building relationships and collaborating through the
TRANSCRIPT

Oncology Nursing Society 43nd Annual CongressMay 17–20, 2018 • Washington, DC 1Advanced Practice
1. Teaming-Up to Treat Elderly AMLDonna Colabroy, RN, MSN, CCM, AOCNSLehigh Valley Health Network Allentown, PA
2. The Process of Oncology Nurse Practitioner Patient Navigation: Triage an Essential ProcessFrances Johnson, PhDTexas Woman’s UniversityHouston, TX
3. The Power of Networking: It’s A Small World After All!Danielle Piseno, RN, BSN, OCNLynn Cancer InstituteBoca Raton, FL
Building Relationships and Collaborating Through the Navigation ProcessFriday, May 18 • 9:45–11 am
Note one action you’ll take after attending this session: ____________________________________________________
________________________________________________________________________________
ONS 43rd Annual Congress
Advanced Practice (Colabroy) 1
Teaming-Up to Treat Elderly AML
Donna Colabroy, MSN, RN, CCM, AOCNSAdvanced Oncology Clinical Nurse Specialist
Lehigh Valley Cancer InstituteAllentown, PA
Disclosures
The speaker has nothing to disclose.

ONS 43rd Annual Congress
Advanced Practice (Colabroy) 2
Lehigh Valley Cancer Institute:
• 4500+ analytic cases• 3 Comprehensive Centers• 3 MO/Infusion Sites• 15 Breast Health Services Sites• 45,062 Infusions• 67,836 Radiation Visits• 8 Surgical Robots• 672 Genetics Visits• 1300 Patients Navigated• 200 Clinical Trials• 7 Multi-Disciplinary Tumor Clinics• 13 Disease Site Tumor Boards
Significance & Background: Elderly AML
• A diagnosis of Acute Myeloid Leukemia (AML) in the elderly adult, age ≥ 60 presents challenges when considering treatment options
• Average age at diagnosis: 68 years
• Adverse predictors of elderly AML survival include: Comorbidities, frailty, prior hematologic disorder, complex cytogenetic profile
• Assessment of both patient & disease‐related characteristics is suggested when determining induction treatment
10,670
Estimated new US cases of AML in 2018
estimated deaths from AML in 2018
19,520
(ACS, 2018)
Elderly AML Algorithm: Purpose, Interventions
Purpose:
• To develop an algorithm for AML Induction in the Elderly Adult, Age ≥ 60
Interventions:
• Retrospective chart review of elderly AML patients seen at Lehigh Valley Health Network (LVHN) from 2010-2014
• Multidisciplinary Team collaboration in the development of an algorithm for AML Induction in the Elderly Patient, Age ≥ 60
ONS 43rd Annual Congress
Advanced Practice (Colabroy) 3
0
20
40
60
80
Primary Secondary
Number of Patients
Morphology
0
50
100
150
Yes No
Number of Patients
Comorbidities
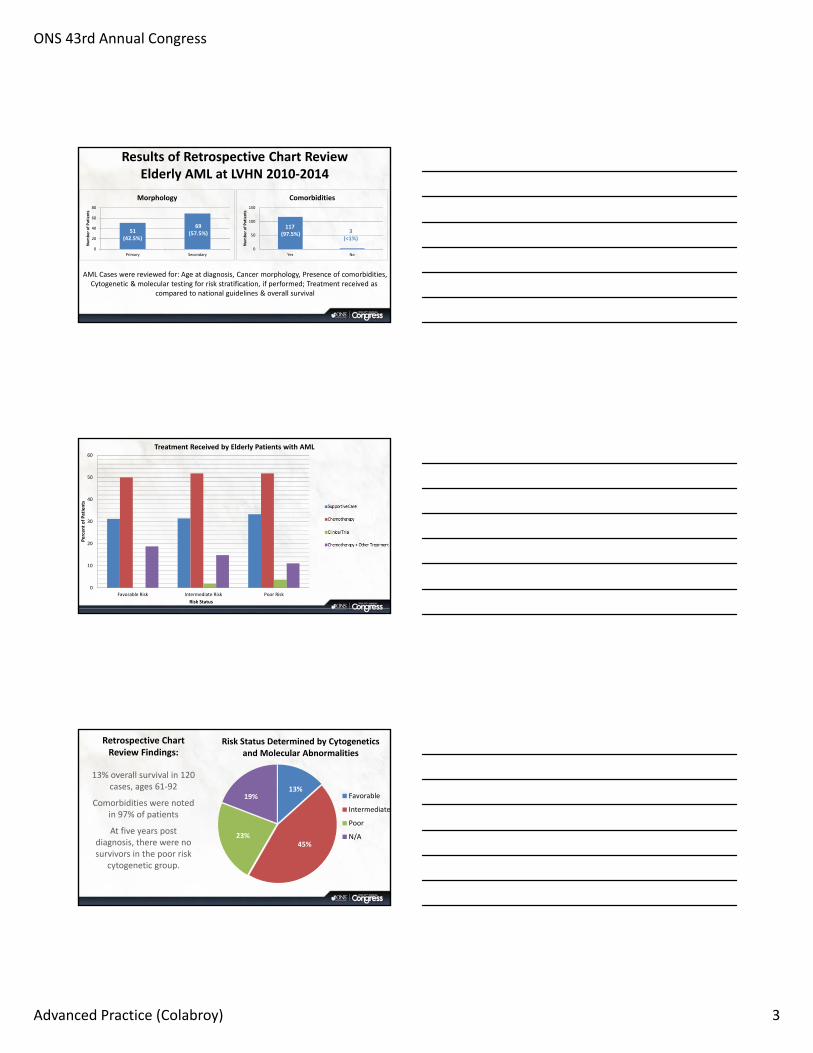
Results of Retrospective Chart Review Elderly AML at LVHN 2010‐2014
51(42.5%)
69(57.5%)
117 (97.5%)
