bundle strategy, partnerships and population health ......3.5 spph16/207 annual plan monitoring...
TRANSCRIPT

Bundle Strategy, Partnerships and Population Health Committee 24 November 2016
Agenda documents
Agenda SPPH 24.11.16 V1.0.docx
10:001 OPENING BUSINESS AND GOVERNANCE10:001.1 SPPH16/200 Apologies for Absence10:011.2 SPPH16/201 Minutes of Meeting Held on 10.10.16 for Accuracy, Matters Arising and Review of Summary
Action LogSPPH16.201 Minutes SPPH 10.10.16 draft public v0.03.docx
SPPH16.201 Summary Action Log Public.docx
10:112 FOR CONSENT10:112.1 SPPH16/202 Betsi Cadwaladr University Health Board Multi-Agency Resilience – Vulnerable Person
ProcessMr Geoff Lang
SPPH16.202 Vulnerable person coversheet.docx
SPPH16.202 Vulnerable person protocol.doc
10:163 FOR DISCUSSION10:163.1 SPPH16/203 Seasonal Plan 2016-17
Ms Morag OlsenSPPH16.203 Seasonal Plan_coversheet.docx
SPPH16.203 Seasonal Plan Version 3.docx
10:313.2 SPPH16/204 Review of the Committee's allocated Risks extracted from the Corporate Risk Register
Mr Geoff LangSPPH 16.204 CRR coversheet.docx
SPPH16.204 CRR Report.pdf
10:413.3 SPPH16/205 Update on Well North Wales
Mr Glynne Roberts to deliver supporting presentationSPPH16.205 Well North Wales_coversheet.docx
SPPH16.205 Well North Wales Update V2.doc
11:063.4 SPPH16/206 Proposed Wylfa Nuclear Development
Mr Geoff LangSPPH16.206 Wylfa update_coversheet.docx
SPPH16.206 Wylfa report.doc
11:213.5 SPPH16/207 Annual Plan Monitoring Report - Quarter 2
Mr Geoff LangSPPH16.207 AOP Q2_coversheet.docx
SPPH16.207 AOP report Q2.doc
11:413.6 SPPH16/208 Annual Operational Plan 2017/18 and NHS Wales Planning Framework

Mr Geoff LangSPPH16.208 AOP and NHS Wales Planning Framework_coversheet.docx
SPPH16.208 AOP and NHS Wales Planning Framework.doc
SPPH16.208 NHS Wales Planning Framework_appendix 1.pdf
12:113.7 SPPH16/209 HMP Berwyn Healthcare Project
Ms Bernie CuthelSPPH16.209 HMP Berwyn Report.docx
12:264 FOR INFORMATION4.1 SPPH16/210 The Welsh Language Standards (Health Sector) Regulations 2016 – BCUHB Consultation
ResponseMr Chris Wright
SPPH16.210 Welsh Language Standards_coversheet.doc
SPPH16.210 Welsh Language Standards Health Sector Regulations - BCUHB Response.doc
4.2 SPPH16/211 Mid Wales Health Collaborative UpdateMr Geoff Lang
SPPH16.211 MWHC Update Report Oct 2016.pdf
4.3 SPPH16/212 Parliamentary Review of Health and Social Care in WalesMr Geoff Lang
SPPH16.212 Parliamentary Review.doc
SPPH16.212 Parliamentary review ToR.pdf
4.4 SPPH16/213 Summary of In Committee Business From 10.10.16Mr Geoff Lang
SPPH16.213 In Committee Items Reported in Public.docx
12:365 CLOSING BUSINESS5.1 SPPH16/214 Issues of Significance to inform the Chair's Assurance Report5.2 SPPH16/215 Any Other Business (at the discretion of the Chair)5.3 SPPH16/216 Date of Next Meeting - 26.1.17 9.30am Carlton Court5.4 SPPH16/217 Exclusion of Press and Public
Agenda documents
1 Agenda SPPH 24.11.16 V1.0.docx
AgendaStrategy, Partnerships and Population Health Committee
Date: 24-11-2016 Time: 10:00 - 13:00 Location: Preswylfa, Boardroom Chairman: Mrs Lyn Meadows Explanation: Item Description 10:00 OPENING BUSINESS AND GOVERNANCE 10:00 SPPH16/200 Apologies for Absence 10:01 SPPH16/201 Minutes of Meeting Held on 10.10.16 for Accuracy, Matters
Arising and Review of Summary Action Log 10:11 FOR CONSENT 10:11 SPPH16/202 Betsi Cadwaladr University Health Board Multi-Agency
Resilience – Vulnerable Person Process Mr Geoff Lang
10:16 FOR DISCUSSION 10:16 SPPH16/203 Seasonal Plan 2016-17 Ms Morag Olsen
10:31 SPPH16/204 Review of the Committee's allocated Risks extracted from the Corporate Risk Register
Mr Geoff Lang
10:41 SPPH16/205 Update on Well North Wales Mr Glynne Roberts - presentation
11:06 SPPH16/206 Proposed Wylfa Nuclear Development Mr Geoff Lang
11:21 SPPH16/207 Annual Plan Monitoring Report - Quarter 2 Mr Geoff Lang
11:36 SPPH16/208 Annual Operational Plan 2017/18 and NHS Wales Planning Framework
Mr Geoff Lang
11:51 SPPH16/209 HMP Berwyn : Progress Report Ms Bernie Cuthel
12:06 FOR INFORMATION

SPPH16/210 The Welsh Language Standards (Health Sector) Regulations 2016 – BCUHB Consultation Response
Mr Chris Wright
SPPH16/211 Mid Wales Health Collaborative Update Mr Geoff Lang
SPPH16/212 Parliamentary Review of Health and Social Care in Wales Mr Geoff Lang
SPPH16/213 Summary of In Committee Business From 10.10.16 Mr Geoff Lang
12:16 CLOSING BUSINESS SPPH16/214 Issues of Significance to inform the Chair's Assurance
Report SPPH16/215 Any Other Business (at the discretion of the Chair) SPPH16/216 Date of Next Meeting - 26.1.17 9.30am Carlton Court SPPH16/217 Exclusion of Press and Public 12:21 IN COMMITTEE BUSINESS SPPH16/218 In Committee Minutes of Meeting Held 10.10.16 and
Review of Summary Action Log V1.0
1.2 SPPH16/201 Minutes of Meeting Held on 10.10.16 for Accuracy, Matters Arising and Review of Summary Action Log
1 SPPH16.201 Minutes SPPH 10.10.16 draft public v0.03.docx
1
Minutes SPPH 10.10.16 Public v0.03
Strategy, Partnerships and Population Health Committee
DRAFT Minutes of the meeting held on 10th October 2016
in Venue Cymru, Llandudno
Present: Mrs Lyn Meadows Cllr Bobby Feeley Mrs Margaret Hanson Mrs Bethan Russell Williams
Independent Member (Chair) Independent Member Independent Member Independent Member
In Attendance: Mrs Sally Baxter Mr Rob Callow Ms Bernie Cuthel Mr John Darlington Mrs Jody Evans Cllr Phil Edwards Ms Lynne Grundy Mrs Eleri Hughes-Jones Mr J Martin Jones Mr Geoff Lang Mrs Katie Sargent Ms Dawn Sharp Mrs Mandy Townsend Mr Chris Wright
Assistant Director - Health Strategy Interim Head of Engagement (part meeting) Prison Health Development Lead (Interim) Assistant Director, Corporate Planning (part meeting) Senior Secretary Chair, Stakeholder Reference Group Assistant Director, Research & Development (part meeting) Welsh Language Services Manager (part meeting) Executive Director of Workforce & Organisational Development Executive Director of Strategy Assistant Director of Communications (part meeting) Assistant Board Secretary Wales Audit Office (observer for structured assessment) Director of Corporate Services
Agenda Item Discussed Action By
SPPH16/79 Apologies for Absence Apologies for absence had been received from Dr Evan Moore, Executive Medical Director.
SPPH16/80 Minutes, Matters Arising and Action Log from the last meeting held on 28th July 2016 SPPH16/80.1 The draft minutes were approved as an accurate record, however it was noted that the Director of Corporate Services had actually tendered apologies. SPPH16/80.2 Updates were provided against the summary action log. SPPH16/80.3 Reference was made to previous discussions as part of the Committee Annual Report item regarding Collaboration with Bangor University. It was agreed that a progress report would be prepared for the January SPPH Meeting.
GL
2
Minutes SPPH 10.10.16 Public v0.03
SPPH16/81 Reconnecting with the Public - An update on Public Engagement SPPH16.81.1 The Assistant Director of Communications and the Interim Head of
Engagement provided an update to the Committee which set out the progress of the
BCUHB’s public engagement activity and planned future activity. An overview of the
key milestones that the BCUHB were expected to deliver were summarised along with
the various phases of activity associated with the key milestones.
SPPH16.81.2 The SPPH noted that the Health Board in July had recruited three
Engagement Officers. The Officers had attended over 50 meetings/events on behalf of
the Health Board in August and September alone which had provided a number of
opportunities to promote Living Healthier Staying Well. Various links had been made
with a range of groups including; Viva (Young Peoples LGBT),and the Local Voluntary
Association. A full list of engagement activity which had taken place over the summer
period was set out in Appendix 2 to the report.
SPPH16.81.3 The Assistant Director of Communications outlined the next steps which
included working with the consultations initiative to discuss a structured piece of work
to ascertain the impact of the work undertaken to date. Cost implications were
acknowledged and it was explained that a proposal would be drafted and presented in
due course.
SPPH16.81.4 A question was raised with regards to poor feedback which had been
observed at a particular town council meeting. The Interim Head of Engagement
confirmed that a series of detailed questions had been asked which required follow up
and that the meeting had been advised that a written response would be provided.
Positive feedback to other events which the team had attended had also been
received and this was welcomed.
SPPH16.81.5 Negative press stories and public perceptions of media coverage
impacting upon the Health Board were raised. The Assistant Director of
Communications and the Interim Head of Engagement confirmed that work was
ongoing with regards to communication of “good news” stories/case studies with
emphasis being placed on the use of Facebook and Twitter as channels of
communication. The Vice Chair of the Health Board stressed that the Health Board
had pro-actively expanded its communication activity since she her appointment and
commended the team on their efforts.
SPPH16.81.6 BCU Press Desk Daily updates – In response to a question from Cllr P
Edwards regarding sharing the communications evening update, the Assistant
Director of Communications agreed to explore options. It was explained that the
document as currently drafted was for internal circulation.
SPPH16.81.7 The Committee expressed sincere thanks to the team and it was also
emphasised the area Engagement posts were absolutely vital to the expansion of the
team and engagement with the public.
SPPH16.81.8 The Committee noted the update on public engagement and thanked
the Assistant Director of Communications and the Interim Head of Engagement for

3
Minutes SPPH 10.10.16 Public v0.03
their attendance.
SPPH16/82 Planning for 2017/18 - Draft Principles SPPH16.82.1 The Executive Director of Strategy informed the Committee that National Guidance had been issued and would be circulated to all Board Members accordingly with regards to timelines and approach. SPPH16.82.2 The Assistant Director of Corporate Planning presented the planning
report of draft principles 2017-18. It was noted that the principles and approach to the
report were built upon the progress made in 2016/17 and supported the development
of the Annual Operational Plan for 2017-18. The paper highlighted principles which
underpinned the approach alongside the timetable for deliverance of the plans from
service/departmental level through to organisational level. A detailed discussion took
place in relation to timescales, resources, capacity and models of change. It was
agreed that a further progress report would be submitted in November and it was
confirmed that a workshop would take place probably in December (which would
include discussion around timescales, in order to frame and review progress).
SPPH16.82.3 In response to a question from the Health Board’s Vice Chair, it was
stated that the Health Board had been well supported by Public Health Wales in key
areas of the work. The shortage of key skills internally for overall development of the
plan was noted. Cllr P Edwards suggested that the paper could be strengthened by
the inclusion of a contextual paragraph at the beginning of the document clearly and
succinctly setting out the Health Board’s key priorities.
SPPH16.82.4 The Committee received the report and supported the principles,
approach and timetable for the operational plan development in 2017/18.
GL
SPPH16/83 Living Healthier, Staying Well: strategy development update report SPPH16.83.1 The Assistant Director of Health Strategy tabled a short presentation which supplemented the detailed report on the development of the Living Healthier, Staying Well Strategy. The report summarised the progress to date; and identified the next key stages. SPPH16.83.2 The draft timeline for the major phases of the strategy was noted. Concern was expressed about the timelines and slippage. The revised timeline would allow for full consideration of the feedback from Welsh Government engagement exercise, “Delivering a Healthier North Wales”, which closed on 18 November. The timeline and the strategy programme would be informed by the results of the Welsh Government exercise. The strategy programme was aligned with the Integrated Medium Term Plan (IMTP) Programme. SPPH16.83.3 In addition to presenting the report, the Assistant Director - Health Strategy gave a presentation on “Living Healthier Staying Well” which included strategic questions which linked with the strategic goals in relation to the strategic frameworks of the special measures areas relating to:- - Primary and Community services

4
Minutes SPPH 10.10.16 Public v0.03
- Mental Health services
- Maternity, Paediatric and Neonatal services
SPPH16.83.4 Members discussed how the Health Board would achieve and encourage culture changes in order for service users to take more responsibility for their own health. Cllr B Feeley agreed to provide some suggested wording for incorporation into the plans. It would be important to clearly articulate key messages in the front of the document. Likewise the outcomes on slide 17 could be summarised. SPPH16.83.5 The Committee received the report and the presentation and also noted
the content and provided comments accordingly.
BF
SPPH16/84 BCUHB Research and Development Strategy 2016/19 SPPH16.84.1 The Vice Chairman of the Board declared a pecuniary interest in this item as a researcher at the University of Chester. SPPH16.84.2 The Assistant Director, Research & Development presented the Strategy to the Committee explaining it set out the direction for research and development within the Health Board for the next three years. The strategy also outlined how high quality research activity and capability would be increased, and supported the creation of a workforce that operated in a research rich learning culture.
SPPH16.84.3 The Vice-Chairman of the Board expressed concern that the Strategy
was limited in terms of its focus on clinical research and development and felt that its
remit should be widened to encompass the broader responsibilities of the Health
Board in terms of population health and wellbeing and include qualitative research in
order to be more holistic.
SPPH16.84.4 The Director of Strategy explained that there were two elements and
that the framing of the document perhaps needed further examination and discussion
outside the meeting. Essentially the document intentionally focussed on the clinical
research and development with the other elements referred to being addressed
separately within the organisation within the organisation.
SPPH16.84.5 The strategy was noted with a view to further discussions taking place
as outlined above prior to its re-presentation.
LG / GL
SPPH16/85 Wylfa Newydd Project Pre-Application Consultation 2 - Update SPPH16.85.1 The Executive Director of Strategy provided an update on the Wylfa
Newydd Project Pre-Application Consultation 2 and the arrangements the Health
Board were putting in place to respond to the associated planning applications that
would follow. The Committee raised concern for the need for additional resource /
funding as the development would potentially put significant pressure on primary and
secondary care as well as ambulance services, unless adequately planned for and
resourced. The Executive Director of Strategy confirmed that there was a group which
had been established to address these issues. Impact upon the area was noted as
significant and it was proposed that the issues should be raised with Welsh
5
Minutes SPPH 10.10.16 Public v0.03
Government and possibly the UK Government in order to raise awareness of the
necessity of funding and capacity requirements. The Executive Director of Strategy
confirmed that the Health Board were working alongside local government and issues
had been flagged with the Chief Executive of Aneurin Bevan University Health Board.
It was also proposed that consideration be given to incorporating the risks associated
with the development on the Corporate Risk Register. The Executive Director of
Strategy agreed to discuss with the Executive Team.
SPPH16.85.2 The Committee agreed to note the PAC2 consultation and the
arrangements the Board had established to respond together with the on-going work
connected with the associated future planning applications.
GL
SPPH16/86 Welsh Government Consultation on the Welsh Language Standards Regulations 2016 - BCUHB Consultation Response SPPH16.86.1 The Director of Corporate Services gave an overview of the response to the consultation which was due for submission to Welsh Government on 14 October 2016. The consultation sought views on the draft Regulations to specify Welsh Language Standards for the health sector. These Regulations would enable the Welsh Language Commissioner to place duties in relation to the Welsh Language on NHS Wales Local Health Boards, National Health Service Trusts in Wales, Community Health Councils, the Board of Community Health Councils in Wales, and the NHS Business Services Authority. SPPH16.86.2 The proposed consultation response, following internal consultation had been presented to the Board Development Session on 6th October. During those discussions, Members of the board had emphasised the importance of the response being framed in a positive context to celebrate the existing achievements across North Wales. Members considered the response as drafted to be negative. It was noted that the Welsh Language Manager was redrafting the response to address the concerns raised. The Committee agreed for the Chair of the Committee in consultation with Independent Member Bethan Russell-Williams to sign off the final iteration on behalf of the Committee in order to comply with the 14th October 2016 deadline.
LM BRW
SPPH 16/87 Equality Update - Chair's Assurance Report from the Strategic Equality and Human Rights Forum SPPH16.87.1 The Executive Director of Workforce and Organisational Development provided an overview of the Chair’s assurance report and asked that the Committee note the issues of significance which had been identified by the Equality and Human Rights Strategic Forum, namely
Implementation, Accountability & Performance Management of Strategic Equality
Plan (SEP)
Assurance of how the equality duties were considered in the Programme Management Office (PMO) Processes.
SPPH16.87.2 Cllr P Edwards raised the issue of Equality Impact Assessments (EQIAs) not referring specifically to poverty but it was acknowledged that poverty was integral to the EQIA. There was a growing expectation on the transparency of
6
Minutes SPPH 10.10.16 Public v0.03
undertaking equality impact assessments and it was suggested that the Committee Business Management Group could perhaps review a full board/committee cycle to see whether they were being undertaken effectively. The Committee agreed to note the issues of significance.
DS
SPPH16/88 - Memorandum of Understanding (MOU) between BCUHB and Amrita University, India SPPH16.88.1The Executive Director of Workforce & Organisational Development
shared with the Committee the proposal which had been considered at a meeting of
the Executive Team held on the 14th September 2016 and which had been referred to
within a presentation to a Board Development session held on the 4th August 2016.
The MOU provided the architecture under which the two institutions would seek to
access the Medical Training Initiative (MTI).
SPPH16.88.2 The Executive Director of Workforce & Organisational Development
summarised that the initiative enabled suitably qualified overseas postgraduate
medical specialists to undertake a fixed period of training in the UK before returning
back to their own healthcare systems.
SPPH16.88.3 The intention was to commence with one post, reflect, adjust and
extend to other posts. Posts might be in the same specialty across BCUHB or in
different specialties on the same site.
SPPH16.88.4 A discussion took place with regards to arrangements with other
organisations and whether MOUs were in place and requested the Board Secretary to
follow this up. It was noted that the MOU could provide a model for the Health Board
to use for future projects of this kind.
SPPH16.88.5 The Committee endorsed the signing of the MOU.
GL / GLP
SPPH16/89 Review of Corporate Risks assigned to the Committee SPPH16.89.1The Executive Director of Strategy presented the report and the details of the risks which had been allocated to the SPPH Committee – namely: CRR1 Improving Population Health
CRR8 Integrated Medium Term Plan
CRR9 Primary Care Strategy
CRR14 Organisational Development
CRR15 Workforce
SPPH16.89.2 It was noted that since presentation of the Corporate Risk Register to the Board on 22nd September CRR8 had been updated and separated out into two risks and GL confirmed that CRR9 had also been updated and assigned to the Chief Operating Officer. SPPH16.89.3 The Committee considered the relevance of the current controls, reviewed the actions in place and considered whether the risk scores remained appropriate. Members emphasised the importance of ensuring that risks were being
7
Minutes SPPH 10.10.16 Public v0.03
managed at the most appropriate level and there was close monitoring of the pace of the cluster development work.
SPPH16/90 Issues of Significance to inform the Chair's Assurance Report The Chair agreed to prepare her assurance report for the board.
SPPH16/91 Any Other Business (at the discretion of the Chair) There were no matters raised under “any other business”.
SPPH16/92 Date of Next Meeting 24 November 2016, Preswylfa, Mold.
SPPH16/93 - Exclusion of the Press and Public
Resolution to Exclude the Press and Public - ''That representatives of the press and other members of the public be excluded from the remainder of this meeting having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest in accordance with Section 1(2) Public Bodies (Admission to Meetings) Act 1960.''
Note: This item together with the closed session item on Berwyn Healthcare Project were taken at the beginning of the meeting.

2 SPPH16.201 Summary Action Log Public.docx
- 1 -
16/11/2016 12:06
BCUHB STRATEGY PARTNERSHIPS& POPULATION HEALTHCOMMITTEE – Summary Action Plan Public Version – last updated 16/11/2016 12:06 (incorporating outstanding actions from the Strategy, Planning and Partnerships Sub-Committee at the point it was disbanded at the end of February 2016)
Officer/s
Minute Reference and summary of action agreed
Original Timescale
Latest Update Position Revised Timescale
26 May 2016
Chris Wright
SP16/52 Implementation of Carers Strategies Annual Report – further report back to Committee in the Autumn.
November
Update to be presented to November Committee
Andrew Jones/Geoff Lang
SP16/55 Housing and Health Working Together – Further report including other initiatives such as 2025 to be presented examining the work in the wider context of how it is mainstreamed within the HB. Also to provide further information on why BCU area has above average winter deaths.
July Update to October meeting November
10 October2016
Geoff Lang SPPH16/80.3 – Collaboration with Bangor University. Progress report tobe prepared for the January SPPH Meeting.
January
Geoff Lang SPPH16/82.2 – Planning for 2017/18 – Draft Principles. Further progress report to be submitted in November and a workshop to take place probably in December.
November / December
Sally Baxter SPPH16/83.4 – Living Healthier, Staying Well: Strategy development update report. Cllr B Feeley agreed to provide some suggested wording for incorporation into the plans. SB to liaise.
November
Lynne Grundy / Geoff Lang
SPPH 16/84.4 BCUHB Research and Development Strategy 2016/19 –Framing of
November

- 2 -
16/11/2016 12:06
the document to be re-examined prior to representation.
Geoff Lang
SPPH16/85.1 Wylfa Newydd Project Pre-Application Consultation 2 – update. Consideration to be given to incorporating the risks associated with the development on the corporate risk register. GL to discuss with the Executive Team.
November
Lynne Meadows / Bethan Russell-Williams
SPPH16/86.2 Welsh Government Consultation on the Welsh Language Standards Regulations 2016 – BCUHB Chair of the Committee in consultation with Independent Member BRW to sign off the final iterations on behalf of the Committee.
14thOct 2016 Action completed. Close
Dawn Sharp SPPH 16.87.2 Equality Update The Committee Business Management Group could perhaps review a full Board/Committee cycle to see whether EQIA’swere being undertaken effectively.
November On agenda for CBMG to discuss at November Meeting.
Close
Geoff Lang / Grace Lewis-Parry
SPPH16.88.4 – Memorandum of Understanding (MOU) between BCUHB and Amrita University India.Board Secretary to ensure that MOUs were in place for other similar arrangements and held centrally. The MOU could provide a model for the Health Board to use for future projects of this kind.
November A Central register is held by the Board Secretary’s Office of similar formal agreements/MOUs
Close

2.1 SPPH16/202 Betsi Cadwaladr University Health Board Multi-Agency Resilience – Vulnerable Person Process
1 SPPH16.202 Vulnerable person coversheet.docx
1
Strategy, Partnerships & Population Health Committee 24.11.16 Item SPPH16.202
To improve health and provide excellent care
Title: Betsi Cadwaladr University Health Board Multi-Agency Resilience –Vulnerable Person Process
Author: Mr John Darlington, Assistant Director, Corporate Planning
Responsible Director:
Mr Geoff Lang, Executive Director of Strategy
Public or In Committee
Public
Strategic Goals (Indicate how the subject matter of this paper supports the achievement of BCUHB’s strategic goals –tick all that apply)
1. Improve health and wellbeing for all and reduce health
inequalities
2. Work in partnership to design and deliver more care
closer to home
x
3. Improve the safety and outcomes of care to match the
NHS’ best
4. Respect individuals and maintain dignity in care x
5. Listen to and learn from the experiences of individuals
6. Use resources wisely, transforming services through
innovation and research
x
7. Support, train and develop our staff to excel.
Approval / Scrutiny Route
The content of this paper has been discussed at Executive Management Group and supported prior to presentation to the Committee.
Purpose: To brief the Committee regarding a new process for collaboration to identify and support vulnerable people during emergency events such as flooding.
Significant issues and risks
A multiagency Vulnerable Person Process has been developed with our partners and through the support from our Joint Resilience Unit and colleagues from across the Health Board. This forms part of our planned programme of resilience to best target limited rescue assets during an emergency
North Wales has seen a number of significant flooding events in recent times, one of which resulted in the tragic loss of life for an elderly resident in our community. This event drove North Wales Police and the Local Resilience Forum to consider how it can best target limited rescue

2
assets during an emergency to support people who have pre-existing vulnerabilities or become vulnerable due to the increased threat posed by the emergency. The Vulnerable Person’s Process aims to provide a robust, reproducible and safe mechanism which allows the Health Board to inform the rescue operation, where evacuation is a key tactical option in the protection of the public.
Special Measures Improvement Framework Theme/ Expectation addressed by this paper
The content of this paper does not address special measures requirements.
Equality Impact Assessment
Recommendation/ Action required by the Committee
It is recommended that the Committee receive the Vulnerable Persons Process and note that this will be in operation for the coming winter period for any potential emergencies occurring as a result of severe weather.
Disclosure: Betsi Cadwaladr University Health Board is the operational name of Betsi Cadwaladr University Local Health Board
Committee Coversheet v10 June 2016
2 SPPH16.202 Vulnerable person protocol.doc
1
Betsi Cadwaladr University Health Board Multi-Agency Resilience – Vulnerable Person Process
1. Purpose of report
To brief the Strategy, Partnerships & Population Health Committee regarding a new process for collaboration to identify and support vulnerable people during emergency events such as flooding.
2. Introduction/Context
Betsi Cadwaladr University Health Board is categorised within the Civil Contingencies Act (2004) (CCA) as a “Category 1 Responder” thereby required to meet the full legislated duties, as well as the non legislated requirements set out within the NHS Wales Emergency Planning Core Guidance (April 2015). The developments above support the Health Board achieve compliance with the Act specifically in regards to:
1. The duty to assess risks within our local communities 2. The duty to co-operate with other local responders 3. The duty to have in place arrangements to mitigate business disruption
3. Main body of the report
A multiagency Vulnerable Person Process has been developed with our partners and through the support from our Joint Resilience Unit and colleagues from across the Health Board. This forms part of our planned programme of resilience to best target limited rescue asset during an emergency. Vulnerable Person Process North Wales has seen a number of significant flooding events in recent times, one of which resulted in the tragic loss of life for an elderly resident in our community. This event drove North Wales Police and the Local Resilience Forum (LRF) to consider how it can best target limited rescue asset during an emergency for people who have pre-existing vulnerabilities or become vulnerable due to the increased threat posed by the emergency. The outcome of which has been to develop a web based tool that allows the Police to co-ordinate the rescue efforts of Fire and Rescue, Mountain Rescue, Royal National Lifeboat Institute and others who provide a capability to rescue victims where evacuation is required. A critical success factor is the ability to target the rescue teams to persons who are known to agencies such as health, social care and others including utility providers, which relies upon the exchange of information between agencies. The Vulnerable Person’s Process (Appendix 1) aims to provide a robust, reproducible and safe mechanism which allows the Health Board to inform the rescue operation, where evacuation is a key tactical option in the protection of the public. The process recognises the sensitivities of sharing health data and therefore
2
challenges the need for sharing data but also recognises that there is an information sharing protocol in existence between the LRF partners and an expectation within the CCA legislation that information sharing will take place in response to an emergency. In developing the process consultation has taken place with key members of the Health Board including information governance, informatics, operations and information communication technology. Colleagues have also participated in tests of the arrangements described.
6. Conclusions / Next Steps
In conclusion this paper describes the work developed by the Joint Resilience Unit which aims to enhance the Health Boards preparedness and ability to react to an increase in multi-agency coordination and response to an emergency.
7. Recommendations
It is recommended that the Committee receive the Vulnerable Persons Process and note that this will be in operation for the coming winter period for any potential emergencies occurring as a result of severe weather.
3
Appendix 1 Vulnerable Persons Process Specific arrangements to support the provision of information where evacuation is a key tactic in the protection of the public during and emergency.
Responsible Manager: Mr. Geoff Lang, Executive Director of Strategy Issues: Draft 0.4 Date: Sept 2016 Review: Sept 2019
Introduction Certain emergencies will pose a significant threat to the safety of the public requiring support to evacuate the immediate vicinity, such as the 2013 flooding in St Asaph or the tidal surge and sea defence failure in Rhyl in 2015. Though there is no legal premise or powers which law enforcement agencies can use to evacuate a resident, in this type of emergency, there is a clear duty of care owed by agencies to ensure the public are informed of the risks and where necessary aided to evacuate if desired. Furthermore, the limited capacity to aid evacuation particularly where the threat is imminent requires rescue agencies to prioritise their resources and focus on those with the greatest vulnerability. As a result North Wales Police have developed an ICT system which can be used to coordinate the rescue of victims from an emergency where evacuation is a tactical option. However, for this system to be truly effective it is dependent on data relating to those individuals who may be at greater risk due to pre-existing risk factors thus increasing their vulnerability. The Health Board along with Local Resilience Forum partners such as Social Services may be asked to share information relating to persons who could be at risk in such a situation. The following process sets out a mechanism where this information can be accessed and shared in a way that is safe and in keeping with the principles set out in the Wales Accord on the Sharing of information. However to achieve this, the Health Board MUST be assured that it is accessing and sharing information in the interests of public safety and only where there is a genuine threat to the safety of our communities. Therefore, those persons identified within the process map must feel confident in challenging any request for data and satisfied that they and the Health Board are acting in the best interests of patient’s safety whilst balancing this against their right to privacy.
4
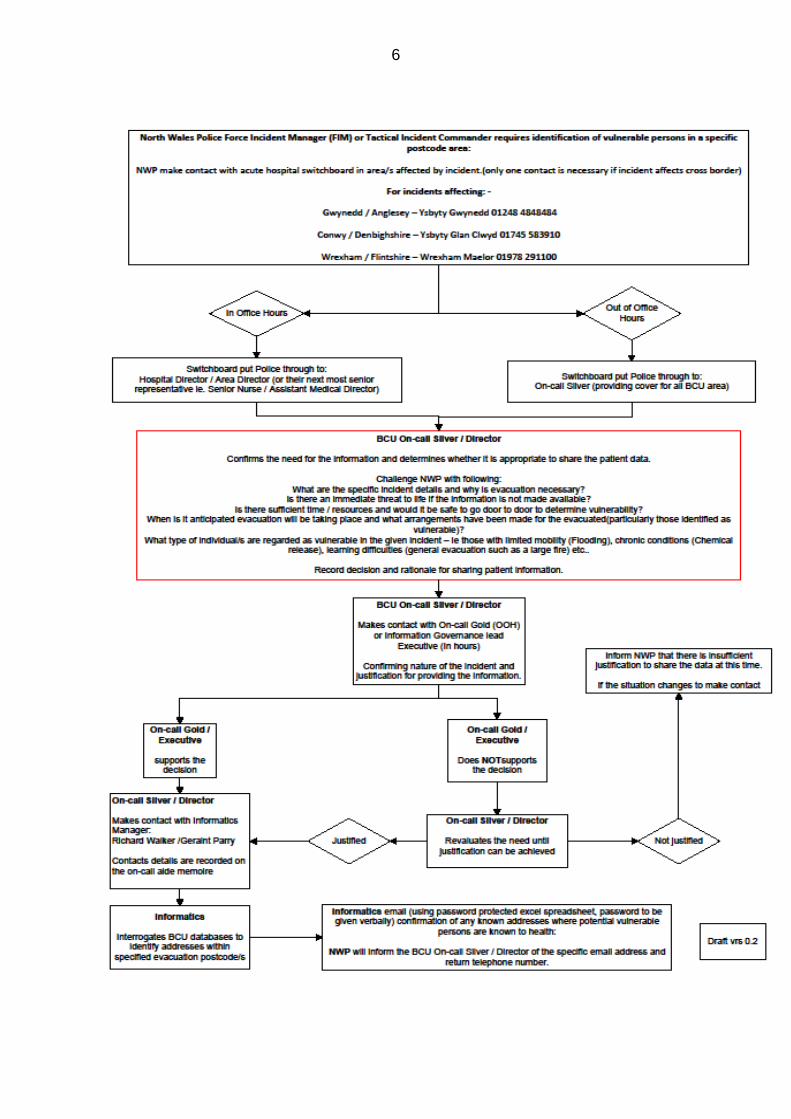
Process: Hospital Switchboard
1. North Wales Police will make contact with the Hospital Switchboard closest to
the incident site.
2. The switchboard operator when asked by North Wales Police to speak with
the Silver put them through to: -
in-hour to either the Hospital Director or Area Director (if neither are
available their most senior representative ie Assistant Director Nursing
/ Operations or Assistant Medical Director)
out of hours to the on-call Silver.
Hospital Director / Area Director
1. On notification the Hospital/Area Director or Silver On-call must satisfy
themselves that there is a legitimate and time imperative need to share
information with North Wales Police. It is unlikely that the NWP Officer who
makes first contact will be of sufficient seniority or have adequate knowledge
of the emergency to fully answer your challenge, however, they will provide
you with the contact details of the most senior officer (likely to be a Silver
Commander or Force Incident Manager) who will. You will need to confirm
their contact details and make contact with them.
2. On contacting the Silver Commander/Force Incident Manager seek
confirmation to the following in order that you can make an informed decision.
What are the specific incident details?
Why is evacuation necessary?
Is there an immediate threat to life if the information is not made available?
Is there sufficient time or resources, and would it be safe to go door to
door, to determine vulnerability?
When is it anticipated evacuation will take place?
What arrangements have been made for those evacuated particularly
those identified with health needs? – Consider what impact this may have
on BCU and what actions you need to take.
What type of individuals are regarded as vulnerable in the given
emergency – ie those will limited mobility (flooding), chronic conditions
(chemical release), learning difficulties (general evacuation such as a large
fire) etc.
5
3. Confirm the name and rank of the Senior Police Officer, contact details and
record their responses to each of your challenges.
4. Implement any actions that need to be taken by the Health Board to prepare
for the emergency, for example providing community staff to support those
with health needs being evacuated, ensuring community teams are informed
of the incident, implement business continuity arrangements to protect Health
Board services, escalate preparedness in preparation for receiving casualties
from the emergency and attend any multi-agency command centres or
activate health command arrangements.
5. Once satisfied there is adequate justification to share the information, inform
the BCUHB On-call Gold and confirm with them your justification and reason
to share the information. If supported by Gold move to the next step. If not
supported by Gold seek additional justification from North Wales Police.
6. Make contact with the informatics team and inform them of the need to send
vulnerable persons data to North Wales Police along with the email address
for the destination: -
Richard Walker: xxxxxx Geraint Parry : xxxxxx
7. Confirm with the Silver Commander / Force Incident Manager whether the
incident needs additional health board involvement.
Informatics Team
1. On notification from the Hospital / Area Director or on-call Silver access
Health Board databases relevant to the postcode area for the affective
evacuation zone/s and identify those who may be regarded as vulnerable.
2. Export the agreed patient identifiable information of those regarded as
vulnerable onto a password protected Excel Spreadsheet and email this to the
contact email address provided by North Wales Police.
3. Make contact with North Wales Police preferably by telephone to inform them
of the Excel spreadsheet password.
4. Inform the Health Board Hospital / Area Director or on-call Silver that the data
has been forwarded and received by North Wales Police.
6
7
Frequently Asked Questions: Q. Is the Health Board, and therefore am I, permitted to share this data as it is potentially patient sensitive? A. Yes: the Health Board has in place an information sharing protocol with our Local Resilience Forum partners which assists us with achieving the expectations to co-operate and share information in an emergency, in its self a duty placed on the Health Board by the Civil Contingencies Act (2004). Furthermore, by challenging the need for the information as described in the process reasonable steps are being taken to justify the need. Q. What will happen if justification cannot be achieved to sharing the information requested? A. The rescue and evacuation will continue, though rescue services will need to go door-to-door, which may delay the effectiveness of the response. Q. What should I do if I cannot get hold of the Senior Police Officer? A. If repeated attempts to contact have failed then make contact with the Force Incident Manager, which is a role that is covered 24/7 in the Force Control Room tel: xxxxxx (this is a confidential number). Remember to record the times when you attempted to make contact. Q. What should I do if I cannot get hold of BCU Informatics/ Gold on-call? A. Request Switchboard to find an alternative number. Q. What information will be shared? A. The Health Board will only share vary basic information indicating those patients who have been recently discharged from hospital, in descending age order at an address within the postcode area of the emergency incident. The Health Board will not provide information relating to the patient’s clinical condition or treatment. Q. How will the information be shared? A. Informatics will send, by email, a password protected spreadsheet to a specific recipient at North Wales Police who has been trained in the evacuation software and information governance. Informatics will make separate contact with North Wales Police to inform them of the password. Q. What should I do if I have concerns about the health needs of those persons being evacuated? A. Discuss these concerns with the Senior Police Officer and work with them to create a plan which supports these needs, which could include for example sending GPs and or Community Nursing Staff to a Rest Centre. Q. Should I record my decision to share information? A. Yes: It is imperative that all decisions and the rationale for them, including the one to share information, are recorded in fulfilling on-call duties. It is likely that there will be a post incident investigation which could lead to some form of enquiry and you may be required to attend to present evidence.
3.1 SPPH16/203 Seasonal Plan 2016-17
1 SPPH16.203 Seasonal Plan_coversheet.docx
1
Strategy, Partnerships & Population Health 24.11.16 Item SPPH16.203
To improve health and provide excellent care
Title: Seasonal Plan 2016/17
Author: Mr Rob Smith, Area Director (East)
Responsible Director:
Ms Morag Olsen, Chief Operating Officer
Public or In Committee
Public
Strategic Goals (Indicate how the subject matter of this paper supports the achievement of BCUHB’s strategic goals –tick all that apply)
1. Improve health and wellbeing for all and reduce health
inequalities
2. Work in partnership to design and deliver more care
closer to home
3. Improve the safety and outcomes of care to match the
NHS’ best
4. Respect individuals and maintain dignity in care
5. Listen to and learn from the experiences of individuals
6. Use resources wisely, transforming services through
innovation and research
7. Support, train and develop our staff to excel.
Approval / Scrutiny Route
Discussed at Executive Management Group
Purpose: The paper sets out the Health Board and local partnership plan to deliver and develop unscheduled care services throughout the winter period of 2016/7. The paper is a requirement of Welsh Government and also an important part of the Health Board planning process. The document has been developed in collaboration with Local Authorities and Wales Ambulance Services Trust (WAST).
Significant issues and risks
The plan is intended to address the risks created by seasonal pressures (see the document) In terms of delivery risks, there are challenges in recruitment to the various elements of the plan.
Special Measures Improvement
The paper describes services being developed in line with the Framework intention of “Providing Care Closer to home”

2
Framework Theme/ Expectation addressed by this paper
Equality Impact Assessment
The changes described represent developments of existing services and there are no budget reductions/
Recommendation/ Action required by the Committee
The Committee is asked to note for information
Disclosure: Betsi Cadwaladr University Health Board is the operational name of Betsi Cadwaladr University Local Health Board
Board Coversheet v8.0 June 2016
2 SPPH16.203 Seasonal Plan Version 3.docx
Seasonal Plan Version -1.02
North Wales Health and Social Care
Seasonal Plan - 2016-17
Ymddiriedolaeth GIG
Gwasanaethau Ambiwlans
Cymru
Welsh Ambulance Services
NHS Trust

Seasonal Plan Version -1.02
Contents
1. Introduction 2. Assessment of At Risk Groups of the Population & Seasonal Plan Performance 3. Identified Risks to Seasonal Plan 4. Capacity & Demand Analysis 5. The Operational Plan 6. Summary of Initiatives to resolve Demand/Capacity 7. Managing the effect of Christmas and New Year 8. Managing Infections and Immunisation 9. Partnership Working 10. Escalation Plan 11. Workforce 12. Financial Implications

Seasonal Plan Version -1.02
1. Introduction and Seasonal Planning Priorities
This document sets out the North Wales Health Board’s seasonal planning and delivery arrangements 2016/17. The plan identifies the at risk population groups, risks to achieving the required standards, a capacity and demand assessment and a description of the system changes that will ensure that unscheduled care standards will be improved.
Pressures within the unscheduled care system lead to delays in treating people in urgent need; it is therefore essential that unscheduled care system works effectively at all times. Through working together with partner organisations, the Health Board aims to ensure residents of North Wales can access high quality timely healthcare when in urgent need, throughout the winter and during forecast periods of pressure.
The plan therefore reflects a whole system approach to the delivery of services over the forthcoming winter period. It builds upon local risk assessments and lessons learnt over recent years and in particular, from winter 2015/16, and sets out the key actions being taken in response. The waiting time at hospital, measured by the 4 hour wait and 12 hour wait as well as ambulance handover delays, are good indicators of system pressure and the ability of the system to cope with demand. For individual patients, delays at hospital can cause distress and may in some cases affect treatment outcomes or length of time within hospital. Delays at hospital therefore drive the urgency for improvement in the unscheduled care system and improvement and will be measured by the 4 hour and 12 hour target performance. Area Teams, Mental Health & Learning Disabilities and Secondary Care Teams have identified the priority themes for improvement, and integrated groups have been introduced to facilitate and improve joint working. The plan has been jointly developed in partnership with WAST and Local Authorities, and this joint work will continue as we implement improvements across the system of care. In addition, the NHS Wales Delivery Unit has been providing targeted support for teams on discharge processes and acute care flow, and this support continues. Projects on reducing length of stay within our hospitals and embedding Expected Date of Discharge in all wards and developing the Single Point of Access (SPOA) model are examples of schemes in place to improve patient care.
1.1 Development and Implementation of the Model
The model and plan for unscheduled care has been informed by a combination of national guidance, Health Board Strategy, responding to local population needs and specific local issues being addressed across North Wales. The principles behind our model of care places the patient or service user at the centre of everything we do, aims to improve care co-ordination and integrated services with our partners, (Care Closer to Home) and supported by a strong programme of prevention and community development Our model therefore supports patients and professionals to navigate around a complex system to find out the right information, care or service and to ensure that health or care need is identified early before a crisis occur.
BCU is also working closely with other Health Boards across Wales as part of the all Wales Unscheduled Care Board and Emergency Ambulance Services Collaborative Commissioning programme. These arrangements aim to improve our system response to managing emergency/ unscheduled Care over 2016/17. In addition, we will be preparing for the introduction of 111 in Autumn of 2017 which will be informed by the pilot and learning from ABMU Health Board as the pathfinder site for 111 and clinical triage.

Seasonal Plan Version -1.02
Our local plans also align with the all Wales framework which utilises a patient-centred unscheduled health and care patient pathway. The following 10 step model describes the Programme’s expectations for delivery of these services to citizens who access them in Wales.
Step 0 - Help to keep me independent Step 1 – Help me choose Step 2 – Answer my call Step 3 – Come to see me Step 4 – Give me treatment Step 5 – Take me to hospital Step 6 – Assess me Step 7 – Provide me with my diagnosis Step 8 – Give me treatment Step 9 – Discharge me from hospital Step 10 – Ensure my continuing care is effective
The model builds on the 10 steps, focuses on the major priorities, and is intended to provide a context for urgent improvement in each of the elements of the model. WAST play an important role in all stages of the patient pathway, and are key partners in these programmes of work.
1.2 The Annual Operating Plan The Operating Plan sets out key actions being taken by the Health Board to improve Unscheduled Care services over the 2016/17 period. This Seasonal Plan describes the very specific and enhanced actions being taken over the seasonal (winter) period and therefore comprises planned improvements already described in the Operational Plan plus additional specific measures to manage Seasonal pressures. The Annual Operational plan provides the metrics for planned improvement. Supporting metrics of reduced admissions and ALOS enablers for improved Unscheduled Care Performance will drive improvements in the experience of patients (measured by the 4 hour target) .Many of the changes will require Area, Mental Health and Secondary Care teams working with WAST, Local Authorities and others partners, not only to ensure whole system resilience but also to draw on experience across North Wales.
1.3 Culture and Communications The improvements in systems set out below will be supported by a communications strategy to ensure “buy in” for the concepts involved. In order to achieve reduced waiting times, secondary and community hospital wards must have beds available at all times. Creating a new “norm” where this is the case will require changes in behaviour in addition to the system improvements. Clinical leadership is paramount to develop the pathways and lead the changes required across the
system.
1.4 Project Management and Governance
The Unscheduled Care transformation group will lead and oversee the programme and delivery of this plan, supported by three health community unscheduled care groups in East, Central and West. This multi-agency approach facilitates working in partnership with Third Sector, Independent Sector and Local Authority partners alongside BCU Health Board Area teams, Secondary Care and Mental Health teams.

Seasonal Plan Version -1.02
2. At Risk or Vulnerable Groups
As part of the context for the Seasonal plan, it is important to understand our populations who are most at risk from winter conditions and to ensure that services changes are targeted to support these sections of the population. In seasonal (winter) planning, the term “vulnerable group” refers to sections of the population particularly at risk, marginalised or under-provided for. During the winter season, these groups may be particularly vulnerable as health and social care resources are more likely to be directed into mainstream approaches to meet the needs of the general population. Extremes in temperature have been shown to have a detrimental on health and wellbeing with higher mortality, morbidity and hospital admissions all occurring in the winter months. As an indicator, “Excess winter deaths” is defined as the difference between the number of deaths in the four winter months (December – March) and the average number of deaths during the preceding four months and the following four months. In the UK as a whole, excess winter deaths represent 5% of all deaths per year and amount to an average of 27,000 additional deaths in winter, as compared with the summer months. The Excess Winter Mortality (EWM) index is produced so that comparisons can be made between sexes, age groups and regions, and is calculated as the number of excess winter deaths divided by the average non-winter deaths, expressed as a percentage. For example, an EWM index of 20 shows that there were 20 per cent more deaths in winter compared with the non-winter period. In 2013/14, Table 1 shows that the EWM Index for Isle of Anglesey (17.2), Denbighshire (22.3) and Wrexham (19.0) Unitary Authorities were all statistically significantly higher than the average for Wales (10.3). The EWM Index has fluctuated across all Unitary Authorities between 2011/12 and 2013/14.
Table 1: Excess winter mortality, Wales and unitary authorities,
2011/12 to 2013/14
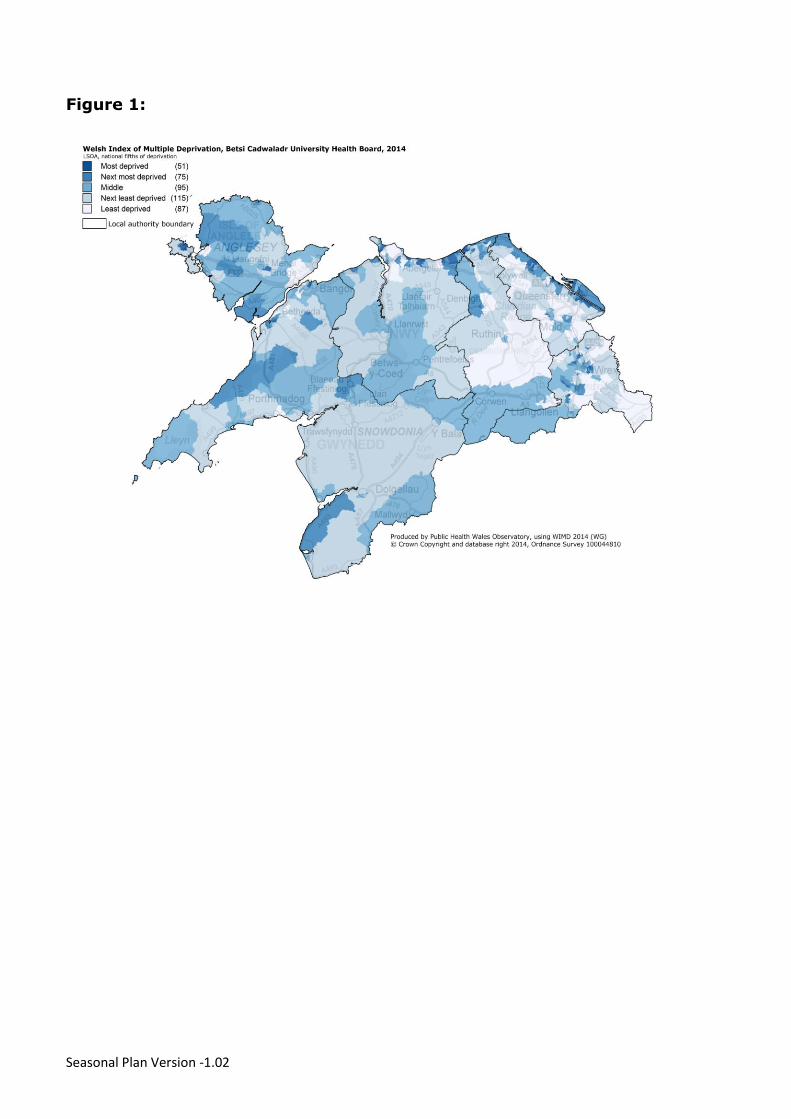
Although EWM is associated with low temperatures, conditions directly relating to cold, such as hypothermia, are not the main cause of excess winter mortality. The majority of additional winter deaths are caused by cerebrovascular diseases, ischaemic heart disease and respiratory diseases. Exposure to cold also increases an individual’s risk of injury from fires and falls, contributes to mental health problems, increases social isolation and has a negative impact on the education of children where houses are not properly heated. During a flu outbreak, which is far more likely to occur in the winter months, large proportions of the population are at risk of infection. However, based on the characteristics of the flu, it is known that certain people are more at risk of developing serious illness if infected. These people are considered to be medically at risk. However, some people may face additional challenges depending on their socio-economic status, factors related to the social determinants of health (e.g. lack of housing, education, employment) and possibly pre-existing chronic conditions. In the future, risk prediction/ stratification tools will help to identify these individuals at risk. Figure 1 shows the distribution of material deprivation across North Wales.
EWD Index LCL UCL EWD Index LCL UCL EWD Index LCL UCL
Wales 1,260 12.8 12.1 13.5 1,850 18.1 17.3 18.9 1,010 10.3 9.7 10.9
Isle of Anglesey -10 : : : 40 13.1 8.8 17.3 40 17.2 12.0 22.5
Gwynedd 90 23.8 18.9 28.8 100 23.7 19.0 28.4 20 5.7 3.3 8.0
Conwy 20 4.6 2.7 6.5 70 15.5 12.0 19.1 20 3.3 1.7 5.0
Denbighshire 60 16.0 11.8 20.2 50 13.2 9.5 16.9 80 22.3 17.4 27.2
Flintshire 70 16.4 12.7 20.2 130 28.0 23.1 32.8 60 14.6 10.9 18.3
Wrexham 50 12.2 8.8 15.6 110 27.5 22.4 32.7 80 19.0 14.8 23.2
2011/12 2012/13 2013/14
Seasonal Plan Version -1.02
Figure 1:

Seasonal Plan Version -1.02
2.1 Older People
Older people can be particularly vulnerable regardless of their social background. They may require ongoing specialised medical care because they are unstable or need end of life care. The may need specific support in order to achieve or maintain independence in daily activities, including supply of consumable medical supplies or equipment (e.g. oxygen) or accessing a carer’s assistance. Lastly, frail or housebound older people may need ongoing supervision from health and social care services.
2.2 Those with an underlying physical or mental health condition
In Wales and across the UK, flu vaccination is routinely offered to people considered to be more at risk of complications from flu. This includes those who:
are aged 65 and over
have a chronic heart condition
have a chronic chest complaint, including asthma which requires regular medication
are pregnant
are living in long-term residential or nursing home Individuals with morbid obesity (BMI >40) have also been found to be at higher risk of complications if they catch flu, so it is recommended this group also receive annual flu immunisation. Additionally, frontline healthcare workers, frontline social care workers, carers, volunteer carers, and members of a recognised voluntary organisation who provide planned emergency first aid at organised public events, and members of the Welsh Ambulance Service Trust community first responder scheme providing first aid directly to the public are also offered vaccination against flu.
2.3 Those who live in poor housing or are homeless
These are largely those in older, energy inefficient or exposed properties. Excess winter mortality is linked to poorly heated housing and low household income. Those living in deprived communities are more likely to have many of the risk factors for seasonal excess deaths and ill health. (this section will be further developed to include a ward breakdown of homelessness/poverty)
2.4 Those living in fuel poverty
Fuel poverty is defined as the inability to obtain adequate energy services for 10 per cent of one’s income. This results from low income and/or fuel inefficiency. Many people on low incomes live in disadvantaged areas with dilapidated and poorly insulated housing, which is relatively expensive to heat. Fuel poverty presents serious health risks for many households in the UK every winter with cold homes contributing to excess winter mortality and to a range of symptomatic illness. People experiencing fuel poverty have various strategies for coping, for example heating only the main living room. This can result in social problems for the household including lack of privacy for individuals and limited opportunity for children to do homework undisturbed.
The Buildings Research Establishment (for Welsh Government) estimated in 2008 that there were 75,000 households in North Wales living in fuel poverty, representing 28% of all households.

Seasonal Plan Version -1.02
2.5 Implications for the Seasonal Plan
It is clear from the preceding analysis that there sections of the population that are more vulnerable from the effects of winter; the elderly, people with underlying health conditions, people living in poverty and vulnerable to fuel poverty. Section 5 of our plan sets out the coordinated actions being taken with partners across the whole system to meet the specific needs of our population
Seasonal Plan Version -1.02
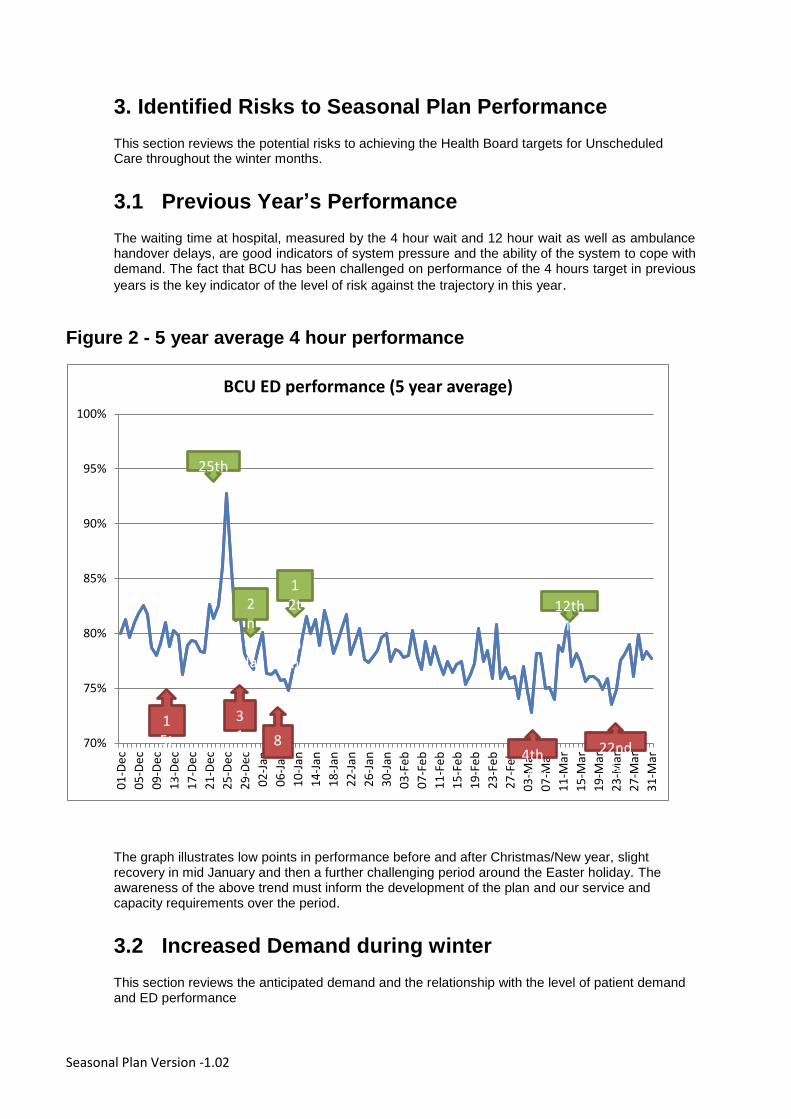
3. Identified Risks to Seasonal Plan Performance
This section reviews the potential risks to achieving the Health Board targets for Unscheduled Care throughout the winter months.
3.1 Previous Year’s Performance
The waiting time at hospital, measured by the 4 hour wait and 12 hour wait as well as ambulance handover delays, are good indicators of system pressure and the ability of the system to cope with demand. The fact that BCU has been challenged on performance of the 4 hours target in previous
years is the key indicator of the level of risk against the trajectory in this year.
Figure 2 - 5 year average 4 hour performance
The graph illustrates low points in performance before and after Christmas/New year, slight recovery in mid January and then a further challenging period around the Easter holiday. The awareness of the above trend must inform the development of the plan and our service and capacity requirements over the period.
3.2 Increased Demand during winter
This section reviews the anticipated demand and the relationship with the level of patient demand and ED performance
70%
75%
80%
85%
90%
95%
100%
01
-De
c
05
-De
c
09
-De
c
13
-De
c
17
-De
c
21
-De
c
25
-De
c
29
-De
c
02
-Jan
06
-Jan
10
-Jan
14
-Jan
18
-Jan
22
-Jan
26
-Jan
30
-Jan
03
-Fe
b
07
-Fe
b
11
-Fe
b
15
-Fe
b
19
-Fe
b
23
-Fe
b
27
-Fe
b
03
-Mar
07
-Mar
11
-Mar
15
-Mar
19
-Mar
23
-Mar
27
-Mar
31
-Mar
BCU ED performance (5 year average)
8
12th Jan
15th Dec
25th Dec
12th Mar
4th Mar
22nd Mar
31st Dec
2nd Jan

Seasonal Plan Version -1.02
Figure 3 - ED Demand and Performance
The graph shows a very slight increase in admissions in December and no increase in attendances over the period. The graph would appear to suggest that demand is relatively consistent and does not indicate a strong correlation between demand and performance. There is strong perception within the hospitals that acuity is increasing, probably as a result of success of admission avoidance programmes. There is however, no evidence to support this perception. However, the pattern and frequency of admissions is also a factor with an increase of attendances around particular dates causing stresses in the system. The following graph reviews ambulance arrivals by day.
0
2000
4000
6000
8000
10000
12000
14000
16000
50%
60%
70%
80%
90%
100%
Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16
BCU ED 4 & 12 Hour Performance
Total Attendances Inpatients - Admissions via ED
4 Hr % Performance 12 Hr % Performance
Seasonal Plan Version -1.02
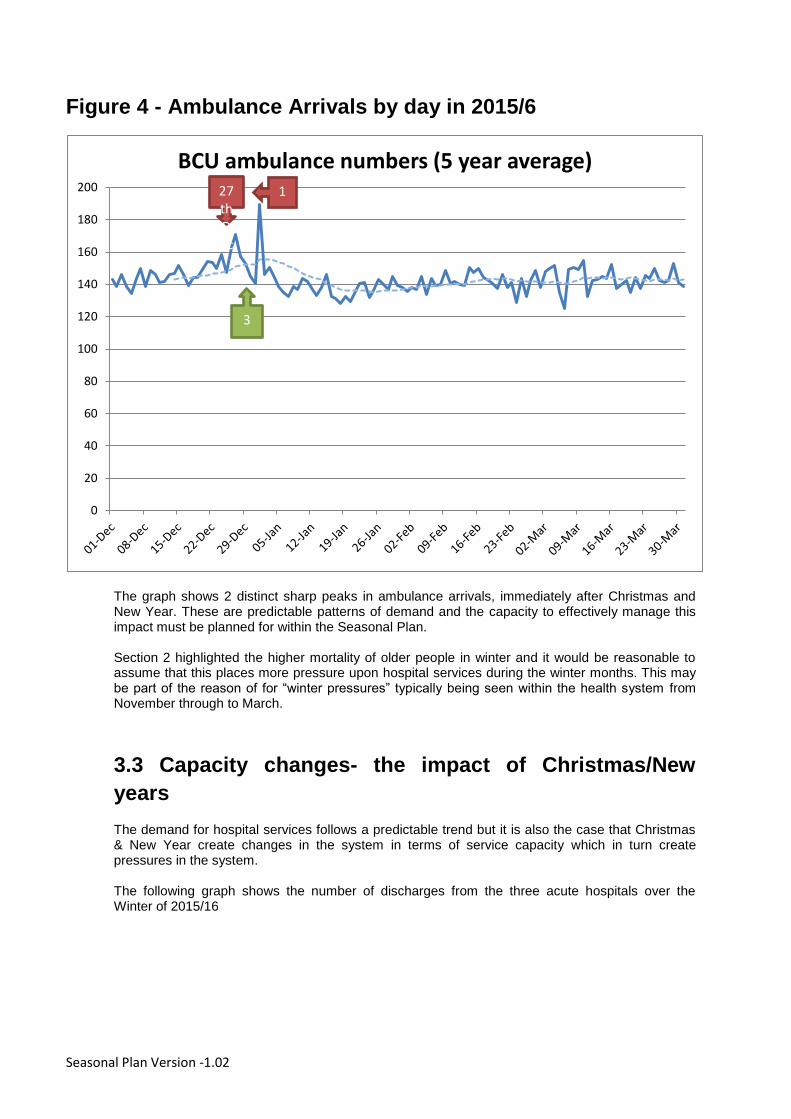
Figure 4 - Ambulance Arrivals by day in 2015/6
The graph shows 2 distinct sharp peaks in ambulance arrivals, immediately after Christmas and New Year. These are predictable patterns of demand and the capacity to effectively manage this impact must be planned for within the Seasonal Plan. Section 2 highlighted the higher mortality of older people in winter and it would be reasonable to assume that this places more pressure upon hospital services during the winter months. This may be part of the reason of for “winter pressures” typically being seen within the health system from November through to March.
3.3 Capacity changes- the impact of Christmas/New
years
The demand for hospital services follows a predictable trend but it is also the case that Christmas & New Year create changes in the system in terms of service capacity which in turn create pressures in the system.
The following graph shows the number of discharges from the three acute hospitals over the Winter of 2015/16
0
20
40
60
80
100
120
140
160
180
200
BCU ambulance numbers (5 year average)
3
27th Dec
1

Seasonal Plan Version -1.02
Figure 5 - Hospital Discharges throughout the Winter of
2015/6
The graph illustrates the effect of the holiday break. Discharges from hospital reduce sharply at Christmas and the New Year. In a health system that is already running at full capacity, the shock to capacity has a significant effect on performance. There is a strong correlation between these holidays and 4 hour performance. Following the New Year period, the system takes time to adapt and struggles to recover through the rest of the winter. The graph also indicates that the increase in discharges from hospital prior to Christmas may be overstated It is a widely held view that transfers out of hospital increase prior to Christmas. The graph indicates that, while there was an increase before Christmas, this actually follows a dip in the preceding week. The average over the two weeks is close to normal but the activity is focussed on the days prior to Christmas. The combined effect of the above impacts create the “perfect storm” feeling within the Acute sites in early January; a sudden increase in demand following a period of reduced discharges leading to severe capacity issues. The challenge that this analysis provides however is that these trends are predictable: activity over the winter period is not expected to increase and spikes in activity follow a known and predictable pattern. The Seasonal plan should therefore focus on planning to reduce the impact of these factors.
0
200
400
600 BCU Discharges

Seasonal Plan Version -1.02
3.4 Current Performance
The following graph illustrates the 4 hours performance from April to October
The graph shows a reduction in performance in early summer followed by a gradual sustained
increase through July to October. The performance level is below the trajectory agreed with Welsh
Government (85%) but there are encouraging signs that the ride range initiatives in place to
improve unscheduled care are of starting to take effect.
3.5 Review of analysis and mitigation of risks
Two key risks emerge from the analysis and both need clear mitigation plans in order to improve performance throughout the winter.
3.6 Baseline capacity/demand- Current performance
Actions to mitigate the Baseline risk- The level of bed occupancy must be reduced prior to December in order to enable performance to be maintained/improved. This baseline improvement will be achieved through the actions within the Operational Plan (see section 5 and 6) and the actions to recover current performance.
Actions to mitigate the Winter effect risk- The “Christmas effect” on capacity and the sudden spikes in activity require a range of further actions to mitigate. The system requires appropriate levels of capacity within services to be able to cope with these impacts and a full range of measures in place to reduce the impact of the variation e.g. management of leave over Christmas and as normal as possible discharge processes in place on all days. This work involves working with partner agencies and the Local Authorities in particular to ensure that services within primary care, community and hospital settings are maintained as close to normal as possible.

Seasonal Plan Version -1.02
4. Capacity Modelling
Capacity planning analysis has been carried out in conjunction with the development of the Operational and Seasonal Plan. The aim of this work is to review the balance of bed capacity and demand on the acute hospital sites and to identify the scale of the changes required to address any gaps. The following section, section will set out the changes planned to address these gaps. The following graph illustrates the summary of the detailed capacity and demand analysis carried out across the three acute hospital sites. The graph is intended to be illustrative of the detailed analysis carried out in the capacity plan. The full capacity plan is contained in a separate document. The graphs compare the beds equivalent capacity required to achieve 85% and 90% occupancy, including other known capacity pressures. The aim is to achieve a consistent level of occupancy of 85% in line with good practice guidance. This level of occupancy would effectively mean that there is a beds available for each new admission.
Figure 6 - Demand and capacity for Acute sites
The gap between the above line (beds required for 85%) and the below line (bed capacity) illustrates that there is currently insufficient capacity. However, the actions which are planned within the Health Board Seasonal plan and Operational Plan for Unscheduled care will have the combined effect of reducing admission (demand) and reducing length of stay (increasing capacity) and are forecast to bring the system into balance at 85% occupancy. The changes required to bring the system into balance will be delivered through the Operational Plan for Unscheduled Care plus additional initiatives identified and set out in the following section.

