bsc thesis computer assisted aphasia therapy - spsc · bsc thesis computer assisted aphasia therapy...
TRANSCRIPT

BSc Thesis
Computer Assisted Aphasia Therapy
conducted at theSignal Processing and Speech Communications Laboratory
Graz University of Technology, Austria
byLina Alexandra Reitz, 1131569
Supervisors:Dipl.-Ing. Dr.techn. Martin Hagmuller
Assessors/Examiners:Dipl.-Ing. Dr.techn. Martin Hagmuller
Graz, January 29, 2015


Abstract
There are different types of aphasia. Its therapy can be supported by computer programs. Theyincrease the intensity of therapy which highly contributes to its success. Supervision of a Speechand Language Therapist/Pathologist (SLT/SLP) is nonetheless still necessary for diagnosing andindividualizing the programs. When it is used supportive to usual therapy, computer assistedtherapy proves effective concerning health condition and costs. A big variety of programs existsthat include a variety of features and exercises for improving the patient’s cognitive abilities.

Statutory Declaration
I declare that I have authored this thesis independently, that I have not used other than thedeclared sources/resources, and that I have explicitly marked all material which has been quotedeither literally or by content from the used sources.
date (signature)


Aphasia Therapy
Contents
1 Language Disorders 91.1 Language and Speech Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91.2 Diagnosis of Aphasia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
1.2.1 Aachener Aphasietest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101.2.2 Western Aphasia Battery . . . . . . . . . . . . . . . . . . . . . . . . . . . 111.2.3 Boston naming test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
1.3 Types of aphasia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 131.3.1 Amnestic aphasia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 131.3.2 Broca Aphasia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 131.3.3 Wernicke Aphasia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141.3.4 Global Aphasia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141.3.5 Other Types of Apahsia . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141.3.6 Typical results in the AAT . . . . . . . . . . . . . . . . . . . . . . . . . . 14
2 Aphasia Therapy 172.1 Methods for Aphasia treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
2.1.1 Therapy by an SLT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172.1.2 Music therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 182.1.3 Tele-therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 182.1.4 Technology-assisted therapy . . . . . . . . . . . . . . . . . . . . . . . . . . 182.1.5 Prognosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
3 Aphasia Therapy 213.1 Literature on Computer assisted Therapy . . . . . . . . . . . . . . . . . . . . . . 21
3.1.1 Setting of the software . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 213.1.2 Effectiveness of the software . . . . . . . . . . . . . . . . . . . . . . . . . . 233.1.3 Mobile applications for aphasia . . . . . . . . . . . . . . . . . . . . . . . . 273.1.4 Advantages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 283.1.5 Problems and their solutions . . . . . . . . . . . . . . . . . . . . . . . . . 28
4 Commercially Available Software 314.1 Commercially available CAT-Software . . . . . . . . . . . . . . . . . . . . . . . . 31
4.1.1 Therapeutic software . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 314.1.2 Supporting software . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
4.2 Final Conclusion and Prospects . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
January 29, 2015 – v –


Aphasia Therapy
1Language Disorders
When a stroke hits, in the majority of cases it causes severe brain damage. Alongside withconstriction of their movement, the patients often also suffer from aphasia. This means notbeing able to speak and/or understand spoken or written language. Especially when the hospitalstay comes to an end, aphasia therapy can profit from computer assisted support. It makes itpossible for patients to practice at home between the sessions with a speech therapist.The intention of this work is to illustrate the different kinds of aphasia, how to diagnose themand therapy methods. Furthermore there will be given an overview over commercially availablesoftware for aphasia treatment.
1.1 Language and Speech Disorders
In Germany approximately 80.000 people suffer from aphasia caused by a stroke per year. Aboutone third of them does not fully recover (AWMFonline, 2012).
At first, it is essential to distinguish between language disorders and speech disorders.
If there is an impairment in processing language, there is a language disorder. This appliesto understanding as well as conveying spoken or written language. Affected patients deal withproblems such as:
Anomia Trouble in finding words
Agrammatism Not being able to compose a grammatically correct sentence
Language comprehension Constricted/lost ability to understand spoken or written language
Pronunciation and articulation Pronunciation problems not caused by motor impairment
Paraphasia and neologisms Substituting letters, syllables or whole words
Illiteracy Lost ability to read and write
Language disorder is caused by a stroke in most cases. Other possible reasons might bedamages of the brain after an accident or a tumor (Mayer, 2014a).There are different types of language disorders, which are distinguished by their severity and
January 29, 2015 – 9 –

1 Language Disorders
their peculiarity. The different types will be described in 1.3.A speech disorder is an impairment of the motor system needed in order to speak. The patienthas lost the ability to fully control the muscles involved in language production (i. e. tongue,lips, ... ). He may face the following problems:
Respiration Reduced control over respiration and therefore reduced length of sentences andsound level
Phonation Paralysis of the vocal folds/the glottis leads to aspirated voice, varying pitch
Resonance vocals are spoken excessively nasally because more air exits through the nose
Articulation loss of coordination of lips, tongue and lower jaw which causes slurred speech(Mayer, 2014b)
There are different classifications of speech disorders, but I exclude them from this thesis asit is not the main matter.Speech disorders may also be caused by a stroke. With that, there often also occurs a hemiplegia,a paralysis of one body-half. This also effects the ability to speak.Language and speech disorders can appear at the same time.
1.2 Diagnosis of Aphasia
The diagnosis of the Aphasia can be done in late acute phase after the stroke. At this point thesymptoms have taken shape in a way they can be diagnosed. The acute phase consists of thetime period four to six weeks after the brain damage.
1.2.1 Aachener Aphasietest
There are different types of Aphasia, depending on the region of the brain that is damaged.They can be distinguished by looking at the different problems the patients face. In order tomake an accurate diagnosis, in the German speaking area, there is the Aachener AphasieTest (AAT) as an instrument. It consists of 6 smaller subtests, that investigate the capabilitiesand problems of the patient in question. On the basis of the result, the Speech and LanguageTherapist (short: SLT) can derive a diagnosis (Mayer, 2014c).The test consists of the following subtests:
• Spontaneous speech: The SLT has a conversation that lasts 10 minutes. He askssomewhat standardized questions about the patients medical condition and environment.In this conversation he examines the following aspects:
◦ General communication behavior
◦ Articulation and prosody
◦ Automatisms
◦ Semantics
◦ Phonematics
◦ Syntax
• Token-Test: The SLT asks the patient to point at a certain geometrical form of a specificcolor and size in order to test understanding and attention. It can be used to distinguishbetween aphasic and non-aphasic impairments.
– 10 – January 29, 2015

1.2 Diagnosis of Aphasia
• Repeating: The SLT names an item which the patient has to repeat. No simultaneousspeaking or multiple tries are allowed. The SLT names a list of 50 items of increasingdifficulty from one-syllable-words to full sentences
• Written language: Testing of:
◦ Reading out loud
◦ Putting together dictated words from cards with letters/words on them
◦ Writing of dictated items
• Naming: Naming of objects, compounds, colors, situations and actions of cards withdrawings on them
• Understanding: The SLT reads out a sentence and the patient has to choose the bestmatching picture out of four
1.2.2 Western Aphasia Battery
Of course there exist more tests that examine patients with speech disorders.Similar to the AAT, there is the Western Aphasia Battery (WAB) in English. It does notonly test the functionality of speech processing but general cognitive abilities. There are eightsubtests that test the different language skills of the patient (Andrew Kortesz, 1982):
• Spontaneous speech: The SLT has a conversation with the patient and asks standard-ized questions about the patients medical condition and environment. In addition, thepatient has to describe a picture. In this conversation the SLT examines the followingaspects:
◦ Information Content
◦ Fluency
◦ Grammatical Competence
◦ Paraphasias
• Auditory verbal comprehension:
◦ Yes/No Questions: The SLT poses 20 Yes/No Questions, the patient may also answergestural or with an eyeblink, if a verbal response is not possible
◦ Auditory word recognition: The patient is asked, to point out certain objects (realobjects, drawn objects, forms, furniture, letters, number, body parts)
◦ Sequential commands: The SLT gives eleven commands of increasing difficulty. Themore difficult the task the more credits can be scored
• Repetition:The SLT names an item which the patient has to repeat. The SLT names alist of 15 items of increasing difficulty from one-syllable-words to full sentences
• Naming:
◦ Object Naming: 20 objetcs are presented that have to be named. Fewer points aregiven when a tactile or phonemic cue is necessary
◦ Word fluency: The patient is asked to name as many animals as possible within oneminute
January 29, 2015 – 11 –

