btec level 3 national health and social care - student book
TRANSCRIPT

1
Credit value: 10
Learning outcomesAfter completing this unit you should:
1 understand effective communication and interpersonal interaction in health and social care
2 understand factors that infl uence communication and interpersonal interaction in health and social care environments
3 understand ways to overcome barriers in a health and social care environment
4 be able to communicate and interact effectively in a health or care environment.
Developing eff ective communication in health and social care
1This unit is designed to help you develop your communication skills. You will explore ways of overcoming barriers to communication and develop your own skills in one-to-one and group interactions.
In order to work with people you must be good at communicating with them. Effective communication requires advanced practical skills in much the same way as driving a car does. Driving a car involves responding to changes in the road ahead, as well as responding to other road users. Effective communication in care involves being sensitive to feedback from others. Sometimes the people you meet may be happy but often they may feel sad, afraid, upset or anxious. You need to be able to recognise and respond appropriately to many different emotional situations. Different contexts will require you to communicate in different ways. Skilled communication requires you to make decisions as to what response would be most effective in the situation you fi nd yourself in. Effective communication involves much more than just giving or receiving information.

2
BTEC’s own resources
Assessment and grading criteriaThis table shows you what you must do in order to achieve a pass, merit or distinction grade, and where you can find activities in this book to help you.
To achieve a pass grade, the evidence must show that you are able to:
To achieve a merit grade, the evidence must show that, in addition to the pass criteria, you are able to:
To achieve a distinction grade, the evidence must show that, in addition to the pass and merit criteria, you are able to:
P1 Explain the role of effective communication and interpersonal interaction in a health and social care context.See Assessment activity 1.1, page 17
M1 Assess the role of effective communication and interpersonal interaction in health and social care with a reference to theories of communication.See Assessment activity 1.2, page 21
P2 Discuss theories of communication.See Assessment activity 1.2, page 21
D1 Evaluate strategies used in health and social care environments to overcome barriers to effective communication and interpersonal interactions.See Assessment activity 1.4, page 40
P3 Explain factors that may influence communication and interpersonal interactions in health and social care environments.See Assessment activity 1.3, page 28
M2 Review strategies used in health and social care environments to overcome barriers to effective communication and interpersonal interactions.See Assessment activity 1.4, page 40
P4 Explain strategies used in health and social care environments to overcome barriers to effective communication and interpersonal interactions.See Assessment activity 1.4, page 40
P5 Participate in a one-to-one interaction in a health and social care context.See Assessment activity 1.5, page 42
M3 Assess your communication and interpersonal skills in relation to each interaction.See Assessment activity 1.5, page 42
D2 Evaluate factors that influence the effectiveness of each interaction.See Assessment activity 1.5, page 42
P6 Participate in a group interaction in a health and social care context.See Assessment activity 1.5, page 42

3
Unit 1 Developing effective communication in health and social care
How you will be assessedYou will need to produce written evidence of examples of the role of communication and interpersonal interaction in health and social care. You will also need to explain theories of one-to-one and group communication. You will need to demonstrate your own skills both in one-to-one and in group interaction situations. Varied assessment tasks are included throughout this unit to help you prepare your work.
Daniel, 17 years oldThis is a very practical unit. Although there’s quite a lot of theory, I found that I ‘sort of knew’ some of the ideas, although I had never put them into words before.
The great thing about studying this unit is that it enables you to explain what’s going on in one-to-one and group situations. The
unit changes the way you understand conversations and the way people behave when they are in groups. Whenever I see people talking,
I start to work out what their body language might mean. I now realise that there are special communication skills that you can use in care work. Sometimes the way you say something can be more important than what you say. There are a lot of barriers in care situations that can stop people from understanding each other. But the unit explains ways of overcoming these problems.
The assignment work is all very practical. To begin with, I had to set up a logbook to record examples of the theory we were studying. We had to study practical examples of the communication cycle and group formation. I went on to explore barriers to communication and how to overcome barriers. I found my supervisor at my practice placement was very helpful in getting me to understand how to overcome barriers. Finally, I had to explore my own skills in one-to-one communication and group situations. I tried analysing several situations that I had experienced before going on to complete my final assignment work.
Over to you!1 Why is skilled communication so important in health and social care work?
2 Do you think effective group or effective one-to-one communication will be the hardest to demonstrate?
3 What part of the practical work for this unit do you think will be most enjoyable?
4
BTEC’s own resources
1 Understanding eff ective communication and interpersonal interaction in health and social care
Changing the way you communicateImagine that you have to interview people in a youth club in a distant city as part of a project. You do not know the members of this club. The members speak English but they are very different from your friends in your local area. The people you are interviewing don’t have to answer your questions.
How would you act to get these people to like you and listen to you?
The way you communicate with other people always depends on the situation or the context you fi nd yourself in. You will have developed effective ways of communicating and interacting with your friends. But if you fi nd yourself in a different context you will need to be able to change the way you act in order to get a good response from people.
Getstarted
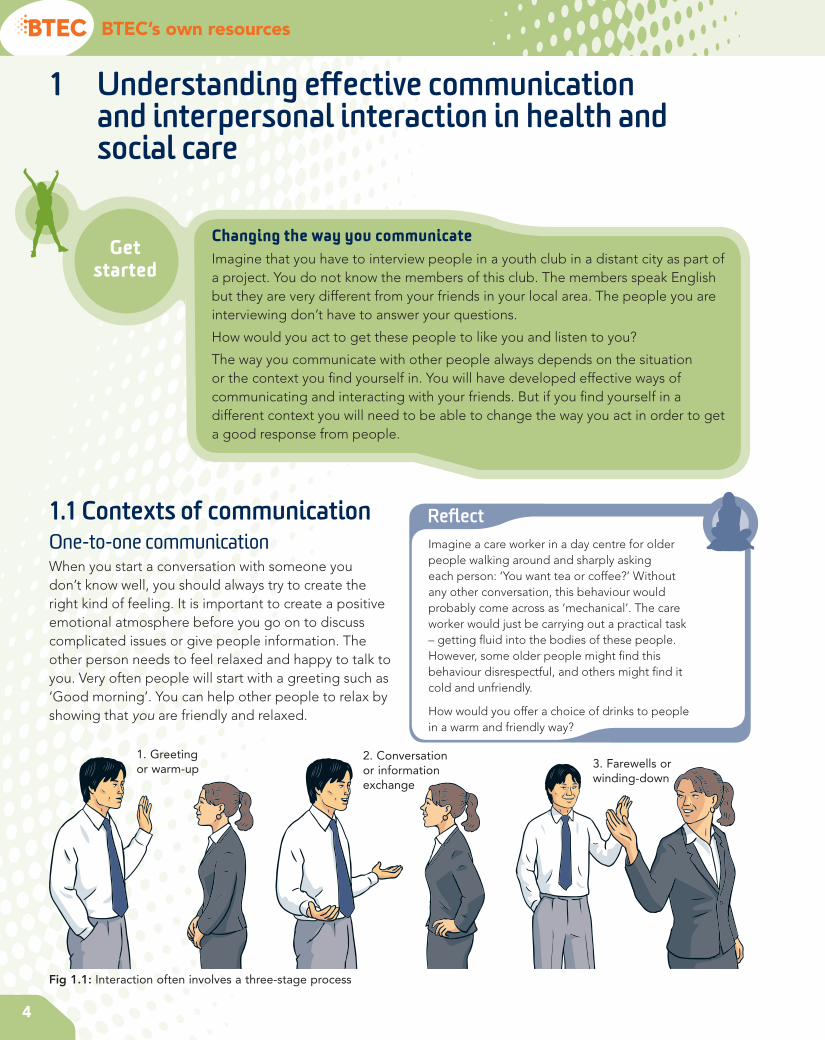
1.1 Contexts of communicationOne-to-one communicationWhen you start a conversation with someone you don’t know well, you should always try to create the right kind of feeling. It is important to create a positive emotional atmosphere before you go on to discuss complicated issues or give people information. The other person needs to feel relaxed and happy to talk to you. Very often people will start with a greeting such as ‘Good morning’. You can help other people to relax by showing that you are friendly and relaxed.
Refl ectImagine a care worker in a day centre for older people walking around and sharply asking each person: ‘You want tea or coffee?’ Without any other conversation, this behaviour would probably come across as ‘mechanical’. The care worker would just be carrying out a practical task – getting fl uid into the bodies of these people. However, some older people might fi nd this behaviour disrespectful, and others might fi nd it cold and unfriendly.
How would you offer a choice of drinks to people in a warm and friendly way?
Fig 1.1: Interaction often involves a three-stage process
2. Conversation or information exchange
3. Farewells or winding-down
1. Greeting or warm-up

5
Unit 1 Developing effective communication in health and social care
Once you have created a good feeling, you can move on to the business – the things you want to talk about. When it is time to finish the conversation, you want to leave the other person with the right kind of emotions so you might say something like ‘See you soon’ to show that you value them. Formal conversations often follow a three-stage model, with an emotional ‘warm-up stage’ at the beginning, a ‘business’ or ‘exchange of information’ stage in the middle, and a ‘winding down stage’ at the end.
Group communicationTaking part in a group discussion involves the same issues as one-to-one communication as well as some additional issues.
How does it feel to be in the group?
Group discussion only works well if people want to be involved. Sometimes people feel threatened if they have to speak within a formal group of people, or they might stay quiet because they are worried about other people’s reactions. It is important that the group has the right emotional atmosphere. People in groups often use humour or other friendly ways of behaving to create the right group feeling, which encourages people to talk. Creating the right group atmosphere involves ‘maintaining’ the group so this aspect of group communication is often called group maintenance.
Is there a group leader?
Some groups, such as team meetings or classroom discussions, have a leader or chairperson. Having a leader is very useful because the leader can encourage people to express their ideas and help them to take turns when talking. Group leaders often encourage people to focus on a particular task within a group.
Have you prepared what you are going to say?
When talking in a formal group you will need to think through your points before sharing them with the whole group. Because of this extra preparation, talking to a group can feel very different from talking in a one-to-one situation.
Are you good at taking turns?
Group communication fails if everybody speaks at the same time. It is harder to work out who should be speaking in a group discussion than in a one-to-one conversation. The skill of taking turns involves identifying the following pattern. When a person is
about to finish speaking they usually signal this by lowering their voice tone, slowing their pace of talking and looking around at other people in the group. The next person to talk knows that it is their turn by watching the eyes of other group members. If people fail to notice these patterns then too many people may try to speak at the same time. If everybody is talking then nobody is listening!
Can everybody see each other clearly?
If people sit in a circle then everyone can see everyone else’s face. This is very important because positive group feeling and successful turn-taking often depend on people being able to understand the messages in other people’s faces. If people sit behind each other or in rows, then some of the group cannot see others’ faces. Bad seating or standing positions can make group communication harder.
Activity 1: Record eye contact and turn-taking in group discussionGet together with five or six colleagues and agree on a current news topic that you would all enjoy discussing for four or five minutes. One of you should use a camcorder to record the eye contact and speech of other group members. Analyse your recording and work out how good people were at taking turns in group discussion.
PLTSIndependent enquirer: This activity will help you demonstrate that you can analyse and evaluate information, judging its relevance and value. The activity may also help to develop team working and participation skills.
Informal communicationWe often use informal communication when we know people well – for example, with friends and family. Some friends or family members may use terms that other people would not understand. Local groups from particular places might also have their own ways of speaking. For example, some people in southern England might say things like ‘Hiya, mate. How’s it goin’?’ If you belong to this group, you will appreciate

6
BTEC’s own resources
this as a warm, friendly greeting. But different groups of people use different informal language so it can sometimes be hard to understand the informal communication of people from different social groups.
Formal communicationHealth and social care work often involves formal communication. For example, if you went to a local authority social services reception desk you might expect to be greeted with the phrase ‘Good morning. How can I help you?’ This formal communication is understood by a wide range of people. Formal communication also shows respect for others. The degree of formality or informality is called the language ‘register’.
Imagine going to the reception desk and being greeted with the phrase ‘What you after then?’ Some people might actually prefer such an informal greeting. It might put them at ease, making them feel that the other person is like them. But in many situations, such informal language could make people feel that they are not being respected. Being ‘after something’ could be a ‘put down’; you might assume that you are being seen as a scrounger. So it is often risky to use informal language unless you are sure that other people expect you to do so. If you are treated informally, you may
interpret this as not being treated seriously, or ‘not being respected’.
So is there a correct way to speak to people when you fi rst introduce yourself? After all, if you are too formal you may come across as pretentious or ‘posh’. Usually care workers will adjust the way they speak in order to communicate respect for different ‘speech communities’.
Communication between colleaguesFamily and friends know you well and will usually understand you, even if you communicate poorly or very informally. Communicating with people at work is different because:
• It is important that care workers communicate respect for each other. Colleagues who do not show respect for each other may fail to show respect to the people who use care services.
• You may often have to greet colleagues by asking if they are well and spend time on ‘warm-up talk’ in order to show that you value them.
• You will need to demonstrate that you are a good listener and can remember details of conversations with your colleagues.
• Colleagues have to develop trust in each other. It is important to demonstrate that you respect the confi dentiality of conversation with colleagues.
• Work settings may have their own social expectations about the correct way to communicate thoughts and feelings. These may differ from social expectations when communicating with your friends and family.
Although communication between colleagues may often be informal it is important that care workers use skilled communication in order to develop respect and trust.
Hiya,I’m ’ere to assess
some geezer who lives’ere – that you?
Fig 1.2: Informality can be seen as a sign of disrespect
PLTSIndependent enquirer: The following activity will help you demonstrate that you can identify questions to answer, and explore issues from different perspectives.
Creative thinker: You may also be able to demonstrate that you can connect your own and other people’s experiences in inventive ways.