AML Cases were reviewed for: Age at diagnosis, Cancer morphology, Presence of comorbidities,Cytogenetic & molecular testing for risk stratification, if performed; Treatment received as
compared to national guidelines & overall survival
3(<1%)
0
10
20
30
40
50
60
Favorable Risk Intermediate Risk Poor Risk
Percent of Patients
Risk Status
Treatment Received by Elderly Patients with AML
Retrospective Chart Review Findings:
13% overall survival in 120 cases, ages 61‐92
Comorbidities were noted in 97% of patients
At five years post diagnosis, there were no survivors in the poor risk
cytogenetic group.
13%
45%23%
19%
Risk Status Determined by Cytogeneticsand Molecular Abnormalities
Favorable
Intermediate
Poor
N/A

ONS 43rd Annual Congress
Advanced Practice (Colabroy) 4
Teaming Up to Treat Elderly AML: Discussion
Team Effort
• Oncology APNs
• Oncology Clinical staff RNs
• Hem‐OncPhysicians/PAs
• Clinical Pharmacist
• Rehab Services
• Palliative Care
• Clinical Trials
• Hematopathologist
Algorithm Components
• Assessment of Patient & Disease related characteristics
• AML‐Score Calculator
• Referrals to Rehab, Palliative Care
• Treatment regimens per NCCN guidelines
Implementation
• Educational offerings for Physicians, CRNPs, PAs, RNs
• Measurement of compliance with algorithms components
• Follow‐up meetings with Multidisciplinary Team
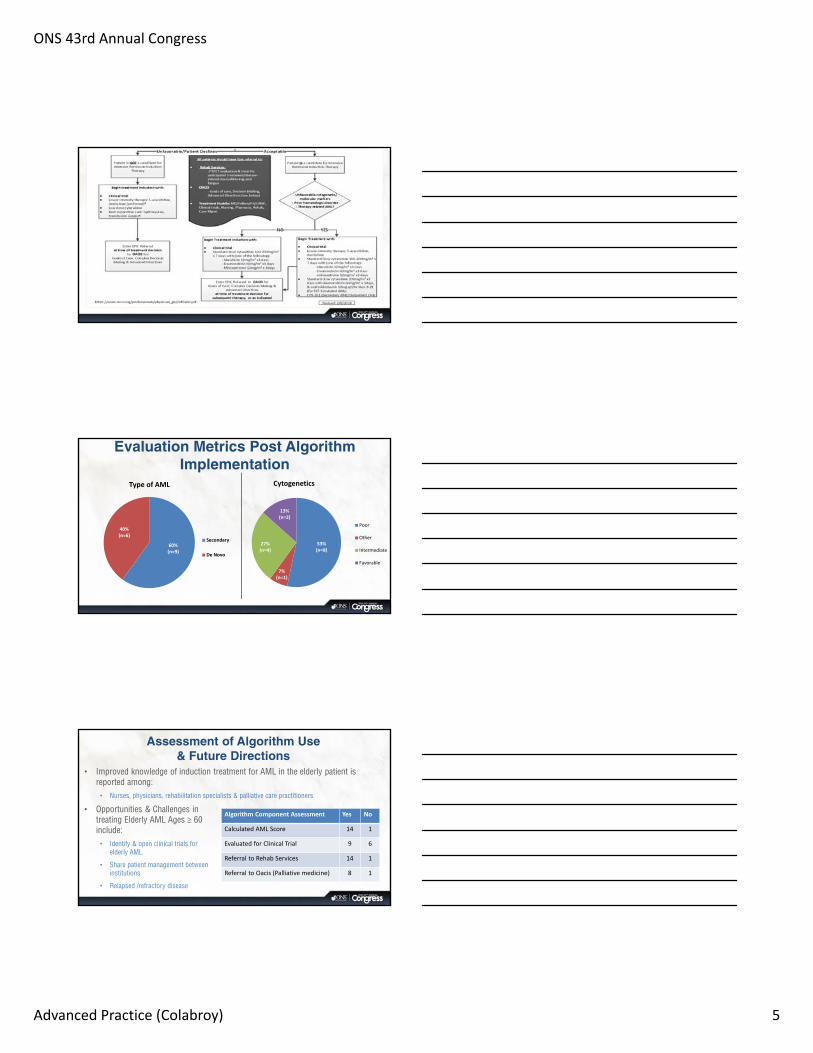
AML Algorithm for Elderly
Adults Age ≥ 60 years
ONS 43rd Annual Congress
Advanced Practice (Colabroy) 5
Evaluation Metrics Post Algorithm Implementation
60%(n=9)
40%(n=6)
Type of AML
Secondary
De Novo
53%(n=8)
7%(n=1)
27%(n=4)
13%(n=2)
Cytogenetics
Poor
Other
Intermediate
Favorable
Assessment of Algorithm Use & Future Directions
• Improved knowledge of induction treatment for AML in the elderly patient is reported among: • Nurses, physicians, rehabilitation specialists & palliative care practitioners
• Opportunities & Challenges in treating Elderly AML Ages ≥ 60 include: • Identify & open clinical trials for
elderly AML
• Share patient management between institutions
• Relapsed /refractory disease
Algorithm Component Assessment Yes No
Calculated AML Score 14 1
Evaluated for Clinical Trial 9 6
Referral to Rehab Services 14 1
Referral to Oacis (Palliative medicine) 8 1
ONS 43rd Annual Congress
Advanced Practice (Colabroy) 6
Clinical Pearls• AML in the elderly can present treatment challenges related to
– Comorbidities
– Performance Status
– Individual cytogenetics
– Secondary vs. de novo disease
• Consideration of patient and disease related characteristics provides for a patient-centered focus
• A multidisciplinary approach to treatment selection and management is recommended for optimal clinical outcomes
References• American Cancer Society, (2018). What are the key statistics about acute myeloid leukemia? www.cancer.org/cancer/acute-myeloid-
leukemia/about/key-statistics.html