1 Language Disorders
◦ Sentence completion: The patient has to add the missing word to a given sentence
◦ Responsive speech: The patient is asked five questions that can be answered with oneor two words
• Reading:
◦ Reading Comprehension of sentences: The patient reads sentences on cards and hasto find the missing word (four different words are suggested)
◦ Reading commands: The patient reads out loud a command and has to perform itafterwards
◦ Written word stimulus - Object choice matching: The patient has to point at theobject that is written on a card
◦ Written word stimulus - Picture choice matching: The patient is presented two pic-tures and has to point out the one that matches the word
◦ Picture stimulus - Written word choice matching: The patient is presented pictures,he has to choose their names from a list
◦ Spoken words - Written word choice matching: The patient has to point out the wordgiven to him orally on a card with 5 different words on it
◦ Spelled word recognition: The SLT spells a word which the patient has to name
◦ Spelling: Patient has to spell words that are given to him orally
• Writing:
◦ Writing on request: The patient is asked to write down his name and address
◦ Written output: The patient is presented a picture. He has to write a story aboutwhat happens in the picture
◦ Writing to Dictation: The patient has to write down a sentence that is dictated tohim. If necessary it can be given to him in shorter parts
◦ Writing of dictated or visually presented words: The patient is asked to write downdictated words. If he does not succeed, the real object is shown, later on the word isspelled orally
◦ Alphabet and numbers: The patient is asked to write down the alphabet and thenumbers from 0 through 20 (order is not important)
◦ Dictated Letters and Numbers: The patient has to write down dictated letters andnumbers
◦ Copying of words of a sentence: The patient is given a sentence on a card which hehas to copy
• Apraxia: The patient is asked to do a number of actions (Certain movements of the armsand face, using of instruments, pretending everyday actions)
• Constructional, visuospatial and calculation tasks:
◦ Drawing: The patient is given a list of items (circle, square, tree, person, ...) whichhe has to draw freehandedly
◦ Block design: The patient is given a number of equal blocks. Their sides are all red,all white or half red and half white. The patient is now asked to put the blockstogether in a way that a presented pattern is achieved
◦ Calculation: The patient is given an easy calculation (addition, subtraction, multi-plication, division) on a card and orally and then has to choose the correct answerout of four possibilities
– 12 – January 29, 2015

1.3 Types of aphasia
1.2.3 Boston naming test
Furthermore, the Boston Naming Test (BNT) is widely distributed and there are versions ina variety of languages (i. e. English, French, Spanish, Greek, ...). It is not only for diagnosis ofaphasia but also used for people with dementia or children with learning disabilities. Differentfrom the AAT and WAB this test only focuses on word retrieval (Nicholas et al., 1989).The SLT presents the patient 60 cards with pictures, the patient has about 20 s to answer, thenthe next card is presented. If there is more than one name for a picture, the patient may choosethe most common. If the patient gives a wrong answer the SLT can give a phonemic cue. TheSLT writes down the patients answer in a code.
However, there are a few problems with the BNT:
• The results vary from test to test and from examiner to examiner for the same patient
• Not enough acceptance of synonyms
• Existence of pictures that are hard to name, even for healthy patients
1.3 Types of aphasia
There are four main types of Aphasia. They differ in severity and exhibited symptoms. Thedifferences have their cause in the different regions that are affected by the stroke. The typesthemselves occur in different stages of severity.
1.3.1 Amnestic aphasia
The main symptom of the amnestic aphasia is anomia, hence difficulties in word finding. De-pending on the severity there is either a still flowing language or long pauses. The patientsoften succeed in using paraphrases or flowers of speech in order to cover the pauses, yet theirdescriptions miss exactness.Anomia also occurs in writing.Understanding of language is only mildly impaired, if at all.The patient is aware of his word finding difficulties (Mayer, 2014d).
1.3.2 Broca Aphasia
Broca Aphasia manifests in great difficulties in speaking fluent language. It is an endeavorfor the patient to construct full sentences. His vocabulary is limited and the sentences lackprepositions, articles and pronouns. He speaks in telegraphic style.The patient uses phonematic paraphasias, i. e. he changes the sound of a word by changing oradding some parts of it.Understanding of language is only impaired when the given sentence is of a complex syntacticstructure.The same problems occur in understanding or creating written language.The patient is, like in amnestic aphasia, aware of his impairment.Often, there is an additional problem with writing as there sometimes occurs a hemiplegia (aparalysis of one body half) when there is a Broca Aphasia (Mayer, 2014e).
January 29, 2015 – 13 –

1 Language Disorders
1.3.3 Wernicke Aphasia
The Wernicke Aphasia stands in opposition to the Broca Aphasia. The patient suffers fromlogghorea, a excessive flow of words. He uses a lot of phonematic paraphasias and neologisms.Often wrong words with a similar meaning as the intended word are used. This is called semanticparaphasia. The patient often uses flowers of speech and extensive descriptions. The sentencesare long and complex, with some parts doubled and grammatical mistakes.The patient has big difficulties in repeating words given to him.Understanding of spoken and written language is heavily impaired.The patient is mostly not aware of the mistakes he makes (Mayer, 2014f).
1.3.4 Global Aphasia
Global Aphasia is - as the name suggests - the most severe type of aphasia. All aspects ofprocessing language (receptive and expressive language processing) are heavily impaired. Thisalso applies to written language. The patient often only repeats the same words / syllables (socalled recurring utterances) or uses automated figures of speech (Mayer, 2014g).
1.3.5 Other Types of Apahsia
The types of aphasia mentioned before are the main types. There are also two further typesthat are less common:
Transcortical Aphasia
The most noticeable symptom of the transcortical aphasia is echolalia. This is the repeating ofheard words. Other areas of processing language are less damaged. It can be distinguished be-tween transcortical motor aphasia and transcortical sensory aphasia. A patient with transcorticalmotor aphasia has problems with spontaneous speech production but not with comprehension.For transcortical sensory aphasia it is the other way round. If both forms occur at the sametime it is called a transcortical mixed aphasia where speech production and comprehension bothare impaired (Mayer, 2014h).
Conduction Aphasia
Speech production and comprehension are mostly intact, but repeating is impaired. The prob-lems increase when the sentences that should be repeated get longer (Mayer, 2014i).
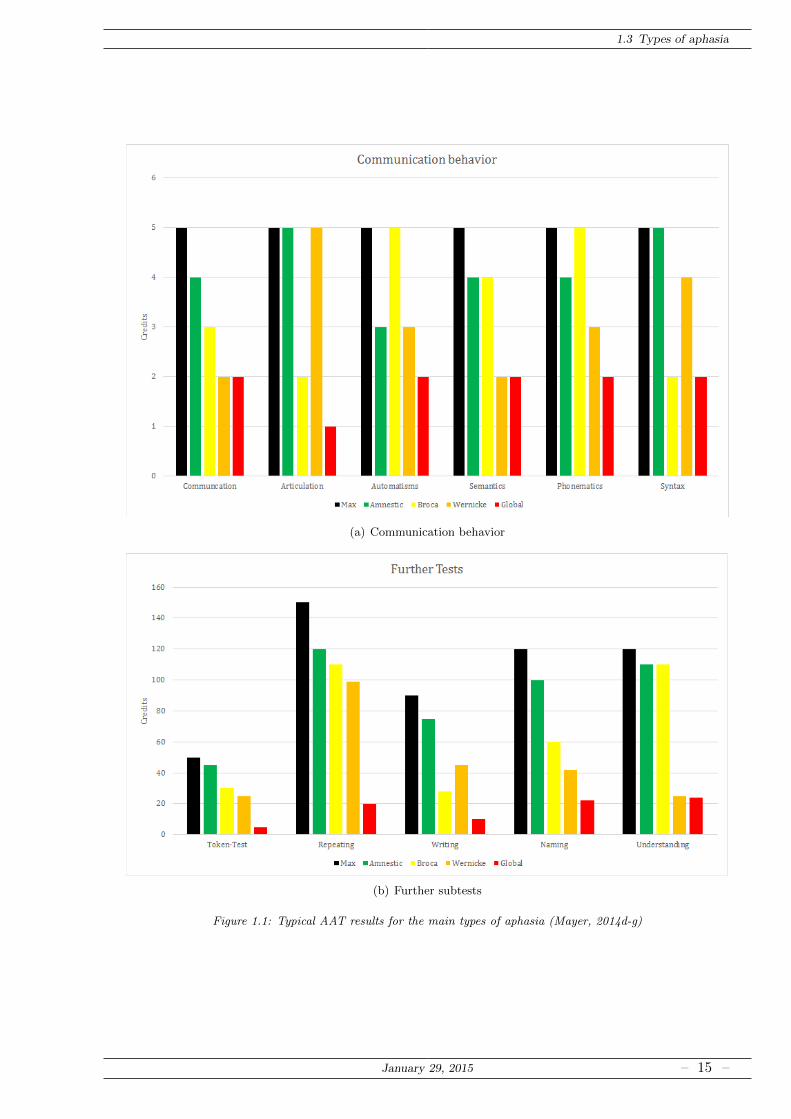
1.3.6 Typical results in the AAT
In the following figures you can see typical results for each of the main types of aphasia in theAachener Aphasie Test in comparison. “Max” shows the highest possible score for each test.(a) shows the results in all categories of the subtest “Communication behavior” in both figures.In (b) the results for the further five subtests are displayed.
Figure 1.1 shows the results of the test for each of the four main aphasia types (Mayer,2014d-g).
Figure 1.2 shows the results of the test for each of the two further aphasia types (Mayer,2014h-i).
– 14 – January 29, 2015
1.3 Types of aphasia
(a) Communication behavior
(b) Further subtests
Figure 1.1: Typical AAT results for the main types of aphasia (Mayer, 2014d-g)
January 29, 2015 – 15 –

