• Red blood cell disorders
• Diabetes

Top Bundles for All Model 3 Participants Represents Participants & Conditions Moved Into Phase 2*
1. Congestive heart failure (94%)
2. COPD, bronchitis/asthma (79%)
3. Simple pneumonia & respiratory infections (77%)
4. UTI (75%)
5. Other respiratory (73%)
6. Acute myocardial infarction (AMI) (64%)
7. Cardiac arrhythmia (63%)
8. Cardiac defibrillator, Cardiac valve, Chest pain, Coronary artery bypass graft surgery, Medical peripheral vascular disorders, Other vascular surgery, Percutaneous coronary intervention, Stroke (63%)
9. Fractures femur and hip/pelvis (56%)
10. Sepsis (55%)
* 84 Model 3 awardees (55%) have moved into Phase 2
Source: CMS.gov, February 2014

Sample data: 1st look
Episodic Stats % Share SNF LOS SNF Rate % HHA HHA Rate
All DRG's 34.0 527$ 50.5% 3,203$
Cardiac 13% 39.7 536$ 54.5% 3,370$
High Cost Ortho 13% 42.8 544$ 56.3% 3,267$
Infection 12% 38.2 512$ 47.7% 3,309$
Low Cost Ortho 27% 24.2 543$ 48.6% 3,098$
Medical 17% 37.6 516$ 50.8% 3,258$
Respiratory 9% 33.7 503$ 45.7% 3,226$
Surgical 9% 31.3 510$ 50.0% 2,910$
Episodic Stats Episodes % Readmit CV $ Episode $ Readmit $ HHA $ SNF $ DME $ MD $ OP $ Outlier
All DRG's 5,370 21.2% 0.47 25,144$ 2,200$ 1,617$ 17,914$ 227$ 2,066$ 700$ 552$
Cardiac 683 24.3% 0.45 28,861$ 2,118$ 1,835$ 21,305$ 170$ 2,102$ 652$ 426$
High Cost Ortho 695 17.3% 0.41 29,891$ 1,739$ 1,838$ 23,291$ 229$ 1,925$ 571$ 236$
Infection 631 30.9% 0.47 28,314$ 3,467$ 1,579$ 19,574$ 192$ 2,416$ 697$ 1,060$
Low Cost Ortho 1,462 12.6% 0.58 18,521$ 1,179$ 1,506$ 13,136$ 215$ 1,750$ 640$ 356$
Medical 907 22.8% 0.51 26,872$ 2,357$ 1,656$ 19,380$ 180$ 2,142$ 612$ 780$
Respiratory 488 21.3% 0.45 24,626$ 2,183$ 1,474$ 16,954$ 241$ 2,028$ 725$ 614$
Surgical 504 32.0% 0.43 26,194$ 4,060$ 1,455$ 15,982$ 453$ 2,586$ 1,252$ 617$

Defined Period of Time
Defined population
Defined period of
time
Quality of care
Fixed price

Start and End of Episode
Start of Episode
• Post-acute care with an episode initiator (SNF, LTCH, IRF, or HHA) within 30 days after discharge from an acute care hospital for an MS-DRG included in a clinical episode associated with the episode initiator
End of Episode • 30, 60, or 90 days after the initiation of the episode

Length of Episodes for Current Model 3 Bundlers
All Episodes
Name of Episode No. Participating % Participating
30-day episodes 0 0.0%
60-day episodes 53 3.0%
90-day episodes 1,729 97.0%
All Episodes Total 1,782 100.0% Source: CMS.gov February 2014

Fixed Price
Defined population
Defined period of
time
Quality of care
Fixed price

Payment Parameters
• Payment from CMS to providers: traditional FFS payments
• Discount provided to Medicare defined by episode length: 3% discount for episodes of 30, 60, or 90 days in length
• Reconciliation:
– Medicare pays awardee difference between target price and actual cost of care for an episode if actual cost of care is less than target price
– Awardee pays Medicare difference between target price and actual spending if actual cost of care exceeds target price

Included Services in Bundle: Which Include Broad Clinical Episode Categories
• Physicians’ services
• Inpatient post-acute care services
• Inpatient hospital readmission services
• Long-term care hospital services
• Inpatient rehabilitation facility services
• Skilled nursing facility services
• Home health agency services
• Clinical laboratory services
• Durable medical equipment
• Part D drugs
• NOTE: HOSPICE IS NOT INCLUDED

