brugada syndrome dr. raj santan
TRANSCRIPT


40 year old male with :FeverRight parotid abscessLeft knee septic arthritis

k/c/o DM – on regular treatment with OHA’SO/E:
PR - 100/ mt ,regularB.P - 120/80 mmhg
C.V.S – S1S2+ , no murmurs
R.S – NVBS, b/l creps+C.N.S – NFND
P/A – Soft, no organomegaly


HR- 100/ mtAxis- LAD sinus rhythmST segment elevation ( coved in shape ) in V1 –
V3
T wave inversion in V1 –V3
Suggestive of BRUGADA SIGN

first described in 1992By Joseph brugada, Pedro brugada
and Ramon brugada

Is a clinical entity characterized by 1.a typical ECG pattern( RBBB and persistent ST elevation in precordialleads) and
2. sudden cardiac death

Inherited in an autosomal
dominant pattern
More common in males.
Higher prevalence in south east Asian
populations.
It is the major cause of sudden unexplained death syndrome (SUDS)

is the most common cause of sudden
death in young men without known
underlying cardiac disease
known colloquially in the Philippines
as bangungut (“to rise and moan in
sleep”), in Japan as pokkuri(“sudden and
unexpectedly ceased phenomena”) and in
Thailand as Lai Tai (“death during sleep”).

The mean age of sudden death is 41, with
the age at diagnosis ranging from 2 days
to 84 years.

20 % of the cases are associated with mutations in the gene coding for sodium channel SCN 5A, located in short arm of 3 rd chromosome
Loss-of-function mutations in this gene
lead to a loss of the action potential dome
of some epicardial areas of the right ventricle

Sodium channelopathy
Loss of action potential dome of some
epicardial areas of right ventricle
Transmural dispersion
of repolarization
Epicardial dispersion
of repolarization
ST-segment elevation and
the development of a
vulnerable window across
the ventricular wall
Facilitates phase 2 re-entry
which generates reentrant
extrasystole that captures
the vulnerable window and
precipitates VT/ V fib

coved ST segment elevation > 2 mm followed by negative T wave in V1 to V3 diagnostic , also called as
“Brugada sign”
saddle back configuration of ST elevation > 2 mm ending in a positive or biphasic T wave In V1 to V3 (atleast 2 leads)
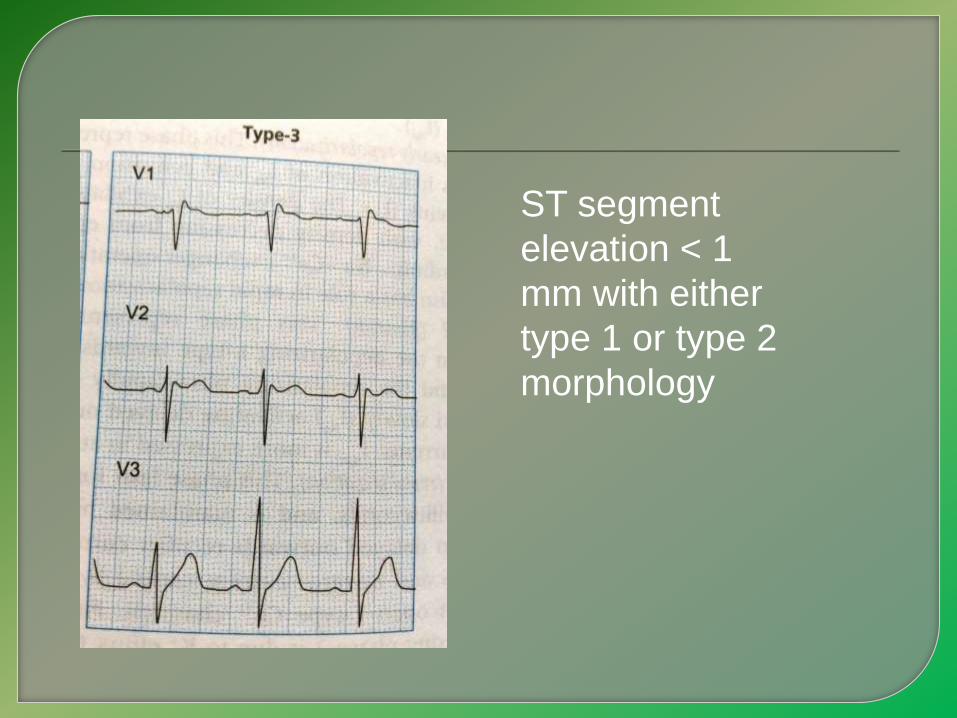
ST segment
elevation < 1
mm with either
type 1 or type 2
morphology

Documented ventricular fibrillation (VF) or
polymorphic ventricular tachycardia (VT).
Family history of sudden cardiac death at
<45 years old .
Coved-type ECGs in family members.
Inducibility of VT with programmed
electrical stimulation .
Syncope.
Nocturnal agonal respiration.

Fever
Ischaemia
Hypokalaemia
Hypothermia
Post DC cardioversion
Drug induced
• Sodium channel blockers eg: Class IC
Flecainide, Propafenone class IA: ajmaline
and procainamide
• Calcium channel blockers
• Alpha agonists
• Beta Blockers
• Nitrates
• Cholinergic stimulation
• Cocaine
• Alcohol




Quinidine has been found to both
decrease the number of VF episodes and
correct spontaneous ECG changes,
possibly via inhibiting Ito channels