7
Unit 1 Developing effective communication in health and social care
Activity 2: Formal and informal communicationGet together with a small group of colleagues and imagine an introductory meeting between a student and a care manager as part of a work practice placement. One person should act as the manager and another as the student. Work out how the manager would welcome the student and explain the work of the care centre. Then work out what questions the student should ask. After you have performed this simulation or role-play, two other students should undertake exactly the same task, but this time they should pretend that they are close friends chatting about the situation.
The whole group should then discuss the differences between these two simulations.
Communication between professional people and people using servicesProfessional people, such as doctors and nurses, often work within their own specialised language community. A language community is a community of people that has developed its own special words, phrases, social expectations and ways of interacting that set it apart from other groups of people. Professionals are usually
Functional skillsEnglish: Your discussion activity may also contribute towards English speaking and listening skills.
well aware of the need to translate technical language into everyday language when they work with people from other professions or people who use services. It is important that professionals check that they are not being misunderstood (see section 2 on the role of feedback).
Communication with professionalsWhen people who use services communicate with professionals there is always a risk of misunderstanding between people from different language communities. It is important that people check that they are being understood correctly. Professional health and social care staff need to check their understanding of issues with people who are communicating with them.
Multi-agency workingHealth and social care professionals often have to communicate with colleagues who work for different organisations. For example, a home care organiser might have to communicate not only with people who use services and care workers but also with community nurses, GPs’ surgeries, hospital services, occupational therapists, voluntary groups, day care groups and many other organisations. It is important not to assume that people from different agencies will understand
Key termLanguage community – A social community of people that has its own special ways of using language in order to communicate between group members.
Case study: AmberThe following conversation took place between members of the same family:
Mother: How was your day at work?
Amber: OK, didn’t do much, walked about a bit. Have to learn where everything is – like.
Mother: Did you enjoy it there?
Amber: Suppose it was all right. I had to listen to a guy going on about stuff but it was boring. Might be better tomorrow. I am going to ‘do’ the residents tomorrow – they should be more fun!
1 If Amber had spoken to her colleagues like this, would they have assumed that Amber respected and valued them?
2 Can you explain why a conversation like this might be acceptable within a family context but not within a work context?
3 Can you explain how Amber should change her comments if she was describing her first day at work to a professional colleague?

8
BTEC’s own resources
the same terminology. Formal communication may help to convey respect and avoid misunderstandings when interacting with unfamiliar professionals in other agencies.
Multi-professional workingProfessionals from different backgrounds often have to work together in order to assess and meet the needs of people who use services. Multi-professional working happens when many different professionals work together. Communication will often need to be formal and carefully planned in order to avoid barriers to understanding.
Refl ectNo one has ever written a rule book defi ning how health and social care workers should behave in all the different contexts listed above. One of the reasons this has not been attempted is that every interaction involves a feedback cycle (see section 2 in this unit). There may not be a single correct way of handling each interaction.
Table 1.1: Degrees of formality in different contexts
Context Degree of formality Key issues
Between colleagues Often informal. Must demonstrate respect for each other.
Between professionals and people using services
Usually informal. Professionals must adapt their language (not use technical terms or jargon) in order to be understood.
With professionals People using services may communicate informally. Professionals may respond formally.
Professionals must take responsibility for checking their understanding.
Multi-agency working Usually formal – unless workers know each other well.
Important not to make assumptions or use technical terminology.
Multi-professional working Usually formal – may need formal planning to produce ‘agendas’ for business.
Different professional people must be careful to check that they are understood.
Case study: KarenKaren is a home care worker. Here are some statements that people have made about the way she works:
‘I always feel better when she visits – she always smiles and cheers me up if I feel down.’
‘She makes you feel important – she always listens to you, even when she is very busy.’
‘She is so easy to talk to – she takes an interest in you. She is never ‘bossy’ or ‘posh’ – she’s like one of my family’.
‘She makes you feel special – not just one of the crowd.’‘She is very kind and considerate. There aren’t very many people like her – it’s a sort of magical touch – you feel different when she is around.’
Karen has excellent interpersonal skills – a ‘magical touch’. Karen’s skills enrich her own life and the lives of other people.
1 Why do some people get on so well with other people?
2 What makes someone good at interpersonal work?

9
Unit 1 Developing effective communication in health and social care
1.2 Forms of communicationCommunication between people enables us to exchange ideas and information but it involves much more than simply passing on information to others. Communication helps people to feel safe, to form relationships and to develop self-esteem. Poor communication can make an individual feel vulnerable, worthless or emotionally threatened.
There are many different types of communication as shown in Fig. 1.3 below.
1.3 Types of interpersonal interactionSpeechDifferent localities, ethnic groups, professions and work cultures all have their own special words, phrases and speech patterns. These localities and groups may be referred to as different speech communities. Some people may feel threatened or excluded by the kind of language they encounter in these speech communities. However, just using formal language will not solve this problem. The technical terminology used by care workers (often called jargon) can also create barriers for people who are not a part of that ‘speech community’.
When people from different geographical areas use different words and pronounce words differently they are often using a different dialect. Some social groups use slang – non-standard words that are understood by other members of a speech community but which cannot usually be found in a dictionary.
Activity 3: Communicating emotionGet together with a small group of colleagues and discuss the relative importance of all the different types of communication in Fig. 1.3 when you try to communicate emotions such as feeling happy or sad. Discuss whether or not spoken words are usually the best way to communicate emotion.
PLTSCreative thinker: This activity will help you demonstrate that you can generate ideas and explore possibilities.
Independent enquirer: The activity may also lead you to identify questions and problems to resolve.
Key termsJargon – Words used by a particular profession or group that are hard for others to understand.
Dialect – Words and their pronunciation, which are specific to a geographical community. For example, people who live in the north west of England might use a different dialect from Londoners.
Slang – Informal words and phrases that are not usually found in standard dictionaries but which are used within specific social groups and communities.
Types of communication
One-to-one spoken communication
between individuals
Text messaging using mobile phones
Unspoken communication using
facial expressions
Spoken (oral) communication within
groups of people
Braille communication using raised marks
on paper that can be touched
Communication using information technology, e.g. emails and other
technological aids to communication
Written communication
The use of signed (visual) languages
Artwork, paintings, photographs,
sculptures, architecture, ornaments and other objects communicate
messages and emotions
Music and drama have been called the language of emotion.
Mime and drama provide powerful ways
of communicating
Fig 1.3: Forms of communication

10
BTEC’s own resources
First language
The author and psychologist Steven Pinker (1994) estimated that there may be about 600 languages in the world that are spoken by more than 100,000 people. There are many more minority languages. Some people grow up in multilingual communities, where they learn several languages from birth. But many people in the UK have grown up using only one language to think and communicate. People who learn a second language later in life often fi nd that they cannot communicate their thoughts as effectively as they might have done using their fi rst language. The fi rst language that people have learned to think in usually becomes their preferred language.
Case study: Professional jargonThe following conversation involves speech from different speech communities.
Relative: If my mother needed care who would pay for it?
Professional: Well the national framework for NHS continuing health care and NHS funded nursing care provides principles and processes for an assessment process that will establish eligibility for NHS continuing health care.
Relative: So the NHS would pay for care?
Professional: No, as I said, the framework provides
for guidance that must be followed by all PCTs to result in a national assessment process supported by a checklist tool, decision support tool, and fast track tool which are used to provide clarity, transparency and consistency in the decision-making process for eligibility.
1 Can you work out what the professional is talking about?
2 Can you see how technical and legal terminology can exclude people?
3 Will the relative feel helped and respected by such a technical answer?
Non-verbal communicationWithin a few seconds of meeting an individual you will usually be able to tell what they are feeling. You will know whether the person is tired, happy, angry, sad, frightened – even before they say anything. You can usually guess what a person feels by studying their non-verbal communication.
Non-verbal means ‘without words’, so non-verbal communication refers to the messages that we send without using words. We send these messages using our eyes, the tone of our voice, our facial expression, our hands and arms, gestures with our hands and arms, the angle of our head, the way we sit or stand (known as body posture) and the tension in our muscles.
Posture
The way you sit or stand can send messages. Sitting with crossed arms can mean ‘I’m not taking any notice’. Leaning back can send the message that you are relaxed or bored. Leaning forward can show interest or intense involvement.
Did you know?Teenagers can be thought of as a speech community with their own slang. Lucy Tobin has published a book called Pimp your vocab, which acts as a dictionary for ‘teek people’ – people who are outside the teenage speech community. This ‘teenglish dictionary’ enables others to understand teenage terminology.
Many people think the book is great fun, but some critics argue that adolescent language changes so rapidly that it is hard to keep up to date and to be sensitive to local variations.
Person 2 Person 1
Fig 1.4: You can see that person 2 is rejecting what person 1 is communicating
Key termFirst language – The fi rst language that a person learns to speak is often the language that they will think in. Working with later languages can be diffi cult, as mental translation between languages may be required.

11
Unit 1 Developing effective communication in health and social care
The way you move
As well as posture, your body movements will communicate messages. For example, the way you walk, move your head, sit, cross your legs and so on will send messages about whether you are tired, happy, sad, or bored.
Facing other people
The way in which you face other people can also communicate emotional messages. Standing or sitting face-to-face may send a message that you are being formal or angry. A slight angle can create a more relaxed and friendly feeling.
Fig 1.5: Square-on orientation can communicate aggression
Gestures
Gestures are hand and arm movements that can help us to understand what a person is saying. Some gestures carry a common meaning in most communities in the UK.
Fig 1.6: Common gestures for ‘good’ and ‘perfect’
Can you see how a person’s emotions can often be interpreted from their facial expression?
Facial expression
Your face often indicates your emotional state. When a person is sad they may signal this emotion by looking down – there may be tension in their face and their mouth will be closed. The muscles in the person’s shoulders are likely to be relaxed but their face and neck may show tension. A happy person will have ‘wide eyes’ that make contact with you – and they will probably smile. When people are excited they move their arms and hands to signal this.
We can guess another person’s feelings and thoughts by looking at their eyes, using eye-to-eye contact. Our eyes get wider when we are excited, attracted to, or interested in someone else. A fixed stare may send the message that someone is angry. In European culture, looking away is often interpreted as being bored or not interested.