Target Price and Reconciliation Process
33
Set Target Price
• Price is set based on baseline episode costs for each selected episode at DRG family level; then 3% discount applied
• May include low-volume adjustment
Upfront FFS Payments
• Medicare pays all Part A and Part B providers who serve patients identified as participating in the initiative using current FFS payment systems
Quarterly Payment Reconciliation
• Approximately six months after patient’s episode ends, actual expenditures are compared to target price:
• If expenditures exceed target price, awardee pays difference to Medicare
• If expenditures less than target price, Medicare pays difference to awardee

$2,200 $17,914 $1,617
$227
$2,066
$552
0% 20% 40% 60% 80% 100%
All DRG's
SNF Episodic Stats: (All) ; (All)
$ Readmit $ SNF $ HHA $ DME $ MD $ OP $ Uncontrol
Target Price: SNF as episode initiator (Sample Case Study)
Historic “bundled Price” =
Mandatory 3% savings =
Projected “target price” =
$25,144
$754
$24,390 OR less
21.2% 90 day readmission rate
50.5% received HH
at $3,203/episode
34 days LOS at $527/day

Quality of Care
Defined population
Defined period of
time
Quality of care
Fixed price

Care Redesign is Integral to Bundling
• Care redesign includes all of the providers and suppliers of care who must work together to achieve goals
• Care redesign focuses on using evidence-based practices to redesign the care provided for a specific bundle that will measurably improve care, prevent readmissions and ED visits, and improve patient outcomes
• Pathways extend from the hospital into the post-acute settings, home health, assisted living, and home
36

Bundling Care Redesign Strategies
37
Evidence-Based Care Practices
Care Pathways
Palliative Care
INTERACT 3.0
Tele-health
PCP/NP On-site Access
Health Coach Certification
Clinical Competency
Risk-Stratification
Care Transitions

Risk and Rewards of Participating in Model 3 Bundling

Bundled Payment: where the risks are
Hospital
HH
SNF
ILF
ALF
Unable to identify “bundled” patients
2:
3: Unable to track bundled patients in continuum
1:
90 Day Episode 4: Patient referred to
non-”Network” provider
6: Medicare penalty due to poor episode management
Not a preferred
provider to hospitals
5: Patient goes to ED or gets readmitted
Payor

0
5
10
15
20
25
30
35
$4,000
$5,000
$6,000
$7,000
$8,000
$9,000
$10,000
$11,000
$12,000
$13,000
Impact of Per Diem and LOS Decreases on Revenue / Case
Revenue/Avg Case Average Length of Stay
Providers’ Optimal Jumping On Point
Payors’ Preferred Jumping Off Point
Time Value of Taking Action When is the right time to take on risk-based reimbursement?
ALOS REV/CASE
Year 1 Year 2 Year 3 Year 4 Year 5 Year 6
Per Diem 400 360 360 340 340 340

Risks and Rewards of Model 3 Bundling
Rewards
Gain experience managing risk
Capture gains from reducing hospitalizations and retain revenues from reducing length of stay
Access valuable data during Phase 1 to learn more about your position in your market
Risks
Insufficient bandwidth to successfully execute bundled payment initiative
Insufficient scale or inadequate management of readmissions leads to making payments to CMS
Acuity level of referrals increases relative to baseline

Keys to Managing Downside Risk in Model 3
Robust care redesign that targets readmissions
Selection of diagnostic families for bundling
Achieving sufficient scale
Stratify patients by risk to customize intensity of interventions

Conveners in Bundled Payment
• May apply with or on behalf of designated awardees
• Not providers themselves, but rely on partner providers
• May choose to bear risk or not bear risk
Source: CMMI Bundled Payment Application, http://innovation.cms.gov/initiatives/Bundled-Payments/bpci-archive.html
Entity that serves an administrative and technical assistance function for one or more designated awardees

Overview of Bundling Arrangements
Submission Type
Risk-Bearing Non–Risk-Bearing
Facilitator
Convener
Single Awardee
(Episode Initiator)Awardee
Convener
Episode Initiator
Designated Awardee
(Episode Initiator)
This entity takes risk
under the facilitator
convener
Designated Awardee
Convener
This entity takes risk
under the facilitator
convener
Episode Initiator

Market Selection Considerations
• Degree of Medicare Advantage penetration
• Are referring hospitals involved in Model 2 bundling
• Are referring hospitals involved in ACOs
• Baseline performance of potential episode initiators

Is your organization ready to consider bundled payments?
• Clinical progress relative to baseline years
• Administrative bandwidth
• Clinical bandwidth to adopt new care strategies
• Episode management
• Primary care resources
• Data management
• Hospital relationships (C- level)
Contact:
Donna Mueller
Vice President of Business Development
Infinity Rehab
1-888-75-REHAB