Seasonal Plan Version -1.02
5. Developing Our Plan
This section describes the changes planned or in place which are aimed at achieving the 85%
occupancy target identified in section 4 (closing the capacity gap)
5.1 Wellbeing
The Health Board has a plan to improve population wellbeing and therefore reduce reliance on
Unscheduled Care Services. The main elements of the operational plan to improve wellbeing are
as follows:
Smoking
The Health Board is committed to achieving the Welsh Government targets for smoking cessation.
The Health Board is on target to achieve the 5% target for referrals to quit services.
The implementation plan for 2016/7 focuses on ensuring that pharmacies are integrated into the
Quite Manager system and addressing variation in smoking cessation within Clusters.
Secondary care smoking cessation services are also being implemented within 2016/7.
Obesity
A lifestyle management approach has been agreed and funded to be implemented in 2016/7. This
is a “level 2” weight reduction service involving lifestyle support for weight reduction. This plan will
be implemented throughout 2016/7.
5.2 Community Resilience
The Health Board is keen to develop the concept of Community Resilience in partnership with local
voluntary organisations. A workshop was held in October where HB staff and representatives from
voluntary organisations reviewed potential for further collaboration, specifically to help people avoid
admission to hospital in the Winter Months. As a result of this workshop, the following three
schemes are being implemented:
The schemes are:
Frequent callers to WAST – Focused work with GP Practices
In order to address the patients that frequently call WAST, the group discussed the need to
commence some focused work relating to the top 10 callers from each GP Practice. This builds on
some work already commenced by WAST colleagues but enhances this, by exploring the support
available through the Third Sector, in taking the focus from a medically led model of support.
Data will be provided, detailing the top 10 patients connected with each GP Practice. A background
picture will be built about each individual case from GP, nursing and local authority records,
including information about the services that the person may already be connected into. This part
of the process will need to be undertaken by a clinician due to confidentiality issues.
The person will then be contacted and, with their agreement, a discussion will commence, which
will detail the amount of admissions that have occurred and the reasons for these. The person will

Seasonal Plan Version -1.02
then be supported to carry out the ‘What matters to me’ conversation (if not already carried out)
and will be offered a meeting with a Navigator from the Third Sector. This discussion will focus on
reducing the need to go into hospital and the supportive mechanisms that will be introduced for the
person to engage in. A plan of support will be offered and put in place and will contain key
elements of social prescribing. Again, this is a key element of the Ein Dyfodol programme, which
will build upon the existing evidence base and provide additionality based on evidence gathered
from social prescribing schemes elsewhere.
The key focus of this process is the navigation role, which supports the initiation of programmes to
support the person, but also monitors the persons’ engagement and the sustainability of the plan of
support that has been put in place. This role also links with the Community Agents, who are
available in a number of areas.
In order to monitor the success of this programme, the Navigator will link with the GP practice to
monitor any further hospital admissions.
It is acknowledged there are other voluntary sector providers who may, following the testing of the
proof of concept, will want to be part of the procurement process for the longer term delivery of
these services. However, it is acknowledged that in order to be able to articulate the requirements
within the service specification that a period to both co-produce and test the believed concepts and
benefits would ensure that the longer term contract process would be far better managed.
This period will also see the initial phase of Ein Dyfodol, building community links and establishing
the programme in areas where there are high rates of unscheduled care demands.
Voluntary Services relieving pressures on ED Departments
A number of suggestions were made regarding the opportunities for the voluntary sector to work in
ED’s, and to support the acute sector in alleviating pressure on the system. Working primarily in
the waiting areas, voluntary sector staff will provide support to elderly people, work with hospital
teams to prevent unnecessary admissions, and assist with arrangements to discharge patients on
time.
Volunteers would have a role to support medical teams to secure earlydischarge of patients who
do not need admission on medical grounds, but are prevented from returning home for social care
reasons.
There will be links with existing schemes, with opportunities for building on current levels of
activity. Examples of what could be undertaken are:
Helping frail or older people by doing their shopping or taking the rubbish out in icy
weather to avoid accidents.
Help patients return home safely and make sure there is food in the fridge –
relieving pressure on social care.
Support those people in the community who are in need of low level care and
reassurance.
Befriending schemes for people who are at risk of being lonely or isolated.
Building on current information and befriending services.
Contribution to social prescribing services.
Seasonal Plan Version -1.02
Reacting to Board Round decisions
Voluntary organisations could work with hospital services to secure early discharge of patients who
do not need a bed for medical reasons, but who require social care not medical attention.
The voluntary sector has established programmes to assist with this, and would work with
discharge managers, particularly when it comes to discharging patients at a weekend. They would
assist in ensuring that patients who need low level support are able to return to, and to settle, at
home. This service aims to help older people leaving hospital to recover, regain confidence and
create social support networks so that they are less likely to be re-admitted.
The schemes set out above are being implemented as “fast track” proposals, with the expectation
that they will have an impact prior to Christmas/New Year.
5.3 Services Closer to Home
The Health Board Operational Plan for Unscheduled Cares sets out a comprehensive and
ambitious plan to develop community services to ensure that, wherever possible, unscheduled
health needs can be met at home or close to home.
This change will be achieved through a series of investments in the Community Resource Team
(CRT). The CRT is a combined resource managed jointly between the Health Board and Local
Authorities. The additional investment is being provided through a combination of Intermediate
Care Funding (ICF), Seasonal planning and core Health Board budgets.
The combined impact of all of these changes will be to reduce admissions to and AVLOS by the
level indicated in the capacity analysis in order to achieve an occupancy level of 85%
The overall approach to community services can be set out as follows:
Seasonal Plan Version -1.02
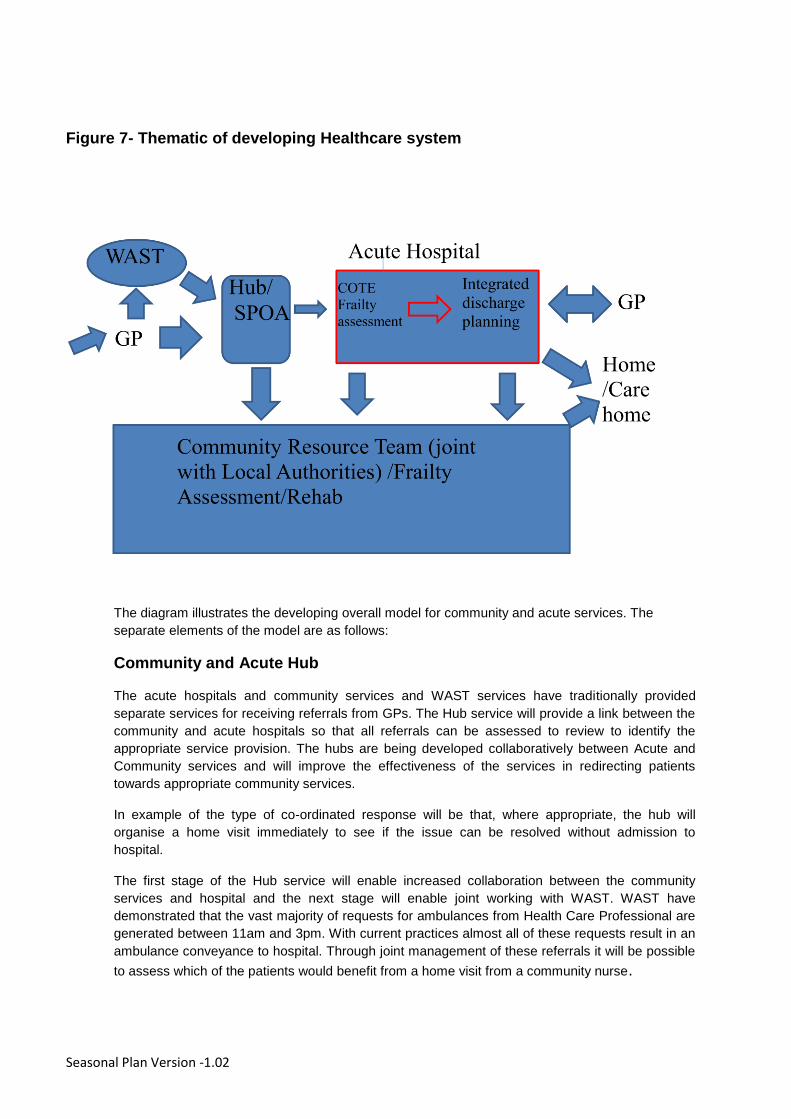
Figure 7- Thematic of developing Healthcare system
The diagram illustrates the developing overall model for community and acute services. The
separate elements of the model are as follows:
Community and Acute Hub
The acute hospitals and community services and WAST services have traditionally provided
separate services for receiving referrals from GPs. The Hub service will provide a link between the
community and acute hospitals so that all referrals can be assessed to review to identify the
appropriate service provision. The hubs are being developed collaboratively between Acute and
Community services and will improve the effectiveness of the services in redirecting patients
towards appropriate community services.
In example of the type of co-ordinated response will be that, where appropriate, the hub will
organise a home visit immediately to see if the issue can be resolved without admission to
hospital.
The first stage of the Hub service will enable increased collaboration between the community
services and hospital and the next stage will enable joint working with WAST. WAST have
demonstrated that the vast majority of requests for ambulances from Health Care Professional are
generated between 11am and 3pm. With current practices almost all of these requests result in an
ambulance conveyance to hospital. Through joint management of these referrals it will be possible
to assess which of the patients would benefit from a home visit from a community nurse.

Seasonal Plan Version -1.02
SPOA (Single Point of Access)
The SPOA is the service that has been developed in collaboration with Local Authorities to provide
a single point of contact for community, Local Authority and volunteer services. The SPOA is being
developed further within the overall plan to include more nursing input and provide services for
longer hours. The SPOAs will work together with the Hub/Acute services to ensure that patients
receive the appropriate treatment.
Community Resource Teams (CRT)
The CRT is the overall term for service provided in the community in partnership between the
Health Board and Local Authority. These services are being developed with 2016/7 with the
support of Intermediate Care Funding. For example, District Nursing is now provided on a 24/7
basis for the first time, patients can now be referred to the DNs at any time of the day or night as
an alternative to hospital admission.
Frailty assessment and Treatment
As part of the development of community services, each of the Areas are developing systems for
identifying patients who would benefit from support and care aimed at preventing crisis and
admission. This support will be provided from multidisciplinary teams working out of new “frailty”
services currently being developed. These services are in the process of being developed and
(unlike the services above) will not be in place in time for winter 2016/7.

Seasonal Plan Version -1.02
6. Summary of actions planned to improve capacity and
demand issues.
The full range of initiatives within the plan and their anticipated impact, are set out in the tables
below.
All of the actions set out below are new initiatives being developed as part of the Operational Plan
for 2016/7. Where there is an apparent continuation of a work stream e.g falls, there is a distinct
set of actions intended to make a difference in 2016/7.
6.1 Pre Admission
Table - 3 Reducing Admissions- Steps 1-7
Detail to be added
Planned Change Outcome To be
implemented
(in line with
Operational
Plan)
At Risk Groups
assisted by this
change
Projected
Impact
Proof of Concept
volunteer services
Support frequent
callers and attenders
at hospitals with
alternative services.
December Elderly, frail,
those with
underlying
conditions
Contribute to a
target reduction
in admissions of
5%
Primary Care- Risk
Identification
Early identification of
patients for pre-
emptive MDT input
December Elderly, frail,
those with
underlying
conditions
Contribute to a
target reduction
in admissions of
5%
Introduction of
Community
agents/social
prescribers
Direct patients to
alternative volunteer
and community
services
December Elderly, frail,
those with
underlying
conditions
Contribute to a
target reduction
in admissions of
5%
Expand operating
hours of
Community
Resource Team
Reduced admissions
in evening and
weekends
Improvements in
place in Q2,
further
improvements
planned
Elderly, frail,
those with
underlying
conditions
Contribute to a
target reduction
in admissions of
5%
WAST Frequent
Call initiative
Review most
frequent callers and
reduce calls by 10%
for this group
Q1 and onwards Those with
underlying
conditions or
mental health
issues
Contribute to a
target reduction
in admissions of
5%
Implement Falls Increase referrals
into falls pathway-
December Elderly, frail Contribute to a
target reduction
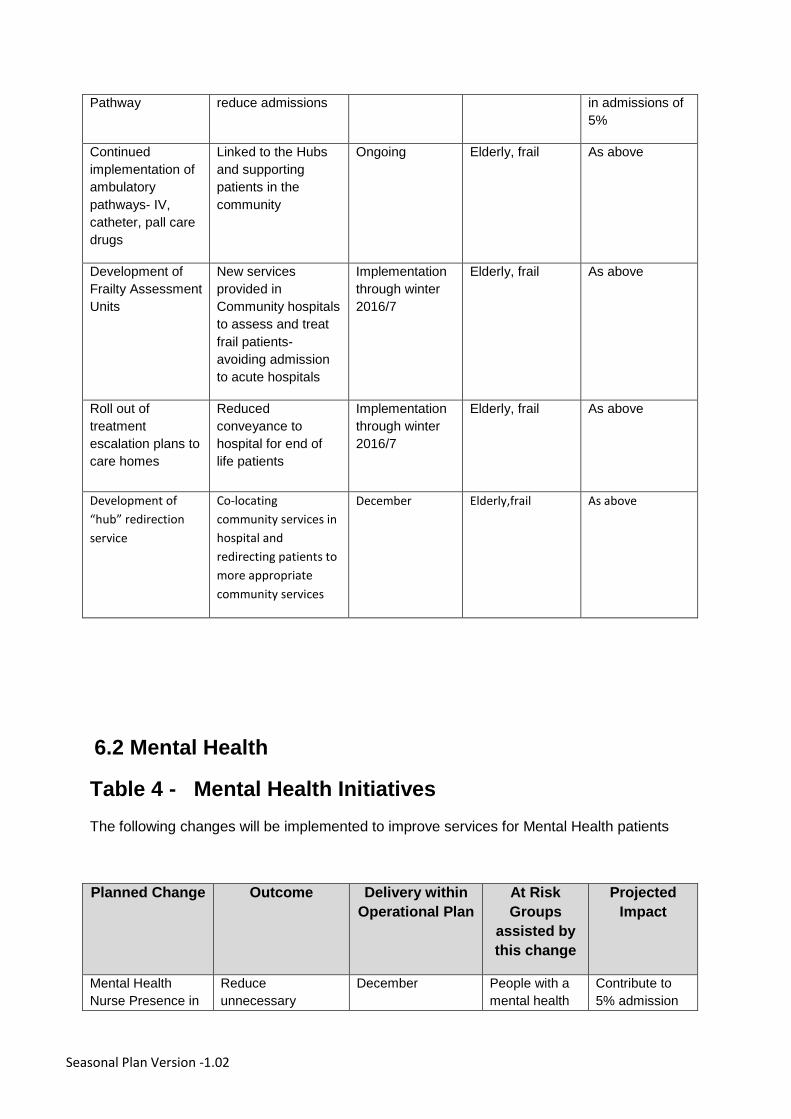
Seasonal Plan Version -1.02
Pathway reduce admissions in admissions of
5%
Continued
implementation of
ambulatory
pathways- IV,
catheter, pall care
drugs
Linked to the Hubs
and supporting
patients in the
community
Ongoing Elderly, frail As above
Development of
Frailty Assessment
Units
New services
provided in
Community hospitals
to assess and treat
frail patients-
avoiding admission
to acute hospitals
Implementation
through winter
2016/7
Elderly, frail As above
Roll out of
treatment
escalation plans to
care homes
Reduced
conveyance to
hospital for end of
life patients
Implementation
through winter
2016/7
Elderly, frail As above
Development of
“hub” redirection
service
Co-locating
community services in
hospital and
redirecting patients to
more appropriate
community services
December Elderly,frail As above
6.2 Mental Health
Table 4 - Mental Health Initiatives
The following changes will be implemented to improve services for Mental Health patients
Planned Change Outcome Delivery within
Operational Plan
At Risk
Groups
assisted by
this change
Projected
Impact
Mental Health
Nurse Presence in
Reduce
unnecessary
December People with a
mental health
Contribute to
5% admission
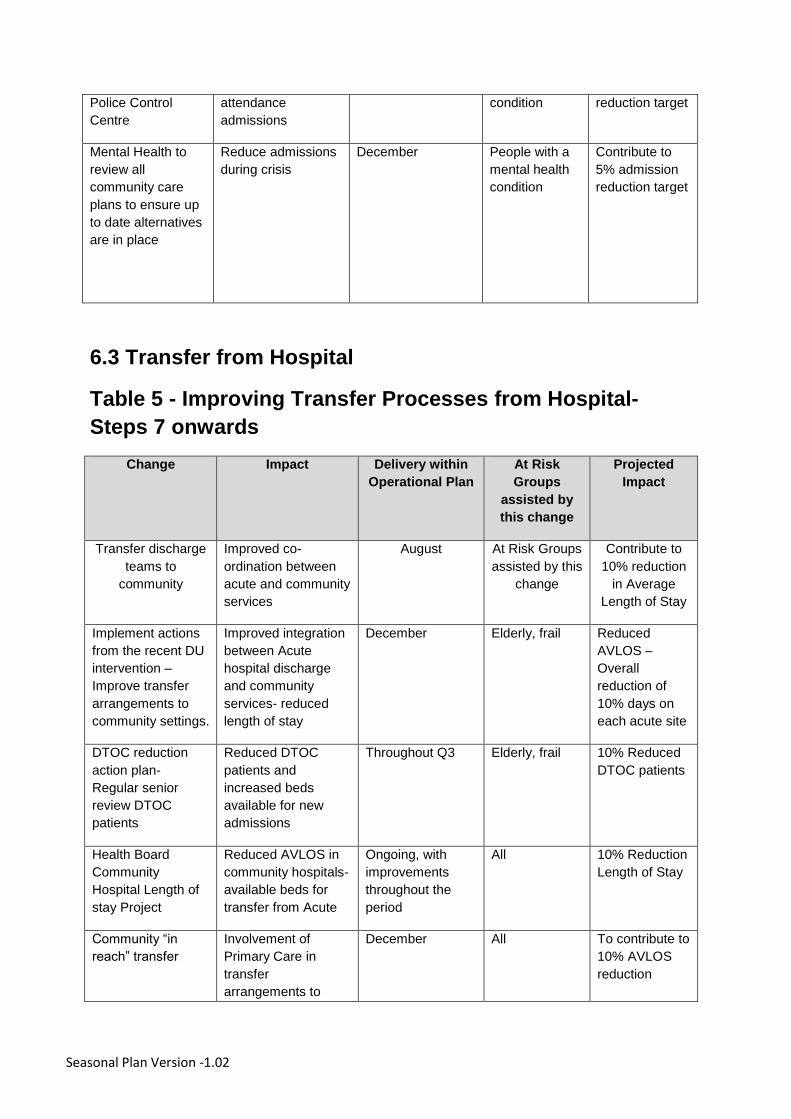
Seasonal Plan Version -1.02
Police Control
Centre
attendance
admissions
condition reduction target
Mental Health to
review all
community care
plans to ensure up
to date alternatives
are in place
Reduce admissions
during crisis
December People with a
mental health
condition
Contribute to
5% admission
reduction target
6.3 Transfer from Hospital
Table 5 - Improving Transfer Processes from Hospital-
Steps 7 onwards
Change Impact Delivery within
Operational Plan
At Risk
Groups
assisted by
this change
Projected
Impact
Transfer discharge
teams to
community
Improved co-
ordination between
acute and community
services
August At Risk Groups
assisted by this
change
Contribute to
10% reduction
in Average
Length of Stay
Implement actions
from the recent DU
intervention –
Improve transfer
arrangements to
community settings.
Improved integration
between Acute
hospital discharge
and community
services- reduced
length of stay
December Elderly, frail Reduced
AVLOS –
Overall
reduction of
10% days on
each acute site
DTOC reduction
action plan-
Regular senior
review DTOC
patients
Reduced DTOC
patients and
increased beds
available for new
admissions
Throughout Q3 Elderly, frail 10% Reduced
DTOC patients
Health Board
Community
Hospital Length of
stay Project
Reduced AVLOS in
community hospitals-
available beds for
transfer from Acute
Ongoing, with
improvements
throughout the
period
All 10% Reduction
Length of Stay
Community “in
reach” transfer
Involvement of
Primary Care in
transfer
arrangements to
December All To contribute to
10% AVLOS
reduction

Seasonal Plan Version -1.02
expedite transfer
6.4 Improving the “Minors” Stream
In addition to the work to improve the effectiveness of the system in avoiding admission and expediting discharge, it is also important that the patients attending for minor illness and injuries are treated quickly. Patients who attend Emergency Department (ED) for minor conditions (not likely to require admission) represent a significant proportion of attendances. If these can reliably be investigated and treated quickly, this will significantly improve overall ED performance on target times.
Table 6- Changes to the Minors stream
Change Impact Operational
Plan
At Risk
Groups
assisted by
this change
Projected Impact
Ensure a
protected
minors
stream in
ED
Deploy medical
and nursing staff
in dedicated
minors areas.
November All, homeless Achieve 95% within 4
hours for minors
patients
Note – the improvement and impact would be variable across the 3 sites linked to current
performance for Minors and the level of activity.

Seasonal Plan Version -1.02
6.5 WAST and BCUHB Specific
BCU and WAST have worked closely together to develop the following action plan. (these are in
addition to supporting multi organisational work, such as the Hubs)
Change Impact Operational
Plan
At Risk
Groups
assisted by
this change
Projected Impact
MIU
Standard
Operating
Procedure
(SOP)
Redirect
ambulances to
MIU in line with
SOP
In place All Contribute to 95%
within 4 hours for
minors patients
Rapid
Handover
PP at all ED
sites
Reduced delays In place All Contribute to 4 hour
trajectory
Community
Assistance
Pilot-
Denbighshire
Combined
working with Fire
services to
reduce
conveyance
In place All Contribute to 5%
reduced admissions
target
Establish
clinical desk
Assessment and
appropriate
treatment of
referrals-
reduced
conveyance
November All Contribute to 5%
reduced admissions
target
25
7. Managing the Christmas/New year effect
From the analysis in section above it is clear that a specific plan is required to reduce the
combined effect of both the reduced discharge activity in the holiday season and the predicted
increase in demand during the first week in January.
Reducing the disruption from Christmas & New Year
A detailed operational plan has been developed in each heath community (Area and Community
Hospital, which will ensure that Christmas and New Year will operate as closely as possible to
normal working days.
Local Authorities are an important contributor to this work and have committed to the principle of
“normal” running on the days in between the holidays. Social Services staff will be working as
normal on these days and this will support continuous hospital discharges throughout the period.
The following principles for Christmas and New Year working have been agreed by the BCU
Unscheduled Care Transformational Group.
Agree staff rotas by the end of November
Ensure rotas for festive holiday periods are sufficiently covered by no later than 1 December.
Appropriate contingency arrangements in place to manage any staffing shortfalls at short notice.
Implementing Estimated Date of Discharge as soon as patients are admitted or scheduled for admission.
Availability of supporting services, including access to diagnostics.
Consultant’s availability to discharge patients throughout weekends and the festive holiday periods.
Agree anticipated levels of social care packages that are likely to be required over the festive period.
Availability of appropriate multi-disciplinary professionals to facilitate discharge.
Pharmacy, transport and social care services should be in place to support the discharge process
Adequate care packages are in place in the community to meet predicted discharge levels.
Ensure that communications between key partners, staff, patients and the public are effective and that key messages are consistent.
The combined aim of all of these actions is to reduce the variation in discharges from hospital following Christmas and New Year. Each acute hospital will monitor the number of discharges and aim to maintain normal levels during this period.
Coping with the January “Surge” in admissions
In addition to the work to reduce the impact of the variation caused by the holiday period, there will
be escalation capacity available in the New Year. Additional beds will be opened on each acute site
as “surge capacity” to cope with the anticipated increase in demand.

26
8. Managing Infections and Immunisation
a. Infection Prevention
The Health Board has a comprehensive plans in place for the prevention of infection (including flu) and for the coping with outbreaks of infections if they arise (link here).
Of particular importance to the seasonal plan for BCUHB are the key points raised in the Flu Protocol:
Vaccination of frontline healthcare workers and people in high risk groups is the most important measure in preventing seasonal influenza infection
Standard Precautions must be maintained at all times in all healthcare settings including when managing known or suspected cases of influenza
Hand hygiene is a very important defence against acquisition of influenza.
Reinforce respiratory hygiene/cough etiquette* with all patients
In addition Droplet Precautions* are required for all cases of known of suspected influenza, until either the diagnosis has been excluded or the patient is no longer deemed infectious
Promotion of these key messages is an essential action to prevent outbreaks in care settings during the winter months when the likelihood of outbreaks of Infuenza and flu-like illness is higher.
Each of the hospital sites has clear protocols in place for coping with Flu and Norovirus and other outbreaks. Side rooms are available and the hospital escalation plan will be adapted to cope with the pressure on capacity created by infection outbreaks. (More detail – key points on how will it be adapted, and why it needs adaption)
b. Immunisation
The Health Board has a plan for reducing the burden of ill health resulting from the seasonal
increase in influenza infections in the community. This is an important element of combating
seasonal ill health because
Influenza is a key contributor to excess winter deaths in those aged over 65, or within
specific risk groups
Influenza is a key contributor to staff sickness rates with a knock on effect on business
continuity
Staff caring for vulnerable individuals can pass on influenza
Severe flue and flu related death in those with clinical risk factors can be reduced by
reducing transmission between children and between children and high-risk adults.
Influenza vaccination rates are a key Tier 1 target and uptake rates are expected to exceed 75%
for those people aged 65 years and those under 65 in designated at risk groups and including
pregnant women. Furthermore, 50% of frontline NHS staff should be vaccinated. There is no
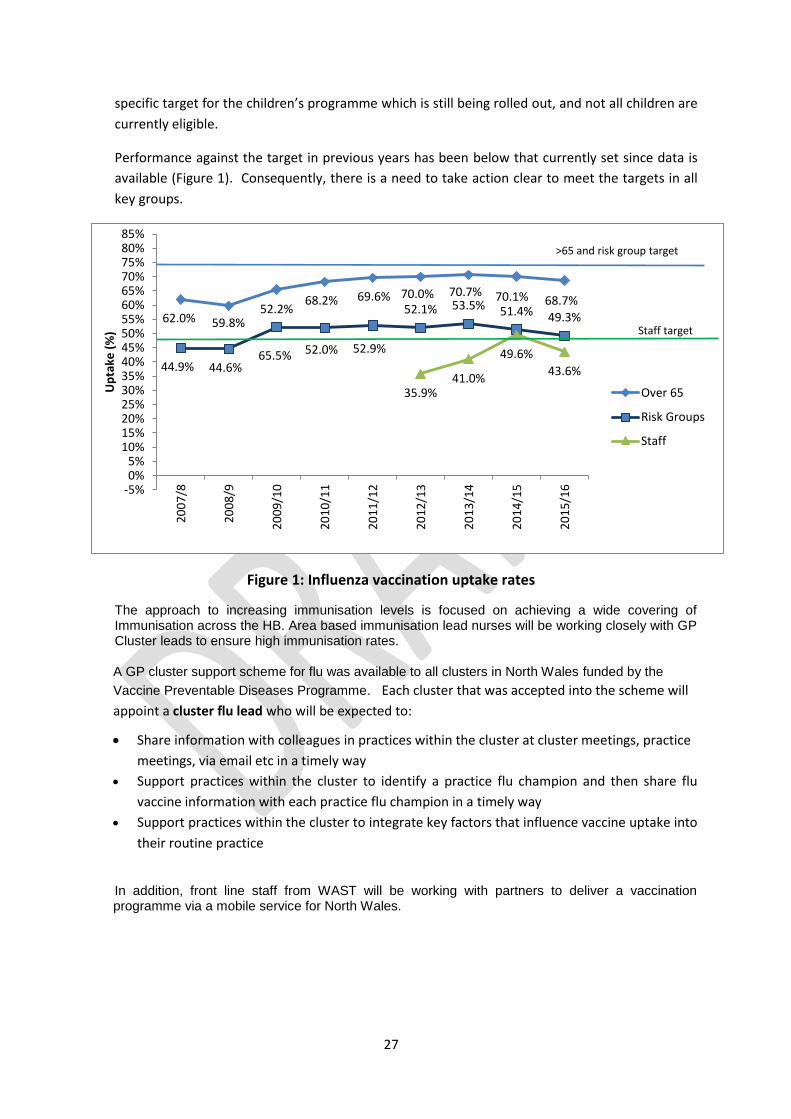
27
specific target for the children’s programme which is still being rolled out, and not all children are
currently eligible.
Performance against the target in previous years has been below that currently set since data is
available (Figure 1). Consequently, there is a need to take action clear to meet the targets in all
key groups.
Figure 1: Influenza vaccination uptake rates
The approach to increasing immunisation levels is focused on achieving a wide covering of Immunisation across the HB. Area based immunisation lead nurses will be working closely with GP Cluster leads to ensure high immunisation rates.
A GP cluster support scheme for flu was available to all clusters in North Wales funded by the
Vaccine Preventable Diseases Programme. Each cluster that was accepted into the scheme will
appoint a cluster flu lead who will be expected to:
Share information with colleagues in practices within the cluster at cluster meetings, practice
meetings, via email etc in a timely way
Support practices within the cluster to identify a practice flu champion and then share flu
vaccine information with each practice flu champion in a timely way
Support practices within the cluster to integrate key factors that influence vaccine uptake into
their routine practice
In addition, front line staff from WAST will be working with partners to deliver a vaccination programme via a mobile service for North Wales.
62.0% 59.8%
65.5%
68.2% 69.6% 70.0% 70.7% 70.1% 68.7%
44.9% 44.6%
52.2%
52.0% 52.9%
52.1% 53.5% 51.4% 49.3%
35.9%41.0%
49.6%
43.6%
-5%0%5%
10%15%20%25%30%35%40%45%50%55%60%65%70%75%80%85%
20
07
/8
20
08
/9
20
09
/10
20
10
/11
20
11
/12
20
12
/13
20
13
/14
20
14
/15
20
15
/16
Up
take
(%
)
Over 65
Risk Groups
Staff
>65 and risk group target
Staff target
28
9. Partnership Working
The Seasonal Plan has been developed as one strand of the ongoing response of the local health
economy to Unscheduled Care. The local Authorities and WAST in particular are involved and
supporting the work on service improvement across North Wales.
The Health Board, Local Authorities and WAST are working closely together across all areas of the unscheduled care agenda, the Local Authorities are represented on the Unscheduled Care Transformational Board.
The Health Board and Local Authorities are collaborating on a range of measures aimed at improving services provided at home and in community settings. This work has been supported by Intermediate Care Funding (ICF) and includes the further development of Single Point of Access (SPOA), expansion of intermediate care teams further development of step up/step down beds across North Wales. The “Choice Policy” which has been agreed in 2016 is being implemented jointly between the LAs and the Health Board.
Each of the six local Authorities are also developing their own plans to ensure that Social Services and Care home support are provided consistently over the Christmas and New Year period.
All councils are committed to support flu immunisation for frontline staff and encourage this across the care sector.
In addition, third sector organisations are working with local Authorities to target at risk groups of the population, such as with good neighbour schemes and community agents.
The joint work on Unscheduled Care can also be seen within the wider context of the partnership working within the local Public Service Boards (PSBs). The PSBs have been established with senior representation from local partners and the Health Board and are currently carrying assessments of Population Needs in line with guidance. These population needs assessments will identify local health priorities, including the identification of vulnerable population groups. The local priorities will then determine the action plans required to address the issues identified in the Population Needs Assessment and improve the lives of the sections of the population most in need.
As the vulnerable and those in most need are also high users of Unscheduled Care services, the work of the PSBs will make an important contribution to the resilience of the unscheduled care system.
10. Escalation
The Health Board follows national guidance on escalation scoring and response actions. These are supplemented by 3 daily integrated conference calls across the Health Board. These calls include Hospital, Community, WAST and LA representation and are chaired by a senior HB manager. This system ensures that there is an immediate Health Board wide response to escalation issues.
In addition the HB is working to implement the LEAP process in conjunction with WAST. A detailed action plan is being finalised and will be completed in Q3 in time for Seasonal Pressure.
29
11. Workforce
Many of the changes indicated in section 5 are dependent on recruitment of additional trained staff.
Funding has been agreed for the overall plan and the recruitment processes are under way to
ensure that sufficient numbers of trained staff are in post to deliver the plan.
There are potential risks to elements of the plan from either delays in recruitment processes and/or
recruitment difficulties. Potential delays to processes are being mitigated through expediting the
decision making and authority processes, so that recruitment could begin as soon as possible.
Mitigation of recruitment risks is more challenging and this should be considered within the context
of the overall Health Board recruitment strategy. There are a range of initiatives in place aimed at
improving the ability of the health board to recruit skilled staff and these will support recruitment for
the seasonal plan. In the meantime, the actions in this plan are being prioritised in relation to the
potential impact on performance within the staffing available.
12. Financial Implications
The Health Board has allocated a budget of £3.1m for the delivery of the Seasonal Plan. The overall plan will be delivered within this budget and, where appropriate, from within the Intermediate Care Fund (ICF) allocation.
3.2 SPPH16/204 Review of the Committee's allocated Risks extracted from the Corporate Risk Register
1 SPPH 16.204 CRR coversheet.docx
1
Strategy, Partnerships & Population Health Committee 24.11.16 Item SPPH16/204
To improve health and provide excellent care
Title: Review of Corporate Risks Assigned to Strategy, Partnerships & Population Health (SPPH) Committee
Author: Ms Kate Parry, Interim Head of Corporate Affairs
Responsible Director:
Mr Geoff Lang, Executive Director of Strategy
Public or In Committee
Public
Strategic Goals (Indicate how the subject matter of this paper supports the achievement of BCUHB’s strategic goals –tick all that apply)
1. Improve health and wellbeing for all and reduce health
inequalities
√
2. Work in partnership to design and deliver more care
closer to home
√
3. Improve the safety and outcomes of care to match the
NHS’ best
√
4. Respect individuals and maintain dignity in care √
5. Listen to and learn from the experiences of individuals √
6. Use resources wisely, transforming services through
innovation and research
7. Support, train and develop our staff to excel.
Approval / Scrutiny Route
The full Corporate Risk Register is scrutinised by the Health Board twice per year and is published on the Board’s external facing website. Individual risks are allocated to one of the Board’s Committees for regular consideration and review.
Purpose: The attached report has been produced from the web-based Datix system and details the risks which have been allocated to the SPPH Committee – namely:
CRR1 Improving Population Health
CRR8 Strategy Development (refreshed risk)
CRR9 Primary Care Sustainability
CRR14 Organisational Development
CRR15 Workforce
CRR17 Development of IMTP (new risk devolved from CRR8)
Significant issues and risks
The Corporate Risk Register provides a position statement regarding current LHB high level risks, actions required and progress to date including timescales.

2
The Committee will see that the action to refresh and separate out elements from CRR8 has been actioned and is reflected in this latest report.
Special Measures Improvement Framework Theme/ Expectation addressed by this paper
Governance – management of risk Mental Health Maternity Services Strategic and Service Planning – concerns and complaints
Equality Impact Assessment
Not applicable for governance paper of this nature
Recommendation/ Action required by the Committee
The Committee is asked to consider the relevance of the current controls, review the actions in place and consider whether the risk scores remain appropriate.
Disclosure: Betsi Cadwaladr University Health Board is the operational name of Betsi Cadwaladr University Local Health Board
Committee Coversheet v10 June 2016

2 SPPH16.204 CRR Report.pdf
Ref Title Opened Principal Risk Executive Lead
Description Risk Rating (initial)
Risk Rating (current)
Risk Rating (Target)
Target Risk Date Due
Controls in place Further action to achieve target risk score Date of Last Review/Update
CRR1 Improving Population Health
01/10/15 Failure to reduce inequalities in health outcomes
Executive Director of Public Health
There is a risk that population health will not improve due to a failure to focus on prevention and early intervention. This will widen the gap in inequality of health outcomes.
20 16 8 31/03/2018 1.Population health profiles updated on a continuing basis2.Local public health strategic framework in place3.Single Integrated Plans with Local Authorities in place4.Strategic groups (e.g. homelessness and vulnerable adults) in place5.Joint partnership group to assess population needs in respect of Social Services and Wellbeing in place and developing assessment in line with timescales required by legislation6.Initial review of Board cycle of business to enable focus on population health issues completed7.Developing processes in place around population wellbeing assessments as required to inform Wellbeing of Future Generations plans
1.Completion of ongoing phase of review of Strategic Partnerships to ensure clarity of purpose, and maximise opportunities for focus on population health issues with partners (Feb 2017)2.Improve the analysis and use of Primary Care data for North Wales to inform IMTP. Improved access to data derived from Primary Care sources is beginning to inform Area planning. Further work needed to maximise benefit gained (March 2017)3.Implement targeted Well North Wales Health Inequalities Programme in a small number of communities. Programme now under review and revision. Reframing of focus and rebranding as “Ein Dyfodol”. (July 2017)4.Set Wellbeing Objectives to achieve identified goals as part of the new duty within the Wellbeing of Future Generations Act. Wellbeing Assessments underway which will inform draft Objectives. Health Board whole system strategy development reflects new legislative context. (March 2017)5.Collaborate and develop local wellbeing plans as member of Public Service Boards. Public Service Boards established and initial developments underway. (March 2018)
11/11/2016
6.Development of HB Strategy Living Healthier, Staying Well puts key emphasis on improving population health through more focus on prevention. Implementation has potential to bring about notable change in emphasis, but timescales are under discussion. Further review in April 2017
CRR8 Strategy Development
01/10/15 Failure to develop coherent strategic plans
Executive Director of Strategy
There is a risk that the Health Board cannot develop a holistic strategy for well-being, health and healthcare and consequently cannot deliver safe and sustainable services to the population of North Wales in the medium to longer term.This will lead to an inability to address and improve health and healthcare services.
20 20 12 31/01/2018 1.Approach to developing a strategy (Living Healthier, Staying Well) approved by SPPH and Board on 21 07 16.2.Priority clinical areas for strategy development such as Primary Care and Mental Health will be progressed during 2016/173.Key areas of clinical risk will be addressed in the 2016/17 plan with actions to maintain quality and safety4.Quality and safety monitored through Quality and Safety Executive with assurance reporting to Quality, Safety and Experience Committee5.Engagement sessions with key stakeholder representatives held in March & July 2016 and to be repeated in autumn 20166.Governance and reporting arrangements for strategy development agreed.7.Quarterly review of Annual Plan and risk assessment undertaken July 20168.PEG established to drive the strategy Aug 20169.Timetable for production of MH, primary care and maternity strategic frameworks confirmed July 2016
1.Primary Care Strategy framework to be published Nov 20162. Maternity, paediatrics and neonatal framework to be published Nov 20163. Mental Health Strategic framework document to be published Nov 20164. Detailed workplansfor future phases of strategy development with milestones for delivery agreed Nov 20165. Timeline for developing 3 Year Plan for 2018-19 to be developed and agreed and synchronised with strategy development.
10/10/2016
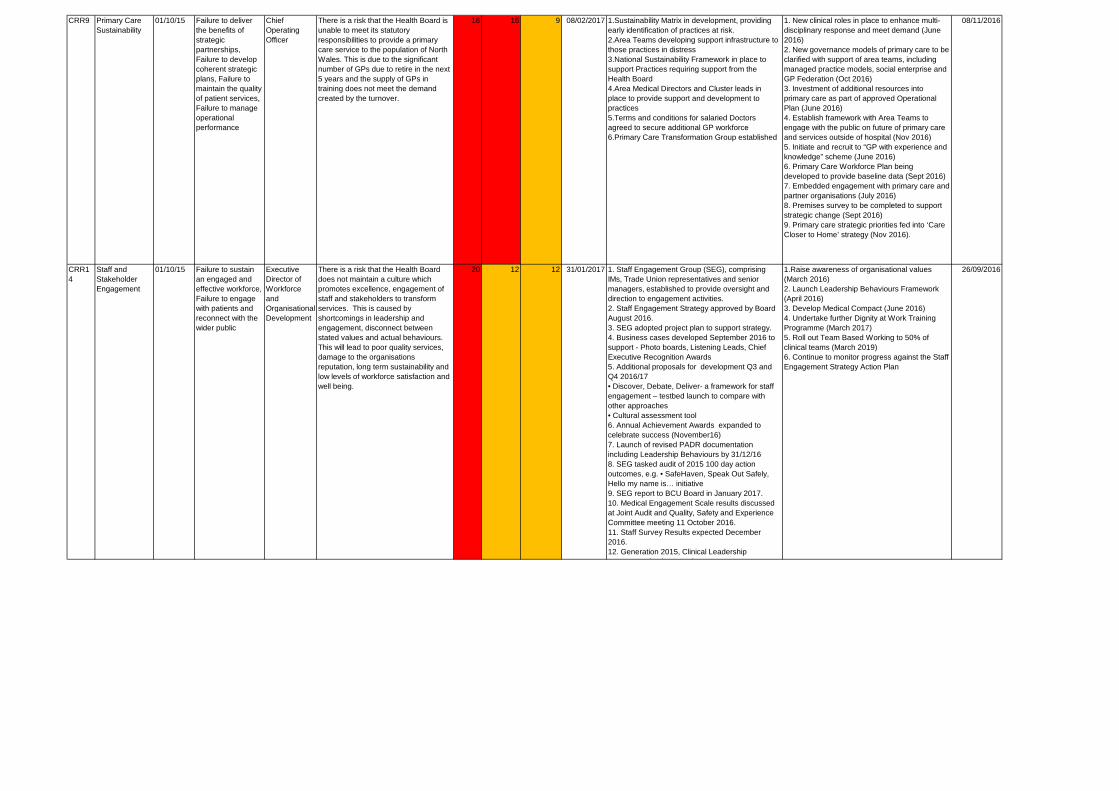
CRR9 Primary Care Sustainability
01/10/15 Failure to deliver the benefits of strategic partnerships, Failure to develop coherent strategic plans, Failure to maintain the quality of patient services, Failure to manage operational performance
Chief Operating Officer
There is a risk that the Health Board is unable to meet its statutory responsibilities to provide a primary care service to the population of North Wales. This is due to the significant number of GPs due to retire in the next 5 years and the supply of GPs in training does not meet the demand created by the turnover.
16 16 9 08/02/2017 1.Sustainability Matrix in development, providing early identification of practices at risk.2.Area Teams developing support infrastructure to those practices in distress3.National Sustainability Framework in place to support Practices requiring support from the Health Board4.Area Medical Directors and Cluster leads in place to provide support and development to practices5.Terms and conditions for salaried Doctors agreed to secure additional GP workforce6.Primary Care Transformation Group established
1. New clinical roles in place to enhance multi-disciplinary response and meet demand (June 2016)2. New governance models of primary care to be clarified with support of area teams, including managed practice models, social enterprise and GP Federation (Oct 2016)3. Investment of additional resources into primary care as part of approved Operational Plan (June 2016)4. Establish framework with Area Teams to engage with the public on future of primary care and services outside of hospital (Nov 2016)5. Initiate and recruit to “GP with experience and knowledge” scheme (June 2016)6. Primary Care Workforce Plan being developed to provide baseline data (Sept 2016)7. Embedded engagement with primary care and partner organisations (July 2016)8. Premises survey to be completed to support strategic change (Sept 2016)9. Primary care strategic priorities fed into ‘Care Closer to Home’ strategy (Nov 2016).
08/11/2016
CRR14
Staff and Stakeholder Engagement
01/10/15 Failure to sustain an engaged and effective workforce, Failure to engage with patients and reconnect with the wider public
Executive Director of Workforce and Organisational Development
There is a risk that the Health Board does not maintain a culture which promotes excellence, engagement of staff and stakeholders to transform services. This is caused by shortcomings in leadership and engagement, disconnect between stated values and actual behaviours. This will lead to poor quality services, damage to the organisations reputation, long term sustainability and low levels of workforce satisfaction and well being.
20 12 12 31/01/2017 1. Staff Engagement Group (SEG), comprising IMs, Trade Union representatives and senior managers, established to provide oversight and direction to engagement activities.2. Staff Engagement Strategy approved by Board August 2016.3. SEG adopted project plan to support strategy.4. Business cases developed September 2016 to support - Photo boards, Listening Leads, Chief Executive Recognition Awards5. Additional proposals for development Q3 and Q4 2016/17• Discover, Debate, Deliver- a framework for staff engagement – testbed launch to compare with other approaches • Cultural assessment tool6. Annual Achievement Awards expanded to celebrate success (November16)7. Launch of revised PADR documentation including Leadership Behaviours by 31/12/168. SEG tasked audit of 2015 100 day action outcomes, e.g. • SafeHaven, Speak Out Safely, Hello my name is… initiative9. SEG report to BCU Board in January 2017.10. Medical Engagement Scale results discussed at Joint Audit and Quality, Safety and Experience Committee meeting 11 October 2016. 11. Staff Survey Results expected December 2016.12. Generation 2015, Clinical Leadership programme implemented.
1.Raise awareness of organisational values (March 2016)2. Launch Leadership Behaviours Framework (April 2016)3. Develop Medical Compact (June 2016)4. Undertake further Dignity at Work Training Programme (March 2017)5. Roll out Team Based Working to 50% of clinical teams (March 2019)6. Continue to monitor progress against the Staff Engagement Strategy Action Plan
26/09/2016
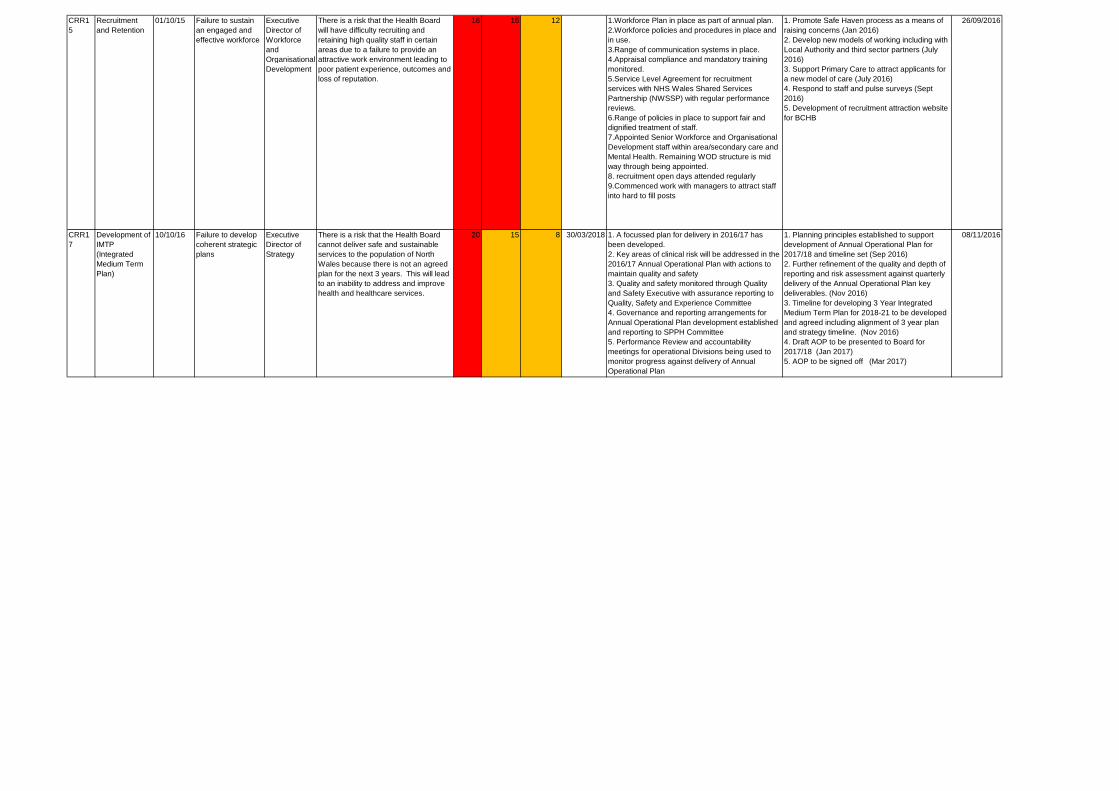
CRR15
Recruitment and Retention
01/10/15 Failure to sustain an engaged and effective workforce
Executive Director of Workforce and Organisational Development
There is a risk that the Health Board will have difficulty recruiting and retaining high quality staff in certain areas due to a failure to provide an attractive work environment leading to poor patient experience, outcomes and loss of reputation.
16 16 12 1.Workforce Plan in place as part of annual plan.2.Workforce policies and procedures in place and in use.3.Range of communication systems in place.4.Appraisal compliance and mandatory training monitored.5.Service Level Agreement for recruitment services with NHS Wales Shared Services Partnership (NWSSP) with regular performance reviews.6.Range of policies in place to support fair and dignified treatment of staff.7.Appointed Senior Workforce and Organisational Development staff within area/secondary care and Mental Health. Remaining WOD structure is mid way through being appointed.8. recruitment open days attended regularly9.Commenced work with managers to attract staff into hard to fill posts
1. Promote Safe Haven process as a means of raising concerns (Jan 2016)2. Develop new models of working including with Local Authority and third sector partners (July 2016)3. Support Primary Care to attract applicants for a new model of care (July 2016)4. Respond to staff and pulse surveys (Sept 2016)5. Development of recruitment attraction website for BCHB
26/09/2016
CRR17
Development of IMTP (Integrated Medium Term Plan)
10/10/16 Failure to develop coherent strategic plans
Executive Director of Strategy
There is a risk that the Health Board cannot deliver safe and sustainable services to the population of North Wales because there is not an agreed plan for the next 3 years. This will lead to an inability to address and improve health and healthcare services.
20 15 8 30/03/2018 1. A focussed plan for delivery in 2016/17 has been developed.2. Key areas of clinical risk will be addressed in the 2016/17 Annual Operational Plan with actions to maintain quality and safety3. Quality and safety monitored through Quality and Safety Executive with assurance reporting to Quality, Safety and Experience Committee4. Governance and reporting arrangements for Annual Operational Plan development established and reporting to SPPH Committee5. Performance Review and accountability meetings for operational Divisions being used to monitor progress against delivery of Annual Operational Plan
1. Planning principles established to support development of Annual Operational Plan for 2017/18 and timeline set (Sep 2016)2. Further refinement of the quality and depth of reporting and risk assessment against quarterly delivery of the Annual Operational Plan key deliverables. (Nov 2016)3. Timeline for developing 3 Year Integrated Medium Term Plan for 2018-21 to be developed and agreed including alignment of 3 year plan and strategy timeline. (Nov 2016)4. Draft AOP to be presented to Board for 2017/18 (Jan 2017)5. AOP to be signed off (Mar 2017)
08/11/2016
3.3 SPPH16/205 Update on Well North Wales
1 SPPH16.205 Well North Wales_coversheet.docx
1
Strategy, Partnerships & Population Health Committee 24.11.16 Item SPPH16/205
To improve health and provide excellent care
Title: Update on Well North Wales
Author: Dr Glynne Roberts, Programme Director, Well North Wales
Responsible Director:
Mrs Bethan Jones, Area director (Central)
Public or In Committee
Public
Strategic Goals (Indicate how the subject matter of this paper supports the achievement of BCUHB’s strategic goals –tick all that apply)
1. Improve health and wellbeing for all and reduce health
inequalities
X
2. Work in partnership to design and deliver more care
closer to home
X
3. Improve the safety and outcomes of care to match the
NHS’ best
X
4. Respect individuals and maintain dignity in care X
5. Listen to and learn from the experiences of individuals X
6. Use resources wisely, transforming services through
innovation and research
X
7. Support, train and develop our staff to excel. x
Approval / Scrutiny Route
This paper provides an update on the Well North Wales programme, which is a multi-agency programme established to tackle health inequalities.
Purpose: To update the Committee on progress with: 1. Developing the concept of Well North Wales.
2. Progress in taking the specified initiatives forward.
3. The outline forward plan for the next phase of the programme
Significant issues and risks
1. Financial: resources for the implementation of the Ein Dyfodol
projects to be confirmed.
2. Accountability: approval required for proposed accountability and
governance arrangements.
Special Measures Improvement Framework Theme/
1. Engagement and consultation with individuals and communities.
2. Partnership working with stakeholders.
2
Expectation addressed by this paper
Equality Impact Assessment
N/A
Recommendation/ Action required by the Committee
The Committee is asked to note the progress made in developing the Well North Wales programme, and to endorse the accountability framework outlined in the paper. Additionally, the Committee is asked to approve the next steps, which will take the programme forward into 2017.
Disclosure: Betsi Cadwaladr University Health Board is the operational name of Betsi Cadwaladr University Local
Health Board
Committee Coversheet v10 June 2016

2 SPPH16.205 Well North Wales Update V2.doc
1
Update on Well North Wales
1. Purpose of report
To update the Committee on progress with:
a) Developing the concept of Well North Wales. b) Progress in taking the specified initiatives forward. c) The outline forward plan for the next phase of the programme
2. Introduction/Context
The concept of Well North Wales has been acknowledged and supported by the Health Board, and numerous papers linked to the project and the issue of health inequalities have been presented. Well North Wales is an umbrella term, under which a range of initiatives aimed at tackling health inequalities are being developed. Health inequalities need to be addressed on a partnership and multi-agency basis, and many of the key issues fall outside the primary domain of the NHS. The Health Board’s commitment to the Well North Wales programme ensures that the health aspect of anti-poverty programmes, and the work around the social determinants of health, is given the prominence, co-ordination and exposure required, and positions the Health Board at the heart of local and regional health inequalities programmes. Within North Wales, the pockets of deprivation are often masked by their proximity to more affluent areas. Consequently, although the rates of inequality in North Wales are lower than for Wales as a whole, there are distinct communities where health inequalities are a real and tangible issue. As evidenced in recent Board papers, the issues around health inequalities impact on a significant proportion of the North Wales population: • 12% of the North Wales population (81,700 people) live in the most deprived fifth
areas in Wales. • People living in these communities are currently experiencing stark differences in
health outcomes. Many of these poor outcomes are modifiable and therefore preventable:
o The mortality rate in the most deprived 20% of areas in Wales is twice that of the least deprived 20% of areas
o The average boy born in the most deprived areas of BCUHB is likely to live just over seven years less than the average boy born in the most affluent area, and likely to spend 14 additional years in poorer health.
o Life expectancy at birth for girls living in the most deprived areas in BCUHB is over five years less than the least deprived areas, and females are likely to spend 13 additional years in poorer health.
o There is a clear link between low birth weight and socio-economic deprivation: the highest rate is in the poorest areas and it is almost twice
the rate found in those areas with the lowest rates of low birth weight o The more deprived communities of North Wales have around a 25% higher
rate of emergency admission after adjustment for age than the more
2
affluent communities There is, therefore, a requirement to tackle issues around deprivation and poverty at a local, community level, and ensure that the views, attitudes and beliefs of communities are fully reflected in any initiatives developed to address the inequalities agenda. Well North Wales is well placed to meet the principles of prudent health, particularly around co-production; maximising the partnership approach to ensure the most appropriate use of resources, and to reduce inappropriate variation using evidence-based practices consistently and transparently. As part of the development of the Well North Wales concept, it was agreed that place-based initiatives, mirroring the established and successful Well London model, would be classified as Ein Dyfodol/ Our Future projects, with the more general inequalities and well being work retained under the broader Well North Wales banner. A Well North Wales Programme Director was appointed in July 2016, and the objectives for the initial period have focused on:
Involving stakeholders from across North Wales and identifying their support for developing a health-initiated programme in specified communities.
Promoting the programme with key partners (including Welsh Government; Well London; the Big Lottery).
Identifying the resources to take forward the Ein Dyfodol projects.
Developing proposals for the further development of targeted initiatives.
Developing the governance and accountability arrangements.
Identifying projects that will form part of the broader Well North Wales programme.
Work during Quarter 2 of the current financial year has built upon the excellent scoping work undertaken by Public Health Wales, which led to the selection of 3 initial communities for the Ein Dyfodol programme. There has also been significant engagement around the broader inequalities agenda, and the contribution the Health Board can make to the prevention agenda. Both dimensions are reflected in this paper. The development of the Ein Dyfodol programmes has been fully supported by the local Public Health Wales team.
3. Strategic context
3.1. Future Generations and Well Being Act Well North Wales will need to respond to, and work closely with, the Public Services Boards (PSBs) in delivering the objectives set out in the Future Generations and Wellbeing Act. To this end, it is suggested that the programme accountability will be to the four PSB’s, ensuring that the focus on communities, needs assessments, and tackling inequalities is at the forefront of both service delivery and strategy.
3
3.2. Links with the 2025 movement 2025 is a voluntary group of individuals and organisations working together with a shared purpose of tackling avoidable health inequality in North Wales. Well North Wales and the 2025 movement are working closely on a number of initiatives to ensure that the relative strengths of both are maximized. Well North Wales will feature prominently in the 2025 annual conference in December 2016, and will utilise the forum to promote best practice. 3.3. External links Well North Wales is affiliated to Well London, which has a ten-year track record in developing a framework for local communities and organisations to work together to improve health and well-being, build resilience, and reduce inequalities (http://www.welllondon.org.uk/4/about-well-london.html). Well London will provide the initial training for Ein Dyfodol co-ordinators and volunteers, as well as on-going support in terms of research and evaluation. To this end, the project has facilitated links between Bangor University and Well London, with Bangor University being a co-applicant to a major research and evaluation bid that, if successful, will enable Well London to extend its scope to a wider network of communities and for Ein Dyfodol to be evaluated using the same rigorous research methodology and resources. There are also links with the Bromley by Bow Centre (http://www.bbbc.org.uk/) who are also keen to support the development in North Wales. Bromley by Bow are currently supporting the Well North initiative, covering nine communities in the north of England, and again there will be informal links with this network to provide advice and examples of good practice for the development of specific North Wales projects. 3.4. Bevan Commission The Ein Dyfodol component of the Well North Wales programme has been accepted as an exemplar project by the Bevan Commission for 2016-17. In addition, the proposed development of a Bevan Innovation Hub within BCU will focus on Inequalities. The Hub will be underpinned by a culture of evaluation and impact assessment. Each theme being considered will be critically evaluated for impact and contribution, and the actions and approaches adopted will be informed through engagement with research based evaluation and context. Bangor University, working in partnership with the Health Board, will seek opportunities to source funding to build capacity in the health inequalities theme, and will seek to link this directly to actions. 3.5. Developing an evaluation framework In addition to the link with Well London and the Bevan Innovation Hub, Bangor University is also working with the Ein Dyfodol project to scope and develop research proposals that will underpin the development of the programme locally. These will focus on community-identified responses, and will utilise the health economics expertise within Bangor University. 3.6. Housing associations Housing conditions are acknowledged as a key issue in improving health and well-being. Formal meetings have been scheduled on a bi-monthly basis with the Chief
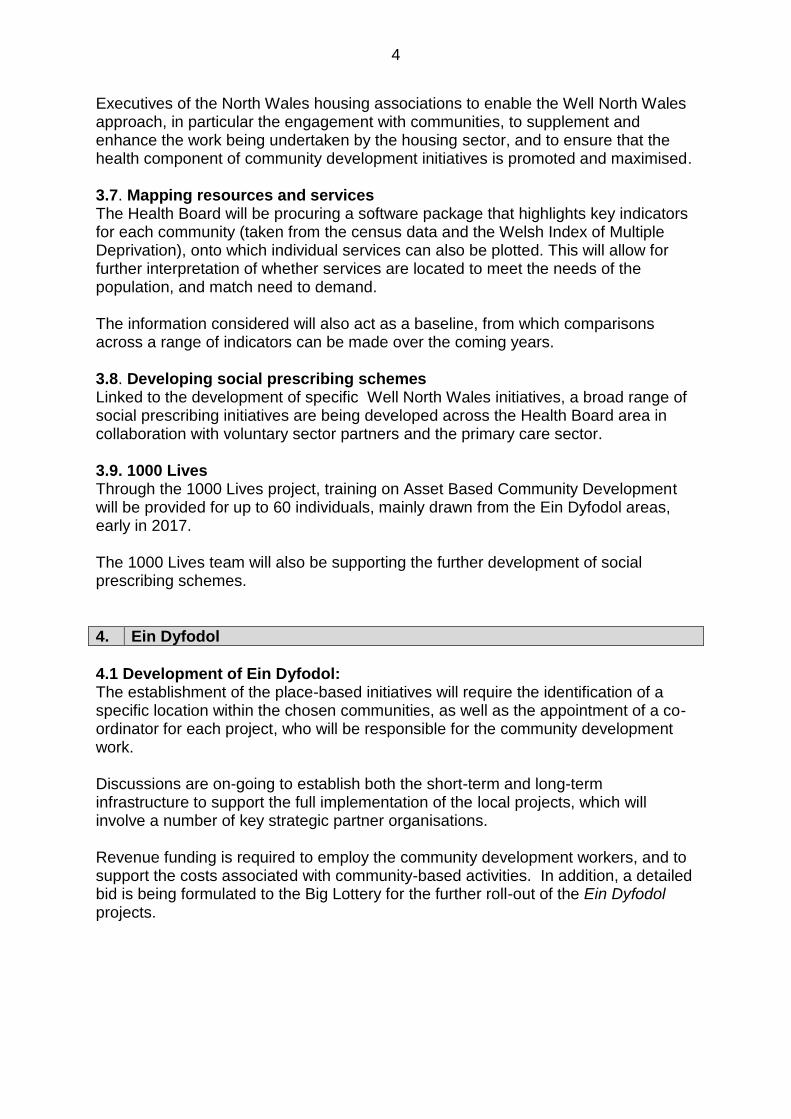
4
Executives of the North Wales housing associations to enable the Well North Wales approach, in particular the engagement with communities, to supplement and enhance the work being undertaken by the housing sector, and to ensure that the health component of community development initiatives is promoted and maximised. 3.7. Mapping resources and services The Health Board will be procuring a software package that highlights key indicators for each community (taken from the census data and the Welsh Index of Multiple Deprivation), onto which individual services can also be plotted. This will allow for further interpretation of whether services are located to meet the needs of the population, and match need to demand. The information considered will also act as a baseline, from which comparisons across a range of indicators can be made over the coming years. 3.8. Developing social prescribing schemes Linked to the development of specific Well North Wales initiatives, a broad range of social prescribing initiatives are being developed across the Health Board area in collaboration with voluntary sector partners and the primary care sector. 3.9. 1000 Lives Through the 1000 Lives project, training on Asset Based Community Development will be provided for up to 60 individuals, mainly drawn from the Ein Dyfodol areas, early in 2017. The 1000 Lives team will also be supporting the further development of social prescribing schemes.
4. Ein Dyfodol
4.1 Development of Ein Dyfodol: The establishment of the place-based initiatives will require the identification of a specific location within the chosen communities, as well as the appointment of a co-ordinator for each project, who will be responsible for the community development work. Discussions are on-going to establish both the short-term and long-term infrastructure to support the full implementation of the local projects, which will involve a number of key strategic partner organisations. Revenue funding is required to employ the community development workers, and to support the costs associated with community-based activities. In addition, a detailed bid is being formulated to the Big Lottery for the further roll-out of the Ein Dyfodol projects.

5
4.2. Update on Ein Dyfodol projects 4.2.1. Penycae 4.2.1.1. Community profile:
Population: 2,205 Description: The area:
Contains one target LSOA, Penycae, which is in the most deprived 20%.
Forms part of Wrexham Urban Villages Communities First area.
Has no obvious community hub from which to run the Ein Dyfodol
programme.
Data highlights:
Performs poorly on housing
Performs well on physical environment and access to services
4.2.1.2. Population profile: The population:
The population is younger than the Welsh average
The population is has peaks 20-35 and <10 indicating young families
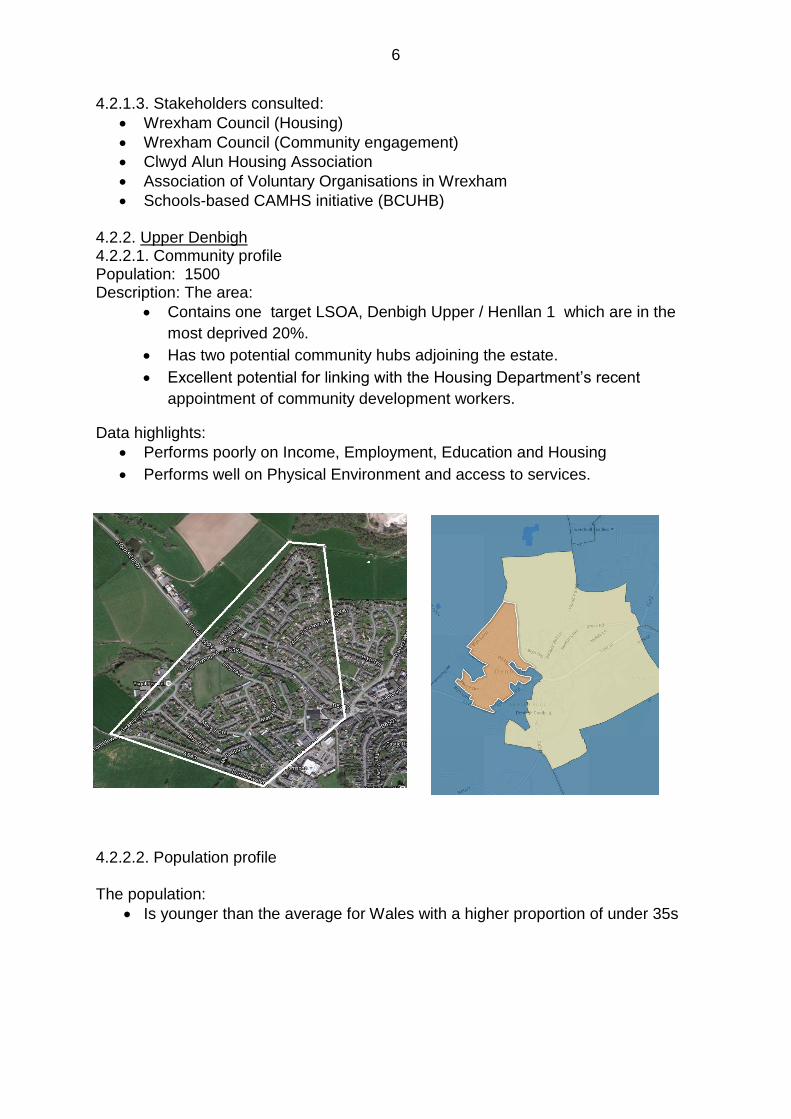
6
4.2.1.3. Stakeholders consulted:
Wrexham Council (Housing)
Wrexham Council (Community engagement)
Clwyd Alun Housing Association
Association of Voluntary Organisations in Wrexham
Schools-based CAMHS initiative (BCUHB) 4.2.2. Upper Denbigh 4.2.2.1. Community profile Population: 1500 Description: The area:
Contains one target LSOA, Denbigh Upper / Henllan 1 which are in the
most deprived 20%.
Has two potential community hubs adjoining the estate.
Excellent potential for linking with the Housing Department’s recent
appointment of community development workers.
Data highlights:
Performs poorly on Income, Employment, Education and Housing
Performs well on Physical Environment and access to services.
4.2.2.2. Population profile The population:
Is younger than the average for Wales with a higher proportion of under 35s
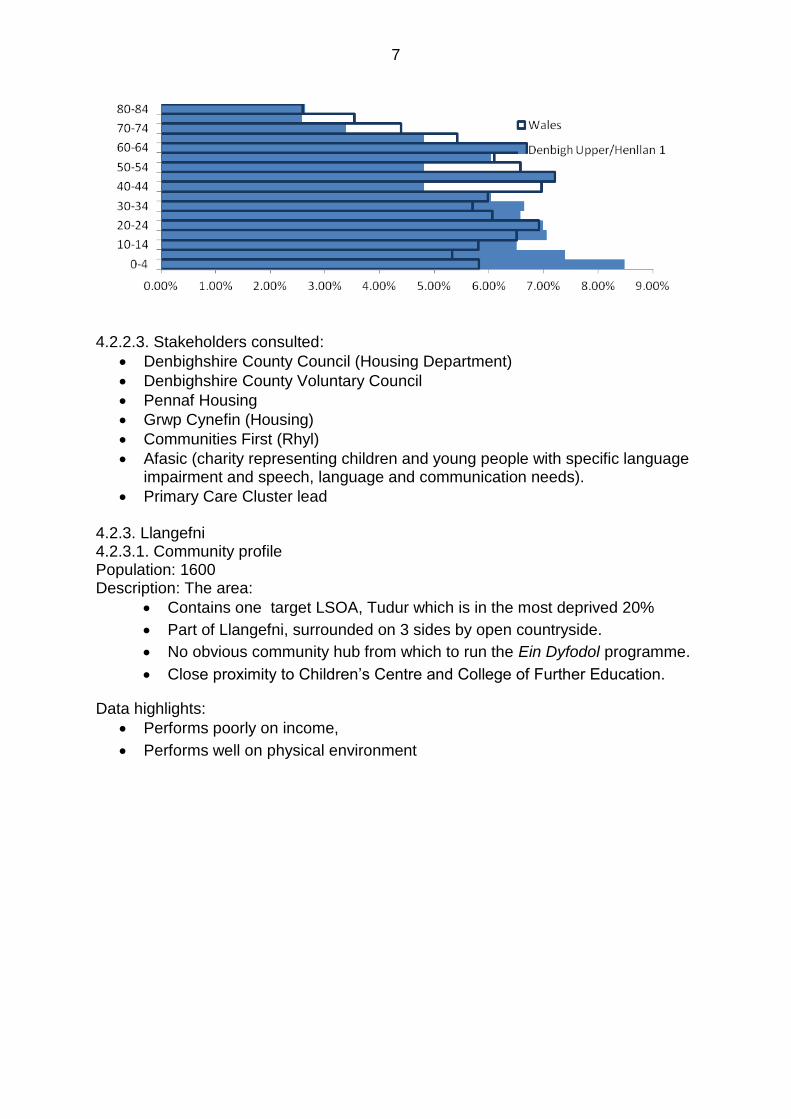
7
4.2.2.3. Stakeholders consulted:
Denbighshire County Council (Housing Department)
Denbighshire County Voluntary Council
Pennaf Housing
Grwp Cynefin (Housing)
Communities First (Rhyl)
Afasic (charity representing children and young people with specific language impairment and speech, language and communication needs).
Primary Care Cluster lead 4.2.3. Llangefni 4.2.3.1. Community profile Population: 1600 Description: The area:
Contains one target LSOA, Tudur which is in the most deprived 20%
Part of Llangefni, surrounded on 3 sides by open countryside.
No obvious community hub from which to run the Ein Dyfodol programme.
Close proximity to Children’s Centre and College of Further Education.
Data highlights:
Performs poorly on income,
Performs well on physical environment
8
4.2.3.2. Population profile The population:
is younger than the Welsh Average
profile indicative of families
4.2.3.3. Stakeholders consulted:
Ynys Môn County Council (Development of anti-poverty strategy).
Ynys Môn County Council (Housing Department)
Medrwn Môn (County Voluntary Council)
Communities First (Holyhead)
Anglesey Community Voice
Pennaf Housing Association
Age Cymru Gwynedd & Môn
Primary Care Cluster lead
Sylfaen Cymunedol
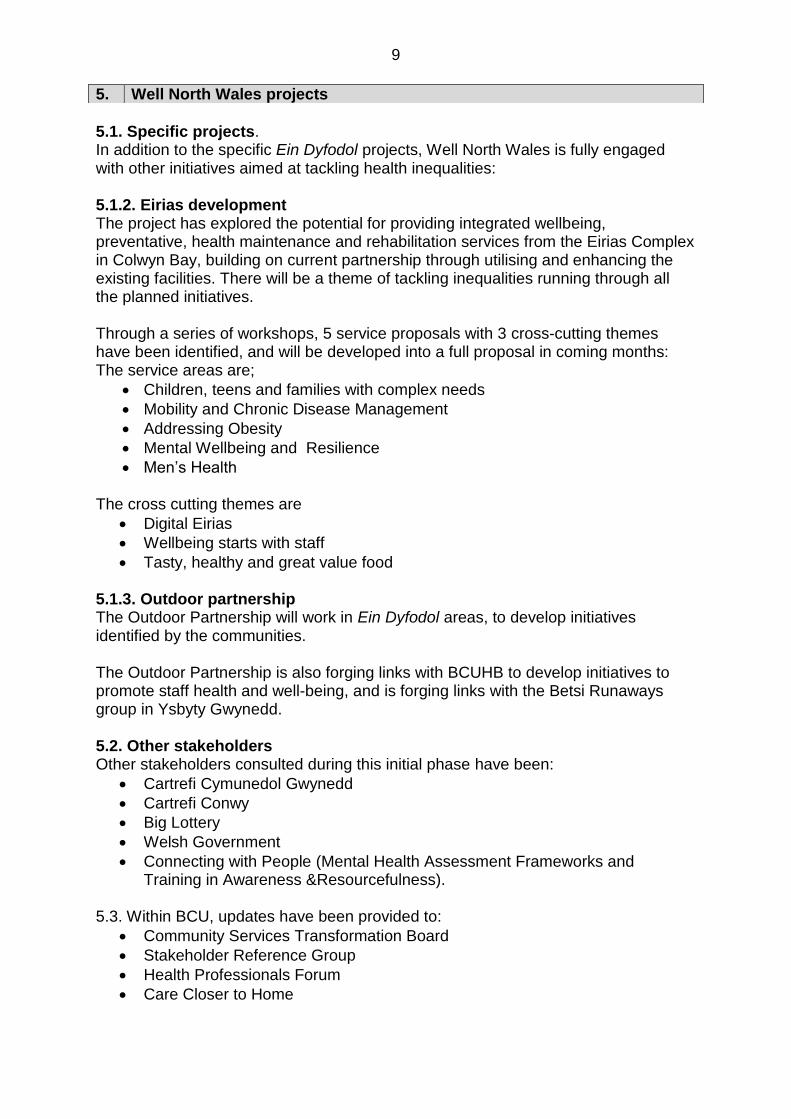
9
5.1. Specific projects. In addition to the specific Ein Dyfodol projects, Well North Wales is fully engaged with other initiatives aimed at tackling health inequalities: 5.1.2. Eirias development The project has explored the potential for providing integrated wellbeing, preventative, health maintenance and rehabilitation services from the Eirias Complex in Colwyn Bay, building on current partnership through utilising and enhancing the existing facilities. There will be a theme of tackling inequalities running through all the planned initiatives. Through a series of workshops, 5 service proposals with 3 cross-cutting themes have been identified, and will be developed into a full proposal in coming months: The service areas are;
Children, teens and families with complex needs
Mobility and Chronic Disease Management
Addressing Obesity
Mental Wellbeing and Resilience
Men’s Health The cross cutting themes are
Digital Eirias
Wellbeing starts with staff
Tasty, healthy and great value food 5.1.3. Outdoor partnership The Outdoor Partnership will work in Ein Dyfodol areas, to develop initiatives identified by the communities. The Outdoor Partnership is also forging links with BCUHB to develop initiatives to promote staff health and well-being, and is forging links with the Betsi Runaways group in Ysbyty Gwynedd. 5.2. Other stakeholders Other stakeholders consulted during this initial phase have been:
Cartrefi Cymunedol Gwynedd
Cartrefi Conwy
Big Lottery
Welsh Government
Connecting with People (Mental Health Assessment Frameworks and Training in Awareness &Resourcefulness).
5.3. Within BCU, updates have been provided to:
Community Services Transformation Board
Stakeholder Reference Group
Health Professionals Forum
Care Closer to Home
5. Well North Wales projects

10
The Well North Wales project is forging number of multi-agency partnerships. Programme accountability will therefore have to be linked to a multi agency forum. The following chart outlines:
The creation of Neighbourhood Advisory Groups for each of the Ein Dyfodol projects. These will be made up of community leaders and relevant stakeholders.
A steering group, which will include Bangor University, to oversee and co-ordinate the development of the Ein Dyfodol projects.
A multi-agency Inequalities Programme Board, which will include the Ein Dyfodol and other health inequalities programmes where the Health Board is a lead organisation.
Accountability within BCUHB to the Improving Health Reducing Inequalities Board.
Direct accountability to the four Public Services Boards to ensure that the multi-agency nature of the partnership working is reflected back into the main multi-agency forum within each area or county.
Close working links with the proposed Bevan Innovation Hub to tie in the research and evaluation component addressing health inequalities.
Reciprocal links with the 2025 movement to ensure co-ordination of activity, and to avoid duplication.
6. Project governance and accountabilities
11
7. Conclusions / Next Steps
The period from July 2016 has seen the engagement with a very wide number of stakeholders and potential partner organisations. The response has been overwhelmingly supportive, and the infrastructure for future programme developments has been embedded into working arrangements that will be taken forward in developing partnership working. Funding for the initial phase of Ein Dyfodol will be identified by the end of November 2016, with the three area projects projected to “go live” early in 2017. The on-going Support from Well London will be invaluable in terms of overall training, support, research and evaluation, and the development of the Bevan Innovation Hub will facilitate the development of a robust locally-tailored research and evaluation framework in partnership with Bangor University. The next steps for Well North Wales are:
Agree the programme accountability and governance arrangements and introduce the management arrangements to take the different strands forward.
Identify the resources required for the introduction of the three initial Ein Dyfodol projects.
Submit a Big Lottery application for phase 2 of the Ein Dyfodol programme (to run from January 2018).
Agree the scope of programmes to be included under the Well North Wales programme.
Continue to promote the Well North Wales branding, and extend the range of stakeholders involved in the development of health inequalities projects.
8. Recommendations
The Committee is asked to note the progress made in developing the Well North Wales programme, and to endorse the accountability framework outlined in Section 6 of this paper. Additionally, the Committee is asked to approve the next steps outlined in Section 7.