• National Comprehensive Cancer Network, (2017). NCCN guidelines version 3.2017 and 1.2018: Acute myeloid leukemia. https://www.nccn.org/professionals/physician_gls/pdf/aml.pdf
• Wang, R., Zeidan, A.M., Halene, S., Xu, X., Davidoff, A.J., Huntington, S.F. . . . Ma, X. (2017). Health care use by older adults with acute myeloid leukemia at the end of life. Journal of Clinical Oncology, 35, 1-8. http://ascopubs.org/doi/pdf/10.1200/JCO.2017.72.7149
• Almeida, A.M., Ramos, F., (2016). Acute myeloid leukemia in the older adults. Leukemia research reports 6, 1-7. http://www.sciencedirect.com/science/article/pii/S2213048916300085
• Medeiros, B., (2015). Treatment of elderly patients with acute myeloid leukemia. The Hematologist, 12, (1), 1-7. http://www.hematology.org/Thehematologist/Ask/3615.aspx
• Walter, R.B., Othus, M., Borthakur, G., Ravandi, F., Cortes, J., Pierce, F.R. . . . Estey, E.H. (2011). Prediction of early death after induction therapy for newly diagnosed acute myeloid leukemia with pretreatment risk scores: A novel paradigm for treatment assignment. Journal of Clinical Oncology, 29, (33), 4417-4423. http://ascopubs.org/doi/pdfdirect/10.1200/jco.2011.35.7525
• Utz, K., Rollig, C., Koschmieder, A., Heinecke, A., Sauerland, M.C., Schaich, M. . . . Muller-Tidow, C. (2010). Complete remission and early death after intensive chemotherapy in patients aged 60 years or older with acute myeloid leukaemia: A web-based application for prediction of outcomes. Lancet 2010, 376, 2000-2008. https://ac.els-cdn.com/S0140673610621058/1-s2.0-S0140673610621058-main.pdf?_tid=2f00e30c-add6-11e7-b549-00000aab0f02&acdnat=1507652288_690b2d827078acfa30997576a68bfe5e
ONS 43rd Annual Congress
Advanced Practice (Johnson) 1
The Process of Oncology Nurse Practitioner Patient Navigation: A
Grounded Theory Approach, Triage an Essential Process
Frances Mary Johnson, PhD, RN, ANP-BC, CNS, AOCN®Oncology Nurse Practitioner
Carl R. Darnell Army Medical CenterFort Hood, Texas
Disclosures
This presentation is a section of my dissertation for my PhD program at Texas
Woman’s University
ONS 43rd Annual Congress
Advanced Practice (Johnson) 2
1. Discuss the significance and back ground of the study2. Delineate the purpose of the study3. Discuss the intervention of the study4. Discuss the evaluative measures to determine rigor5. Discuss nursing literature pertaining to triage and related tools6. Discuss the findings of the study as relates to triage in ONP
patient navigation7. Discuss the practice innovation (practical ideas and steps for
integrating triage systems along the cancer continuum) 8. Discuss the implications for further research
Background of Study• Processes influence outcomes and vise versa
(Donabedian,1966)• Evidence exists showing that NP navigators expedite