12
BTEC’s own resources
Most people can recognise emotions in the non-verbal behaviour of others. You will also need to understand how your own non-verbal behaviour may infl uence other people.
Touch
Touch is another way of communicating without words. Touching another person can send messages of care, affection, power over them or sexual interest. The social setting and a person’s body language will usually help you to understand what their touch might mean. But touch can easily be misinterpreted. You might try to comfort someone by holding their hand but they may interpret this touch as an attempt to dominate. Sometimes it can be a good idea to ask if you may
Case study: TonyaTonya is 15 years old and attends meetings of a youth group. She often sits with her arms crossed and her head turned away, looking out of the window. She avoids making eye contact with people who are speaking to the group. When asked if she feels OK, she does make eye contact, changes her body posture and says she is happy to be in the group.
1 What messages would crossed arms and avoidance of eye contact normally send?
2 How many reasons can you think of to explain why someone might sit with their arms crossed, looking out of the window, while other people are speaking?
3 How can you fi nd out what an individual’s body language means?
touch, or gesture in a way that allows another person to refuse your touch, before proceeding.
People may also look at, or feel, the degree of muscle tension that you show when you communicate with them. The tension in your feet, hands and fi ngers can tell others how relaxed or tense you are. If someone is very tense their shoulders might stiffen, their face muscles might tighten and they might sit or stand rigidly. A tense person may have a fi rmly closed mouth, with lips and jaws clenched tight, and they might breathe quickly.
Silence
One defi nition of friends is ‘people who can sit together and feel comfortable in silence’. Sometimes a pause in conversation can make people feel embarrassed – it looks as if you weren’t listening or you weren’t interested. Sometimes a silent pause can mean ‘let’s think’ or ‘I need time to think’. Silent pauses can be OK, as long as non-verbal messages that show respect and interest are given. Silence doesn’t always stop the conversation.
Voice tone
When you speak to other people, your tone of voice is important. If you talk quickly in a loud voice with a fi xed tone, people may think you are angry. A calm, slow voice with a varying tone may send a message of being friendly.
Proximity
The space between people can sometimes show how friendly or ‘intimate’ the conversation is. Different cultures have different customs regarding the space between people when they are talking.
In Britain there are expectations or ‘norms’ as to how close you should be when you talk to others. When talking to strangers we usually keep ‘an arm’s length’ apart. The ritual of shaking hands indicates that you have been introduced – you may come closer. When you are friendly with someone you may accept them being closer to you. Relatives and partners might not be restricted at all in how close they can come.
Proximity is a very important issue in health and care work. Many people have a sense of personal space. A care worker who assumes it is fi ne to enter the personal space of a person who uses services, without asking or explaining why, may be seen as dominating or aggressive.
.
Fig 1.7: Gestures and words give a person the option of refusing touch
13
Unit 1 Developing effective communication in health and social care
Reflective listening
We can often understand other people’s emotions just by watching their non-verbal communication. However, we can’t always understand someone’s thoughts without good listening skills.
Listening skills involve hearing another person’s words, then thinking about what their words mean, then thinking about how to reply to the other person. Sometimes this process is called ‘active listening’ and sometimes ‘reflective listening.’ The word ‘reflective’ is used because the person’s conversation is reflected back (like the reflection in a mirror) in order to check understanding. As well as remembering what a person says, good listeners will make sure that their non-verbal behaviour shows interest.
Skilled listening involves:
• looking interested and communicating that you are ready to listen
• hearing what is said to you
• remembering what was said to you, together with non-verbal messages
• checking your understanding with the person who was speaking to you.
We can learn about people who are different from us by checking our understanding of what we have heard. Checking understanding can involve listening to what the other person says and then asking questions. Reflection may also involve putting what a person has just said into our own words (paraphrasing) and saying it back to them, to check that we have understood what they were saying.
When we listen to complicated details of other people’s lives, we often begin to form mental pictures based on what they tell us. The skill of listening involves checking these mental pictures. Good listening involves thinking about what we hear while we are listening and checking our understanding as the conversation goes along – we reflect on the other person’s ideas.
Good listening can feel like really hard work. Instead of just being around when people speak, we have to build an understanding of the people we communicate with.
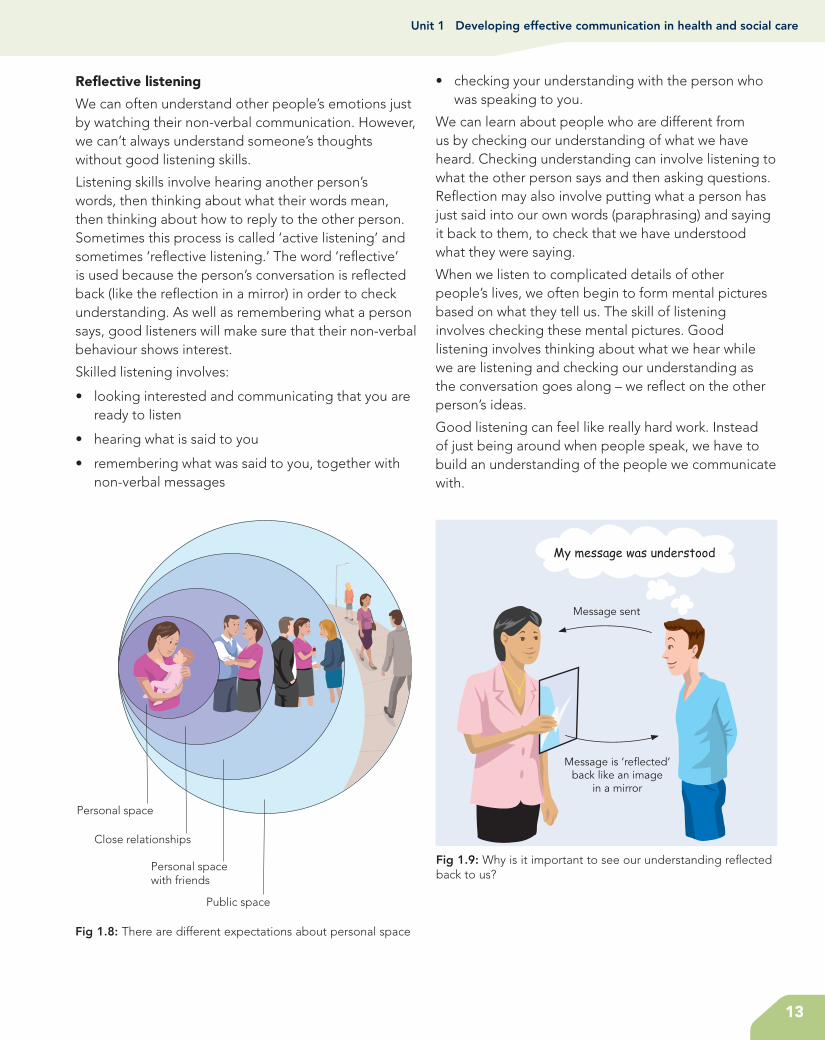
Personal space
Close relationships
Personal spacewith friends
Public space
Fig 1.8: There are different expectations about personal space
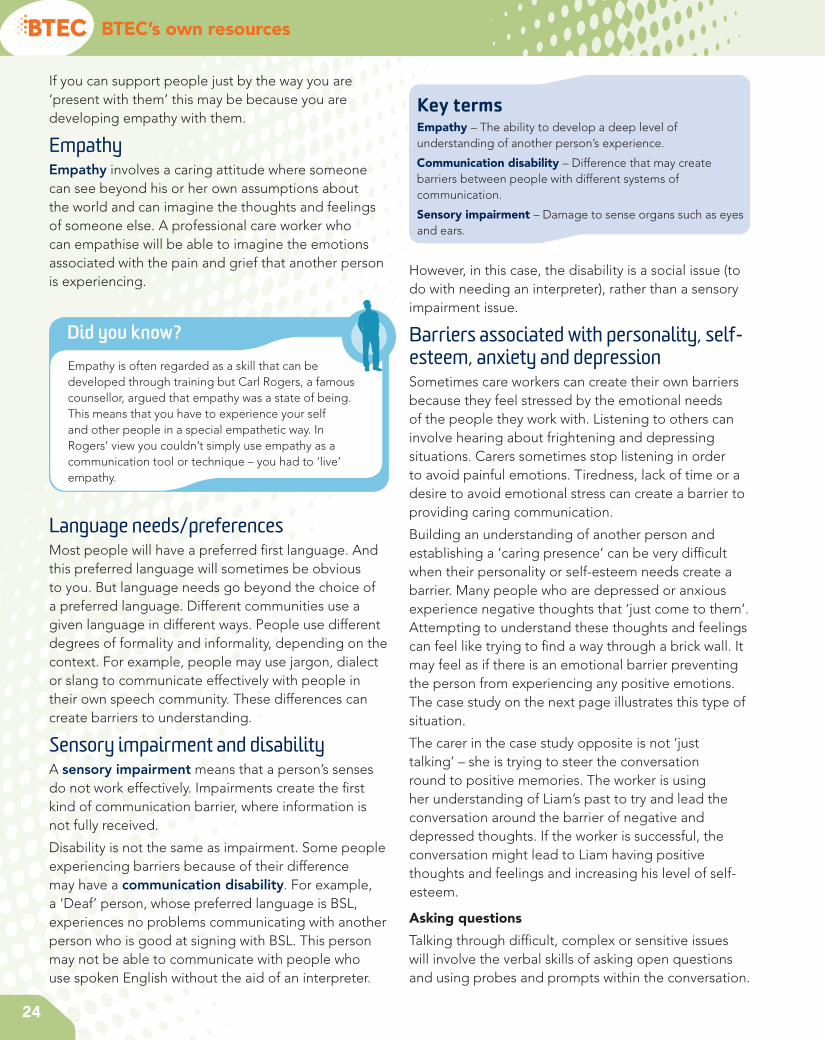
Message is ‘re�ected’back like an image
in a mirror
Message sent
Fig 1.9: Why is it important to see our understanding reflected back to us?

14
BTEC’s own resources
1.4 Communication and language needs and preferencesSpoken and written English are not the preferred system of communication for everyone. The fi rst (or main) language of many Deaf people may be a signed language. People who are registered blind may use Braille, as opposed to written text, in order to read information.
British Sign LanguageBritish Sign Language is a language in its own right – not simply a signed version of spoken English. The British Deaf Association explains that British Sign Language is the fi rst or preferred language of many Deaf people in the United Kingdom. The British Deaf Association also explains that BSL was recognised as an offi cial British language in 2003 and the Association campaigns for the right of Deaf people to be educated in BSL and to access information and services through BSL. Many Deaf people argue that the Deaf
Case study: SarahSarah is unemployed and is looking for work in a specialised fi eld. She looks worried and says ‘I don’t know what to do. I keep looking for work and going for interviews but I never get a job offer.’ Given that you know nothing about the kind of job she is looking for, how can you respond in a skilled way? Consider some of the possibilities below:
• Try to be reassuring, e.g. ‘I’m sure you will get a job eventually.’Unless you are an expert with detailed knowledge of the job market, reassurance is likely to sound false. You may come across as trying to avoid the topic or trick the person.
• Offer advice, e.g. ‘Why don’t you see a careers adviser?’Receiving unwanted advice can sometimes be very irritating. The person may have already thought of seeing an adviser. You might come across as trying to sound clever and superior to Sarah. You might be seen as trying to avoid the issue, i.e. ‘This is all I can think to say, please don’t talk to me about this any more.’
• Repeating what was said, e.g. ‘You never get a job offer.’Parroting some phrases back to a person may sound mechanical. The person might say: ‘That’s what I just said – didn’t you hear me?’
• Refl ecting the other person’s message, e.g. ‘It must be worrying when you can’t get a job.’This shows that you have listened and it may be seen as an invitation to keep talking. Being able to talk to someone who is actively involved may make the other person feel that they are being taken seriously.
1 What is the difference between saying things such as ‘Why don’t you see an adviser’ or ‘I’m sure you will get a job eventually’ and just saying ‘I don’t want to talk to you about it’?
2 Can you explain the difference between just repeating or parroting the words you have heard and the idea of refl ective listening?
3 Why might another person feel that you care about them because you can refl ect back what they have said?
community should be identifi ed as ‘culturally Deaf’ by using a capital ‘D’ for Deaf. This emphasises that ‘Deaf’ people use another language system, as opposed to ‘Deaf’ people who are perceived to be impaired.
Further details of BSL can be found at www.bda.org.uk
Details of signs and a fi nger spelling alphabet can be found at www.british-sign.co.uk and at www.royaldeaf.org.uk
MakatonMakaton is a system for developing language that uses speech, signs and symbols to help people with learning diffi culties to communicate and to develop their language skills. People who communicate using Makaton may speak a word and perform a sign using hands and body language. There is a large range of symbols to help people with learning diffi culties to recognise an idea or to communicate with others. Further information on Makaton can be found at www.makaton.org

15
Unit 1 Developing effective communication in health and social care
Activity 4: Research people’s understanding of BSLDo people understand what British Sign Language is? Plan a short series of questions and ask people who are not studying this course if they have ever heard of British Sign Language and what kind of language it might be? You may find that the majority of people think that BSL is a way of signing English words – in other words that to sign in BSL you would first have to know English. Only a few people might understand that BSL is a separate language developed within the Deaf community. Discuss what consequences your research might have for both Deaf and hearing people.
PLTSIndependent enquirer: This activity will help you demonstrate that you can plan and carry out research and appreciate its consequences.
Written communicationThere is a Chinese saying that ‘the faintest ink is stronger than the strongest memory’! Written records are essential for communicating formal information that needs to be reviewed at a future date. When people remember conversations they have had, they will probably miss out or change some details. Written statements are much more permanent and, if they are accurate when they are written, they may be useful later on.
Pictures and objects of referencePaintings, photographs, sculptures, architecture, ornaments and other household objects can communicate messages and emotions to people. People often take photographs or buy souvenirs to remind them of happy experiences and emotions. Sometimes an object – such as a cuddly toy – can symbolise important personal issues and provide a source of meaning and comfort for an individual.
Fig 1.10: What meanings do these signs communicate?
BrailleBraille (a system of raised marks that can be felt with the fingers) provides a means of written communication, based on the sense of touch, for people who have limited vision. The communication system known as Braille was first published by Louis Braille, a blind 20-year-old, in 1829. This system is now widely used, for reading and writing, by people who cannot see written script.
Modern computer software can translate written material into Braille, which can be printed out using special printers. Further details on Braille can be found at www.brailleplus.net
Use of signs and symbolsGestures made with hands or arms, written symbols or diagrams (such as traffic signs) all communicate messages to people.
Key termObject of reference – An object of reference is a physical object or picture that has become associated with an activity, person or other special meaning.
Objects can sometimes be used to communicate with people who do not use much signed or spoken language. A child or adult with a learning disability might understand that a cup stands for ‘would you like a drink’. An object like a spoon tied to a card might communicate that it is time for dinner when the spoon is presented. A person without language might use a patch of cloth to communicate that they wish to sit in a favourite chair covered in that type of cloth. Sometimes a person might learn a symbol, perhaps a symbol like a horseshoe that can be used to label possessions or identify his or her room.
Finger spellingPeople who use a signed language, such as British Sign Language, also use finger spelling. Finger spelling enables signers to spell out words that do not have a general sign, or words that may be misunderstood such as the names of people and places.