3.4 SPPH16/206 Proposed Wylfa Nuclear Development
1 SPPH16.206 Wylfa update_coversheet.docx
1
Strategy, Partnerships & Population Health Committee 24.11.16 Item SPPH16/206
To improve health and provide excellent care
Title: Proposed Wylfa Nuclear Development – Health Board’s Response to Horizon Nuclear Power’s Pre Application Consultation 2 (PAC2)
Author: Mr Wyn Thomas, Assistant Area Director, Primary Care
Responsible Director:
Mr Geoff Lang, Executive Director of Strategy
Public or In Committee
Public
Strategic Goals (Indicate how the subject matter of this paper supports the achievement of BCUHB’s strategic goals –tick all that apply)
1. Improve health and wellbeing for all and reduce health
inequalities
X
2. Work in partnership to design and deliver more care
closer to home
X
3. Improve the safety and outcomes of care to match the
NHS’ best
4. Respect individuals and maintain dignity in care
5. Listen to and learn from the experiences of individuals
6. Use resources wisely, transforming services through
innovation and research
X
7. Support, train and develop our staff to excel. x
Approval / Scrutiny Route
Previous reports have been submitted to the Strategy, Partnerships and Population Health Committee regarding the proposed development.
Purpose: This report has been prepared to brief the Committee regarding the Health Board’s response to the PAC 2 Consultation being undertaken by Horizon, which ended on 25th October, and an update on other measures being taken.
Significant issues and risks
On 31st August 2016 Horizon published its PAC 2 consultation regarding the proposed nuclear development at Wylfa. This consultation ran until 25th October 2016. The consultation identified a potential rapid growth in population during the construction phase of the development which will present significant challenges for NHS services. The precise nature of these challenges and the demand which arises for health services will be influenced by a number of factors, most notably the age and sex of the workforce, the degree to which workers settle with their families and the proportion of

2
the workforce drawn from the local population. Primary and secondary care services in North Wales face significant challenges in terms of recruitment and retention, demographic changes and the capacity of the operational estate. Against this background a sudden increase in the population such as that referred to in the consultation will have an impact which will require additional resource to be provided. The Board provided its formal response by the 25th October setting out the Board’s initial assessment of the key areas likely to impact upon local services due to the growth in demand expected during the construction phase as well as where further information is required. Further work will take place over the coming months to enable costed plans, revenue and capital, to be ready as part of the response to a number of Town and Country Planning applications and Development Control Order submissions currently planned from February 2017.
Special Measures Improvement Framework Theme/ Expectation addressed by this paper
Strategic and Service Planning
Equality Impact Assessment
Potential equality impacts will be identified and assessed at each stage of the proposed development.
Recommendation/ Action required by the Committee
That the Committee note the response to the PAC2 consultation, the key issues which it raises for the Health Board and the urgent requirement for detailed discussions to take place between the Health Board and Horizon to enable detailed planning for health needs and health services in the affected areas to be undertaken.
Disclosure: Betsi Cadwaladr University Health Board is the operational name of Betsi Cadwaladr University Local
Health Board
Committee Coversheet v10 June 2016

2 SPPH16.206 Wylfa report.doc
1
Proposed Wylfa Nuclear Development – Health Board Response to Horizon Nuclear Power’s Pre Application Consultation 2 (PAC2)
1. Purpose of report
This report has been prepared to brief the Committee regarding the Health Board’s response to the PAC 2 consultation which was undertaken by Horizon between 31st August and 25th October 2016.
2. Introduction/Context
On 31st August 2016 Horizon published its PAC 2 consultation regarding the
proposed nuclear development at Wylfa. This consultation ran until 25th October
2016. Horizon previously undertook an initial consultation process PAC 1 and the
Health Board responded to PAC 1 Consultation on 5th December 2014. At that point
the Health Board noted the lack of detailed information within the consultation which
compromised the Board’s ability to respond fully and assess the impact of the
proposed development on primary and secondary care services in the area.
The Health Board is working with a number of public and third sector bodies to ensure that a co-ordinated and consistent response to consultations and future planning applications is delivered. This co-ordinated work is being led by the Isle of Anglesey County Council. In addition the Health Board is working with the Regional Leadership Board to understand the impacts upon North Wales in a broader context and develop appropriate responses. In order to respond effectively to the consultation and to oversee the development of plans to meet the health needs of the temporary workforce and to minimise the impact on the resident population, the Health Board has established a ‘Primary and Secondary Care Impacts and Mitigation Programme Board, chaired by the Director of Strategy. The programme board includes representatives from primary and secondary care, Welsh Ambulance Services NHS Trust, Public Health Wales and the Isle of Anglesey Council.
To support the project, a business case has been produced and submitted to Horizon, seeking financial support for a Project Manager and administrative support to co-ordinate the work, undertake data collection and analysis, draft papers and collate necessary submissions. To date no response has been received from Horizon regarding the application. The work of the Programme Board is reported to the Strategy, Partnerships and Population Health Committee for assurance purposes.

2
3. The Consultation
PAC 2 commenced on 31st August and ended on 25th October 2016.
The Programme Board oversaw the response to the PAC 2 consultation document and will continue to meet to prepare for the associated planning applications that are planned to be submitted to Isle of Anglesey County Council between October this year and February 2017 in advance of the Development Control Order submission which is planned for May 2017. Public Health Wales and the Welsh Ambulance Services NHS Trust also responded to the consultation.
4. Key Issues for the Health Board
A copy of the full response is attached as appendix 1 of this report. In summary the key points to note are: General Comments
The PAC 2 documentation provided further information beyond that previously available regarding the numbers of workers over the construction period and it also clarified the preferred locations of the temporary workers accommodation, however there are concerns that the documents demonstrate a limited understanding of the potential impact of the development on existing health services and do not identify what mitigation is to be put in place to address the impact.
Statements are made that there will not be significant effects on public
services (including GPs) because Horizon has made a commitment to provide all the additional services that will be required to support the increased population. Whilst we welcome these commitments, we expected the consultation documents to be more explicit about what these services would include, their locations and how, if at all they would link in to the statutory services provided by the BCUHB.
The informal consultation undertaken in January stated that Horizon was in
the process of deciding the best way to provide healthcare services for construction workers. In doing so it asked whether health services should be delivered by enhancing existing local health services or by the provision of separate services for use specifically by the workers. The consultation documents still leave this question open.
The Health Impact Assessment Interim Report (HIA) in Para 9.3 states that
“Service planning discussions between BCUHB and other service providers are in progress to determine how and where services would be provided for construction workers.” In this regard the documents imply more joint planning and agreement between Horizon and BCUHB than is the case in reality.

3
We understand that the HIA will be updated in October and that a Health and Well-being strategy is being developed. It is regrettable that the consultation did not have access to these as they may have provided further information regarding Horizon’s plans for health care services and enabled a more constructive consultation.
The HIA has only dedicated 4 of its 101 pages to the demand for medical and
healthcare services. It has highlighted the development’s potential impact on GP services, mental health services, dentists, pharmacies, health protection services, and acute hospital services. Whilst we accept that the list may not have been intended to be exhaustive, it is essential at this stage to record that we anticipate that there will also be effects on a range of community services including nursing, therapies, children’s services, midwifery services and substance misuse services.
The HIA’s assessment of the overall health effect of demand for medical and
healthcare services (after mitigation) is considered to be neutral (Para 9.20). Given our comments and concerns we do not agree with the assessment. In the absence of a clear understanding of how services will be provided and a comprehensive mitigation plan, this statement cannot be supported.
We welcome the clarity on the projected number of temporary workers over
the construction period and the proposals for accommodating them. Further information is however required regarding the likely demography and ethnicity of the workforce to enable us to assess potential health needs and impacts.
We support the focus on developing temporary workers accommodation in three areas, Holyhead, Amlwch and on site, subject to robust plans being in place to meet the healthcare needs of the local and temporary populations.
The descriptions of the various accommodation options include provision of medical treatment/first aid rooms. It is unclear from the documents what this actually means in practice. Similarly the plans for the main site do not appear to show a major health facility.
The temporary accommodation developments are expected to provide accommodation for up to a maximum of 5,700 workers and in these geographic locations we will be able to undertake an assessment of the impact on local services. The same cannot be said for the 3,320 workers anticipated to be housed in existing stock across the island and the Arfon area of Gwynedd.
It is also important to note that National grid is consulting on an associated development currently which estimates some additional 400 workers as part of that development. These workers will also need to assess health care services and a co-ordinated response would be helpful in this regard.
4
Meeting the Health Needs of the Temporary Workforce
Currently primary and secondary care services in North Wales face significant challenges in terms of recruitment and retention, demographic changes and physical estate capacity. In this context a sudden increase in the population will have an impact on service provision which must be planned for and resourced.
Currently Anglesey GPs are, on average, responsible for 1,620 patients per GP whole time equivalent (WTE) with Arfon GPs responsible for an average of 1,777 per GP WTE. The impact of the temporary workforce accommodation at its maximum, based on information provided of likely accommodation locations will be to increase these to 1,831 and 1,791 respectively.
Lead times for estate enhancement, training and recruitment of staff are challenging given the proposed development timetable and this emphasises the need to urgently address gaps in the information available to enable the design of appropriate service responses.
There is concern that existing clinical and administrative staff may migrate to new services (displacement effect) thereby adversely impacting on existing health services.
The scale and complexity of this proposed development is such that a comprehensive response plan for health services is required. Based on the limited information available we have discussed this with local GPs, our staff and the Welsh Ambulance Service Trust. We have identified a range of issues which require further work and discussion with Horizon to enable an appropriate service response to be implemented, as follows – a) There is a need for Horizon to make available a health provision for
workers on the Wylfa site to meet immediate health needs for their
workforce. It is considered that this is the most effective way of reducing
negative impacts on existing services such as minor injuries and routine
primary care.
b) Regardless of the level of health provision on site there will be an
increased demand from workers and their families in Holyhead and
Amlwch for access to core primary care services. Additional investment in
staff and accommodation for the Holyhead and Amlwch areas to meet this
potential increased demand will be required.
c) Additional revenue investment in primary care, community and secondary
hospital services will be required to meet the unfunded increase in
demand for services.
.
5
d) We have seen assessments of the additional dental requirements which
identify the number of additional dentists required. Existing dental services
provide regular access to NHS dentistry for approximately 50% of the
resident population, with significant capacity constraints. To meet the
needs of the temporary workforce we believe that Horizon should make
specific arrangements for the workforce, potentially linked to the proposed
on site facility.
The consultation is silent on opportunities the development will have to promote improved health and well-being for the workers with initiatives such as smoke free environments, healthy eating, green travel etc. We would wish to see a clear emphasis and commitment from Horizon to promoting and protecting the health of its workforce.
Impact on Transport and Travel
We have concerns about the impact the significant increase in road traffic will have on a range of issues including increased road traffic accidents and delays for emergency and routine travel to health care facilities both on and off the island for patients, emergency services and staff.
5. Equality Impact Assessment
Potential equality impacts will be identified and assessed at each stage of the proposed development.
6. Conclusions / Next Steps
The consultation has provided further information on the scale and impact of the development. However, we are concerned that there is still a lack of clarity about Horizon’s plans for meeting the health needs of the temporary workforce and their dependants. Further information is required about the demography, ethnicity and potential families of the workforce to enable a detailed assessment to be undertaken and a model of health services developed to meet the assessed need. The Health Board believes that the development and the scale of the associated temporary workforce will have a significant impact on existing services, unless mitigated against, which must be planned for in terms of service delivery, physical capacity and financial resources, both capital and revenue. We have identified a potential impact on a wide range of services. We consider the need for an on-site service at Wylfa to be essential, with close connections to primary and community services. There are clear workforce challenges and risks which must be addressed in a co-ordinated manner to avoid detrimental effects on existing services to the local population. While the Health Board welcomes the commitments from Horizon to supporting the health needs arising from the development we remain concerned at the lack of
6
detailed planning at this stage. We believe there is a need for urgent discussions regarding the model of service to be provided and how this will be delivered and resourced. The Chief Executive has written formally to Horizon setting out the need for detailed discussions regarding this.
7. Recommendations
That the Committee note the PAC2 consultation response, the key issues which it raises for the Health Board and the intention to seek one to one discussions with Horizon to understand their plans for meeting the health care needs of the workforce and how this will fit in with local primary and secondary health care services.
7
Appendix 1 Betsi Cadwaladr University Local Health Board
Wylfa Newydd Project - PAC 2 Consultation Response
Introduction The following is the Betsi Cadwaladr University Health Board’s (BCUHB) response to the Horizon PAC2 Consultation. The response has been informed by the Board’s own assessment of potential impacts, discussions with the GP practices in Holyhead and Amlwch and Welsh Ambulance Services NHS Trust. BCUHB previously responded to PAC 1 in 2014 and the informal consultation undertaken in January 2016. Both of these responses highlighted our concerns about the impact on primary, community and secondary care health services of the significant increase in the local population of the Anglesey and Gwynedd areas during the construction stage of the Wylfa Newydd development. In our response to the informal consultation we did express a concern that we did not have a formal process of engaging with Horizon and that we felt that the impact on local health provision during construction stages had not been given sufficient focus. Furthermore, we identified deficiencies in the information available to assess the impact so as to be able to respond robustly to future planning applications and DCO submissions. 1. General Comments
The PAC 2 documentation has provided further information beyond that previously available regarding the numbers of workers over the construction period. It has also clarified the preferred locations of the temporary workers accommodation, however we are concerned that the documents demonstrate a limited understanding of the potential impact of the development on existing health services and do not identify what mitigation is to be put in place to address the impact. This is disappointing given the extent of information and the detailed understanding there appears to be on a range of other issues such as transport, highway improvements, habitats and Welsh Language etc. Para 10.12 in the Preliminary Environment Information Report states that “there would be no significant effects on public services (including GPs) because Horizon has made a commitment to provide all the additional services that would be required to support the increased population”. The Health Impact Assessment Interim Report (HIA) also states in Para 9.8 that “local people would not be worse off because Horizon is committed to providing for the healthcare of the construction workforce.” Whilst we welcome these commitments, we expected the consultation documents to be more explicit about what these services would include, their locations and how, if at all they would link in to the statutory services provided by the BCUHB. The informal consultation undertaken in January stated that Horizon were in the process of deciding the best way to provide healthcare services for construction workers. In doing so it asked whether health services should be delivered by enhancing existing local health services, or by the provision of separate services for

8
use specifically by the workers. The consultation documents still leave this question open. The HIA in Para 9.9 states “a mix of ....options is likely to be appropriate.” These statements are concerning to the Health Board as we are unclear of the process and timescales proposed to agree the final health care model, which will, we believe, have significant service and financial implications for the Health Board. The Health Impact Assessment Interim Report (HIA) in Para 9.3 states that “Service planning discussions between BCUHB and other service providers are in progress to determine how and where services would be provided for construction workers.” While the Health Board and other public sector bodies are participants in a number of fora discussing the proposed development, we do not believe that to date we have had the detailed discussions or the requisite information to plan how and where services should be provided. In this regard the documents imply more joint planning and agreement between Horizon and BCUHB than is the case in reality. Going forward we believe there is an urgent need for focussed discussions between the Health Board and Horizon to address this deficit and agree a model, so as to ensure health services for the local and temporary population are not adversely affected during the development stage. We understand that the HIA will be updated in October and that a Health and Well-being strategy is being developed. It is regrettable that the consultation did not have access to these as they may have provided further information regarding Horizon’s plans for health care services and enabled a more constructive consultation. The HIA has only dedicated 4 of its 101 pages to the demand for medical and healthcare services. It has highlighted the development’s potential impact on GP services, mental health services, dentists, pharmacies, health protection services, and acute hospital services. Whilst we accept that the list may not have been intended to be exhaustive, it is essential at this stage to record that we anticipate that there will also be effects on a range of community services including nursing, therapies, children’s services, midwifery services and substance misuse services. A significant omission from the schedule is the Out of Hours GP service that would likely be responsible for the primary care needs of the significantly increased population during evenings and weekends . The HIA’s assessment of the overall health effect of demand for medical and healthcare services (after mitigation) is considered to be neutral (Para 9.20). Given our comments and concerns above we do not agree with the assessment. In the absence of a clear understanding of how services will be provided and a comprehensive mitigation plan, this statement cannot be supported. 2. Temporary Workers Accommodation
We welcome the clarity on the projected number of temporary workers over the construction period and the proposals for accommodating them. Further information is however required regarding the likely demography and ethnicity of the workforce to enable us to assess potential health needs and impacts. In addition, we believe there is potential for a significant number of workers to bring their families to the area which will impact on a broad range of services that may not be identified if the focus

9
is purely on the workforce. Further information on this aspect is fundamental to providing a definitive response. Our response to the informal consultation expressed a preference that temporary accommodation be focused on one area, however subsequent discussions with local GPs has revised this view. We support the focus on three areas, Holyhead, Amlwch and on site, subject to robust plans being in place to meet the healthcare needs of the local and temporary populations. The descriptions of the various accommodation options include provision of medical treatment/first aid rooms. It is unclear from the documents what this actually means in practice; what level of service provision is proposed and how this will be provided. Similarly the plans for the main site do not appear to show a major health facility. We require clarity on these as it is one of the key issues that affect our planning for the impact on existing primary care and other services in the immediate areas. With regard to the accommodation proposals for Holyhead (Land and Lakes) the consultation document refers to the Section 106 agreement with Isle of Anglesey County Council (IACC) for health contributions to mitigate the impact on health facilities during occupation of the development by nuclear workers (Para 15.25). Whilst this is welcomed, we believe we need to look at the impact of the Wylfa development in totality and the cumulative effect of the development, rather than plan and mitigate on a site by site basis. The above developments are expected to provide accommodation for up to a maximum of 5,700 workers and in these geographic locations we will be able to undertake an assessment of the impact on local services. The same cannot be said for the 3,320 workers anticipated to be housed in existing stock across the island and the Arfon area of Gwynedd. These people will potentially access services in the vicinity of their accommodation and more work is required to assess how this demand can be met without having a detrimental effect upon existing local services. It is also important to note that National grid are consulting on an associated development currently which estimates some additional 400 workers as part of that development. These workers will also need to assess health care services and a co-ordinated response would be helpful in this regard. 3. Meeting the Health Needs of the Temporary Workforce
Currently primary and secondary care services in North Wales face significant challenges in terms of recruitment and retention, demographic changes and physical estate capacity. In this context a sudden increase in the population will have an impact on service provision which must be planned for and resourced. Currently Anglesey GPs are, on average, responsible for 1,620 patients per GP whole time equivalent (WTE) with Arfon GPs responsible for an average of 1,777 per GP WTE. The impact of the temporary workforce accommodation at its maximum, based on information provided of likely accommodation locations will be to increase these to 1,831 and 1,791 respectively. The situation in Holyhead at present is 2,059 patients per GP WTE which would increase to 2,418, and in Amlwch from 1,760 to
10
2,142. These increases relate to the bespoke accommodation provision and do not include a proportion of those living in private accommodation, which would increase these numbers further. These increases are clearly significant and represent a step change in demand which could not be accommodated without additional capacity. We are particularly aware that while the Holyhead and Amlwch areas currently have fully staffed GP practices, they would not be able to meet the needs of the additional population in their current practice buildings or with their current staffing. To attempt to do so would have a clear negative impact on the provision to the indigenous population. In addition as stated above there will be a maximum of a further 3,320 workers who will be accommodated across the island and the Arfon area. Lead times for estate enhancement, training and recruitment of staff are challenging given the proposed development timetable and this emphasises the need to urgently address gaps in the information available to enable the design of appropriate service responses. The scale and complexity of this proposed development is such that a comprehensive response plan for health services is required. Based on the limited information available we have discussed this with local GPs , our staff and the Welsh Ambulance Service Trust. We have identified a range of issues which require further work and discussion with Horizon to enable an appropriate service response to be implemented, as follows -
a) There is a need for Horizon to make available a health provision for
workers on the Wylfa site to meet immediate health needs for their
workforce. It is considered that this is the most effective way of reducing
negative impacts on existing services such as minor injuries and routine
primary care.
Further discussion is required to define this model, but we believe it should seek to provide a broad range of services which could potentially include minor injuries, minor illness, chronic disease management and repeat prescribing. It is essential that any on site provision has a clear link with local health services to ensure continuity of care and a positive health experience for the workers. The role that local GPs and other health staff play in providing this service and the associated resource implications needs to be developed in partnership with Horizon. There is concern that existing clinical and administrative staff may migrate to such services (displacement effect) thereby impacting on existing health services. This could be mitigated by maximising the connection between on site and local NHS services. Likewise a potential detrimental effect could be seen in the care industry supporting people at home and in nursing and residential homes if planning is not sufficiently co-ordinated. We believe it will be necessary to increase the pool of clinical staff in the area by funding core and advanced training for a number of professions in advance of the development to support the services for the resident and temporary population in the area.

11
b) Regardless of the level of health provision on site there will be an
increased demand from workers and their families in Holyhead and
Amlwch for access to core primary care services. Additional investment in
staff and accommodation for the Holyhead and Amlwch areas to meet this
potential increased demand will be required.
The current practices are already dealing with increased demand for services and have limited or no scope to expand the physical space available to provide for this additional need. Investment in infrastructure would not only be crucial to cope with the demand during the construction period, but would also provide a longer term legacy for the population. We do have concerns about the timescales to agree, plan and construct any estate requirements in time for the start of the construction work in 2019, although we do acknowledge that we have more time to plan for the more significant increases in the workforce which arise later in the project.
c) Additional revenue investment in primary care, community and secondary
hospital services will be required to meet the unfunded increase in
demand for services.
The core funding streams available to the Health Board will not meet the potential additional costs which will arise directly as a result of this development. Services are currently stretched and any un-resourced increase in demand will impact negatively on services to local residents.
d) We have seen assessments of the additional dental requirements which
identify the number of additional dentists required. Existing dental services
provide regular access to NHS dentistry for approximately 50% of the
resident population, with significant capacity constraints. To meet the
needs of the temporary workforce we believe that Horizon should make
specific arrangements for the workforce, potentially linked to the proposed
on site facility.
The consultation is silent on opportunities the development will have to promote improved health and well-being for the workers with initiatives such as smoke free environments, healthy eating, green travel etc. We would wish to see a clear emphasis and commitment from Horizon to promoting and protecting the health of its workforce.
4. Impact on Transport and Travel
We have concerns about the impact the significant increase in road traffic will have on a range of issues including increased road traffic accidents and delays for emergency and routine travel to health care facilities both on and off the island for patients, emergency services and staff. We note that while there are plans to improve the road from Valley to Cemaes there are no plans to improve the road from Cemaes to Amlwch. Given that accommodation will be provided in Amlwch and that workers will be bussed in from

12
both east and west of the Wylfa site we are concerned about the effect of the increase in journeys and the potential for increased road accidents, especially where the roads have not been improved. We note from the consultation that there is currently no intention of providing a park and ride facility on the mainland. The Health Board would be interested in exploring the potential for such a development with Horizon as there are current pressures on parking at Ysbyty Gwynedd which such a facility could support, as well as bringing benefits to other employers in the area. 5. Conclusion
The Health Board welcomes the clarity provided in relation to the proposed temporary workforce and the clear preferences of Horizon for temporary accommodation to be sited at Holyhead, Amlwch and Wylfa. We are concerned that there is still a lack of clarity about Horizon’s plans for meeting the health needs of the temporary workforce and their dependants. Further information is required about the demography, ethnicity and poltential families of the workforce to enable a detailed assessment to be undertaken and a model of health services developed to meet the assessed need. The Health Board believes that the development and the scale of the associated temporary workforce will have a significant impact on existing services which must be planned for in terms of service delivery, physical capacity and financial resources, both capital and revenue. We have identified a potential impact on a wide range of services. We consider the need for an on-site service at Wylfa to be essential, with close connections to primary and community services. There are clear workforce challenges and risks which must be addressed in a co-ordinated manner to avoid detrimental effects on existing services to the local population. While the Health Board welcomes the commitments from Horizon to supporting the health needs arising from the development we remain concerned at the lack of detailed planning at this stage. We believe there is a need for urgent discussions regarding the model of service to be provided and how this will be delivered and resourced. The Health Board wishes to establish a mechanism for continued dialogue with Horizon with regards to the on-going review process required over the medium and longer terms, as the true impact of the development evolves and wider impacts upon healthcare in North Wales become evident. The Health Board will seek support in both revenue and capital terms through the Town and Country Planning Act provisions to ensure that the health needs of the workers at Wylfa can be met in a manner which does not negatively impact upon services to the local population.
Geoff Lang, Director of Strategy 25.10.2016

3.5 SPPH16/207 Annual Plan Monitoring Report - Quarter 2
1 SPPH16.207 AOP Q2_coversheet.docx
1
Strategy, Partnerships & Population Health Committee 24.11.16 Item SPPH16.207
To improve health and provide excellent care
Title: Annual Plan Monitoring Report – Quarter 2
Author: Mr John Darlington, Assistant Director, Corporate Planning
Responsible Director:
Mr Geoff Lang, Executive Director of Strategy
Public or In Committee
Public
Strategic Goals (Indicate how the subject matter of this paper supports the achievement of BCUHB’s strategic goals –tick all that apply)
1. Improve health and wellbeing for all and reduce health
inequalities
x
2. Work in partnership to design and deliver more care
closer to home
x
3. Improve the safety and outcomes of care to match the
NHS’ best
x
4. Respect individuals and maintain dignity in care x
5. Listen to and learn from the experiences of individuals x
6. Use resources wisely, transforming services through
innovation and research
x
7. Support, train and develop our staff to excel. x
Approval / Scrutiny Route
The progress assessment set out in the report has been subject to scrutiny at Executive Team prior to presentation to the Committee.
Purpose: This paper presents a high level summary of progress made in quarteragainst the Annual Operating Plan Key Deliverables 2016/17 which were agreed by theBoard in May 2016.
Significant issues and risks
The Board’s Annual Operational Plan summary of key deliverables set out the key priorities for the Health Board during the financial year 2016/17. The document clearly defined quarterly actions which were required to deliver the commitments over the financial year.
These deliverables reflect the Board’s responsibilities and commitment as a Health Board to focus upon improving the health of the people of North Wales whilst also striving to continually improve the quality, safety and accessibility of health services.
The report summarises the progress made against delivery of the plan in the period April to September 2016. The first report, which was produced in July identified good early progress, however a number of

2
actions which were due to be completed in quarter 1 were outstanding at the end of that period. These actions are picked up in this report with progress as at the end of September summarised for each. There were 51 actions at the end of quarter 1 which remained outstanding. Of these, 33 have now been completed and 18 remain outstanding as at the end of quarter 2. This equates to 85% of actions from quarter now completed.
For quarter 2 there were 111 actions set out for achievement. Against these actions the assessment of progress shows that 71 have been achieved in full and 39 achieved in part and 1 not met. This equates to 64% completion in quarter. The comparable completion rate in quarter 1 was 59%.
Overall, 75% of all actions planned for completion from 1st April to 30th September have been fully delivered.
It should be noted that the report does not provide a detailed assessment against performance trajectories as this is contained in the Integrated Quality and Performance Report which is received by the Board on a monthly basis.
Special Measures Improvement Framework Theme/ Expectation addressed by this paper
The operational plan key deliverablesset out the actions agreed by the Board to respond to all aspects of the Special Measures framework.
Equality Impact Assessment
The operational plan was subject to an Equality Impact Assessment at the time of its development.
Recommendation/ Action required by the Committee
That the Committee note the content of the report and consider the progress made at end of quarter 2
Disclosure: Betsi Cadwaladr University Health Board is the operational name of Betsi Cadwaladr University Local Health Board
Committee Coversheet v10 June 2016

2 SPPH16.207 AOP report Q2.doc
1
ANNUAL PLAN MONITORING REPORT – QUARTER 2
Purpose
This paper presents a high level summary of progress made in quarter 2 against the Annual Operating Plan Key Deliverables 2016/17 which
were agreed by the Board in May 2016.
Background and Introduction
The Board’s Annual Operational Plan summary of key deliverables set out the key priorities for the Health Board during the financial year
2016/17. The document clearly defined quarterly actions which were required to deliver the commitments over the financial year. These
deliverables reflect the Board’s responsibilities and commitment as a Health Board to focus upon improving the health of the people of North
Wales whilst also striving to continually improve the quality, safety and accessibility of health services.
The report summarises the progress made against delivery of the plan in the period April to September 2016.
Assessing Progress
This is the second report prepared to assess progress against the key deliverables for 2016/17 which were agreed by the Board in May 2016.
The deliverables were defined against a series of key themes from the Annual Operational Plan and set out clear quarterly milestones against
which progress could be tracked as the year progresses.
Progress against actions has been assessed using a Red, Amber, Green (RAG) status as set out below.
RAG Status – Summary
Action Delivered in Full
Action Partially Delivered
Action not Progressed
The first report, which was produced in July identified good early progress, however a number of actions which were due to be completed in
quarter 1 were outstanding at the end of that period. These actions are picked up in this report with progress as at the end of September
summarised for each. There were 51 actions at the end of quarter 1 which remained outstanding. Of these, 33 have now been completed and
18 remain outstanding as at the end of quarter 2. This equates to 85% of actions from quarter now completed.

2
For quarter 2 there were 111 actions set out for achievement. Against these actions the assessment of progress shows that 71 have been
achieved in full and 39 achieved in part and 1 not met. This equates to 64% completion in quarter. The comparable completion rate in quarter 1
was 59%.
Overall, 75% of all actions planned for completion from 1st April to 30th September have been fully delivered.
The full details of the RAG status are shown in Appendix 1 and the section below summarises the key themes from this assessment, both in
terms of positive progress and areas where focussed action is required to recover performance.
In addition to the quarterly schedule of deliverables the Board agreed trajectories for performance improvement throughout the year. Progress
against these trajectories is reported through the Integrated Quality and Performance Report which is received by the Board on a monthly
basis.
Improving Health
Summary Actions Completed %
Quarter 1 Position as reported in July 2016 10 48%
Quarter 1 Status at 30th September 2016 19 90%
Quarter 2 Actions completed at 30th September 2016 16 73%
Quarter 1 and 2 Actions completed at 30th September 35 81%
Significant progress has been made against a number of priority areas for improving health and reducing inequalities. Positive performance has
been maintained in terms of immunisation and activities to enhance access to smoking cessation services. The role of community pharmacy in
smoking cessation is being optimised. Work to expand opportunities to promote health and wellbeing advice through brief intervention training
and adopting the “make every contact count” approach is progressing.
The Board’s “Well North Wales” programme is developing with wide engagement with partners taking place. Three communities have now
been identified for early adoption of this programme. Clear leadership in this area is evident through the Programme Director and supporting
governance structures are developing.

3
Whilst general access to smoking cessation services is increasing in line with expectations, the results achieved in terms of quit rate are not
matching this growth in numbers and further action is required in the remainder of the year to address this deficit. Investment in capacity to
support smoking cessation activities with pregnant women has progressed but some delays in recruitment have slowed progress. This will be
recovered in quarter 3 as roles are filled and targeted support is deployed. Further training and adoption of the MECC approach is required in
quarter3 to scale up its impact across the Health Board.
Primary and Community Care
Summary Actions Completed %
Quarter 1 Position as reported in July 2016 14 64%
Quarter 1 Status at 30th September 2016 19 86%
Quarter 2 Actions completed at 30th September 2016 12 60%
Quarter 1 and 2 Actions completed at 30th September 31 74%
There are a number of areas of positive development within the primary and community care elements of the plan. At an operational level the
Health Board has responded positively to the need to take on the management of a number of GP Practices due to resignations and has met
this challenge during quarter 2 specifically in Wrexham. The role and contribution of Clusters is developing, with plans submitted and
developments progressing utilising the additional resources allocated in year.
Examples of innovative services developing in the community, transferring work from secondary care include heart failure services and
diabetes. Clinical pathways to support access to multi disciplinary teams have been developed in rheumatology and diabetes. Additional
capacity has been commissioned in General Dental Services to ease pressures on access during the remainder of the financial year. The pace
of implementation of some service changes has been impacted by recruitment challenges. Workforce mapping in primary care has progressed
but gaps in data available have resulted in the commitment to develop a workforce plan by the end of quarter 2 not being delivered. This work
will continue in quarter 3.
Work with partners is progressing through the Intermediate Care Fund. Health and social care workers have been introduced across North
Wales and access to services is operating via county based “single point of access”. District nursing services are expanding and the roll-out of
24 hour access to district nursing has commenced.

4
Work to progress estate improvements in primary care is ongoing. Both Benllech and Colwyn Bay primary care centres were completed and
opened in accordance with the project plan. The review of primary care estate condition has concluded and its findings will now be used to
inform estate planning for 2017/18 and beyond.
Alongside this positive progress, the RAG assessment identifies a number of areas where increased focus is required. The development of
referral pathways and demand management within medical specialties has not progressed at the rate expected. Further work is required to
ensure optimal benefit from the diabetes and rheumatology work above and to develop in specialties such as cardiology and dermatology.
Service design work to define the future roll of community hospitals has not progressed at the rate anticipated in the plan resulting in delay.
This will be addressed in quarter 3.
Work to implement patient based risk stratification has not progressed and is assessed as RED at the end of quarter 2. This work has been
escalated for quarter 3 and models are being explored including evidence from Australia.
Unscheduled Care
Summary Actions Completed %
Quarter 1 Position as reported in July 2016 1 11%
Quarter 1 Status at 30th September 2016 8 88%
Quarter 2 Actions completed at 30th September 2016 8 73%
Quarter 1 and 2 Actions completed at 30th September 16 80%
Significant work has been undertaken in quarter 2 to recover actions that were outstanding at the end of quarter 1 including clinical triage
models working with WAST, dynamic divert and the development of unscheduled care hubs.
Positive progress has been reported in the implementation of new pathways in the community which are beginning to impact upon patient flow.
Work to enhance the response to meet the needs of patients with mental health problems, particularly in the emergency department setting has
progressed. More capacity is available in liaison services and this is being focussed to have a positive impact upon unscheduled care delivery.
The Seasonal Plan was developed by the end of quarter 2 as expected and has been presented to the Board. Further work is ongoing in a
number of areas and the final version is being developed in Q3.

5
Progress with the development of some community response services has been compromised due to recruitment challenges and this remains
a risk to delivery going forward. Work to develop a better understanding and a new approach to independent sector resilience and market
development has been progressed in partnership with Local Authorities on a regional basis, however the expected timeline for this work has not
been met. Further leadership capacity has been identified to progress at a faster rate in quarter 3 to achieve the joint priorities identified.
Planned Care
Summary Actions Completed %
Quarter 1 Position as reported in July 2016 5 36%
Quarter 1 Status at 30th September 2016 8 57%
Quarter 2 Actions completed at 30th September 2016 3 50%
Quarter 1 and 2 Actions completed at 30th September 11 55%
Work has continued in quarter 2 to address pathways and access to planned care services. Pathways to optimise the use of audiology services
and a revised pathway for cataracts have been adopted. Where external capacity is available this has been commissioned in line with plans
and is making a positive contribution to elective capacity. Plans for quarter 3 and 4 for RTT have been developed in accordance with the
timescales set.
Work has progressed to identify capacity needs and strategic options for orthopaedic services supported by strong clinical engagement.
Options will be discussed with the Board in quarter 3 to inform future years’ plans.
Limited progress is reported in outpatient and theatre productivity compared to that anticipated within the plan. Focussed plans are in place to
address these areas further in quarter 3 as part of the Board’s PMO programme of work.
Positive progress has been reported in relation to reducing follow up backlog across the Health Board but this is not at the scale or pace
required to reduce the potential clinical risks to patients associated with this position. Further action is required in quarter 3 to increase the pace
of delivery in this area.
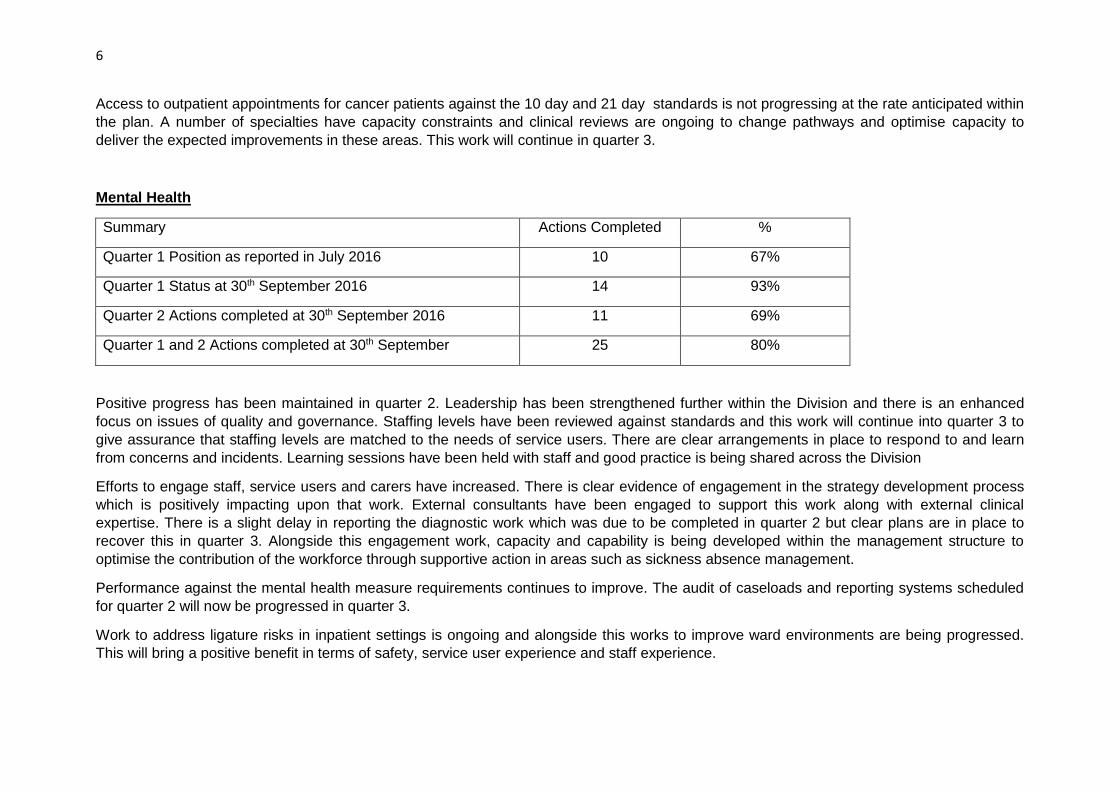
6
Access to outpatient appointments for cancer patients against the 10 day and 21 day standards is not progressing at the rate anticipated within
the plan. A number of specialties have capacity constraints and clinical reviews are ongoing to change pathways and optimise capacity to
deliver the expected improvements in these areas. This work will continue in quarter 3.
Mental Health
Summary Actions Completed %
Quarter 1 Position as reported in July 2016 10 67%
Quarter 1 Status at 30th September 2016 14 93%
Quarter 2 Actions completed at 30th September 2016 11 69%
Quarter 1 and 2 Actions completed at 30th September 25 80%
Positive progress has been maintained in quarter 2. Leadership has been strengthened further within the Division and there is an enhanced
focus on issues of quality and governance. Staffing levels have been reviewed against standards and this work will continue into quarter 3 to
give assurance that staffing levels are matched to the needs of service users. There are clear arrangements in place to respond to and learn
from concerns and incidents. Learning sessions have been held with staff and good practice is being shared across the Division
Efforts to engage staff, service users and carers have increased. There is clear evidence of engagement in the strategy development process
which is positively impacting upon that work. External consultants have been engaged to support this work along with external clinical
expertise. There is a slight delay in reporting the diagnostic work which was due to be completed in quarter 2 but clear plans are in place to
recover this in quarter 3. Alongside this engagement work, capacity and capability is being developed within the management structure to
optimise the contribution of the workforce through supportive action in areas such as sickness absence management.
Performance against the mental health measure requirements continues to improve. The audit of caseloads and reporting systems scheduled
for quarter 2 will now be progressed in quarter 3.
Work to address ligature risks in inpatient settings is ongoing and alongside this works to improve ward environments are being progressed.
This will bring a positive benefit in terms of safety, service user experience and staff experience.

7
As described under the unscheduled care section work is progressing to improve liaison services and unscheduled care response. At this stage
the redesign of the pathways for unscheduled care has not been progressed as envisaged in the plan. This work will now be progressed under
the strategy development work, whilst the in year focus remains on delivering improved responses with the additional resources available.
Maternity
Summary Actions Completed %
Quarter 1 Position as reported in July 2016 4 80%
Quarter 1 Status at 30th September 2016 5 100%
Quarter 2 Actions completed at 30th September 2016 4 80%
Quarter 1 and 2 Actions completed at 30th September 9 90%
Positive progress against the milestones within the Plan continues to be reported. Medical staffing levels are improved, with consultant
recruitment progressing successfully to support the revised medical staffing model. Further appointments are scheduled for quarter 3. Work to
develop service models for the future has commenced, engaging clinical leaders and reflecting upon the report of the Royal College of
Obstetrics and Gynaecology.
The SuRNICC business case was presented to Welsh Government in accordance with the agreed timescale and has been positively received.
Work on the development will commence in quarter 3.
Risk assessment and management continues to function effectively and is providing increased levels of assurance with regard to safety and
sustainability of services. Performance against the Welsh Government dashboard of indicators is reported and reviewed on a regular basis.
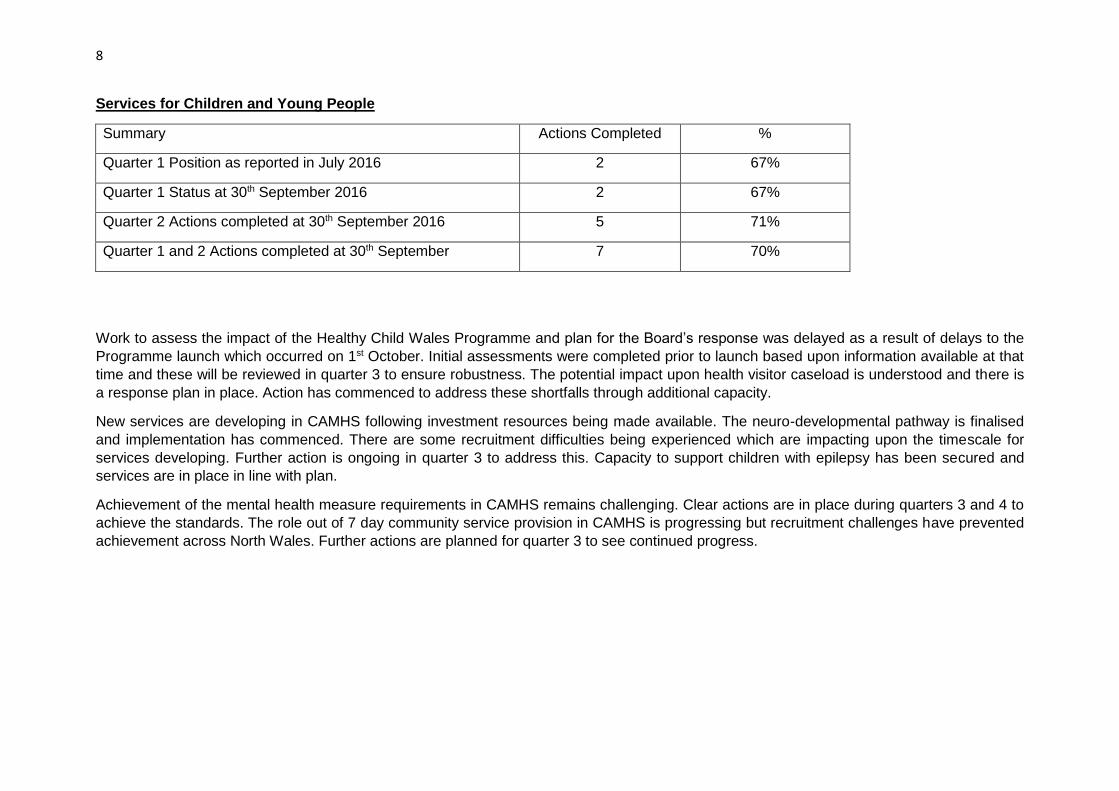
8
Services for Children and Young People
Summary Actions Completed %
Quarter 1 Position as reported in July 2016 2 67%
Quarter 1 Status at 30th September 2016 2 67%
Quarter 2 Actions completed at 30th September 2016 5 71%
Quarter 1 and 2 Actions completed at 30th September 7 70%
Work to assess the impact of the Healthy Child Wales Programme and plan for the Board’s response was delayed as a result of delays to the
Programme launch which occurred on 1st October. Initial assessments were completed prior to launch based upon information available at that
time and these will be reviewed in quarter 3 to ensure robustness. The potential impact upon health visitor caseload is understood and there is
a response plan in place. Action has commenced to address these shortfalls through additional capacity.
New services are developing in CAMHS following investment resources being made available. The neuro-developmental pathway is finalised
and implementation has commenced. There are some recruitment difficulties being experienced which are impacting upon the timescale for
services developing. Further action is ongoing in quarter 3 to address this. Capacity to support children with epilepsy has been secured and
services are in place in line with plan.
Achievement of the mental health measure requirements in CAMHS remains challenging. Clear actions are in place during quarters 3 and 4 to
achieve the standards. The role out of 7 day community service provision in CAMHS is progressing but recruitment challenges have prevented
achievement across North Wales. Further actions are planned for quarter 3 to see continued progress.

9
Quality and Safety
Summary Actions Completed %
Quarter 1 Position as reported in July 2016 6 85%
Quarter 1 Status at 30th September 2016 6 85%
Quarter 2 Actions completed at 30th September 2016 0 0%
Quarter 1 and 2 Actions completed at 30th September 6 55%
The VTE audit planned for September has not taken place. This will now take place in quarter 3. Whilst there has been some progress in
relation to Falls this is limited and further action is required in quarter 3 to recover (see also Health Improvement section).
The implementation of a revised system of mortality reviews has been delayed and is now expected to deliver in quarter 4. In the mean time
consistent systems for mortality reviews at stage 1 and stage 2 are now in place across the Health Board.
There is a clear plan in place to address infection prevention and control, however progress in reducing the rates of C Diff and MRSA at the
level envisaged in the Plan is not evident. YGC and YMW are areas of concern as a result of increased incidence and there is a clear plan of
action ongoing in quarter 3 to secure improvement.
The World Health organisation Safer Procedures Checklist has been implemented in radiology and other clinical areas are developing such as
anaesthetics in YG. There will be further rollout of this approach during quarter 3.
Engagement
Summary Actions Completed %
Quarter 1 Position as reported in July 2016 4 67%
Quarter 1 Status at 30th September 2016 6 100%
Quarter 2 Actions completed at 30th September 2016 5 100%
Quarter 1 and 2 Actions completed at 30th September 11 100%

10
Positive progress is reported against each of the key actions set out in the Plan. A new engagement strategy has been adopted and
engagement activities within the 3 Areas are established as expected. Activities through social media are increasing and the “get involved”
website is operating effectively. The strategy development work also has its own web presence, linked to “get involved”.
The perception survey for the north wales population which was planned has now been replaced by the Welsh Government’s engagement
exercise. The feedback from this will be utilised to develop the Board’s plans going forward.
Work is ongoing with the Consultation Institute to pilot an approach to assessing the effectiveness of the Board’s engagement activities.
Strategic and Service Planning
Summary Actions Completed %
Quarter 1 Position as reported in July 2016 8 67%
Quarter 1 Status at 30th September 2016 10 83%
Quarter 2 Actions completed at 30th September 2016 3 33%
Quarter 1 and 2 Actions completed at 30th September 13 62%
The Board’s management of concerns and incidents is covered in this section of the Plan due to the Special Measures Framework. Progress in
eradicating concerns where responses are provided in a timeframe over 6 months is progressing. Likewise 30 day response performance is
improving, however the pace of improvement is a cause for concern. Further escalation of actions in quarter 3 are planned to improve
performance. Whilst there has been improvement in the approach to learning lessons through, for example, learning lessons workshops and
strategic learning groups for falls and pressure ulcers, inconsistencies remain and progress is not as rapid as is required.
Work to develop the Board’s overall strategy is ongoing, following the Board’s agreement to the approach and timescale in July. This timescale,
which aligns with the Welsh Government’s listening exercise amended some of the timescales envisaged in the Board’s Plan for 2017/18.
Workstreams impacted by this change will now progress in quarter 3 and quarter 4.
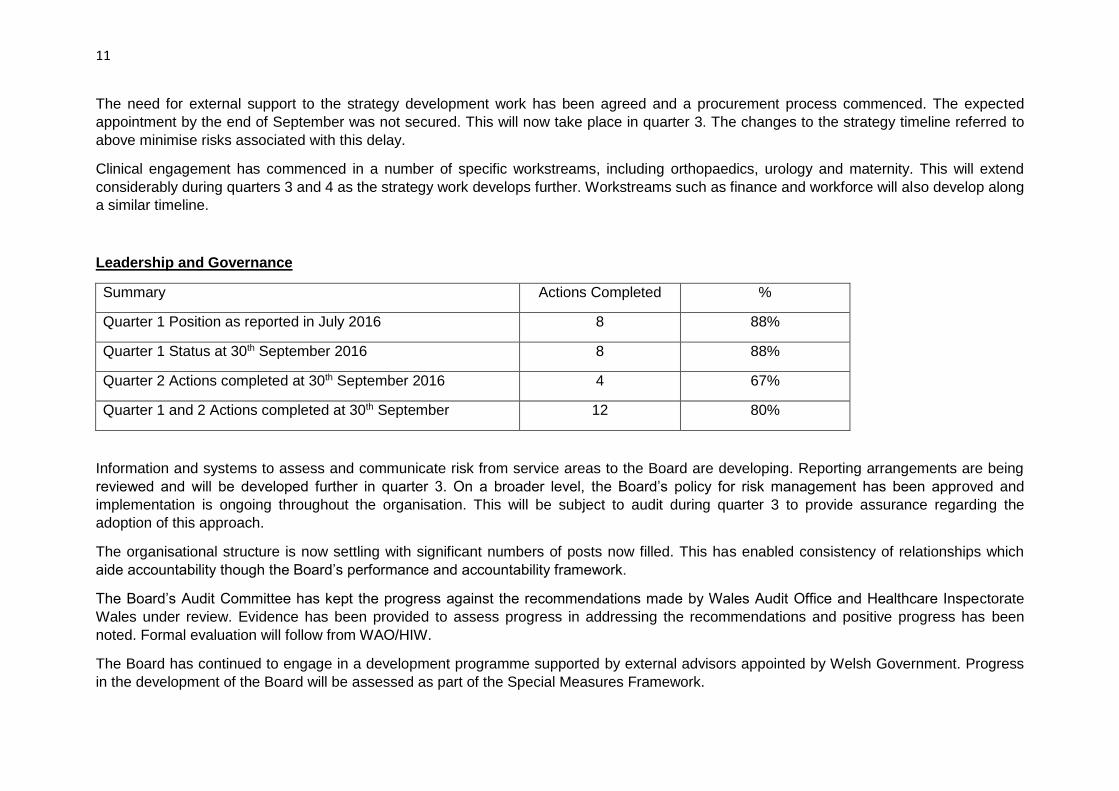
11
The need for external support to the strategy development work has been agreed and a procurement process commenced. The expected
appointment by the end of September was not secured. This will now take place in quarter 3. The changes to the strategy timeline referred to
above minimise risks associated with this delay.
Clinical engagement has commenced in a number of specific workstreams, including orthopaedics, urology and maternity. This will extend
considerably during quarters 3 and 4 as the strategy work develops further. Workstreams such as finance and workforce will also develop along
a similar timeline.
Leadership and Governance
Summary Actions Completed %
Quarter 1 Position as reported in July 2016 8 88%
Quarter 1 Status at 30th September 2016 8 88%
Quarter 2 Actions completed at 30th September 2016 4 67%
Quarter 1 and 2 Actions completed at 30th September 12 80%
Information and systems to assess and communicate risk from service areas to the Board are developing. Reporting arrangements are being
reviewed and will be developed further in quarter 3. On a broader level, the Board’s policy for risk management has been approved and
implementation is ongoing throughout the organisation. This will be subject to audit during quarter 3 to provide assurance regarding the
adoption of this approach.
The organisational structure is now settling with significant numbers of posts now filled. This has enabled consistency of relationships which
aide accountability though the Board’s performance and accountability framework.
The Board’s Audit Committee has kept the progress against the recommendations made by Wales Audit Office and Healthcare Inspectorate
Wales under review. Evidence has been provided to assess progress in addressing the recommendations and positive progress has been
noted. Formal evaluation will follow from WAO/HIW.
The Board has continued to engage in a development programme supported by external advisors appointed by Welsh Government. Progress
in the development of the Board will be assessed as part of the Special Measures Framework.
12
Conclusion
This report summarises progress against the key deliverables agreed by the Board in May 2016. There is clear evidence of progress in a
number of areas with 75% of actions completed at the end of September. There are however a number of milestones which have not been met
on time. Focussed action is required to ensure that slippage against these milestones is recovered during quarter 3 with a specific focus upon
quality and safety and planned care milestones.
Recommendation
That the Committee note the content of the report and consider the progress made at end of quarter 2.
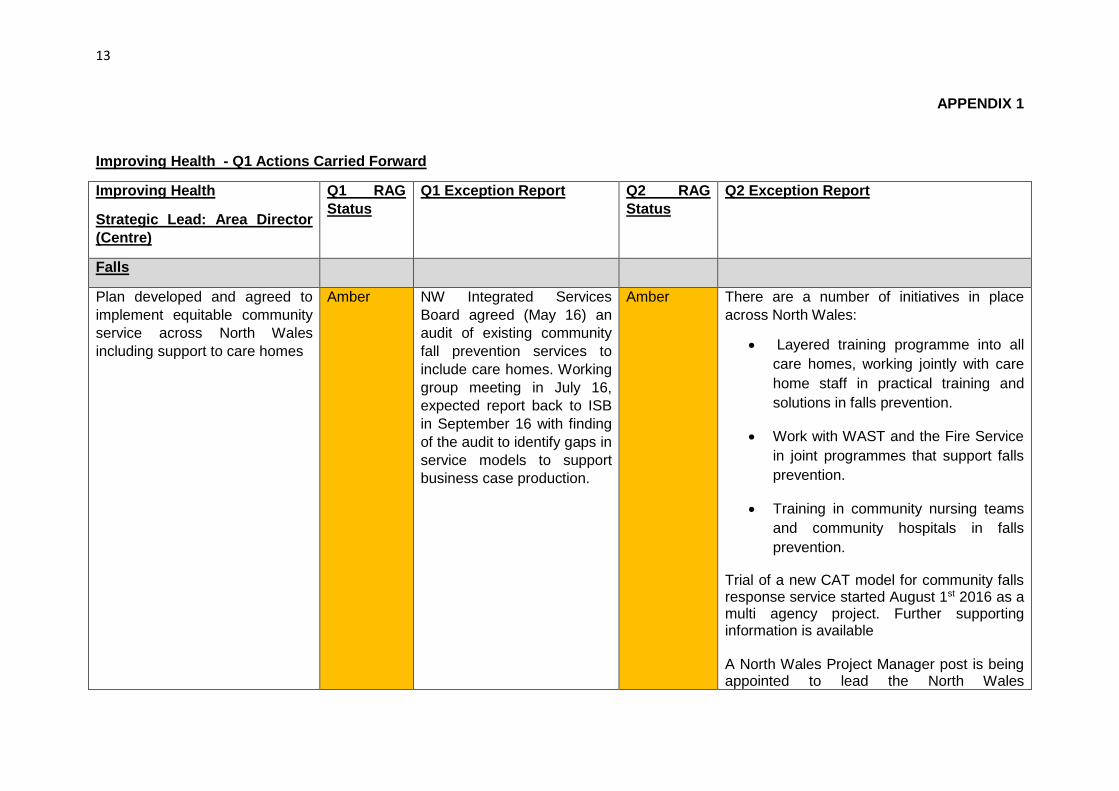
13
APPENDIX 1
Improving Health - Q1 Actions Carried Forward
Improving Health
Strategic Lead: Area Director
(Centre)
Q1 RAG
Status
Q1 Exception Report Q2 RAG
Status
Q2 Exception Report
Falls
Plan developed and agreed to
implement equitable community
service across North Wales
including support to care homes
Amber NW Integrated Services
Board agreed (May 16) an
audit of existing community
fall prevention services to
include care homes. Working
group meeting in July 16,
expected report back to ISB
in September 16 with finding
of the audit to identify gaps in
service models to support
business case production.
Amber There are a number of initiatives in place
across North Wales:
Layered training programme into all
care homes, working jointly with care
home staff in practical training and
solutions in falls prevention.
Work with WAST and the Fire Service
in joint programmes that support falls
prevention.
Training in community nursing teams
and community hospitals in falls
prevention.
Trial of a new CAT model for community falls response service started August 1st 2016 as a multi agency project. Further supporting information is available A North Wales Project Manager post is being appointed to lead the North Wales

14
programme from December 2016. An audit is planned for Nov-Dec in order to inform discussions on community fall prevention services for ICF and other funding streams for 17/18.
Smoking Cessation
Plan developed for Pharmacies
integrated onto Quit Manager
Amber Plans are being progressed
to ensure pharmacies are
integrated into quit manager.
Green A plan has been developed and agreed with
PHW to pilot the integration of Community
Pharmacy NECAF information onto Quit
Manager database with the pharmacists in
Rhyl. Information governance requirements
are being finalised to go live early November.
This pilot will run until the end of March and
will inform next steps for the whole of North
Wales and Wales.
Population variation mapped to
target commissioning
Amber Population data being
mapped and planning
meetings arranged to
progress and target further
commissioning and roll out.
Green Achieved. Area cluster profiles developed by
PHW detailing current activity and additional
activity required to meet referral targets.
Cluster plans have been written based on
needs assessment.
Cluster plans now have smoking cessation
included. Area teams are working with PHW
to understand the cluster profile data and how
it can be used to meet referral targets.
Public Health Wales Smoking Cessation
report for QTR 1 just published This will be
used to develop plans and target actions and
improve services where outcomes are
stronger. We are exploring the development

15
of a community mapping and analysis system
to demonstrate service provision compared to
deprivation and spend. This work also has the
potential to support Social Return on
Investment initiatives
Proposals developed for
secondary care smoking
cessation service for patients
and staff
Amber Outline proposal developed
with detailed implementation
plan being progressed for q2
Green Achieved. Outline proposal developed for
secondary care smoking cessation service
Smoking lead nurse to be identified; Focus
will be on rehab patients and to deliver a
smoking cessation service by mental health
staff
Evidence of partner agencies
supported to promote cessation
for their staff
Amber Smoking cessation priority is
included within LA corporate
wellbeing plans and we
continue to work with
partners to monitor impacts.
Green Achieved. Evidence of engagement and
support through for example, Well North
Wales programme, Big Lottery proposal.
Target 1,450 smokers / quarter
starting treatment and 276
pregnant smokers / quarter
receiving first consultation.
N/A Data available from q2 Amber Achieved in Central and plans to improve
performance in q3 onwards in East and West
have been developed.
Immunisations
Cluster plans established for Flu
campaign
Amber Immunisation operational
group is established and Flu
action plan for the clusters is
being developed in q2.
Green Achieved. All Area cluster plans incorporate
flu campaign actions. Further detailed
evidence is available.
Brief Intervention Training
MECC framework implemented Amber Awareness of MECC is
improving and will be further
Amber Area teams working with cluster leads and
develop MECC within wider partnership plans

16
developed and pursued
through the Prevention and
Health Improvement
Programme within Areas.
to embed this. Expected to deliver in Q3.
Staff for training in MECC
identified
Amber Staff groups have attended
the training (health visitors
and school nurses). Further
work in q2 to identify further
staff groups to be prioritised
for training.
Green Achieved. Staff for training in MECC have
been identified and progressing for example,
training sessions for staff across clusters and
work is being piloted with cluster leads to
embed the programme into plans.
Staff for additional training
(smoking / alcohol) identified
Amber Health Visitors and School
Nurses have received
training which will be rolled
out further in q2.
Green Achieved. Staff for additional training
(smoking / alcohol) have been identified
Obesity – Adults
Approach to Lifestyle
Management and level 2
programme agreed
Amber EMG agreed business case
and agreement to develop
level 2 service in a
partnership model which will
be further developed in q2.
Green Achieved. Approach to Lifestyle Management
and level 2 programme agreed
Funding has been agreed through EMG.
East Area to lead. This work is in early stages
of development to be delivered in Qtr 3
Obesity – Children
Develop action plans working
with partners
Amber Early discussions have been
held with partners to roll out
examples of good practice –
Cook and Eat, Healthy
School Menus, Ante Natal
Breast Feeding initiatives
Green Achieved. Action plans developed with
partners and examples of partnership working
are available
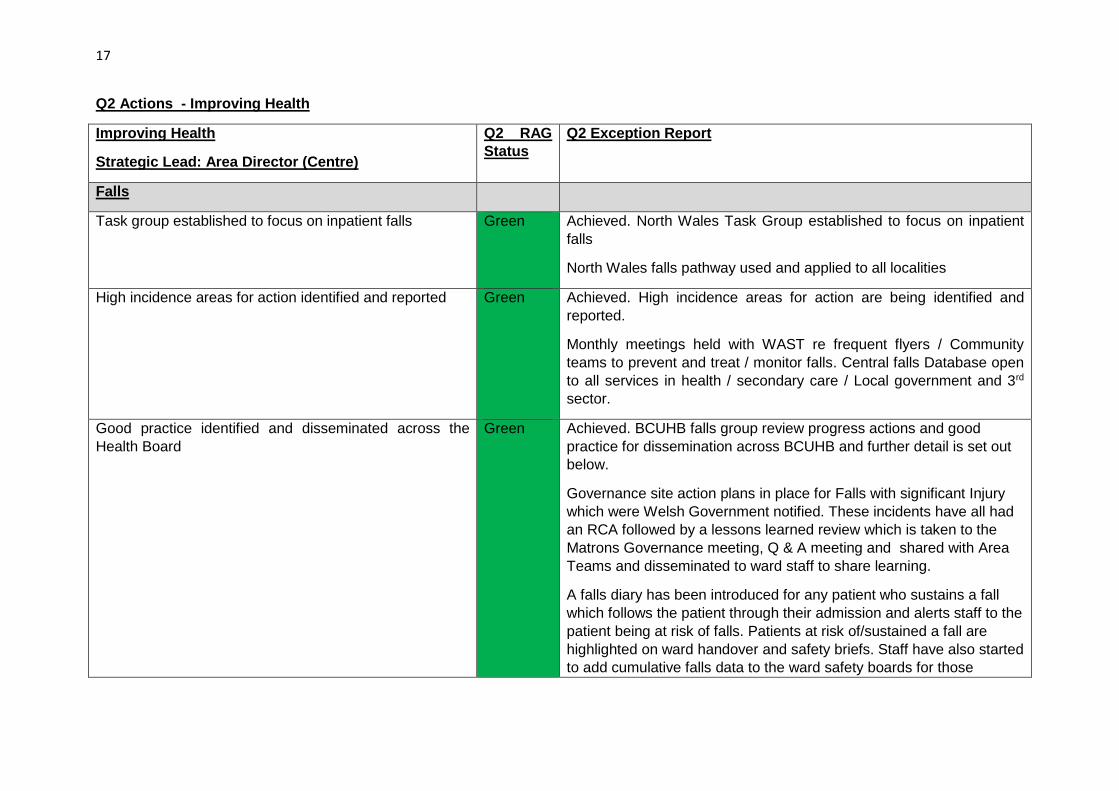
17
Q2 Actions - Improving Health
Improving Health
Strategic Lead: Area Director (Centre)
Q2 RAG
Status
Q2 Exception Report
Falls
Task group established to focus on inpatient falls
Green Achieved. North Wales Task Group established to focus on inpatient
falls
North Wales falls pathway used and applied to all localities
High incidence areas for action identified and reported
Green Achieved. High incidence areas for action are being identified and
reported.
Monthly meetings held with WAST re frequent flyers / Community
teams to prevent and treat / monitor falls. Central falls Database open
to all services in health / secondary care / Local government and 3rd
sector.
Good practice identified and disseminated across the
Health Board
Green Achieved. BCUHB falls group review progress actions and good
practice for dissemination across BCUHB and further detail is set out
below.
Governance site action plans in place for Falls with significant Injury
which were Welsh Government notified. These incidents have all had
an RCA followed by a lessons learned review which is taken to the
Matrons Governance meeting, Q & A meeting and shared with Area
Teams and disseminated to ward staff to share learning.
A falls diary has been introduced for any patient who sustains a fall
which follows the patient through their admission and alerts staff to the
patient being at risk of falls. Patients at risk of/sustained a fall are
highlighted on ward handover and safety briefs. Staff have also started
to add cumulative falls data to the ward safety boards for those

18
patients with reoccurring falls to prompt staff to upgrade supervision.
Falls stickers are being trialled to go in the patients notes to prompt
medical teams.
New falls pathway developed by the strategic falls group
The Governance team provide monthly data which is also shared at
the Matrons Governance meeting, Q & A meeting and Consultants
meeting to review in patients falls with significant injury.
Well North Wales
Stakeholders fully engaged and target outcome areas clearly defined
Green Achieved. Stakeholders identified and engaged in Well North Wales.
Programme Director in place from August 2016.
Governance arrangements established and approved
Amber Partially achieved. Formal Board established, with paper to EMG
expected in November 2016 to ratify arrangements. Governance
arrangements also to be discussed with Public Services Boards
Chairs.
3 pilot communities identified
Green Achieved. 3 Areas identified as : Upper Denbigh, Penycae and
Llangefni, as part of the Ein Dyfodol aspect of the programme, with
initiatives also being identified in other communities.
Monitoring and evaluation framework agreed
Amber Partially achieved. Discussions commenced with Well London, re
Long Term evaluation project and discussions with Bangor University
re local evaluation proposals. Discussions also scheduled with Social
Value Cymru to determine possibilities around Social return on
Investment opportunities.
Smoking Cessation
Practice’s identified for participation in Integrated
Community Smoking cessation projects
Green Achieved. Practice’s have been identified for participation in Integrated
Community Smoking cessation projects. Further detail set out below.
Public Health Wales have met with locality leads to review their Local

19
Enhanced Service for Smoking. The goal is to develop a new service
which will reward GP practices for improved quit rates and ensure that
wherever patients preference for treatment is, it will meet the Russell
Standards.
GP practices and community pharmacies in Holyhead, Rhyl and
Wrexham received MECC training for staff. West: Holyhead, Anglesey
participating awaiting evaluation report. Centre: GP practices and
community pharmacies in Rhyl received MECC training for staff. Pilot
undertaken at Clarence House, Rhyl.
Social marketing activity enhanced
Green PHW are now running the ‘Quit for Them’ campaign in-house. They
have an identified budget for the social media marketing until the end
of March, with Facebook and other media platforms utilised to target
those areas with highest prevalence rates. The website and the quit
kits offered will be refreshed with additional content will be placed on
the website. A communication strategy will also be developed to take
this work forward. In addition, a bid was submitted to the cluster
fund/primary care monies to enhance this campaign.
Transition to Quit Manager supported
Green Achieved. Transition to Quit Manager supported. Rhyl community
pharmacies trialling Quit Manager from 1st October 2016. Rollout
planned to all North Wales pharmacies by March 2017 if successful
Staff identified to deliver secondary care service Green Staff have been identified to deliver a secondary care service, and
trained in brief interventions. The Secondary Care Nurse Director,
and site Assistant Directors of Nursing lead on this across Secondary
Care, with out-patient clinics being a major interface with patients.
Actions are well embedded across acute sites and include:
Nicotine replacement therapy is available in all clinical areas
On discharge a referral is sent to the GP to confirm that the patient has commenced NRT for follow up
Discharge packs have details of helpline included