cancer care and patient satisfaction (Johnson, 2015)• The process of ONP navigation is not well defined
(Johnson, 2015);(2016)
Research QuestionWhat processes do oncology nurse practitioners navigators use in caring for cancer patients?
ONS 43rd Annual Congress
Advanced Practice (Johnson) 3
Semi-structured Interview QuestionnaireInitially Four Questions with Probes
• Themes included were: typical day, mentoring, skills that help do the job well?
Later Revised on the Premise that Process Drives Outcomes
• Themes included were: overall goals, structure used for navigation plan of care, difference between NP and
Navigator duties, how to navigator from start to finish, how is the process monitored?
Includes age, race, years in nursing, years as a navigator in the current setting, type of hospital?
Steps to Ensure Rigor• Credibility
• Information congruent with reality• Well established research technique of grounded theory• Trusting relationship with participants stressing confidentiality
• Transferability• Findings can be applied to other studies• Core category explaining navigation• Demographic questionnaire and participant inclusion criteria designed to recruit highly
experienced ONPs from various settings
• Dependability• Detailed reporting of processes• Accuracy of taped transcriptions rechecked• Use of NVivo software
• Confirmability• Data is true to participant experience• Data reviewed with research chair• Audit trail (Lincoln & Guba, 1985; Shenton, 2004)
Coding• Open Sampling• Script reviewed for events that explained concepts • Line by line concept coding(Glaser, 1978) with NVivo software• Memoing used in data analysis• Returned to site to find answers to questions (Corbin & Strauss, 2008)•• Constant Comparison• Constantly compared incidents in the research process • Noted ways in which the data was the same or different from
previous incidents• Variations classified using NVivo (Corbin & Strauss, 1990)
• Open Coding• “breaking data apart and delineating concepts to stand for blocks
of raw data” (Corbin & Strauss, 2008, p.195• Interview #7 • Seventy-two concepts emerged
ONS 43rd Annual Congress
Advanced Practice (Johnson) 4
Coding• Axial Coding• Concepts linked into conceptual families
(Corbin & Strauss, 2015• Interview #10 • Theoretical saturation; eleven thematic categories
• Selective Coding• Formulation of relationships between concepts into theoretical frameworks • Core category identified• Collapsed into seven categories• Cross-referenced with literature • Basic Social Process identified (Corbin & Strauss, 2015)• Interview nineteen: diagram• Interview twenty: process confirmed with only NP to navigate to survivor stage
Core Category and Basic Social ProcessCORE CATEGORY (CC)
• The overall goal of the ONP navigation process is to expedite care along the cancer continuum.