16
BTEC’s own resources
Communication passportsCommunication passports are usually small personalised books containing straightforward practical information about a person and their style of communication. The passport may help health and care workers to understand the needs of a person with communication diffi culties. Communication passports often include photographs or drawings that may help care workers to gain a better understanding of the person who owns the passport. They are put together by working with the person with communication diffi culties and his or her carers; the person tells their own story of their likes, dislikes and communication styles.
Technological aids to communicationInformation technology offers a wide range of facilities to help with communication. It is possible to provide enlarged visual displays or voice description for people with visual impairment. Electronic aids – such as the minicom for people with a hearing disability or voice typing for people with dyslexia – can turn
speech into writing. Some electronic communication systems can be activated by air pressure, so that a person can communicate via an oral tube connected to computerised equipment. At a simpler level, aids such as fl ash cards or picture books can also improve communication with people who do not use a spoken or signed language. Text messaging, using a mobile phone, provides an effective way of staying in touch for many people. For people with a hearing disability, text messaging may provide a major form of communication.
Think about the way children communicate through play using objects
Refl ectImagine that you had to spell every word in a phone conversation – it would take a long time and the conversation would not be very enjoyable. For this reason, people who use signed languages do not generally use fi nger spelling to communicate, other than for specifi c terms.
Did you know?In August 2009 a Roman Catholic Archbishop, Vincent Nichols, was reported as saying that ‘too much exclusive use of electronic information dehumanises what is a very, very important part of community life and living together... We’re losing social skills, the human interaction skills, how to read a person’s mood, to read their body language.’
How far do you think email and text messages may spoil or improve relationships between people?
When you send text messages to friends, do you use symbols and shortened words that would not be acceptable in more formal academic work? If you send emails, do you use abbreviations, symbols and special terms or do you only use formal English? Do you think it should be acceptable to use ‘texting’ symbols and abbreviations for academic work? How formal should English be?
Human aids to communicationMany people have specifi c communication needs. It may be important to employ an interpreter if a person uses a different language such as BSL. Some carers learn to use communication systems, such as Makaton, in order to help them communicate with people.
If you are communicating with a person with a hearing impairment you should make sure that the person can see your face clearly so that they can see your expressions and the way your lips move. Sometimes people use clues from facial expression and lip movement to interpret what you might be saying. It is also important to speak in a clear, normal voice. If you raise your voice, your face and lips will become distorted. A person with a hearing impairment may realise that you are shouting and may assume that you

17
Unit 1 Developing effective communication in health and social care
are angry! It is also important to try and speak in an environment with little background noise.
If people have limited vision, it may be important to use language to describe issues that a sighted person might take for granted, such as non-verbal communication or the context of certain comments. Touch may be an important aspect of communication. For instance, some registered blind people can work out what you look like if they can touch your face in order to build an understanding of your features.
It is always important to choose the right style of language in order to communicate with people from different language communities.
Variation between culturesSkilled carers use a range of conversational techniques when working with others. These include being sensitive to variations in culture.
Culture means the history, customs and ways of behaving that people learn as they grow up. People from different regions of Britain use different expressions. Non-verbal signs vary from culture to culture. White middle-class people often expect people to ‘look them in the eye’ while talking. If a person looks down or away a lot, they think it is a sign that the person may be dishonest, or perhaps sad or depressed. In some other cultures – for example, among some black communities – looking down or away when talking is a sign of respect.
No one can learn every possible system of cultural variation in non-verbal behaviour but it is possible to learn about the ones that are used by the people you are with! You can do this by first noticing and remembering what others do – in other words, what non-verbal messages they are sending. The next step is to make a guess as to what messages the person is trying to give you. Finally, check your understanding (your guesses) with the person. This involves reflective listening and thinking carefully about the person’s responses.
Key termCultural variation – Communication is always influenced by cultural systems of meaning. Different cultures interpret verbal and non-verbal communication behaviours as having different meanings.
Care workers must be careful not to assume that statements and signs always have the same meaning. Cultural differences and different settings can alter what things mean. A vast range of meanings can be given to any type of eye contact, facial expression, posture or gesture. Every culture, and even small groups of people, can develop their own system of meanings. Care workers have to respect differences but it is impossible to learn all the possible meanings that phrases, words and signs may have.
P1Assessment activity 1.1
Explain, using examples you have observed, the role of communication and interpersonal interactions in health and social care.
Grading tipP1 Maintain a logbook to record notes of
interactions you have observed in class role plays, informally with your peers, with others at work and in school/college or in public spaces and particularly in health and social care settings when visiting or in placements. Note behaviours, non-verbal communication skills and how the communication cycle is/is not demonstrated. Remember that your notes should maintain
the anonymity of individuals and any details that might enable individuals or settings to be identified.
Consider what is meant by ‘effective’ when discussing communication and interpersonal interactions in health and social care.
Consider formal and informal communication, differences between different language communities and cultures and the role of verbal and non-verbal communication in interpersonal interactions.
Include examples of different language needs and preferences in your explanation.

18
BTEC’s own resources
2 Understand factors that infl uence communication and interpersonal interaction in health and social care environments
2.1 Theories of communicationThe communication cycleEffective communication involves a two-way process in which each person tries to understand the viewpoint of the other person. Communication is a cycle because when two people communicate they need to check that their ideas have been understood. Good communication involves the process of checking understanding, using refl ective or active listening.
Michael Argyle (1972) argued that interpersonal communication was a skill that could be learned and developed in much the same way as learning to drive a car. Argyle emphasised the importance of feedback in skilled activities. When you drive a car you have to change your behaviour depending on what is happening on the road. Driving involves a constant cycle of watching what is happening, working out how to respond, making responses and then repeating this cycle until you reach your destination.
According to Argyle, skilled interpersonal interaction (social skills) involves a cycle in which you have to translate or ‘decode’ what other people are communicating and constantly adapt your own behaviour in order to communicate effectively. Verbal and non-verbal communication is not always straightforward. The communication cycle involves a kind of code that has to be translated. You have to work out what another person’s behaviour really means.
Key termCommunication cycle – Most important communication in care work involves a cycle of building understanding using an active process of refl ecting on, and checking out, what the other person is trying to communicate.
One way of looking at this cycle might be:
1 An idea occurs: You have an idea that you want to communicate.
2 Message coded: You think through how you are going to say what you are thinking. You put your thoughts into language or into some other code such as sign language.
3 Message sent: You speak, or perhaps you sign or write, or send your message in some other way.
4 Message received: The other person has to sense your message – they hear your words or see your symbols.
5 Message decoded: The other person has to interpret or ‘decode’ your message (i.e. what you have said). This is not always easy, as the other person will make assumptions about your words and body language.
6 Message understood: If all goes well then your ideas will be understood but this does not always happen fi rst time!
1. Ideas occur
2. Message coded
3. Message sent
4. Message perceived
5. Message decoded
6. Feedback – what was understood
Fig 1.11: What are the stages in the communication cycle?

19
Unit 1 Developing effective communication in health and social care
Tuckman’s stages of group interactionCommunication in groups can also be influenced by the degree to which people feel they belong together. When people first meet in a group they often go
through a process of group formation. Many groups may experience some sort of struggle before people unite and communicate effectively. One of the best-known theorists to explain group formation stages is Tuckman (1965). Tuckman suggested that most groups go through a process involving four stages. These are:
1 forming
2 storming
3 norming
4 performing.
The first stage (forming) refers to people meeting for the first time and sharing information. The second stage (storming) involves tension, struggle and sometimes arguments about the way the group might function. The third stage (norming) sees the group coming together and consciously or unconsciously agreeing on their group values. Once they have established common expectations and values, the group will reach the fourth stage of being an effectively performing group.
PLTSIndependent enquirer: This activity may help you demonstrate that you can analyse and evaluate information.
Functional skillsICT: Discussing this activity may help you demonstrate that you can evaluate the selection and use of ICT tools and facilities used to present information.
Key termGroup values – Group members need to share a common system of beliefs or values in order for the group to communicate and perform effectively. You may be able to identify these values when you watch a group at work.
Case study: KarenKaren is talking to Jasmin, whose partner has died.
Jasmin: I can’t believe it. I don’t know how I’m going to cope on my own, I can’t sleep or eat.
Karen: You must feel awful, it must have been a terrible shock.
Jasmin: I’ll say it was – I just feel so anxious. I know I won’t be able to cope.
Karen: Can you tell me a little about your life together?
In this brief example, there is no helpful advice or information that Karen can offer. Karen is careful to reflect back what Jasmin has said. This results in a communication cycle in which Jasmin can begin to share her feelings.
1 Can you explain why it is so important for care workers to say back what they understand?
2 What might have happened if Karen had responded with ‘Don’t worry, you’ll feel better as time goes by’?
3 How can understanding the communication cycle help care professionals to develop skilled communication?
Activity 5: Observe the communication cycleWork in a small group and plan how to record the speech and faces of two people talking. Agree on a topic of conversation and record pairs of people talking to each other for up to five minutes. Analyse your recordings in terms of the six stages of the communication cycle.

WorkSpace
1 Using Tuckman’s theory, can you identify which stage of group formation this group is at?
2 Can you identify different norms that are being argued about in the group?
3 Can you identify the different ‘sides’ being taken in the discussion and how Jenna is starting to use her group leader role to get the team to focus on common values?
4 If this group is to succeed in working they will have to share common ‘norms’. Can you guess on what norms the group might eventually agree?
5 If you were in Jenna’s position, how would you lead the conversation on from Shanice’s last comment in order to reach the ‘norming stage’ of team working?
20
André: Yes, but he didn’t burn himself and he is learning to become independent. I
think it’s important to let people take risks. I could never have become independent if my parents hadn’t let me take risks!
Deja: So it’s all right for Drew to burn himself, is it? Is that what you’re saying?
Shanice: I can’t believe you just said that! André is talking about the importance of independence and you turn that round to saying he doesn’t care about people burning themselves. That’s not what he
said – you didn’t listen!
Deja: Now you listen to me! What I am saying is that we don’t take safety seriously enough. These people are vulnerable, they can hurt themselves if we don’t take proper care.
Jenna: OK, we all know that both safety and independence are central to our work here. So why are we talking as if we can’t have both?
Deja: Well, I agree that both are important, but safety comes fi rst as far as I’m concerned.
Shanice: Well I don’t think things are that simple. It is possible to concentrate too much on safety and then we might stop people from reaching their
potential of independence. It’s a matter of getting the balance right.
Think about it!
Pinewoods is a day centre for adult people
with learning disabilities. Jenna is the team leader for a new group of care workers who have only been working
together for the past two weeks. They have regular team meetings and this is an extract from their third meeting in which they are discussing the activities that they lead with day centre members.
Jenna: Let’s talk about the cookery sessions. I think that members are really enjoying learning to cook.
Carly: Maybe, but I worry about what we’re doing. We don’t watch people carefully enough. For example, Drew nearly
burned himself last Tuesday because nobody was watching what he was doing.
Je� a BlackDay centre team leader
André:himself and he is learning to become independent. I
together for the past two weeks. They have regular team meetings and this is an extract from their third meeting in which they are discussing the activities that they lead with day centre members.
Jenna:really enjoying learning to cook.
Carly:

21
Unit 1 Developing effective communication in health and social care
2.2 Environmental factors that infl uence communicationIt is very hard to hear what someone is saying if there is a lot of background noise. It is also very diffi cult to make sense of other people’s facial expressions if you can’t see their faces properly due to poor lighting. Rooms with awkward seating positions might mean that a group of people cannot see each other comfortably. People sometimes feel uncomfortable if they are trying to communicate with a person who is too close or at a distance. A room that is too hot, stuffy or cold may inhibit communication if it makes people feel tired or stressed.
The environment also plays an important role in the effectiveness of communication aids. For instance, hearing aids will amplify background noise as well as the voice of the speaker. A noisy environment may therefore be diffi cult and unpleasant for someone who is using a hearing aid. Good lighting will be critical for someone who supports their understanding of speech with lip reading. Time limits on how long you can use a room can also interfere with communication.
Assessment activity 1.2
Using examples from your experience, discuss theories of communication. This assessment could be integrated with Assessment Activity 1.1.
For M1, you should also include an assessment of the role of effective communication and interpersonal interaction in health and social care.
Grading tipsP2 Consider how communication theory helps to
explain effective communication in health and social care contexts.
Consider one-to-one and group interactions, formal and informal communication, different types of communication and different forms of interpersonal interaction in your discussion.
Reviews of fi lmed class role-plays in which you and your peers have participated would be helpful to gain understanding of the communication cycle.
Participation in a series of group tasks with the same group of individuals over a period of several weeks and an analysis of how your work with each other changes over time could provide useful understanding of Tuckman’s theory. This could involve group work in class with your peers or how you settle into working with a group of individuals in a work experience placement or any employment.
M1 Integrate your assessment by using the examples explained for P1 and discussed in P2.
The assessment should consider strengths and weaknesses of communication and interpersonal interactions you have observed in relation to theories relating to the communication cycle and group formation
Remember to consider a range of health and social care contexts, different forms of communication and different types of interpersonal interaction in your assessment.
P2 M1
PLTSCreative thinker: This activity will help you demonstrate that you can generate ideas and explore possibilities and perhaps try out alternatives.
2.3 Barriers to communicationA barrier blocks things and stops them ‘getting through’. There are different types of communication barrier that stop communication from being effective. Three types are shown in Table 1.2 on page 22.
Where the fi rst and second types of barriers exist, it will usually be obvious that communication has failed. However, distorted understanding is not always easy to identify. Skilled use of the communication cycle may help you to check what has been understood or what communication barriers may exist.
Activity 6: Plan a good environment for group communicationGet together with a group of colleagues and make a list of what an ideal environment for videoing a group discussion would involve. Work out what practical changes you may be able to introduce into your own working environment.
Je� a BlackDay centre team leader

22
BTEC’s own resources
Table 1.2: Communication barriers
Type of barrier Examples
1 Communication is not received
Not responding to language needs or preferences. Not understanding sensory impairment or disability.
Examples: Speaking to a Deaf person who uses a signed language. The sounds are not received.
Environmental barriers:
Background noise can stop you from hearing a message. You can’t receive full non-verbal communication if you can’t see a person’s face or body.
2 Communication is received but not understood
A person using slang, jargon or complex technical terminology can be heard, but their message may not be understood.
3 Understanding is distorted A wide range of emotional and psychological factors can act as barriers, resulting in distorted understanding of communication.
Fig 1.12: Consider why barriers can mean that no information is communicated
,
Fig 1.13: How can psychological factors create communication barriers by distorting perception of a message?
Key termCommunication barrier – Anything that stops the development of understanding when people interact.