20
Maternal smoking cessation implemented in early sites
(Women’s Division has been given funding to appoint 6
WTE Health Care Support Workers to deliver a bespoke
Smoking Cessation Service for pregnant women
following BCUHB’s success of this model in the MAMMS
project. The 6 WTE smoking cessation workers will work
across all localities of BCUHB and be focused in the
areas of greatest deprivation. They will form part of the
community midwifery teams taking referrals directly from
community midwives and have close links with the Stop
Smoking Wales Service.)
Amber Partially achieved; good initial progress made. with actions being
taken to recover progress in respect to expediting recruitment.
Currently all Community midwives have been trained in brief
intervention for smoking cessation and all have access to carbon
monoxide monitoring equipment. As part of their contact with women
during pregnancy the community midwives refer to stop smoking
Wales services and regularly liaise with a Public Health Worker for
additional support. Upon recruitment of the Health Care Support
Workers they will focus on increasing referrals to ultimately help
women to stop smoking.
Maternal mental health service is established. This model was
extremely efficient in the MAMMS project and achieved the best quit
rates.
Budget agreed & lead identified and implementation plans being
developed. Job Descriptions have been finalised for job banding and
recruitment.
Models identified to support people with mental health
needs to quit smoking
Amber Partially achieved. Model in development to support people with
mental health needs to quit smoking
Health Care Support Workers who will be employed as smoking
cessation workers will be allocated by the Community Team Leaders
to provide focus to support women with identified mental health needs
in their effort to stop smoking. This will start at the end of Q3
dependent on recruitment.
One of 3 recently appointed lead nurses will be smoking lead. Aim will
be to train staff to deliver specialist stop smoking service in rehab and
longer stay wards and working closely with 3rd sector organisations.
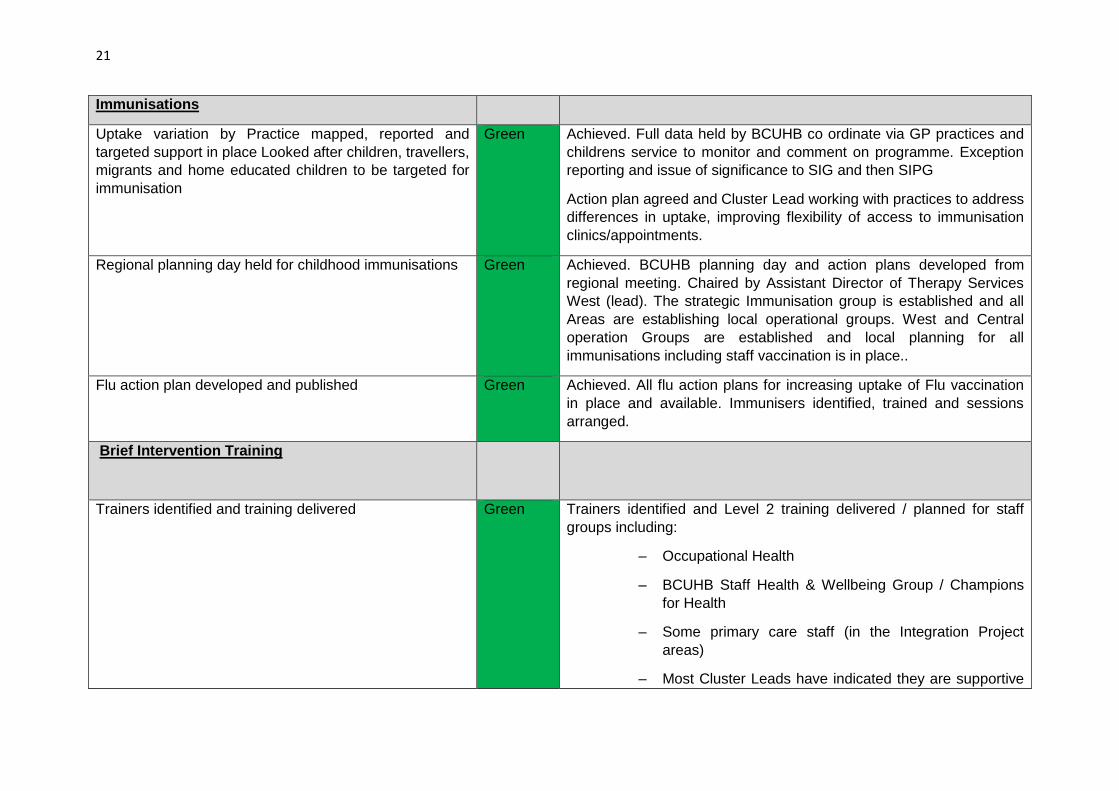
21
Immunisations
Uptake variation by Practice mapped, reported and
targeted support in place Looked after children, travellers,
migrants and home educated children to be targeted for
immunisation
Green Achieved. Full data held by BCUHB co ordinate via GP practices and
childrens service to monitor and comment on programme. Exception
reporting and issue of significance to SIG and then SIPG
Action plan agreed and Cluster Lead working with practices to address
differences in uptake, improving flexibility of access to immunisation
clinics/appointments.
Regional planning day held for childhood immunisations
Green Achieved. BCUHB planning day and action plans developed from
regional meeting. Chaired by Assistant Director of Therapy Services
West (lead). The strategic Immunisation group is established and all
Areas are establishing local operational groups. West and Central
operation Groups are established and local planning for all
immunisations including staff vaccination is in place..
Flu action plan developed and published Green Achieved. All flu action plans for increasing uptake of Flu vaccination
in place and available. Immunisers identified, trained and sessions
arranged.
Brief Intervention Training
Trainers identified and training delivered Green Trainers identified and Level 2 training delivered / planned for staff
groups including:
– Occupational Health
– BCUHB Staff Health & Wellbeing Group / Champions
for Health
– Some primary care staff (in the Integration Project
areas)
– Most Cluster Leads have indicated they are supportive
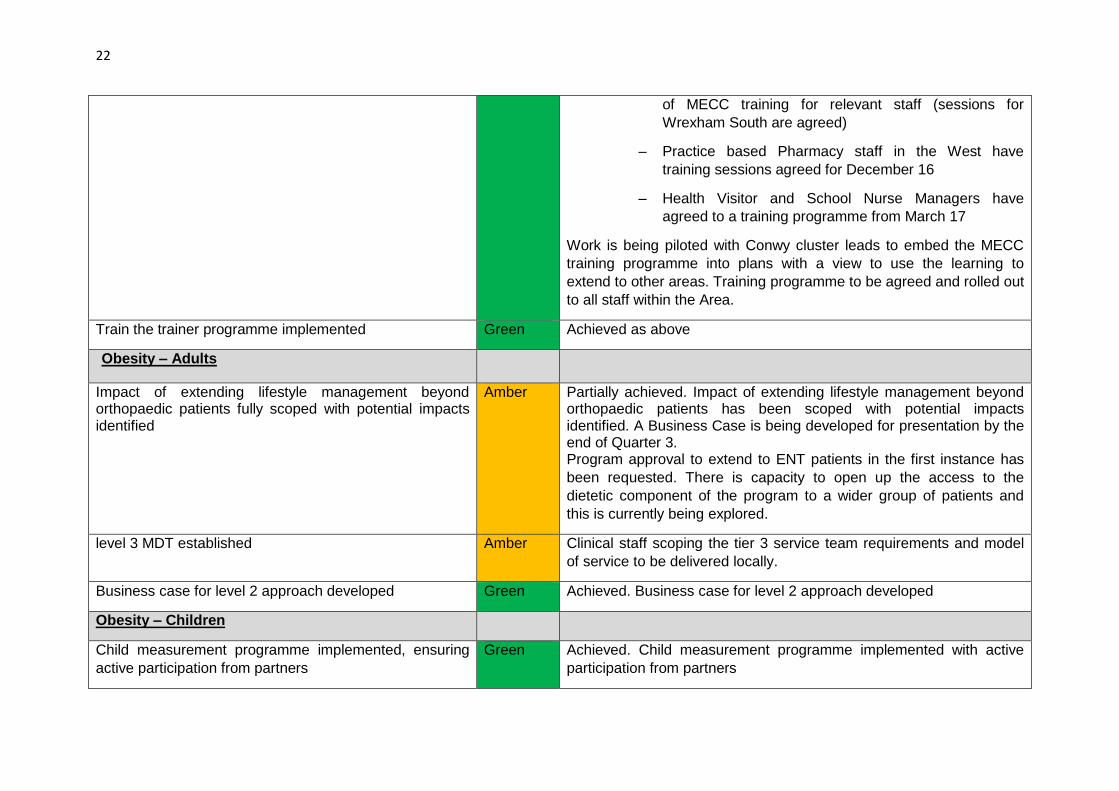
22
of MECC training for relevant staff (sessions for
Wrexham South are agreed)
– Practice based Pharmacy staff in the West have
training sessions agreed for December 16
– Health Visitor and School Nurse Managers have
agreed to a training programme from March 17
Work is being piloted with Conwy cluster leads to embed the MECC
training programme into plans with a view to use the learning to
extend to other areas. Training programme to be agreed and rolled out
to all staff within the Area.
Train the trainer programme implemented Green Achieved as above
Obesity – Adults
Impact of extending lifestyle management beyond orthopaedic patients fully scoped with potential impacts identified
Amber Partially achieved. Impact of extending lifestyle management beyond orthopaedic patients has been scoped with potential impacts identified. A Business Case is being developed for presentation by the end of Quarter 3. Program approval to extend to ENT patients in the first instance has
been requested. There is capacity to open up the access to the
dietetic component of the program to a wider group of patients and
this is currently being explored.
level 3 MDT established
Amber Clinical staff scoping the tier 3 service team requirements and model
of service to be delivered locally.
Business case for level 2 approach developed Green Achieved. Business case for level 2 approach developed
Obesity – Children
Child measurement programme implemented, ensuring
active participation from partners
Green Achieved. Child measurement programme implemented with active
participation from partners
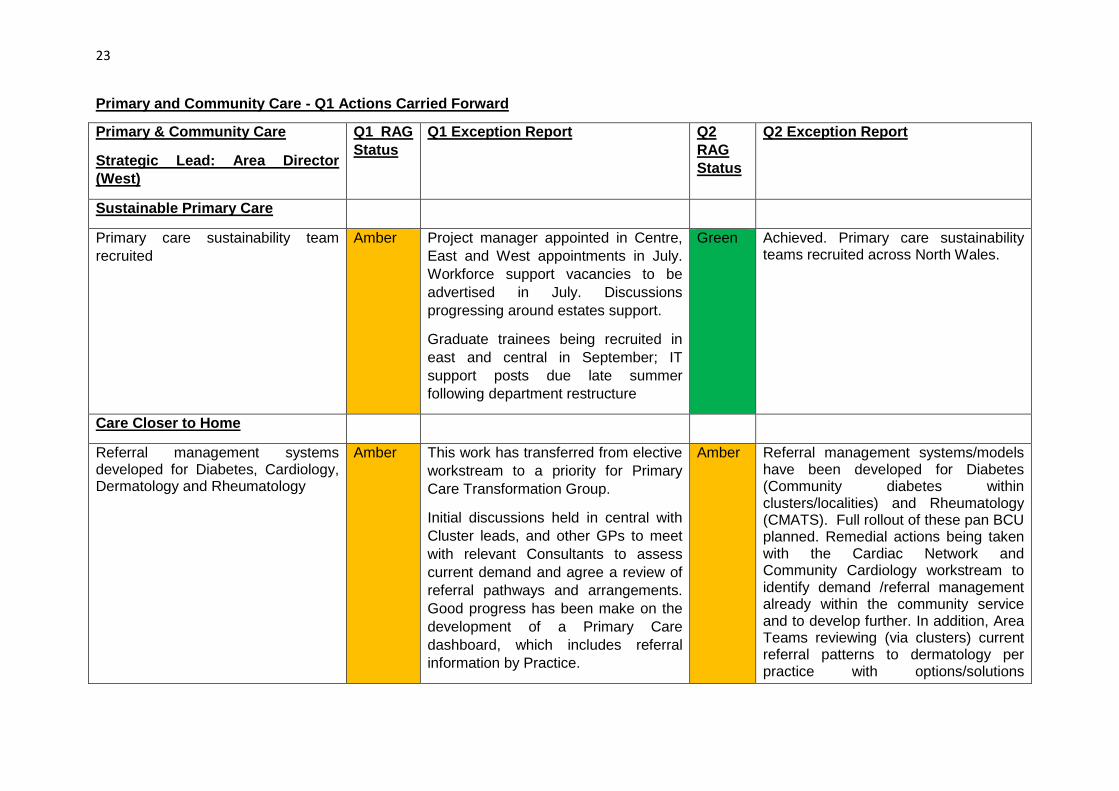
23
Primary and Community Care - Q1 Actions Carried Forward
Primary & Community Care
Strategic Lead: Area Director
(West)
Q1 RAG
Status
Q1 Exception Report Q2
RAG
Status
Q2 Exception Report
Sustainable Primary Care
Primary care sustainability team
recruited
Amber Project manager appointed in Centre,
East and West appointments in July.
Workforce support vacancies to be
advertised in July. Discussions
progressing around estates support.
Graduate trainees being recruited in
east and central in September; IT
support posts due late summer
following department restructure
Green Achieved. Primary care sustainability teams recruited across North Wales.
Care Closer to Home
Referral management systems developed for Diabetes, Cardiology, Dermatology and Rheumatology
Amber This work has transferred from elective
workstream to a priority for Primary
Care Transformation Group.
Initial discussions held in central with
Cluster leads, and other GPs to meet
with relevant Consultants to assess
current demand and agree a review of
referral pathways and arrangements.
Good progress has been make on the
development of a Primary Care
dashboard, which includes referral
information by Practice.
Amber Referral management systems/models have been developed for Diabetes (Community diabetes within clusters/localities) and Rheumatology (CMATS). Full rollout of these pan BCU planned. Remedial actions being taken with the Cardiac Network and Community Cardiology workstream to identify demand /referral management already within the community service and to develop further. In addition, Area Teams reviewing (via clusters) current referral patterns to dermatology per practice with options/solutions

24
Work streams established to progress
e.g. Triage of Dermatology - tele-
dermatology model established across
2 cluster areas to inform future referral
guidelines for GPs. Consideration to be
given to benefits of rolling this out
further Full roll out of cameras for
photo triage to all practices will also
help reduce demand for USC and
learning from this also to inform future
referral guidelines.
Review of current CMATS triage
system to improve rheumatology
referral management (referrals in West
and Centre are already managed via
the CMAT service). Work to progress
inclusion of Rheumatology referrals in
the East to be undertaken in Q2.
Discussions with GPs held regarding
referrals for diabetes and how
pathways could be changed, these will
be developed further in Q2.
Diabetes – workstream to link into
rollout of community models funded via
primary care.
generated thereafter.
Admission avoidance pathways
developed
Amber Pathways developed for Blocked
Catheter, Palliative care treat
escalation plans, falls and Community
IV therapy which is being made
available in community hospitals within
Green Achieved. Admission avoidance pathways developed as follows: Blocked Catheter – pathway fully implemented
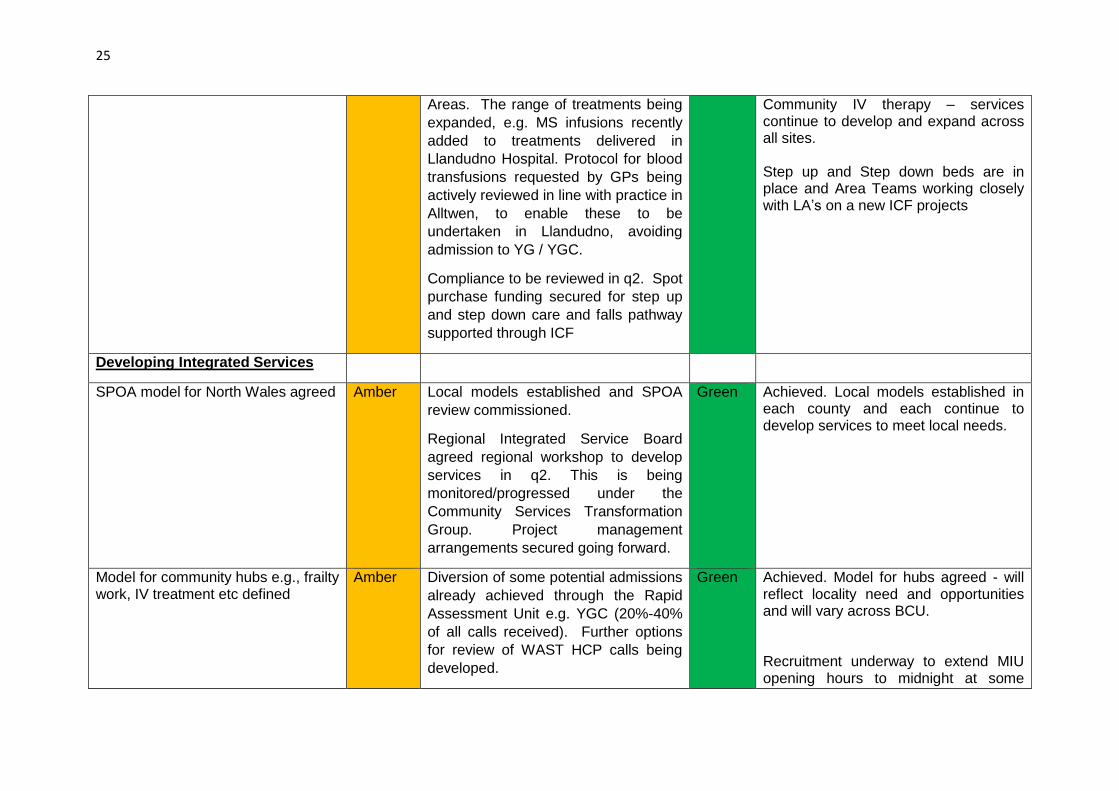
25
Areas. The range of treatments being
expanded, e.g. MS infusions recently
added to treatments delivered in
Llandudno Hospital. Protocol for blood
transfusions requested by GPs being
actively reviewed in line with practice in
Alltwen, to enable these to be
undertaken in Llandudno, avoiding
admission to YG / YGC.
Compliance to be reviewed in q2. Spot
purchase funding secured for step up
and step down care and falls pathway
supported through ICF
Community IV therapy – services continue to develop and expand across all sites. Step up and Step down beds are in place and Area Teams working closely with LA’s on a new ICF projects
Developing Integrated Services
SPOA model for North Wales agreed Amber Local models established and SPOA
review commissioned.
Regional Integrated Service Board
agreed regional workshop to develop
services in q2. This is being
monitored/progressed under the
Community Services Transformation
Group. Project management
arrangements secured going forward.
Green Achieved. Local models established in each county and each continue to develop services to meet local needs.
Model for community hubs e.g., frailty work, IV treatment etc defined
Amber Diversion of some potential admissions
already achieved through the Rapid
Assessment Unit e.g. YGC (20%-40%
of all calls received). Further options
for review of WAST HCP calls being
developed.
Green Achieved. Model for hubs agreed - will reflect locality need and opportunities and will vary across BCU. Recruitment underway to extend MIU opening hours to midnight at some
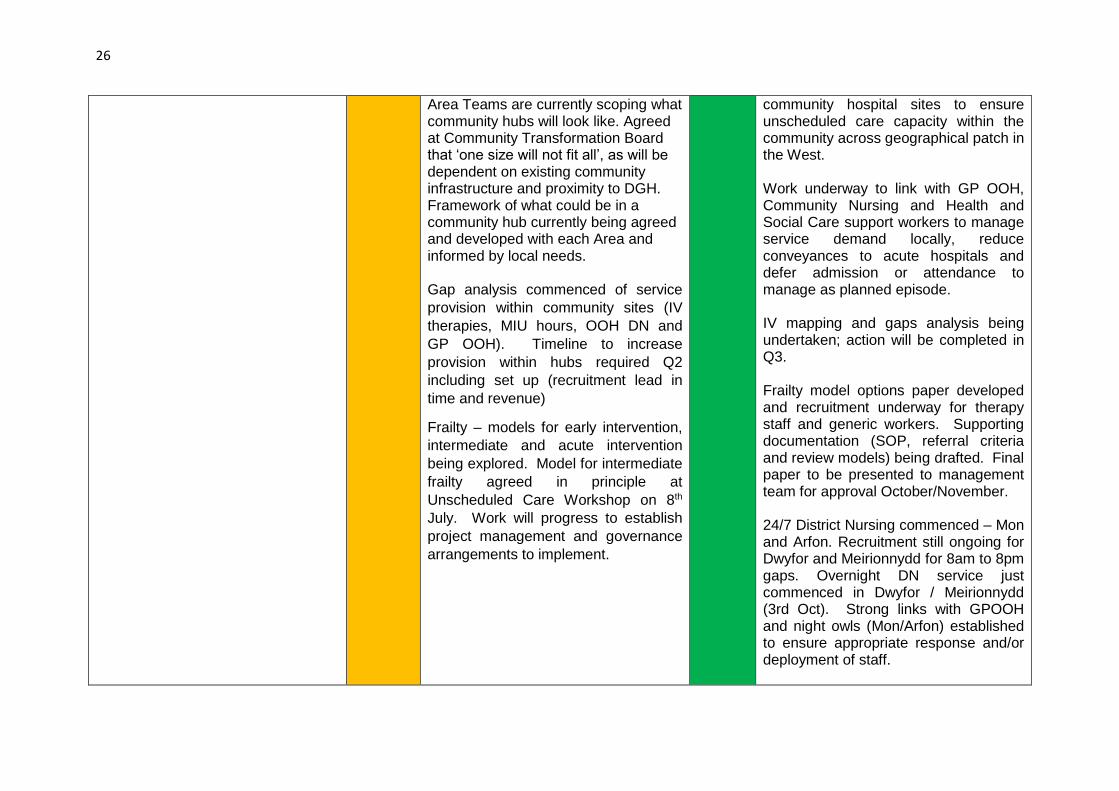
26
Area Teams are currently scoping what community hubs will look like. Agreed at Community Transformation Board that ‘one size will not fit all’, as will be dependent on existing community infrastructure and proximity to DGH. Framework of what could be in a community hub currently being agreed and developed with each Area and informed by local needs. Gap analysis commenced of service
provision within community sites (IV
therapies, MIU hours, OOH DN and
GP OOH). Timeline to increase
provision within hubs required Q2
including set up (recruitment lead in
time and revenue)
Frailty – models for early intervention,
intermediate and acute intervention
being explored. Model for intermediate
frailty agreed in principle at
Unscheduled Care Workshop on 8th
July. Work will progress to establish
project management and governance
arrangements to implement.
community hospital sites to ensure unscheduled care capacity within the community across geographical patch in the West. Work underway to link with GP OOH, Community Nursing and Health and Social Care support workers to manage service demand locally, reduce conveyances to acute hospitals and defer admission or attendance to manage as planned episode. IV mapping and gaps analysis being undertaken; action will be completed in Q3. Frailty model options paper developed and recruitment underway for therapy staff and generic workers. Supporting documentation (SOP, referral criteria and review models) being drafted. Final paper to be presented to management team for approval October/November. 24/7 District Nursing commenced – Mon and Arfon. Recruitment still ongoing for Dwyfor and Meirionnydd for 8am to 8pm gaps. Overnight DN service just commenced in Dwyfor / Meirionnydd (3rd Oct). Strong links with GPOOH and night owls (Mon/Arfon) established to ensure appropriate response and/or deployment of staff.

27
Frailty model in West will have referral/access criteria for the unit. It will be COTE led with MDT input working with a patient centered systems approach. The unit will manage unscheduled care admissions with a predicted LOS of 72 hours or less and will operate 24/7. With appropriate staffing levels will also manage pre-crisis referrals via GPs (reducing demand for OPD). Centre: Identified frailty model, and agreed location in Llandudno. Identified financial support through seasonal plan. Project has been established. Facilitated multi-agency Workshop took place at Parc Eirias community hub, on 14th September. Work commenced on analysing feedback. Healthy Prestatyn Iach went live on 1st April 2016. Feedback from patients has been positive so far. IV suites have been established in Llandudno & Denbigh hospitals.
Dental Services
CDS provision review commenced Amber Lead Assistant Director identified to
provide leadership and management
across CDS and GDS services. As part
of this role a review of CDS will
Amber Partially achieved. Work has commenced on a CDS strategy which will guide the future service provision review.

28
commence in q2 CDS Strategy will be completed during October and submitted to North Wales Oral Health Strategy Group for review and approval. A paper regarding the establishment of a pan-BCU Dental Directorate for consultation is expected during Q3 and a new Dental Management Team will commence the review once in place.
Primary Care Estate
Project teams for Corwen and Conwy
/ Llandudno established
Amber
Initial meetings held with Corwen
Practice, CDS, LA and patient
participation group to revisit options
and determine solutions going forward.
New premises are a priority in
Conwy/Llandudno Junction and
solutions are being explored as part of
the primary care sustainability work.
Formal Project Teams have not been
established, but discussions have
commenced with key stakeholders,
including GP’s, Estates, Dental, Local
Authorities, Patients Representatives.
Project Teams will be established
during Qtr 2.
Green Achieved. The Project Board for Corwen Health Centre Development is established. Regular meetings are held with Patient Participation Group and GPs and Dental Services. The Business Case for the development of a federation of practices in Conwy/Llandudno Junction has been approved by the Board. Project arrangements are in place, with a Project Board and Project Team established.
Cluster Development
Priorities for transferring services to clusters agreed
Amber Work has commenced to identify
priorities for transferring to community
settings.
Amber Partially achieved. Cluster plans received by 30th September. Further analysis required during quarter 3 to identify priorities for progressing and

29
Further work is in place to use cluster
plans to inform transfer of services
(which will be identified by q2) and
transition plans developed thereafter.
inclusion in Operational plan 2017-18.
Q2 Actions Primary and Community Care
Primary and Community Care
Strategic Lead: Area Director (West)
Q2 RAG
Status
Q2 Exception Report
Sustainable Primary Care
Practice Nurse / Management development programme
developed
Green
Achieved - A Practice Nurse Development programme has been developed. Nurses training in primary care have been appointed and are supported in practices as supernumerary to ensure robust opportunities for mentoring. Partially Achieved - Practice Management Development Programme in progress. Managers’ meetings are established and some training opportunities have been identified internally and via the 1000 Lives programme. This will be coordinated and developed further. Clusters have prioritised training/learning and development for all primary care workforce from Cluster Funds. Navigation training has been arranged for frontline practice staff.
Amber
Task groups for key developments – e.g. Wylfa Newydd
established
Green Achieved - A programme board has been established to develop
the Health Board’s response to the Wylfa Newydd consultation,
launched on 28th August and closing on 25th October 2016. The
Board will continue to meet and develop the necessary
responses to the associated town and country applications and
Development Control Order (DCO) that will be submitted to
IoACC between October 2016 and February 2017.

30
Project Boards in place for the development of the full Business Case for the North Denbighshire Community Hospital, supported by a project manager with a project office established in the Royal Alexandra Hospital. The Project Board continues to meet to support the development of Healthy Prestatyn / Rhuddlan.
Primary care workforce plan published
Amber Workforce planning annual cycle developed and workforce baseline data collection captured. Lack of availability of comprehensive data remains a challenge. Baseline data collection will inform draft Plan including numbers
and sessions for GPs, dentists, pharmacists, opticians and
therapists as well as age profiles. This is being progressed in
line with the workforce planning annual cycle. The Head of
Strategy is working with HR to map workforce and reporting to
the Primary Care Transformation Group.
Direct access pathways and diagnostics established for
Radiology
Amber Partially achieved. Plans have been developed and are being
implemented to increase access to diagnostics by primary care
with more work required to roll out and spread best practice
across North Wales. See Planned Care section for further detail.
Transition plans in place for Wrexham managed practices Green Achieved - Two Wrexham practices became managed practices on the 1st of October. GPs and staff are in place with significant support provided by the Area.
Care closer to home
Care co-ordinator access established to MDT for diabetes
and heart failure
Green Achieved. Care co-ordinator access established to MDT for
diabetes and heart failure across all Areas.
Heart Failure
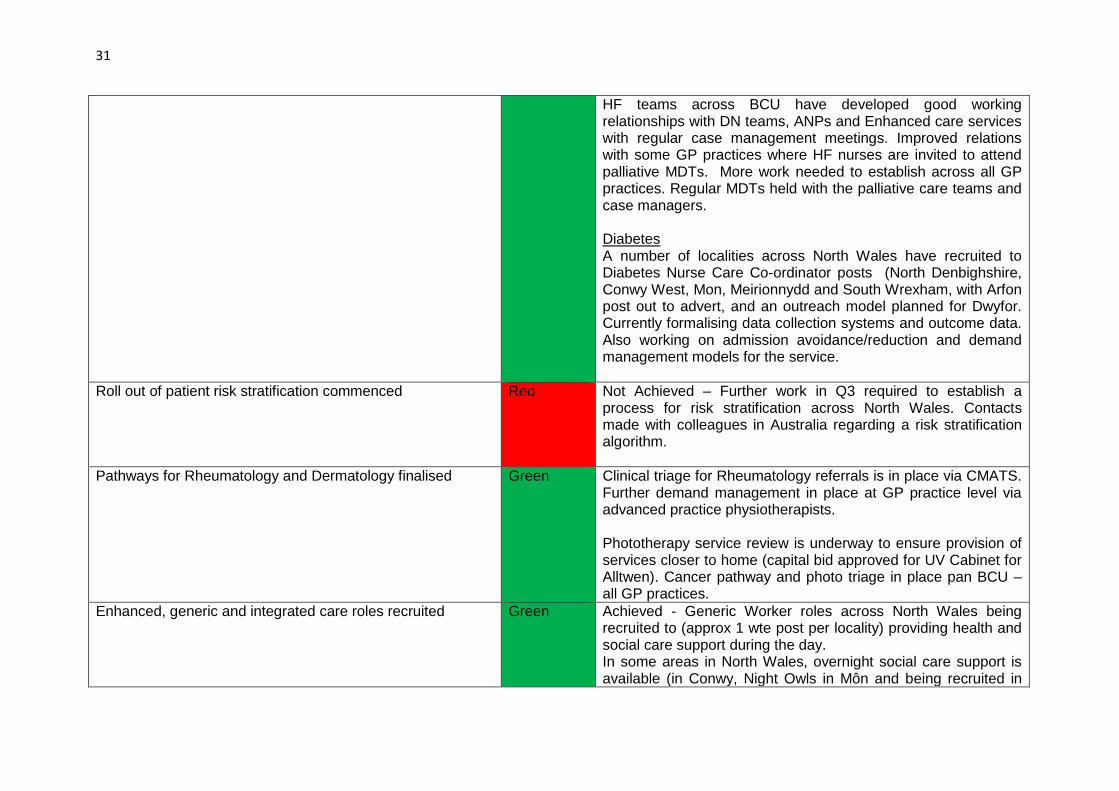
31
HF teams across BCU have developed good working relationships with DN teams, ANPs and Enhanced care services with regular case management meetings. Improved relations with some GP practices where HF nurses are invited to attend palliative MDTs. More work needed to establish across all GP practices. Regular MDTs held with the palliative care teams and case managers. Diabetes A number of localities across North Wales have recruited to Diabetes Nurse Care Co-ordinator posts (North Denbighshire, Conwy West, Mon, Meirionnydd and South Wrexham, with Arfon post out to advert, and an outreach model planned for Dwyfor. Currently formalising data collection systems and outcome data. Also working on admission avoidance/reduction and demand management models for the service.
Roll out of patient risk stratification commenced
Red Not Achieved – Further work in Q3 required to establish a process for risk stratification across North Wales. Contacts made with colleagues in Australia regarding a risk stratification algorithm.
Pathways for Rheumatology and Dermatology finalised
Green Clinical triage for Rheumatology referrals is in place via CMATS. Further demand management in place at GP practice level via advanced practice physiotherapists. Phototherapy service review is underway to ensure provision of services closer to home (capital bid approved for UV Cabinet for Alltwen). Cancer pathway and photo triage in place pan BCU – all GP practices.
Enhanced, generic and integrated care roles recruited Green Achieved - Generic Worker roles across North Wales being recruited to (approx 1 wte post per locality) providing health and social care support during the day. In some areas in North Wales, overnight social care support is available (in Conwy, Night Owls in Môn and being recruited in
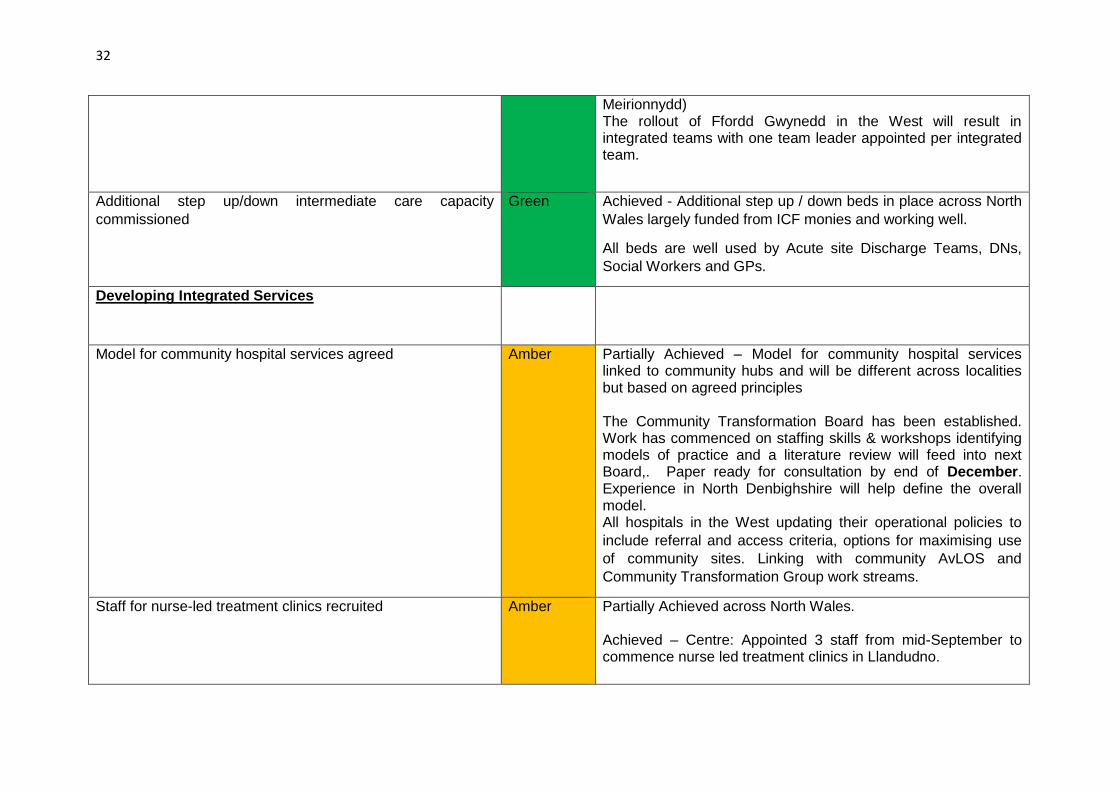
32
Meirionnydd) The rollout of Ffordd Gwynedd in the West will result in integrated teams with one team leader appointed per integrated team.
Additional step up/down intermediate care capacity
commissioned
Green Achieved - Additional step up / down beds in place across North
Wales largely funded from ICF monies and working well.
All beds are well used by Acute site Discharge Teams, DNs,
Social Workers and GPs.
Developing Integrated Services
Model for community hospital services agreed
Amber Partially Achieved – Model for community hospital services linked to community hubs and will be different across localities but based on agreed principles The Community Transformation Board has been established. Work has commenced on staffing skills & workshops identifying models of practice and a literature review will feed into next Board,. Paper ready for consultation by end of December. Experience in North Denbighshire will help define the overall model. All hospitals in the West updating their operational policies to
include referral and access criteria, options for maximising use
of community sites. Linking with community AvLOS and
Community Transformation Group work streams.
Staff for nurse-led treatment clinics recruited
Amber
Partially Achieved across North Wales. Achieved – Centre: Appointed 3 staff from mid-September to commence nurse led treatment clinics in Llandudno.

33
Partially Achieved - West: Recruitment in progress for Treatment clinics to be established at Ysbyty Penrhos Stanley in quarter 3.
Additional staff for OOH services recruited Green Achieved – Overnight District nursing in place in Arfon, Mon and Meirionnydd in the West. Still recruiting in Dwyfor and for small rota gaps in other areas. 24/7 District Nursing now based in out of hours.
Dental Services
GDS procurement process commenced Green Achieved - EMG has given approval for commissioning of non-recurring and recurring activity in year up to the limit of the Dental Ring-fence. Contracts began to be amended during August to reflect the non-recurring element and further amendments for both elements should be completed by the end of October. Mid-year reviews of all GDS contracts will enable an estimate of any further funds available during the 2016/17 financial year. Investment in permanent new chairs in the West, prioritising areas of low access has been agreed and the commissioning process will commence during Q3.
Contingency plan for in-year slippage agreed
Green Achieved as above
Priorities for CDS provision identified Amber Partially Achieved – Priorities will emerge from the work to develop a CDS Strategy which is being completed during October and submitted to North Wales Oral Health Strategy Group for review and approval. A paper is being developed regarding the establishment of a pan BCUHB Dental Directorate for consultation. This is expected during Q3 and a new Dental Management Team will commence the review once this is in place.

34
Primary Care Estate
Benllech PCC commissioned
Green Achieved - Completion is scheduled end of October 2016
Colwyn Bay PCRC commissioned Green Achieved - West End Health Centre, Colwyn Bay opened in July
2016. This includes the Rysseldene & Rhoslan GP practices,
along with a number of Community Services.
Cluster Development
Cluster plans submitted and shared Green Achieved - All Cluster plans submitted and shared with PCSU at
the end of September.
These will be shared across the Area Teams with a focus on
delivering key actions identified, supported by the newly
appointed cluster co-ordinators.
Performance management process for plans clearly defined Amber Partially Achieved – staff recruited to support clusters across North Wales. Performance management processes are now being defined and will be implemented during Quarter 3. Monitoring arrangements for the implementation of the cluster
plans are in place across all Area Teams, supported by cluster
coordinators.
Revised template devised which encourages increased
reference to performance management. Seeking to integrate
fully in year.
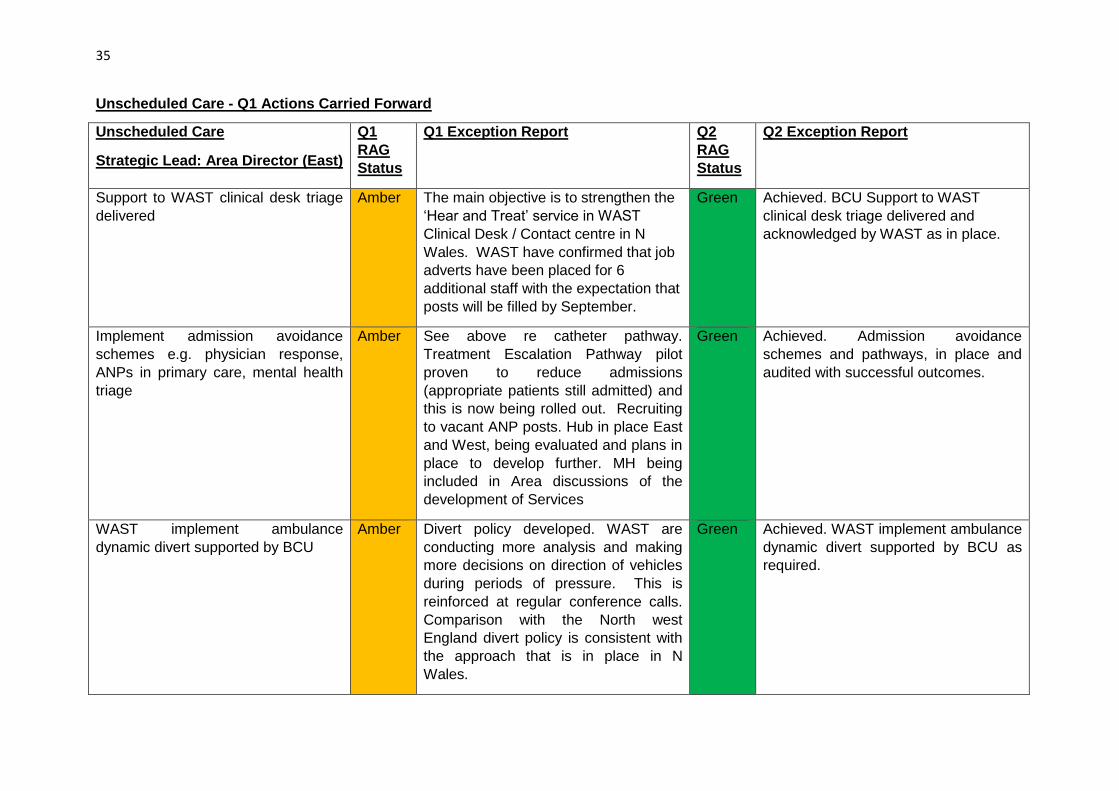
35
Unscheduled Care - Q1 Actions Carried Forward
Unscheduled Care
Strategic Lead: Area Director (East)
Q1
RAG
Status
Q1 Exception Report Q2
RAG
Status
Q2 Exception Report
Support to WAST clinical desk triage
delivered
Amber The main objective is to strengthen the
‘Hear and Treat’ service in WAST
Clinical Desk / Contact centre in N
Wales. WAST have confirmed that job
adverts have been placed for 6
additional staff with the expectation that
posts will be filled by September.
Green Achieved. BCU Support to WAST
clinical desk triage delivered and
acknowledged by WAST as in place.
Implement admission avoidance
schemes e.g. physician response,
ANPs in primary care, mental health
triage
Amber See above re catheter pathway.
Treatment Escalation Pathway pilot
proven to reduce admissions
(appropriate patients still admitted) and
this is now being rolled out. Recruiting
to vacant ANP posts. Hub in place East
and West, being evaluated and plans in
place to develop further. MH being
included in Area discussions of the
development of Services
Green Achieved. Admission avoidance
schemes and pathways, in place and
audited with successful outcomes.
WAST implement ambulance
dynamic divert supported by BCU
Amber Divert policy developed. WAST are
conducting more analysis and making
more decisions on direction of vehicles
during periods of pressure. This is
reinforced at regular conference calls.
Comparison with the North west
England divert policy is consistent with
the approach that is in place in N
Wales.
Green Achieved. WAST implement ambulance
dynamic divert supported by BCU as
required.
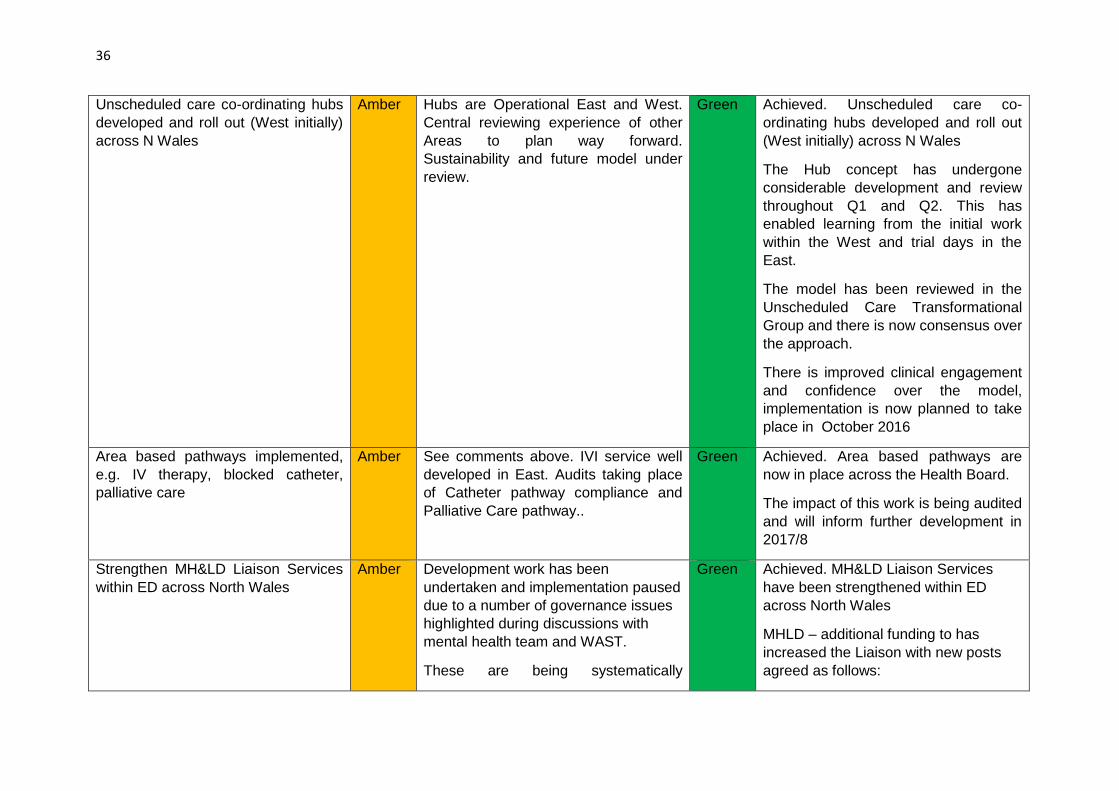
36
Unscheduled care co-ordinating hubs
developed and roll out (West initially)
across N Wales
Amber Hubs are Operational East and West.
Central reviewing experience of other
Areas to plan way forward.
Sustainability and future model under
review.
Green Achieved. Unscheduled care co-
ordinating hubs developed and roll out
(West initially) across N Wales
The Hub concept has undergone
considerable development and review
throughout Q1 and Q2. This has
enabled learning from the initial work
within the West and trial days in the
East.
The model has been reviewed in the
Unscheduled Care Transformational
Group and there is now consensus over
the approach.
There is improved clinical engagement
and confidence over the model,
implementation is now planned to take
place in October 2016
Area based pathways implemented,
e.g. IV therapy, blocked catheter,
palliative care
Amber See comments above. IVI service well
developed in East. Audits taking place
of Catheter pathway compliance and
Palliative Care pathway..
Green Achieved. Area based pathways are
now in place across the Health Board.
The impact of this work is being audited
and will inform further development in
2017/8
Strengthen MH&LD Liaison Services
within ED across North Wales
Amber Development work has been
undertaken and implementation paused
due to a number of governance issues
highlighted during discussions with
mental health team and WAST.
These are being systematically
Green Achieved. MH&LD Liaison Services
have been strengthened within ED
across North Wales
MHLD – additional funding to has
increased the Liaison with new posts
agreed as follows:

37
addressed by the mental health division
linking with Cardiff to learn from
experience and pathways which are in
place within South Wales and to ensure
this is implemented across North Wales
in q2.
Band 6 Mental Health Practitioners
(older adults)-3 West, 2 Central, 0.6
Central and West advertised these
posts on a secondment and have
recruited internally.
Speciality Doctors in Liaison
Psychiatry-x3 (one across each hospital
site). Advanced Heath Care Support
Worker-Band 4x 3(one per site).
Occupational Therapist in Psychiatric
Liaisonx3.
Recruitment anticipated recruitment
beginning Q3.
Mental health pathway implemented
as an alternative to ED attendance
Amber (Note this has been identified as a
specific and new action for q2 onwards)
Amber Mental health pathway implemented as
an alternative to ED attendance
Partially achieved.
Clinical Network Managers for each site
and one for Specialist Services (x4 in
total) have now been appointed to and
will actively be engaged with the
relevant managers, services and site to
ensure the division is more responsive
to demand and improve
communication.
Further actions to deliver in q3 are set
out below which form an integral part of
our seasonal plan for 2016/17
The team from Cardiff presented their
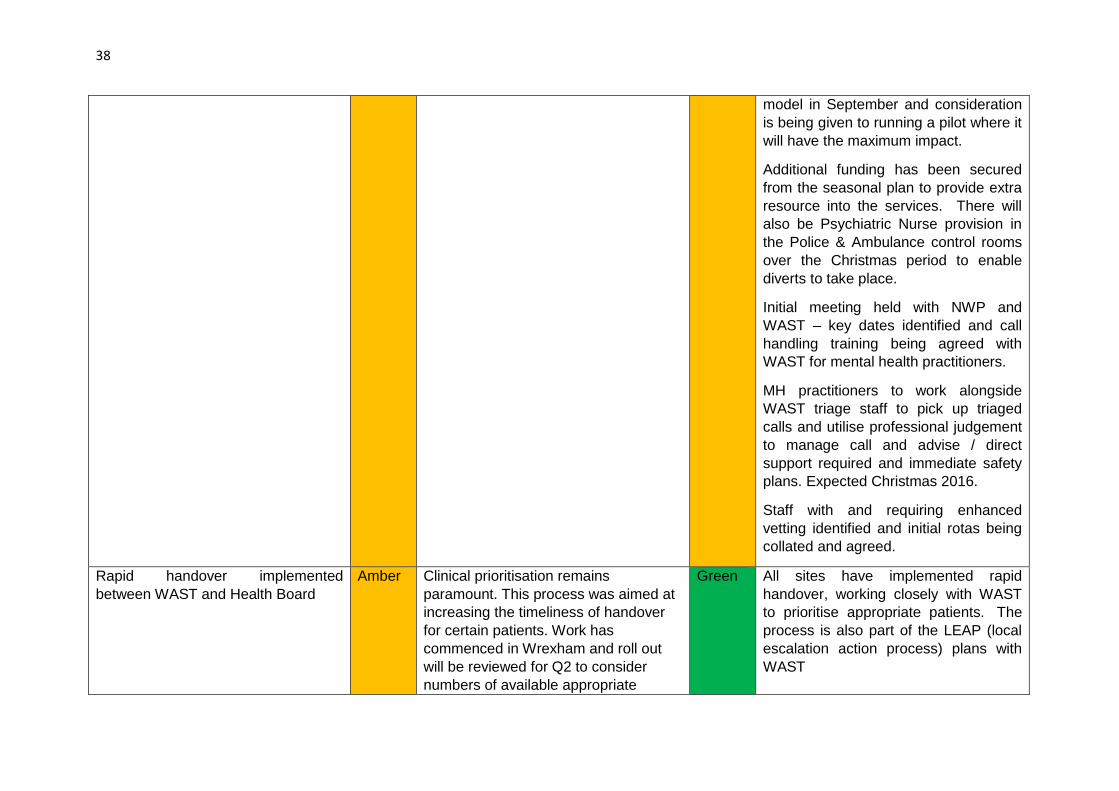
38
model in September and consideration
is being given to running a pilot where it
will have the maximum impact.
Additional funding has been secured
from the seasonal plan to provide extra
resource into the services. There will
also be Psychiatric Nurse provision in
the Police & Ambulance control rooms
over the Christmas period to enable
diverts to take place.
Initial meeting held with NWP and
WAST – key dates identified and call
handling training being agreed with
WAST for mental health practitioners.
MH practitioners to work alongside
WAST triage staff to pick up triaged
calls and utilise professional judgement
to manage call and advise / direct
support required and immediate safety
plans. Expected Christmas 2016.
Staff with and requiring enhanced
vetting identified and initial rotas being
collated and agreed.
Rapid handover implemented
between WAST and Health Board
Amber Clinical prioritisation remains
paramount. This process was aimed at
increasing the timeliness of handover
for certain patients. Work has
commenced in Wrexham and roll out
will be reviewed for Q2 to consider
numbers of available appropriate
Green All sites have implemented rapid
handover, working closely with WAST
to prioritise appropriate patients. The
process is also part of the LEAP (local
escalation action process) plans with
WAST

39
patients, as well as offload space.
However, all 3 sites utilise pathways
direct to wards/assessment.
More effective and integrated
discharge planning developed
through ICF and primary care
changes
Amber Discussions have taken place between
Primary Care and CoTE over increased
use of GPs in discharge process
Green Achieved. More effective and integrated
discharge planning developed through
ICF and primary care changes
A variety of arrangements have been
put in place to improve
acute/community discharge processes.
The discharge teams have been
transferred to the community and these
teams are now working jointly with
Community Resource teams to
expedite discharges/transfers.
There are improved processes in place
for review and escalation of DTOC and
long stay patients.
Q2 Actions Unscheduled Care
Unscheduled care
Strategic Lead: Area Director (East)
Q2 RAG
Status
Q2 Exception Report
Frailty tool and approach developed Green Achieved. Frailty tool and approach developed
The Frailty assessment model has been developed in each Area
and reviewed collectively within the Unscheduled Care
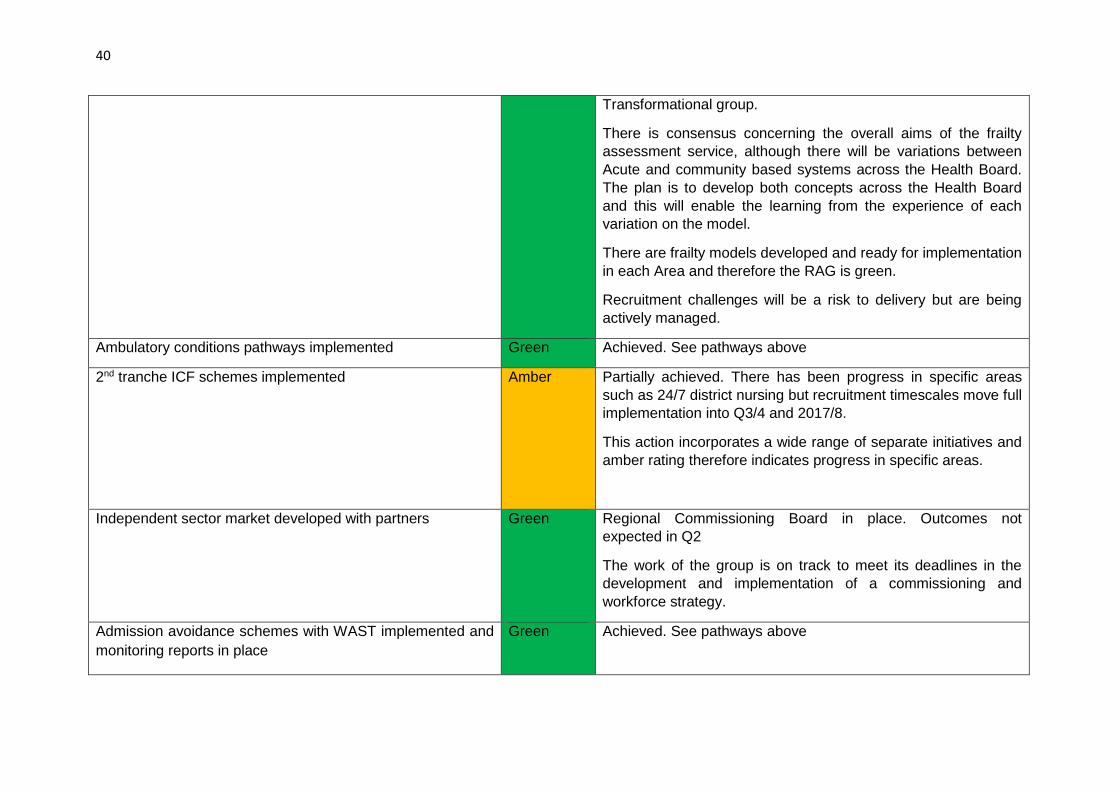
40
Transformational group.
There is consensus concerning the overall aims of the frailty
assessment service, although there will be variations between
Acute and community based systems across the Health Board.
The plan is to develop both concepts across the Health Board
and this will enable the learning from the experience of each
variation on the model.
There are frailty models developed and ready for implementation
in each Area and therefore the RAG is green.
Recruitment challenges will be a risk to delivery but are being
actively managed.
Ambulatory conditions pathways implemented Green Achieved. See pathways above
2nd tranche ICF schemes implemented
Amber Partially achieved. There has been progress in specific areas
such as 24/7 district nursing but recruitment timescales move full
implementation into Q3/4 and 2017/8.
This action incorporates a wide range of separate initiatives and
amber rating therefore indicates progress in specific areas.
Independent sector market developed with partners
Green Regional Commissioning Board in place. Outcomes not
expected in Q2
The work of the group is on track to meet its deadlines in the
development and implementation of a commissioning and
workforce strategy.
Admission avoidance schemes with WAST implemented and
monitoring reports in place
Green Achieved. See pathways above

41
RAU pathways implemented linked to community response
teams
Green Achieved. RAU pathways implemented linked to community
response teams
EDD roll out across all wards Green Achieved. EDD roll out across all wards across North Wales
Training and assurance of quality of care within the
independent sector working with partners and Care
Standards Wales
Green Achieved. Training and assurance of quality of care within the
independent sector has improved working with partners and
Care Standards Wales. The number of homes in escalation
continues to reduce.
Primary care links to ED enhanced and key interventions
identified
Green Achieved. This action is being incorporated within the Hub
development, which is where the community/primary care
presence within the hospitals will be based.
Model for future role of community hospitals agreed Amber Partially achieved and now being managed within the
Community Services portfolio see above. Model for community
hospital services linked to community hubs and will be different
across localities but based on agreed principles
The Community Transformation Board has been established. Work has commenced on staffing skills & workshops identifying models of practice and a literature review will feed into next Board. Paper ready for consultation by end of December. Experience in North Denbighshire will help define the overall model. All hospitals in the West updating their operational policies to
include referral and access criteria, options for maximising use
of community sites. Linking with community AvLOS and
Community Transformation Group work streams..
Seasonal plan signed off
Amber Partially achieved. Seasonal plan developed and presented to
Board in Sept. Some amendments required by the board and
being finalised in November.

42
Planned Care - Q1 Actions Carried Forward
Planned Care
Strategic
Lead:
Secondary
Care Director
Q1
RAG
Status
Q1 Exception Report Q2 RAG
Status
Q2 Exception Report
Demand
management
initiatives
implemented
e.g. CMAT,
pain,
dermatology
Amber CMAT is in place and
discussions held with the
key teams to develop
further demand
management initiatives,,
e.g therapy pathway as an
alternative to traditional
medical model, linked to
referral management
section above.
Amber Partially achieved. Demand management initiatives have been
implemented and more being done to roll out and spread best practice
across North Wales.
Diabetes triage model pilot for Mon will be rolled out if successful. Similar
models being considered for dermatology. CMAT s in place in West for
Rheumatology referrals. APPs (physio) within primary care also
contributing to demand management for primary care as well as onward
referrals to secondary care.
Plans being developed with Pain Team and Therapy Services in the East
with scoping work complete. Potential to relocate Pain Service with
CMATs and Therapy and developing links to the Community extended
scope practitioners.
Actions to improve: CMAT Central is currently working through revised
options for clinical input to the team. Additional support will be provided by
members of the Consultant Orthopaedic and Rheumatology Team during
quarter 3.
The Deeside Community Pain Service Pilot has now been formalised.
Hosted by Central the Deeside Service will initially receive transfers of
care from East to support RTT, and will receive referrals directly from
revised catchment areas from Quarter 3 onwards. The Deeside service
provides multi-disciplinary triage prior to secondary care attendance.

43
Clinic capacity
established to
deliver 10 day
cancer referral
to consultation
and new
referrals to
‘one stop’
services within
21 days for 62
day pathway
Amber All sites and teams are
focused on the
improvements, but some
capacity (staff) gaps
remain due to sickness
and vacancy. Recruitment
is underway. Current
performance is 56% for 10
days, and 61% for 21 days
Amber Partially achieved.
The Cancer Performance Group oversees the recovery plans which have
been implemented to support delivery of target.
Key challenges for sustainable delivery are:
East - Gastroenterology which has been constrained by workforce issues.
Centre – Colorectal. The straight to test pilot commenced with North
Denbighshire Practices which is to be reviewed with the potential to extend
more widely. An opportunity to review referral software is also being
examined. Endoscopy services transferred to the Surgical Directorate in
the Centre and this will enhance the opportunity for improvement.
10 day target: BCU as at end Sep – 54%
During quarter 2 gastro capacity in the East was increased with middle grade seeing USC. Additional WLI clinics were arranged in Central with overall reduction in waits, however, the 10 days target was not met.
21 day target: BCU as at end Sep – 63%
Central urology – a number of additional clinics were set up at the beginning of October with internal transfers to support improved delivery of target. The Directorate will work to maintain these additional clinics during quarter 3.
Central Breast – during quarter 2 clinic capacity was reinstated and this has supported reductions in waiting times; East Skin – patients booked days 22-32 following increase in demand in late summer and in September Actions to Improve: The Cancer Performance Group is well established and will continue to review cancer performance during quarter 3. The Group oversees the recovery plans which have been implemented to support delivery of target. Weekly Scheduled Care Groups on each

44
site monitor the delivery of this target through rigorous review of future un-booked capacity to ensure that USC OPD capacity is optimized and remedial plans put in place.
Additional Endoscopy Nursing staff recruited in YGC.
Colorectal – straight to test review meeting arranged with Clinical Director
and Colorectal/Gastro consultants for 2nd November 2016. Options to
support straight to test expansion and supporting software will be
considered.
The review of all clinic templates to support capacity planning for 17/18
commenced in Quarter 2 which will also identify USC demand and
capacity. This will be completed during quarter 3.
Sustainable
plans
developed to
ensure new
diagnostic and
surveillance
capacity in
place to deliver
access
standards
throughout the
year
Amber New Radiology equipment
commissioned in YG and
YGC to improve
management of demand. .
Specific capacity issues
identified within endoscopy
which has seen a rise in
demand. A review of
booking process as well as
a focus on demand
management is in place to
ensure a sustainable
model of endoscopy in
place by q2. All sites have
worked on creation of
additional capacity, e.g
introduction of nurse
endoscopists to
Amber Partially achieved.
- 99.15% of patients received diagnostic tests within the 8 week target.
East and West delivered 8 week diagnostics in endoscopy at the end of
Quarter 2. Significant improvements were delivered in the centre for
Endoscopy Services with reduction of 174 backlog during August and
September 2016. The use of Medinet to support delivery has reduced on
all sites during Quarter 2.
The West’s third endoscopy room has now been commissioned and will be
operational by March 2017. The East redevelopment Group is focused
upon the development of fit for purpose endoscopy facilities, which will
include a third endoscopy suite, planning in place to deliver. The Centres
sustainable plan is focused upon enhancing nursing support to the service.
All sites are compliant with surveillance timescales with the exception of
colonoscopy in the West and East,
The diagnostic 8 delivery for Q1 and Q2 was as follows:
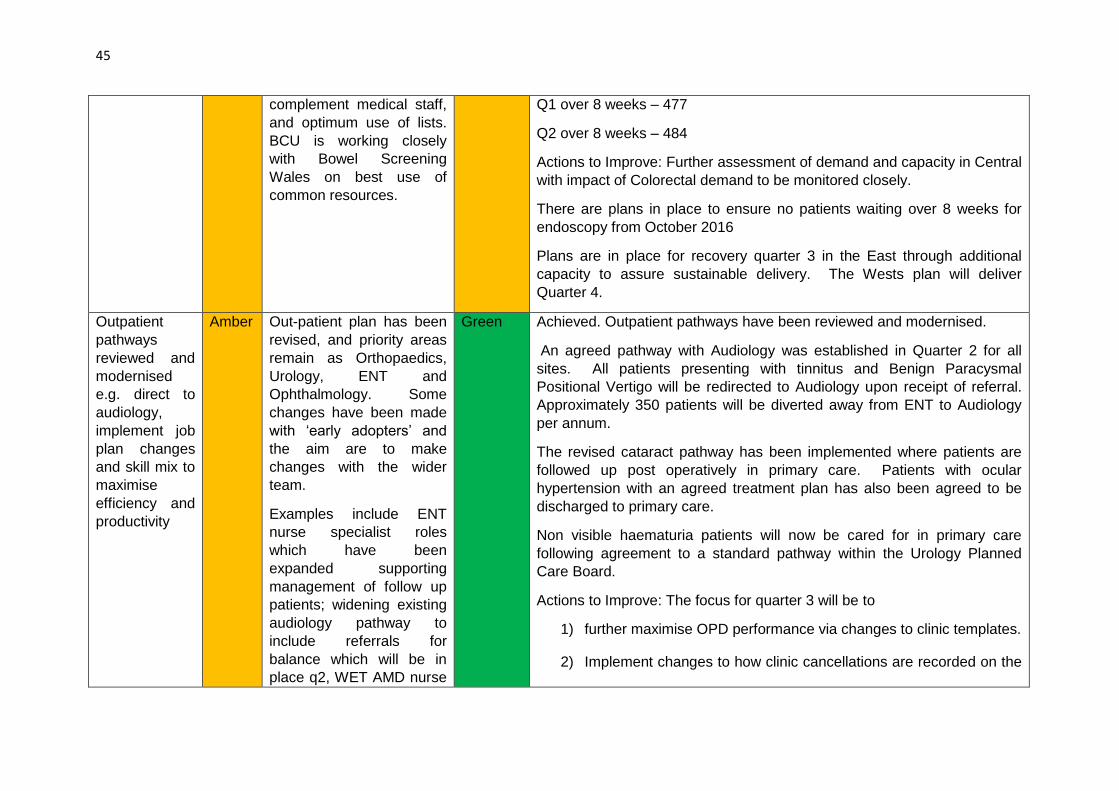
45
complement medical staff,
and optimum use of lists.
BCU is working closely
with Bowel Screening
Wales on best use of
common resources.
Q1 over 8 weeks – 477
Q2 over 8 weeks – 484
Actions to Improve: Further assessment of demand and capacity in Central
with impact of Colorectal demand to be monitored closely.
There are plans in place to ensure no patients waiting over 8 weeks for
endoscopy from October 2016
Plans are in place for recovery quarter 3 in the East through additional
capacity to assure sustainable delivery. The Wests plan will deliver
Quarter 4.
Outpatient
pathways
reviewed and
modernised
e.g. direct to
audiology,
implement job
plan changes
and skill mix to
maximise
efficiency and
productivity
Amber Out-patient plan has been
revised, and priority areas
remain as Orthopaedics,
Urology, ENT and
Ophthalmology. Some
changes have been made
with ‘early adopters’ and
the aim are to make
changes with the wider
team.
Examples include ENT
nurse specialist roles
which have been
expanded supporting
management of follow up
patients; widening existing
audiology pathway to
include referrals for
balance which will be in
place q2, WET AMD nurse
Green Achieved. Outpatient pathways have been reviewed and modernised.
An agreed pathway with Audiology was established in Quarter 2 for all
sites. All patients presenting with tinnitus and Benign Paracysmal
Positional Vertigo will be redirected to Audiology upon receipt of referral.
Approximately 350 patients will be diverted away from ENT to Audiology
per annum.
The revised cataract pathway has been implemented where patients are
followed up post operatively in primary care. Patients with ocular
hypertension with an agreed treatment plan has also been agreed to be
discharged to primary care.
Non visible haematuria patients will now be cared for in primary care
following agreement to a standard pathway within the Urology Planned
Care Board.
Actions to Improve: The focus for quarter 3 will be to
1) further maximise OPD performance via changes to clinic templates.
2) Implement changes to how clinic cancellations are recorded on the
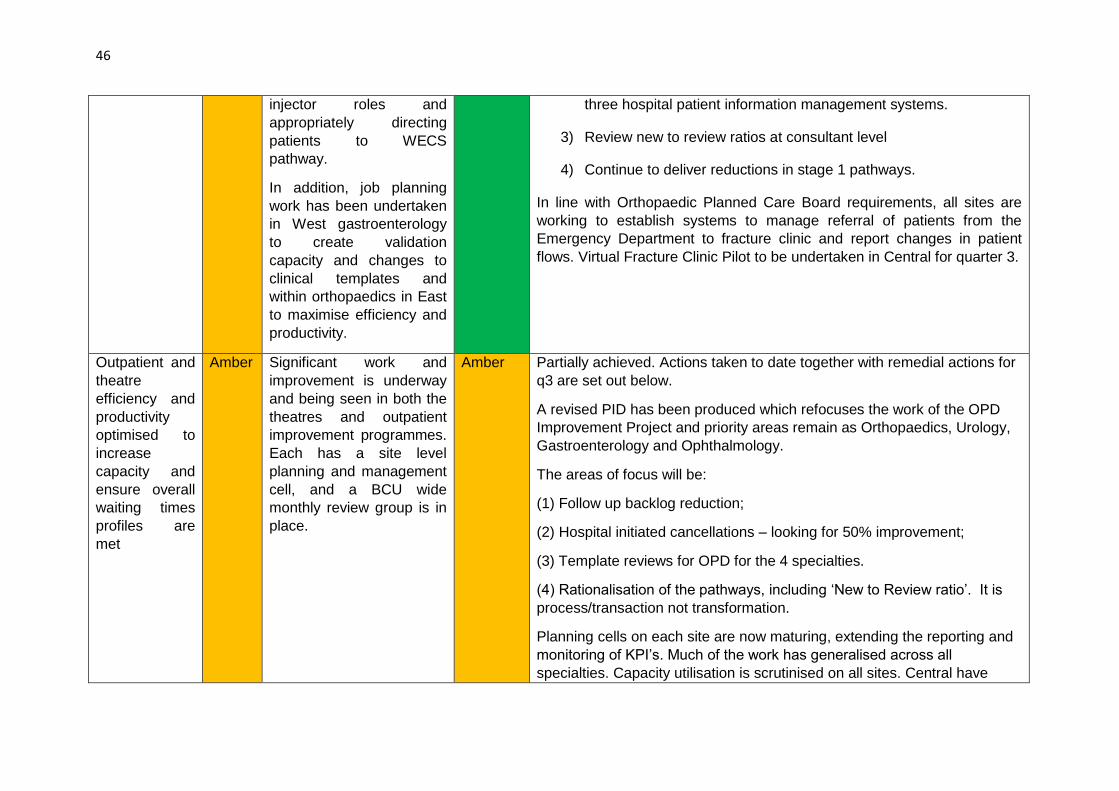
46
injector roles and
appropriately directing
patients to WECS
pathway.
In addition, job planning
work has been undertaken
in West gastroenterology
to create validation
capacity and changes to
clinical templates and
within orthopaedics in East
to maximise efficiency and
productivity.
three hospital patient information management systems.
3) Review new to review ratios at consultant level
4) Continue to deliver reductions in stage 1 pathways.
In line with Orthopaedic Planned Care Board requirements, all sites are
working to establish systems to manage referral of patients from the
Emergency Department to fracture clinic and report changes in patient
flows. Virtual Fracture Clinic Pilot to be undertaken in Central for quarter 3.
Outpatient and
theatre
efficiency and
productivity
optimised to
increase
capacity and
ensure overall
waiting times
profiles are
met
Amber Significant work and
improvement is underway
and being seen in both the
theatres and outpatient
improvement programmes.
Each has a site level
planning and management
cell, and a BCU wide
monthly review group is in
place.
Amber Partially achieved. Actions taken to date together with remedial actions for
q3 are set out below.
A revised PID has been produced which refocuses the work of the OPD
Improvement Project and priority areas remain as Orthopaedics, Urology,
Gastroenterology and Ophthalmology.
The areas of focus will be:
(1) Follow up backlog reduction;
(2) Hospital initiated cancellations – looking for 50% improvement;
(3) Template reviews for OPD for the 4 specialties.
(4) Rationalisation of the pathways, including ‘New to Review ratio’. It is
process/transaction not transformation.
Planning cells on each site are now maturing, extending the reporting and
monitoring of KPI’s. Much of the work has generalised across all
specialties. Capacity utilisation is scrutinised on all sites. Central have
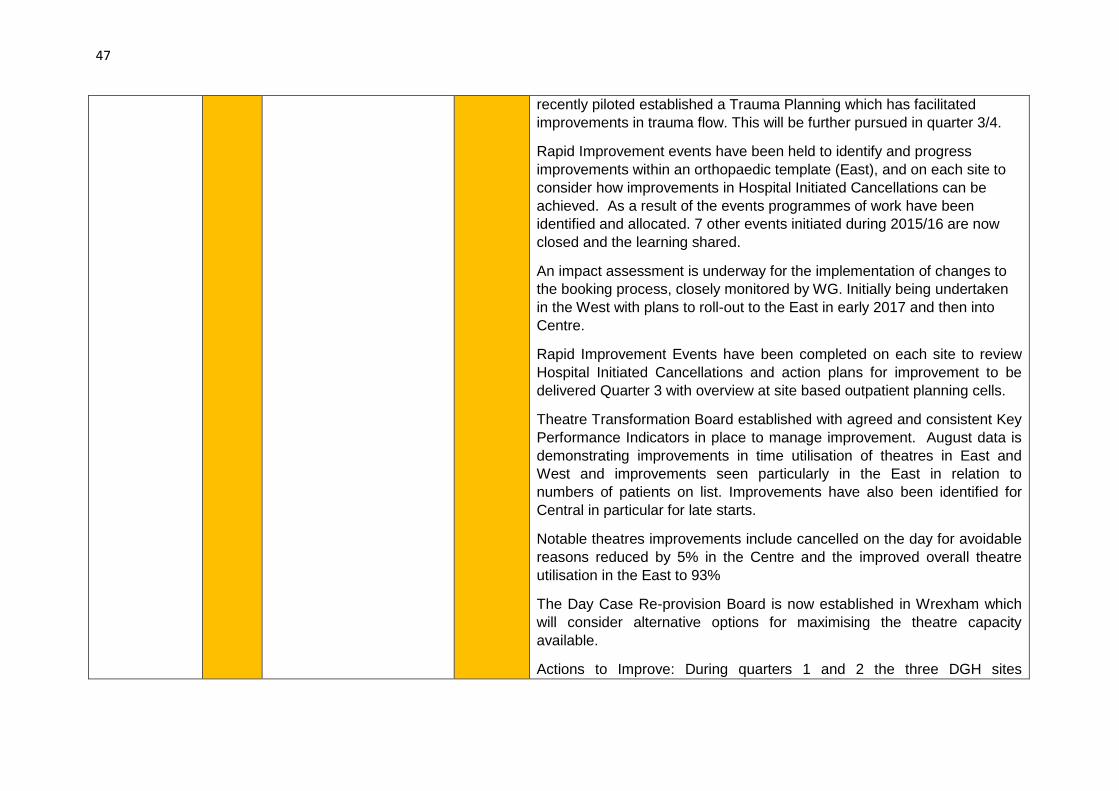
47
recently piloted established a Trauma Planning which has facilitated
improvements in trauma flow. This will be further pursued in quarter 3/4.
Rapid Improvement events have been held to identify and progress
improvements within an orthopaedic template (East), and on each site to
consider how improvements in Hospital Initiated Cancellations can be
achieved. As a result of the events programmes of work have been
identified and allocated. 7 other events initiated during 2015/16 are now
closed and the learning shared.
An impact assessment is underway for the implementation of changes to
the booking process, closely monitored by WG. Initially being undertaken
in the West with plans to roll-out to the East in early 2017 and then into
Centre.
Rapid Improvement Events have been completed on each site to review
Hospital Initiated Cancellations and action plans for improvement to be
delivered Quarter 3 with overview at site based outpatient planning cells.
Theatre Transformation Board established with agreed and consistent Key
Performance Indicators in place to manage improvement. August data is
demonstrating improvements in time utilisation of theatres in East and
West and improvements seen particularly in the East in relation to
numbers of patients on list. Improvements have also been identified for
Central in particular for late starts.
Notable theatres improvements include cancelled on the day for avoidable
reasons reduced by 5% in the Centre and the improved overall theatre
utilisation in the East to 93%
The Day Case Re-provision Board is now established in Wrexham which
will consider alternative options for maximising the theatre capacity
available.
Actions to Improve: During quarters 1 and 2 the three DGH sites
48
coordinated clerical and clinical validation across all specialties. Additional
validation clerks will be recruited to support this work during quarter 3.
BCU is currently delivering circa 8% validation across the three DGH sites.
Each site has reviewed its cancellation rate position. Work to improve and
standardise data on each patient administration system has been identified
as a key priority for Q3.
Directorates will revise clinics templates by 31/10/16. This will inform the
OP capacity planning process for 2017/18.
As part of the national outpatient improvement work, additional scrutiny will
be applied to new to review ratios in quarter 3 and 4. Consultant level
information has been issued to the Directorates and these will inform both
outpatient improvement and consultant job plan/performance meetings.
The Central team will Implement Planning Cell in Abergele Hospital
(Orthopaedics)
Reviews of templates are being undertaken on all sites in order to inform
capacity planning.
A live webpage showcases the work undertaken and will be further
developed during Q3.
Support current and developed additional PDSAs for each site to reduce
avoidable cancellations on the day which is a key feature to the
improvement of productivity on each site.
Theatre Utilization has remained consistent across the three sites during
quarter 2 with no significant changes. Alturos is now implemented across
the majority of specialties, and the impact of the scheduling processes will
be monitored closely during quarter 3.
Transfer of theatre information management and reporting to BCU
Information Department in November 2016.
49
Increased
access to
diagnostics by
primary care
Amber Implementation of a
referral pathway in Central
for colorectal patients.
Referrals from primary
care triaged to
endoscopy/CT
colonoscopy as
appropriate based on their
symptoms. Pilot is being
supported by the lower GI
team in YGC.
Standardised referral pathway for MRI in low back pain developed and being led by CMATS. The pathway has been agreed and staff being recruited. Meetings held with primary care to develop pathways for renal and neurological referrals in q2 onwards.
Amber Partially achieved. Plans have been developed and being implemented to
increase access to diagnostics by primary care with more work required to
roll out and spread best practice across North Wales.
Faecal Calprotectin (FCP) diagnostic testing in surgeries in Anglesey and
Arfon clusters are being piloted to determine the effectiveness of the
diagnostic test which supports clinicians in identifying the differential
diagnosis of inflammatory bowel disease (IBD) or Irritable bowel syndrome
(IBS) and directs them down an appropriate pathway for treatment –
avoiding unnecessary referrals to secondary care / colonoscopy treatment.
Pilot study undertaken in surgery in Amlwch (Anglesey) to test the effectiveness of Point of Care (PoC) C-Reactive Protein (CRP) testing in GP surgeries to guide antibiotic prescribing Funding confirmed from WG for an additional 10 CRP machines to be rolled out to outlier GP surgeries in Gwynedd and Anglesey. The effectiveness of the additional CRP machines once implemented in other GP surgeries will be evaluated.
Anaemia Pathway for patients requiring Blood Transfusion drafted and
discussed with Cluster leads in West for GPs refer patients requiring blood
transfusion directly to the appropriate medical speciality team if the patient
is already known to them and the anaemia is related to that condition who
will then be treated via the therapies unit at Ysbyty Gwynedd. Following
approval pathway to be piloted.
Additional
external
activity
contracted
within
diagnostics
and elective
specialties to
Amber We have utilised all
available capacity from
providers (both NHS and
private), e.g. Countess of
Chester have supported
Gynaecology. However,
capacity available falls
Green Achieved. In Quarter 2 320 orthopaedic procedures were commissioned
from external providers and 210 general surgery procedures for delivery
through to March 2017. Medinet continued to provide additional capacity
in endoscopy albeit reducing. FDC capacity is still commissioned from an
external provider to support delivery of the profile for East.
Actions to Improve: A review of FDC capacity will be undertaken early
quarter 3 for Central FDC. Recent changes in reporting of GA and