• The Basic Social Process (BSP) is staying connected to the patient and to the system (Johnson, 2016)
Triage• ONP’s are responsible for quality of care• Lack of streamlined care produces poor outcomes
-Diagnosis of cancer at a later stage (Alsamarai et. al, 2013)-ER admissions (Laberta, 2016)-Unmet survivorship needs -Uncoordinated end-of life care (Beckstrand, Smith, Luthy, & Macintosh, 2017)

ONS 43rd Annual Congress
Advanced Practice (Johnson) 5
Emergency Nurses Association Position Statement
• Triage is a process of collecting pertinent information about patients who are seeking emergency care and initiating a decision making procedure that uses a valid and reliable triage acuity designation system.-collecting patient information and performing a focused assessment-assigning an acuity level-prioritizing needs in a time sensitive manner-establishing boundaries of physical and psychological stability and-predict the potential trajectory of the patient’s condition (ENA, 2017).
Triage Tool• Emergency Severity Index (ESI)
5 tier system most urgent to least urgent based on resources and acuity1) Dying 2) shouldn’t wait 3) vital signs 4) one resource 5) no resources (AHRQ, 2013)
Triage Tool • Canadian Emergency Department and Acuity
Scale (CTAS)-developed by a group of Canadian emergency physicians
(Beveridge & Ducharme, 1997); (Bevridge, R., Clarke, B., Janes, L., Savage, N., Thompson, J., Dodd, G., . . .2018). .
-national standard in Canada for ED triage-hospital are required to submit data to the Canadian government
on all ED visits.1. Resuscitation 2. Emergent 3. Urgent 4. Less urgent/semi-urgent 5. Nonurgent

ONS 43rd Annual Congress
Advanced Practice (Johnson) 6
ONP Navigation Triage• Utilizes the nursing process• Utilizes a involving a comprehensive assessment,
which sets priorities for the removal of barriers with the goal of expediting care.
• It simultaneously involves care coordination, and in doing so pulls in resources in the most expeditious manner to facilitate care (Johnson, 2016)
ONP Navigation Triage• Mostly used in the diagnostic phase• Some evidence showed thatit also occurred throughout the cancer continuum• Occurred individually, in groupsof two or even teams with the goal of expediting care (Johnson, 2016)
Patient Triage on an Initial AppointmentDiagnostic Phase
“… I try to focus on that first visit, …to relax and get re-centered…learn about the disease, …and what is really scaring you…and how would you really feel about if you had to have your breasts removed…Some worksheets help them with –everybody thinks they’re going to die…then giving them a timeframe on you’re going to see your surgeon first, and then, you’re going to see the medical oncologist before your surgery, and this is what’s going to happen next for you. teaching them, and then setting up appointments and referrals for them, and maybe additional testing, like going ahead and ordering a breast MRI because of breast issues, there’s a history, and it’s appropriate to go ahead and get an MRI, and get that going, and that way the process is started and the patient has a schedule, and then as all this starts happening, following up with patient…(#18).”
Prescribing, Setting up Priorities in Order of Importance, Expediting Care

ONS 43rd Annual Congress
Advanced Practice (Johnson) 7
“…getting them seen quickly, getting their treatment well organized…So I was able to get her started with genetic screening so that’s sort of done, because she wasn’t going to be getting her MRI for a couple of weeks, and she wasn’t going to be seeing a surgeon, but a little bit after the MRI. So at least the genetics is started up front. Those results might be back by the time they’re making a surgical decision, so it’s kind of coordinating that too… so things happen in a good flow…(#10)”
Prescribing, Setting up Priorities in Order of Importance, Expediting Care
Facility Triage on the Initial Contact“Yeah, I think with that initial contact to identify people that maybe don’t have any resources, as far as they don’t have any family help or they have a very limited help. If they have barriers like they don’t drive, or, they’re in a financial mess. So at least some of those rise to the top, and they will get more help than someone that is very squared away, and can sort of self-navigate. I think that helps too; to sort of pick and choose the ones that need a little more support, or people that might live in unsupportive care, or have a touch of dementia, or that, so that’s helpful to kind of figure out who really needs the help and direct it that way…..(#10).”