1 Language Disorders
(a) Communication behavior
(b) Further subtests
Figure 1.2: Typical AAT results for the further types of aphasia (Mayer, 2014h-i)
– 16 – January 29, 2015

Aphasia Therapy
2Aphasia Therapy
2.1 Methods for Aphasia treatment
The therapy aims at an improvement of the patient’s abilities concerning verbal communicationand taking part in social life. Depending on the diagnosis, an individual recovery plan shouldbe elaborated.Part of the therapy is to re-erect lost communicational abilities and to correct acquired errorssuch as automatisms (DeutscherBundesverbandFurLogopadenE.V., 2013).Requirement for the therapy is the patient’s ability to be treated concerning cognitive and mo-tivational skills.The success of the recovery depends highly on the beginning of the therapy and its intensity.The therapy should begin as early as possible. It should be done daily, with at least five toten hours per week to ensure progress. This should be done for the first 12 months after theincident. After that a more gentle pace can be established.In this late phase the focus is on maintaining the re-erected abilities.
There are three basic categories of treatment:
• Activation of the linguistic center of the brain in order to rebuild lost language skills(especially in the early state)
• Training adapted to specific deficits for a reorganization of the linguistic system. Thisreorganization happens mostly by learning processes
• Maintaining of the achieved progress for successful master everyday-life
These categories are used in every phase of the recovery but with various weighting.
2.1.1 Therapy by an SLT
The main goal of the therapy is to enable the patient to take part in everyday life. Differentmethods can be helpful here.Other means of communication such as use of gestures, drawings or symbols can be established.That is - of course - only possible when the motor system is not damaged too much. Also the useof AAC (alternative and augmented communication) can be established. This is technology that
January 29, 2015 – 17 –

2 Aphasia Therapy
can replace missing linguistic skills. A more precise explanation will be given in the followingchapter.The therapy involves role play games and dialogue training that resemble real life situations, socalled Activities of Daily Living (ADL).It is of utmost importance to include family members in the exercises. The family members alsoshould be informed about how to deal with a patient that suffers from aphasia. They need todevelop a certain degree of awareness of the patient’s problems and take care of using speechthat is easy to understand (Short words and sentences, slow pace) (GAB and DGNKN, 2000).
The therapist should follow a few schemata based on didactic principles (GAB and DGNKN,2000):
• Going step-by-step from preparation to application and repetition
• Choosing the right amount of stimuli (no overstimulation or lack of stimulation) in a waythe patient is challenged overwhelmed
• Taking the patients capabilities into account
• Determining and saving the results
• Alternating between tension and relaxation
2.1.2 Music therapy
Music therapy is mainly a psychotherapeutic approach. It enables the patient to express himselfin non-verbal means of communication. The music therapists have an assortment of instrumentssuch as drums, mallet instruments and keyboard instruments that are easy to play. Having sucha way of expressing themselves, reduces emotional stress as a compensation of accumulatedfrustration is possible.A functional training can also be deducted by rhythmical exercises and singing. The exer-cises can be active (performing music) or passive (listening to music improvised by the thera-pist)(Baumann, 2006).
2.1.3 Tele-therapy
As the means of technology have been getting more and more powerful over the last years,it is only reasonable to include it in medical treatments. In tele-therapy this is applied viavideo-chats that replace face-to-face meetings wit the SLT at the clinic. Many exercises can bedone without physical presence of the therapist. So it is possible to have more sessions that aresupervised (Evocare, 2008).
2.1.4 Technology-assisted therapy
How technology-assisted therapy is conducted in the specific case of aphasia therapy will beelaborated in chapter 3.
2.1.5 Prognosis
After 6 months 44% of the patients that survive fully recover from their aphasia (Pederson,1995).The cause of the aphasia has a great impact on the prognosis. A minor stroke improves the
– 18 – January 29, 2015

2.1 Methods for Aphasia treatment
chances of a full recovery whereas a malignant tumor in the left hemisphere involves a highlethality. The size and location of the lesion as well as age and and health condition of thepatient influence the recovery process. For most patients a recovery - at least to some degree- can be achieved. The chances are better when language comprehension is not or not muchimpaired.For the different aphasia types there are different chances for rehabilitation:Amnestic aphasia and Broca’s aphasia often can be cured completely. Many of those with mildaphasia can recover within one week (Dobkin, 2011).Wernicke’s aphasia can’t be cured as good as Broca’s but there is recovery to some degree.The recovery from global aphasia takes more time. More progress can be made in the timebetween 6 and 12 months poststroke, not in the first half year after the incident.When the patient suffers from an untreatable tumor or neurodegenerative disease his chancesto recover are poor (Howard S Kirshner, 2014).
January 29, 2015 – 19 –


Aphasia Therapy
3Aphasia Therapy
3.1 Literature on Computer assisted Therapy
In the following there is a description of the typical setting of software for computer assistedaphasia therapy (CAT). Its effectiveness regarding health condition and costs will be analyzed onthe basis of different studies conducted to this subject. There also is an overview over differenttypes of software that are not intended for therapy but for support in everyday life of an aphasiapatient. Therapists and patients have to deal with some problems related to the use of therapysoftware. These will be illustrated furthermore.
3.1.1 Setting of the software
There are different elements that can be found in CAT software. There are different types ofexercises that typically are found in the software:
• Matching words/sentences to pictures: There is a picture of an item or an action anda certain number of words. One of these words or sentences matches the picture. Thereis a rising number of words or longer and more complicated sentences with increasingdifficulty.
• Matching pictures to words/sentences: There is a word or sentence given an a certainnumber of pictures. One picture matches the word or sentence.
• Spelling Exercises: An anagram has to be solved, the right spelling has to be chosen ora word has to by typed in.
• Building Sentences: Training of building syntactically correct sentences (cases, wordorder)
• Grammar exercises: Exercises for cases, tenses etc.
• Specific exercises for word classes: Exercises for adjectives, prepositions, articles
Examples on how these exercises can look like can be seen in figure 3.1.
January 29, 2015 – 21 –