50
ensure all q1
profiles are
met.
short of requirements. increase in FDC OPCs code reporting have generated additional demands
on the service. Central will also be seeking to appoint a 4th Consultant
Urologist in quarter 3.
Q1 Outpatient
follow up and
programmed
reduction
through GP
LES and virtual
consultant
clinics
delivered
Amber There has been a 10%
reduction overall in
outpatient backlog across
North Wales in q1.
The Follow Up Task &
Finish Group will continue
to focus on a managed
reduction programme
within secondary care.
Changes to protocols
within specialties (to avoid
unnecessary follow-ups),
additional virtual clinics
(with consultants reviewing
notes only), and additional
follow up clinics to confirm
discharge are all being
deployed by teams.
Primary Care represented
with senior GPs, and
options to transfer
appropriate patients back
to the care of their GP are
being explored.
Amber Partially achieved.
Virtual clinics running for COTE and movement disorder for patients in
Dwyfor and Dolgellau. Teledermatology in place for North Anglesey and
Dwyfor – further rollout not possible until fully established (1 WTE
consultant vacancy). Centre: The uptake in both Conwy and
Denbighshire was quite low 7 practices are officially signed up in each
county.
Actions to Improve: Further VC consultations under review as options and
will be progressed via planned care transformation group during quarter 3.
Develop plans
for Q2-Q4 in
light of
discussions
Amber Operational teams have
met with Welsh
Government (WG)
throughout June and early
Green Achieved
A WG Outpatient Transformation Steering Group has been established
and BCUHB is represented by a clinician, area manager and OP project

51
with WG July. The review of data
and assumptions has been
comprehensive, and the
WG Delivery Unit has
confirmed the quality of the
BCU data. Final
confirmation of Q2 plan
with WG.
lead. Examples of transformation have been submitted. Public
engagement events are being planned across Wales in order to inform a
comprehensive OP strategy for Wales.
Actions to Improve: The BCU OP Transformation Group will oversee
delivery of plans across the DGH sites via site specific planning cells.
RTT (36 and 8 week) deliverables for Q3 and Q4 have been agreed with
WG, and discussion continues on the framework for this.
Q2 Actions -Planned Care
Planned Care
Strategic Lead: Secondary Care Director
Q2 RAG
Status
Q2 Exception Report
All Wales review of nerve conduction service
provision supported
Green Achieved. WHSCC are currently setting up a process to develop their
Commissioning Plan for Specialised Neurosciences over the next 3 years,
with the overall aim of undertaking an assessment of the current provision of
specialised neurosciences services for patients in Wales. This work will
include an evaluation of progress against the recommendations from the
previous reviews of neurosciences services conducted between 2007 and
2010, in order to inform the development of a clear commissioning plan for
specialised neurosciences services for the next five to ten years.
Clinical and administrative validation completed to
ensure compliance with RTT rules
Green Achieved. Validation teams are established on each site within Surgery and
Medicine who undertake full pathway validation for the longest waiting
patients. Lessons learnt and themes/issues identified are used as a learning
tool to ensure RTT compliance. A review of outcome form compliance has
been completed specifically with regard to USC.
Medium and longer term delivery of orthopaedic
services for North Wales reviewed
Green Achieved. Good progress has been made with the appointment of an
Orthopaedic Transformation Lead to oversee the process for the BCU. A
workshop was been held with key stakeholders on the 29th September 2016

52
during which potential strategic options were considered.
Outpatient and theatre efficiency and productivity
optimised to increase capacity and ensure overall
waiting times profiles are met
Amber Partially achieved and tight monitoring arrangements in place to track
progress. For quarter 2 efficiency and productivity monitored via Weekly BCU
Access group meetings with site specific analysis undertaken via weekly
Planning Cells. Productivity key performance indicators are established for
key specialties
Actions to Improve: Full implementation of Alturos theatre scheduling process
across all sites. Efficiency improvements will continue to be pursued via
weekly planning cells.
Theatre Transformation Group will continue to oversee delivery of KPIs for
each site, with PDSA work focusing on the reasons for non-delivery of
optimum productivity.
Speciality
Best in class
target
Actual (end
of Sept)
Gen Surg 2.1 1.8
Urol 3.2 3.1
T&O 2.2 2
ENT 2.9 2.6
Ophthal 6 4.6
MF 2.4
Q2 Outpatient follow up programmed reduction
delivered
Amber Partially achieved across north Wales.
As at end of quarter 2 (year to date):
East delivered reduction of 3445 patients, with majority in Ophthalmology
(911).

53
Central delivered reduction of 2,619 patients, of which 1,186 was delivered in
Urology.
West delivered reduction of 3562, of which 1262 delivered in Ophthalmology
Actions to Improve: All sites will continue to identify capacity to continue the
reduction in overall backlog, focusing on overdue unbooked and areas of
highest potential clinical risk (including Ophthalmology and Urology).
The approach is to:
- Add additional capacity (in parallel with extra RTT work), for both
validation/virtual clinics and face to face clinics
- Clinical and clerical validation
- Changes to pathways including use of alternate pathways
Operational challenges include medical workforce capacity.
The Follow up Group will oversee delivery of reduction trajectories for each
site.
Actions to deliver agreed profile of reduction as
agreed with WG implemented
Amber BCU continues to work closely with WG to ensure agreed profile for 36
weeks RTT (With confirmed target of zero > 8 weeks)
During Q3, operational teams will work to a Q3 end position of 4200 > 36
weeks and 0 > 8 weeks

54
Mental Health & Learning Disabilities - Q1 Actions Carried Forward
Mental Health
Strategic Lead: Director of Mental
Health
Q1
RAG
Status
Q1 Exception Report Q2
RAG
Status
Q2 Exception Report
Staff Engagement
Staffing levels fully assessed against
quality and safety
Amber Mental Health and LD division is
currently implementing the All Wales
Acuity programme for mental health
workload assessment. Implementation
of phase 1 has been completed with a
total of 7 wards being included in the
pilot stage. Whilst there was a variation
no risks were identified. Phase 2 of the
pilot is due to commence with a further
third of mental health wards included.
Public Health Wales will be supporting
the roll out of phase 2 and supporting
BCU with a workshop and also to
explore our learning from Phase 1.
Completion of the project is anticipated
September 2016.
Green Achieved. Staffing levels have been
fully reviewed against quality and
safety.
A full establishment review has being
undertaken; all MH wards will
undertake the establishment review
against the All Wales workload
assessment tools. A report will be
produced that triangulates planned
establishment versus actual
establishment versus professional
judgement.
It is expected a report will be produced
by mid November 2016.
Mental Health Measure
Good practice exchange implemented
within the Division
Amber Refreshed training programme starting in September 2016.
Green Achieved. Good practice exchange has been implemented within the Division through MHM training. Dates for the refreshed training 2 year programme are from 13th October 2016 across the Division with 3 levels of
55
training agreed. This programme has been refreshed to highlight areas of process and good practice and evidence from the patient satisfaction survey.
Strategy Development
Multi-Agency approval to strategy development agreed
Amber The development of an Integrated
Strategy with partners is key to being
able to demonstrate population health
improvements in mental health and
wellbeing. The impact of mental health
problems and difficulties impact on all
aspects of life and therefore on many
services provided by the public and
third sector.
In order to secure involvement of all
sectors, a governance model is
currently being developed to include
Local Authorities, Police, Ambulance,
Fire and Third sector representatives.
This is in the early stages of
development, but signals an important
step in the development of a strategy
which encompasses not only health,
but housing, education, crime and
justice, leisure, community safety as
well as social care.
Progress has been made in establishing user and carer engagement in the shaping of the
Green Achieved. Multi agency approval has
been agreed.
A paper outlining the integrated
approach to the MH Strategy was
presented and agreed at the Part 9a
Partnership Board in May 2016. This
group is undertaking further work to
agree the priorities, but it is likely that
MH may be identified.
September 2016 – an update on the
development of the MH Strategy was
presented to the Directors of Social
Services across North Wales and the
proposal for an integrated strategy was
supported. It was agreed that a review
would be undertaken on the current
strategy governance arrangements with
recommendations on future
arrangements to be presented at a
future meeting.

56
mental health strategy. A number of engagement events were held in the summer of 2015, attended by 250 users and carers and 150 staff and have provided the Health Board with an early indication of priorities for action for the development of mental health services in North Wales. These priorities have now been shared with third sector organisations for validation, comment and feedback. In addition a draft engagement strategy for older people’s mental health services has been developed by Flynn and Eley Associates and has been consulted upon. Agreement has been secured with the North Wales Cross Sector Chief Executives Leaders and Chairs Group for the development of an integrated strategy to mental health and well being. A programme management approach has been put in place to include; needs assessment, workforce planning across all sectors, user and carer engagement and finance and commissioning. This multi agency approach will direct the timescale for delivery of the strategy. There has also been agreement of a good settlement for Prison Health

57
T4MH Partnership re-launched Amber Together for Mental Health, the Welsh Government’s 10 year strategy to improve mental health and wellbeing was published in 2012 following significant engagement and consultation with key partner agencies, stakeholders, services users and carers It is a cross-government strategy and covers all ages, ranging from a whole population approach in improving the mental well-being of all residents in Wales, through to the support needed for those with a severe and enduring mental illness. The strategy consists of five chapters and is underpinned by 18 outcomes. These were subject to detailed formal consultation in 2012 and remain unchanged for the lifetime of this delivery plan. These outcomes have been mapped to the Goals contained within the Wellbeing of Future Generation (Wales) Act 2015. There are a number of engagement events scheduled throughout 2016.
Amber Partially achieved. A key requirement of the Together for Mental Health Delivery Plan 2016-2019 is to review the Partnership Board. This work will be undertaken over the coming 3 months and will be part of the wide-ranging review of governance to support the development of the strategy. Initial work has been undertaken but further work required as part of the strategy. This will be worked through in Q3 – complete in Q4.
External assessment and review
commissioned
Amber A strategic review of mental health services in North Wales is to be commissioned to ensure that future mental health and well-being services not only reflect the needs of the population but the priorities identified by users and carers for mental health services and in addition develop models of care based on research and best practice.
Green Achieved. External assessment and review has been commissioned. The strategic partners have now been appointed and have commenced the strategic review which is due to report November 2016.

58
This review is in the process of being commissioned, informing not only the strategic direction of Mental Health, but the overarching Clinical Services strategy. Further engagement is required to continue staff and user/carer involvement to ensure that they contribute to the development of the strategy and assist in the shaping of future services for the population of North Wales.
Additionally, the review will focus on
prevention and mental health and well
being, Inclusion of the wider
determinants of health, Education,
Housing and Employment and will
cover the full range of services
including Child and Adolescent Mental
Health Services, Adults of Working
Age, Forensic services, Substance
Misuse Services, Learning Disabilities
and Older People’s Mental Health
Services.

59
Q2 Actions -Mental Health and Learning Disabilities
Mental Health & Learning Disabilities
Strategic Lead: Director of Mental Health
Q2 RAG
Status
Q2 Exception Report
Leadership
Briefing / communication arrangements with the division
developed including roadshows / workshops
Green Achieved. Communication arrangements have been developed.
A range of briefings/communications and workshops have taken
place across the Division over the last six months. There is,
however, the need to develop a wider communication plan for
the Division. This has been commenced, but due to the scale
and scope required, it is proposed that the Division require some
dedicated communications support.
Staff Engagement
Attendance and staff productivity optimised with metrics
reported
Green Achieved.
External consultant has undertaken a training programme to
ensure staff understanding and adherence to the All Wales
Sickness Absence policy.
Appointment of Clinical Network Managers where sickness
levels will be performance managed as part of an agreed set of
metrics via the newly convened Divisional Finance &
Performance monthly meeting, which will provide increased
scrutiny on metrics and targets.
Funding from Special Measures has been authorised to provide
additional dedicated WOD posts who will now take over the
Sickness Absence monitoring, training and reporting going
forward working closely with the Clinical Network Managers.
60
Physical Health
Access to GP held information / health records improved Amber Partially achieved. WCCIS is the single Information solution
supporting integrated delivery of community health and social
care. Mental Health are now engaged with the Project Board &
Team and have convened a Divisional Operational Group to
implement the system commencing in West in April 2017.
WCCIS will allow shared access to records supporting patient
centred care which will be coordinated and integrated.
There is also the iFIT project underway which MHLD East is
engaged with implementation from October 2016.
Awaiting update from regional Board expected end of October
regarding roll-out programme for WCCIS.
Workstreams established to identify key areas of
improvement
Green Achieved. Workstreams have been established to identify key
areas of improvement.
An area of good practice has been identified in West and
consideration is being given to replicate the practice across
other areas to monitor physical health in secondary care
patients.
Agreed a revitalisation of smoking cessation across the Division
led by the Lead Nurses and linked with CANIAD to ‘train
trainers’.
Funded by Health Inequalities via WG a Lead has been
identified to conduct physical health screening on clients with
enduring MH problems throughout Gwynedd, mainly in Primary
care and Community Mental Health Teams. This includes
teaching sessions for GP surgeries, links with Bangor University
and Public Health Wales.

61
Information to families and carers provided Green Achieved. Information to families and carers is being provided
Families are carers are all part of the CTP process under the
MHM legislation. Compliance for this in patient areas will be
monitored through the monthly Q&S audits. CTP’s are co-
produced with patients and care co-ordinators.
Part 2 CTP compliance is reported weekly to local managers
and SMT.
A process for community audit needs to be agreed.
MH&LD will link with Patient Experience teams to ensure that
timely information is passed to carers and families.
Mental Health Measure
Data collection and audit refined Amber Partially achieved. Current audit process is underway to ensure
there is adequate assurance regarding sharepoint data
collection and accuracy. Recommendations will be reported in
November 2016 for action in Q3.
Regular use of exception reports to validate performance Green Achieved. The Division reports monthly by exception and
continual improvements to compliance have been noted for
MHM.
Caseload audit undertaken Amber Partially achieved. Current audit / validation is underway to
ensure there is adequate assurance regarding sharepoint data
collection and accuracy and that all patients once accepted into
part 2 services are reflected on sharepoint. This work links
closely with the revised training programme and dates are now
scheduled to visit teams until the end of October. The
recommendations and findings will be reported by 1st December
2016.
62
Performance requirements met Green Achieved. Performance requirements have been fully met.
Weekly monitoring of the MHM is reported direct to the newly
appointed Clinical Network Managers who are directly
accountable for the performance against the MHM. Revised
training programmes underway from October 2016 and key
actions are:
• Weekly monitoring of team performance.
• Weekly communication to individual practitioners
regarding their non-compliant cases.
• Feedback to managers, who are the accountable
managers for the delivery of the measure standards.
• Responsible Managers following local action plans.
• Data cleansing reports sent out to avoid any errors in the
data collection.
Monthly reports to the Divisional Finance & Performance Group
for scrutiny.
Environment & Estate
Short term estate plan for improvement developed Green Achieved. Short term estate plan for improvement developed Review completed of potential ligature points within all current mental health in-patient accommodation and classified on the basis of an agreed risk profile. Three contract frameworks established and a Contractor
appointed to each Area.
Anti-ligature works have been completed within the Ty Llewellyn
63
wards.
Works have commenced in the Cemlyn, Cynan, Careg Fawr and
Messen Fach units.
Environmental improvements implemented Amber Partially achieved. Detailed environmental surveys completed.
Some works have been completed or, are underway with
planned completion by end of Q4.
Detailed schedule of works completed for all anti-ligature and
environmental works with outline programme. The works are
planned over two years. Bid submitted for 16/17 & 17/18 funding
for both inpatient and other units
The bid for £4.2million for 16/17 has been approved covering
elements of both anti-ligature and environmental works.
A series of options have also been developed for alterations to
the internal reconfiguration of the existing acute inpatient units.
Outline bid submitted and further work required for end of
October.
The following additional units are being programmed to start,
with some completed this year:
- Heddfan, all wards
- Bryn Hesketh
- Bryn y Neuadd, Foelas, Tan y Coed & Llys
Meddyg
- Hergest – Taliessen
- Coed Celyn
- Tan y Castell
64
- Risk assessment tool piloted
The following actions are being taken forward over the coming
month.
Revised governance structure being implemented with
meetings at locality level and an overall project board.
This will aid decision making, improve engagement
within localities and support contract management.
Brief locality teams in detail on work programme.
Continue mobilisation of contractors on agreed sites.
Develop the reconfiguration options further with locality
teams for consideration by Division and Executive Team
to allow recommendations to be made to the Health
Board in line with the timetable for Operational Plan.
Target to submit to 25/10/16 Finance & Planning
Committee.
Commence rollout of risk assessment tool into wards,
starting with Coed Celyn and Tan y Castell.
Governance, Quality & Safety
Governance reporting reflected in accountability reviews Green Achieved.
MHLD QSE report was submitted in September for Board QSE
meeting. Regular tracking of governance KPI’s is undertaken in
monthly accountability review.
Learning cascade system implemented within the Division Green Achieved.
The Division has developed a monthly ‘Learning from Incidents
and Complaints’. Version 1, September 2016 has been
cascaded throughout the division. There were three themes

65
addressed: Communication; Involvement of friends and family
and reaffirming the Therapeutic Engagement and Observation
Policy. This also gives an opportunity to provide positive
feedback to staff, general themes being; approachable,
supportive, kind, friendly, patience and compassion.
The Division also has a ‘Learning Event’ scheduled for
November 2016 (postponed from September 2016). Speakers
will include launch of Safe Wards and also a case study will be
presented with input from the patient’s family.
Engagement plans signed off and implementation
commenced
Green Achieved.
A new strategy for mental health services by the spring of 2017.
The development of the strategy is being led by the Head of
Strategy and Partnership for BCUHB and is being supported
through the diagnostic phase by Mental Health Strategies and
Professor Steve Trenchard.
To support the development of that strategy and to ensure that
the development is co-produced, a series of workshops has
been arranged. These build on engagement events from the last
year where around 500 colleagues have shared their ideas on
what they’d like to see in the future. All workshops are to be
completed by November 2016.
Strategy Development
Widespread engagement with service users / carers and
stakeholders
Green Achieved.
CANIAD have been appointed and are taking a leading role on
the engagement to undertake a series of events in services. This
will include 360 surveys to be completed by the end of October
2016 gathering information from current service users and
carers or, those who have recently left services.

66
Engagement work being undertaken with general public – using
the BCUHB 3 area Engagement Officers using the ‘5 Ways to
Well Being’ and ‘Time to Change Wales’.
Senior Management Team are to have ‘open’ meetings once a
month across the Division to invite staff along to ask questions.
Diagnostic assessment complete and reported Amber Partially achieved as above – due to report in November 2016
Mental Health Strategies has been commissioned to undertake
this work which has commenced.

67
Maternity - Q1 Actions Carried Forward
Maternity
Strategic Lead: Secondary Care
Director
Q1
RAG
Status
Q1 Exception Report Q2
RAG
Status
Q2 Exception Report
Medical Staffing increased Amber Detailed recruitment work undertaken
to date which has increased the overall
Medical cover across north Wales and
reduced locum cover rates from 60% in
October 2015 to 24% at end June
2016.
Significant focus will remain on this and
will be progressed in Q2 with plans to
reduce locum cover to 20% in q2 and
18% in Q3.
Green Achieved. A detailed Medical Model is being developed as part of the Sustainable Plan for Delivery of Women’s Services. To date four permanent Resident on Call Consultant posts have been appointed in West on 23/9/16. Interviews for four permanent Resident on Call Consultant posts for East are scheduled in Q3 – (28/10/16). Plan to recruit to posts in Central to be secured in Q3.Significant focus will remain on reducing locum use in Q3 to the projected 18%. A paper will be brought to the Executive Management Group in early Nov to provide a detailed case for the establishment of permanent resident consultant staff, as well as bring the Anaesthetic on call capacity to the level necessary for sustainable rotas
68
Q2 Actions - Maternity
Maternity
Strategic Lead: Secondary Care Director
Q2 RAG
Status
Q2 Exception Report
RCOG report findings fed into service planning Green Achieved.
RCOG recommendations detailed in the report form part of the
evidence considered in relation to developing a Framework for
Maternity, Neonatal and Paediatrics as part of the requirements
of Special measures which remains an action for Q3.
Surnicc FBC submitted to WG Green Achieved.
The FBC was formally approved at the public meeting of the
Health Board on 21st July and submitted to Welsh Government
for consideration the following day. During August and
September it underwent the normal scrutiny process before
being considered by the Infrastructure Investment Board, which
was held on 28th September. The Recommendations made by
the Infrastructure Investment Board will be presented to the
Cabinet Secretary week commencing 3/10/16 and a definitive
decision will follow.
Potential service models identified Amber Partially achieved. Potential Service Model – During Q2 the Acute Hospital Care Programme has been established. This is one of the 3 Key Programmes which will develop the longer term Living Healthier, Staying Well Strategy. A baseline assessment has been commenced for Women’s services and will be finalised in Q3. Again the RCOG recommendations will be considered as part of the longer term strategy development.
Clinical risk management on-going Green Achieved Women’s Services has been retained as a pan North Wales
69
Service, led by a Head of Midwifery with a team of 3 Clinical Directors, overall Medical Lead, Senior Clinical Lead Managers and a designated Exec Lead, to maintain continuity in monitoring the governance arrangements and to drive the improvements required for a service in special measures. The Clinical Leadership Structure and staffing on all 3 sites continue to reflect the Workforce Governance standards recommended in the RCOG/RCM Safer Childbirth Report. The Clinical Leadership Team on site in YGC has been further supported by the appointment of a new Clinical Lead for the Inpatient Area and an interim Midwifery Labour Ward Lead. A Consultant Midwife appointed to the clinical team will support and promote the normality agenda in North Wales. Commenced in post in Q2 - (22/8/16).
Locally the service is monitored on a 4 hourly basis using specific KPIs introduced to monitor staffing, safety and capacity within maternity. This daily reporting informs a weekly dashboard which is presented to WG as part of the Special Measures Monitoring on a fortnightly basis.
Performance against the national maternity outcome measures and key performance indicators are monitored locally at Women’s QSE & Board and submitted for inclusion to the national dashboard monthly. Monthly Exception Reporting is escalated to the Board’s QSE Committee specifically in relation to c-section rates and low birth weight rates. Partnership working with Bangor AEI, LSA & RCM (Wales) as part of a strategic plan to improve the learning and care environment is ongoing. An Action plan was presented to the
70
NMC and WG as evidence of the progress achieved to date. A meeting was held between AEI and Service, and a joint decision was made to return midwifery students in Q2 - 5/9/2016. An External OD Company has been commissioned to support the plan to improve the culture and multidisciplinary team working within maternity services focusing initially on the YGC site. Communication and diagnostic phase of the programme commenced in July 2016. An OD Development Plan will be presented to the Executives in Q3 – (November 2016).
Maternity standards performance reviewed and reported Green Achieved. The service will be presenting its performance data and improvement plans for Q1 and Q2 to WG Maternity Performance Board in Q3 – (21st, November 2016). NMC Follow Up Review of the LSA in Wales and Statutory Supervision in BCUHB completed – verbal feedback was positive. Written Report is outstanding. The LSA Annual Audit Review was undertaken on 21st and 22nd September – Q2. Preliminary feedback positive with all Rules and Standards Met.
Written Report will be made available in Q3 (December 2016).
71
Services for Children and Young People - Q1 Actions Carried Forward
Children and Young Peoples’
Services
Strategic Lead: Area Director
(Centre)
Q1
RAG
Status
Q1 Exception Report Q2
RAG
Status
Q2 Exception Report
Implications of Healthy Child Wales Programme fully reviewed and potential phasing of implementation agreed
Amber Healthy Child Programme has not been
formally launched in Wales, however
preparatory work already in place.
Clinical Service Managers have
identified gaps in workforce and plans
will be developed in accordance with
national programme.
Amber Partially achieved. Programme launched 1st October, Impact assessment complete (further detail available)
We are still waiting the FRAIT and the acuity tool to utilize with each caseload, which will take into consideration if they are low, medium or high need and therefore give us a realistic total per caseload.
The programme is dependent upon
Child Health Departments systems
being updated so that scheduling of
appointments for week commencing 3
Oct 2016 can take place.
Q2 Actions Children and Young Peoples’ Services
Children and Young Peoples’ Services
Strategic Lead :Area Director (Centre)
Q2 RAG
Status
Q2 Exception Report
Health Visitor caseload assessed and reduction plan
developed
Green Achieved. Health Visitor caseload assessed and reduction plan
developed. Recruitment of Health Visitors commenced
Additional hours given to current Health Visitors to reduce the
72
caseload sizes amounting to 2.3 wte. In total 29.5 wte is
required,
West - a further 5.76wte
Centre – a further 8.74wte
East – a further 13 wte
Peri-natal mental health training implemented for Health
visitors
Green Achieved. Peri-natal mental health training has been
implemented for Health visitors (from Oct – March).
New record training and raising HCWP awareness sessions
completed
Implementation of new CAMHS roles commenced Green Achieved. Implementation of new CAMHS roles has
commenced and appointments made to date as follows:-
Posts appointed Vacancies
West Admin Band 3 1.64wte Paediatrician 0.27wte
Band 6 Nurse 0.78wte
Band 6 Nurse 0.30wte
Psychology 8A 0.30wte
Consultant
Psychiatry 0.40wte
Admin Band 3
0.35wte
Psychologist
0.40wte
S< 0.33wte
OT 0.13wte
Nursing 0.53wte
Band 8A Family
Therapist 1.00wte
Central Band 6 nurse 2 WTE Consultant

73
(start dates 10th October)
Psychology 8A 1WTE
combined additional
resource to 1 post
Psychiatry 1.00wte
Paediatrician
0.30wte
S< 0.37wte
OT 0.15wte
Nursing 0.59wte
Band 8A Family
Therapist 1.00wte
East Admin Band 3 3.30wte
Psychologist 0.66wte
Paediatrician
0.44wte
S< 0.55wte
OT 0.22wte
Recruitment has been difficult due to the decreasing pool of
practitioners available with CAMHS experience. 5 psychiatrists
required, advertised twice without success, two locums have
been appointed.
Clinical psychologists, particularly at the newly qualified level are
difficult to recruit. The psychological therapy posts have been
delayed in WOD re job evaluation delaying recruitment of the
systemic family therapy and child psychotherapy which are new
posts with the new monies.
Implementation of neuro-developmental pathway in Green Achieved.

74
community paediatrics commenced Implementation of neuro-developmental pathway in community
paediatrics has commenced.
The pathway has been partially implemented – the gateway is
no-longer a mental health assessment, however recruitment of
community paediatricians is delaying full implementation of the
pathway.
Speech and Language therapy and occupational therapy staffing
recruitment has commenced. Psychology and support staff
vacancies to be advertised. Training for community
paediatricians regarding ASD/ADHD awareness has been
prepared and will be delivered October & November 2016.
Current waiting list reduction strategies including additional
assessment sessions are being arranged. Training and
information sharing for referrers to be prepared and delivered
December 2016/ January 2017
Recruitment of additional staff for epilepsy support Green Achieved
Central Area recruited and appointed to vacancy, all Areas now
have equity of resource.
Additional diabetic support services introduced Amber Partially achieved. Recruitment of diabetic nurses, psychology,
dietetics commenced. Parents now regularly attend a working
group to ensure the service moves forward and are actively
involved in service design.
Community CAMHS outreach expanded to 7 day service Amber Partially achieved . 7 days achieved in East, 6 days in West and
Central due to recruitment difficulties
The regional KITE outreach Tier 4 service has also recruited to
give additional cover for high risk cases over the weekend and
evenings, they have also established link practitioners who are
working with the areas.
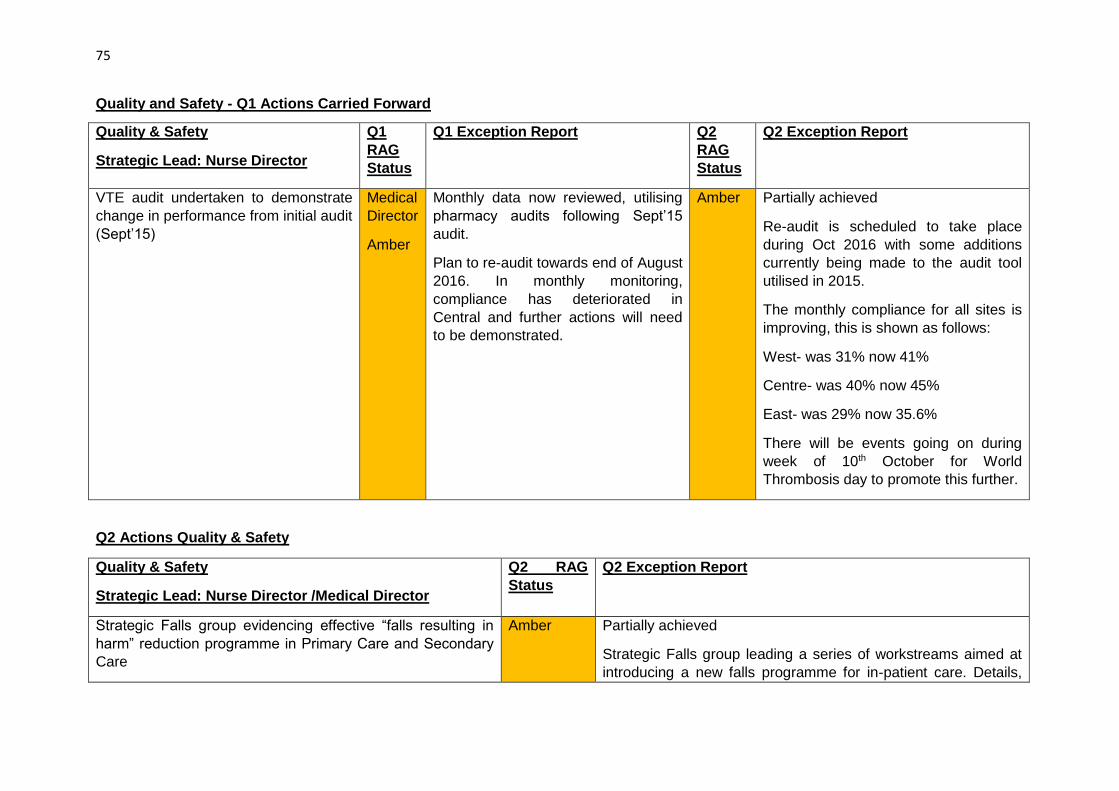
75
Quality and Safety - Q1 Actions Carried Forward
Quality & Safety
Strategic Lead: Nurse Director
Q1
RAG
Status
Q1 Exception Report Q2
RAG
Status
Q2 Exception Report
VTE audit undertaken to demonstrate
change in performance from initial audit
(Sept’15)
Medical
Director
Amber
Monthly data now reviewed, utilising
pharmacy audits following Sept’15
audit.
Plan to re-audit towards end of August
2016. In monthly monitoring,
compliance has deteriorated in
Central and further actions will need
to be demonstrated.
Amber Partially achieved
Re-audit is scheduled to take place
during Oct 2016 with some additions
currently being made to the audit tool
utilised in 2015.
The monthly compliance for all sites is
improving, this is shown as follows:
West- was 31% now 41%
Centre- was 40% now 45%
East- was 29% now 35.6%
There will be events going on during
week of 10th October for World
Thrombosis day to promote this further.
Q2 Actions Quality & Safety
Quality & Safety
Strategic Lead: Nurse Director /Medical Director
Q2 RAG
Status
Q2 Exception Report
Strategic Falls group evidencing effective “falls resulting in
harm” reduction programme in Primary Care and Secondary
Care
Amber Partially achieved
Strategic Falls group leading a series of workstreams aimed at
introducing a new falls programme for in-patient care. Details,
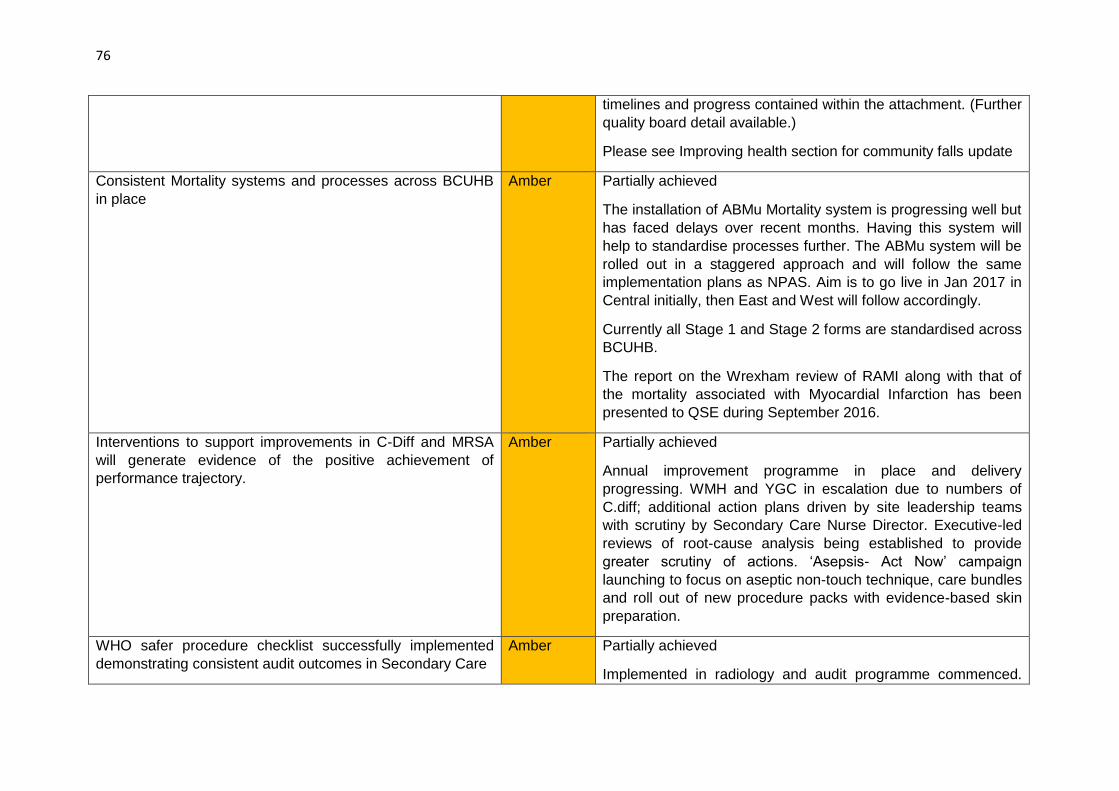
76
timelines and progress contained within the attachment. (Further
quality board detail available.)
Please see Improving health section for community falls update
Consistent Mortality systems and processes across BCUHB
in place
Amber Partially achieved
The installation of ABMu Mortality system is progressing well but
has faced delays over recent months. Having this system will
help to standardise processes further. The ABMu system will be
rolled out in a staggered approach and will follow the same
implementation plans as NPAS. Aim is to go live in Jan 2017 in
Central initially, then East and West will follow accordingly.
Currently all Stage 1 and Stage 2 forms are standardised across
BCUHB.
The report on the Wrexham review of RAMI along with that of
the mortality associated with Myocardial Infarction has been
presented to QSE during September 2016.
Interventions to support improvements in C-Diff and MRSA
will generate evidence of the positive achievement of
performance trajectory.
Amber Partially achieved
Annual improvement programme in place and delivery
progressing. WMH and YGC in escalation due to numbers of
C.diff; additional action plans driven by site leadership teams
with scrutiny by Secondary Care Nurse Director. Executive-led
reviews of root-cause analysis being established to provide
greater scrutiny of actions. ‘Asepsis- Act Now’ campaign
launching to focus on aseptic non-touch technique, care bundles
and roll out of new procedure packs with evidence-based skin
preparation.
WHO safer procedure checklist successfully implemented
demonstrating consistent audit outcomes in Secondary Care
Amber Partially achieved
Implemented in radiology and audit programme commenced.
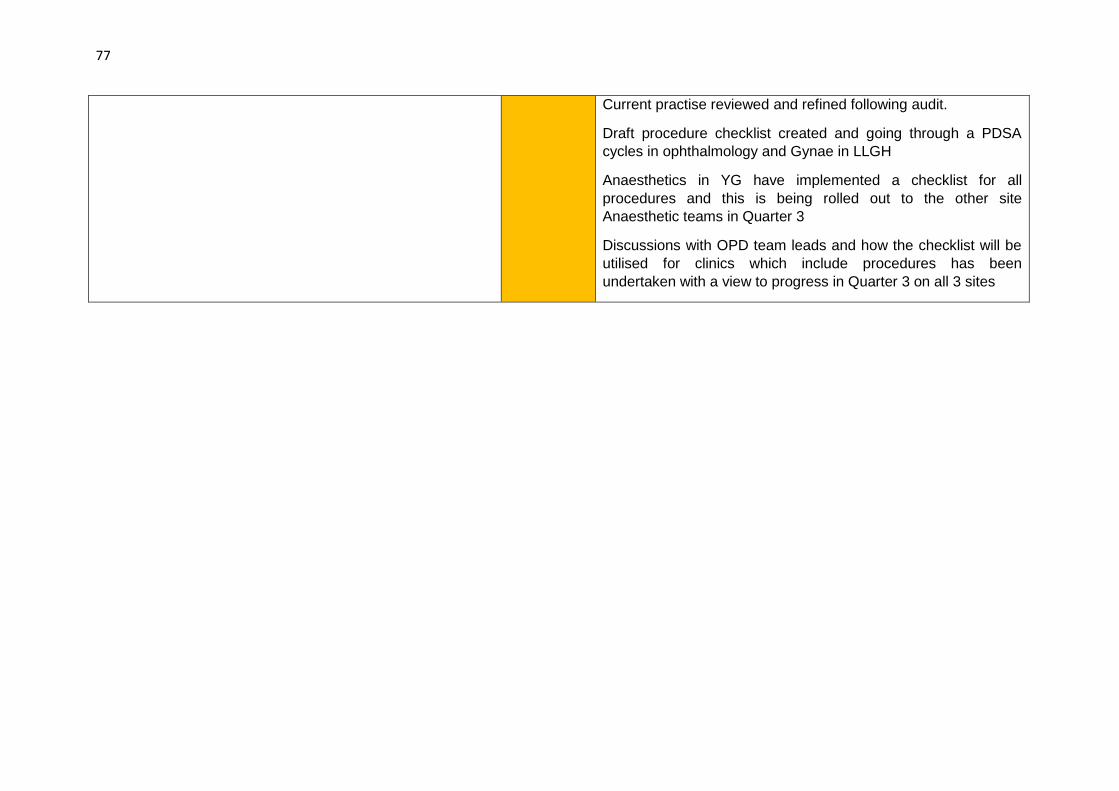
77
Current practise reviewed and refined following audit.
Draft procedure checklist created and going through a PDSA
cycles in ophthalmology and Gynae in LLGH
Anaesthetics in YG have implemented a checklist for all
procedures and this is being rolled out to the other site
Anaesthetic teams in Quarter 3
Discussions with OPD team leads and how the checklist will be
utilised for clinics which include procedures has been
undertaken with a view to progress in Quarter 3 on all 3 sites

78
Engagement - Q1 Actions Carried Forward
Engagement
Strategic Lead: Corporate Services
Director
Q1
RAG
Status
Q1 Exception Report Q2 RAG
Status
Q2 Exception Report
Public involvement scheme launched Amber This has been completed but is
undergoing testing and feedback on
functionality prior to formal launch.
We are on target however to launch
the scheme in Q2
Green Achieved. The Involvement Scheme was
launched on 14 August
www.bcugetinvolved.wales/
www.pbccymrydrhan.cymru and over 250
individuals or groups have registered to
join the scheme in the first month. All
have been sent a BCUHB newsletter.
We are encouraging more people to sign
up at the public events we are attending
across North Wales. We are also asking
partners to spread the word and promote
the site via their digital channels.
Review of approach to survey of public
perceptions and levels of influence and
involvement undertaken
Amber A light touch review has been
undertaken of the questions and
outcome measures we want to
address from public surveys. Due to
fact that there are a number of
Regional and County surveys being
undertaken as part of the population
needs assessment during this quarter
and Q2 there is a danger of
communities experiencing “survey
fatigue”. It has been decided
therefore that our public survey will be
delivered in Q3. Welsh Government
has agreed this revised timeframe.
Green Achieved
In relation to longer term monitoring of
public perceptions, we are working with
the Consultation Institute and Welsh
Government to launch a national pilot
project around measuring the impact of
continuous engagement and the impact
of specific activities on public views.
Launch expected in early January 2017

79
Q2 Actions Engagement
Engagement
Strategic Lead: Corporate Services Director
Q2 RAG
Status
Q2 Exception Report
Engagement website created to promote work and
involvement opportunities
Green Achieved – see above
Community engagements meetings established in each Area
– 3 meetings a quarter
Green Achieved. Engagement networks have been established by the
Engagement Officers in each area team with almost 100
meetings attended in the last quarter.
Active communications of service strategy work established
through website, social media etc
Green Achieved. There is a dedicated communications and
engagement plan for the development of the Living Healthier,
Staying Well strategy which covers a broad range of
communications channels including information for staff
(including meetings, Team Brief, intranet) and the wider public
(bilingual flyer, a dedicated section on the Get Involved website,
social media activity and discussion at meetings with
stakeholders and partners)
Database of contacts expanded to participate in engagement
activity
Green Achieved -As above
Public perception survey conducted Green Achieved. A direct public perception survey is being undertaken
by Welsh Government as part of the “Delivering a Healthier
North Wales” programme.

80
Strategy and Service Planning - Q1 Actions Carried Forward
Strategic & Service Planning
Strategic lead: Director of Strategy
Q1
RAG
Status
Q1 Exception Report Q2
RAG
Status
Q2 Exception Report
Lessons learnt clearly evidenced Amber Evidenced in a number of areas (eg Infection Control, development of strategic learning groups for falls and HAPUs) but not yet embedded across all services. Information flow and reporting arrangements approved by QSE. Further work being undertaken to implement fully including the development of a learning framework in Q2.
Amber Partially Achieved Evidenced in a number of areas (eg Infection Control, development of strategic learning groups for falls and HAPUs) but not yet embedded across all services. Learning workshop held with over 80 participants Look-back exercise undertaken with WMH; to be repeated for other acute sites in Q3 Information flow and reporting arrangements approved by QSE. Further work being undertaken to implement fully including the development of a learning framework. Divisions mapping their frameworks Roles of QAE and QSE under discussion Learning template included in revised concerns procedure, intranet page developed and a quarterly newsletter in
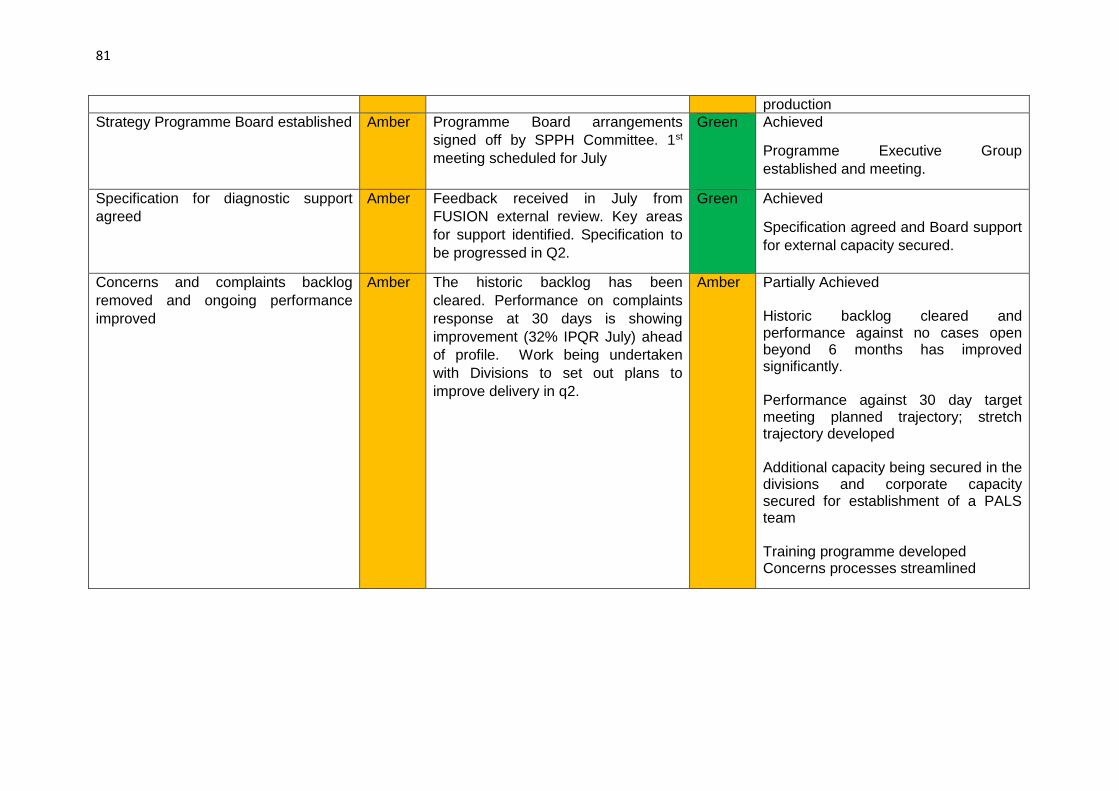
81
production
Strategy Programme Board established Amber Programme Board arrangements
signed off by SPPH Committee. 1st
meeting scheduled for July
Green Achieved
Programme Executive Group
established and meeting.
Specification for diagnostic support
agreed
Amber Feedback received in July from
FUSION external review. Key areas
for support identified. Specification to
be progressed in Q2.
Green Achieved
Specification agreed and Board support
for external capacity secured.
Concerns and complaints backlog
removed and ongoing performance
improved
Amber The historic backlog has been
cleared. Performance on complaints
response at 30 days is showing
improvement (32% IPQR July) ahead
of profile. Work being undertaken
with Divisions to set out plans to
improve delivery in q2.
Amber Partially Achieved Historic backlog cleared and performance against no cases open beyond 6 months has improved significantly. Performance against 30 day target meeting planned trajectory; stretch trajectory developed
Additional capacity being secured in the divisions and corporate capacity secured for establishment of a PALS team Training programme developed Concerns processes streamlined

82
Q2 Actions Strategy and Service Planning
Strategy and Service Planning
Strategic Lead: Director of Strategy
Q2 RAG
Status
Q2 Exception Report
Support for diagnostic phase in place Amber Partially Achieved
Specification is agreed and procurement commenced. Capacity
will be in place before the end of November.
Clinical workstreams established Amber Partially Achieved
Clinical workstreams in place for Mental Health, Orthopaedics,
Urology. Further streams to be established in Q3
Standards and evidence base defined Amber Partially Achieved
Timeline for strategy development amended in line with
discussions with Welsh Government. Revised approach agreed
by Board in July. Baseline assessment to be completed in Q3.
Workforce and financial modelling commenced Amber Partially Achieved
Workstreams deferred in line with revised timeline. Engagement
period extended in Autumn. Baseline assessment to be
completed in Q3 with modelling commencing in Q4.
Programme Business Case structure defined Amber Partially Achieved
Timeline for strategy development amended in line with
discussions with Welsh Government. Revised approach agreed
by Board in July
Mental health external expert review findings finalised Amber Partially Achieved
Findings will be reported on 28th October
83
Engagement method and model implemented Green Achieved
Engagement continues in line with revised programme plan
Progress against Annual Plan priorities reported Green Achieved
Qtr 1 reported in July to SPPH Committee. Qtr 2 to report in
November
Approach to 2017/18 planning defined
Green Achieved
Plan development timeline and approach agreed by Executive
Management Group and Executive Team. Reported to SPPH
10th October
84
Leadership and Governance –Q1 Actions Carried Forward
Leadership & Governance
Strategic Lead: Board Secretary
Q1 RAG
Status
Q1 Exception Report Q2
RAG
Status
Q2 Exception Report
Quality and safety operational arrangements in place to identify risk issues and respond urgently with key actions
Amber A new system of ward handover
safety briefings, shift by shift, has
been put in place in acute hospitals
together with arrangements for
auditing compliance and
effectiveness. This feeds into a twice
daily reporting system from each
hospital site. A programme of revised
senior leadership safety walkrounds
has also been established. The
walkrounds are supported by prompt
cards to help individuals completing
the visits to focus on patient safety
and quality. All data are then
triangulated within a software
programme together with information
arising from Health & Care Standards
monitoring. An example of how the
organisation has responded to
emerging risks is the establishment of
strategic groups looking at falls and
pressure damage.
Quality & Safety Groups have been
established in operational structures.
Their purpose is to monitor quality,
review clinical risk profile, review
Amber Partially Achieved
There is also more to be done to
improve reporting from ward to Board
around safety issues, to ensure that
lessons are learnt, that there is
adherence to the procedures that have
been put in place, and that escalation is
taking place. Some disconnect from
ward to Board still exists.

85
concerns and SUIs and identify
learning. Reporting is through the
Performance and Accountability
regime now in place.
The Quality Assurance Executive
Group has an overview of clinical risks
and standards and the Quality
Improvement Strategy. It monitors
trends and directs action as
necessary to address emerging
issues.
Template reporting on themes and
trends is being developed to inform
the Quality and Safety agenda.
A safehaven system has been
established and publicised through
the Office of the Medical Director to
support the Health Board’s whistle
blowing arrangements (to be reviewed
for effectiveness by Ann Lloyd).
Further work is required in respect of
the new ward handover system, which
needs to be rolled out into community
settings and monitored/tested for
effectiveness.

86
Q2 Actions Leadership & Governance
Leadership & Governance
Strategic Lead: Board Secretary
Q2 RAG
Status
Q2 Except Report
Further implementation of organisational structure
progressed
Green Achieved. The agreed organisational structure has been published
widely, with sufficient detail to give clarity on senior roles and
responsibilities.
Performance and accountability arrangements in place
and operating effectively
Green Achieved. The Health Board has established a new operational model
with clear lines of accountability at all levels. There are three Area Team,
each coterminous with two local authorities responsible for primary and
community services. A Secondary Care Director has been appointed and
has responsibility for each main hospital site. Each site is led by a
Hospital Management Team. A holding structure has been put in place
for the Mental Health & Learning Disabilities Division. The Health Board
is working to communicate more widely its revised operational
management structure.
A revised performance management strategy was scrutinised by the
Finance & Performance Committee and approved by the Audit
Committee in September 2016. This document sets out the strategic
context, lines of accountability, performance management processes and
the key outcomes expected. It reflects the current operational
arrangements.
Demonstrable progress against WAO/HIW
recommendations evidenced
Amber Partially Achieved. An assimilation process has taken place to produce a
closedown report following the HIW/WAO follow-up review. HIW and
WAO will conduct a further joint review follow-up in early 2017 and the
Structured Assessment 2016 is now ongoing.
A position statement has been agreed between WAO and the Health
Board with regard to all outstanding recommendations, which have now
migrated and been incorporated into the Special Measures Action and

87
Progress Log. Detailed evidence of the progress being made is reported
to the public Board and Welsh Government separately.
Board development programme ongoing Green Achieved. The Board is engaged in an ongoing Board Development
Programme facilitated by Mrs Ann Lloyd as part of the special measures
arrangements. This has included a self-assessment against the Well-Led
Framework and a skills audit. Arrangements are in hand to secure a
provider to deliver the 2017 Board Development Programme.
In year, Board Development sessions have focused on the key priorities
agreed with Board members and Mrs Ann Lloyd as Independent Adviser
to the Health Board. These have included staff culture and engagement,
estates strategy, performance monitoring, public engagement strategy,
partnership governance, recruitment and mental health services.
Risk management approach implemented across the
organisation
Amber Partially Achieved. A revised Risk Management Strategy was approved
in April 2016 and a further revision was approved by the Audit Committee
in September. In addition the Board approved a move to a new reporting
approach involving combining the Board Assurance Framework with the
Corporate Risk Register, to produce a Corporate Risk & Assurance
Framework (CRAF). It is acknowledged that the implementation and
embedding of the overall risk management approach will take a longer
period of time.
Special measures assurance tracked by Board sub-
group
Green Achieved. The Special Measures Task & Finish Group meets monthly to
track progress. It provides monthly assurance reports to the Board and
oversees the production of the End of Phase reports for Welsh
Government. The Task & Finish Group has planned an additional ‘deep
dive’ day in October to scrutinise in detail the evidence of progress made
in key areas. This will inform the End of Phase 2 Report.

3.6 SPPH16/208 Annual Operational Plan 2017/18 and NHS Wales Planning Framework
1 SPPH16.208 AOP and NHS Wales Planning Framework_coversheet.docx
1
Strategy, Partnerships & Population Health Committee 24.11.16 Item SPPH16.208
To improve health and provide excellent care
Title: Annual Operational Plan 2017/18 and NHS Wales Planning Framework
Author: Mr John Darlington, Assistant Director – Corporate Planning
Responsible Director:
Mr Geoff Lang, Executive Director of Strategy
Public or In Committee
Public
Strategic Goals (Indicate how the subject matter of this paper supports the achievement of BCUHB’s strategic goals –tick all that apply)
1. Improve health and wellbeing for all and reduce health
inequalities
√
2. Work in partnership to design and deliver more care
closer to home
√
3. Improve the safety and outcomes of care to match the
NHS’ best
√
4. Respect individuals and maintain dignity in care √
5. Listen to and learn from the experiences of individuals √
6. Use resources wisely, transforming services through
innovation and research
√
7. Support, train and develop our staff to excel. √
Approval / Scrutiny Route
The Committee has previously approved the planning guidance and timescale for the development of the Annual Operational Plan
Purpose: The purpose of this report is –
to ensure that the planning approach within the Health Board is aligned to and meets the expectations of National Planning Framework as set out in (WHC/ 2016/044).
to provide an update on progress against our agreed programme for developing the 2017/18 Annual Operational Plan.
Significant issues and risks
The Health Board’s local planning principles document was presented to the Committee on 10th October and agreed. The Health Board received the finalised National Planning Framework (WHC/ 2016/044) in October which sets out the expectations for organisations across NHS Wales. The Planning Framework sets out clearly the expectations of Welsh Government in relation to the scope and coverage of Health Board plans.
2
The Health Board continues to operate in the context of special measures, within which Welsh Government have set out clear expectations of the Health Board to produce an Annual Operational Plan for 2017/18 as a step towards the development of a full IMTP in March 2018. Within this expectation it is clear that the Health Board’s plan will need to follow the overall structure that applies to the development of IMTPs. The development of an annual operational plan is instrumental to delivering actions to improve health and wellbeing as well as improved services to meet the changing needs of the population of North Wales. The approach to this previously agreed by the Committee is in line with the requirements as set out by Welsh Government in the NHS Wales Planning Framework. Progress is being made against the key actions set out in the Board’s planning guidance document and this will need to be closely monitored over the coming weeks to ensure that the core content and priorities for the plan is produced in time to enable the presentation of the draft Plan to the Board in January.
Special Measures Improvement Framework Theme/ Expectation addressed by this paper
The preparation of an Annual Operational Plan in 2017/18 is a requirement of Special Measures, leading to the development of a full Integrated Medium Term Plan in 2018.
Equality Impact Assessment
A full equality impact assessment will be undertaken on the operational plan as this develops. The Strategy & Planning Equality Scrutiny Group of the Health Board will provide support, scrutiny and challenge throughout the process.
Recommendation/ Action required by the Committee
The Committee is asked to:
note the requirements of NHS Planning Framework in terms of the expected content and format of the Board’s plan
note the alignment between the planning guidance agreed by the Committee and the National Framework
note progress being made in developing the plan for 2017/18.
Disclosure: Betsi Cadwaladr University Health Board is the operational name of Betsi Cadwaladr University Local Health Board
Committee Coversheet v10 June 2016
2 SPPH16.208 AOP and NHS Wales Planning Framework.doc
1
Annual Operational Plan 2017/18 and NHS Wales Planning Framework
1. Purpose of report
The purpose of this report is –
to ensure that the planning approach within the Health Board is aligned to and meets the expectations of National Planning Framework as set out in (WHC/ 2016/044).
to provide an update on progress against our agreed programme for developing the 2017/18 Annual Operational Plan.
2. Introduction
The Health Board’s local planning principles document was presented to the Committee on 10th October and agreed. This identified the approach to the development of our Annual Operational Plan for 2017/18 and included the key local requirements and timetable. At the time that document was prepared the National Planning Framework had not been published. This paper has therefore been prepared to: 1. Appraise the Strategy, Partnerships & Population Health (SPPH) Committee
of the national planning requirements. 2. Ensure that national requirements are reflected within our local planning
arrangements. 3. Provide an update to SPPH Committee of progress against our local timetable NHS Wales Planning Framework Requirements The Health Board received the finalised National Planning Framework (WHC/ 2016/044) in October which sets out the expectations for organisations across NHS Wales. The framework is attached in Appendix 1. The NHS Wales Planning Framework seeks to build on and consolidate progress made in 2016/17. There are also some key changes in the Framework this year, for example the need to respond to the requirements of the Wellbeing of Future Generations Act, which will require a new way of working across organisations and public sector bodies. The National Planning Framework covers the period 2017 to 2020 and is intended to guide the development of Integrated Medium Term Plans (IMTP). The Planning Framework sets out clearly the expectations of Welsh Government in relation to the scope and coverage of Health Board plans. This is largely consistent with previous years but there are a number of key areas which are worthy of note –
The Guidance explicitly references the changing legal context in particular the effects of the Wellbeing of Future Generations Act and the Social Services and Wellbeing Act; plans will be expected to fully reflect this context
The Guidance helpfully clarifies the relationship between the longer term strategies of Boards and the IMTP. This helpfully supports the approach the

2
Board has initiated in terms of the development of its longer term strategy Living Healthier, Staying Well
There is an increasing alignment between the NHS Delivery Framework, which is the means by which Welsh Government assesses organisational performance and the longer term planning priorities particularly in relation to public health outcome indicators.
The need for stand alone plans for key disease specific groups along with separate reporting processes has been amended. These will now form part of the Board’s overall plan.
There is a clear structure set out for the Plan (section 8) which will allow Welsh Government to look across the NHS in Wales and identify overall actions and expectations of improvement.
Developing the Health Board’s Plan The Health Board continues to operate in the context of special measures, within which Welsh Government have set out clear expectations of the Health Board to produce an Annual Operational Plan for 2017/18 as a step towards the development of a full IMTP in March 2018. Within this expectation it is clear that the Health Board’s plan will need to follow the overall structure that applies to the development of IMTPs. The requirements that are contained in the Framework align with the agreed local planning principles and service transformational group themes which have been established to underpin the development of the Board’s operational plan. The core elements align in the following areas -
Improving health and reducing health inequalities
Primary care
Community services
Children
Maternity services
Mental health and learning disabilities
Planned care
Unscheduled care. The Framework also identifies older people and major health conditions as key areas for planning. Our approach will therefore need to identify and reflect these areas appropriately. Developing our Plan – Progress to date
Action Timescale
The finalised Planning Principles and timetable for 2017/18 was issued to all divisions
11th October
Operational leads and planning links identified for all Together for Health Major Conditions delivery plans to ensure these are linked
25th October

3
into operational plans.
First draft capital priorities have been received from all divisions including estates, medical devices and IM&T.
31st October
Final planning and commissioning statement of intentions issued
4th November
Divisional planning arrangements established and in place e.g. local meetings and workshops established to identify priorities for improvement. E.g. Central Area Team workshop on 17th November Secondary care workshop held on 28th October. Additional planning support secured to support the development of secondary care service and departmental plans.
October/ November
Organisational wide Planning and Service Development Group established to support plan co-ordination - fortnightly meetings arranged involving corporate and divisional teams
15th November onwards
In addition to the planning intentions, performance profiles for the year ahead, aligned to the new Delivery Framework are being developed. These will be incorporated within Divisional plans. Work to pull together Divisional plans into the service themes identified in the National Framework will be progressed through the Transformation Groups. An initial assessment of priority actions profiled over the coming year was scheduled for production by mid November. The key priorities for the year ahead have been identified through the planning intentions document, however the profiling of actions has not progressed. This will now take place early in December in order that this work can be presented to the Committee in a workshop session on 22nd December. This will enable feedback from the Committee to be reflected in the preparation of the draft plan which will be presented to the Board in January.
4. Assessment of risk and key impacts
The potential consequences of failure to develop a comprehensive plan for the Health Board are significant. This is a key measure within the Special Measures Improvement Framework.
5. Equality Impact Assessment
A full equality impact assessment will be undertaken on the operational plan as this develops. The Strategy & Planning Equality Scrutiny Group of the Health Board will provide support, scrutiny and challenge throughout the process.
6. Conclusions / Next Steps
The development of an annual operational plan is instrumental to delivering actions to improve health and wellbeing as well as improved services to meet the changing needs of the population of North Wales. The approach to this previously agreed by

4
the Committee is in line with the requirements as set out by Welsh Government in the NHS Wales Planning Framework. Progress is being made against the key actions set out in the Board’s planning guidance document and this will need to be closely monitored over the coming weeks to ensure that the core content and priorities for the plan is produced in time to enable the presentation of the draft Plan to the Board in January.
7. Recommendations
The Committee is asked to:
note the requirements of NHS Planning Framework in terms of the expected content and format of the Board’s plan
note the alignment between the planning guidance agreed by the Committee and the National Framework
note progress being made in developing the plan for 2017/18.
3 SPPH16.208 NHS Wales Planning Framework_appendix 1.pdf
1
NHS Wales Planning Framework
2017/20
2
Contents Message from the Cabinet Secretary Message from the Chief Executive of the NHS in Wales
1. Introduction
2. Policy context
3. Strategy
4. IMTP
5. Priorities for 2017/20
6. Process and timetable
7. Significant service change
8. IMTP Structure
9. Summary
Appendices Appendix A: OECD report Appendix B: NHS Finance (Wales) Act 2014 Appendix C: Mandatory templates Appendix D: Good Governance Institute maturity matrix

3
Message from the Cabinet Secretary
I am delighted to be introducing the NHS Wales Planning Framework for 2017/20. It
gives me an opportunity to record my thanks to you and the staff in your
organisations. We are fortunate in NHS Wales to have professional, dedicated and
hard-working staff who are committed to providing the best possible care for our
patients and I want to see that good work continue.
We have published our Programme for Government and the First Minister is clear
that our focus must be on delivering real improvements to the population of Wales.
We want a Wales that is healthy and active. To achieve this, we have committed to
recruiting and training more staff, reducing waiting times and working with parents
and schools to give every child a healthy start in life. We need to reduce health
inequalities and listen to, and act on, the voice of our citizens, in the spirit of prudent
healthcare, so that together we can plan and provide the care that people deserve.
All this needs to be undertaken in a challenging financial climate. This year, there
will be an increasing focus on efficiencies, ensuring that money is put to the best use
possible.
The Well-being of Future Generations Act sets a new expectation of integrated
planning based on population needs, going beyond the traditional health boundaries,
into areas such as housing and education. To achieve this, we need to continue to
develop and strengthen relationships with key partners, third sector, social services
and others involved in the provision of high quality care for our patients. This will
mean different ways of working, providing innovative services that support the patient
along their pathway.
Ultimately plans are only as good as the services they deliver: and these plans need
to deliver with pace and purpose, working seamlessly across health and partner
provider boundaries. I want to see organisations working together more to resolve
strategic delivery issues that cross boundaries, pooling skills and resources to
achieve mutual benefit. There is an expectation that plans will show progress
against strategic and government priorities. I want organisations to continue to
challenge themselves so that we can ensure that we are delivering ever-improving
services for people in Wales.
This year, for the first time, there is a requirement that all organisations develop long
term strategies which will set the direction of travel for your IMTPs.
Planning across the health service in Wales continues to develop and progress over
the last three years since the NHS Finance (Wales) Act 2014 was introduced. Next
year, I would like to see more organisations achieving approval. I have tasked my
officials in Welsh Government to work closely with all NHS organisations to realise
this aim.