23
Unit 1 Developing effective communication in health and social care
Types of communication: difficult, complex or sensitiveSome communication between people is simply about sharing or ‘transmitting’ information. For example, someone might want to know what number bus to catch, or they might ask for a drink of water. Sometimes communication will be complex. For example, a relative may want to know about funding arrangements for care. A communication about funding might involve a great deal of complex information. In this situation it would be important to check what the relative already knew, and whether or not the individual understood the information you were providing.
A great deal of communication in care work involves building an understanding of another person and providing emotional support. Burnard and Morrison (1997) argue that caring and communicating are inseparably linked. Communication that involves emotional issues is often experienced as being difficult or sensitive.
There is no advice or information that is likely to be very useful to a person who is overwhelmed by grief, but many people do want someone to be with them. Communication in this difficult or sensitive situation
should focus on emotional needs, rather than giving out information.
Engebretson (2003) uses the idea of a caring presence to explain what is needed in these situations. Creating a caring presence is about sharing an understanding of the feelings that other people may be experiencing. Sometimes simply being with a person who is lonely, anxious or depressed can provide comfort. If you believe that your carer understands your needs and is concerned about you, then just knowing that they are near you can help you to feel supported. Non-verbal communication may sometimes communicate emotions and feelings more effectively than words.
ReflectWhat can you say to a person who is upset and crying because they can’t cope, following the death of their partner?
Key termCaring presence – Being open to the experience of another person through a ‘two-way’ encounter with that person.
Case study: KarenInterviewer: Some people who need care have
problems with understanding and memory. How do you know if a person has understood what you are talking about?
Karen: It’s not easy but sometimes you can tell from a person’s face. When a person looks puzzled, or if they don’t respond, then you know you’ve got to try and explain something in a different way.
But some people will nod and smile although they haven’t really understood you. So I try to keep the conversation going and find a way to check understanding. For example, I had to explain I would come on a different day. Now, I couldn’t ask the person a direct question like
‘Can you remember what I told you?’ If I did that, the person might feel I was treating them like a child. So instead I asked them about what they would be doing on the day that I had changed from. They said that I would be coming to see them – and that was wrong – and so I was able to remind them of the change. One way of preventing misunderstanding is to just keep somebody talking.
1 Can you explain why Karen does not like to ask direct questions such as ‘What did I just tell you?’ or ‘When am I coming next then?’
2 Can you think of some reasons why people might nod and smile as if they understand, even if they don’t understand what you have tried to communicate?
3 In the example above, how is Karen using the communication cycle?
24
BTEC’s own resources
If you can support people just by the way you are ‘present with them’ this may be because you are developing empathy with them.
EmpathyEmpathy involves a caring attitude where someone can see beyond his or her own assumptions about the world and can imagine the thoughts and feelings of someone else. A professional care worker who can empathise will be able to imagine the emotions associated with the pain and grief that another person is experiencing.
However, in this case, the disability is a social issue (to do with needing an interpreter), rather than a sensory impairment issue.
Barriers associated with personality, self-esteem, anxiety and depressionSometimes care workers can create their own barriers because they feel stressed by the emotional needs of the people they work with. Listening to others can involve hearing about frightening and depressing situations. Carers sometimes stop listening in order to avoid painful emotions. Tiredness, lack of time or a desire to avoid emotional stress can create a barrier to providing caring communication.
Building an understanding of another person and establishing a ‘caring presence’ can be very diffi cult when their personality or self-esteem needs create a barrier. Many people who are depressed or anxious experience negative thoughts that ‘just come to them’. Attempting to understand these thoughts and feelings can feel like trying to fi nd a way through a brick wall. It may feel as if there is an emotional barrier preventing the person from experiencing any positive emotions. The case study on the next page illustrates this type of situation.
The carer in the case study opposite is not ‘just talking’ – she is trying to steer the conversation round to positive memories. The worker is using her understanding of Liam’s past to try and lead the conversation around the barrier of negative and depressed thoughts. If the worker is successful, the conversation might lead to Liam having positive thoughts and feelings and increasing his level of self-esteem.
Asking questions
Talking through diffi cult, complex or sensitive issues will involve the verbal skills of asking open questions and using probes and prompts within the conversation.
Key termsEmpathy – The ability to develop a deep level of understanding of another person’s experience.
Communication disability – Difference that may create barriers between people with different systems of communication.
Sensory impairment – Damage to sense organs such as eyes and ears.
Did you know?Empathy is often regarded as a skill that can be developed through training but Carl Rogers, a famous counsellor, argued that empathy was a state of being. This means that you have to experience your self and other people in a special empathetic way. In Rogers’ view you couldn’t simply use empathy as a communication tool or technique – you had to ‘live’ empathy.
Language needs/preferencesMost people will have a preferred fi rst language. And this preferred language will sometimes be obvious to you. But language needs go beyond the choice of a preferred language. Different communities use a given language in different ways. People use different degrees of formality and informality, depending on the context. For example, people may use jargon, dialect or slang to communicate effectively with people in their own speech community. These differences can create barriers to understanding.
Sensory impairment and disabilityA sensory impairment means that a person’s senses do not work effectively. Impairments create the fi rst kind of communication barrier, where information is not fully received.
Disability is not the same as impairment. Some people experiencing barriers because of their difference may have a communication disability. For example, a ‘Deaf’ person, whose preferred language is BSL, experiences no problems communicating with another person who is good at signing with BSL. This person may not be able to communicate with people who use spoken English without the aid of an interpreter.

25
Unit 1 Developing effective communication in health and social care
• Open questions: These cannot be answered with a yes or no response – they require a person to think about their answer. Open questions are likely to involve a complex communication cycle in order to discuss issues. They include questions such as ‘How would you describe your quality of life?’
• Probes: These are very short questions such as ‘Can you tell me more?’ Probes are used to dig deeper into the person’s answer – they probe or investigate what the other person has just said.
• Prompts: These are short questions, which you offer to the other person in order to prompt them to answer. Prompts are questions such as ‘Would you do it again?’
Barriers associated with aggression and submissivenessWhen a person experiences strong emotions or their self-esteem is threatened, that person may become aggressive or withdrawn, creating barriers to communication.
See pages 30–33 for further information on aggression and submissiveness.
Barriers associated with assumptionsBuilding an understanding of other people’s needs takes time and effort. Jumping to conclusions and making assumptions can save mental effort and time, but assumptions may cause us to misinterpret what another person is trying to communicate. For example, you might believe that you don’t need to listen to a person because you already know what their needs are. But care workers who use the communication cycle are less likely to make assumptions because they check their understanding. Assumptions can create a barrier because people stop listening and checking their understanding of other people’s communication.
Some people make assumptions that people who have a disability are damaged ‘normal’ people. When disabled people are seen in this way, they might be pitied or ignored. People with communication
Key termAssumption – An idea that people think is true or correct without bothering to check.
Case study: LiamLiam: You can’t possibly understand what it feels
like to be me. Absolutely everything is wrong with my life, I’ve got no reason to be alive and you can’t help me – what’s the point of talking?
Carer: But perhaps I could be useful if I knew more about your life?
Liam: What do you want to know? I’ve got no money, no job, no future, no one cares about me – there’s no point in going on.
Carer: Right, so it feels really terrible, really bad, but was there a time before things went wrong – a time when you were happy?
Liam: Yes, a few years back everything was good – but now I feel even more miserable because you are reminding me of how much I’ve lost!
There is no simple way of removing this emotional barrier but some skilled workers might try to keep the conversation going so that they could continue to learn about the person. It might be possible to positively influence the person’s self-esteem as the conversation continues.
Carer: So when you ran your own taxi business you were on top of everything – nothing could get you down?
Liam: Yeah – but I’ve got health problems now, I’m finished, that time is all gone.
Carer: Yes, I know it feels terrible, but tell me about the good times. You dealt with problems then. I’d like to understand how you made it all work back then.
Read the information on probes and prompts below and answer the following questions.
1 Can you identify how the carer has used questions, probes and prompts in order to keep the conversation going?
2 Can you explain how the carer may have used reflective listening in order to build an understanding of Liam’s situation?
3 Can you explain the importance of building an understanding of another person during a difficult and sensitive interaction?

26
BTEC’s own resources
differences are sometimes assumed to be mentally impaired. Older people are sometimes seen as demented or confused if they do not answer questions quickly, correctly and clearly. If care workers do not bother to check their assumptions about people, these assumptions can turn into prejudices. And a prejudice or pre-judgement can result in discrimination.
Barriers associated with values and belief systemsPeople have different belief systems – about what is important in life and how people should live their lives. Values are the principles that we think of as being important or valuable, in terms of how we live our lives.
Barriers associated with cultural variationCulture refers to the different customs and assumptions that communities of people adopt. Different ethnic and religious groups may have different cultures, but different age, occupational and geographical groups also make different cultural assumptions.
Words and non-verbal communication can be interpreted differently depending on the context and on the culture of the person using them. For example, the word ‘hot’ can have different meanings depending on the context in which it is used and the culture of the person using it. In a formal context, ‘hot’ refers to having a high temperature. But in other speech communities an object might be ‘hot’ if it has been ‘stolen’ or if it is perceived as ‘very desirable’. A hot person might be very good at something, or be someone who is overcome with sexual desire! If communication is interpreted only from a fi xed cultural standpoint, serious misunderstandings can arise. To make sense of spoken and non-verbal language, you need to understand the context of the interaction and the intentions of the person communicating.
Key termsBelief systems – The assumptions we use to make sense of our lives. Our belief systems often include our values.
Values – What we think of as being important or valuable in terms of how we live our lives.
Fig 1.14: Why does learning about other people’s beliefs help to avoid barriers to communication?
When people have different belief systems and values it is easy for them to misinterpret one another’s intentions when attempting to communicate. Like assumptions, belief systems and values can therefore create barriers to understanding. It is important to try to learn about other people’s beliefs and values in order to make sense of what they are trying to communicate.
Refl ectThink of some words that can mean different things depending on the cultural context in which they are used. ‘Chilling’ is one example.

27
Unit 1 Developing effective communication in health and social care
An example of a non-verbal cultural variation might be the hand gesture in which the palm is held up and facing forward. In Britain this means ‘Stop, don’t do that’, whereas in Greece it can mean ‘You are dirt’ and is considered a very offensive gesture. Why do the same physical movements have different meanings? One explanation could be that the British version of the palm-and-fingers gesture means, ‘I arrest you, you must not do it’, whereas the Greek interpretation goes back to medieval times when criminals had dirt rubbed in their faces to show how much people despised them.
It is important not to make assumptions about non-verbal messages – they should always be checked. Non-verbal messages can mean different things depending on the circumstances of the people who are sending them.
If you cannot control and make decisions about your own life you may fail to develop, or you might lose your sense of being a worthwhile person. If care workers control and manipulate you, your self-esteem may be damaged.
Care workers should seek to empower people who use services. Empowerment means giving power to others. People who use services should be empowered to believe that they can make their own choices and take control of their lives.
Case study: GerardGerard is a tall, muscular, middle-aged man who regularly talks to staff about his son’s care. He prefers to stand squarely face-to-face and speaks quickly, using a loud voice. Staff say that they feel uncomfortable talking to Gerard because he sometimes ‘stares at you’ with a fixed gaze. Staff say ‘He is in your face’ because they feel that he stands too close to them. Some staff think that Gerard is aggressive and demanding because of the way he acts.
1 Can you identify how ‘cultural variation’ might be important when trying to understand this situation?
2 Can you think of possibilities, other than being demanding and aggressive, that might explain the non-verbal behaviours described above?
3 How could you check what certain non-verbal behaviours might mean during a conversation?
Use and abuse of powerThe General Social Care Council (GSCC) Code of Practice for Social Care Workers (2002) requires all workers to respect individuality and support people who use services to control their own lives. However, there is always a danger that, if a care worker is short of time, they will seek to control people who use services. It is an abuse of power if care workers deliberately control and manipulate others.
Key termsEmpowerment – This enables a person who uses services to make choices and take control of their own life.
Power – In the context of interpersonal behaviour, ‘power’ means the ability to influence and control what other people do.
In order to empower others, care workers need to understand and value each person’s unique story. Care workers must support the people they work with, in taking control of important decisions. Care workers must also carry out their work on the basis that everyone is of equal status. The care worker does not have higher status than people who use services.
Fixed eye contact
Difference in height
Inappropriate use of touch
Worker ignores feedback
Fig 1.15: How do these non-verbal messages express power and domination?