3 Aphasia Therapy
(a) Word-picture-matching (b) Sentence-picture-matching
(c) Anagram (d) Sentence building
(e) Exercise for cases (f) Preposition exercise
Figure 3.1: Screenshots from SpeechCare Aphasia for iPad ((a)-(d) and (f)) and Neuroling (e)
– 22 – January 29, 2015

3.1 Literature on Computer assisted Therapy
3.1.2 Effectiveness of the software
Effectiveness considering health condition
Study: Piloting the Effectiveness of a Tablet-Based Home Practice Program inAphasia Treatment (Kurland et al., 2014)This Study explores the effectiveness of therapy effectiveness when using a tablet PC. Theeffectiveness is measured by the patients performing in naming. There are four categories ofwords that are tested. The first two of them were practiced at home. All four of them wereprompted to test the progress.
• TR-PR: Trained to be practiced
• UNTR-PR: Untrained to be practiced
• TR-UNPR: Trained and not practiced
• UNTR-UNPR: Neither trained nor practiced
Figure 3.2: Average Effect of the Training (Kurland et al., 2014)
In figure 3.2 the progress of the patients over time can be seen. It shows their performancein naming for the first days of training (TX1 to TX10), immediately after the training (PostTX1 to Post TX4) and over the following 6 months after the training (Post Month 1 to PostMonth 6). The most interesting word group is the one for UNTR-PR, the trend can be seen inthe figure(dotted line). It clearly shows an upward development.
Figure 3.3 shows the difference of the performance for each patient (performance at the re-spective day minus performance on the first day of practicing) and the performance weighedwith the severity of the aphasia of each patient. The severity is mapped to a scale from 1 to 5where 1 is the least severe and 5 is the most.
January 29, 2015 – 23 –

3 Aphasia Therapy
(a) Performance (b) Performance weighed with severity
Figure 3.3: Performance of the patients (Kurland et al., 2014)
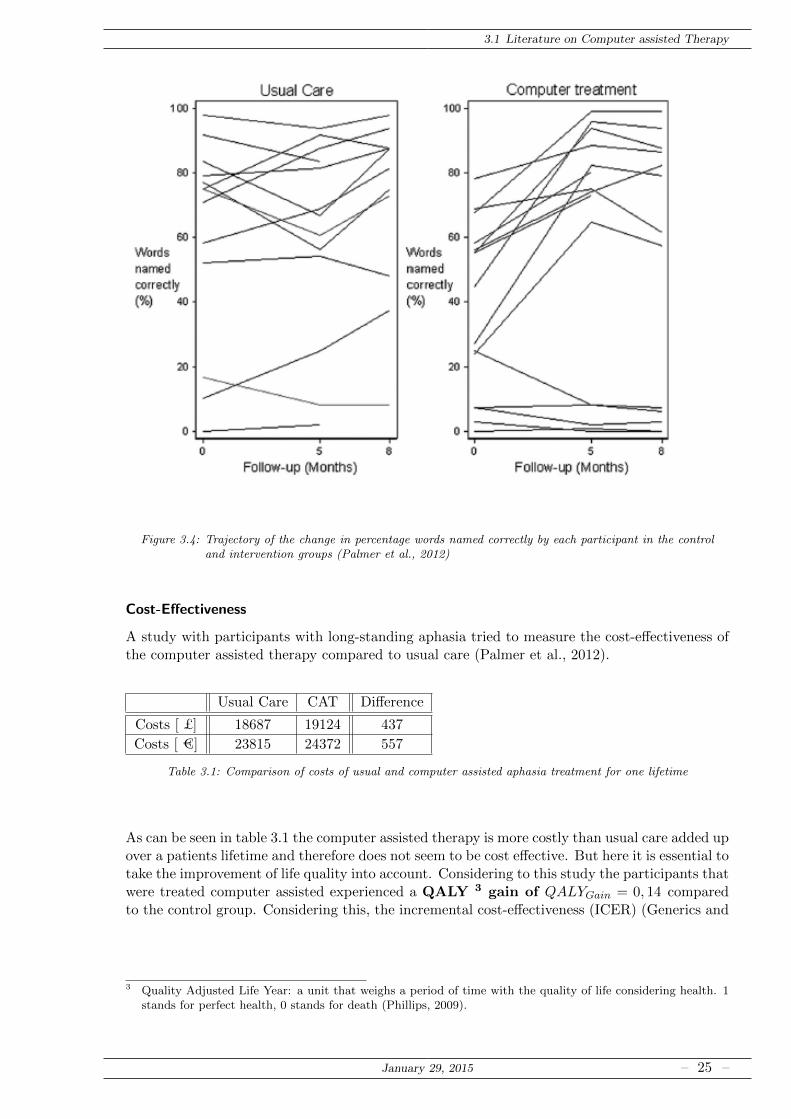
Study: Computer Therapy Compared With Usual Care for People With Long-Standing Aphasia Poststroke (Palmer et al., 2012)This study compared an intervention group of aphasia patients who got computer assisted treat-ment to a control group that got usual treatment. “Although the mean difference in change wasnot statistically significant (at 5%) at 8 months, the percentage change was still greater in theintervention group. [...]Although there is considerable variation in the performance of the control group between baselineand 5 months, the intervention group shows a more consistent trend for improvement betweenbaseline and 5 months. It is clear that this trend is not applicable to participants who wereable to name <10% of words at baseline. Excluding these participants in both groups from theanalysis (intention-totreat), the intervention was associated with 23.1% (95% CI 1, 7.2%–39.0%;P=0.007 2) mean improvement in change in percentage of words named correctly at 5 months”(Palmer et al., 2012).Figure 3.4 shows the naming performance of each patient, the general upward trend in thecomputer treatment group can clearly be seen.
Study: Computer-based script training for aphasia: Emerging themes from post-treatment interviews (Cherney et al., 2011)Patients and/or a significant other person where interviewed about their perception of the com-puter treatment they were given. It was analyzed if there was a perceptible change and whichareas were affected (Figure 3.5 (a)). The numbers show the quantity of patients, that commentedon the subject. It is obvious that most of the patients did perceive a change. The percentage ofthe patients that found a change was evident varies between 85,7% (Improved communicationskills evident in other modalities) and 100% (Changes in ADL and community activities). 87,0%felt their verbal communication skills were altered.Furthermore the number of comments made by the interrogator and the patient concerning theconduction of the study and the used computer program were counted. It can be assumed,that a subject that the patient mentions by himself, he is more engaged with (Figure 3.5 (b)).62,5% of the comments that suggested recommendations were made by patients. The smallestpercentage of comments by patients can be found in the category Computer Program designand use (17,3%).Figure 3.6 shows the distribution of comments to the different subjects.
1 95% Confidence Interval: Interval in which the true value of the parameter is found with a probability of 95%2 P-value: Value that indicates the significance of the studies’ outcome, the smaller the value, the more significant
it is
– 24 – January 29, 2015
3.1 Literature on Computer assisted Therapy
Figure 3.4: Trajectory of the change in percentage words named correctly by each participant in the controland intervention groups (Palmer et al., 2012)
Cost-Effectiveness
A study with participants with long-standing aphasia tried to measure the cost-effectiveness ofthe computer assisted therapy compared to usual care (Palmer et al., 2012).
Usual Care CAT Difference
Costs [ £] 18687 19124 437
Costs [ €] 23815 24372 557
Table 3.1: Comparison of costs of usual and computer assisted aphasia treatment for one lifetime
As can be seen in table 3.1 the computer assisted therapy is more costly than usual care added upover a patients lifetime and therefore does not seem to be cost effective. But here it is essential totake the improvement of life quality into account. Considering to this study the participants thatwere treated computer assisted experienced a QALY 3 gain of QALYGain = 0, 14 comparedto the control group. Considering this, the incremental cost-effectiveness (ICER) (Generics and
3 Quality Adjusted Life Year: a unit that weighs a period of time with the quality of life considering health. 1stands for perfect health, 0 stands for death (Phillips, 2009).
January 29, 2015 – 25 –