Diagnosing, Priortizing, Expediting Care
Community Level Triage“I have all of the oncologists in the area that I have as my leads…so that if they are seeing patients I review their patients…..now some of them are going to be hematology…like DVT…or thrombocytopenia…those are not on my radar…..some I can immediately knock off…so that in any given day I review in all earnestness 10-20 patients in the morning before I even head to the hospital…because there are two hospitals…and if I review patients…I triage…and see which patients need more help…and this is the hospital I go to…and I prioritize throughout the day (#2).”

ONS 43rd Annual Congress
Advanced Practice (Johnson) 8
Partnerships
“Pretty much during the day I’m usually making phone calls, I’m also taking phone calls from patients…contacting with, following up with other departments if we had a patient and that they were finishing out of their chemo, and we wanted to go ahead and get them in radiation. I’m usually the one that contacts radiation. Makes sure the patient is on schedule, or/and say the patient needed some type of—say we wanted to get them in right away for a peg myself and my MA, we usually try to get the patient in. (#13).”
Treatment Planning“….we say this is a newly diagnosed lung cancer…let’s do a multidisciplinary clinic for them…so that we can get a very fast treatment plan together for them...and what that includes is that the patient will be presented at the 0730 conference …and the patient will be seen in the office by a round robin of physicians…a short meeting will follow after the patient is seen by the specialists…again to discuss concerns…and every one is in agreement with what the recommendations are ..and then the patient meets that day with the treatment plan in place…and that is probably the most expedited way to move through our system(#2).”
Survivorship“I would approach them during their waiting visit after theyhave first checked in, accompanying them to their blood draws, and their doctor visit, administer vital signsin the waiting room to the doctor’s visit, and then afterwardsideally to my office where we sit down, and I give them a written treatment summary to make sure that they fully understand their follow-up. I do a distress screening, veryinformal at that time to see if they have needs as survivors,and to let them know that there could be in the futurelong term effects, and we are available as far as a resource for them (#20)”.
ONS 43rd Annual Congress
Advanced Practice (Johnson) 9
End of Life
“I felt we did everything that we could and in her finally days helping the family with the hospice program …you know the husband, she was I guess 50 when she died, but young, not near retirement…you know, he was trying to work …the hospitalization…., the whole thing…interesting, she died like right before the girl graduated from high school… I thought it was successful, even though the patient died, she was well navigated. We helped her with her equipment, her pulmonary, lung drainage kits for the lung metastasis, helped her get what she needed and then when it was all over the husband wanted to get rid of things. I said “just bring them to me and we will take care of all of that” because just he couldn’t in his heart throw it away it was stuff that wasn’t opened and we have some programs that would be more than happy to take some of those supplies that were intact so… (#18)”
Examples of Navigation Tools• It involves the use of tools, would refer you
to the recent publication in Med CRAVEhttp://medcraveonline.com/JCPCR/JCPCR-08-00306.pdf
Examples of Triage ToolsPatient/Facility/Community tools• Patient
-Gail Model Risk Assessment, Lung Nodule Screening CriteriaFacility
• -software programs (NurseNav, Beacon, Home Grown Programs)-pathology report reporting process
• Community –focus groups, smoking cessation program (dovetailed to CT lung screening program);
• (Johnson, 2016)

ONS 43rd Annual Congress
Advanced Practice (Johnson) 10
Practice Application• determine where the bottlenecks on the
patient/facility/community level occur and build triage processes to speed up the process of timely access through the system.