4
I look forward to working with you to tackle the challenges that lie ahead of us next
year, and to seeing real improvements delivered to our population in 2017.
Vaughan Gething AM
Cabinet Secretary for Health, Wellbeing and Sport
5
Message from the Chief Executive of NHS Wales
As we move into a new government we can expect intense interest and scrutiny in
health services in Wales. This will inevitably bring changes, challenges and
opportunities.
The new Programme for Government will continue to shape our short, medium and
long term goals and you will want to reflect on this now published document. As the
Wellbeing of Future Generations comes into force it extends integrated planning
beyond traditional health boundaries, and changes the way that we work with our
partner organisations, third sector and social services to improve health care across
the life course.
Earlier this year, the OECD report acknowledged the progress you are making
through our planned approach, and highlighted opportunities for further development
that we can build on going forward. This remains a key report for our system to
respond to, not least to meet our ambition for quality and excellence.
Some of these changes present challenges but also significant opportunities over the
next three, five, ten years and longer. This year we have recognised the maturing
process around NHS planning by separating the long term strategy from the 3 year
cycle of IMTPs. I realise that not all of you will have a developed long term strategy
yet and officials will work with you to develop this within an appropriate time scale
that we will agree with individual organisations. Further to the publication of the
Programme for Government, we will be producing the next vision and strategy for
NHS Wales to move beyond Together for Health. This will be inextricably linked to
the commitment for a Parliamentary Review. We will keep you informed on the
timetable for the next NHS Wales strategy as this progresses.
I have also had the chance to meet with many of you, and listen to your views on
how we can continue to improve the planning system.
You wanted greater alignment with the IMTPs and the Delivery Framework. This will
be a gradual process as the Delivery Framework changes, but we are working
towards aligning this through the use of public health outcomes.
You said you wanted clear information about the Well-being of Future Generations
Act. We have included a section specifically on this, as well as an enabler to show
what good looks like. You also asked for a clearer steer from government on the
content of the IMTPs; so we are looking for some more standardised information to
enable us to build a clear picture of how services are developing across Wales. We
have therefore set out a proposed structure for your IMTP in section 8, including a
suggested page limit.
Plan development is only the first step in the integrated planning journey.
Implementing the plans will take strong leadership as well as the development of a
learning culture within and across organisational boundaries, so that we embrace
6
change as a vehicle to service improvement. Developing leadership at all levels in
our organisations is key to this aim. Building trust and relationships across health
board and wider boundaries will enhance the progress we continue to make and help
address some of the strategic challenges with the pace and purpose needed to
deliver a quality driven NHS in Wales. To support this, I am interested in proposals to
strengthen planning skills. I have been particularly pleased to see that the bi-annual
learning and peer review events now have a firm place in your calendars. I would
also encourage as many people as possible to take advantage of the learning
programme, and particularly the demand and capacity training from the Delivery Unit,
to develop these key skills across the NHS
I know that you, your teams and all the staff in your organisations continue to work
hard to improve health services for citizens and communities. This year has been
particularly challenging with the first of the rolling three year financial and planning
cycles providing a significant marker in terms of governance and transitions for the
NHS in Wales. Our jobs are not easy, but I am confident that with your ongoing
commitment that we can achieve our ambition of improved health outcomes for our
population.
Andrew Goodall
Chief Executive of NHS Wales
7
This section places Integrated Medium Term Plans (IMTPs) within the strategic context. The Welsh NHS Planning, rather than the market, is the basis of the healthcare system in Wales. Health boards, NHS trusts and their partners are required to work together to secure and deliver services for their populations, collaborating with partners at various levels to assess population need and to plan and deliver services, through the local health board, public services boards and 64 primary care clusters. They are expected to have a long-term view and to be clear about the actions they will take in the more immediate future to deliver high quality, accessible and sustainable services within the national policy context. The OECD report published in 2016 acknowledged the progress that is being made through this planned approach. (see Appendix A). It also highlighted opportunities for further development of our system and made four main recommendations:
Secure accountability, drive standards and promote innovation
Put primary care front and centre as a force for dynamic system change
Make Wales a data-driven system
Do more to promote the patient voice
The report highlighted the need to strike the right balance between local freedom, innovation and sensitivity to population needs, and achievement of core standards which must be consistent and centrally driven. This guidance aims to take the next step towards achieving the right balance within the Welsh system. Strategic Vision
Local health boards in Wales have a duty under their directed functions, flowing from sections 1-3 of NHS Wales Act 2006, to continue the promotion in Wales of a comprehensive health service designed to secure improvements in the physical and mental health of the people of Wales. This means that local health boards are under a duty to consider the broader picture and consider how in exercising their functions they can contribute to the improvement of the health service across Wales. Whilst local health boards are responsible for the health of their resident populations they must also take account of these wider statutory responsibilities in planning and delivering health services. All NHS organisations should have a strategy, approved by their Board, which clearly sets out their long-term vision for how they will meet the needs of the communities they serve.
1. INTRODUCTION

8
The long term strategy of each organisation is critical in setting the direction of travel and in providing the context within which key strategic decisions about the shape of services and the use of resources can be taken. These include decisions about service models, pathways, workforce planning, finance and infrastructure investment.
Robust wellbeing and population needs assessments are essential to inform strategies, and are a requirement of the Wellbeing of Future Generations and the Social Services and Wellbeing Acts. NHS organisations must work closely with their Public Services Boards, Regional Partnership Boards and the communities they serve, as they develop their needs assessment, gap analysis and responses to inform their strategic plans. NHS organisations are expected to collaborate in addressing strategic delivery issues that impact on the delivery of services for patients, and are encouraged to explore strategic alliances to resolve consistent challenges. Plans should make clear where issues are beyond the scope of an individual organisation, and should clearly set out an agreed response at an all Wales, and / or regional and sub regional level. The collaborative arrangements across Wales should support the alignment of actions within individual organisational plans. In assessment of plans Welsh Government will expect there to be a clear read across to the agreements and actions to be taken by all organisations that have collective responsibility for delivery of the strategic intentions. Integrated Medium Term Plans
The introduction of Integrated Medium Term Plans (IMTPs) in 2014 signalled a move away from a focus on annual plans, towards a medium-term approach linked to organisational strategies. IMTPs should set out clearly what will be done over the next three year period in pursuit of the organisation’s longer-term strategic objectives and plans. Every organisation must have a more immediate plan setting out the actions it will take as it works towards its strategic objectives. A three-year focus allows organisations to set out clearly what they intend to do in a medium-term period and avoids the “stop/start” behaviours which can be associated with a focus on a single year. The IMTP should set out the actions organisations will take in pursuit of their long-term strategies, through measurable, clearly defined and resourced actions which address key areas of population health need, improve health outcomes and the quality of care, and ensure best value. This year’s Planning Framework is intended to:
provide guidance to organisations on developing both long-term strategies and medium-term plans (IMTPs)
provide strategic and policy context to the current planning round
describe the requirements on health boards and NHS trusts to comply and reflect the ambition of the Well-being of Future Generations (Wales) Act 2015 (WbFGA) and Social Services and Well-being (Wales) Act 2014 (SSWbA)
emphasise the importance of quality and the patient/user experience
9
set out the key deliverables required of NHS Wales
explain how delivery plans will be managed through the IMTP process
set out the timetable for submission and approval for 2017/18
describe the monitoring and escalation process associated with IMTPs.
Planning is a dynamic and continuous process and it is not expected that IMTPs will set out a fixed picture for the next three years. It is however important that they are sufficiently clear to provide confidence that the organisation understands its priorities, opportunities and challenges over the medium-term, and that the actions it will take are linked to its longer-term strategy.
The expectation is that IMTPs will set out clearly the detailed actions and deliverables for years one and two, and an outline of priorities and actions for year three.
There needs to be greater clarity about plans across the three year period if an organisation is seeking agreement to substantial commitments in years one and two which require financial support to be recovered in year three. Regional/All Wales Planning
NHS organisations must plan together where appropriate to ensure that high quality services are available to their residents, wherever these services are provided. It applies particularly, but not exclusively, to tertiary or specialist services. This includes services commissioned through WHSSC and EASC, and also service planning led by the NHS Collaborative.
NHS Support Organisations
A central tenet of healthcare in Wales is integration and co-operation between organisations. This is intended to share expertise, avoid duplication and ensure that we do things “once for Wales”.
The Welsh Health Shared Services Committee (WHSSC), the NHS Wales Shared Services Partnership (NWSSP), the Emergency Ambulance Services Committee (EASC) and NHS Wales Informatics Services (NWIS) support health boards and NHS trusts to deliver efficient and effective high quality services to patients/users. They bring expertise in fields such as commissioning for high cost specialist services, informatics, recruitment and payroll to organisations in Wales.
Although not a statutory requirement under the NHS Finance (Wales) Act 2014, these organisations should also produce three year plans, and develop their own long term strategies. Plans for these organisations need to be approved by their own relevant governing body or the joint committees formed from the NHS organisations that they support. The jointly agreed plans should then be incorporated into the statutory NHS organisations’ IMTPs for Board approval.
There is an expectation that the statutory NHS organisations which make up the relevant joint committees will require these support organisations to develop their plans in sufficient time to inform their own plans. This means that support

10
organisations will need to provide their plans to health boards and trusts earlier than in previous years. This timescale will be developed by the joint committees.
Engagement and Partnership
NHS organisations are expected to work closely with the communities they serve and their partner organisations as they develop their plans. Co-production is a central tenet of prudent healthcare, and a fundamental part of giving patients a voice in their healthcare. The Well-being of Future Generations Act which came into effect on 1 April 2016 requires NHS organisations 1 and other public bodies to act in accordance with the sustainable development principle and set and publish well-being objectives which are designed to maximise their contribution to the seven well-being goals. In addition, they are required to work collectively with partner organisations through public service boards to jointly contribute to improving the economic, social, environmental and cultural well-being of the local area. This Act strengthens the existing governance arrangements for improving the well-being of Wales. For health, the Act provides a platform from which public services can collectively tackle the long term challenges facing communities, such as health inequalities, poverty and climate change. An integrated and collaborative approach across the public services, and with other partners, is essential in the understanding of health and well-being. It must be understood that this is not just the absence of disease and treatment of illness. An integrated and collaborative approach also allows for a renewed focus on prevention and determining how different public services can help to tackle the wider determinants of health. The sustainable development principle also requires services to foster ways of working which are long term and citizen centred - maximising the benefits public services can offer to communities in pursuit of the well-being goals set out in the Well-being of Future Generations Act. Welsh Government will expect to see evidence in IMTPs of collaborative work and service integration shaped and informed by the joint response to the well-being assessments.
Planning Framework
This document supersedes the 2016/17 NHS Planning Framework and applies to health boards, NHS trusts and NHS support organisations. As the statutory and other duties differ for each type of organisation, there will be recognised differences in both approach and detailed content. Expectations will be discussed with individual organisations during preparation of IMTPs.
Financial Allocations Details of financial allocations will be provided in the Financial Allocations letter which will be published by 31st December. This letter will include details of the financial requirements associated with the duty to achieve a balanced budget over a three year period.
1 (1) While WAST is not formally subject to WbFGA it is expected to reflect the ambition of the Act and
delivery in the IMTP.

11
2. POLICY CONTEXT
Welsh Government has set out the policy context within which NHS organisations should work with their partners as they develop their future plans. This section outlines some of the key policy requirements. The overarching policy direction is set by “Taking Wales Forward”, the programme for government. Many other statements of policy will be familiar to the NHS and are not rehearsed in this framework. The Programme for Government, “Taking Wales Forward” clearly sets out four areas for development for Wales over the next five years. It sets out an ambition for Wales to be: Prosperous and Secure Healthy and Active Ambitious and Learning United and Connected From a health perspective, provision of health care will need to be clearly focused on:
primary care, ensuring that patients receive prompt, cost effective and high quality care as close to home as possible
the provision of timely care, reducing the time that patients wait before treatment
mental health, at all levels of care, and also within the workplace to ensure that we support our staff; and
improving integration between health and social services.
Plans need to demonstrate how they will deliver the key messages and aims within “Taking Wales Forward”.

12
The Well-being of Future Generations (Wales) Act 2015
The Well-being of Future Generations (Wales) Act (WbFGA) came into effect on 1 April 2016. It aims to improve the social, economic, environmental and cultural well-being of Wales. The act sets out seven well-being goals, and five ways of working in order to support the implementation of these goals:
Seven well-being goals for Wales Five ways of working
Long-term
Collaboration
Integration
Involvement
Prevention
Under the Act, each specified organisation has both an individual and a collective duty to set and publish objectives that are designed to maximise its contribution to the well-being goals, and to take all reasonable steps to meet these objectives. The Act also places an additional duty on specified public bodies, including health boards, to act jointly via public services boards to improve the well-being of their area by contributing to the achievement of the well-being goals. The Act provides for better decision making by ensuring that both individual organisations and public services boards take account of the long-term, help to prevent problems occurring or getting worse, take an integrated and collaborative approach, and consider and involve people of all ages (the “sustainable development principle”). Through the sustainable development principle, public bodies will need to make sure that when making their decisions they take into account the impact they could have on people living their lives in Wales in the future. This includes balancing short-term needs to safeguard the ability to meet long-term needs and acting to prevent problems getting worse or occurring in the first place. This means that the priorities that public bodies set (well-being objectives) must be designed to contribute to the seven well-being goals in the Act, and in delivering these priorities they must take into account the five key ways of working.
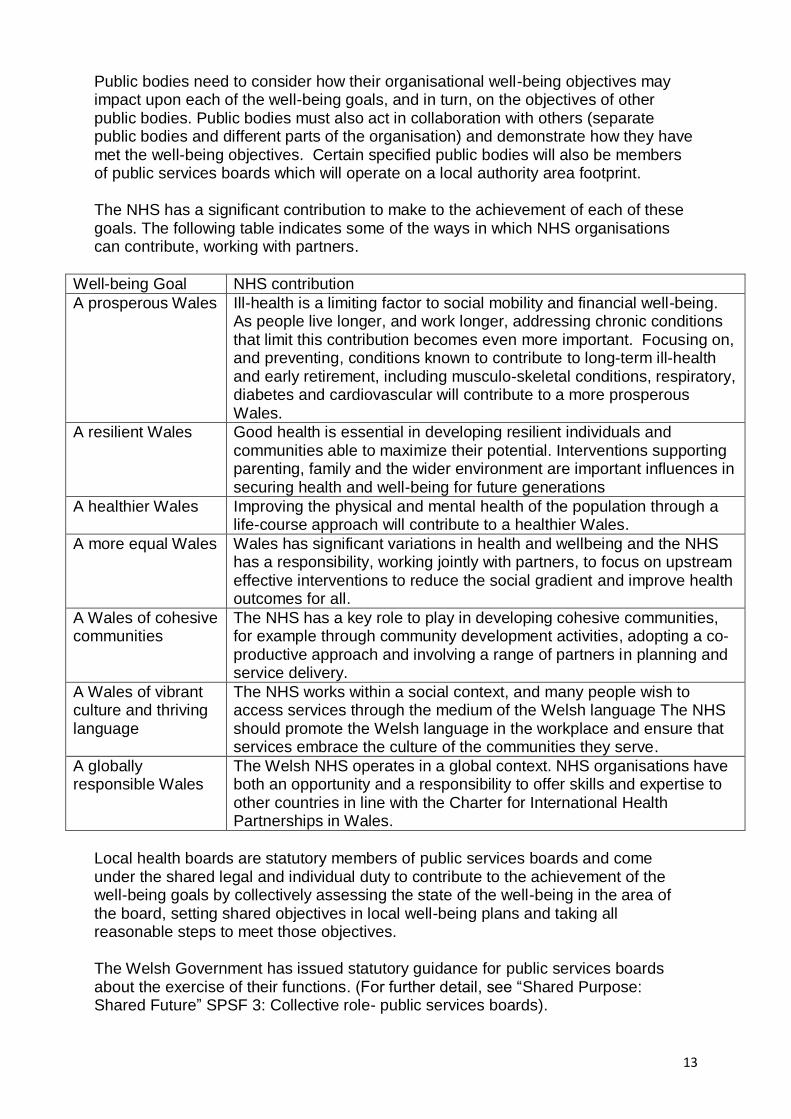
13
Public bodies need to consider how their organisational well-being objectives may impact upon each of the well-being goals, and in turn, on the objectives of other public bodies. Public bodies must also act in collaboration with others (separate public bodies and different parts of the organisation) and demonstrate how they have met the well-being objectives. Certain specified public bodies will also be members of public services boards which will operate on a local authority area footprint. The NHS has a significant contribution to make to the achievement of each of these goals. The following table indicates some of the ways in which NHS organisations can contribute, working with partners.
Well-being Goal NHS contribution
A prosperous Wales Ill-health is a limiting factor to social mobility and financial well-being. As people live longer, and work longer, addressing chronic conditions that limit this contribution becomes even more important. Focusing on, and preventing, conditions known to contribute to long-term ill-health and early retirement, including musculo-skeletal conditions, respiratory, diabetes and cardiovascular will contribute to a more prosperous Wales.
A resilient Wales Good health is essential in developing resilient individuals and communities able to maximize their potential. Interventions supporting parenting, family and the wider environment are important influences in securing health and well-being for future generations
A healthier Wales Improving the physical and mental health of the population through a life-course approach will contribute to a healthier Wales.
A more equal Wales Wales has significant variations in health and wellbeing and the NHS has a responsibility, working jointly with partners, to focus on upstream effective interventions to reduce the social gradient and improve health outcomes for all.
A Wales of cohesive communities
The NHS has a key role to play in developing cohesive communities, for example through community development activities, adopting a co-productive approach and involving a range of partners in planning and service delivery.
A Wales of vibrant culture and thriving language
The NHS works within a social context, and many people wish to access services through the medium of the Welsh language The NHS should promote the Welsh language in the workplace and ensure that services embrace the culture of the communities they serve.
A globally responsible Wales
The Welsh NHS operates in a global context. NHS organisations have both an opportunity and a responsibility to offer skills and expertise to other countries in line with the Charter for International Health Partnerships in Wales.
Local health boards are statutory members of public services boards and come under the shared legal and individual duty to contribute to the achievement of the well-being goals by collectively assessing the state of the well-being in the area of the board, setting shared objectives in local well-being plans and taking all reasonable steps to meet those objectives. The Welsh Government has issued statutory guidance for public services boards about the exercise of their functions. (For further detail, see “Shared Purpose: Shared Future” SPSF 3: Collective role- public services boards).
14
Local health boards will be setting well-being objectives as individual bodies and as part of public services boards. These are distinct, but complementary, duties – requiring public bodies to think both about what their own objectives as an organisation are and about the shared objectives for the areas they operate in. This means that over time local health boards’ strategic and medium-term planning will be expected to be informed by and, where appropriate, align to public services boards’ local well-being plans. While the first local well-being plans will not be published until mid 2018 the first assessments of local well-being should be available in mid 2017. Social Services and Well-being (Wales) Act 2014
The Social Services and Well-being (Wales) Act 2014 places duties on statutory bodies to improve services, work together with the public to promote well-being and give people a greater voice in and control over their care. This puts the individual at the centre, promoting independence and responsibility and co-ordinating services around people, motivating self-care and meeting their needs at or as close to home as possible. Section 14 of the Act places a duty on health boards and local authorities to jointly undertake an assessment of the local population’s care and support needs, including the support needs of carers. This assessment must also identify:
the extent to which those needs are not being met
the range and level of services required to meet those needs
the range and level of services required to deliver the preventative services required in the Act; and
how these services will be delivered through the medium of Welsh. The population assessment will ensure health boards and local authorities jointly produce a clear and specific evidence base to inform their planning and operational decisions including those out in the IMTPs. The Part 2 Code of Practice (General Functions) states that population assessments will inform and be informed by IMTPs
Part 9 of the Act provides for local authorities and local health boards to establish regional partnership boards. These must be established on the health board footprint and respond to the population assessment. They will ensure effective services, care and support are in place to best meet the needs of their respective population. Further details about regional partnership boards are set out in the Part 9 Statutory Guidance. Prudent Healthcare The Cabinet Secretary for Health, Well-being and Sport has confirmed the importance of prudent healthcare as a key policy driver for the NHS. The principles of prudent healthcare are familiar to the NHS:
15
achieve health and well-being with the public, patients and professionals as equal partners through co-production
care for those with the greatest health need first, making the most effective use of all skills and resources
do only what is needed, no more, no less; and do no harm
reduce inappropriate variation using evidence based practices consistently and transparently.
IMTPs are expected to demonstrate that prudent principles underpin the work of the organisation, building on our expectations for a quality-driven service. Plans must use the prudent healthcare principles to drive improved experience and outcomes for patients and citizens and the efficient and effective use of resources. At national level, a number of programmes have been established under prudent healthcare principles to provide a collective and authoritative focus on specific areas. The programmes in Unscheduled Care, Planned Care and Informatics are well established. IMTPs should demonstrate how organisations are maximising the benefits from the work of these programmes in service delivery and planning. The Primary Care programme is newly established, and organisations will be expected to contribute to its work and be guided by its recommended actions as they emerge. These programmes will support the implementation of best practice and reduce variation leading to improvements in the consistency, effectiveness and quality of care. Primary Care
The Primary Care Plan (November 2014) sets out the policy aim of developing a
“social” model of health, which promotes physical, mental and social well-being
rather than just the absence of ill health.
The plan highlights the importance of all relevant organisations, services and people
working together to ensure the root causes of poor health are addressed. This
includes the NHS, social services, housing, education, transport, environment and
leisure services, the third sector, independent sector, carers and people themselves.
There are five priority areas for action:
Planning care locally
Improving access and quality
Equitable access
A skilled local workforce
Strong leadership.
The overall principles underpinning this plan are:
Prevention, early intervention and improving health, not just treatment
Co-ordinated care where generalists work closely with specialists, and wider

16
support in the community to prevent ill-health, reduce dependency and effectively treat illness
Active involvement of the public, patients and their carers in decisions about their care and well-being
Planning services at a community level of 25,000-100,000 people
Prudent healthcare.
A primary care service for Wales, based on the principles of prudent healthcare, is
the mainstay of the NHS: tackling the root causes of ill health, preventing people from
being admitted to hospital unnecessarily, helping those who have been admitted to
get home quickly with the right support; motivating and supporting people with
chronic conditions and long-term illnesses to manage their health at home.
This approach is entirely consistent with the Well-being of Future Generations
(Wales) Act and one of the key recommendations from the OECD report.
The 64 primary care clusters will become a mechanism for building this collaborative
approach to integrated service planning and delivery. Clusters provide an appropriate
building block for joint work which makes the best use of available financial,
workforce and other resources. This includes not just the resources of the NHS but
also those of local authorities, the third and independent sectors and the assets of
local communities. This model will result in a wider perspective, focussed on
communities, and more local planning boundaries and levels, rather than
organisations.
A data driven system “Informed Health and Care: a digital health and social care strategy for Wales” was published in December 2015 and presents the Welsh Government’s five-year vision for the use of digital technology within both the Welsh NHS and in Wales’s social services. The strategy describes how access to the latest technology will make positive changes for both the patient and staff within the NHS and social services. Patients will have the opportunity to connect to online services to book appointments, order repeat prescriptions and access their own health record. Staff will be able to use mobile devices to support them in a variety of settings and will have access to the up-to-date record of care for their patient or service user, accessible wherever and whenever it is needed. Organisations will be expected to develop a strategic outline programme (SOP), led by a named board-level executive and clinical lead with accountability for delivery. The SOP should set out a clear five year view of investment requirements for technology and digitally-enabled service change in both revenue and capital terms. This must be approved by the Board. In developing this, organisations must be clear about the anticipated benefits, risks, challenges and opportunities available to them through developing digital health. These plans may cross organisational boundaries, and there must be clear evidence that they have been developed collaboratively.

17
3. STRATEGY
The introduction to this framework set out the expectation that every organisation will have a board-approved long-term strategy. This should be a separate document to the IMTP, which will demonstrate how the actions to be taken in the three year period help achieve the long-term vision of the organisation set out in the strategy. The strategy should be based on the population health needs assessment referred to in section 2, and be developed with the full engagement of communities and partners. It should reflect the particular opportunities and challenges within the communities served by the organisation, and set out the long-term direction of the organisation within the national policy context. The strategy should demonstrate a commitment to the patient/user experience, quality and safety, innovation, service transformation, and workforce development. It should highlight key strategic challenges and opportunities facing the organisation and proposed solutions, including service sustainability and infrastructure development. Health board strategies should demonstrate that they are maximising the opportunities from being university or teaching boards. NHS trusts will wish to provide similar evidence of strong research, teaching and innovation. In essence, the strategy should set out the organisation’s strategic goals; outline the “roadmap” which the organisation will follow; and describe how it will address any key strategic challenges or opportunities. The strategy should be formally reviewed and Board approved periodically or in the light of significant change, risks or developments which impact on the long-term direction. NHS Wales Strategy A new strategy for NHS Wales will be developed following the Programme for Government. The longer term strategy will be informed by the finding of the Parliamentary Review into the longer term future of health and social care in Wales. This Review was announced in the Programme for Government and will begin its work later this year with the aim of an initial report within 12 months. The Programme for Government, “Taking Wales Forward”, the Well-being of Future Generations (Wales) Act, the Social Services and Well-being (Wales) Act, Prudent Healthcare and the Primary Care Plan are key policies which will underpin the strategy. Organisations should continue to develop their long-term strategic plans based on their health and population needs assessments, and their in-depth knowledge of the local opportunities and challenges that lie ahead.

18
4.INTEGRATED MEDIUM TERM PLANS (IMTPs)
Health boards are required under the NHS Finance (Wales) Act 2014 to prepare a three year IMTP for approval by the Cabinet Secretary for Health, Well-being and Sport. A Ministerial direction placed the same requirement on NHS trusts. The IMTP should be shaped and informed by the long-term plan, needs
assessments, earlier rolling IMTPs and also 3 year plans drawn up at cluster level to
set out the actions the organisation will take during the next three years in pursuit of
its strategic goals.
Whilst the IMTP must cover three years, it is acknowledged that the level of detail for
each of the three years will be different:
Year 1: should clearly describe, through both the narrative and completed
mandatory templates, the actions and milestones for the coming year.
Preparatory work to support delivery in future years should be set out, for
example a service development programme which will shape service delivery
in year 2 or 3, or preparation of capital and service business cases.
Year 2: should indicate priorities, actions and risks for the second year.
Details should be provided on key plans and metrics, including performance
trajectories. Work on major challenges or opportunities should be outlined, for
example remodelling a critical service or addressing a significant workforce
challenge.
Year 3: should show how the organisation proposes to make continued
progress towards its strategic objectives. This should include as much detail
as possible should be provided. Significant issues should be highlighted, for
example in service and workforce sustainability, balancing resources or
capital/service investment, together with an indication of the actions which will
be taken to address them.
IMTPs should focus on quality, safety, sustainability and the patient/user experience.
Plans should be integrated, with coherence between service, workforce,
infrastructure and financial elements. Plans must be deliverable and demonstrate a
clear understanding of risks and mitigating actions. They must show how the
organisation plans to operate within available workforce and financial resources.
IMTPs should describe actions to make progress towards each of the seven goals
set out in the Well-being of Future Generations Act.
Organisations must demonstrate the actions they will take across the full span of
their responsibilities, whether or not there are specific performance targets attached
to them. This includes work “upstream” to develop healthy communities, build
resilience, tackle inequalities and foster prosperity, as well as to manage demand for
healthcare services.

19
Accurate whole-system demand and capacity models, based on a robust population
health needs assessment, informed by needs assessments produced at cluster level,
are central to the IMTP. This is key to clarity about system requirements, as well as
giving organisations a vehicle to model the impact of alternative modes of delivery
and to assess resource impacts. Welsh Government will continue to work with health
boards and trusts to develop these models.
Whilst rolling IMTPs cover three years, they must be agreed by Boards and
submitted to Welsh Government for approval annually. This recognises the nature of
medium-term planning, which is dynamic and must be responsive both to actual
progress made each year and to changing external factors.
The primary audience for IMTPs is local. The plan should describe to local
communities what the organisation intends to do in the coming planning period. The
organisation will wish to ensure that their communities, partners and staff can see in
appropriate detail how services will be developed and improved each year.
Chapter 8 of the Planning Framework provides more detail about the structure of the
IMTP. Following this guidance will allow the Health and Social Services Group to
develop an all-Wales IMTP, showing intended achievements and planned quality and
service improvements across the country. The Delivery Framework clearly sets out
what needs to be achieved.
The maturity matrix produced by the Good Governance Institute provides a helpful
way for organisations to test the maturity of their plans, and is attached at Appendix
D.
Delivery Framework From 2017, the NHS Delivery Framework is changing. It will start to align more
closely with the public-health framework, working towards the production of only one
outcome framework. This means that there will be one health outcome framework
using public health indicators, instead of the current two frameworks.
This change is intended to demonstrate how NHS delivery measures contribute to
wider health gains (outcome indicators) and should support partnership working to
deliver sustainable health and well-being outcomes. By using public health
outcomes, linked to national Well-being of Future Generation indicators, public sector
boards will work towards the same measures. Health boards, trusts and partnership
organisations will be able to demonstrate how they are working together to meet the
goals of the Well-being of Future Generations (Wales) Act.
This will be a gradual change. The current delivery measures remain extant.
Performance and service teams will be involved in ongoing work to some of the
measures to agree definitions and data collection, and you will be kept informed of
progress.

20
While there will remain a national focus on certain target areas, organisations must
plan for and deliver improvement across the range of health improvement indicators
and measures. Organisations should consider and understand how a variety of
measures working together will impact across a range of patient experience and
efficiency. For example, sustainably reducing waiting times for elective surgery
improves the quality of patient experience, may also reduce emergency admissions
and avoidable harm and avoid high cost waiting list solutions such as waiting list
initiatives.
This year, the templates have been slightly changed and simplified. Boards and
trusts will have more detailed plans for their own use to manage their performance.
The detailed performance information behind these templates may be considered in
performance discussions with Welsh Government such as Quality and Delivery
meetings.
National programmes including primary care, unscheduled and planned care
programmes are intended to support organisations to implement and achieve
performance indicators. We expect that organisations will engage with these national
programmes to assist sustainable delivery and reflect this in their IMTPs.
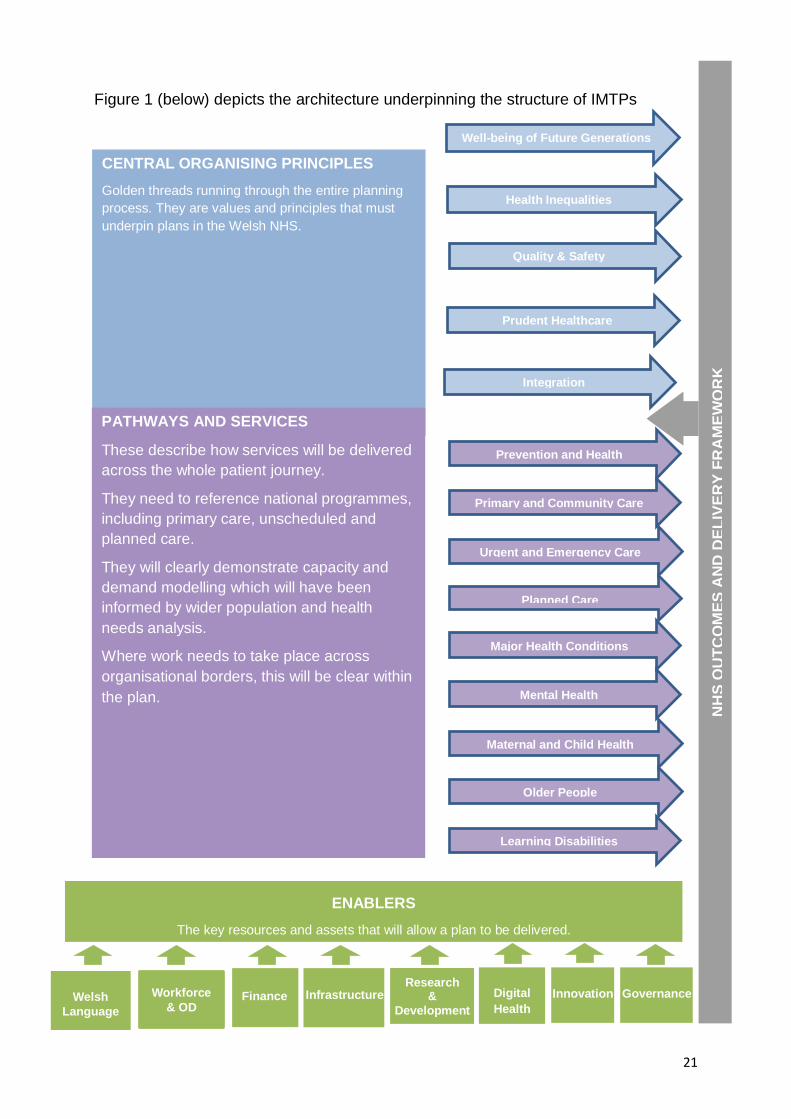
21
Welsh
Language
Infrastructure Finance
NH
S O
UT
CO
ME
S A
ND
DE
LIV
ER
Y F
RA
ME
WO
RK
Digital
Health
Innovation Research
&
Development
Governance
ENABLERS
The key resources and assets that will allow a plan to be delivered.
CENTRAL ORGANISING PRINCIPLES
Golden threads running through the entire planning
process. They are values and principles that must
underpin plans in the Welsh NHS.
PATHWAYS AND SERVICES
These describe how services will be delivered
across the whole patient journey.
They need to reference national programmes,
including primary care, unscheduled and
planned care.
They will clearly demonstrate capacity and
demand modelling which will have been
informed by wider population and health
needs analysis.
Where work needs to take place across
organisational borders, this will be clear within
the plan.
Figure 1 (below) depicts the architecture underpinning the structure of IMTPs
Well-being of Future Generations
Health Inequalities
Prudent Healthcare
Quality & Safety
Integration
Prevention and Health Improvement
Primary and Community Care
Urgent and Emergency Care
Planned Care
Maternal and Child Health
Major Health Conditions
Mental Health
Older People
Learning Disabilities
Workforce
& OD
22
5. PRIORITIES FOR 2017/20
This framework has clearly described the importance of a strategic view to underpin
medium-term IMTPs. Each organisation must ensure that it has a clear strategy,
approved by its Board, to provide the context for its IMTP and how the strategy will
be delivered.
NHS organisations are large and complex, with a wide range of responsibilities.
IMTPs should demonstrate an understanding by the NHS organisation of the actions
it needs to take across the full portfolio of its responsibilities.
Welsh Government indicates through the Planning Framework areas of priority which
the NHS is expected to pay particular attention to. This does not mean that other
areas are unimportant. A good IMTP will demonstrate that the organisation is
focussed on all of its responsibilities. The seven themes below reflect cross cutting
areas that IMTPS need to address.
Quality and Safety IMTPs should demonstrate a core focus on quality and safety. This includes ensuring
that services are patient/user centred, accessible and timely, efficient, effective and
sustainable, providing the best possible outcomes and experience for the greatest
number of people. Best practice should be used to inform service design with a focus
on continuous quality improvement, underpinned by robust quality assurance
mechanisms.
IMTPs should identify areas where action is required to ensure service sustainability,
including proposals for changes to service models or locations to promote quality and
reduce risks.
Timely Access to Care The public expects timely access to the services they require, wherever they are
delivered. This includes access to GPs and wider primary care services as well as to
secondary care or mental health. In some areas there are national targets for
timeliness, and IMTPs must set out how the organisation plans to achieve those
targets, with improvement trajectories where required.
Access to timely care is a key indicator of quality, and delays can result in harm. The
focus must not be exclusively on those areas in which there is a national target. Each
organisation should set its own expectations for timeliness through their plan.
An Ageing Population
Meeting the needs of our ageing population is a significant issue for the NHS. This
includes much more than just the provision of medical treatments and support. It also
relates to focussing on dignity and independence, and the environment in which care
is delivered for older people, in the community and in hospital settings. Physical
23
activity, maintaining independence and promoting preventive health (including mental
well-being) are extremely important for this group.
IMTPs should demonstrate how organisations are working with partners and older
people, and the specific and measurable actions which will be taken to meet their
needs.
Integration and Shift of Services
IMTPs must reflect an integrated approach informed by the work of the public
services boards and regional partnership boards and demonstrate integrated service
solutions in areas of common interest identified as part of joint needs analysis, for
example the care of children or older people.
Most people receive most of their health care most of the time close to home rather
than in a hospital setting. A key Welsh Government policy objective is to maximise
the opportunities to develop local community-based care. IMTPs should set out how
the organisation plans to achieve this policy objective.
Mental Health
Mental illness affects 1 in 4 people, and represents over 20% of the burden of
disease and 12% of the NHS budget. Health boards must give it proportionate
consideration in their IMTPs. A new three year delivery plan has been issued to
underpin the “Together for Mental Health” strategy. This sets out clear priorities and
IMTPs must demonstrate the organisation’s delivery of these priorities.
IMTPs should demonstrate how the organisation is meeting its statutory
responsibilities under the Mental Health (Wales) Measure 2010 and how the
organisation is delivering improved access and outcomes for service-users from the
additional significant investment by Welsh Government in targeted areas of provision.
More generally, IMTPs should clearly set out the organisational service change
programmes to ensure the availability of high quality, sustainable, accessible and
timely care with associated timescales and risks.
Engagement
Organisations must demonstrate that their IMTPs have been developed with
engagement from the public, staff and partners. Co-production continues to be a key
design principle, and IMTPs should provide evidence of how service plans have been
developed with the people who require them. Organisations should note that co-
production with communities is a potentially powerful way in which public sector staff
can respond to the social gradient of health needs.

24
Efficiency, Productivity and Variation
In light of the ongoing financial constraints, the need to deliver more efficient and
productive healthcare services has never been greater.
A review of traditional efficiency measures (e.g. Average Length of Stay and DNA
rates) has identified that, despite past efforts to address such issues, there still
remains significant scope for savings by reducing variation, remove low value activity
and working towards “best in class”, whilst at the same time achieving better
user/patient experience.
Key Deliverables
IMTPs must demonstrate how organisations are planning to deliver in a number of
key performance areas. Not all of these are relevant to all NHS organisations.
Discussions will be held with those organisations which have specific areas of focus
to agree their key deliverables. This applies to Powys tHB, Public Health Wales NHS
Trust, Velindre NHS Trust and the Welsh Ambulance Services NHS Trust.
Delivery plan processes have been streamlined in response to comments from the
service. The IMTP will need to provide assurance about the actions, timeframes and
monitoring arrangements that will deliver these critical services for patients. There is
no longer a requirement to submit local delivery plans to Welsh Government.
Organisations will of course still need to plan for these important services and reflect
the key areas of intended improvement in their three year plans. The detail required
is set out in chapter 8.
Key elements of the seasonal plan should also be integrated within the IMTP,
including the management of risk over the winter period. For example, performance
trajectories such as unscheduled care and RTT should reflect the predicted impact of
seasonal flux. Predicted changes in bed utilisation such as “step up/step down” beds
and assumptions around staffing requirements are also needed within the IMTP.
25
6. PROCESS AND TIMETABLE
Figure 2 sets out the timetable for the IMTP process. In addition to the formal
submission in January and March, Welsh Government will provide additional support
at peer review stage, and also through one to one meetings with planners. The
intention is to encourage better defined plans earlier in the process, to ensure that
plans are well developed for the January board approval. Health boards and trusts
are encouraged to share drafts or outline plans with the Welsh Government planning
team to provide initial advice in advance of the January submission. The intention is
to help NHS organisations to have plans suitable for adequate assessments and
feedback to inform the March submission.
Joint committees governing NHS support organisations will require these
organisations to develop their plans earlier, so that joint committee approved plans
can be aligned and incorporated into the LHB and Trust IMTP planning cycle. To
ensure sufficient time to inform health board and NHS trusts plans the joint
committee may develop and set a timetable that requires support organisation plans
to be advanced, at a minimum, by at least one month from the main timetable.
All plans submitted as ‘final draft’ in January must demonstrate how key priorities will
be delivered, be financially balanced and approved for submission by NHS Boards.
Fully populated mandatory templates are required in order for boards to understand
the detail of plans, and so that Welsh Government can assess them. Any IMTP
submitted without the necessary information will be returned to the organisation.
The final submission in March, informed by feedback and with any agreed
adjustments, must be balanced and formally approved by the board before it is sent
to Welsh Government for consideration by the Cabinet Secretary for Health, Well-
being and Sport.
The Chief Executive of any organisation which is unable to submit an IMTP which
meets these criteria will be required to write, no later than the set submission date, a
formal Accountable Officer letter to the Director General/Chief Executive of NHS
Wales copied to his/her Chair explaining the position, the action they are taking and
when their IMTP will be completed.
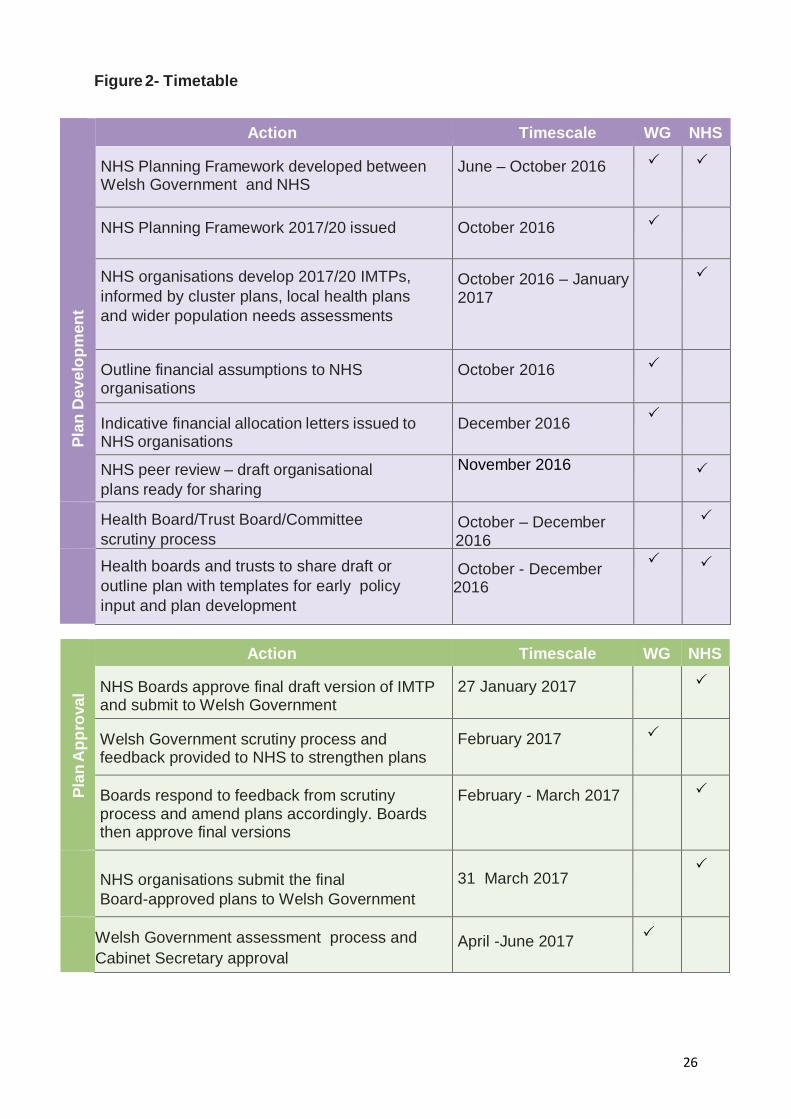
26
Figure 2- Timetable
P
lan
Dev
elo
pm
en
t
Action Timescale WG NHS NHS Planning Framework developed between Welsh Government and NHS
June – October 2016
NHS Planning Framework 2017/20 issued
October 2016
NHS organisations develop 2017/20 IMTPs,
informed by cluster plans, local health plans
and wider population needs assessments
October 2016 – January 2017
Outline financial assumptions to NHS organisations
October 2016
Indicative financial allocation letters issued to NHS organisations
December 2016
NHS peer review – draft organisational
plans ready for sharing
November 2016
Health Board/Trust Board/Committee
scrutiny process
October – December 2016
Health boards and trusts to share draft or
outline plan with templates for early policy
input and plan development
October - December 2016
P
lan
Ap
pro
va
l
Action Timescale WG NHS NHS Boards approve final draft version of IMTP and submit to Welsh Government
27 January 2017
Welsh Government scrutiny process and feedback provided to NHS to strengthen plans
February 2017
Boards respond to feedback from scrutiny process and amend plans accordingly. Boards then approve final versions
February - March 2017
NHS organisations submit the final
Board-approved plans to Welsh Government
31 March 2017
Welsh Government assessment process and
Cabinet Secretary approval
April -June 2017

27
Plan assessment and approval
The expectation is that plans, issues and risks are shared with Welsh Government as
IMTPs are being developed. The onus is on individual organisations to contact Welsh
Government colleagues to discuss the matter as soon as they become aware that
they face difficulties in developing an approvable IMTP. There should be no surprises
in IMTP submissions in January and March.
Welsh Government will conduct a full assessment and provide feedback in writing by
28 February 2017 on the January submissions. Meetings will be set up between
Welsh Government officials and each health board or trust to discuss the feedback
and inform the final plan.
Following assessment of the final IMTP, officials will provide advice to the Cabinet
Secretary. This process will run between 1 April and 30 June 2017. The assessment
process will be undertaken as quickly as possible. Any requirement for further
information will delay the process of consideration and plan approval.
Advice to the Cabinet Secretary will be based on the criteria set out in the Finance
(Wales) Act 2014 (See Annex B) and the requirements set out in this Planning
Framework. Approval letters will be issued by 30 June 2017.
Plan Delivery
The test of any plan lies in its implementation and the resulting improvements in
outcomes, service delivery and patient experience.
The public, NHS Boards and Welsh Government have shared expectations that the
planning process will support the delivery of improved outcomes for patients. NHS
Boards will be expected to hold their organisations to account for delivery of board-
approved IMTPs. In turn, Boards can expect to be held to account by Welsh
Government for delivery of plans approved by the Cabinet Secretary.
Effective assurance and performance management arrangements, both locally and
from Welsh Government, are critical to monitoring progress and providing early
indications if performance varies from plan.
Performance Management by Boards All NHS organisations are required to have approvable IMTPs. Welsh Government
will expect each organisation’s internal mechanisms to provide visible assurance to
the Board on delivery and any necessary corrective action. The following
arrangements must be in place:
robust arrangements for monitoring and intervening at directorate, divisional, cluster, and corporate departments levels;
effective risk identification and mitigation arrangements appropriate monitoring arrangements to hold NHS support organisations, such
28
as NWSSP, to account for timely delivery of agreed activities which support health board/trust performance
clear arrangements through which the Board of each LHB assures itself about the quality of services commissioned and provided for their populations by other organisations, including other LHBs, NHS Trusts in Wales and other providers in Wales or England. This should include assurance about the work of WHSSC and EASC which are formally joint sub-committees of all the Health Boards and act on their behalf
arrangements to monitor quality and delivery against plan on a monthly basis. As a minimum, there should be an executive group to oversee plan delivery and a board sub-committee or group to scrutinise and challenge progress and performance on a regular basis.
The board should receive an overall assessment of progress against the plan in
public session at least bi-annually.
Performance Management by Welsh Government All health boards and trusts will be expected to deliver their approved IMTPs,
including agreed delivery profiles.
Welsh Government will require quarterly updates on delivery of the IMTP from all
organisations. Detailed requirements and submission dates will be notified during the
IMTP development phase. Specific deliverables will be monitored at appropriate
frequencies, for example ambulance response times or unscheduled care
performance.
Organisations can expect the Welsh Government to monitor, performance manage
and hold them to account through a range of meetings and actions. The precise
mechanisms and frequency will vary according to an assessment of risk based on
plan approval status, delivery track record, and actual performance against plan
tracked throughout the year.
Routine Welsh Government performance management arrangements will include:
Standard returns
Submission of board and committee planning updates
Quality & Delivery (Q&D) meetings to discuss progress in detail. The frequency of
Q&D meetings will be determined by plan status and the delivery confidence
assessment based on performance trends and risk analysis
Specific meetings to discuss particular variations from plan or quality standards
Joint Executive Team (JET) meetings to include progress against plan delivery.
Organisations without approved IMTPs
Any health board or NHS trust whose IMTP is not approved will be expected to put in place a one-year plan whilst they improve their ability to develop a three-year IMTP.

29
Failure to develop an approved IMTP is a significant governance concern as it breaches one of the two duties of a health board or NHS trust. Any organisation which is in this position can expect significant increased scrutiny and potentially escalation under the Escalation and Intervention Arrangements. Immediate actions may include:
increased frequency of reporting, meetings and scrutiny;
detailed examination of areas of non-delivery, and the requirement for recovery plans and revised delivery trajectories;
support from the Delivery Unit and other relevant mechanisms to support, challenge and provide assurance;
more frequent Quality & Delivery meetings; and
increase in frequency of Joint Executive Team meetings.

30
7. SIGNIFICANT SERVICE CHANGE
The expectation is that all plans for service change are grounded in evidence and are
informed and shaped by effective engagement with patients, clinicians, staff, other
partners and local communities. Health boards should have appropriate approaches
in place to involve everyone in the conversation about the case for change and the
options for providing the best solution that will meet the needs of the population.
Evidence has shown that effective and early engagement will help to ensure that
plans can be developed and taken forward with energy and pace and deliver the
intended benefits.
All organisations are continuously striving to improve. A number of projects and
changes in practice will be underway or in development to enable a complex
organisation to keep pace with emerging clinical practice and respond to growing and
changing demand.
Some changes will be significant. A change in the underlying clinical strategy and
processes will fundamentally change the way that the whole organisation behaves,
including its culture, decision-making and team behaviours. This might involve a shift
from secondary to primary and community care, where activity, workforce and
financial resources are expected to be moved into primary care to support care
closer to home. A new model for the delivery of specialist services that will mean
centralisation at fewer hospital sites to improve patient outcomes is another example
of a significant change.
Further examples may be found in substantial changes in delivering planned care,
integration with social care to improve care for older people and collaborative working
across organisational boundaries.
Plans should identify services in which there is a potential need for significant change
which will be explored during the planning period. Wherever possible, the
engagement and planning approach which the organisations will follow should be
described.
This year, the Planning Framework asks for narrative to describe significant service
changes, in addition to a template. The narrative should provide the rationale for
change, timescale and milestones and cross-reference to other relevant sections of
the plan (such as primary care, delivery plans, urgent and emergency care,
workforce, or finance) and demonstrate clearly how the benefits of the change will be
realised.
31
8. IMTP STRUCTURE
Balancing Local Discretion and Consistency
Whilst IMTPs need to be owned locally by the individual organisations, there must be
sufficient consistency in presentation and content to allow Welsh Government to
have a clear picture across Wales and to be able to compare plans. Part of that
consistency can be gained through the mandatory templates. These do not however
capture some of the broader planned developments which cannot be expressed in
purely numerical terms.
Welsh Government will require IMTPs to be structured under a number of headings
as set out in Figure 3. The detail of how the document is crafted under those broad
headings is a matter for the individual organisation, as long as it is possible to draw
out from each section:
the key developments/actions the organisation is planning to take
why those are important and how they link to overall strategic direction
what those developments/actions will achieve
when those benefits will be realised, including improvement trajectories where relevant
key risks and dependencies and how they will be managed, for example recruitment.
One presentational option would be to provide a table in each section of the IMTP
highlighting key developments/actions. Officials would welcome discussions on
presentation with individual organisations as they develop their IMTPs.
IMTP Coverage and Structure
This section provides a structure for a health board IMTP, and incorporates guidance
notes covering organising principles, pathways and services and enablers that set
out in broad terms the characteristics of a good plan in that area. These should not
be seen as exhaustive, but as indicators of some of the aspects that the IMTP should
address.
Welsh Government recognises that not all NHS organisations have the same set of
responsibilities. Powys tHB and the three NHS trusts each have specific portfolios or
organisational features which mean that the “standard” framework applicable to
health boards needs to be adapted to be relevant. Officials will discuss with each of
these organisations the expected coverage of their IMTPs, and agree its structure.
As outlined in section 4, the IMTP is a three year plan. The more detailed the plan is
in all years, the more confidence the organisation, the public and Welsh Government
can have in it.

32
Figure 3: IMTP Structure
1. Foreword
2. Executive Summary
3. Introduction
4. Strategic Overview, encompassing organising principles:
Well-being of Future Generations Act
Social Services and Well-being Act
Health inequalities
Quality and Safety
Prudent Healthcare
Integration
5. Achievements in 2016/17
6. Opportunities and Challenges in 2017/2020
7. Significant Service Change
8. Thematic chapters
Pathways and Services
Prevention and health improvement
Primary and community care
Urgent and emergency care
Planned care
Major health conditions
Mental health
Maternal and child health
Older people
Learning Disabilities
Enablers
Workforce & OD
Finance
Infrastructure investment
Research &development, and innovation
Digital Health
Governance
Welsh Language
Mandatory Appendices
33
The sections that follow are intended to provide further guidance on the required
structure.
Foreword – by Chair and Chief Executive.
Executive Summary – a brief summary of the IMTP. Introduction – purpose, scope, relationship to the separate organisational strategy,
process of development including engagement and partnership working.
Strategic Overview – key elements of the organisations strategy cross referenced to
separate document, including population needs assessment, challenges,
opportunities, key strategic developments/proposals which influence the next 3 year
plan. This section will demonstrate how the organising principles, set out in figure 3,
form a foundation for the organisational plan.
Achievements in 2016/17 – summary of key achievements the organisation expects
to have made by the end of 2016/17 which forms the baseline going into year 1 of the
2017/2020 IMTP.
Opportunities and Challenges in the IMTP period – an outline of key opportunities
and challenges in the three year period which narrows the focal length from long-
term strategy to the medium and shorter term opportunities and risks. There may be
overlap with the longer term strategic challenges, but a shorter term focus should be
possible. For example, a key strategic objective may be to address inequalities. A
shorter term IMTP opportunity or challenge may be linked to impending changes in
primary care, or to the development of specific plans with a local authority for joint
service provision in an area of deprivation. Similarly, particular recruitment
challenges may be looming, or the opening of a new facility may present
transformational opportunities to improve quality or the patient experience. Care
should be taken not to simply repeat content covered in other sections.
Significant Service Changes 2017/20 – a description of significant changes
planned or requiring development within the three year period. Significant service
change takes place over a period of time. This section may describe early work
towards achieving change, or describe how this work is being embedded. It must be
clear about rationale, milestones, actions, resources and benefits.
The plan narrative must be supported by completed mandated templates which
provide sufficient detail to the board about addressing population needs, service
commissioned and deliverables, workforce planning and resourcing to enable
approval of a credible and deliverable plan.
Previous years’ IMTPs have tended to be very lengthy documents which are hard to
navigate and follow clearly. Longer documents make it harder to identify coherence
and connections. This may be because many have tried to be both a strategic
document and a medium-term plan. This Planning Framework draws a distinction
34
between a strategic document concerned with the long-term direction of travel
(15/20+ years) and an IMTP covering a three year period.
By definition, longer term direction changes and evolves more slowly than shorter
term three year plans. This has led to IMTPs in which large sections have not
changed from one year to the next, making it much harder to identify the distinct
actions the organisation plans to take in the next period.
Clearly the IMTP must sit within the context set by the longer term strategy; however,
trying to write a single accessible document of manageable length which covers both
is very difficult. This is why the Planning Framework requires that the organisation’s
long term strategy is separate from its medium term plan, and recognises they are
complementary and cross-referenced.
It should be unusual for an IMTP to be longer than 150 pages in length plus
mandatory appendices. If further detail is required by a board or by Welsh
Government to provide assurance about aspects of an IMTP, it can be specifically
requested. Boards will have their more detailed operational plans which are used to
manage the detail of the organisation’s work. These should cover any additional
information which Welsh Government is likely to require.
The sections that follow provide advice on the thematic chapter headings set out in
section 8. They are intended to support organisations to ensure that relevant
information is included, as well as guiding towards relevant strategies and
documents.
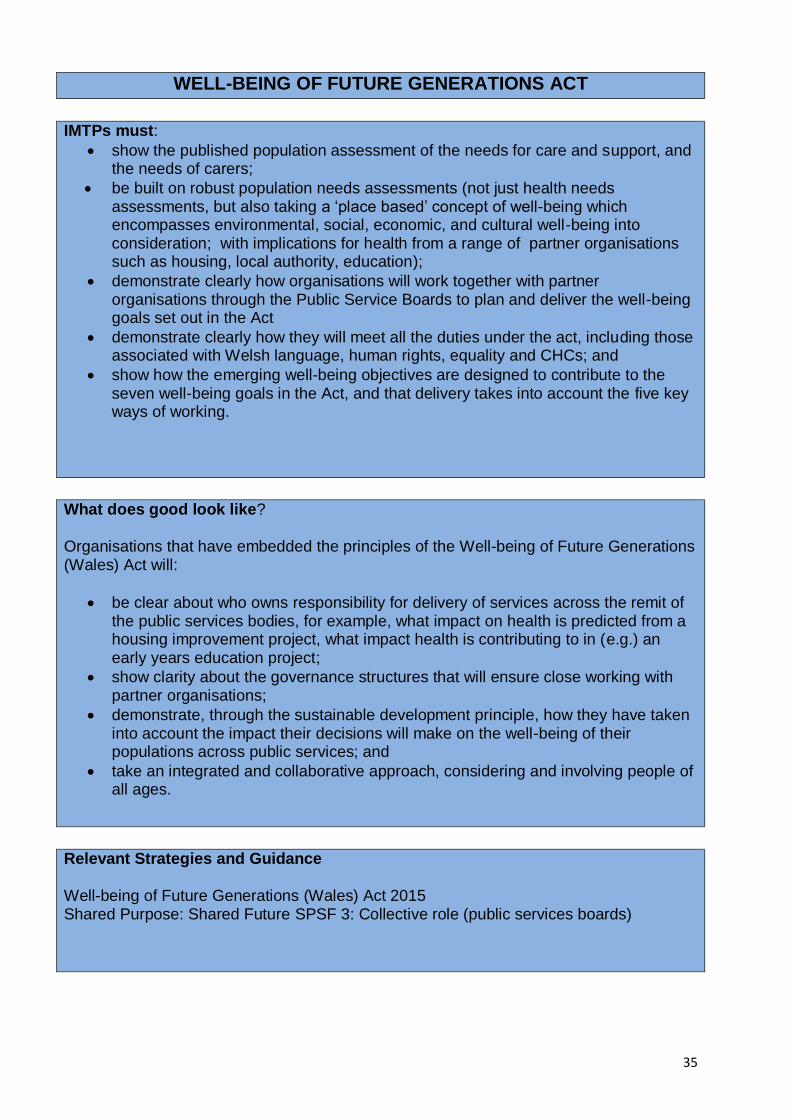
35
WELL-BEING OF FUTURE GENERATIONS ACT
IMTPs must:
show the published population assessment of the needs for care and support, and the needs of carers;
be built on robust population needs assessments (not just health needs assessments, but also taking a ‘place based’ concept of well-being which encompasses environmental, social, economic, and cultural well-being into consideration; with implications for health from a range of partner organisations such as housing, local authority, education);
demonstrate clearly how organisations will work together with partner organisations through the Public Service Boards to plan and deliver the well-being goals set out in the Act
demonstrate clearly how they will meet all the duties under the act, including those associated with Welsh language, human rights, equality and CHCs; and
show how the emerging well-being objectives are designed to contribute to the seven well-being goals in the Act, and that delivery takes into account the five key ways of working.
What does good look like?
Organisations that have embedded the principles of the Well-being of Future Generations (Wales) Act will:
be clear about who owns responsibility for delivery of services across the remit of the public services bodies, for example, what impact on health is predicted from a housing improvement project, what impact health is contributing to in (e.g.) an early years education project;
show clarity about the governance structures that will ensure close working with partner organisations;
demonstrate, through the sustainable development principle, how they have taken into account the impact their decisions will make on the well-being of their populations across public services; and
take an integrated and collaborative approach, considering and involving people of all ages.
Relevant Strategies and Guidance
Well-being of Future Generations (Wales) Act 2015 Shared Purpose: Shared Future SPSF 3: Collective role (public services boards)
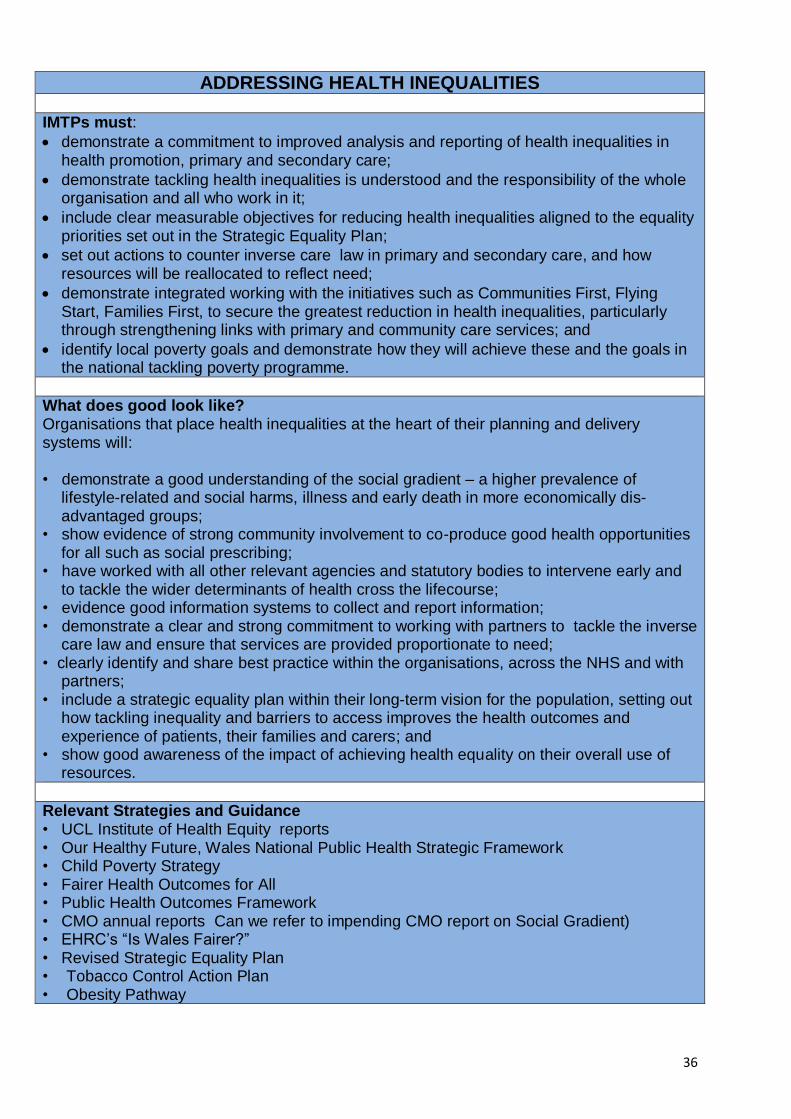
36
ADDRESSING HEALTH INEQUALITIES
IMTPs must:
demonstrate a commitment to improved analysis and reporting of health inequalities in health promotion, primary and secondary care;
demonstrate tackling health inequalities is understood and the responsibility of the whole organisation and all who work in it;
include clear measurable objectives for reducing health inequalities aligned to the equality priorities set out in the Strategic Equality Plan;
set out actions to counter inverse care law in primary and secondary care, and how resources will be reallocated to reflect need;
demonstrate integrated working with the initiatives such as Communities First, Flying Start, Families First, to secure the greatest reduction in health inequalities, particularly through strengthening links with primary and community care services; and
identify local poverty goals and demonstrate how they will achieve these and the goals in the national tackling poverty programme.
What does good look like? Organisations that place health inequalities at the heart of their planning and delivery systems will: • demonstrate a good understanding of the social gradient – a higher prevalence of
lifestyle-related and social harms, illness and early death in more economically dis-advantaged groups;
• show evidence of strong community involvement to co-produce good health opportunities for all such as social prescribing;
• have worked with all other relevant agencies and statutory bodies to intervene early and to tackle the wider determinants of health cross the lifecourse;
• evidence good information systems to collect and report information; • demonstrate a clear and strong commitment to working with partners to tackle the inverse
care law and ensure that services are provided proportionate to need; • clearly identify and share best practice within the organisations, across the NHS and with
partners; • include a strategic equality plan within their long-term vision for the population, setting out
how tackling inequality and barriers to access improves the health outcomes and experience of patients, their families and carers; and
• show good awareness of the impact of achieving health equality on their overall use of resources.
Relevant Strategies and Guidance • UCL Institute of Health Equity reports • Our Healthy Future, Wales National Public Health Strategic Framework • Child Poverty Strategy • Fairer Health Outcomes for All • Public Health Outcomes Framework • CMO annual reports Can we refer to impending CMO report on Social Gradient) • EHRC’s “Is Wales Fairer?” • Revised Strategic Equality Plan • Tobacco Control Action Plan • Obesity Pathway
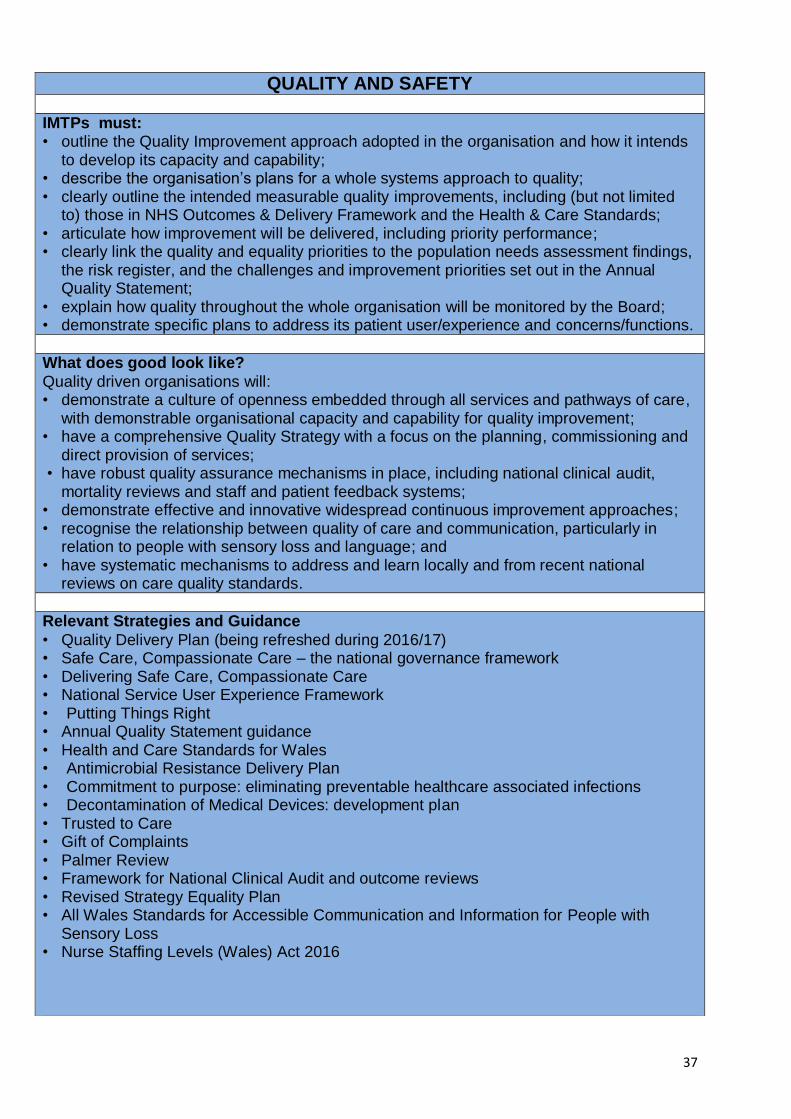
37
QUALITY AND SAFETY
IMTPs must: • outline the Quality Improvement approach adopted in the organisation and how it intends
to develop its capacity and capability; • describe the organisation’s plans for a whole systems approach to quality; • clearly outline the intended measurable quality improvements, including (but not limited
to) those in NHS Outcomes & Delivery Framework and the Health & Care Standards; • articulate how improvement will be delivered, including priority performance; • clearly link the quality and equality priorities to the population needs assessment findings,
the risk register, and the challenges and improvement priorities set out in the Annual Quality Statement;
• explain how quality throughout the whole organisation will be monitored by the Board; • demonstrate specific plans to address its patient user/experience and concerns/functions.
What does good look like?
Quality driven organisations will: • demonstrate a culture of openness embedded through all services and pathways of care,
with demonstrable organisational capacity and capability for quality improvement; • have a comprehensive Quality Strategy with a focus on the planning, commissioning and
direct provision of services; • have robust quality assurance mechanisms in place, including national clinical audit,
mortality reviews and staff and patient feedback systems; • demonstrate effective and innovative widespread continuous improvement approaches; • recognise the relationship between quality of care and communication, particularly in
relation to people with sensory loss and language; and • have systematic mechanisms to address and learn locally and from recent national
reviews on care quality standards.
Relevant Strategies and Guidance
• Quality Delivery Plan (being refreshed during 2016/17) • Safe Care, Compassionate Care – the national governance framework • Delivering Safe Care, Compassionate Care • National Service User Experience Framework • Putting Things Right • Annual Quality Statement guidance • Health and Care Standards for Wales • Antimicrobial Resistance Delivery Plan • Commitment to purpose: eliminating preventable healthcare associated infections • Decontamination of Medical Devices: development plan • Trusted to Care • Gift of Complaints • Palmer Review • Framework for National Clinical Audit and outcome reviews • Revised Strategy Equality Plan • All Wales Standards for Accessible Communication and Information for People with
Sensory Loss • Nurse Staffing Levels (Wales) Act 2016
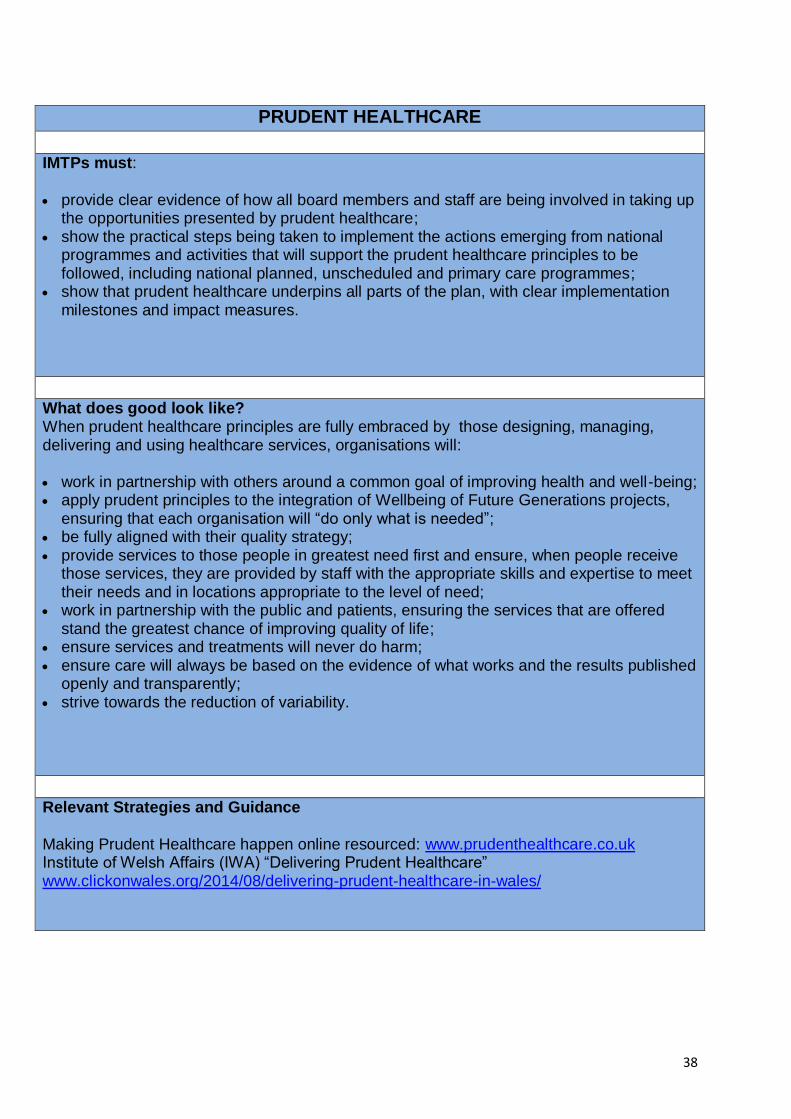
38
PRUDENT HEALTHCARE
IMTPs must: provide clear evidence of how all board members and staff are being involved in taking up
the opportunities presented by prudent healthcare; show the practical steps being taken to implement the actions emerging from national
programmes and activities that will support the prudent healthcare principles to be followed, including national planned, unscheduled and primary care programmes;
show that prudent healthcare underpins all parts of the plan, with clear implementation milestones and impact measures.
What does good look like? When prudent healthcare principles are fully embraced by those designing, managing, delivering and using healthcare services, organisations will: work in partnership with others around a common goal of improving health and well-being; apply prudent principles to the integration of Wellbeing of Future Generations projects,
ensuring that each organisation will “do only what is needed”; be fully aligned with their quality strategy; provide services to those people in greatest need first and ensure, when people receive
those services, they are provided by staff with the appropriate skills and expertise to meet their needs and in locations appropriate to the level of need;
work in partnership with the public and patients, ensuring the services that are offered stand the greatest chance of improving quality of life;
ensure services and treatments will never do harm; ensure care will always be based on the evidence of what works and the results published
openly and transparently; strive towards the reduction of variability.
Relevant Strategies and Guidance Making Prudent Healthcare happen online resourced: www.prudenthealthcare.co.uk Institute of Welsh Affairs (IWA) “Delivering Prudent Healthcare” www.clickonwales.org/2014/08/delivering-prudent-healthcare-in-wales/