28
BTEC’s own resources
Barriers associated with the eff ects of alcohol/drugsAlcohol and drugs can infl uence a person’s ability to send clear verbal and non-verbal messages. Drugs that affect the functioning of the central nervous system can easily result in messages not being received or
understood and also in distorted interpretations of the message. Alcohol and drug abuse can therefore create all the barriers to communication shown in Figure 1.16 on page 29. People with a distorted perception of other people’s communication may be more likely to become frustrated or aggressive.
Assessment activity 1.3
Again, use the examples used in the previous assessment activities to explain the factors that infl uence communication and interpersonal interactions.
P3
Case study: KarenInterviewer: Why do a lot of people worry about having care services?
Karen: Some people are afraid that you will come in and take control of their lives, boss them about, and make them feel stupid.
Interviewer: But care work is all about giving power to people who use services, making sure people are in control of their own lives – so why do people worry?
Karen: Well, I am always short of time and it is tempting to just take over and do everything my way to get it done quickly. It’s easy to think you know best – but if you make that assumption, you upset people and make them feel powerless.
Interviewer: Don’t some people like to sit back and let you be in control?
Karen: Some people say, ‘You do what you like, buy me whatever you think I need – I don’t care.’ But that is a problem too. Sometimes people lose control of their lives and give up – they become ‘helpless’. They want you to make all the decisions – have all the power. I still try to encourage them to make choices.
Interviewer: There is so much to think about when you are working with people. How do you manage?
Karen: You have to have the right attitude – it’s a sort of feeling. If you’ve got the right attitude you tend to say and do the right things anyway. I enjoy
meeting people and getting to know them. I value everyone I work with; I think of them as important. I am interested in their lives and I listen to what they tell me. I think values – what you believe in – are at the heart of how you work with people.
Interviewer: So do you really need theories like refl ective listening and the communication cycle to be a good carer?
Karen: These ideas can help you to be more sensitive and to understand what might be going on. But care work is really about values, attitudes and feelings. Technical knowledge on its own, without the right values, isn't enough if you want to enjoy caring for others and if they are going to enjoy working with you.
1 Why should care workers not aim to control the lives of the people they work with?
2 Why does Karen try to encourage people to make choices, even if they appear not to want to?
3 Can you explain what is meant by power in the context of interpersonal behaviour?
4 Can you identify what values Karen uses when she talks to people who use care services?
5 What does Karen mean when she says ‘If you’ve got the right attitude then you tend to say and do the right things anyway’?
6 Explain why Karen thinks technical knowledge, without the right values, isn’t enough?
Grading tipP3 Integrate the evidence for this task with that for assessment
Activities 1.1 and 1.2.
Consider both positive and negative infl uences.Consider one-to-one and group interactions, different forms of communication and different types of interpersonal interaction.

29
Unit 1 Developing effective communication in health and social care
3 Understand ways to overcome barriers in a health and social care environment
3.1 Communication and interpersonal interactionStaff trainingMany skills, such as communicating effectively with anxious, depressed or aggressive people, cannot be developed simply by obtaining information. Instead, people often develop their skills by reflecting on their own practice experience and discussing thoughts and experiences with colleagues. Formal training courses usually provide opportunities to practise important skills as well as theories about how to overcome communication barriers.
Assessment of need and using preferred methods of communicationIt is important to build an understanding of the needs of people you work with in health and social care. Very often, people will make their preferred method of communication obvious. Sometimes a professional social work or medical assessment may be needed in order to clarify the person’s needs and their preferred method of communication.
Promoting rightsAs well as general human rights, people who use services have a range of rights that are established in
national standards, codes of practice and legislation. People who use services may be seen as having the following rights.
Confidentiality
Confidentiality is an important right for all people who use services because:
• People may feel confident about sharing information if they know that their care worker won’t pass things on. They may not trust a carer if the carer does not keep information to themselves.
• Keeping information confidential demonstrates respect for people who use services. A lack of confidentiality may threaten people’s self-esteem.
• A professional service, which maintains respect for individuals, must keep private information confidential – in the same way that medical practitioners and lawyers have always maintained confidentiality.
• There are legal requirements (data protection) to keep personal records confidential.
• A person’s safety may be put at risk if details of their property and habits are shared publicly. For example, if your home was empty and other people knew where you kept your money, someone might be tempted to break in.
Fig 1.16: What are the rights of people who use services?
A service user’s rights
To be treated as an individual
To be respected
To be protected from danger or harm
To be treatedin a digni�ed way
To be given privacy
To be cared for in a way that meets their
needs and takes account of choices
To be allowed access to information about
themselves
To be treated equally and not discriminated
against
To be able tocommunicate using their
preferred method

30
BTEC’s own resources
AssertivenessFear and aggression are two basic emotions that we all experience. When we feel stressed, it is easy to give in to our basic emotions and be either submissive or aggressive. Assertion is an advanced skill, which involves controlling the basic emotions that usually prompt you to run away or fi ght. It involves a mental attitude whereby you try to negotiate, and try to solve problems rather than give in to emotional impulses.
During an argument, an aggressive person might insist that they are right and other people are wrong. They will want to win, while others lose. The opposite of aggression is submission. A submissive person accepts that they will lose, get told off, or be put down emotionally. Assertive behaviour is different from both these responses. In an argument, an assertive person will try to fi nd an answer that means no one has to lose or be ‘put down’. Assertion is a skill that helps create ‘win-win’ situations.
To be assertive, a person usually has to:
• understand the situation they are in (including facts, details and other people’s perceptions)
• be able to control personal emotions and stay calm
• be able to act assertively, using the right non-verbal behaviour
• be able to communicate assertively, using the right words and statements.
Some of the emotions, attitudes and behaviours involved in assertion are summarised in Table 1.3 on page 31.
Staying calm and in control of your emotions, displaying respect for others, using refl ective listening and building an understanding of another person’s viewpoint are all part of being assertive. Assertion is the skill of being able to understand another person’s viewpoint, while being able to help them to understand your viewpoint. Assertion skills create a situation where negotiation is possible.
Assertion does involve a special kind of attitude. You are going to stick up for yourself – but you are not trying to dominate or get power over other people. You are trying to reach the best outcome for everyone. It is very easy to be aggressive – it is in our ‘animal nature’ to attack people who cause us problems.
Key termAssertion – Assertion is different from both submission and aggression. It involves being able to negotiate a solution to a problem.
Case study: Justin and TylerThe manager of a care centre has asked that either Justin or Tyler should stay for an extra half-hour at the end of their shift to complete some paper work. Neither Justin nor Tyler want to do this work, so Justin could argue, using:
Aggression: Don’t think I’m going to do it. I need to get away early and you’re not going to stand in my way. I don’t care what you say – either you do it or nobody does.
Assertion: Look – neither of us wants to stay late, but one of us has to stay. Let’s work out a fair way to decide which of us stays.
Submission: I didn’t really want to stay late, but if you don’t want to stay, then I suppose I’ll have to.
1 With a submissive response, Tyler will get what he wants and Justin will lose. But what are the likely consequences for their ability to work together in the future?
2 Justin will not necessarily win using aggression. Both people could become trapped in a cycle of aggressive responses. If one person does force the other to give in, will they be able to trust each other later?
3 Assertion is the most skilful response. Can you identify the skills that Justin would need in order to make this approach work?

31
Unit 1 Developing effective communication in health and social care
Table 1.3: Differences between aggressive, assertive and submissive behaviours
Aggressive behaviour Assertive behaviour Submissive behaviour
Main emotions Anger Control of own behaviour Fear – wanting to please
Attitudes Trying to winWanting your own wayMaking demands
Trying to create a situation in which everyone winsNegotiating with othersTrying to solve problems
Accepting that you will lose Letting others dominate Agreeing with others
Behaviours Not listening to other peoplePutting other people downShouting or talking very loudly
Listening to other points of viewShowing respect for othersKeeping a clear, calm voice
Not putting your own views acrossWithdrawing or showing fearSpeaking quietly or not speaking at all
Body language Fixed eye contact, tense muscles, waving of hands and arms, looking angry
Varied eye contact, relaxed face muscles, looking ‘in control’, keeping hands and arms at your side
Looking down, not looking at others, looking frightened, tense muscles
Case study: KarenInterviewer: You must have to deal with some rude and aggressive people?
Karen: Yes, the first thing I do is to think to myself ‘stay calm – don’t feel threatened’. Very often people are rude or aggressive because they feel threatened. They are upset that you are in
their home – they want to control you, to make themselves feel safe. For many people the only way they know to defend themselves is to get angry. Thinking this way helps me to stay calm.
Interviewer: That’s a wonderful attitude – but don’t people take advantage of you if you think like that?
Karen: No, you have to have the right attitude, you have to be patient, stay calm and try to get
people to talk to you. You have to show that you’re not going to try and dominate or threaten them. But you can’t let yourself be pushed around either. When people cross the line, I will talk firmly about how they make me feel, and what the consequences might be for them. Services can be withdrawn from really offensive people. Usually I think you get respect if you can put yourself in other people’s shoes, but if you also stick up for yourself.
1 Do you think Karen has good assertiveness skills?
2 If Karen did behave aggressively towards people who use services, what would be the risks for her and the people she works with?
3 Why does Karen believe it is important to ‘put herself in other people’s shoes’?
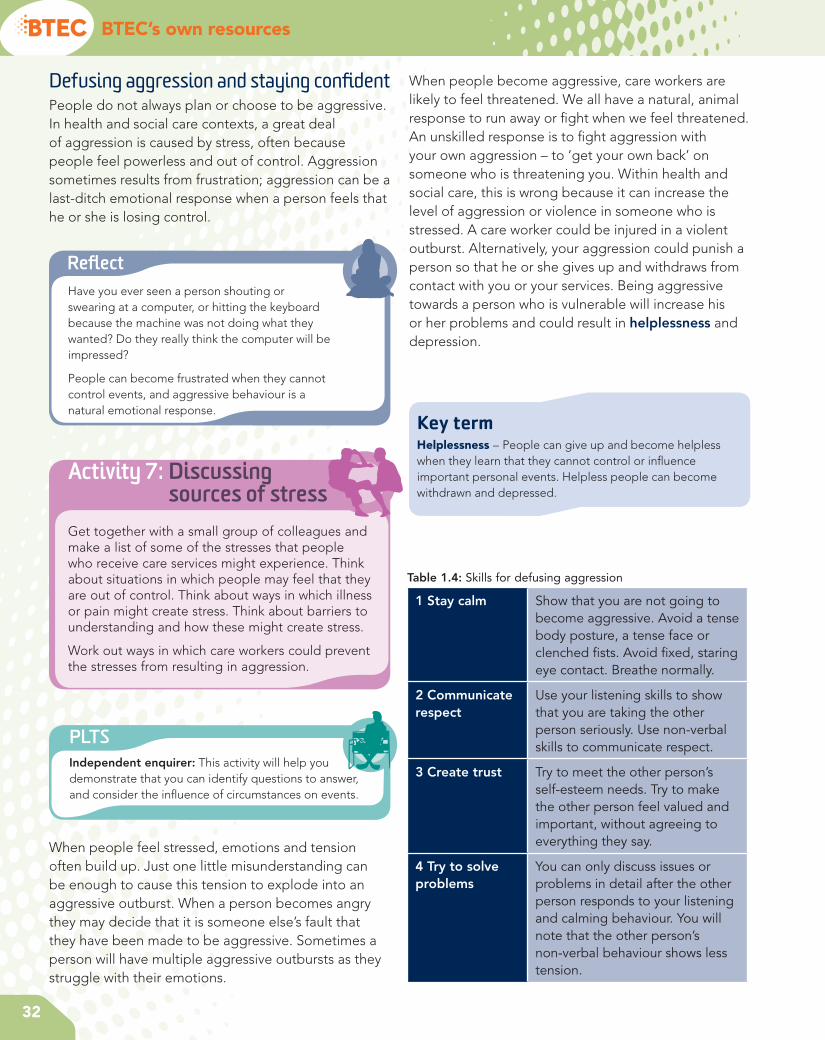
32
BTEC’s own resources
Defusing aggression and staying confi dentPeople do not always plan or choose to be aggressive. In health and social care contexts, a great deal of aggression is caused by stress, often because people feel powerless and out of control. Aggression sometimes results from frustration; aggression can be a last-ditch emotional response when a person feels that he or she is losing control.
When people become aggressive, care workers are likely to feel threatened. We all have a natural, animal response to run away or fi ght when we feel threatened. An unskilled response is to fi ght aggression with your own aggression – to ‘get your own back’ on someone who is threatening you. Within health and social care, this is wrong because it can increase the level of aggression or violence in someone who is stressed. A care worker could be injured in a violent outburst. Alternatively, your aggression could punish a person so that he or she gives up and withdraws from contact with you or your services. Being aggressive towards a person who is vulnerable will increase his or her problems and could result in helplessness and depression.
Refl ectHave you ever seen a person shouting or swearing at a computer, or hitting the keyboard because the machine was not doing what they wanted? Do they really think the computer will be impressed?
People can become frustrated when they cannot control events, and aggressive behaviour is a natural emotional response.
PLTSIndependent enquirer: This activity will help you demonstrate that you can identify questions to answer, and consider the infl uence of circumstances on events.
When people feel stressed, emotions and tension often build up. Just one little misunderstanding can be enough to cause this tension to explode into an aggressive outburst. When a person becomes angry they may decide that it is someone else’s fault that they have been made to be aggressive. Sometimes a person will have multiple aggressive outbursts as they struggle with their emotions.
Key termHelplessness – People can give up and become helpless when they learn that they cannot control or infl uence important personal events. Helpless people can become withdrawn and depressed.
Table 1.4: Skills for defusing aggression
1 Stay calm Show that you are not going to become aggressive. Avoid a tense body posture, a tense face or clenched fi sts. Avoid fi xed, staring eye contact. Breathe normally.
2 Communicate respect
Use your listening skills to show that you are taking the other person seriously. Use non-verbal skills to communicate respect.
3 Create trust Try to meet the other person’s self-esteem needs. Try to make the other person feel valued and important, without agreeing to everything they say.
4 Try to solve problems
You can only discuss issues or problems in detail after the other person responds to your listening and calming behaviour. You will note that the other person’s non-verbal behaviour shows less tension.
Activity 7: Discussing sources of stress
Get together with a small group of colleagues and make a list of some of the stresses that people who receive care services might experience. Think about situations in which people may feel that they are out of control. Think about ways in which illness or pain might create stress. Think about barriers to understanding and how these might create stress.
Work out ways in which care workers could prevent the stresses from resulting in aggression.
33
Unit 1 Developing effective communication in health and social care
Care workers are likely to break professional codes of conduct if they allow themselves to become aggressive. Instead it is vital that care workers learn the skills needed to defuse aggression.
It is not easy to stay calm if someone is threatening you. You will need to feel confident that you know how to work with the other person. If you have already established a sense of trust, it may be easier to cope with their aggression than with aggressive behaviour from a stranger. You will need to be sensitive about possible misunderstandings and barriers to understanding when you start to work with an angry person. You must avoid any spark that could light the fuse leading to an angry explosion.
All the skills of recognising and overcoming barriers to communication will be useful in helping you to avoid triggering aggression. Reflective listening skills are vital in order to make the other person feel valued.
Building relationships and appropriate verbal and non-verbal communicationBuilding relationships with people who use care services involves skilled listening, together with appropriate verbal and non-verbal communication. It may be important to use warm, friendly non-verbal behaviour that expresses interest in another person such as:
• making effective eye contact (varied and appropriate contact with another person’s eyes)
• adopting a relaxed and calm body posture
• smiling – looking friendly rather than ‘cold’ or frozen in expression
• using hand movements and gestures that show interest
• nodding your head slightly while talking to communicate messages such as ‘I see,’ or ‘I understand,’ or ‘I agree’
• using an appropriate gentle tone of voice.
Case study: Bill and TonyBill is a resident in a care home, who has been diagnosed with dementia. Tony is a care worker who knows Bill well. Bill will sit for long periods of time and then become agitated. While sitting in his chair he has started to shout angrily at other residents.
Bill (very angry): You lot can get out of here, I don’t want you round here anymore.
Tony (calm and gentle tone of voice): Hello Bill, I am going to bring some coffee around in a minute. Would you like a cup?
Bill (raising his fist): You can get out of here too. Go on, get off or I’ll have you!
Tony (stepping back and lowering his head in a non-threatening way): Bill, you remember me. You told me about your time in the Merchant Navy back in the fifties.
Bill (still angry): Don’t remember you – you weren’t there!
Tony (calm, gentle, serious): No – but you told me all about your time on the Sea Princess. How you went to South America, how you met your first wife.
Bill (less angry but accusing tone): How do you know all that about me? Have you been spying on me?
Tony (serious, sincere but calm): No Bill, honest, I would never spy on you. We had a long talk yesterday and I really enjoyed hearing about all the things you used to get up to. I was really interested – you’ve lived an exciting life. I was wondering whether you might have time to tell me a few more stories?
Bill (calmer tone of voice): Well, what about all these people in here?
Tony (expressing genuine interest): We could leave them for the moment – tell me more about your time in South America.
Bill (calm): Not sure I can remember, what were we talking about?
1 What might have happened if Tony had confronted Bill and told him to stop shouting at the other residents?
2 Can you explain how Tony showed respect and created trust?
3 Why did Tony avoid talking about the other residents?
4 How did Tony use his personal knowledge of Bill to help defuse aggression?