3 Aphasia Therapy
(a) Communication
(b) Computer Program and Study Protocol
Figure 3.5: Comments of the patients to different subjects (Cherney et al., 2011)
(a) Communications (b) Computer Program and Study Protocol
Figure 3.6: Comments of the patients to different subjects (Cherney et al., 2011)
– 26 – January 29, 2015

3.1 Literature on Computer assisted Therapy
BiosimilarsInitiative, 2010) can be calculated:
ICERCAT =CostsCAT − CostsusualEffectCAT − Effectusual
=CostsCAT − Costsusual
QALY Gain
= 3058.21 £ (per 1 gained QALY)
The threshold for effectiveness considering QALY is set at
ICERthresh = 20 000 £ (per 1 gained QALY)
Now the values can be compared:
ICERCAT = 3058.21 £ < 20 000 £ = ICERthresh
As the ICER is smaller than the threshold, the computer assisted therapy proves cost effectivecompared to usual therapy.
3.1.3 Mobile applications for aphasia
Therapy software can not only be found on personal computers but also on mobile devices. Thenature of mobile devices is that they are carried around with the owner all day long. This opensthe door for various applications that may help an aphasia patient (Brandenburg et al., 2013).At first there are the impairment-focused practice devices:
• Therapy apps: This kind of app includes numerous features. It provides exercises for thepatient and gives feedback. There are different types of exercises for practicing expressiveand receptive language skills. They also have features that ease the use of the softwarefor an aphasia patient such as spoken output when reading is not possible. The patient’sprogress is analyzed. It replaces the contact to the therapist to some degree. Of coursethe therapy can’t be done completely by the app, but relieves the SLT and improves theexercising intensity which leads to better chances of recovery. Especially in the beginningthe patient should be assisted in the use of the app, e. g. the level of difficulty should bechosen together with the SLT.
• Stimulus representation: As the name suggests this app type gives stimuli such asflashcards. Different from the therapy apps the patient does not get feedback if he is right.It can be used by a patient at home for practicing or by an SLT. It is often handier andmore organized to have the flashcards in this mobile application than to work with a pileof paper cards.
• Behavior tracking: The user can enter behavior concerning his aphasia (e. g. wordfinding problems) into this app to keep track of reoccuring errors, but also of his progress.Usually there are no apps specifically for aphasia patients but there are some for autisticpatients that can easily be accustomed to the aphasic patient’s needs.
• Clinician tools: These tools can be used by the clinician for diagnosis and assessmentof the patient’s data.
• Environmental/Bio-Feedback: Environmental noise or a speakers voice (either thepatient or a healthy person) can be recorded and a real time feedback can be given. Inthat way the patient can gain awareness of is own errors or record healthy speech fortraining purposes.
January 29, 2015 – 27 –

3 Aphasia Therapy
Secondly there are apps that help the patient with communication:
• Educational apps: Dictionaries (with pictures) or similar apps can help the patient withword finding and simplifie the communication
• AAC apps: AAC stands for alternative and augmented communication. It can replacehuman speech when the patient is not able to do so. The patient can type in sentences orchoose from extensive (depending on the app) presets that are read aloud by the app tocope with everyday situations.
3.1.4 Advantages
Using software for aphasia therapy comes with a number of advantages.The patient is able to train at home without supervision of an SLT. This means that it is possibleto practice more often on a regular basis. The efficiency of the therapy is therefore enhanced.This applies mainly to exercises regarding reading, spelling and expressive language. It can bepracticed even more often when the therapy software is installed on a mobile device which thepatient carries with him most of the time.The training at home is also cost efficient when taking the gain of life quality of the patient intoaccount.Especially on mobile devices it is easy to customize to the patients needs, e. g. designing of bigbuttons.
3.1.5 Problems and their solutions
General Problems
A number of barriers exists concerning the use of computer assisted therapy (Brandenburg et al.,2013).
Health condition: Having suffered from a stroke, the patients often suffer not only fromaphasia, but also other impairments which impede the use of a computer or mobile device.The language deficit makes it hard to handle the device, as often reading or writing is necessaryto do so. Being unable to ask questions makes matters worse.Age and motor impairments caused by the stroke make it hard for the user to use a keyboardand a mouse. Also the eyesight of some patients is bad.Patients with a more severe form of aphasia are unable to use the software without assistance.If possible, a volunteer should be there to assist in handling the computer and answer occuringquestions. Mobile devices can also offer help by using a layout that is easier to handle and givingan audio-output when reading is not possible. In general it is beneficial to have big buttons anda big font that is easy to read. Sometimes a special keyboard with big buttons and letters inalphabetic order and a trackball are preferred.
Individual barriers: There is a number of individual factors that influence the usefulnessof the software such as personal motivation to exercise regularly. It quickly falters when theexpectations considering the speed of success aren’t fulfilled.Furthermore the motivation to use technology based therapy methods depends strongly on theexperience the patient has had with technology before suffering of the stroke. Computer illiter-acy is a big barrier, because there is much more that has to be learned additionally. Here it isimportant to ensure software with a handling that is as intuitive as possible.Some patients also lack the necessary cognition abilities to use the software.
– 28 – January 29, 2015

3.1 Literature on Computer assisted Therapy
To most patients it is important to have support by their family. But it occurs that fam-ily members are overstrained when dealing with the patient and don’t always can empathize.When looking for assistance in dealing with the computer it is often wise to choose someone fromoutside of the family with an education that suits the situation (e. g. a volunteer SLT student).Nevertheless, forming a personal bond to that assistant can be quite beneficial (Golashesky,2008).
Nature of technology: As mentioned before, there are physical barriers like small screensand buttons that impair the use of a computer. It is also not beneficial if the computer ormobile device has too many features that make their handling more complicated.The security of private data also concerns some users. Especially because very personal dataabout their health condition are handled. In the consequence passwords and safe communicationcanals in the internet are essential.Finding the right software that fits the personal needs can be troublesome as there’s so muchavailable. Choosing one that benefits the recovery the most and does not solely look for profitscalls for a lot of research.When it comes to mobile devices, on the other hand, the app developers lack awareness of themarket of aphasia patients and the variety of apps than can be targeted at them.If there is no availability of the technology it can’t be used. There has to be a sufficient internetcoverage in the area the patient lives in. And the patient has to be able to afford a device thatruns the software. A support by healthcare services would be useful here.
January 29, 2015 – 29 –