39
INTEGRATION
IMTPs must: reflect the shared priorities that have been agreed with public service partners through
the Public Service Boards, Local Service Boards and partner agencies; reflect partnership priorities and progress in other key areas, e.g. Mental Health
partnership programmes; show how integration is underpinning the other programmes described within this
framework, notably the work on planned, urgent and emergency care and primary care; demonstrate how priority performance indicators of reducing delayed transfers of care will
be achieved.
What does good look like? Organisations with a robust approach to integration across the life-course will: demonstrate how services are being built with, and for, people and the local community.
Services will be co-designed with the people who will use them and shaped around their needs rather than functional boundaries;
be pro-active in the promotion of independence and autonomy for service users; show that the building blocks of locality network sand clusters are utilized to drive
integrated solutions through local engagement; demonstrate how best practice is being used to help shape integrated services across the
life course; demonstrate how the workforce is used effectively in a way that is open to innovations in
skill mix and staff substitution; show how, working closely with others, their activities are being refocused around those
people receiving care and ensure existing barriers to integrated working and delivery are eliminated;
demonstrate how they are developing and maximizing the use of local partnership working arrangements to secure a healthier population;
show awareness of the barriers to current models of healthcare that are experienced by people from disadvantaged groups and how changes to services (integration) will lead to better access and outcomes.
Relevant Strategies and Guidance
Integration – cooperation and partnership Making integrated care happen at scale and pace, Kings Fund, March 2013 Shared Delivery, Shared Purpose
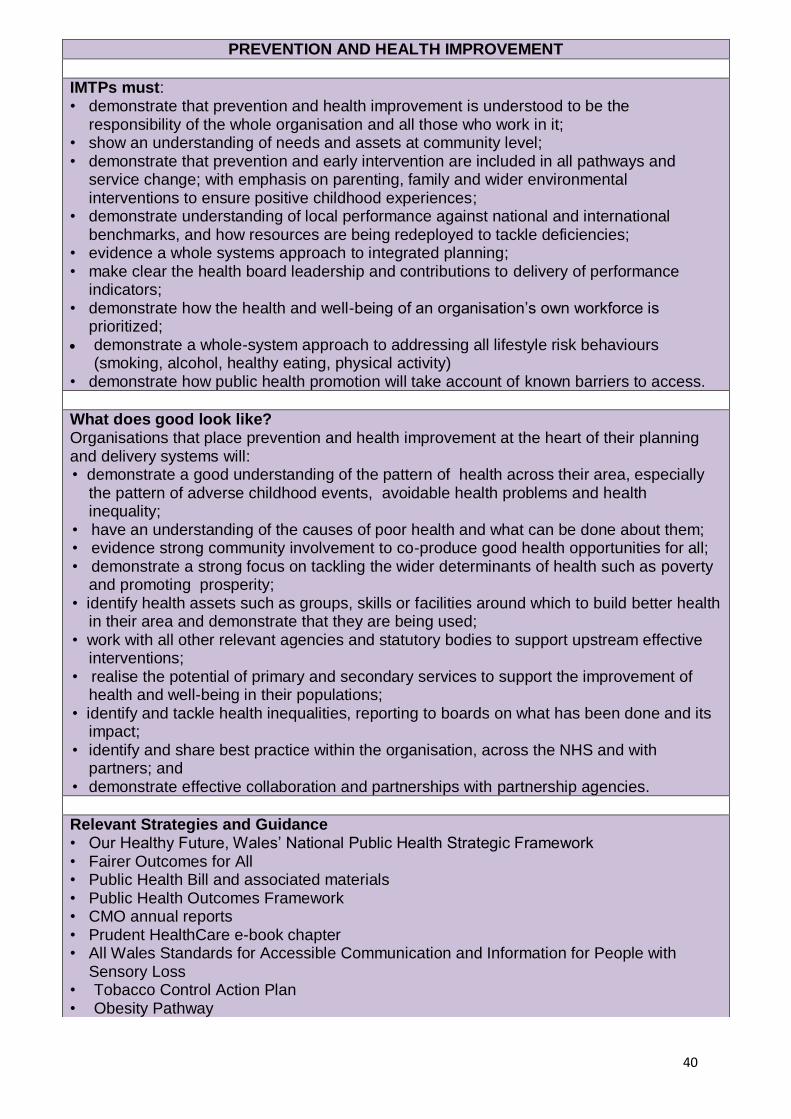
40
PREVENTION AND HEALTH IMPROVEMENT
IMTPs must: • demonstrate that prevention and health improvement is understood to be the
responsibility of the whole organisation and all those who work in it; • show an understanding of needs and assets at community level; • demonstrate that prevention and early intervention are included in all pathways and
service change; with emphasis on parenting, family and wider environmental interventions to ensure positive childhood experiences;
• demonstrate understanding of local performance against national and international benchmarks, and how resources are being redeployed to tackle deficiencies;
• evidence a whole systems approach to integrated planning; • make clear the health board leadership and contributions to delivery of performance
indicators; • demonstrate how the health and well-being of an organisation’s own workforce is
prioritized; demonstrate a whole-system approach to addressing all lifestyle risk behaviours
(smoking, alcohol, healthy eating, physical activity) • demonstrate how public health promotion will take account of known barriers to access.
What does good look like? Organisations that place prevention and health improvement at the heart of their planning and delivery systems will: • demonstrate a good understanding of the pattern of health across their area, especially
the pattern of adverse childhood events, avoidable health problems and health inequality;
• have an understanding of the causes of poor health and what can be done about them; • evidence strong community involvement to co-produce good health opportunities for all; • demonstrate a strong focus on tackling the wider determinants of health such as poverty
and promoting prosperity; • identify health assets such as groups, skills or facilities around which to build better health
in their area and demonstrate that they are being used; • work with all other relevant agencies and statutory bodies to support upstream effective
interventions; • realise the potential of primary and secondary services to support the improvement of
health and well-being in their populations; • identify and tackle health inequalities, reporting to boards on what has been done and its
impact; • identify and share best practice within the organisation, across the NHS and with
partners; and • demonstrate effective collaboration and partnerships with partnership agencies.
Relevant Strategies and Guidance • Our Healthy Future, Wales’ National Public Health Strategic Framework • Fairer Outcomes for All • Public Health Bill and associated materials • Public Health Outcomes Framework • CMO annual reports • Prudent HealthCare e-book chapter • All Wales Standards for Accessible Communication and Information for People with
Sensory Loss • Tobacco Control Action Plan • Obesity Pathway

41
PRIMARY & COMMUNITY CARE
IMTPs must: • be based on local health needs assessments, including pharmaceutical, dental and
optometric needs, that highlight the needs of communities; • reflect the actions within the Plan for Primary Care Services for Wales with a particular
focus on improving access to services; • include workforce plans that deliver appropriate capacity and capability of multi-skilled
primary care teams with the most appropriate professionals delivering care; • articulate quantifiable quality improvements in primary care and how they will be
achieved; • articulate the programme of development for primary care clusters, including plans for
increasing autonomy to improve local planning and delivery, including new models and incentives;
• describe how people with chronic conditions will be supported to manage their conditions; • demonstrate how improved primary care will be improved, measured and reported,
including tracking the shift of resources; • be guided by the recommendations of the Welsh Language Commissioner’s Primary
Care Report; • detail an estate strategy based on evidence service needs.
What does good look like?
Organisations that are committed to strengthening primary and community care will: • use local population (25,000 to 200,00 population) health needs assessments, including
pharmaceutical needs, to plan services for localities; • use financial, workforce and other resources to strengthen primary care, with a particular
focus on responding to customer feedback; • identify how pathways can be rebalanced, with appropriate components provided in
primary and community care, reducing reliance on secondary care; • focus on developing multi-skilled working in primary care settings; • meet the access needs of their populations in a timely way, including encouraging the
use of e-systems; • have systems to ensure continuity of care; • report transparently on quality and performance of primary care and population health
outcomes; • ensure integrated information is available to all professional staff to enable informed
decision making and reduce duplication and error.
Relevant Strategies and Guidance
A Plan for Primary Care Services for Wales, 2014 Delivery Plans for Oral Health, Eye Health, End of Life Care and major conditions Mid Wales Framework of Action The Welsh Government’s response to the Welsh Language Commissioner’s Review into
A Plan for Primary Care Services for Wales Social Services and Well-being (Wales) Act 2014.

42
URGENT & EMERGENCY HEALTH CARE IMTPs must:
• align to the steps of the national unscheduled care programme; • demonstrate how a clear and focused approach to quality, safety and patient experience
in the context of urgent and emergency care is reported within the organisation and to the public;
• demonstrate a clear understanding of demand and capacity across the patient pathway, identifying the level of resources which will be deployed to effectively meet demand at all stages of escalation;
• describe how an integrated model incorporating community, primary, secondary and social care services is delivered seamlessly, safely and reliably, putting the individual at the centre;
• identify the opportunities offered by the Public Service Boards and Regional Partnership Boards to promote independence and well-being ;
• show clear plans to reduce unnecessary referrals to secondary care, describing alternative and direct access pathways where appropriate;
• describe how plans to improve the flow of patients through the urgent and emergency care system will be transferred to operational implementation, and what the expected impact will be in a measurable format;
• describe how communications, interfaces and relationships across health and social care will be improved to enhance partnership working and patient flow;
• describe performance trajectories for key access targets, demonstrating how they will be achieved, reviewed and evaluated.
What does good look like? A patient receiving quality driven, evidence based and patient focused urgent and emergency care will: • know what is expected of them to take responsibility for their own health and well being; • be navigated to the most appropriate service as quickly as possible, as close to home as
possible; • receive a response based on their clinical need and always in a timely and efficient
manner regardless of their location in Wales or the time of day, week, month or year; • be placed at the centre of decisions made by all involved with planning and delivering
their care; • be sent home to recover, if admitted to hospital, as early as clinically appropriate without
unnecessary waiting; and have an opportunity to feedback on their experience to help improve delivery of care or
support to others.
Relevant Strategies and Guidance
Prudent healthcare Informed Health and Care: A digital health and social care strategy for Wales Plan for a primary care service for Wales up to March 2018 National Collaborative Commissioning Quality and Delivery Framework for Emergency
Ambulance Services NHS Wales Unscheduled Care Programme Delivery Plan 2016/17 NHS Wales Hospital Handover Guidance Passing the Baton - A Practical Guide to Effective Discharge Planning
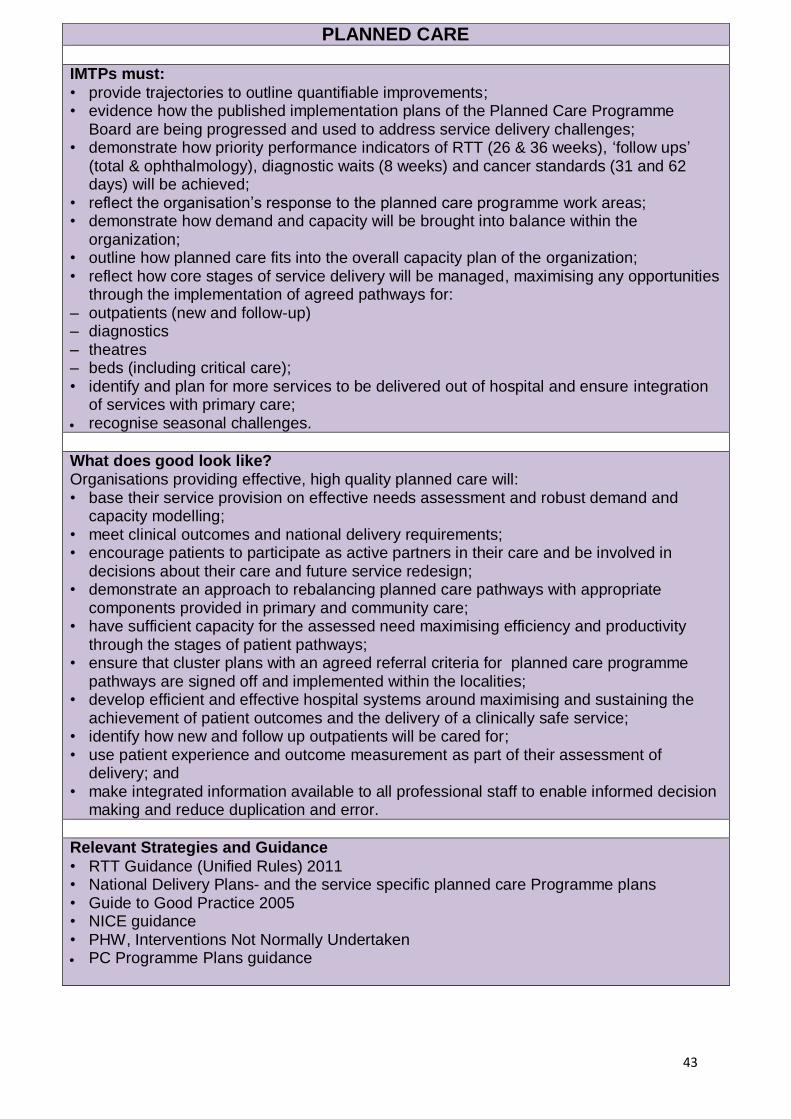
43
PLANNED CARE IMTPs must:
• provide trajectories to outline quantifiable improvements; • evidence how the published implementation plans of the Planned Care Programme
Board are being progressed and used to address service delivery challenges; • demonstrate how priority performance indicators of RTT (26 & 36 weeks), ‘follow ups’
(total & ophthalmology), diagnostic waits (8 weeks) and cancer standards (31 and 62 days) will be achieved;
• reflect the organisation’s response to the planned care programme work areas; • demonstrate how demand and capacity will be brought into balance within the
organization; • outline how planned care fits into the overall capacity plan of the organization; • reflect how core stages of service delivery will be managed, maximising any opportunities
through the implementation of agreed pathways for: – outpatients (new and follow-up) – diagnostics – theatres – beds (including critical care); • identify and plan for more services to be delivered out of hospital and ensure integration
of services with primary care; recognise seasonal challenges.
What does good look like? Organisations providing effective, high quality planned care will: • base their service provision on effective needs assessment and robust demand and
capacity modelling; • meet clinical outcomes and national delivery requirements; • encourage patients to participate as active partners in their care and be involved in
decisions about their care and future service redesign; • demonstrate an approach to rebalancing planned care pathways with appropriate
components provided in primary and community care; • have sufficient capacity for the assessed need maximising efficiency and productivity
through the stages of patient pathways; • ensure that cluster plans with an agreed referral criteria for planned care programme
pathways are signed off and implemented within the localities; • develop efficient and effective hospital systems around maximising and sustaining the
achievement of patient outcomes and the delivery of a clinically safe service; • identify how new and follow up outpatients will be cared for; • use patient experience and outcome measurement as part of their assessment of
delivery; and • make integrated information available to all professional staff to enable informed decision
making and reduce duplication and error.
Relevant Strategies and Guidance
• RTT Guidance (Unified Rules) 2011 • National Delivery Plans- and the service specific planned care Programme plans • Guide to Good Practice 2005 • NICE guidance • PHW, Interventions Not Normally Undertaken PC Programme Plans guidance
44
DELIVERY PLANS: MAJOR HEALTH CONDITIONS
9 Major Health Conditions (End of Life, Stroke, Liver, Heart Disease, Cancer, Diabetes, Neurological Conditions, Critically Ill and Respiratory)
IMTPs must:
• establish a vision for local services and clearly articulate how local priorities link to national priorities and actions within the national delivery plan;
• be based on robust local needs assessment and audits; • link local and national priorities and actions within the delivery plan; • set out links to the strategic context; • show how local actions are improving patient outcomes, reducing inequalities and driving
service change; • include timescales, milestones and outcomes; and • set out how progress will be sustained across the three years of the IMTP
What does good look like? Organisations with strong delivery plans will: • use robust needs assessment to allow them to understand and address the well being of
the whole population; • align and reference links to other sections within the IMTP including primary care, planned
and unscheduled care as well as finance, workforce, performance and capital and estates;
• have timely access to services; • evidence how resources will be managed to deliver on both national and local priorities; • show partnership working with other statutory agencies and the third sector; • cross condition boundaries to provide holistic care; • demonstrate systems to ensure continuity of care; • identify how pathways can be rebalanced, with appropriate components provided in
primary and community care, reducing reliance on secondary care;
Relevant Strategies and Guidance
End of Life Care Delivery Plan –
http://gov.wales/docs/dhss/publications/130416careen.pdf Stroke Delivery Plan - http://gov.wales/docs/dhss/publications/121206visioned.pdf Liver Delivery Plan - http://gov.wales/docs/dhss/publications/150505liveren.pdf Cancer Delivery Plan - http://gov.wales/docs/dhss/publications/150427planen.pdf Neurological Conditions Delivery Plan -
http://gov.wales/docs/dhss/publications/140508neurologicalen.pdf Diabetes Delivery Plan -http://gov.wales/docs/dhss/publications/130923diabestesen.pdf Heart Disease Delivery Plan – http://gov.wales/docs/dhss/publications/130503hearten.pdf Critically Ill Delivery Plan – http://gov.wales/docs/dhss/publications/130611deliveryen.pdf Respiratory Delivery Plan -
http://gov.wales.docs.dhss/publications/140429respiratoryen.pdf Please ensure that you refer to the latest version of the delivery plan as some plans are being refreshed during 2016/17.

45
MENTAL HEALTH IMTPs must:
• demonstrate an understanding of the mental health and mental well-being needs of the population across the life-course;
• include a capacity and demand analysis which also demonstrates how the HB is actioning the areas for improvement;
• show progress against the actions in the 3 year delivery plan that underpins T4MH; • set out clear actions, measureable milestones for implementation, analysis of risks to
delivery, and measures of success; • evidence the quality of service provision and the involvement of service users and families
at all levels of care; • clearly articulate the priorities for improvements in mental health provision covering
CAMHS; • show expenditure over the previous year against the mental health ring-fenced allocation
and the future spending plans against that budget;
What does good look like? Organisations delivering the best mental health will: • use robust needs assessment to allow them to understand and address the mental health
and well-being of the whole population; • demonstrate how preventative measures and early intervention treatment plans take into
account an individual’s language and cultural needs; • demonstrate how they contribute to reducing the impact of mental health problems and/or
mental illness on individuals, their families and carers, communities and the economy more widely;
• give individuals increased control over related decisions; • offer timely access to mental health services; • demonstrate an understanding of how the values, attitudes and skills of those treating or
supporting individuals of all ages with mental health problems or mental illness will be improved;
• demonstrate partnership working with other statutory agencies and with the third sector.
Relevant Strategies and Guidance • Mental Health Measure (Wales) 2010 and Duty To Review Report 2015 • Together for Mental Health and new supporting delivery plan: 2016-2019 • Annual Reports on the Strategy Implementation • Together for Children and Young People Service Improvement Plans and its supporting
Framework for Improvement • Policy Implementation Guidance on Mental Health Services for Prisoners in Wales • Policy Implementation Guidance on Healthcare for Gypsy Travelers • Talk to Me 2 • Policy implementation guidance for the admission of children to adult mental health wards • The Crisis Care Mental Health Concordat

46
MATERNAL & CHILD HEALTH
IMTPs must:
• demonstrate how improved outcomes for health improvement strategies targeted at maternal health, children and young people will be achieved, including childhood and maternal immunization, Families First and Flying Start programmes;
• demonstrate how health care will be delivered to all children, including a lead clinician role for coordinating health support for SEN/additional learning needs;
• plan to deliver substantial improvement in maternal smoking rates; • demonstrate the implementation schedule for the action plan agreed at the Maternity
Performance Board for increasing breast feeding rates, reducing caesarian sections rates and improving data capture;
• demonstrate an implementation schedule for the Healthy Child Wales Programme over the next 3 years, informed by: – detailed analysis and mapping of need; – engagement with local partners; and – adoption of national guidelines and evidence of what works locally to target support.
• include updated programme to achieve delivery and maintenance of NSF standards for children, young people and maternity services;
• demonstrate how the organization will integration with the national CAMHS service change programme;
• evidence compliance with child safeguarding requirements for staff recruitment and training; • demonstrate support and alignment with the maternity network; and • evidence the steps taken to overcome any identified barriers to effective joint working.
What does good look like? Organisations with good maternal and child health plans will: • have methods to promote early access to maternity services to promote and maintain
maternal mental and physical well-being in pregnancy and infancy; • ensure domestic violence is identified and addressed via a coordinated programme; • have sufficient provision for all healthy women with straightforward pregnancies to give birth
in Midwife Led Units; • adopt the UN convention on rights of the child (UNCRC) as a guiding principle; • have strong links with local partners, with joint plans and appropriate exchange of
information in place to deliver against shared outcomes; • have programmes in place to reduce caesarian section rates and increase breastfeeding; • have programmes to deliver antenatal and postnatal mental health services, and ensure
delivery of mental health requirements as well as adequate availability of all tiers of CAMHS support;
• have programmes to offer integrated services for disabled children, children in special circumstances and integrated health, education and social care services for children;
• assess staff and skill requirements as a children’s workforce, including safeguarding; and • have effective IT systems, offering integration with maternity, education and safeguarding.
Relevant Strategies and Guidance • NSF For Children, Young People and Maternity Services • Strategic Vision for Maternity Services in Wales Strategy • CYP specific sections of Welsh Government Delivery Plans • WG Screening and Immunisation Policy • Healthy Child Wales Programme • Special Educational Needs guidance
47
CARE OF OLDER PEOPLE
IMTPs must:
• demonstrate how they will assess and meet the needs of an ageing population, with a view to supporting independence within the home environment;
• evidence a whole systems approach to integrated care, led by primary and community care services;
• show efficient and effective discharge processes; • Clearly demonstrate partnership working with health, local authorities, third and
independent sectors including residential homes and hospices; • demonstrate clear links to delivery plans and dementia care; • provide evidence of preventative strategies to support ageing well and build resilience; • demonstrate how assistive technologies are being used to support the care of older;
people and maintain independent living; and • demonstrate workforce skills in adult safeguarding to meet legislative requirements.
What does good look like? Organisations which effectively meet the needs of older people will: • demonstrate collaboration, integration and shared decision making between all
providers; • ensure provision of health and care services within age friendly environments; • keep older people and their representatives, carers and families involved in service
planning, delivery and evaluation; • show a full understanding of the needs of older people, including those with complex
needs, in their communities and how they will work across settings and sectors to meet those needs;
• provide holistic and coordinated care which minimises the risk of excessive medication and multiple appointments with healthcare providers;
• focus timely end of life conversations about treatment, care and acceptable outcomes on quality of life and make these discussions routine practice;
• identify those who are frail and elderly and ensure that they have pro-active community-based assessments and interventions that help reduce hospital admissions; and
• ensure their staff are skilled and equipped to deal with the new adult safeguarding.
Relevant Strategies and Guidance • The Strategy for Older People in Wales 2013-2023 • Best Practice Guidance for Engagement and Consultation with Older People on
Changes to Community Services in Wales – Older People’s Commissioner for Wales, July 2014
• Carers Strategy for Wales • Delivering Safe and Compassionate Care • The National Dementia vision for Wales • Ageing Well in Wales programme • Framework for delivering integrated health and social care for older people with
complex needs • Dignified Care, Two Years On

48
CARE FOR PEOPLE WITH LEARNING DISABILITY
IMTPs must: demonstrate how organisations will assess and meet the needs of people with
learning disabilities within their population, including how they will avoid unnecessary hospital admissions;
demonstrate evidence that population health assessments have been undertaken; set out plans for the development of integrated children’s services across health,
social care and education clearly demonstrating partnership working with local authorities;
demonstrate how they will reconfigure NHS residential services for people with learning disabilities to achieve the best outcome;
have clear plans to implement the refreshed autism strategy; describe plans for patients to be repatriated; and clearly demonstrate how people accessing acute services will be identified and
supported through their care journey, including discharge.
What does good look like? Organisations which effectively meet the needs of people with learning disabilities will: demonstrate full compliance with the learning disability care bundle for people
accessing acute services, including an effective hospital liaison service; review activities in terms of funding, and explore opportunities for jointly funded
packages of care; develop acute and primary care liaison; develop advance practice and nurse consultant roles; ensure people with learning disabilities are cared for in appropriate settings and
repatriated to Wales wherever possible.; and ensure that all people with a learning disability have their annual health check. .
Relevant Strategies and Guidance • Learning Disability Strategy: Section 7 guidance on service principles and service
responses. Welsh Government, 2004 (updated January 2011)
49
Enablers - Welsh Language
IMTPs must: • demonstrate that the organisation meets the statutory requirements set out in the Welsh
Language (Wales) Measure 2011 and forthcoming Welsh language standards; • demonstrate that services are planned and delivered in line with the strategic framework
for health and social care in Wales, “More than just words” and the Welsh Government’s response to the Welsh Language Commissioner’s Primary Care Inquiry Report;
• promote the use of Welsh language in the primary care sector; • recognise that patient is receiving care in their first language is a key patient experience
and quality issue; • demonstrate that the organisation has a Welsh Language Bilingual Skills Strategy in
place which is monitored through local teams; • show that in the development of service change and improvement plans there is due
regard to the need to actively offer services through the medium of Welsh; and • show that health needs assessments identify issues of language and that the population
assessment is undertaken in line with the Social Services and Well-being (Wales) Act 2014.
What does good look like? Organisations that meet the statutory requirement to plan and deliver services bilingually will: • ensure that patients and service users are immediately aware that the service is centred
on their communication needs rather than those of the provider; • empower patients to express their needs and be able to fully participate in their care as
equal partners; • ensure that patients are able to see and hear the Welsh language, and feel comfortable
with the environment and services they receive; • make patients aware that the service has a supportive ethos, where Welsh is used as a
natural means of expression; • make patients aware that the service recognises that language is more than a means of
communication and are able to express their ideas and emotions effectively; • put the strategic framework for health and social care in Wales, “More than just words”
into practice and make the “Active Offer” is available; and • show respect for patients’ culture and identity, making sure that they can access Welsh
language services without obstacles, whilst recognising this may be fulfilled through a multi-disciplinary workforce.
Relevant Strategies and Guidance • ‘More than just words’ – Strategic Framework for Welsh Language Services in Health,
Social Services and Social Care • ‘My Language, My Health’ - the Welsh Language Commissioner’s Inquiry into the
Welsh Language in Primary Care. • Welsh Language (Wales) Measure 2011 • Social Services and Well-being (Wales) Act 2014

50
Enablers – Workforce & OD
IMTPs must:
summarise priority actions for workforce redesign, restructuring, and new ways of working to facilitate service change; Include key milestones for delivery;
demonstrate a clear read across from workforce to financial information;
identify areas of workforce that pose a risk to delivery and set out actions to manage this risk;
identify centrally funded education and training requirements;
demonstrate clearly how they will implement the requirements of the Nurse Staffing Levels (Wales) Act 2016, showing that there are sufficient nurses to allow time to care for patients sensitively. The duty to calculate and maintain nurse staffing levels will be commenced on 6 April 2018;
reflect any programme of OD work required to deliver other elements of the IMTP;
demonstrate how priority performance indicators of increased staff engagement, reduced sickness absence and increased appraisal completion rates will be achieved; and
include clear links to accepted governance frameworks for adequate assurance of quality and safety.
What does good look like? An organisation that undertakes effective workforce planning and organisational development will: have a long term approach; be responsive to national priorities; be informed by an understanding of local population needs across the life-course; ground workforce planning in the organisation’s agreed service change priorities
and emerging models of delivery; assess the impact that the service change will have on the current workforce; develop timely implementation plans to enable delivery; maintain robust data on the current workforce and use this information effectively to
identify areas of challenge and plan for action; be proactive in planning the long-term organisational development and educational
requirements of the directly employed workforce; undertake nurse workforce planning (including planning the recruitment, retention,
education and training of nurses), and incorporate this into budgets; implement systems and processes to monitor, review and learn from nurse staffing
shifts of concern in order to allow nurses time to care sensitively for patients; consider the requirements for registered nurses as part of workforce planning and
implement systems to assure the quality of these services where securing the provision of nursing services;
reflect cross boundary and organisational workforce planning (e.g. service, organizational or geographical collaborations);
reflect organizing principles of prudent healthcare principles, quality and safety; enable the swift improvement and up-skilling of staff from Board; exploit opportunities to enable staff to work in partnership and across boundaries
and pursue continuing professional development in developing new workforce models; and
recognise the totality of the workforce assets including directly employed staff, directly contracted staff and the voluntary sector.
51
Enablers – Finance
IMTPs must:
include a balanced medium term financial plan (MTFP) as part of a viable and sustainable IMTP;
place the balanced financial plan within the resource allocation and planning parameters set out in the NHS Allocation Letter and NHS Planning Framework;
focus on value and totality of resources applied rather than focus on the marginal changes, pressures and opportunities;
align with the MTFP with clinical, service, workforce and other elements of the IMTP;
be affordable, in line with the availability of revenue and capital resources, and prioritised in line with Board and Ministerial priorities;
provide assurance that plan actions are real, sustainable and deliverable, and that scenarios, risks, opportunities, equality impact and mitigating actions are clearly set out; and
include clear cross-referencing and alignment with clinical, service and workforce plans, which detail the rebalancing of the healthcare system, through a prudent lens, through the strengthening of care delivered in primary and community settings.
What does good look like? Organisations with a good approach to planning and financial planning will: ensure complete alignment of their financial plan and other component elements
of the IMTP. The revenue and capital plans are enablers to the commissioning, clinical and service plans, which set out how NHS organisations will address the population healthcare needs within available resources;
set out the financial resources required, allocated and agreed, to deliver services and transformation;
detail the resources, and resource shifts, underpinning service changes, innovation and the transfer of services both closer to communities, from secondary to primary and community care, and between communities to address gaps identified in population health needs analysis;
identify and profile the resources, including investments and disinvestments, enabling Boards to address priorities such as reducing health inequalities; and
identify the risk assessed and profiled robust savings plan, linked to service and workforce plans.
Relevant Strategies and Guidance
NHS Allocation Letter 2017/18 Standing Orders and Standing Financial Instructions NHS Finance (Wales) Act 2014 WHC/2015/014 – Statutory and Administrative Financial Duties of Local Health Boards and NHS Trusts Making fair financial decisions: guidance for decision-makers – Equality and Human Rights Commission (updated in 2015) Nurse Staffing Levels (Wales) Act 2016
52
Enablers – Infrastructure Investment
IMTPs must: ensure that Capital and Revenue infrastructure investment is clearly prioritised in
line with Board and Ministerial priorities, defined and linked to the plan;
align infrastructure investment with the service and other elements of the IMTP;
provide infrastructure investment plans that are affordable and drive out maximum efficiencies;
demonstrate clear improvements in the patient quality and safety environment across the NHS in Wales;
articulate the impact on other planning areas including performance, quality, workforce as well as revenue affordability;
have clearly defined benefits and benefits realisation plans to demonstrate the impact of investment and service change, particularly regarding patient outcomes;
include the impact of monitored Estate Key Performance Indicators such as backlog maintenance, space utilisation and out of date equipment.
include primary and community care; and
demonstrate a year-on-year growth in investment in information technology and digitally-enabled service models in line with the principles and vision set out in the Digital Health and Care Strategy.
What does good look like?
Organisations with a good approach to infrastructure investment will:
have a prioritised strategy with clear links to clinical strategy and service planning, articulating the necessary asset base to meet current and future service needs;
promote schemes that support the delivery of sustainable and accessible services and facilitate high standards of patient care, demonstrating clear alignment with the principles of prudent health care;
support changes to streamlining and transforming healthcare provision and promote the use of information and innovation to improve the quality of care and to deliver service change;
support programmes and projects of strategic importance with clear links to investment criteria as set out by the Minister (and reinforced by the NHS Wales Infrastructure and Investment Guidance WHC (2015) 012:
have infrastructure investment plans that maximise health gain;
promote clinical and skills sustainability;
ensure affordability;
provide value for money;
promote equity; and
be supportive of investment that will assist the shift away from the acute sector towards primary and community care and care closer to home.
Relevant Strategies and Guidance
Together for Health 2011 Wales Infrastructure Investment Plan May 2012 NHS Wales Infrastructure and Investment Guidance WHC (2015) 012 published on 30 March 2015.

53
Enablers – Research & Development IMTPs must:
• demonstrate how the health board or trust will improve patient outcomes through participation in research and maximising impact from research results;
• demonstrate the active promotion of the value of research through clear communication strategies with a range of audiences, i.e. patients, clinicians and local organisations including HEIs;
• describe the arrangements in place to ensure research feeds into the organisation’s mechanisms for uptake of best practice, innovation and service change;
• demonstrate how the organisation will meet the key indicators and targets set out in the Delivery Framework for Performance Management of NHS R&D 2015/16; and
• demonstrate how the organisation will set expectations for appropriate inclusion of children and young people into research.
What does good look like?
Organisations with a good R&D function will: • have an up-to-date R&D strategy covering commercial and non-commercial
activity, and demonstrating clear integration into the wider organisation’s innovation, knowledge mobilisation and quality improvement agenda;
• provide visible leadership and actively integrate R&D into local planning, financial and decision making structures including representation of R&D on the Board of the NHS organisation;
• promote a culture that values and promotes research through leading and/or hosting studies, ensuring that all staff recognise and understand the role that research plays in increasing and delivering good quality care, including staff recruitment, retention and development;
• provide equity of access to opportunities that enable participation in research for patients and service users, especially in under-researched populations such as children and young people;
• have transparent and efficient mechanisms to allocate resources and recover costs from relevant sources (industry, research grants); and
• have an evidence-based decision making culture of which R&D is a key component.
Relevant Strategies and Guidance • Health and Care Research Wales Strategic Plan 2015-2020 • Industry Engagement, NISCHR • Report on Knowledge Transfer, NISCHR AHSC • Welsh Government Delivery Framework for the Performance Management of
NHS R&D 2015/16 • RCPCH Guidance on clinical research involving infants, children and young
people

54
Enablers – Digital Health & Care
IMTPs must:
fully embrace the opportunities that digital technologies, including assistive technologies, can bring to transforming service models and supporting our ambitions;
show how they work with NWIS, Welsh Government and NHS Leads for Informatics to deliver a strategy implementation programme which prioritises the key deliverables and actions in Informed Health and Care;
detail digital health and care developments, fully aligned and integrated with the service and workforce change priorities in their IMTPs. These should include implementation of agreed national system, services and products delivered with NWIS, with a clear articulation of the outcomes and benefits of implementation.
What does good look like? Organisations with good digital health and care will: show clear leadership to implement the Informed Health and Care strategy; have a named board-level executive and clinical lead(s) with accountability for the
delivery of the informatics developments; be developing a strategic outline programme (SoP) to set out a clear five-year
view of investment requirements for technology and digitally-enabled service change in both revenue and capital terms which establishes a clear resource requirement across NHS Wales;
ensure that the SoP is approved and resourced by the relevant board and be fully integrated and aligned with the service change, financial, workforce and quality improvement plans at a local level as well as prioritising plans to roll out national systems, services and products in line with the national informatics delivery programme;
have robust governance and assurance arrangements to manage the risks, benefits, interdependencies and prioritisation of local and national implementation plans; and
• demonstrate effective stakeholder engagement.
Relevant Strategies and Guidance • Informed Health and Care; a digital health and social care strategy for Wales
(2015) • Improving Informatics Programme – high level principles document (October
2014) • Digital Wales Strategy • Enabling the delivery of Prudent Healthcare through information technology
http://www.prudenthealthcare.org.uk/information-technology
55
Enablers – Innovation
IMTPs must:
• demonstrate how innovation and service improvement will be developed with specific description of methods and approaches employed, and the structures which will support and deliver them;
• reflect a strategic approach to promoting innovation to staff, patients and public; • identify the resources that will be deployed in innovation activities and the
expected outputs and benefits; • describe formal arrangements and plans to establish innovation partnerships; and • have visible accountability for innovation through a named board level Executive
Director and a named clinical lead.
What does good look like? An organisation which constantly seeks a better way of delivering healthcare and improving services will: respect and reward inquiry and ideas; have the skills to develop and apply new practice and products; dedicate resources to create space for innovation and improvement have a clear process to support the translation of knowledge into practice and
products, which is understood throughout the organisation; • dedicate resources and expertise to accelerate selected innovation projects; • demonstrate a systematic approach to the identification and adoption of better
value practice and products; • have a systematic approach to evaluating current practice and products,
addressing unmet needs and discarding approaches that do harm or offer poor value;
• demonstrate a structured approach to managing partnerships with external organisations including industry and investors;
• show visibly committed leadership at senior level; and • have a clear line of sight to the Board.
Relevant Strategies and Guidance
• Recommendations on Health and Wealth, Health and Well-being Best Practice and Innovation Board
• Information Driven Improvement, Health and Well-being Best Practice and Innovation Board
• Final Report, Health and Well-being Best Practice and Innovation Board • Industry Engagement, NISCHR • Innovation Wales • Report on Knowledge Transfer, NISCHR AHSC • Report on IP Management and Commercialisation, EST, Welsh Government

56
Enablers – Governance
IMTPs must:
• demonstrate that the plan has been developed and agreed following meaningful engagement with public, staff and stakeholders;
• confirm that the required agreements have been reached in terms of collaborative agreements, including WHSSC, EASC, NWSSP and NWIS;
• have been subject to a high level of board and committee scrutiny; • be approved by the organisation’s board before submission; • set out internal governance arrangements to ensure delivery of the plan,
including how delivery will be reported and non delivery addressed; • outline the key risks and approach to risk management; and • confirm that equality impact assessments and consideration of the Welsh
language have been taken on board.
What does good look like?
NHS organisations with good and effective governance arrangements will: • have a board approved long term strategy, built on robust needs assessment,
which is understood and clear to the whole organisation; • have a strategy that is underpinned by a drive for quality improvement and is
aligned with national policies and strategies; • actively engage with public, patients, staff and stakeholders - the output from
this engagement will inform the board’s strategy and plan; • ensure the required capacity and capability is in place across the organisation to
develop and deliver the IMTP; • ensure that all statutory obligations and duties are understood and discharged; • ensure that there are clearly defined and well understood processes for
escalating and resolving issues and managing performance; • have a robust approach to risk management; • have a range of local actions, incentives and sanctions available to be deployed
in the case of non-delivery; • demonstrate effective use of robust and relevant management information; and • have effective mechanisms in place to embed health and care standards.
Relevant strategies and guidance
• NHS Governance e-manual • www.wales.nhs.uk/governance-emanual/home • Academi Wales – The Good Governance Guide for NHS Wales Boards • NHS Finance (Wales) Act 2014 • Standing Orders & Standing Financial Instructions • Maturity Matrix Appendix I of 2016/17 NHS Planning Framework • An Overview of Governance Arrangements Betsi Cadwaladr University Health
Board, Healthcare Inspectorate Wales and the Wales Audit Office, June 2013 • An Overview of Governance Arrangements - Betsi Cadwaladr University Health
Board, Healthcare Inspectorate Wales and the Wales Audit Office, July 2014 • Health and Care Standards Governance and Scrutiny: a guide for boards in respect of equality impact
assessments – NHS CEHR, 2015

57
Appendices:
Appendix A
OECD Reviews of Health Care Quality: United Kingdom 2016
The OECD report published in 2016 acknowledged the progress that is being
made through the planned approach. It also highlighted opportunities for
further development of our system and made four main recommendations:
• Secure accountability, drive standards and promote innovation
• Put primary care front and centre as a force for dynamic system change
• Make Wales a data-driven system
• Do more to promote the patient voice
The report highlighted the need to strike the right balance between local
freedom, innovation and sensitivity to population needs, and achievement of
core standards which must be consistent and centrally driven.
Further detail is contained in the link below.
https://www.oecd.org/els/health-systems/oecd-reviews-of-health-care-quality-
united-kingdom-2016-9789264239487-en.htm
58
Appendix B
NHS FINANCE (WALES) ACT 2014
Key criteria for approval:
The NHS Finance (Wales) Act 2014:
Places a duty on each local health board in Wales to ensure that its
expenditure does not exceed its funding over a period of three financial years;
Provides the Welsh Ministers with a power to require local health boards in
Wales to prepare a plan setting out its strategy to ensure that expenditure
does not exceed its funding, while improving:
o the health of the people for whom it is responsible, and
o the provision of health care to such people;
Places a duty on each local health board in Wales to submit such plans for
approval by Welsh Ministers.
59
Appendix C
IMTP Mandatory & Discretionary Templates 2017/18 to 2019/20 The information requested in these spreadsheets represents the minimum data-set required. The majority of these annexes are critical to the assurance of plans. However, some are essential to inform some other key national planning processes, notably the commissioning of educational workforce numbers. This information may be supplemented by any other detailed schedule the organisation may wish to include.
Mandatory Templates - Sheets
C1 Outcomes Framework - Delivery of Measures
C2 Service Shift from Secondary to Primary and Community Care
C3 Finance - Plan Summary
C4 Finance – Resource Planning Assumptions
C5 Finance – Statement of Comprehensive Net Income/Expenditure – 3 yrs
C6 Finance – Statement of Comprehensive Net Income/Expenditure – Profiles
C7 Finance – Revenue Resource Limit Assumptions
C8 Income and Expenditure Assumptions (Wales NHS)
C9 Finance – Year 1 Savings Plan
C10 Finance – Years 2 & 3 Savings Plan
C11 Finance – Risks and Mitigating actions
C12 Asset Investment Summary
C13 Asset Investment Detail
C14 Revenue Funded Infrastructure
C15 Workforce - WTE
C16 Workforce - £'000
C17 Workforce - Recruitment Difficulties
C18 Educational Commissioning information
C18.1 Undergraduate Education
C18.2 Post Graduate Education
C18.3 Assistant Practitioners & HCSW
C18.4 Medical & Dental
Discretionary Template - Sheet
C19 Delivery - LHB & Trust Specific Internal Service Delivery Plans & Measures

60
APPENDIX D:
GOOD GOVERNANCE INSTITUTE: MATURITY MATRIX
Progress levels 0 Not achieved No evidence
1 Basic level Principle accepted and
2 Early progress Early progress in
3 Results Initial achievements
4 Maturity Comprehensive assurance in
5 Exemplar Others learning from our consistent
Key elements evidence of commitment to delivery
development evident place achievements
RISK HIGH HIGH HIGH / MEDIUM MEDIUM MEDIUM/LOW LOW 1. Plan Alignment: Evidence No alignment is visible in Alignment is visible in plans. Evidence of quality, service Evidence that estate and Coherent aligned plan is Plan is achieving triple aim success of alignment between plans. and/or workforce changes. workforce have been performance managed, with (cost, outcomes, experience); elements
strategy and components of Tested for cost impact. tailored to a clear service variance recorded and of plan are shared and adopted the plan (quality, outcomes, Robust and profiled transformation. ameliorative actions taken and elsewhere.
productivity, workforce, projections. staff largely own and behave in finance, capital). response. 2. National/Local Strategy: No evidence of a clear Clear understanding of priorities Health strategies embedded Plan reflects national Local plans and national policy Board contributes to national policies, Responds to national and understanding of on all Wales and local basis but into organisational plans. health and partnership are aligned, demonstrating a strategies and innovation efforts. Active
local priority drivers (beyond priorities on all Wales and sometimes seen as central Some recognition of priorities and is broader contribution to the wider exporter of skills and techniques. just health) - translation of local basis. dictates and not evidenced into partnership planning. than health and social care economy as well as having an Working across public and third sector. national policies in local organisational responses. (for example, transport, impact on the health and well- Having demonstrable benefits to
clinical strategy and housing etc. priorities are
being of the population. populations.
organisational vision. evidenced). 3. Best Practice: Ambition to No evidence of ambition Published commitment to best Benchmarking within NHS Benchmarking beyond Plans are future proofed to Centres of excellence for a number of deliver best practice levels to achieve best practice. practice with training and with international NHS with UK & impacts of changes of clinical and/or teaching services. High
of efficiency, effectiveness No evidence of improvement/innovation comparators delivers international comparators technology, healthcare performing across non clinical measures and safety. Benchmarking. strategy in place. Improvements. delivers improvements. innovation reflecting clinical (staff survey, corporate standard).
Excellence. 4. Dynamic and Engaged No evidence that plan is Board, clinical and other staff Stakeholders engaged in Joint development and Plan is benefiting partners, Board members are recognised Planning: Reflecting a owned across the and partners are all aware and priority setting. Plan B in communication of plan neighbours and local health advocates of engagement with dynamic and engaged organisation and within engaged in plan development. place for delays. with key partners and economy. Planning is a routine stakeholders. Evidence that output from approach to planning rather the community. Organisational staff respond to Organisational engagement neighbours including health, operational matter that is co- engagement activities inform plans and than an annual event. Carried corporate requirements but do is improving. boards, trusts, LA’s and third
sector. ordinated across and up the influence change and is delivering
out by a corporate not buy into the process. sector. Organisation organisation. Feedback from agreed outcomes. Feedback loop in department. Process is engagement is evident in engagement is influencing and place. Track record of high performance
impacting on outcomes. practice and reflected in plan.
challenging the plan. and engagement with stakeholders.
5. Realistic and Deliverable: No evidence that plan is IMTP articulates how Key risks (quality, service, Both track record and Forward look risk assessments Ability to modify plans and actions to A sensitivity analysis, risk credible and deliverable. the vision will be achieved over access, workforce, finance) current performance anticipates problems to assure keep on track is recognised by others.
assessment of deliverability a three year period, with identified in plan with illustrates achievement on resilience. with reference to track reference to what outcomes evidence of controls and a wide range of issues and record of delivery. Plan is will be delivered by when and assurance. themes. Evidence of plans sustainable and affordable. how. for delivery and
Implementation. 6. Assurance: Clarity on Insufficient assurance on Board clear on roles and Board demonstrates how it Board has track record of Succession planning and Board members are recognised monitoring/assurance and the local accountabilities. will ensure effective dealing successfully with external independent advocates of good governance. Clear
delivery mechanism. monitoring/assurance leadership, governance with difficult issues. Delivery, assurance provides confidence and robust arrangements for tracking
and delivery mechanism. adequate capacity and monitoring and evaluation of resilience. Delivery of plan delivery.
process in place to deliver mechanisms in place. objectives managed effectively goals. through core processes.

3.7 SPPH16/209 HMP Berwyn Healthcare Project
1 SPPH16.209 HMP Berwyn Report.docx
1
Strategy, Partnerships & Population Health Committee 24.11.16 Item SPPH16/209
To improve health and provide excellent care
Title: HMP Berwyn Healthcare Project
Author: Ms Bernie Cuthel Prison Health Development Lead (interim)
Responsible Director:
Mr Andy Roach , Director of Mental Health
Public or In Committee
Public
Strategic Goals (Indicate how the subject matter of this paper supports the achievement of BCUHB’s strategic goals –tick all that apply)
1. Improve health and wellbeing for all and reduce health
inequalities
√
2. Work in partnership to design and deliver more care
closer to home
3. Improve the safety and outcomes of care to match the
NHS’ best
√
4. Respect individuals and maintain dignity in care √
5. Listen to and learn from the experiences of individuals
6. Use resources wisely, transforming services through
innovation and research
√
7. Support, train and develop our staff to excel. √
Approval / Scrutiny Route
The Prison project is reported through the BCUHB Programme Board to this Committee and locally through the shadow Partnership Board which includes National Offender Management Services and Wrexham County Borough Council. In addition, the project is reported through the National Programme Board, held by National Offender Management Services, the Executive Agency of the Ministry of Justice responsible for prisons across the United Kingdom.
Purpose: This paper provides an update on progress in delivering the prison programme and identifies the key risks and mitigating actions being taken.
Significant issues and risks
The mobilisation of the health care service for the prison carries a number of risks, with the main focus being Recruitment and the implementation of the Clinical Information System
Equality Impact Assessment
The equality impacts upon a potentially diverse prison population will be assessed as the project develops.
Recommendation/ Action required by the Committee
1. Note the Governance arrangements in place to mobilise the Health
service at HMP Berwyn
2. Note the key risks and mitigation in delivering the Prison Health
Programme
Disclosure: Betsi Cadwaladr University Health Board is the operational name of Betsi Cadwaladr University Local Health Board

2
HMP Berwyn Healthcare 1. Background
The new prison in North Wales, HMP Berwyn, will open in Spring 2017. It will be a Category C training prison for sentenced adults and young adult men and will provide a resettlement function for prisoners from North Wales. The prison will also have a remand facility for 200 un-sentenced, adults from the courts within North Wales, who at the moment are held in prisons in England, usually HMP Altcourse, in Liverpool. This is likely to equate to 30% of the Berwyn population.
BCUHB is responsible for the delivery of Health Care Services to 2100 men who will reside in HMP Berwyn which will be populated in a phased approach over a period of 12-18 months. The prison will be the largest in the UK and is established as three House Blocks, a Health and Well Being Centre, two Industrial Units and an Education Centre. BCUHB has been commissioned by Welsh Government to provide the Healthcare Services within the Prison, comprising a full range of in-house Healthcare Services including Primary Care Services including minor injuries and ailments, Dental services, Therapies, Mental Health and Learning Disabilities, Substance Misuse, Pharmacy and X-Ray. Secondary Care Services will be provided primarily by Wrexham Maelor Hospital and the Ambulance Service by Welsh Ambulance Services Trust. Social Care will be provided by Wrexham County Borough Council.
2.Governance Arrangements
2.1 National Programme Board The HMP Berwyn Programme Board, is chaired by the Senior Responsible Officer for the National Offender Management Services and meets monthly to review programme progress across all agencies, identifying risks and mitigating actions. This is a critical forum for BCUHB in ensuring that any issues or obstacles identified locally as part of our local programme plan are escalated and resolved. This is a monthly meeting attended by a range of stakeholders.
2.2 Prison Partnership Board It is a formal requirement for a Prison Partnership Board to be established locally, as the mechanism to ensure that the accountability agreement between the Health Board, Wrexham County Borough Council and the National Offender Management Service is delivered. During the mobilisation phase, Welsh Ambulance Services Trust have been co-opted to the Board, to ensure communication regarding pathways of care from the prison to secondary care services is strengthened.
2.3 BCUHB Prison Programme Board The BCUHB internal Healthcare Programme Board meets on a monthly basis and is attended by Heads of Service across the following workstreams:
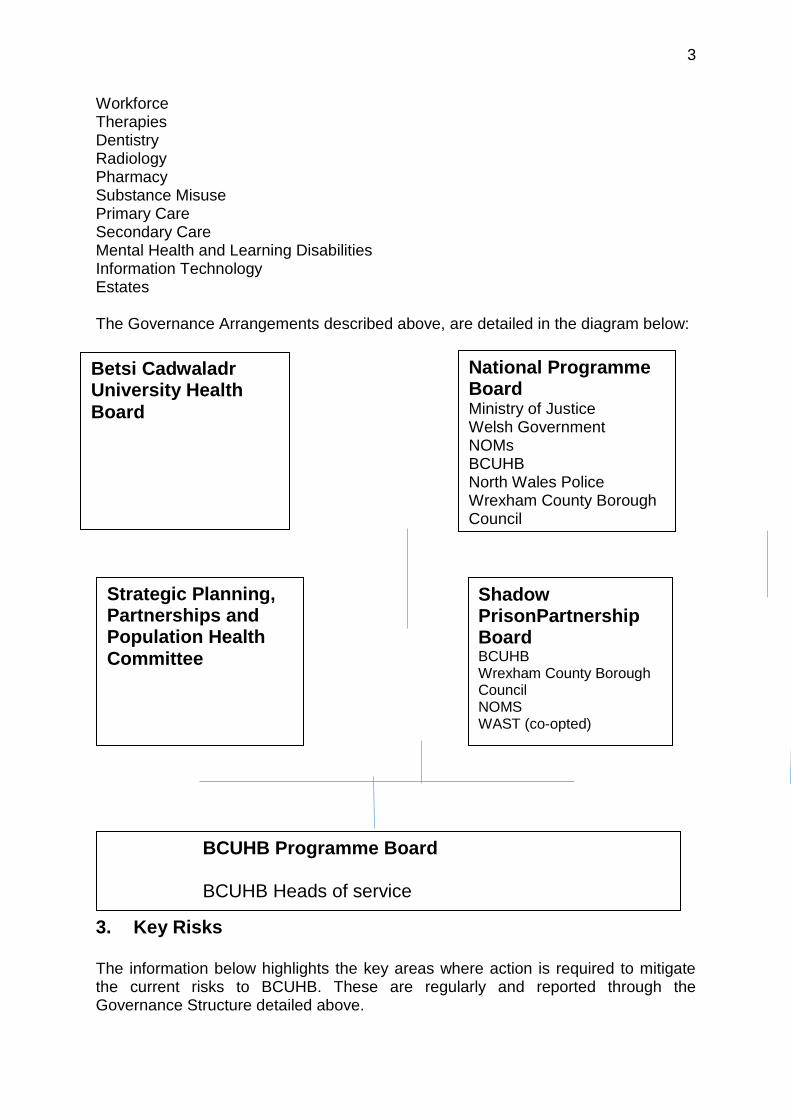
3
Workforce Therapies Dentistry Radiology Pharmacy Substance Misuse Primary Care Secondary Care Mental Health and Learning Disabilities Information Technology Estates The Governance Arrangements described above, are detailed in the diagram below:
3. Key Risks
The information below highlights the key areas where action is required to mitigate the current risks to BCUHB. These are regularly and reported through the Governance Structure detailed above.
Betsi Cadwaladr University Health
Board
National Programme Board Ministry of Justice Welsh Government NOMs BCUHB North Wales Police Wrexham County Borough Council
Shadow PrisonPartnership Board BCUHB Wrexham County Borough Council NOMS WAST (co-opted)
BCUHB Programme Board BCUHB Heads of service
Strategic Planning, Partnerships and Population Health Committee

4
3.1 Workforce The Recruitment of the Healthcare Workforce for HMP Berwyn has being identified as a Strategic risk for the Health Board for a number of reasons:
The ability of the Health Board to recruit in excess of 100 healthcare staff in
light of the well documented recruitment challenge for healthcare staff in North
Wales.
In successfully recruiting the healthcare staff required, the potential to
destabilise existing BCUHB services if the staff recruited are all existing
BCUHB staff
The capacity for shared services to conduct the required NOMS security
clearance within a limited timescale.
3.1.2 Recruitment Phases The recruitment for the prison was planned in four phases as follows: Phase 0 1st July 2016 Phase1 1st December 2016 Phase 2 1st April 2017 Phase 3 1st April 2017 These phases were established at the beginning of 2016, based on the ‘ramping up’ figures from NOMs. Our progress to date is detailed in the table below: Phase Date Year WTE % recruitment
profile
Phase 0 1ST July 2016 16/17 10.52 8.66
Phase 1 1st Dec 2016 16/17 54.5 44.87%
Phase 2 1st April 2017 17/18 31.45 25.89%
Phase 3 1st July 2017 17/18 25 20.58%
TOTAL 121 100%
Our current recruitment stands at 61 staff, so we are already at 60% of our overall recruitment, ahead of the 44.87% of our December timeline The table below illustrates the current position in terms of internal/external recruitment and provides assurance that the recruitment to the Prison has not significantly impacted upon BCUHB services. Key messages:
61 people have been recruited (offers accepted subject to employment and security checks)
54% of these are external and new appointments to BCU 46% are internal appointments 70% of all appointments are for nursing posts (registered and unregistered)
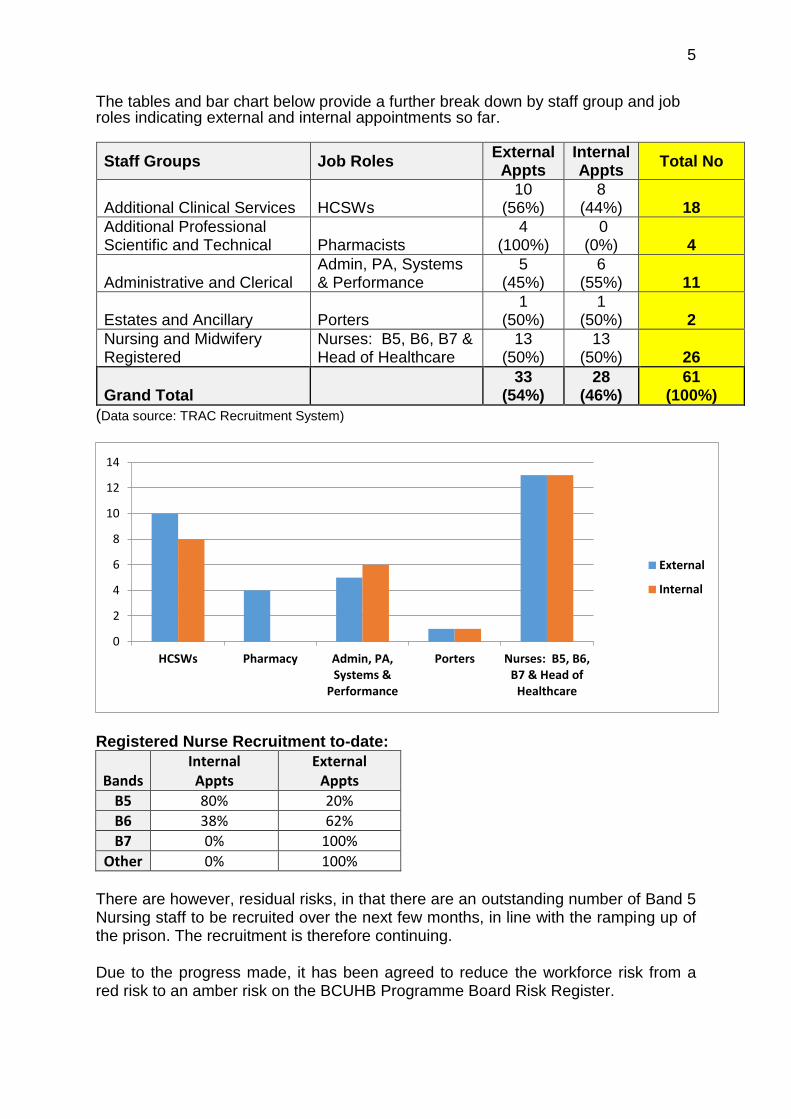
5
The tables and bar chart below provide a further break down by staff group and job roles indicating external and internal appointments so far.
Staff Groups Job Roles External
Appts Internal Appts
Total No
Additional Clinical Services HCSWs 10
(56%) 8
(44%) 18
Additional Professional Scientific and Technical Pharmacists
4 (100%)
0 (0%) 4
Administrative and Clerical Admin, PA, Systems & Performance
5 (45%)
6 (55%) 11
Estates and Ancillary Porters 1
(50%) 1
(50%) 2
Nursing and Midwifery Registered
Nurses: B5, B6, B7 & Head of Healthcare
13 (50%)
13 (50%) 26
Grand Total
33 (54%)
28 (46%)
61 (100%)
(Data source: TRAC Recruitment System)
Registered Nurse Recruitment to-date:
Bands Internal Appts
External Appts
B5 80% 20%
B6 38% 62%
B7 0% 100%
Other 0% 100% There are however, residual risks, in that there are an outstanding number of Band 5 Nursing staff to be recruited over the next few months, in line with the ramping up of the prison. The recruitment is therefore continuing. Due to the progress made, it has been agreed to reduce the workforce risk from a red risk to an amber risk on the BCUHB Programme Board Risk Register.
0
2
4
6
8
10
12
14
HCSWs Pharmacy Admin, PA,Systems &
Performance
Porters Nurses: B5, B6,B7 & Head of
Healthcare
External
Internal
6
3.2 Information Technology All Prison Health services across the United Kingdom use a Clinical information System called ‘SystmOne’. This enables clinical records to be maintained electronically and to be easily accessed, should an individual be transferred to or from, another Prison. The current ‘SytmOne’ software is being updated, and Wales will receive the updated version 3 months following implementation in England. However, there is a delay in the updating of the software, so BCUHB is now working with Welsh Government and NHS Wales Information Services to secure an alternative option. In order to provide safe clinical care, it is critical that a Clinical Information System is in place to enable the transfer of men into the prison from day one. All parties; Welsh Government, BCUHB, National offender Management Services and NHS Wales Information Services are now working closely to secure a resolution which will meet clinical safety and quality requirements for the timely opening of the prison.
3.3 Estates and Capital Equipment There have been a number of reviews of the build timeline which has impacted upon the handover timeline and the availability of accommodation for the healthcare staff who have been appointed. The project team are working closely with the Governor and his senior team to ensure that the clinical facilities are fit for purpose and that the installation of key equipment is concluded in time for the opening deadline. Due to the changes in the timeline, alternative accommodation is in the process of being secured with the support of the BCUHB Estates department, to house those staff who have already been appointed. 3.4 Finance BCUHB has secured resources to provide in-house healthcare to the Prison and access to appropriate Secondary and Tertiary services. However, as the prison is not yet open and the demand for these services is unknown, coupled with the current pressures in the secondary care system, a Memorandum of Understanding (MoU) is being established between the Health Board and Welsh Government. This MoU will provide the opportunity for BCUHB to monitor demand on Secondary Care Services and to access contingency funding should this be required. This will assist in mitigating both the financial and operational risk to BCUHB in the establishment of a new service with an unknown demand. The MoU is currently with Welsh Government for review and agreement and it is expected that this will be signed off in November 2016.
Recommendations The Committee:
Note the Governance arrangements in place to mobilise the Health service at
HMP Berwyn
Note the key risks and mitigation in delivering the Prison Health Programme
4.1 SPPH16/210 The Welsh Language Standards (Health Sector) Regulations 2016 – BCUHB Consultation Response
1 SPPH16.210 Welsh Language Standards_coversheet.doc
1
Strategy, Partnerships & Population Health Committee 24.11.16 Item SPPH16/210
To improve health and provide excellent care
Title: The Welsh Language Standards (Health Sector) Regulations 2016 – BCUHB Consultation Response
Author: Mrs Eleri Hughes-Jones, Welsh Language Services Manager
Responsible Director:
Mr Chris Wright, Director of Corporate Services
Public or In Committee
Public
Strategic Goals (Indicate how the subject matter of this paper supports the achievement of BCUHB’s strategic goals –tick all that apply)
1. Improve health and wellbeing for all and reduce health
inequalities
2. Work in partnership to design and deliver more care
closer to home
3. Improve the safety and outcomes of care to match the
NHS’ best
4. Respect individuals and maintain dignity in care
5. Listen to and learn from the experiences of individuals
6. Use resources wisely, transforming services through
innovation and research
7. Support, train and develop our staff to excel.
Approval / Scrutiny Route
Following discussion and scrutiny at the Board Development session on 6 October 2016 and at the Strategy, Partnership and Population Health Committee on 10 October 2016, comments received were taken into account and reflected in the final response. Final approval and sign off was granted by the Chief Executive, with the response sent to Welsh Government on 17 October 2016.
Purpose: The Welsh Government held a consultation on the draft Welsh Language Standards Regulations for the health sector. The purpose of the consultation was to seek views on the draft Regulations to specify Welsh Language Standards for the health sector. These Regulations will enable the Welsh Language Commissioner to place duties in relation to the Welsh language on NHS Wales local health boards, National Health Service trusts in Wales, Community
2
Health Councils, the Board of Community Health Councils in Wales, and the NHS Business Services Authority. Following a thorough internal consultation process, views and evidence provided by the workforce was taken into account in forming the final response. This paper presents the Health Board’s response to the draft regulations, with the comments provided outlining any concerns in terms of the reasonability and proportionality of the draft regulations.
Significant issues and risks
There are inherent legislative risks in the case of any failures to deliver the Welsh Language Standards. These are to be managed and mitigated as part of detailed implementation arrangements to ensure there is no detrimental impact on the quality and safety of services.
Special Measures Improvement Framework Theme/ Expectation addressed by this paper
http://www.wales.nhs.uk/sitesplus/861/page/81806 N/A
Equality Impact Assessment
No EqIA is considered necessary for this paper.
Recommendation/ Action required by the Committee
The Committee is asked to note this paper for information.
Disclosure: Betsi Cadwaladr University Health Board is the operational name of Betsi Cadwaladr University Local Health Board
Committee Coversheet v10 June 2016
2 SPPH16.210 Welsh Language Standards Health Sector Regulations - BCUHB Response.doc
The Welsh Language Standards (Health Sector) Regulations 2016
Betsi Cadwaladr University Health Board’s
Consultation Response
October 2016
2
Welsh Language Standards (Health Sector) Regulations Betsi Cadwaladr University Health Board welcomes the opportunity to respond to the Welsh Government’s consultation on the Welsh Language Standards Regulations for the Health Sector in Wales.
The Welsh Language (Wales) Measure 2011
The Health Board fully supports the premise of the Welsh Language Standards under the Welsh Language (Wales) Measure 2011. The draft regulations afford clarity in terms of their purpose in delivering the new legislative framework in Wales . The Health Board is in agreement that the regulations need to reflect the Measure’s principles of ensuring that standards placed on organisations are “reasonable” and “proportionate”. This needs to be taken into account when forming, placing and delivering the regulations.
Internal Consultation Process In order to ensure a cross-section of perspectives across the organisation has been taken into account, a robust internal consultation process has been undertaken by the Health Board. All members of staff have been afforded the opportunity to comment on the standards and whether they would affect current practices within their own service areas. A specific e-mail account was created to gather comments, information and views to inform the Health Board’s response. Specific specialist services were also targeted with tailored workshops held with clinical functions across Secondary Care Services. Workshops were also held with community teams, as well as Mental Health Services. A specific workshop was held with the Board, with corporate workshops held with the Workforce and Organisational Development Department focusing on key areas within the Standards, as well as engagement with the Estates and Procurement Services. A Welsh Language Roadshow was also taken across all acute and community hospitals to ensure operational staff delivering services on the ground were afforded the opportunity to share their expert knowledge and experience.
Consultation Response This process has ensured that the Health Board was able to explore all avenues in its approach to the delivery of the regulations and this collated response reflects the outcomes of all discussions. This response includes comments received as part of our local consultation and therefore reflects the views, experience and perspectives offered by medical, clinical, administrative and corporate individuals and groups.
Existing arrangements and initiatives that address the implementation of the standards
Progressive work has been ongoing since the establishment of Betsi Cadwaladr University Health Board in 2009 to plan, deliver and improve services to its Welsh speaking patients. Since the launch of the Welsh Government’s first Strategic Framework for Welsh Language Services in Health, Social Services and Social Care, ‘More than just words’ in 2012, the “Active Offer” principle has been at the forefront of the Health Board’s activities, with the follow-on framework mainstreamed into the planning and commissioning of services. The Health Board welcomes the fact that the standards have been aligned with the objectives set out within ‘More

3
than just words’. In light of this, the Health Board would like to draw attention to some examples of initiatives and work undertaken that has already paved the way for the implementation of the standards.
Derwen – Integrated Team for Disabled Children
This example demonstrates service delivery compliant with Standards relating to case conferences (Standard 26)
The services provided by Derwen in Gwynedd provides intervention and support in responding to referrals for assesments / provision. Responsibility for provision lies with the health organsiation and local authority. In order to ensure a sufficient baseline to guarentee a formal agreement between the two organisations, Language Guidelines were produced and formally approved to ensure equal responsibility and accountability for providing the best possible service for patients. As a result, Derwen developed arrangements that would allow service users to receive intervention in their first language. The guidelines focused on delivering services, providing information, staff recruitment, supporting current staff as well as ensuring bilingual meetings via simultaneous translation services as required. The success of this arrangement ensured seamless bilingual provision for one of the most vulnerable patient groups.
Bilingual Skills Strategy
This strategy supports the Health Board in implementing Standards relating to a body developing Welsh language skills through planning and training its workforce (Standards 137-147) and Standards relating to a body recruiting and appointing (Standards 148-152)
The Bilingual Skills Strategy is designed to enable effective workforce planning and the recruitment of staff to ensure the delivery of bilingual services through the medium of Welsh and English, according to individual choice and the needs of the population in the area. To deliver this, the Bilingual Skills Strategy has four key workstreams to ensure that appropriate Welsh language skills are available within the workforce to deliver a bilingual service:
Audit of current workforce Welsh language skills
Assessment of the Welsh/bilingual service needs
Identifying skills gaps
Workforce planning and recruitment
The objective is to provide a service that satisfies the needs of Welsh speakers and their families or carers, by ensuring that they can receive services in their own language and the Bilingual Skills Strategy ensures that the Health Board is taking a forward planning approach to mainstreaming the standards’ requirements into its internal processes.
Identify Patients’ Language Choice
4
This initiative supports the Health Board in delivering the Standards relating to recording patients’ first language.
In view of the challenges posed through the limited functionality of ICT Systems, the Health Board has been pro-active in developing local initiatives to identify patients’ first language. The ‘Speaking Welsh’ emblem magnets are placed on patient white boards on the ward so that staff are able to identify Welsh speaking patients within their local area. This allows the ward to plan its workforce so that Welsh speaking staff are paired with Welsh speaking patients. This ‘opt in’ system has also ensured that large ‘Speaking Welsh’ magnets are displayed above a patient’s bed. This has also helped in ensuring that teams based away from the Ward (e.g. physiotherapists, pharmacists and the wider clinical workforce) to plan their care to meet a patient’s language needs. This was initially piloted on two wards in Ysbyty Gwynedd with dementia patients, and the aim now is to roll out to other wards and community hospitals.
Training Provision
The Health Board’s current Welsh language training provision ensures compliance with:
Standard 141: You must provide opportunities during working hours – (a) For your employees to receive basic Welsh language lessons, and (b) For employees who manage others to receive training on using the Welsh
language in their role as managers
Standard 142: You must provide opportunities for employees who have completed basic Welsh language training to receive further training, free of charge, to develop their language skills. The Health Board has always offered staff opportunities to develop their Welsh language skills, either through internally produced/delivered courses or by sending staff on courses in the community. Courses have also been offered to senior staff to develop their Welsh language skills in their role as a manager. In order to provide further support for staff, the Health Board is currently in the process of recruiting a Welsh Language Tutor which will provide flexibility in increasing the level of training that we are able to offer to our staff.
Primary Care Providers Partnership working developed with many primary care providers supports and encourages compliance with Standards relating to primary care (Standards 83 – 97).
Following a concern raised in 2014 regarding the provision of bilingual prescriptions, the Health Board pro-actively responded to resolving the issue. A project was developed collaboratively between the Health Board and Bangor

5
University to provide cautionary instructions on prescribed medicines, for the first time, in Welsh. This innovative provision, endorsed by the Chief Pharmaceutical Officer for Wales, now ensures that bilingual labels on prescription medicines are available to patients. A team comprising of language specialists and pharmacists has made the first step by translating 30 cautionary instructions given to patients on prescription medicines. These will now become available to all pharmacies and doctors, increasing the amount of health support provided in Welsh within the NHS in Wales. The labels are available in the online edition of the British National Formulary, the standard pharmaceutical reference text used by prescribers, nurses and pharmacists within the NHS, and has appeared in the printed edition. A further example of pro-active working within primary care is the partnership established with Bron Derw Medical Centre in Bangor, with the Practice Manager actively working with the Health Board’s Welsh Language Team to provide bilingual correspondence to its patients. The Centre makes full use of the Health Board’s Translation Team to ensure letters, information and pamphlets are provided bilingually. The Centre has also undertaken a data cleanse project to update patients’ medical records, asking patients to update their language details. Forms were provided to patients in the surgery to encourage them to note their spoken language and preferred language of care. Posters were also displayed at reception to inform them that a Welsh language service was available, whilst ensuring visibility was given to the Welsh language in the form of the Welsh Language Commissioner’s ‘Working Welsh’ resources. Work has also been undertaken with the Centre to develop a bilingual website to improve accessibility for patients in their first language.
Welsh Language in Healthcare Awards
The Health Board received eight awards at the last Welsh Language in Healthcare Awards. Derwen, the Integrated Team for Disabled Children won the award for ‘Work done with priority groups’ for the creation of, ‘May I join you?’, a bilingual booklet to support parents in developing their children’s needs. In the ‘Working in Partnership Category’ the Gyda’n Gilydd Team, bringing together Gwynedd Council’s Early Years Unit, the Health Board, Barnados and Citizens Advice was awarded for providing a wide range of preventative services bilingually to families in Gwynedd. Denbighshire’s Single Point of Access provision between Denbighshire County Council and the Health Board, including British Red Cross were also successful in the same category for developing an integrated model of community services for preventative and rehabilitation work for adults. The Health Board also received two awards in the ‘Technology and the Welsh Language’ category for the innovative fully Bilingual Appointment Reminder Service and The North Wales Cancer network Patient Forum for an online bilingual cancer information resource. Three members of staff were awarded Welsh Leaners of the Year titles for learning Welsh to an exeptional standard.
The Health Board recently collaborated with Menter Iaith Bangor to hold a Primary Care Conference for local providers to raise awareness about the standards, ‘More than just words’ and the support that is available to providers.