34
BTEC’s own resources
Appropriate environmentThe following ideas can help to reduce communication barriers in the environment:
• Improve the lighting.
• Reduce any noise.
• Move to a quieter or better-lit room.
• Work with smaller groups to see and hear more easily.
• Organise any seating so that people can see and hear each other.
Meeting self-esteem needs and maintaining an appropriate attitudePeople who use services are often vulnerable. Many vulnerable people do not have the emotional security that comes from a high level of self-esteem. If a person feels dominated or threatened he or she may develop low self-esteem. If children don’t feel valued, they may not develop self-esteem. Adults who do not feel valued may have diffi culty in maintaining a high level of self-esteem.
Your communication with people in care settings should involve understanding and responding to their emotional needs.
Key termSelf-esteem – This is how you value or feel about yourself.
Table 1.5: Aspects of communication that increase self-esteem
Appropriate non-verbal behaviour
• Smiling• Relaxed body posture• Looking interested• Being calm
Appropriate communication
• Using correct level of formality
• Using language appropriate to speech community
• Using appropriate preferred language
• Using technological aids
Listening skills • Using refl ective listening• Having an appropriate
attitude and valuing other people
• Being willing to build an understanding of another person’s views
Case study: KarenInterviewer: You talk about having the right attitude and ‘putting yourself in other people’s shoes’ but doesn’t that often make you feel sad and depressed?
Karen: No, you can understand how someone might feel without becoming overwhelmed. I always try to
leave feeling happy or at least a little bit happier than when I arrived.
Interviewer: So how do you do that?
Karen: Well, keep people talking – most people have some happy memories. I try to get them to talk about some of the good things. I try to get a positive feeling going. Sometimes, if it feels right, I mention happy things in my life or else talk about
about some of the good things in the news – soaps and things like that! I try to create a happy atmosphere because that can sometimes make a person feel included and valued and increase their self-esteem.
Interviewer: So just talking through positive things in your life might make life seem more worthwhile – you value yourself more.
Karen: Yes, thinking over the good things is often a way to increase self-esteem.
1 What is self-esteem?
2 Why would talking about positive past life experiences help some people to increase their self-esteem?
3 How is Karen likely to know if she has been successful in making an individual feel happier after working with them?
35
Unit 1 Developing effective communication in health and social care
Whether you work with children, older people or people with health needs, or physical or learning disabilities, it is always possible to think of ways to help increase another person’s self-esteem.
3.2 Aids to communicationHuman aidsThere are several services that may assist people to communicate or help to remove the barriers to effective communication.
Advocates
Sometimes, when people have a very serious learning disability or illness (such as dementia) it is not possible to communicate with them. In such situations, care services will often employ an advocate. An advocate is someone who speaks for someone else. A lawyer speaking for a ‘client’ in a courtroom is working as an advocate for that person. In care work, a volunteer might try to get to know someone who has dementia or a learning disability. The volunteer tries to understand and then communicate the person’s needs and wants. Advocates should be independent of the staff team and therefore able to argue for people’s rights without being influenced by what is the easiest or cheapest thing to do.
Key termAdvocate – Someone who speaks for someone else.
Advocacy is not straightforward; volunteers may not always understand the feelings and needs of the people for whom they are advocating. Some people argue that it would be better if people who use services could be trained and supported to argue their own case. Helping people to argue their own case is called self-advocacy.
Interpreters, translators and signers
Interpreters are people who communicate meaning from one language to another. This includes interpreting between spoken and signed languages such as English and British Sign Language. When an interpreter works with people, they become part of a communication cycle with that person.
Translators are people who change recorded material from one language to another. Translating and interpreting involve communicating meaning between different languages. Translating and interpreting are not just technical acts of changing the words from one system to another. Many languages do not have simple equivalence between words. Interpreters and
Case study: KarenInterviewer: You talked about creating ‘positive feelings’ – is there any more to this, other than just talking about positive past experiences?
Karen: Well, sometimes it’s little things that make people feel good. First, you have to make the
right relationship. I think it’s important to be cheerful. I always think this is ‘their time’. I have to be cheerful for them – and very often when I come out from a visit being cheerful with that person has made me feel better too. Then I always try to remember the little details from a previous visit. I think people often feel valued if you remember things about them. It always helps to give people a choice about how they want work done, what products they want and so on. I think people need to feel in control of their lives in order to maintain a sense of self-esteem. Then I think it’s important to listen to people. If people listen to you then you matter, don’t you? If people cut you short – well, then, perhaps you’re not worth much.
1 What verbal and non-verbal behaviours might help to create a cheerful atmosphere?
2 Why does choice have anything to do with self-esteem?
3 Why is listening to people linked to self-esteem?

36
BTEC’s own resources
translators have to grasp the meaning of a message (decode the message) and fi nd a way of expressing it in a different language system. This is rarely easy, even for professional translators.
Interpreters may be professional people who are employed by social services or health authorities in order to communicate with people who use different spoken or signed languages. They may also be friends or family members who have suffi cient language ability to be able to explain messages in different circumstances.
When people do not use English as their fi rst language, they may experience diffi culty accessing health or care services, unless they are supported by translators and interpreters. People who use signed languages may also need assistance from interpreters and translators – see page 14 for further details of signed languages.
Mentors
Mentors are usually people who are highly experienced in a particular job or activity; they advise others who are new to the activity or less experienced. Mentors need effective communication skills, coupled with some ability to explain issues and provide guidance. If a person is referred to as a mentor, it might be assumed that they will provide guidance based on their experience and knowledge of an issue.
Functional skillsICT: This activity may help you demonstrate ICT skills associated with presenting information and English: skills associated with reading and understanding text.
Table 1.6: Important issues in interpretation
Knowledge of the subject matter
A professional interpreter may be able to explain details of legislation or procedures for claiming benefi t because they understand the issues. If a relative or friend is acting as an interpreter, they will have to make sense of the technical details before they can communicate clearly.
Trust People must have confi dence in their interpreter. Some people may fi nd it hard to trust a member from a different community. Many women may not feel safe and confi dent discussing personal issues using a male interpreter. The issue may not be about the interpreter’s language competence, but about the interpreter’s ability to understand and correctly convey what a person wants to say.
Social and cultural values
The choice of an interpreter must support the self-esteem needs of people who need to access interpretation services. Many people may feel that it is inappropriate to discuss personal details using an interpreter of the opposite sex. Some Deaf people do not feel confi dent using interpreters who have not experienced deafness themselves.
Confi dentiality Confi dentiality is a right. Professional interpreters are likely to offer guarantees of confi dentiality. Using a relative or volunteer may not necessarily provide people with the same guarantee of confi dentiality.
Appropriate attitude A professional interpreter is likely to offer advanced interpersonal skills, which include the ability not to judge what is being said. Volunteers, relatives and friends may have language competence, but these people may not be able to interpret without involving their own values, attitudes and beliefs.
Activity 8: Exploring ICT translationsUse an automatic language translation system to translate a website that is written in a language other than English. You may fi nd examples of confusing or even funny mistakes that the system makes. Compare your results with your colleagues’ research and discuss the problems that can arise when words are simply changed to another language without any input from a human translator.

37
Unit 1 Developing effective communication in health and social care
Befrienders
Befrienders seek to create a supportive relationship with others. A befriender will have good communication skills that enable them to listen to, and build an understanding of, another person’s views and feelings. A befriender will work ‘as if’ he or she was a friend. Befrienders will not be assumed to have any particular professional knowledge.
Technological aidsHearing aids
Hearing aids are battery-powered electronic devices with small microphones to pick up and increase the volume of sound received by a person. Hearing aids will often amplify background sounds as well as the voice or other signal that the person wants to hear. For this reason, a hearing aid will not always work effectively in a noisy environment.
Text phones, relay systems and minicoms
Text phones and minicoms have a small screen and a keyboard to enable messages to be typed. The reply can then be seen on the screen. The Royal National Institute for Deaf People (RNID) operates a text relay service, whereby an operator can enable conversations between speech phones used by hearing people and text phones used by people who may be Deaf or hard of hearing. A person can text their message to the operator, who will read it to the hearing person. The
What qualities do you think a befriender should have?
operator hears the reply and types what is said so that the Deaf person can read the typed message.
Loop systems
A loop system enables people who use hearing aids to hear sounds more clearly. A cable surrounds a given area such as a public area, room or even a car. Sound from a TV, microphone or music system can then be amplified into the loop. People with appropriate hearing aids can switch their aid to a special setting, enabling them to hear the amplified signal from the loop.
Voice-activated software
Voice-activated software enables a person to use speech commands to get their computer to perform a
Case study: JasuJasu is 10 years old. Her father does not speak English although Jasu has grown up to be multilingual. Jasu’s father is in poor health and needs to explain his problems to a health worker.
If Jasu had to interpret her father’s problems in English:
1 How might she be affected emotionally while explaining her father’s illness to someone she does not know?
2 Would Jasu be likely to find the right terminology to explain complex health issues to a professional?
3 Why might the services of a professional interpreter be more appropriate in this situation?