Aphasia Therapy
4Commercially Available Software
4.1 Commercially available CAT-Software
There is a variety of programs on the market. These programs are made for different platformsand have different features. As described in the previous chapter, there are different types ofhelpful software for aphasia. At first there will be a description of the programs designed fortraining. A selection of them will be analyzed regarding available exercises, additional features(for customization etc.) and aphasia-friendly interface. Furthermore it will be looked at howthey deal with the problems mentioned in 3.1.5.The analysis is based on the trial versions of the software (respectively the full version of Re-vivo). I took a look on the software in order to evaluate the accessibility and handling. Byperforming the exercises myself, I can evaluate how intuitive and user friendly the tested soft-ware is. I commented on these attributes in the sectors “Interface” and “Conclusions” for all ofthe analyzed programs.
4.1.1 Therapeutic software
These programs are designed to support the SLT in the training of the patients. They usuallyconsist of different types of exercises.
Sentence Shaper
SentenceShaper is an extensive therapy software. It comes at the price of 199 US$ (status:23.11.2014 according to website, about 160e) It only supports the operating system MicrosoftWindows, its language is English.The system has to meet the following requirements (Sentenceshaper, 2015):
• Windows XP/Vista/7/8
• disk space for the software (460 MB; trial version: 315 MB) and a lot more additionalspace for the audio recordings
• sound card, loudspeakers and microphone
• mouse or trackball
January 29, 2015 – 31 –
4 Commercially Available Software
• screen resolution of at least 1024 x 768 pixels
Main functions:
• Recordings: The user records single words or parts of sentences, so called “snippets”.These can be heard again and put in order to build sentences. These then can be combinedto full stories. When snippets are combined to sentences there are small pauses between thewords, even when the recordings starts and ends at the beginning/the end of the recordedword. It makes a less natural sound but it is possible that the patient can understandbetter at this slower pace.
• Exercises: There are several workbooks with different exercises. Depending on the work-book there are different vocabulary cues that may help the patient with word finding. Allof them use the recording of snippets.
Further Features:
• Word finder: A dictionary with categories like “people”, “things”, “feelings” etc. Whenthe user clicks on a term it is read aloud. Furthermore he can record him/herself speakingthe word and listen to that.
• Customization: Personal workbooks can be created. The creator of the workbooks canenter own pictures (e. g. photos of family members or pets of the patient) and createown cues (Written cues and a recording of them). The personal workbook can also beassembled from existing workbooks in order to individualize the exercises.
Interface:
• Tutorial: The software has an obligatory tutorial workbook which has to be finishedbefore the user can do anything else. It leads through the menus and exercises in detail. Itenables patients who are not good with computers to use the software without problems.
• Use of hardware: The handling of the software is mostly mouse-operated. The exercisesare done via ‘point-and-click’ respectively ‘drag-and-drop’. When there are letters to beentered the patient can choose between the real keyboard and a virtual keyboard that isoperated with the mouse. The interface is designed aphasia friendly, there are big buttons,pictures can be enlarged and the surface is kept simple to avoid distraction.
Conclusion:This app is well structured, but focuses only on the building of sentences. The well compre-hensible tutorial work book makes it easy even for people who are not familiar with computersto handle the software. It is necessary to operate a mouse or a trackball, if there is a motorimpairment, assistance is needed. Pictures can be enlarged so they can be seen better when thepatient’s eyesight is bad. The software is not suitable for patients who are not able to read.Also it does not give real feedback. The patient has to choose on his own by the means of hisrecordings if his answers were correct. Alternatively he needs assistance in order to know.This software is most beneficial for patients with Wernicke’s Aphasia that lack awareness ofwhat they are saying.Screenshots of this software can bee seen in Figure 4.1 and 4.2.
– 32 – January 29, 2015

4.1 Commercially available CAT-Software
(a) Summary (b) How it helps
Figure 4.1: Screenshots from the Sentence Shaper tutorial workbook
(a) How to enlarge a picture (b) An easy sentence
Figure 4.2: Further screenshots from Sentence Shaper
Parrot Software
Parrot Software offers a variety of 78 programs for patients with aphasia and brain injury. Thereare exercises for language impairment but also for general cognitive skills. The individual pro-grams can be bought or an internet subscription can be made. The subscription allows accessto all of the programs for a price of 24.95 US$/ month. There are also conditions for hospitalsand rehabilitation centers from a 5-patient-version(39.95 US$/month) up to a version for an un-limited number of patients (125.00 US$/month).The internet subscription requires a browser (it is optimized for Google Chrome and Internet Ex-plorer) and for the speech recognition exercises a low noise unidirectional microphone is needed.The programs on CD-ROM run on Windows XP/7 and need at least 512 MB of RAM (Parrot-Software, 2014).
Main functions:
• Cognitive Skills: 36 exercises concerning Functional skills, cognitive reasoning, Memoryand Attention.
• Language Exercises: There are 42 exercises that train language skills. They includeexercises for spelling, reading comprehension, grammar, word recall and speech recognition.Many exercises ask the user to speak the answer into the microphone. In these the usercan usually choose, if he wants the task to be read out loud or not. After each completedtask there is a verbal feedback. A more detailed explanation of the exercises will be givenin the following. A list with descriptions of the exercises is provided on the Homepage. It
January 29, 2015 – 33 –

4 Commercially Available Software
can be seen below. Next to it there will either be a comment on its functionality or a “X”which implies, that the use is well possible and intuitive without any handling problems.
X
X
X
X
Open Definitions requires specific knowl-edge, e. g. about celebrities that are known inthe USA (but not necessarily anywhere else)
X
Spelling and Word Finding: Sometimes itis hard to find exactly the term the exerciseis looking for. If you use a similar term or asynonym, it is not accepted
X
– 34 – January 29, 2015

4.1 Commercially available CAT-Software
X
X
Completion from Partial Information requiresspecific knowledge, e. g. about celebrities thatare known in the USA (but not necessarilyanywhere else)
X
X
X
X
Multiple Meaning Words was quite hardfor me as a healthy person, but it is possiblethat this is because I am no English nativespeaker
January 29, 2015 – 35 –

4 Commercially Available Software
X
X
X
X
X
Using Adjectives works fine in general, butit has a minor bug, so it is not stated, that thelesson is completed
X
X
Word order does not accept alternative so-lutions that would be correct, too.
– 36 – January 29, 2015

4.1 Commercially available CAT-Software
Advanced Word Recall does not work. Typingdoes not work at all and speech recognitionworks only sometimes
X
X
X
Visual Confronting Naming: Typing doesnot work and speech recognition sometimesdoes not understand the right words
X
X
January 29, 2015 – 37 –

4 Commercially Available Software
X
X
X
Using propositional speech: The instruc-tions are not clear, it is not apparent, how todo the exercise
X
X
Further Features:
• Quick Performance summary: After finishing each exercise a table and graph thatshow the users performance and progress are evaluated. In that way you can see yourprogress at a glance. In the main menu you can also access a table where all results arelisted. (Fig 4.3 c))
• Personalization: A workbook can be created in the categories Reading Comprehension,Word Finding, Reasoning, Word Recognition and Sentence Formulation and it can bechosen between three levels of difficulty. The created workbook can be printed out andthe exercises can be done by writing with the hand. Another feature is, that the programuses your name in order to encourage you during the exercises. (Fig. 4.3 d))
• Baseline Tests: Test for Executive Function, Cognitive Reasoning, Memory, Vocabularyand Word Recall. Its not yet well-engineered, there is a design flaw which make it almostimpossible to read the answers that are for choice and the speech output is not reliable.
Interface:
• Speech Recognition and Synthesis: Many Exercises use speech recognition (Parrotuses the built-in speech recognition tool of the Internet browser). In general it works well,
– 38 – January 29, 2015

4.1 Commercially available CAT-Software
but with some terms it did not understand what was said, even after several (about ten)tries (e. g. “Salad”). This might be founded in the fact that the speech recognition algo-rithms are adjusted for American English and my pronunciation did not fit the recognitionpatterns. The speech synthesis is mostly natural, the words it doesn’t know are given letterby letter (e. g. “T-O” or “C-A-R”)
• Handling: The handling of the software inside the exercises is mostly easy. There areonly few buttons and detailed instructions can be looked at in every moment. In mostcases the instructions and “Help-Buttons” suffice for doing the exercise, a patient who iscapable of ‘point-and-click’ can manage the exercises. The navigation in the menu is morecomplicated as there are so many programs and many of the exercises contain up to 20levels of difficulty. The patient should be assisted by an SLT when choosing the exercisesfor him. Assistance should also be granted for adjusting the microphone settings so thatthe speech recognition can function well.
Conclusion:This program offers exercises for a big number of specific deficits. It can be helpful for variousimpairments of the brain. It also allows to keep track of the progress. Few exercises do notwork correctly or could be improved. In general I would recommend this software, especiallythe use of speech recognition can prove very beneficial. With a little assistance in the beginningthe software can easily be handled.Examples from this software can bee seen in figure 4.3.
Neuroling
Neuroling is a software consisting of three packages, each comes at the price of 129e. Each ofthem can be downloaded separately and fits the needs of different forms of aphasia. The packagesare: “Satzbau” (Syntax), “Wortfindung” (word finding) and “Sprachverstandnis” (languagecomprehension). The three packages will be analyzed separately. The software language isGerman.The system has to fulfill he following requirements (Neuroling, 2003):
• Windows 95 or better
• Pentium Processor or better
• Graphic Card with at least 2 MB RAM
• CD-ROM drive
• sound card and loudspeakers
• mouse or trackball
• 15” monitor or bigger
Syntax
Main functions:
• Single word exercises: There are four different exercises for cases, verbs, adjectives andprepositions. A sentence is given which has to be completed, the user can select from twoup to seven choices. The user is not given any cues, but he gets an acoustic feedback if hisanswer is correct or not.
January 29, 2015 – 39 –