6
Implementation and monitoring of the standards The Health Board has already developed its Welsh Language Strategic Plan for 2016-2019 which sets out its direction and approach for the next three years by providing a framework of support to ensure organisation-wide ownership and planning for the delivery of the Welsh Language Standards and ‘More than just words’. Our strategic plan is built around three dimensions :
Strategic Intervention has set the vision for the Health Board going forward, ensuring we are working towards the same goal through workforce and service planning.
Behavioural Change ensures that the Health Board creates a context that encourages and supports staff to use their language skills.
Performance and Monitoring will ensure that the standards and ‘More than just words’ remain a live work in progress through a continuous cycle of monitoring, with actions set and measured against to allow for clear reporting and evidence of compliance.
The strategic plan aligns to the standards, and internal action plans and control systems are in place as we develop more comprehensive bilingual service provision for our patients and our staff.
National leadership and support In order for health sector organisations to achieve certain standards, there are a number of specific issues that will require Welsh Government intervention and support:
Information and Communications Technology Systems There are four systems that will require the health sector to record the language choice of either the public, our patients and staff. The systems utilised within the health sector to capture such data include:
Patient Administration Systems
GP Referral Systems
Electronic Staff Register System (ESR)
E-rostering System
Not all systems have the facility to record language of choice. These systems are designed and controlled nationally and therefore require an all Wales solution if they are to be fit for purpose. The Health Board has a pro-active Informatics Team which is already raising these issues in national forums. However, the Health Board will require the Welsh Government’s leadership and directive if these issues are to be addressed and resolved.
Professional Education

7
There is a national challenge in relation to both the recruitment of clinicians in some specialities which, in relation to the Standards, is further exacerbated by a general shortage of Welsh speaking clinical practitioners. This concern was also previously raised as part of the Health Board’s response to the Welsh Government’s follow-on Strategic Framework for Welsh Language Services in health, Social Services and Social Care, ‘More than just words’. A national focus is needed to identify ways of increasing the number of Welsh-speaking graduates in Welsh higher education establishments and retaining them in NHS Wales or encouraging and incentivising Welsh-speakers to return to Wales if they have studied elsewhere in the UK. Whilst the Health Board would always want to ensure that patients, families and staff were communicated with in their first language without such an intervention there will be significant challenges to delivery of the standards.
Resources
The Standards will have potentially significant financial consequences for the Health Board which will need to be considered in relation to annual central budget setting if additional financial pressures are to be avoided. Similarly, there is a finite level of internal and external translation support and simultaneous translation availability which will have an impact on the ability of organisations to fully meet the proposed Standards. Therefore, a phased introduction of the Standards is suggested to ensure that the necessary resources and systems could be developed over time to avoid a potentially major impact on the timely delivery of services.
Introductory comments There are 185 standards in total, and the Health Board welcomes the principle of each standard and believes them to be an extension of current bilingual provision. There are a number of areas where challenges to implementation have been recognised. In formulating this response an effort has been made to reflect the views of front line staff and put forward constructive alternative suggestions in terms of the framing of the legislative requirements.
SCHEDULE 1 – Service Delivery Standards The Health Board welcomes these standards and, for the most part, believes that the draft regulations reflect and build upon current practices already established through our Welsh Language Scheme under the Welsh Language Act 1993.

8
The following comments were received as part of the Health Board’s internal consultation process and have been included to provide an overview of the perspectives of members of staff from a wide variety of backgrounds, both clinical and administrative. Standards relating to correspondence sent by a body (Standards 1-7)
Achieving the aim of the standard
Standard 2: When you correspond with an individual (“A”) for the first time, you must ask A whether A wishes to receive correspondence from you in Welsh, and if A responds to say that A wishes to receive correspondence in Welsh you must:
(a) keep a record of A’s wish, (b) correspond with A in Welsh when corresponding with A from then onwards,
The Health Board welcomes this standard in that correspondence sent out by an organisation should be bilingual. As described above, not all patient administration systems currently have the facility to record language choice which is a barrier to successful implementation without a significant bureaucratic and administrative impact.
The Health Board is implementing a systems upgrade on a phased roll out across the three geographical areas commencing November 2016. Within the new Welsh Patient Administration System (WPAS) system there will be the functionality to be able to draw staff attention to any sensory loss requirements for patients. The WPAS system is replacing the current PAS system in Central, and will eventually be rolled out to East and West replacing their current systems also, which then would allow us to be able to add in this flag for patients across the board. This is one area that will require national action to ensure clinical systems incorporate language of choice.
Concerns were raised as part of the internal consultation process regarding the transferring of this information from one function or service to another, e.g. this information would not be held by medical secretaries directly involved in individual patient correspondence and care. In terms of practicality, feasibility of translation capacity was raised as a potential challenge, namely individual follow up letters that are sent to patients on an extremely large scale following all patient appointments. For example, approximately 4700 appointment letters (excluding follow-up letters) are sent out across the Health Board on a daily basis. This information is limited to main patient administration systems and does not include other services such as oncology, palliative care and haematology, radiology, all therapy services and audiology across North Wales. In relation to outpatient follow-up letters, approximately 3000 letters are sent to patients and their GPs on a daily basis across the organisation. The translation workload for these letters alone could range from 500,000 – 1,500,000 per day. Capacity is of concern here as it would be problematic to deliver this service without taking into account the timely despatch of important clinical information.
9
Current practice and achievements
Initial correspondence to one or more individuals is currently bilingual with all outpatient appointment letters and general correspondence for the public being bilingual. All correspondence received by the Health Board in Welsh automatically receives a Welsh response.
Work ongoing to achieve the aim of the standard
Work is currently ongoing to standardise letters for the new WPAS to ensure consistency in all initial outpatient and inpatient appointments. Currently not all inpatient letters are sent out bilingually, and the Health Board is eager to ensure this development is implemented. In terms of the WPAS functionality, there is no short term solution for this element. There are national policy and legal requirements concerning the collection of data around accessibility, language and protected characteristics. Therefore, a nationally led policy drive is required to enable NHS business processes to capture these. Such requirements could then be mapped and built into IT systems. For example, there is a single GP registration form for Wales. If this was amended to include a number of these requirements, and then the GP system, Welsh Clinical Communications Gateway (WCCG) and WPAS were amended to record them, we would have a national approach which could also be quantified and measured. The Health Board has a pro-active Informatics Team which is already raising these issues in national forums. Whilst the Health Board would aspire to produce all patient correspondence in the language of choice there are a number of risks to delivery:
The volume of clinical correspondence from follow up appointments
The capacity of translation services (internal and external)
The need for timely information to be provided to patients and families
The gaps in IT systems described above
Standards relating to telephone calls made and received by a body (Standards 8-21)
Achieving the aim of the standard
Standard 20: When you telephone an individual (“A”) for the first time you must ask A whether A wishes to receive telephone calls from you in Welsh, and if A responds to say that A wishes to receive telephone calls in Welsh you must keep a record of that wish, and conduct telephone calls made to A from then onwards in Welsh.
Comments received as part of the Health Board’s internal consultation process identified challenges in relation to how this information would be captured and

10
transferred at a later stage between different clinical areas which do not have a common medical records system.
Current practice
The Health Board currently strives to ensure that staff greet callers bilingually. Work has been undertaken in recent months to further support this element, with specific ‘bilingual greeting’ cards having been produced and distributed to staff across the Health Board. Reminder notices have also been sent via weekly noticeboard messages to ensure staff are aware of their requirement. Betsi Cadwaladr Community Health Council has undertaken a mystery shopper exercise, monitoring the Health Board’s compliance in this area. A further audit is to be conducted focusing on reception and ward areas during the latter part of 2016. Evidence will be used to identify areas of non-compliance with further work then being done to support and strengthen the service.
Additional comments
The Health Board has additional comments in relation to the standards below. Standard 9: When a person contacts you on your main telephone number (or numbers), or on any helplines numbers or call centre numbers, you must inform the person that a Welsh language service is available. Standard 17: When there is no Welsh language service available on your main telephone number (or numbers), or to any helpline numbers or call centre numbers, you must inform persons calling, in Welsh (by way of an automated message or otherwise), when a Welsh language service will be available.
The Health Board is disappointed in the fact that these standards are potentially a retrograde step in terms of what is currently being offered, as a Welsh service should be available at any time. A bilingual greeting adequately informs the caller that a bilingual service is available. It is felt the standards as currently written risks treating the Welsh language less favourably, which is in direct contrast to one of the core aims of the Measure. It is suggested that the above standards be removed from the final regulations.
Standards relating to a body holding meetings that are not open to the general public (Standards 22-24)
Achieving the aim of the standard Standard 22: If you invite one person only (“P”) to a meeting, you must offer to conduct the meeting in Welsh; and

11
if P informs you that P wishes for the meeting to be conducted in Welsh, you must conduct the meeting in Welsh (without the assistance of a simultaneous or consecutive translation service).
A number of individuals and staff groups voiced concern in relation to one aspect of the above standard as part of the Health Board’s internal consultation process. It was noted that many meetings are conducted regularly within various departments and services, with some requiring specialist knowledge and expertise. Not all individuals are Welsh speaking and in order for these meetings to go ahead, simultaneous translation would be required to facilitate discussions.
Proposed approach to meet the standard
The Health Board currently provides simultaneous translation services at public meetings and conferences to ensure that non-Welsh speakers are able to participate in the discussions. The Health Board would like to emphasise that this current practice does not in any way undermine the activity taking place as it ensures engagement and participation from all individuals, both Welsh speakers and non-Welsh speakers. The use of simultaneous translation at meetings demonstrates the same level of commitment, and allows the meeting to be held bilingually, with no detrimental effect on the service. This would also ensure that the appropriate individuals are able to present at meetings. The Health Board welcomes this standard of offering participations in Welsh or English at all defined meetings. To support delivery of the Standard it is therefore suggested that the clause “without the assistance of a simultaneous or consecutive translation service” be removed from the final regulations.
Standard relating to clinical consultations (Standard 25)
Achieving the aim of the standard Standard 25: When an individual (“A”) attends a clinical consultation carried out or provided by you for the first time you must— (a) ask A whether A wishes to receive Welsh language support at the clinical consultation, (b) if A informs you that A wishes to receive Welsh language support at the clinical consultation, keep a record of that wish, and (c) provide Welsh language support to A at clinical consultations from then onwards (unless you carry out or provide the clinical consultation in Welsh).
Welsh language ‘support’ is defined as “providing support in the Welsh language to an individual to ensure that the individual understands what is happening during the clinical consultation (for example by providing a Welsh speaking member of staff to check in Welsh that the individual understands what has been said or to explain in Welsh what has been said or by providing a translation service).”
This standard has led to complex and detailed internal discussions. Specific feedback was requested from multiple specialities within multiple settings where clinical consultations would take place. The following is a general overview of the comments received: Clinical risk

12
Concerns were raised that information and clinical nuances could be lost in translation, especially if the individual providing the ‘support’ was not clinically qualified to be able to understand what is being conveyed to the patient. Despite Welsh language ‘support’ not being defined as a translation service, there still remains a risk in accurately interpreting what has been said by the clinician bearing in mind that clinical advice is often complex, with different meanings and understanding leading to potential misunderstanding in terms of the outcome of the consultation, or severity of what has been discussed. This could impact on the patients’ understanding of the full implications of their diagnosis and future plans for care. There is also a concern that the clinician would not know whether his advice has been interpreted correctly in line with professional guidance.
Some members of Welsh speaking staff would not feel confident in delivering this service in Welsh as they don’t think their Welsh would be good enough. Also, some non-clinical staff would not feel comfortable in certain situations that are unfamiliar to them.
This would lead to additional pressure on clinical staff, and on other services if Welsh speakers were to be called upon to assist in delivery. As this is outside current Job Descriptions and responsibilities, the Health Board would not be able to enforce this on individual members of staff as it would mean that they would be working outside their capabilities.
Volume of appointments
There are approximately 1000 daily outpatient appointments in the West area alone. The Health Board would not be able to ensure Welsh speaking members of staff in each individual appointment or clinic. Taking into account the demographics of the local area, Gwynedd alone has 65% Welsh speakers therefore we would be looking at the possibility of 65% of outpatients activity in Gwynedd requiring Welsh speakers on a daily basis. This would not be practical or financially possible to arrange simultaneous translation for consultations.
This is without taking into consideration inpatient requirements – operations, ward rounds / consultations, pre-op, assessments, therapy and home visits.
Workforce capacity
In terms of recruitment, there are current challenges across the organisation with certain speciality posts which are very challenging to recruit to in terms of both medical and nursing vacancies. The health sector operates in an international recruitment market and healthcare workers are sought across the world.
Although the demand for Welsh language support in clinical consultations may be lower in the Central and East areas in line with the local demographics, it is also known that there are fewer Welsh speaking members of staff which would make it more difficult to ensure appropriate members of staff were available to deliver this standard across the organisation. These figures demonstrate the percentage of fluent Welsh speakers (Levels 4 and 5 in line with the Association of Language Testers in Europe Framework):
Region Level 4 Higher
Level 5 Proficiency

13
Across Total 6.40% 10.64%
Central Total 2.48% 8.01%
East Total 2.37% 2.99%
West Total 21.55% 22.06%
Grand Total 8.31% 10.80%
This is the current situation across the Health Board and will take time to increase these figures according to workforce planning, Welsh language training provision and professional education.
Staff availability in clinical settings can prove problematic, and therefore there would need to be reliance on non-clinical staff at times which again raises the issue of clinical safety.
Wider obligations of conducting Welsh medium consultations
The remit of this standard is unclear in terms of what is encompassed in ‘clinical consultation’, and whether there is reference to assessing, diagnosing and treating patients. As such, valid informed consent through the Welsh language would need to be taken into consideration, as well as using validated assessing measures e.g. dementia measures, Speech and Language Therapy assessments etc where communication is essential. Despite excellent work having recently been implemented in the translation and validation of cognitive dementia assessment tools, it is important to take into account that there is still a lack of such measures across Wales.
Consultant-Patient Relationship
A number of consultants have expressed concern regarding the presence of an additional individual in the dialogue between them and the patient. It was noted that 85% of patient-consultant interaction is via body language, facial expressions and eye contact. In involving a third person these crucial aspects of assessing and diagnosing patients would be lost, adversely affecting the care and treatment provided.
Record keeping
In line with the comments in the first two sections in relation to recording language choice via the Health Board’s internal systems infrastructure, the element within this standard of keeping a record of a patient’s wish to receive Welsh language support at clinical consultations and act upon it would prove problematic. See comments above with regard to written correspondence and telephone communications.
Training the workforce
Standard 140 states that “organisations must provide training (in Welsh) on using Welsh effectively in clinical consultations”. This is a very wide and vague request in terms of what level of training would be required and who would provide the training (a tutor isn’t clinically qualified, and a clinician is not educationally qualified).
Other considerations
During extensive discussions and workshops, other avenues were explored:

14
Differentiating between unscheduled care and scheduled care
Certain members of staff noted that facilitating this standard within scheduled care would be more achievable due to appointments and treatment being planned in advance. Challenges within unscheduled care would mean an inability to guarantee Welsh speakers being available at short notice in an emergency situation.
Although the Health Board would be eager to explore the scheduled care element further, concerns still remain as to the practicalities of how this would be implemented, delivered and monitored. System constraints in recording and transferring the information, as noted above, would prohibit the consistency of provision.
Focus on vulnerable groups
A proposal was also explored to focus this standard on the vulnerable groups of children and young people, mental health service users, people with learning difficulties and people with disabilities. Despite acknowledging the importance of providing support to vulnerable groups, the same issues of clinical risks and lack of capacity within these specialist service areas were highlighted as common problems.
Proposed approach
It was noted that this practice already exists in some areas within the Health Board but delivered on an informal basis. Some healthcare professionals (predominantly nurses and senior nurses) who routinely assist patients in clinical appointments note that this naturally occurs in certain situations and areas. However, this occurs when there are Welsh speaking members of staff on duty, and is not a uniform approach across all services or functions. Staff aren’t able to ensure that all patients are offered this service, and in enforcing this standard, the Health Board is concerned that this may not be practically possible in all situations. The Health Board is required to comply with the Welsh Government’s Follow-on Strategic Framework for Welsh Language Services in Health, Social Services and Social Care 2016-2019, ‘More than just words’, with the core principle of the framework being the “Active Offer”. This framework has a patient centred approach, with the actions fully embedding requirements in the planning, commissioning, contracting and delivery stage of services. In focusing its efforts on the delivery of the “Active Offer” to improve patient experience, we are working to increase the linguistic capacity of our workforce, which will increase the availability of Welsh language support. The original ‘More than just words’ framework brought about the development of a number of initiatives which showed how it was possible to ensure that Welsh speakers can receive health and social services in their first language by making the best use of existing skills and resources. Rather than focusing on the individual, the Health Board proposes that the standard focuses on planning its workforce accordingly. Services could aim to ensure, through the E-rostering system, that the Welsh language skills of staff is recorded and taken into account when creating rotas. Local directories could be created so that staff are aware of who speaks Welsh within their immediate service area. It will ensure that organisations operate in a consistent manner by mainstreaming Welsh language services as an integral
15
part of their service delivery and workforce planning. There needs to be a balance between the determination and drive to provide this service, but also the elements of clinical risks, pragmatism and practicality. Therefore the Health Board proposes that this standard in its current form is amended to enforce organisations to plan its workforce to ensure that there are Welsh speaking staff on duty to be called upon in such circumstances. This would be reinforced by the objectives relating to workforce planning and the “Active Offer” within ‘More than just words’ and supported through the Health Board’s implementation plans. Whilst the Health Board supports the aim of the Standard as currently drafted there are a number of issues raised during the internal consultation that highlight potential risks. It is felt that to mandate this Standard immediately from the introduction of the regulations would present significant challenges and a distinction should initially be made between unplanned/emergency episodes of care (when the primary aim is to provide potentially life-saving care when Welsh language support may not be immediately available) and planned care where every effort is already made to provide language support.
Standard relating to a body producing and publishing documents (Standards 37-47)
Current practice
Standard 37: Any agendas and minutes you produce that are available to the public, which relate to Board, Trust, Authority or Council meetings must be produced in Welsh.
The Health Board currently translates its monthly public Board agenda and minutes, as well as its bi-monthly Stakeholder Reference Group agenda and minutes. Simultaneous translation is also provided at these meetings.
Other considerations
The Board has ten sub-committees relating to its business. Based on a standard agenda being 200 words, with standard minutes approximately 3500 words, and in line with frequency of meetings, the number of additional words to be translated per annum would be a minimum of 210,900. Submission and governance turnaround of papers for Committees are also areas that would present significant challenges. Firstly, there is a risk there would not be adequate capacity to translate this additional number of words within the timescales needed for Committee work to be conducted in a timely way. Secondly, due to the anticipated volume, much of the translation work would need to be outsourced at additional financial cost to the Health Board.
Alternative Proposal
The standards relating to simultaneous translation being available at all meetings held in public would ensure that proceedings were conducted bilingually.
16
In light of the potential implications of this draft standard it is suggested that the implementation is phased – with agendas only being translated initially and minutes following in the second phase to give the opportunity for additional internal and external translation support to be in place.
Standards relating to a body receiving visitors at its buildings (Standards 60-63)
General comments
The Health Board would like to draw attention to an issue highlighted in relation to the below standard: Standard 63: You must ensure that staff at the reception who are able to provide a Welsh language reception service wear a badge to convey that.
Concern has been expressed regarding the enforcement element of wearing a badge or lanyard to denote Welsh speakers. Whilst the intent is fully supported some Welsh speaking staff believe that it should be up to individual choice.
Proposed alternatives
The Health Board suggests that the standard be amended in line with Standards 147 and 147A to respect individual beliefs: Standard 147 You must make available to members of staff who are able to speak Welsh a badge for them to wear to convey that. or Standard 147 You must promote to members of staff the wearing of a badge that conveys that a member of staff is able to speak Welsh
Standards relating to primary care (Standards 83 – 97)
Current practice
The Health Board welcomes the inclusion of the primary care standards in their current form and believes that the requirements reflect the findings of the Welsh Language Commissioner’s Inquiry into Primary Care Services, ‘My Language, My Health’. The Health Board has been pro-active in the development of close working partnerships with the contractors and their staff. See page 4 for examples. Encouragement and support is provided in the delivery of bilingual service in terms of
language awareness, resources and sporadic translation provision. The Health Board believes that these set of standards would strengthen and build upon its current work programme and relationships already established with certain primary care providers.

17
Additional comments in relation to primary care services
Following detailed discussions at a national level, the Health Board is encouraged that these standards reflect the concerns expressed if standards were to be placed on primary care providers directly via local health boards. Within the Health Board’s region, there are currently:
114 GP Surgeries
83 Opticians
91 Dental Surgeries
155 Community Pharmacies The Health Board currently does not have the capacity to deliver and monitor this at such a large scale. However, the Health Board is of the opinion that primary care services should be held to account on certain aspects of bilingual service delivery rather than enforcement via health boards. Providers are expected to comply with other legislated requirements such as health and safety and equalities and it is felt that Welsh language legislation should not be treated differently. Despite GP Referral Systems also having a first language field, many primary care providers are not aware of its existence and the field is not mandatory. Discussions have been held as to how this information would be best captured, and suggestions proposed that the demographics section on systems would be more accessible for practices. This issue requires attention and development at national level but would also require a seamless transition, starting with GP practices, rather than at the secondary care stage. This information would then also facilitate Health Boards to review the way preferred language is utilised in service planning and delivery, with the aim of actively providing better care for patients.
SCHEDULE 2 – Policy Making Standards
General comments
The Health Board welcomes these set of standards, and would like to provide evidence to support its position. The Health Board already assesses all policies, new or revised, for effects on the Welsh language as required by our Welsh Language Scheme. We do however acknowledge that the scrutiny levels currently in existence require strengthening to ensure policies are also assessed for the opportunity or lack of opportunity to use the Welsh language, as well as treating the Welsh language no less favourably. The Health Board welcomes the addition of these requirements and has already put actions in place to address these standards. It must also be noted that a number of NHS policies are developed on an all Wales basis and would require intervention at a national level.
18
SCHEDULE 3 – Operational Standards
The Health Board fully acknowledges and embraces the opportunity for individuals, whether employees or members of the public to have the freedom to use the Welsh language. Certain aspects of these set of regulations are new to the Health Board and will require a transitional period of streamlining its current processes. However, this is a very positive step forward and will lead towards greater use of the language in every day life. Standards relating to the use of Welsh within a body’s internal administration (Standards 108-121)
General comments and actions required – Standard 114
The Health Board has concerns in relation to the below standard. Standard 114: You must ask each employee whether he or she wishes to receive any forms that record and authorise— (a) annual leave, (b) absences from work, and (c) flexible working hours, in Welsh; and if that is an employee’s wish, you must provide any such forms to him or to her in Welsh.
The Health Board has a long establish procedure to provide annual leave request forms and absences from work forms in Welsh. However, this ‘paper format’ has now been replaced and the Health Board is moving to a full roll-out of an IT based staff information system - the National Electronic Staff Register (ESR). This is an English based NHS System and therefore there is currently no Welsh functionality. This is also the case with the E-rostering system which is used to plan staff shifts. National support for the implementation of bi-lingual functionality on both these systems would be required to facilitate implementation of the Standard as drafted (as described above). These issues have been raised at all Wales meetings by pro-active members of the Health Board’s Workforce and Organisational Development Department but an agreed way forward has yet to be determined. The Health Board would be more than happy to lead on this with national support.
General comments and actions required – Standards 115-121
Standards 115-121 states that any policies published in English, must also be published in Welsh. A number of the NHS policies are developed on an all Wales basis and would therefore require translation at an all Wales level. Locally produced policies would incur a substantial translation cost which would be difficult to meet in the current financial climate. In terms of bilingual services, the emphasis has always been on translation.
19
However, there is more to bilingual provision than written translation. The requirements to ensure Welsh language is taken into consideration as part and parcel of forming policies, rather than the policy itself being in Welsh, is fundamental, and that is why the Health Board is encouraged by the inclusion of Schedule 2 in relation to ‘Policy Making Standards’.
Standards relating to complaints made by a member of a body’s staff (Standards 122-125) and Standards relating to a body disciplining staff (standards 126-129)
Achieving the aim of the standards
The Health Board wishes to draw attention to concerns raised by some members of staff as part of the internal consultation process. Standard 123: If you receive a complaint from a member of staff or a complaint about a member of staff, and a meeting is required with that member of staff, you must—
(a) offer to conduct the meeting in Welsh, and (b) if the member of staff wishes for the meeting to be conducted in Welsh, conduct the meeting
in Welsh (without the assistance of a simultaneous or consecutive translation service).
Standard 127: If you organise a meeting with a member of staff regarding a disciplinary matter that relates to his or to her conduct you must—
(a) offer to conduct the meeting in Welsh; and (b) if the member of staff wishes for the meeting to be conducted in Welsh, conduct the meeting
in Welsh (without the assistance of a simultaneous or consecutive translation service).
Meetings in relation to concerns and disciplinary procedures are conducted within various departments and services, with some requiring specialist knowledge and expertise. In these circumstances, there would also be a requirement for Trades Union representatives to be present at these meetings. In such circumstances, the Health Board currently strives to ensure that staff are provided with the opportunity to use the Welsh language. In terms of investigations, the Health Board has 11 External Disciplinary Investigation Officers, of which 3 are Welsh speakers. Taking into account the number of disciplinary procedures held on an annual basis, it would be difficult to ensure Welsh speakers were allocated to all staff wishing to conduct such meetings in Welsh. This would incur a delay in the process, with an average case turnaround of 140 days. Not all individuals are Welsh speaking and in order for these meetings to go ahead, it would be impossible to do so without the assistance of simultaneous translation.
Proposal to achieve the aims of the standards
The Health Board welcomes this standard and will continue with current practice to try to ensure Welsh speakers are available at every opportunity. However, in the rare cases where this is not possible, the Health Board believes that the use of simultaneous translation is needed to support the individual and other parties
20
involved, and would like to emphasize that this would not in any way undermine the activity taking place and would ensure both Welsh speakers and non-Welsh speakers were able to participate accordingly. The member of staff would still be subject to the same rights, having such meetings conducted in Welsh, and the use of simultaneous translation at meetings demonstrates the same level of commitment, and allows the meeting to be held bilingually, with no detrimental effect on the service. However, it is suggested that the clause for conducting meetings “without the assistance of a simultaneous or consecutive translation service” be removed from the final regulations. The use of simultaneous translation at such meetings would demonstrate the same level of commitment whilst ensuring familiarity for Welsh speaking members of staff. The use of simultaneous translation would also ensure that non-Welsh speakers could be on the panel, whilst still ensuring that proceedings could be conducted bilingually.
Standards relating to a body’s information technology and about support material provided by a body, and relating to the intranet (Standards 131-136)
Challenges to fully achieving the standards
The Health Board supports the intent of this Standard but there are a number of barriers to implementation that require further consideration. In terms of the functionality of the system utilised by the Health Board (provided by NWIS to all Boards and Trusts), a new wireframe would need to be built to cater for the dual structure as the current system does not accommodate this. There are currently over 200 devolved editors with access to uploading content to the Health Board’s intranet site via the content management system. This number reflects the sheer volume of content being uploaded on a regular basis. As a result, this would put immense pressure on both the Communications and Welsh Language Teams to keep pace with these constant changes and would restrict the pace at which content was uploaded. Restricting the pace of uploading content would have serious consequences in relation to policies, key documents and clinical information. The primary purpose of the intranet site is to provide information, resources and guidance for all staff. Currently we have 7000 intranet pages, 15,000 uploaded documents, self-posting areas such as ‘Classified Adverts’ (this area would need to be abolished) and 4 micro sites feeding off the main intranet site that would also need to comply. In terms of translation, there would be severe implications in the initial phase if all text currently displayed required translation. On average there are approximately 700 words on each page, and with 7000 pages, this would amount to 4.9 million words. If these were to be translated at a cost of £75 per 1000 words this would incur an initial translation cost of £367,500. With hundreds of pages being updated on a daily basis, it would not be feasible for the translation team to undertake this amount of work along with the inability to control the updated pages and sections. The Health Board believes that these standards are not reasonable or proportionate and that translation resources would be focused on translating pages of internal text
21
rather than translating crucial information for patients and the public. The sustainability of securing translation of for each new or updated page would be equally challenging.
Current practice and achievements
In line with Standard 135, the Health Board has developed a designated Welsh Language Section on its intranet which provides services and support material to promote the Welsh language and to assist staff to use the language. The designated Welsh Language Section equips staff with the relevant information regarding service delivery, workforce planning and the every day use of the Welsh language (via detailed information about the Welsh Language (Wales) Measure 2011, the Health Board’s Bilingual Skills Strategy and ‘More than just words’) along with online packages for staff to learn the language and details of supporting resources available. The impact and advantages of this section far outweighs the limited impact of ensuring that every page on the intranet is bilingual.
Alternative proposal
The Health Board is concerned that full translation of the current intranet would be unachievable within a reasonable timescale and the current system does not have the necessary functionality. This standard therefore could not be delivered. In view of this it is believed that a revised national system needs to be designed/introduced to facilitate the provision of a fully bilingual system and the standard should be deferred until such time as this is available. The standard could be adapted at this point to require Boards and Trusts to include a prominent section on Welsh Language at the front of the Intranet.
Standards relating to a body developing Welsh language skills through planning and training its workforce (Standards 137 – 147)
Achieving the aim of the standard
Standard 138 You must provide training in Welsh in the following areas, if you provide such training in English—
(a) recruitment and interviewing; (b) performance management; (c) complaints and disciplinary procedures; (ch) induction; (dd) health and safety.

22
Certain services within the organisation have voiced concerns in relation to one of the standards within this section as part of the internal consultation process. Training is provided by subject experts that would mean trainers in those areas would need to be Welsh speaking. Currently there aren’t sufficient staff in the existing workforce in the above areas that speak Welsh.
Comments and way forward
This standard would at present pose challenges due to the lack of Welsh speakers within the areas noted in the standard. It would not be possible to call upon other Welsh speaking members of staff to support or provide the training in those areas because training must be delivered by subject experts. However, the Health Board is eager to support this element of the standards. We would ensure that any future recruitment to posts in relation to the above areas would be Welsh speaking. This would be achieved as part of its Bilingual Skills Strategy and would ensure that this standard could be achieved. It is therefore suggested that this Standard is deferred to a second phase of implementation.
Standards relating to a body recruiting and appointing (Standards 148-152)
Current practice
Standard 150: You must ensure that your application forms for posts provide a space for individuals to indicate that they wish an interview or other method of assessment in Welsh and if an individual so wishes, you must conduct any interview or other method of assessment in Welsh (without the assistance of a simultaneous or consecutive translation service).
The Health Board welcomes the proposal to conduct interviews bilingually and currently provides simultaneous translation at interviews where no Welsh speaking expert is available to be part of the interview panel. With some posts where specialist medical or clinical knowledge was not required, members of the Welsh Language Team have participated as an additional panel member to allow interviews to be conducted bilingually.
Concerns were raised as part of the Health Board’s internal consultation events, that the Health Board recruits within many specialist areas, with a low number of Welsh speakers in certain services. The majority of interview panels would include two to three people, including the prospective line manager and technical or medical assessor. It was raised that it would not be possible to ensure all panel members at all interviews were Welsh speakers and therefore not allowing simultaneous translation would be a major barrier.
Proposed way forward to fully achieve the aim of the standard
The Health Board proposes that the clause to conduct meetings “without the assistance of a simultaneous or consecutive translation service” be removed from the standard.

23
The use of simultaneous translation at interviews which, as noted above, is a practice already in use within some areas of the Health Board, would ensure the individual’s right to have his / her interview in Welsh, and would also ensure that non-Welsh speakers that may be required on the panel, would not be excluded from the decision making process. This would still ensure that interviews could be conducted bilingually, demonstrating the same level of commitment whilst having a possible positive impact on the outcome. The use of simultaneous translation would also ensure that the appropriate individuals were present in line with recruitment code of practices to ensure a fair and consistent approach to the process.
SCHEDULE 4 – Record Keeping The inclusion of this set of regulations is welcomed, as they will support the Health Board in ensuring that its robust mechanisms are updated and maintained to record and monitor its delivery of Welsh language services. The Health Board has previously noted as part of its response that a strategic plan has already been put into action to this end.
General comments in relation to practicality
Standard 163 You must keep a record of the number of members of staff who wear a badge (made available to them in accordance with standard 147) at the end of each financial year.
Concerns were raised as part of the internal consultation process regarding the above standard. Due to the copious amount of work undertaken over recent years to promote the wearing of ‘Speaking Welsh’ badges or lanyards through various campaigns such as ‘Diwrnod Su’mae’ and ‘Diwrnod y Bathodyn’ (‘Badge Day’), there is a high percentage of staff already in possession of these resources. The Health Board proposes that this standard be amended to record the number of badges or lanyards distributed during that financial year rather than the number of staff.
Further Comments
The Health Board would like to provide additional comments in relation to the standards.
Standards eliminated from the initial draft regulations In relation to the standards that have been eliminated from the initial draft regulations, the Health Board would like to emphasise and concur with the decision taken. Standard 18 in the initial draft regulations:

24
When a person contacts one of your departments on a direct line telephone number, and that person wishes to receive a service in Welsh, you must provide that service in Welsh.
This standard would have been very difficult to deliver in terms of telephone calls regarding specific, specialist services where there are no Welsh speakers available to deal with a specialist query. Standard 36 in the initial draft regulations: When you produce documents for public use you must produce them in Welsh.
This standard would have meant that all documents produced for Board meetings would have had to be translated, with a significant impact on the translation service. See information below regarding the potential cost of translating the Health Board’s public Board meetings:
Average word count for monthly Board meeting
papers
110,000 words
Monthly cost £8,250 (110,000 x £75 per 1000
words)
Cost per annum £99,000
In addition to the cost element, there is also the issue of submission and turnaround of papers, requiring set deadlines for each individual paper. The Health Board’s translation team would not be able to accommodate this work load. Standard 62A in the initial draft regulations: You must provide a face to face reception service in Welsh for a person at your reception if you have arranged a visit or appointment for that person in advance and (a) the person has informed you in advance that he or she wishes to receive the service in Welsh, or (b) you were already aware that the person would wish to receive the service in Welsh.
This standard would have been impossible to achieve in all areas at all times as a result of systems not being able to record information on patients’ preferred language, in addition to capacity issues in terms of Welsh speaking staff to be able to deliver and guarantee this provision.
Geographical dimensions and considerations Betsi Cadwaladr University Health Board provides services to the population of North Wales covering its six counties. The 2011 Census showed there were 204,406 Welsh speakers in the region (all ages), amounting to a total of 30.8 per cent of the whole population of North Wales. However, there are significant differences across the geography in relation to the number of Welsh speakers:
Demographics of Welsh speaking population within each county served by the Health
County % of Welsh speakers
Number of Welsh speakers
Gwynedd 65.4% 77,000
Anglesey 57.2% 38,568

25
Board Conwy 27.4% 30,600
Denbighshire 24.6% 22,236
Flintshire 13.2% 19,343
Wrexham 12.9% 16,659
The above figures broadly reflect the proportion of Welsh speaking staff employed across its services, but not in all areas. As previously stated, the Health Board is supportive of the Standards and any areas of challenge have been highlighted above. In Phase 1 of Compliance Notices not all authorities across North Wales were subject to the same number of standards. The Health Board would therefore request that this is taken into consideration during the implementation of the final standards and that the standards are proportionate to the geography and demographics of North Wales. The recognition of the varying degrees of capacity and capability to deliver certain standards has been reflected in local authority compliance notices and this factor also needs to be reflected within the regulations set on the Health Board.
Implementation Timeframe Recognising the issuing of compliance notices will be the responsibility of the Welsh Language Commissioner, the Health Board would like to take this opportunity to draw attention to the importance of the timeframe provided to implement specific standards. The Health Board is aware that imposition dates posed as part of compliance notices are provided for each individual standard and the Health Board is therefore eager to highlight this important element in terms of our ability to deliver taking into account the comments relating to specific Standards included in this submission. Many of the standards are current practice, whilst others will require planning and implementation for short term delivery. However, there are a number of standards that require careful consideration in determining compliance timeframes. The Regulations have identified the need to scrutinise, review and amend certain current practices if the standards are to be achieved. Some practices require a change in systematic functions, whilst others require a strategic approach to workforce planning, allowing the freedom for individuals to use the Welsh language. Consideration is also required in terms of upskilling and training the workforce. The Health Board is currently recruiting a Welsh Language Tutor that will provide staff the opportunity to further develop their Welsh language skills, in line with Standard 141. However, learning a language is an extensive and continuous process, with individuals requiring up to 300 hours of lessons to become fluent. Programmes will be developed to target specific areas and staff groups to increase their ability to speak Welsh in delivering services. The Health Board acknowledges that not all staff will be required to reach Level 5 fluency (in line with the Association of the Language Testers in Europe Framework) with lead time required to ensure there are sufficient staff with the appropriate language skill levels to meet some elements of the standards in all service areas.
26
Betsi Cadwaladr University Health Board is confident that it will meet its obligations to the public and its staff through the implementation of the Welsh Language Standards. A long term vision and implementation programme of continued improvement is paramount to the successful delivery of the Welsh Language (Wales) Measure 2011. The Health Board will continue to work with key partners and stakeholders in taking forward the standards and will actively support developments required on a national level to fully achieve the aims and objectives set out as part of the Measure. We hope that you find our comments informative and constructive for the purposes of this consultation. Should you require any further explanation regarding the comments in this response, please contact the Health Board for further information.

4.2 SPPH16/211 Mid Wales Health Collaborative Update
1 SPPH16.211 MWHC Update Report Oct 2016.pdf
1
PROGRESS REPORT ON THE WORK OF
THE MID WALES HEALTHCARE COLLABORATIVE (MWHC)
OCTOBER 2016 1. INTRODUCTION The following report provides an update on the work undertaken by the MWHC and the areas of work that are being progressed and achievements that are being made to implement the recommendations of the Mid Wales Healthcare Study. This report is intended to ensure that the collaborative healthcare organisations of the MWHC are kept up to date on the progress of the work of the MWHC and provides an opportunity to highlight future planned areas of work for reporting to the collaborative healthcare organisations of the MWHC. 2. KEY ACHIEVEMENTS A significant amount of work and good practice has been undertaken by the MWHC. The MWHC Board met on 5th September 2016 at Aberaeron at which detailed updates were received from three of the Innovation sub-groups - i) Primary Care and Community Services, ii) Communications, Engagement and Involvement and In Hospitals Services with update reports from the update reports from the five other Innovation sub-groups included in the report of the Lead Chief Executive, Mr Steve Moore. The MWHC Planning & Co-ordination group continues to co-ordinate and oversee the work programme on behalf of the MWHC Board. Key progress to date is detailed in the following sections. 2.1 Recommendation 1 – Mid Wales Healthcare Collaborative The MWHC was launched on the 12th March 2015 by the Welsh Government Minister for Health and Social Care, Professor Mark Drakeford at the Mid Wales Rural Healthcare Conference. It is a joint Committee comprising the Chair and Chief-Executive of Betsi Cadwaladr University Health Board (BCUHB), Hywel Dda University Health Board (HDUHB), Powys Teaching Health Board (PTHB), Welsh Ambulance Services NHS Trust (WAST) and the Leaders and Chief Executives of Ceredigion County Council, Gwynedd County Council and Powys County Council. The MWHC is led by two independent co-chairs Dr Ruth Hall and Mr Jack Evershed. The MWHC is accountable to Welsh Government, to the three Health Boards, WAST and to the scrutiny mechanisms for local government. Welsh Government has provided £100K funding over two years to support the administration to establish the MWHC. This has been matched by each Health Board over two years providing an additional total of £300K. The funding for individual projects is provided through the approval of business cases to the Health Boards to fund from their budget or to Welsh Government to fund through additional resources that they have made available e.g. telehealth budget, primary care workforce plan budget.

2
2.2 Recommendation 2 - Improved Public Engagement The MWHC Board meeting on 5th September 2016 was held at the Ceredigion Council Chamber, Penmorfa, Aberaeron. For the first time this meeting was streamed live over the internet and positive feedback was received from the public regarding this new venture. During the Board meeting members of the public were provided with the opportunity to raise questions, issues and provide feedback during a specific agenda item, “Listening to You” at MWHC Board meetings. They were also provided with the opportunity to meet with members of the MWHC before and after Board meetings in order to allow them the opportunity to discuss any issues which they wish to raise. The next MWHC Board meeting will be held on 9th December 2016 at the Council Chamber, Powys County Council Offices, Llandrindod Wells. This meeting will be streamed live over the internet and the ‘Listening to You’ session will once again form a part of the agenda for this meeting. The third and final series of community meetings will be held during November 2016. Each will have a specific theme relating to the work of some of the Innovation Groups. Details of the events are as follows: – Friday 11th November 2016 at the Morlan Centre, Aberystwyth, Ceredigion.
Topics for discussion will be Mental Health Services, In Hospital Services at Bronglais General Hospital, Health and Well Being and Primary Care and Community Services.
– Thursday 17th November 2016 at Glan Wnion Leisure Centre, Dolgellau, Gwynedd with topics for discussion being Telehealth, Palliative Care Services and Access and Transport.
– Tuesday 22nd November 2016 at the Elephant and Castel Hotel, Newtown, Powys and the topics to be discussed will be Primary Care and Community Services, Telehealth and Mental Health Services.
This final series of planned community events will allow the MWHC to discuss the progress that has been made in the last few months and the public will have the opportunity to provide their feedback on the work undertaken to date. The Innovation sub-groups are working closely with members of the public who have expressed an interest in becoming more involved in their work. 2.3 Recommendation 3 - Local Action on Primary Care The Physicians Associate Students from Birmingham University have now taken up their training placements in Bronglais General Hospital and will be moving on to placements in primary care across Mid Wales in the next few months. The development of a bespoke training and development course for practice nurses is being investigated. This will have an emphasis on the development of practical skills and competences required by practice nurses in rural areas. A Steering group will be established design and implement general anaesthetic dental services from Bronglais General Hospital.

3
Capacity has been made available at a Newtown dental clinic to receive patients from HDdUHB. This will prevent unnecessary patient travel from the northern reaches of the HDdUHB area to South Wales. The Assessing Alternative to Admissions team (AA2A) been in place since May 2016. This service is embedded alongside the discharge liaison service and links closely with health and social care community teams. The recording and monitoring systems are being established and will link in to the County Performance Management systems. Complex discharge pathways are being rolled out on the wards in Bronglais General Hospital over the next few weeks. This will improve patient flow and will improve engagement with families/carers in relation to safe timely discharge. HDdUHB is currently advertising for a jointly funded Discharge Liaison Nurse to assist with the complex discharge of Powys residents. If a successful appointment is made an extension to include patients from the BCUHB area will be considered, however, this will be dependent on the availability of funding. There are different models of delivering community care across the Mid Wales region as follows: - Virtual wards have only been rolled out in North Powys (PTHB) in the last
few months and are still under evaluation. - The Enhanced Care Service (ECS) being delivered by BCUHB provides
short term ‘step up’ intensive community based care as a credible alternative to hospital admission and also provides ‘step down’ support to enable timely early discharge from hospital.
- In HDdUHB the Community Resource Team model builds upon the concept of the Virtual Ward model adopted elsewhere in the country.
As different models are prevalent across Mid Wales the concept of the ‘virtual ward’ is in place across all parts of the MWHC area. However, they are at different stages of development and the Primary and Community Care sub-group will undertake an evaluation to ensure consistency. 2.4 Recommendation 4 - National Primary Care Plan The MWHC team is working with the GP Clusters to agree the joint priorities for Mid Wales. A more detailed report will be available at the December 2016 meeting of the MWHC Board. 2.5 Recommendation 5 – 8 – Bronglais General Hospital and Staff
Engagement Staff Engagement The staff engagement exercise undertaken during the Summer 2016 identified 10 members of staff who expressed an interest in becoming MWHC Champions to work with the MWHC to improve staff engagement and involvement in the future. Dr Phil Jones, Hospital Director of Bronglais General Hospital will chair the innovation sub-group in future and is reviewing the membership following the period of staff engagement.
Clinical Strategy A staff engagement workshop was held on 21st July 2016 and was attended by staff from Bronglais General Hospital, the community, primary care and Welsh Government. There was good representation from consultants, other healthcare professionals and managers. An overview of the work previously undertaken by

4
members of the Bronglais Innovation Sub-Group and the feedback from the recent staff engagement exercise was presented and discussed. It was agreed that the work done to date reflects staff views and forms the foundation of the clinical services strategy for Bronglais General Hospital. It was agreed that further work is needed by the Bronglais Innovation sub-group to develop the strategy further including opportunities for developing multi-professional working and closer working between primary care, community and hospital services. As part of the review of the membership of the group representation from Powys Teaching Health Board and Betsi Cadwaladr University Health Board will be agreed. Workshops will be arranged with the Royal College of Physicians to discuss the future model for cardiology services and with the Royal College of Obstetricians and Gynaecologists to discuss the future model for obstetric services in Bronglais General Hospital.
Recruitment Campaign It has been agreed that a new, different campaign is required to attract consultants to work in Bronglais General Hospital that differentiates the offer from the competition and highlights the benefits of working in Mid Wales. Part of the workshop on 21st July 2016 for staff was led by a branding consultant who presented an innovative approach to developing a recruitment campaign specific for Bronglais General Hospital. It has since been agreed by HDdUHB that:
• A further workshop will be arranged with wider staff involvement to develop the recruitment campaign further.
• The development of a brand for Bronglais General Hospital that will be used to underpin a recruitment campaign.
• The medical recruitment campaign will be launched in the autumn with an open day arranged for 14th October 2016 for potential applicants.
Surgical Services The Royal College of Surgeons in collaboration with the Royal College of Surgeons of Edinburgh (RCSed) and Hywel Dda University Health Board held a conference on 10th October 2016 at Aberystwyth to discuss ‘Sustainable surgery in rural Wales’. The aim of the event was to address the issues in delivering a model for rural surgery, present the findings from the recent RCSed report on Standards Informing Delivery of Care in Rural Surgery published in March 2016 and discuss the future of surgery in rural Wales. The conference was aimed at surgeons of all grades, medical directors and other management personnel. The outcomes of this conference will help inform the surgical model for Bronglais General Hospital. MRI Scanner A project meeting in respect of the MRI Scanner was held on 1st July 2016 where it was confirmed that the Welsh Government had put aside funding to replace the MRI scanner. An options paper has been produced with the proposed location for the new MRI scanner at Bronglais General Hospital. A 12 week testing programme has been undertaken to determine the suitability of the proposed location the results of which showed that it was close to being viable and as a result further tests were undertaken for which the results are currently awaited. Another project meeting is in the process of being arranged to develop a time line for this project.
5
2.6 Recommendation 9 - Access and Transport A new service model for Non Emergency Patients Transport Service has been agreed which involves coordination between a variety of different providers and is currently being implemented.
A workshop is being arranged to look at the development of the Emergency Medical Retrieval Service from a 12 hour service to a 24 hour service. Patient pathways across Mid Wales and across organisational boundaries from primary care to secondary care and back to home are being identified to look at the opportunity for implementing Telemedicine and Telehealth to deliver care closer to home.
2.7 Recommendation 10 - Advanced Paramedic Practitioners The findings of the WAST review of the training required for advanced paramedic practitioners to work in rural areas review is still awaited and will be implemented through the work of the Centre for Excellence in Rural Health and Social Care. 2.8 Recommendation 11 – Telehealth, Telemedicine and Telecare Telehealth Grant Funding There is a balance of approximately £200,000 available from the grant funding which was awarded to the MWHC by the Welsh Government for Telehealth initiatives for Mid Wales. The MWHC organisations have been invited to develop business cases for Telehealth projects / initiatives across Mid Wales and these are currently under development. The original Efficiency Through Technology Fund forms are being used for the development of cases as members of the sub-group are familiar with these and some cases have already been developed using these forms. The next sub-group meeting focused on reviewing the Business Cases where it was agreed that further detailed information was required to ensure they met the scoring criteria adopted for the Efficiency Through Technology Fund and the key priority areas identified in the Mid Wales Healthcare Study. A report providing details of the business cases awarded funding will be available for the December 2016 MWHC Board meeting. Telemedicine equipment A project manager is now nearing the end of the 6 month project to ensure that the telemedicine equipment in Mid Wales is working, sited in the best place and that staff are trained to use it.
Telemedicine Strategy for Mid Wales Preliminary work has commenced on the development of a Telemedicine Strategy and Implementation Plan for Mid Wales. This will provide a clear vision, strategy and a detailed implementation plan for Telemedicine across Mid Wales with the key aims being to:
• Identify and maximise the opportunities for Bronglais General Hospital to reach outwards via Telemedicine services;
• Identify and maximise opportunities for people to reach inwards to Bronglais General Hospital via Telemedicine services;
6
• Identify opportunities for Clinician to Clinician communication and collaboration via Telemedicine services including primary care and the community;
• Establish Bronglais General Hospital as a Telemedicine learning centre for Clinical staff across Wales.
A Task & Finish Group, whose membership will include key staff (clinical and non-clinical) from the MWHC organisations, will lead on the development of the Strategy and Implementation Plan. The group met in mid September 2016 to agree the Project Initiation Document, confirm the priority areas for action and agree the way forward for the development of the Strategy which will include engagement with key partners and clinicians to ensure effective liaison and a Clinical workshop.
A detailed paper will be presented to the MWHC Board at its Board meeting in December 2016 in order to allow the Board to shape the direction of travel and indicate its support. The final version of the Strategy and detailed Implementation plan will be presented to the MWHC Board meeting in March 2017 (date to be confirmed). It is proposed that the implementation of this Strategy will commence in April 2017. 2.9 Recommendation 12 – Centre for Excellence in Rural Health and Social
Care On 24th March 2016 Professor Mark Drakeford, the previous Welsh Government Minister for Health and Social Care launched the Centre for Excellence in Rural Health and Social Care (CfERH). The vision of the CfERH is to lead the way in accessing and undertaking relevant research to inform the models of prevention, treatment and care that need to be implemented to improve the health and wellbeing of the communities and population within rural areas in Wales. In collaboration with partner organisations, the CfERH will inform the development of services that deliver appropriate access to services, based on principles of informed patient choice, prevention, diagnosis and self-care. The CfERH will establish a network of relevant individuals, research units and groups, from within Wales and further afield to access and verify evidence to support the research, innovation and development agenda and enable decision-makers and policy colleagues to be fully cognisant of the scope, opportunities, issues and challenges in implementing prudent healthcare within the context of a rural environment. The CfERH will also work with professional bodies and Higher Education Institutions to ensure that structured education and training programmes for doctors, dentists, nurses, midwives, pharmacists, allied healthcare professionals, paramedics, optometrists and social care staff are available to equip them with the skills and knowledge to deliver high quality care in rural areas. Hosting Arrangements As host organisation for the MWHC and on behalf of the organisations within the MWHC, HDUHB will formally host the CfERH. HDUHB will lead on the governance, liability and accountability arrangements for the CfERH including the employment of the staff. A Memorandum of Understanding has been developed for all partner organisations of the CfERH to sign up to. It confirms the intention of the Health Boards, Welsh Ambulance Services Trust and the Local Authorities that are members of the MWHC, Y Coleg Cymraeg Cenedlaethol and the Universities

7
across Wales to collaborate in establishing the CfERH. The document has been circulated to all partner organisations for signature.
CfERH Sub-committee The CfERH sub-committee met on 11th October 2016 and agreed to approve in principle further work on the development of the following projects to support the establishment of the CfERH: i. Conduct a literature search and developed an evidence base relating to
workforce provision in rural health and social care systems similar to those in Wales.
ii. The development of materials to support a recruitment campaign in Mid Wales.
iii. The development of a website and repository for information. iv. Set up a mechanism for professional networking of groups providing health
and care services in a rural environment. v. Green prescribing and community resilience. vi. Develop proposals for a system of accreditation of health initiatives in a rural
environment. The CfERH Management Board will meet in November/December 2016 to agree the detailed business cases for these projects. 2.10 Mental Health & Learning Disabilities sub-group Priority area 1 - Innovative approaches to crisis management (lead BCUHB) This priority area will develop innovative approaches to crisis management across organisational boundaries and sectors. The work programme will review the outcomes to the differing current cross-sector approaches to dealing with crisis and Section 136, and the associated transportation challenges. Crisis response and management needs to be joined and availability and access to alternatives to hospital based care will be examined in terms of the development of crisis or sanctuary beds in the Mid Wales area. The outcome will be a multi agency and organisation Section 136 suite that will be staffed to support people effectively and quickly. Those who need time away from home but not necessarily hospital will have access and overnight residential support in a multi agency and organisation community setting. Progress to date on the work undertaken around this priority area includes:
• Section 136 practice – Peer review event regarding Section136 held on 26th May 2016 and the focus of the meeting on 6th September 2016 will be on the outcomes of the peer event and the implementation of the crisis concordat.
• Crisis pathways across sectors – Linking into crisis concordat implementation work with specific consideration of options for the Mid Wales region.
• Transportation and conveyance – WAST representation secured / linking work to “clinical desk” and Street Triage initiatives across the region.
• Access to crisis / sanctuary beds – Meeting to share the work of the Transforming MH programme (HDdUHB) held with BCUHB / PTHB MH Leads. Visits scheduled for teams to visit HDdUHB to link in with transformation / twinning work and consider inter HB commissioning with the Third Sector to develop local crisis / recovery beds in Aberystwyth with a potential SLA across HB’s for clinical pathways.

8
Priority area 2 - Telemedicine and helping to connect people (lead PTHB) The Mental Health & Learning Disabilities (MHLD) Innovation Sub-Group will link with the Telemedicine Innovation Sub-Group to review and extend the programme of innovation in mental health telemedicine currently being undertaken in Powys. The outcome will be a choice for the Mid Wales population about how they access mental health services which include Telemedicine new consultations and follow up appointments.
Dr. Wasi Mohammed is linked in to the Telehealth Sub-Group. Telemedicine priorities which were agreed focused on the roll-out of existing PTHB Skype for Business pilot with NWIS and EU funding and linking to the potential funding bid with Telehealth sub-group.
Priority area 3 - Optimise self-management and share resources to build resilience (Lead PTHB/WWAMH) The MHLD Innovation Sub-Group is committed to optimising the opportunities for mental health self-management and resilience building and will therefore link with the Health & Well-Being Innovation Sub-Group to ensure that mental well-being is a key priority of the programme. The outcome will be a clear hub for mental health self management information that will be accessible and accessed directly by the population.
Excellent examples of Third Sector initiatives have been presented by BCUHB, HDUHB and PTHB areas and a linked resource information is to be shared across the region.
Key activities planned for the next few months are a visiting programme for BCUHB and PTHB in respect of the Transforming MH programme, consideration of pilot areas for identified innovation. Initial contact has been made with all individuals who expressed an interest at the engagement events and priority area leads will now make contact with those individuals who had shown an interest in their area of work.
2.11 Palliative Care and End of Life Innovation sub-group
Rapid review: The rapid review has been completed by the Marie Curie Research Centre, Cardiff University with key findings as follows:
• Sustainability in rural areas is likely to be more successful where service models are developed by an existing service provider. Stand alone outreach services are unlikely to be successful.
• Integrated working between health, social care and the third sector will enhance efficiency, human resources and equipment costs.
• Ineffective communication between care settings and between primary and secondary care is a threat to the quality and safety of services for patients.
• In the literature knowledge and skills deficits for GPs and community nurses are consistently defined as a barrier to receiving quality palliative care services. Academic and skills training for primary care providers is core.
Project scoping exercise:
• The project has been extended by two months as a result of long term sick leave by the former Senior Project Manager. A new part-time Senior Project Manager has been appointed and is working on a part-time basis to

9
complete the scoping work by October 2016.
• A detailed distribution plan has been developed and a bi-lingual service scoping template and covering letters produced. The scoping template has been circulated extensively – responses are awaited.
• A Working Group has been established to provide direction and support to the project scoping exercise. The Working Group has met twice in June and July 2016 with a further meeting planned for September 2016.
• A Specialist Information Analyst has been appointed for a three month period to provide specialist information support to the Senior Project Manager. The Working Group is providing expert advice and guidance in supporting the data analyst to identify relevant databases and historical information in order to underpin the project proposals.
• The development of ‘service maps’ to inform the scoping work.
• A Report with emerging findings following approximately 50 one-to-one stakeholder discussions / interviews has been produced.
2.12 Health and Wellbeing Innovation sub-group The MWHC, Ceredigion County Council’s Carers Unit and the Hywel Dda University Health Board’s Investors in Carers Scheme have worked in partnership to develop a training programme to build resilience and improve the well-being of carers across Ceredigion. This is the first time this exciting and well trusted training programme has been adapted and trialled with carers in the whole of the UK. Ceredigion has been specially chosen to provide it with the opportunity to be one of the first in UK to take part. By doing this programme carers will gain skills and knowledge that will support them in their caring role, and which they will be able to use what they know to help to shape the programme for carers in the future.
The first workshop to focus on tobacco control and smoking cessation arranged for August 2016 was cancelled due to the high number of apologies received from key stakeholders and this is now being rearranged for Autumn 2016. 3. RISKS AND ISSUES A Risk and Issues Strategy is in place for the management of issues and risks in order to ensure the project maintains visibility of and proactively manages all factors that may adversely affect the achievement of its objectives. Risks and issues have been identified during the initial start-up of the MWHC when considering the milestones to be achieved. Additional risks and issues are identified via Innovation sub-group update reports. The Clinical Programme Director formally analyses the risks and issues identified and determines the next steps to be taken. The Clinical Programme Director, on behalf of the Planning and Co-ordination group, monitors and reviews the risk register. The latest version of the risk register has the following high ‘red’ scoring risks.
• Inadequate resource to implement MWHC programme;
• Lack of commitment / co-operation amongst partners;
• Failure to achieve agreed milestones;
• Inability to identify and release key staff for involvement;
• Competing priorities for collaborative health organisations.

10
4. RECOMMENDATION 4.1 For information – Collaborative organisations are asked to note the progress
on the work undertaken by the MWHC and the areas of work that are being progressed and achievements that are being made.
KEY
BCUHB Betsi Cadwaladr University Health Board
CfERH Centre for Excellence in Rural Health and Social Care
HB Health Board
HDdUHB Hywel Dda University Health Board
MHLD Mental Health & Learning Disabilities
MWHC Mid Wales Healthcare Collaborative
NWIS NHS Wales Informatics Service
PA Physician Associate
PAVO Powys Association of Voluntary Sector Organisations
PHW Public Health Wales
PTHB Powys Teaching Health Board
SATH Shrewsbury and Telford NHS Trust
THB Teaching Health Board
UHB University Health Board
WAST Welsh Ambulance Services NHS Trust
WG Welsh Government
WWAMH West Wales Action for Mental Health
4.3 SPPH16/212 Parliamentary Review of Health and Social Care in Wales
1 SPPH16.212 Parliamentary Review.doc
STATEMENT
BY
THE WELSH GOVERNMENT
TITLE Parliamentary Review of Health and Social Care in Wales
DATE 1 November 2016
BY Vaughan Gething AM, Cabinet Secretary for Health, Well-being and
Sport
We believe, as other parties do, that the time is right for a rounded and mature conversation about how we shape the future of health and social care services in Wales.
The Parliamentary Review of health and social care in Wales was agreed as part of our compact ‘Moving Wales Forward’ with Plaid Cymru. I would like to take this opportunity to thank all parties here for their contribution and co-operation in agreeing the terms of reference and the panel membership, enabling us to move this forward.
The Panel will review the best available evidence to identify key issues facing our health and social care services and draw out the challenges these will present over coming years. For example, the challenge of NHS finances within a reducing Welsh Government budget, workforce planning, recruitment and retention, meeting the rising demand for healthcare and public expectations. The review will examine options for the way forward and will make recommendations about what the health service of the future could look like.
The review team will of course draw on work that has already been carried out in Wales by the Health Foundation, the OECD, the Nuffield Trust, the Bevan Commission and the King’s Fund. It will draw their findings together and identify gaps in the evidence and knowledge that the review will seek to fill. The terms of reference have been discussed with other parties and will be published later today. The Panel will meet to discuss them later this month.
We have agreed the review panel should be independent – comprising prominent leaders, stakeholders and academics with a range of backgrounds.
Today I am pleased to announce that Dr Ruth Hussey has agreed to chair the review. Ruth was born in North Wales, is an ex Chief Medical Officer of Wales, has been regional director of public health at NHS North West and has worked with the Public Health England transition team at the Department of Health. She has also been the director of public health for Liverpool and senior lecturer in public health at Liverpool University.

Ruth brings with her a wealth of experience, a depth of knowledge of the system in Wales as well as a wider view of health and social care beyond our borders. She will be joined on the review panel by:
Prof Anne Marie Rafferty, Professor of Nursing and Dean of the Florence Nightingale School of Nursing and Midwifery, King's College London. She is also a Fellow of the Royal College of Nursing.
Prof Keith Moultrie, the head of the Institute of Public Care at Oxford Brookes University who has worked directly with the Department of Health and the Department for Education, the Care Quality Commission and the Scottish Joint Improvement Team.
Prof Nigel Edwards Chief Executive at the Nuffield Trust. He has been an expert advisor with KPMG’s Global Centre of Excellence for Health and Life Sciences and a Senior Fellow at The King’s Fund as well as the Policy Director of the NHS Confederation for 11 years.
Dr Jennifer Dixon the Chief Executive of the Health Foundation having been the Chief Executive of the Nuffield Trust from 2008 to 2013. She has previously been the policy advisor to the Chief Executive of the National Health Service.
In order to further widen the perspective, there will also be a business representative on the panel. There will be three further ex–officio members of the panel:
Professor Sir Mansel Aylward, Chair of the Bevan Commission, Professor of Public Health Education at Cardiff University and former Chief Medical Advisor at the Veterans Agency in the Ministry of Defence;
Professor Don Berwick, President Emeritus and Senior Fellow at the Institute for Healthcare Improvement, former Professor of Paediatrics and Health Care Policy and currently Lecturer in the Department of Health Care Policy at Harvard Medical School, and a leading international authority on health care quality and improvement;
Dame Carol Black, Principal of Newnham College Cambridge, a former President of the Royal College of Physicians and of the Academy of Medical Royal Colleges. This will allow the panel to benefit from their extensive international expertise and experience.
Between them this panel has the expertise and capability to deliver a comprehensive and independent assessment of how best to tackle the big issues facing us around health and social care. The review team will be supported by a wider stakeholder reference group made up of representatives of professional bodies and social service organisations. I expect the review to take around a year to prepare its report – I also expect that interim findings could be available before then. This will allow time for recommendations to be implemented within this Assembly term. I will update the Assembly as the work progresses.
2 SPPH16.212 Parliamentary review ToR.pdf

4.4 SPPH16/213 Summary of In Committee Business From 10.10.16
1 SPPH16.213 In Committee Items Reported in Public.docx
1
Strategy, Partnerships and Population Health Committee 24.11.16 Item SPPH16/213
To improve health and provide excellent care
Title: Summary of In Committee Board business to be reported in public
Author: Ms Kate Parry, Acting Head of Corporate Affairs
Responsible Director:
Mr Geoff Lang, Executive Director of Strategy
Public or In Committee
Public
Strategic Goals (Indicate how the subject matter of this paper supports the achievement of BCUHB’s strategic goals –tick all that apply)
1. Improve health and wellbeing for all and reduce health
inequalities
2. Work in partnership to design and deliver more care
closer to home
3. Improve the safety and outcomes of care to match the
NHS’ best
4. Respect individuals and maintain dignity in care
5. Listen to and learn from the experiences of individuals
6. Use resources wisely, transforming services through
innovation and research
7. Support, train and develop our staff to excel.
Approval / Scrutiny Route
The issues listed below were considered by the Committee at its private in committee meeting of 10.10.16.
Purpose: Standing Order 6.5.3 requires the Board to formally report any decisions taken in private session to the next meeting of the Board in public session. This principle has been applied to Committee discussions.
Significant issues and risks
Issues were considered as follows: Progress report on the planning and development of the HMP
Berwyn Healthcare project
Special Measures Improvement Framework Theme/ Expectation addressed by this paper
Leadership and Governance

2
Equality Impact Assessment
No equality impact assessment is considered necessary for this paper.
Recommendation/ Action required by the Committee
The Committee is asked to note the paper
Disclosure: Betsi Cadwaladr University Health Board is the operational name of Betsi Cadwaladr University Local Health Board
Committee Coversheet v10 June 2016