38
BTEC’s own resources
variety of tasks. Some people use speech recognition software to type messages without using a computer keyboard and this facility is particularly useful for people with dyslexia, who may fi nd it harder to communicate using typing or writing.
Table 1.7: Ideas for reducing barriers to communication where people have a disability
Visual disability
• Use language to describe things.• Assist people to touch things (e.g. they might want to touch your face to recognise you).• Explain details that sighted people might take for granted.• Check what people can see (many registered blind people can see shapes, or tell light from
dark).• Check glasses, other aids and equipment.
Hearing disability
• Don’t shout. Use normal clear speech and make sure your face is visible for people who can lip-read.
• Show pictures or write messages.• Learn to sign (for people who use signed languages).• Ask for help from, or employ, a communicator or interpreter for signed languages.• Check that hearing aids and equipment are working.
Physical and intellectual disabilities
• Increase your knowledge of disabilities.• Use pictures and signs as well as clear, simple speech.• Be calm and patient.• Set up group meetings where people can share interests.• Check that people do not become isolated.• Use advocates – independent people who can spend time building an understanding of the
needs of specifi c individuals to assist with communication work.
PLTSIndependent enquirer: This discussion and thinking activity may help you demonstrate that you can support conclusions, using reasoned arguments and evidence.
Activity 9: Discussing barriers to communicationThink of particular examples of barriers to communication (perhaps taken from the table opposite) and discuss the strengths and weaknesses of different strategies to overcome them. Your discussion activities may help you to work out some reasoned arguments for using particular strategies within your work placement.
Case study: GloriaGloria grew up in the Caribbean and came to the UK 60 years ago. She now lives in a residential care home because she has developed some memory loss and disorientation associated with Alzheimer’s disease. Gloria also has some hearing loss and uses a hearing aid. Gloria’s fi rst language is English but care workers sometimes have diffi culty understanding her speech.
Sometimes Gloria will talk about places and events from the past that care staff have diffi culty identifying with. Some care staff think that Gloria is ‘confused’
and that trying to communicate with her is a waste of time. Gloria sometimes becomes distressed because she is lonely and there is no one to talk to.
1 Can you list the barriers to communication that Gloria is experiencing?
2 Can you list ideas for overcoming these barriers?
3 How could you use communication skills in order to increase Gloria’s self-esteem?

39
Unit 1 Developing effective communication in health and social care
Table 1.8: Strategies for overcoming communication barriers
Type of barrier Possible strategies
Communication that involves difficult, complex or sensitive issues
Use listening skills/skilled use of the communication cycle. Develop a ‘caring presence’. Professional workers may develop empathy.
Unmet language needs or preferences
Assessment of needs. Staff training to enable assessment of need. Use of preferred language. Training to learn to communicate using different languages or systems.
Sensory impairment Use human or technological aids to compensate for impairment.
Disabilities See Table 1.7 on page 38 for strategies.
Communication involving personality or self-esteem needs, or anxiety or depression
Use listening skills/skilled use of the communication cycle. Try to make the other person feel valued. Develop a ‘caring presence’. Use open questions, keep the conversation going. Avoid focusing on/discussing emotionally negative issues.
Aggression/submissiveness Stay calm, show respect. Use skills associated with assertion and defusing aggression (see pages 30–33).
Assumptions, values or beliefs Use listening skills/skilled use of the communication cycle to detect barriers. Use reflective learning skills to question own values, beliefs or assumptions. Staff training to develop reflective learning skills.
Jargon Use listening skills/skilled use of the communication cycle to detect barriers. Use appropriate language for other people.
Cultural variations Use listening skills/skilled use of the communication cycle to detect barriers and check your understanding. Learn about the cultural variations among people you work with. Staff training to learn about cultural variations. Avoid making assumptions about people who are different. Consider involving advocates who will represent the best interests of others.
Abuse of power Try to empower others. Reflect on and question own assumptions. Avoid behaviours aimed at controlling or manipulating other people.
Alcohol or drugs Stay calm, show respect. Use appropriate non-verbal behaviour, avoid making demands. Assess risk of assault.

40
BTEC’s own resources
4 Be able to communicate and interact eff ectively in a health or care environment
4.1 ContextsYou will practise interactions and discuss their effectiveness before you present evidence of your own practical work. To begin with, you might watch videos or fi lm clips of interpersonal interactions. You should practise identifying and describing different behaviours that you have seen and/or heard in recorded material. As you become more confi dent, you can role-play or simulate communicating in various contexts including: formal; one-to-one; group; with people using services; with professionals/colleagues.
This section of the unit is about your own skills in communicating in interpersonal interactions. It is your opportunity to demonstrate your ability to apply what you have learned from the unit.
4.2 Communication skills and eff ectivenessTo begin with, you might demonstrate your communication skills using role-play or simulation. In role-play you have to behave in such a way that other people can – at least temporarily – believe in the character you are portraying. Simulation does not require you to use acting skills or portray a character. If you simulate a conversation, you simply say (or sign) the appropriate responses. You do not expect people observing your behaviour to perceive you as anyone but yourself. Both simulation and role-play involve thinking through appropriate responses but role-play involves a greater level of acting skill.
To demonstrate your communication skills, you will need to cover verbal and non-verbal skills such as listening and responding, tone, pace, language, appropriate environment, proximity, clarifying or repeating, questioning, responding to diffi cult situations and defusing anger.
Assessment activity 1.4
Using examples from class activities, your placement or visits to health and social care environments, explain how barriers to effective communication and interpersonal interaction may be overcome in health and social care. For M2, review these strategies against best practice in communication and interpersonal interactions, particularly in relation to overcoming barriers. For the D1 evaluation, you will need to include judgements about the effectiveness of different strategies for overcoming barriers to communication and support these with suitable explanations using theories of communication and comparisons between different health and social care environments.
Grading tipsP4 Use examples already explained and discussed
in the previous three assessment activities, plus others as appropriate, to explain the strategies used.
Continue to use the notes in your logbook as a source of examples to illustrate points you make.
A strategy is a plan of how things are intended to be done but actual practice may not be the same. Comparison of what is intended and what actually happens could be helpful.
M2 Consider strengths and weaknesses of observed interactions and communication practice and compare these with theories.
In preparation for the assessment, take part in role-plays designed to simulate possible barriers to communication and discuss in class the effectiveness of how they were overcome.
D1 An evaluation requires both a judgement to be made eg whether something is or is not effective in overcoming barriers and a justifi cation or explanation of how this judgement has been reached.
Your evaluations should include references to relevant published sources in addition to your log book evidence or understanding gained from this book.
P4 D1M2

41
Unit 1 Developing effective communication in health and social care
Table 1.9: Checklist for analysing communication and interpersonal interaction
One-to-one interaction • How did you start and finish your interaction? Did you try to meet the person’s emotional needs?
• Could you identify a communication cycle involving feedback on your understanding of the other person’s ideas?
Group interaction • Were you able to take effective turns in speaking?• Could you identify group values and/or purposes within the group?• Was there a group leader? How was the interaction managed?
Context • Who was involved in the interaction? People who use services? Professionals? Colleagues? What role did you play?
Verbal listening and responding skills
• How effective was your use of language, pace of speech and level of formality? Was there any use of specialist language? How far did you encourage others to talk?
Non-verbal listening and responding skills
• How appropriate was your voice tone, posture, facial expression, eye contact and proximity?
Reflective listening skills
• How did you use reflective listening and the communication cycle? Can you identify examples of clarifying your understanding or repeating important ideas?
Questioning skills • Did you keep the conversation going using open questions? Can you identify probes and prompts that you used?
Environment • Did the environment create any barriers? Could everybody see and hear each other clearly?
Barriers • What barriers did you detect? Were there any barriers to interpreting communication, such as language differences?
• Were there any barriers to understanding, such as cultural differences, assumptions values or beliefs?
Difficult situations • Did you act in a calm and respectful way? What skills did you use to interact with people with strong emotions?
Defusing anger • Were you able to act in an appropriate, calm and respectful way? Were you able to avoid triggering aggression? Were you able to use assertive skills appropriately?

42
BTEC’s own resources
PLTSSelf-manager: This activity will enable you to demonstrate your ability to organise your own time and resources.
Refl ective learner: This task will enable you to demonstrate
Assessment activity 1.5
For P5 take part in a one-to-one interaction. For P6 take part in an interaction with a small group of individuals in a health and social care environment. At least one of the interactions should be with individuals using services although one could involve a specifi c interaction with a professional in the environment relating to an important aspect of care.
For both interactions produce evidence to demonstrate your role in each interaction. This should include a witness testimony from a professional in the environment who has been present whilst you have carried out the interactions. You should also provide your own account of each interaction.
For M3 you will need to include a detailed description of the skills you used in the interactions and how these related to the context of each interaction and the responses made by the individuals involved. For both interactions, you should explain how and why you applied theory, took account of infl uences on the interactions and minimised or overcame any barriers.
For D2 the account of the interactions should also include an evaluation of each and of the skills you used.
Grading tipsP5 P6 Gain written consent to carry out the
interactions from a suitable professional in the health and social care environment and include this in your assignment.
Both interactions need to be specifi c planned activities for the purpose of the assessment and you should obtain confi rmation from your tutor that the plans are appropriate before carrying out the interactions. It is not possible to achieve these criteria from casual, ongoing day-to-day interactions in a placement. If you
are not in placement, you may need to visit the environment in advance to better understand the context and likely infl uences so you can take these into account when preparing for the interactions. The interaction may be focused on a specifi c activity eg a creative activity or other care task and your preparation would include appropriate planning for this activity as well as the communication skills you will use.
Your contributions to the interactions do not necessarily need to be transcribed but your evidence should consider the skills you used, infl uences and context of the interactions and you should demonstrate respect for the rights and confi dentiality of the individuals involved in all records/notes you do make of the interactions and in your assignment evidence.
M3 To achieve a merit grade, you must refl ect on your own communication and interpersonal skills and provide an analysis, preferably including your strengths and weaknesses within each interaction. This refl ection should cover both one-to-one and group interactions. You could discuss the notes you have made on your one-to-one and group observations with your supervisor or tutor to help you develop the ability to analyse your own interpersonal skills.
D2 At this level, you need to go further and evaluate the quality of your communication and interpersonal skills in one-to-one and group interactions. Your evaluation will involve a more in-depth discussion of the factors that have infl uenced the effectiveness of your own interaction. Emphasise your good points and also those skills which you fi nd diffi cult and need to practise more often.
P2 D2M2P5 M3P6
4.3 Eff ectivenessYou should demonstrate effective communication in both group and one-to-one situations including an awareness of the needs and preferences of others,
interpersonal skills, attitudes, overcoming barriers, adjusting interactions, and your own assertiveness.
The checklist in the table below may be useful as a starting point for assessing role-plays and recordings of real interactions.
the ability to assess yourself and review progress. You may evaluate your experience and learning and communicate what you have learned in different ways.

43
Unit 1 Developing effective communication in health and social care
Resources and further readingArgyle, M. (1972) The Psychology of Interpersonal Behaviour, second ed. Harmondsworth: Pelican
Burnard, P. (1996) Acquiring Interpersonal Skills, second ed. London: Chapman & Hall
Burnard, P., Morrison, P. (1997) Caring and Communicating Basingstoke and London: Macmillan Press Ltd
Engebretson, J. (2003) ‘Caring presence: a case study’ in Communication, Relationships and Care Robb, M., Barrett, S., Komaromy, C., Rogers, A. (eds) London & New York: OU & Routledge
Pinker, S. (1994) The Language Instinct Harmondsworth: Penguin
Tuckman, B. (1965) ‘Development Sequence in Small Groups’, Psychological Bulletin, Vol. 63, No. 6
Useful websitesBraille www.brailleplus.net
British Sign Language www.bda.org.uk
Makaton www.makaton.org
Signs and finger spelling alphabet www.british-sign.co.uk and at www.royaldeaf.org.uk
BTEC’s own resources
Just checking
Assignment tips1 Before you start to make logbook records you might like to state how you will record details of
conversations and other interactions. You could include a statement about how you will respect confi dentiality, respect the rights of others, and show respect for other people. You must also be sure that if you take notes about people who use services your note-taking will not create any misunderstandings or cause any stress to these people.
2 Use video recording of role-plays or simulations to help you identify how theories of communication work before attempting to analyse workplace interactions.
3 A range of potential barriers and misunderstandings can infl uence communication in care settings. Very often there will be a number of issues that are relevant to any particular observation you have noted.
4 Use role-play and simulation followed by discussion to help you develop skills for reviewing and evaluating strategies to overcome barriers.
5 It may be a good idea to record a practice one-to-one and group interaction and discuss your performance with colleagues, supervisors and/or tutors before undertaking the observation that you use for your assignment. If you practise taking notes and discussing the quality of your interaction you may pick up some good ideas that you can incorporate in your fi nal assignment.
6 When you make notes about a one-to-one or group interaction you should make your notes immediately after the conversation or meeting. These notes will help you describe your interactions at a later date. You will not be able to remember everything that you said or did, or that other people did. You should aim to recall some of the key things you said and to remember the responses others made. You should also make notes about some of the non-verbal behaviours you saw in others as well as your own non-verbal behaviour.
1 Why is tone of voice categorised as a non-verbal rather than a verbal issue?2 Is it true that effective, caring, communication can be defi ned as ‘clear, concise transmission of
information between people’?3 What is refl ective listening and why is it important?4 Rachel says, ‘I never let anyone else win an argument with me – I always get my own way!’ Is it
correct to describe Rachel’s attitude as being assertive?5 If you met a person who said, ‘I can’t hear you, I need to put my glasses on’ what sense could you
make of this communication?6 Is it possible for a person who has no knowledge of the English language to be able to sign using
British Sign Language?7 What problems might arise if a relative (with the necessary language skills) acts in place of a
professional translator?
44