4 Commercially Available Software
(a) Speech Recognition (b) Talk Your Way through a Maze
(c) A summary of the progress (d) Personalized encouraging
(e) Word-picture-matching (f) Spelling exercise: details are important
(g) Word order: Only the bottom one is accepted, al-though the other one is also correct
(h) Specific knowledge is asked
Figure 4.3: Screenshots from Parrot Software
– 40 – January 29, 2015

4.1 Commercially available CAT-Software
• Sentence exercises: The words of a sentence are given and the user has to put them inthe correct order. An acoustic cue is given and there is an acoustic feedback if the answeris right or wrong.
Further Features:
• There are no further features. It could be helpful to have some statistics to keep track ofthe progress.
Interface: The facts and problems mentioned here can also be found in the other two packages.
• Handling: There is no tutorial which makes it necessary to explore the software by oneself.The use is not always intuitive, even a computer literate person can sometimes only tryhow to do something correctly. If reading is not possible this software can’t be used. Onthe other hand there are big buttons and there are not many confusing features that woulddivert the patient.
• Use of hardware: The window can’t be maximized and the pictures can’t be zoomed in.So this software can only be used, when a big enough screen is available.
Conclusion:It is mainly made for Broca and Wernicke aphasia patients. Amnestic aphasia patients mayprofit from the sentence building exercise when there are deficits in this area. Although thereare not many operating elements, the handling can only be learned by trial-and-error which cangenerate frustration in the beginning. Assistance should be provided here. This also applies forthe other packages of Neuroling.In figure 4.4 examples for tasks can be seen
(a) Exercise for cases (b) Sentence building
Figure 4.4: Screenshots from Neuroling Syntax
January 29, 2015 – 41 –

4 Commercially Available Software
Word finding
Main functions:
• Word finding exercises: This is the easiest stage in the software.
◦ Anagrams: The user is given a picture of an item, its first letter and the other lettersare also given. They have to put in the right order.
◦ Separate exercises for vocals, consonants and syllables: A part of the wordand a picture are given and the missing vocals, consonants or syllables have to beadded in the right order.
• Cueing: A picture, an acoustic and a written representation (the user can choose, whetherhe wants to see the written word) of an item are given. The user has to choose the matchingterms from a list of words.
• Self-Cueing: A picture, an acoustic representation and - if wanted - matching terms foran item are given. The user has to type in the correct word. If he is wrong he can tryagain or look at the solution
Further Features: See “Syntax”
Interface:
• There is no screen-keyboard that can be handled via mouse, a real hardware-keyboardmust be used
Conclusion:The app teaches word finding step-by-step. It gives the user techniques to come up with thecorrect term in everyday life by cueing himself. It teaches the patient to teach himself.In general it aims at all aphasia types, but it can only be operated by someone who can readand write with a keyboard.
(a) Learning cueing (b) What to do when an error occurs
Figure 4.5: Screenshots from the Neuroling Word Finding
– 42 – January 29, 2015

4.1 Commercially available CAT-Software
Figure 4.5 shows screenshots from the cueing and self-cueing exercise. When you click on “derF”, the full word is shown. If you click on the pictures, the acoustic representation of the termis given.
Language Comprehension
Main functions:
• Meaning of pictures: There is a set of four pictures, the patient has to find the odd oneout. There are acoustic cues, reading is not necessary in this exercise
• Meaning of words:
◦ Word-picture-matching: A word is given and one picture out of four has to bechosen. There are several levels of difficulty in which the degree of discriminabilitybetween the pictures decreases.
◦ Abstract relations: a picture is given and a term has to be chosen that matchesthe situation best (Picture of a car → “repair”)
• Meaning of sentences:
◦ Sentence-picture-matching: A sentence is given and one picture out of four has tobe chosen. There are several levels of difficulty in which the degree of discriminabilitybetween the pictures decreases.
◦ Abstract relations: A sentence is given that has to be complemented by a matchingterm
Further Features:
• Illiteracy: In these exercises reading is not necessary, therefore it can be used by patientswith severe forms of aphasia. By pressing the key “F3” the terms are read aloud so thepatient can memorize them and choose the correct one.
Interface:See above
Conclusion:It is made for global and Wernicke aphasia patients. Listening as well as reading comprehensioncan be trained step by step.You can see some screenshots in figure 4.6.
Revivo
Revivo focuses on speech training. The user rehearses autonomously, the software itself doesnot give feedback. The full version can be downloaded for free. It only supports the operatingsystem Microsoft Windows, its language is German.The system has to meet the following requirements (Revivo, 2015):
• Windows
• disk space for the software (258 MB)
• sound card, loudspeakers
January 29, 2015 – 43 –

4 Commercially Available Software
(a) Find the odd one out (b) Word-picture-matching: adjectives
(c) Reading comprehension (d) Abstract language comprehension
Figure 4.6: Screenshots from Neuroling language comprehension
• mouse or trackball and keyboard
Main functions:
• Speech exercises: In these exercises single letters or words are presented. They arewritten down and a video is played in which the necessary mouth movements are displayed.The task is to say the letter or word. Originally the program had a speech recorder, so thatthe user could record himself and listen to what he said. Then he has to decide if it wascorrect. This function does not work anymore. On the homepage it is recommended tobuy an additional recording device. The user should also look into a mirror while speakingin order too see, if his mouth movements resemble the ones in the video. To verify, thatthe mouth movements were correct it can be helpful to have someone to assist.
• Further Exercises: These exercises give examples for everyday speaking. A picture isgiven and a matching sentence can be played aloud and repeated by the patient. Thereare no videos with these exercises.
– 44 – January 29, 2015

4.1 Commercially available CAT-Software
Further Features:
• AAC for written communication: One exercise can be used to create texts frompresets or to type them in letter for letter. These texts can be copied and pasted and usedin E-mails.
• Music Therapy: There are a few short video clips of a music therapist who encouragesthe user to sing some traditional German folk songs.
Interface:
• The handling of the software is mostly mouse-operated. There is not much interactionbetween user and software as it requires the user to practice speaking and listen to record-ings of it. It is not optimal that the patient has to use an external device for recording, itmakes the use of the software more complicated.
• In some exercises there are many small buttons, which can be quite confusing. The speechoutput of the AAC and the sound of the music therapy videos is a bit noisy, but it is stillcomprehensible.
• The font size can be set so everything is legible.
Conclusion:Other than the previous software solutions, this one is for free. Therefore it lacks the featuresand user (and aphasia) friendly surface. Nevertheless is has features like the mouth motionvideos and the singing videos that ease the training and contribute to a successful rehabilitationwhen used additionally to usual therapy.Figure 4.7 displays screenshots from Revivo.
January 29, 2015 – 45 –

4 Commercially Available Software
(a) Spelling exercise (b) Terms for very day life
(c) AAC environment (d) Music therapy
Figure 4.7: Screenshots from Revivo
4.1.2 Supporting software
Especially on mobile devices there can be found a variety of applications, that support aphasiapatients in everyday life. When searching i. e. the Apple Store there are many results for thekey words ”Aphasie”, ”Aphasia”, ...In the previous section there is already an example for aphasia training software on a tabletPC. In the following table there is a small selection of other applications and their description.There are a lot more applications, but this way one can get an overview over the offerings andthe pricing.
– 46 – January 29, 2015