Research Questions
• Importance in the navigation process (Johnson, 2016)-randomized controlled trials involving the patient/facility/community systems which involve all phases of
the cancer continuum, in all levels of care-involve specific standardized metrics, utilizing standardized
measurement tools-developed by systems analysis patient/community/facility level
Existing Patient Tools• Advanced care planning (Hsueh, Dorcy,
2016) • Distress screening (NCCN, 2017)• Symptom management (Stacey et al.,
2016); (COSTAR, 2016)
ONS 43rd Annual Congress
Advanced Practice (Johnson) 11
Existing Facility Tools• Target disease processes (Clark, 2017/2018) • Provide cancer specific emergency service NP
model (Beck, 2017) • Cancer specific toolkit (UKONS, 2018)• Point of referral entry (Sykes, 2017)
ToolsBuild tools that are oncology specific-natural history of the disease-proactive in screening for oncologic emergencies-rate treatment side effects, and treat according to protocol-use established care maps for psychosocial issues-rate barriers to treatment from most important to least important in all areas of the cancer continuum-incorporate a systematic assessment of survivorship and end of life needs and triaging (most important to least important), so that needs are met in a timely fashion
Do what you can, with what you have, where you are.” — Theodore Roosevelt
ONS 43rd Annual Congress
Advanced Practice (Johnson) 12
References• Agency for Healthcare Research and Quality (2013). A triage tool for emergency department. Content last revised February 2013. Retrieved from
http://www.ahrq.gov/professionals/systems/hospital/esi/index.html• Alsamarai, S., Yao, X., Cain, H.C., Chang, B.W., Chao, H.H., Connery, D.M., . . . Rose, M.G. (2013). The effect of lung cancer care coordination program on timeliness of care. Clinical
Lung Cancer, 14, 527–534.• Beck, B. (2017). Oncology emergency department: A nurse practitioner care model. (2017). Advanced Practice Spotlight, (43)6, 575-577. doi: https://doi.org/10.1016/j.jen.2017.08.005• Beck strand, R., Smith, K. E., Luthy, K. E., & Macintosh, J. L. (2017). Emergency nurses suggestions for improving end- of -life care. Journal of Emergency Nursing 43(3), 214-220. doi:
http://dx.doi.org/10.1016/j.jen.2017.03.012• Bevridge, R., Clarke, B., Janes, L., Savage, N., Thompson, J., Dodd, G., . . .(2018). Implementation guidelines. Retrieved form http://caep.ca/resources/ctas/implementation-
guidelines• Beveridge R, Ducharme J (1997). Emergency department triage and acuity: Development of a national model [Abstract]. Academic Emergency Medicine 4(5):475.• Clark, D. (2017/2018). Early diagnosis of pancreatic cancer in a nurse-led, one stop jaundice service. Nursing 10(15), S22-28. • Cooper, J., Loeb, S, & Smith, C. (2010) The primary care nurse practitioner and cancer survivorship care. Journal of the American Academy of Nurse Practitioners, 22(8), 394-402. Doi.10
111/j.1745-7599.2010.00528.x• Corbin, J. & Strauss, A. (1990). Grounded theory research: Procedures, canons, and evaluative criteria. Qualitative Sociology, 13(1), 3-21.• Corbin, J. & Strauss, A. (2008). Basics of qualitative research 3e. Thousand Oaks, CA: Sage Publications, Inc. • Corbin, J. & Strauss, A. (2015). Basics of qualitative research: Techniques and procedures for developing grounded theory. Thousand Oaks, CA: Sage Publications, Inc. • COSTaRS (2016). Remote symptom practice guides for adults on cancer treatments• of the Pan-Canadian Oncology Symptom Triage and Remote Support (COSTaRS) Team. Retrieved https://ktcanada.ohri.ca/costars/COSTaRS_Practice_Guides_ENGLISH_March2016.pdf• Emergency Nurses Association (2017). Triage qualifications and competency. Journal of Emergency Nursing, 43(6), 571-574. doi: https://doi.ord/10.1016/jen.2017.08.008• Glaser, B. G. (1978). Theoretical sensitivity. Mill Valley, CA: The Sociology Press.• Hsueh, M. T., & Dorcy, K. S. (2016). Improving transitions of care with an advanced practice nurse: A pilot study. Clinical Journal of Oncology Nursing, 20(3), 240-243. • Johnson, F. M. (2015). Systematic review of nurse practitioner oncology navigation metrics. Clinical Journal of Oncology Nursing, 19(3), 308-313. doi: 10.1188/15.CJON.308-313• Johnson, F. (2016). The process of oncology nurse practitioner patient navigation: A Pilot Study. Clinical Journal of Oncology Nursing, 20(2), 207-210. doi: 10.1188/16.CJON.207-210• Johnson, F. M. (2016). The process of oncology nurse practitioner patient navigation: A grounded theory approach. (Unpublished doctoral dissertation). Texas Woman’s University,