4.2 Final Conclusion and Prospects
Name Type Description Price
SpeechCare Aphasie Therapy, Stimulipresentation
tasks in 3 levels of difficulty, ger-man
49.99e
Comprehension Apha-sia
Therapy, Stimulipresentation
Listening comprehension is ex-amined by yes/no questions, en-glish
17.99e
i-MEC fr Therapy, Stimulipresentation
diagnosis test, exercises, french 62.99e
SpeechCare Aphasie- Bildkarten fur Lo-gopaden Kinder undErwachsene
Stimuli presenta-tion
flashcards (number can be cho-sen) for SLT
39.99e
Speech4Good Behavior Track-ing, feedback
delayed auditive feedback andtacking notes, is made for SLT,english
49.99e
Behaviour Tracker Behavior Track-ing
Intended for austixtic children,can be customized for aphasiapatients
0.89e
Token Test Clinician tool for SLT: Evaluation and manage-ment of patient data
5.49e
Bildworterbuch fur dieReise - BabelDeck
Dictionary pictures and description in 30languages
1.79e
TalkTablet AAC pictures are used to create sen-tences, multiple languages
69.99e
EZSpeechPROMale/Female
AAC Typing-to-speech, english 89.99e
Healthcare communica-tion App
AAC AAC for communication betweenpatients and caregivers, english
44.99e
... ... ... ...
Table 4.1: Applications
4.2 Final Conclusion and Prospects
By taking a look at the literature concerning computer assisted aphasia therapy and analyzingsome of the available programs, I can determine the beneficial contribution to recovery this kindof therapy provides. In addition to usual care, great progress can be made and life quality canbe enhanced. When engaging in computer treatment, the patient should be supported by histherapist to find the software that suits his needs best. The therapist should take care that thepatient is granted any assistance that he needs for handling the soft- and hardware. After thisanalysis, computer therapy as a part of the patient’s recovery plan can be recommended. Ingeneral, technology can ease everyday life for the patient - either by supporting his recovery orby directly helping with communication.From this point, further development can be made. Some features of the programs such asstatistics that can be used to track the patients progress and included standardized baselinetests should be generally established. Regarding baseline tests, it could also be interesting tohave programs that adjust themselves to the needs of the patient according to these tests andthe users performance in the exercises.Also the use of speech recognition has great potential. This could eventually be supplemented
January 29, 2015 – 47 –

4 Commercially Available Software
by face recognition algorithms that use the webcam of the computer. In this manner, patientswith speech disorder can get a feedback that relies not only on the spoken words but also ontheir mouth movements. Specific exercises for that purpose could be developed.These are possibilities that would make the patient less dependent on an SLT and the softwarecould be used more autonomously.
– 48 – January 29, 2015
Aphasia Therapy
Bibliography
AWMFonline, “AWMFonline Leitlinien,” 2012. [Online]. Available: http://www.awmf.org/leitlinien/detail/ll/030-090.html
J. Mayer, “Aphasien,” 2014. [Online]. Available: http://www2.ims.uni-stuttgart.de/sgtutorial/aphasien.html
——, “Differentialdiagnose,” 2014. [Online]. Available: http://www2.ims.uni-stuttgart.de/sgtutorial/diffdiag.html
——, “Aachener Aphasie Test,” 2014. [Online]. Available: http://www2.ims.uni-stuttgart.de/sgtutorial/aat.html
F. R. P. Andrew Kortesz, M.D., “Western Aphasia Battery Test Booklet,” Department ofClinical Neurological Sciences University of Western Ontario, 1982. [Online]. Available:http://www.strokestrategy.ab.ca/Capital Tools/UAHSTRK0220070928094730.pdf
L. E. Nicholas, R. H. Brookshire, D. L. MacLennan, J. G. Schumacher, and S. A. Porrazzo,The Boston Naming Test: Revised Administration and Scoring Procedures and NormativeInformation for Non-Brain-Damaged Adults. College-Hill Press, 1989, pages 103-115.
J. Mayer, “Amnestische Aphasie,” 2014. [Online]. Available: http://www2.ims.uni-stuttgart.de/sgtutorial/amnestische.html
——, “Broca-Aphasie,” 2014. [Online]. Available: http://www2.ims.uni-stuttgart.de/sgtutorial/broca.html
——, “Wernicke Aphasie,” 2014. [Online]. Available: http://www2.ims.uni-stuttgart.de/sgtutorial/wernicke.html
——, “Globale Aphasie,” 2014. [Online]. Available: http://www2.ims.uni-stuttgart.de/sgtutorial/globale.html
——, “Transkortikale Aphasie,” 2014. [Online]. Available: http://www2.ims.uni-stuttgart.de/sgtutorial/transkortikale.html
——, “Leitungsaphasie,” 2014. [Online]. Available: http://www2.ims.uni-stuttgart.de/sgtutorial/leitungs.html
DeutscherBundesverbandFurLogopadenE.V., “DBL Aphasie,” 2013. [Online].Available: http://www.dbl-ev.de/kommunikation-sprache-sprechen-stimme-schlucken/stoerungen-bei-erwachsenen/stoerungsbereiche/sprache/aphasie.html
G.-B. GAB and D. DGNKN, “Qualitatskriterien und Standards fur die Therapie von Patientenmit erworbenen neurogenen Storungen der Sprache (Aphasie) und des Sprechens (Dysarthrie)Leitlinien 2000,” 2000. [Online]. Available: http://www.aphasiegesellschaft.de/files/6013/6268/2690/LL 2000 GAB DGNKN.pdf
M. Baumann, “Musiktherapie fur Aphasie,” 2006. [Online]. Available: http://mit-musik-geht-reha-besser.de/html/aphasie.html
January 29, 2015 – 49 –

Bibliography
Evocare, “Teletherapie bei Aphasikern,” 2008. [Online]. Available: http://www.evocare.de/Supervidierte Teletherapie Aphasiker.pdf
Pederson, Aphasia in Stroke, ser. Annals of Neurology, October 1995, vol. Vol 38 No 4, no.Pedersen et al: Aphasia in Strok.
B. H. Dobkin, “Rehabilitation and Recovery of the Patient with Stroke,” pp. 1116–1133, 2011,cited By (since 1996):1. [Online]. Available: www.scopus.com
M. Howard S Kirshner, “Aphasia Follow-up,” 2014. [Online]. Available: http://emedicine.medscape.com/article/1135944-followup
J. Kurland, A. R. Wilkins, and P. Stokes, “iPractice: Piloting the effectiveness of a tablet-basedhome practice program in aphasia treatment,” Seminars in speech and language, vol. 35,no. 1, pp. 51–63, 2014. [Online]. Available: www.scopus.com
R. Palmer, P. Enderby, C. Cooper, N. Latimer, S. Julious, G. Paterson, M. Dimairo, S. Dixon,J. Mortley, R. Hilton, A. Delaney, and H. Hughes, “Computer therapy compared with usualcare for people with long-standing aphasia poststroke: A pilot randomized controlled trial,”Stroke, vol. 43, no. 7, pp. 1904–1911, 2012, cited By (since 1996):8. [Online]. Available:www.scopus.com
L. R. Cherney, A. S. Halper, and R. C. Kaye, “Computer-based script training foraphasia: Emerging themes from post-treatment interviews,” Journal of communicationdisorders, vol. 44, no. 4, pp. 493–501, 2011, cited By (since 1996):4. [Online]. Available:www.scopus.com
C. Phillips, “What is a QALY,” 2009. [Online]. Available: http://www.medicine.ox.ac.uk/bandolier/painres/download/whatis/QALY.pdf
Generics and BiosimilarsInitiative, “What is the incremental cost effective-ness ratio,” 2010. [Online]. Available: http://www.gabionline.net/Generics/General/What-is-the-incremental-cost-effectiveness-ratio-ICER
C. Brandenburg, L. Worrall, A. D. Rodriguez, and D. Copland, “Mobile computing technologyand aphasia: An integrated review of accessibility and potential uses,” Aphasiology, vol. 27,no. 4, pp. 444–461, 2013, cited By (since 1996):1. [Online]. Available: www.scopus.com
C. Golashesky, “Technology applications at the Adler Aphasia Center,” Topics in StrokeRehabilitation, vol. 15, no. 6, pp. 580–585, 2008, cited By (since 1996):2. [Online]. Available:www.scopus.com
Sentenceshaper, “Computer requirements,” 2015. [Online]. Available: http://sentenceshaper.com/computer-requirements/
ParrotSoftware, “Frequently asked quenstions,” 2014. [Online]. Available: http://www.parrotsoftware.com/home/faq.htm
Neuroling, “Computer requirements,” 2003. [Online]. Available: http://www.neuroling.de/software.htm
Revivo, “FAQ,” 2015. [Online]. Available: http://www.aphasie.com/faq.html
finanzen.at, “Wahrungsrechner,” 2014. [Online]. Available: http://www.finanzen.at/waehrungsrechner
– 50 – January 29, 2015