Houston, Texas.• Johnson, F. (2017). The process of oncology nurse practitioner patient navigation: A grounded theory approach: Navigation tools. Retrieved from
http://medcraveonline.com/JCPCR/JCPCR-08-00306.pdf• Laberta, V. (2016). Perfecting Triage: Keeping oncology patients out of the ED. Oncology Times, 38(25), 4-15. • Lee, J. Y., Oh, S. H., Peck, E. H., Lee, J. M., Park, K. N., Kim, S. H., …Youn, C. S. (2011). The validity of the Canadian triage and acuity scale in predicting resource utilization and the
need for immediate life-saving interventions in elderly emergency department patients. Retrieved from https://sjtrem.biomedcentral.com/articles/10.1186/1757-7241-19-68• Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic inquiry. Newbury Park, CA: Sage Publications.• NCCN (2018). Distress management. Retrieved from https://www.nccn.org/professionals/physician_gls/pdf/distress.pdf• Shenton, A. K. (2004). Strategies for ensuring trustworthiness in qualitative research projects. Education for Information, 22, 63-67.• Stacey, D., Green, E., Ballantyne, B., Tarasuk, J., Skrutkowski, M., Carley, M., . . .Howell, D. (2016). Implementation of symptom protocols for nurses providing telephone-based cancer
symptom management: A comparative case study. Worldviews on evidenced based nursing, 13(6), 420-431. doi: 10.1111/wvn.12166• United Kingdom Oncology Nursing Society (2018). The UKONS oncology/hematology - 24 hour triage - rapid assessment and access tool kit. Retrieved from
http://www.qualityincare.org/oncology/case_studies/the_ukons_oncologyhaematology_-_24_hour_triage_-_rapid_assessment_and_access_tool_kit

ONS 43rd Annual Congress
Advanced Practice (Piseno) 1
Disclosures• Nothing to disclose.
The POWER of Networking:It’s a Small World After All!
Danielle Piseno, BSN, OCNDirector of Clinical Oncology Programs
Lynn Cancer Institute
(crissienonline.com)
ONS 43rd Annual Congress
Advanced Practice (Piseno) 2
100% CHANCE that anyone in this room can add remarkable value to your life!
(Ching, Gordon. 2013)
Why Network??
BUILD RELATIONSHIPS
CONNECTIONS
OPPORTUNITES CAREER ENHANCEMENTS
IDEA BUILDERS
COLLABORATIONS
RESOURCES
Where To Network…
ONS: Local Chapters ONS Congress ONS Community Digest Organizational Events (employer and community) Pharmaceutical Events Journal Authors LinkedIn American Cancer Society Events

ONS 43rd Annual Congress
Advanced Practice (Piseno) 3
How to Build Your Personal Network!
Put Yourself Out There!!!Put Yourself Out There!!!
Be AuthenticBe Authentic
Listen With IntentListen With Intent
Be a Resource Be a Resource
Ask for IntroductionsAsk for Introductions
Putting It In Motion…
Attend a local chapter meeting Introduce yourself to at least one person you do not know Have one KEY question prepared that you will ask to
strike a meaningful conversation Exchange contact information (phone and or email)
Stay Connected!In a timely manner, send a follow up email or brief call to your new contactFor an introduction, send a thank you and keep in touch on how the referral is goingLook for your new connections on Social Media. Facebook & LinkedIn are the 2 most
utilized resources for social networking for all age groups.
(Statista.com, 2014).
(Statista.com, 2014).

ONS 43rd Annual Congress
Advanced Practice (Piseno) 4
Collaborate Share Best Practices Competencies Policies/Procedures Performance Improvement Projects
Personal Experiences
Key Takeaways• Involvement in professional organizations and collaborating
with colleagues not only enhances the oncology nurses' professional development, but ultimately improves patient care.
• Oncology nurses may not fully be aware of the power of networking and the value with being actively involved in professional organizations.
• Utilizing social media, competitions, and rewards are strategies to engage millennials in enhancing oncology patient care and their professional development.

ONS 43rd Annual Congress
Advanced Practice (Piseno) 5
References
• Ching, Gordon. (2013, October 23). The Power of Networking. Retrieved from www.slideshare.net
• Crissien. (2018). Retrieved from https://crissienonline.com
• Pew Research Center. (2014, September). Retrieved from https://statista.com