bronchiectasis in 2016 - société suisse de cardiologie · bronchiectasis in 2016 ... rate of...
TRANSCRIPT
Bronchiectasis in 2016
James D Chalmers MD PhD FRCPE
Senior Lecturer and Honorary Consultant Physician
University of Dundee and Ninewells Hospital and Medical School
Scotland, UK

Presenter disclosures
Clinical TrialsAstraZeneca, Aradigm corporation, Bayer Healthcare, GSK
Research Grant SupportWellcome Trust, Chief Scientist Office, Medical Research Council, AstraZeneca, EU Innovative Medicines Initiative, European Respiratory Society, Tenovus Scotland, Bayer Healthcare, Aradigm Corporation, Griffols, Pfizer inc
ConsultancyBayer Healthcare, Griffols, AstraZeneca, Basilea, Napp, Raptor
An old disease re-emerging
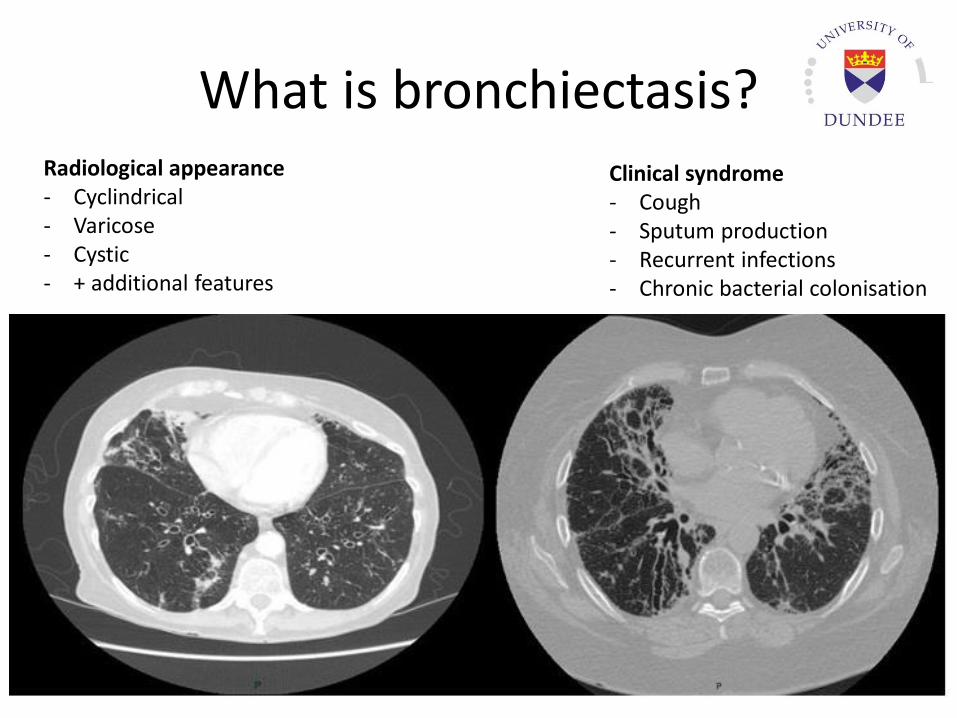
What is bronchiectasis?Radiological appearance- Cyclindrical- Varicose- Cystic- + additional features
Clinical syndrome- Cough- Sputum production- Recurrent infections- Chronic bacterial colonisation
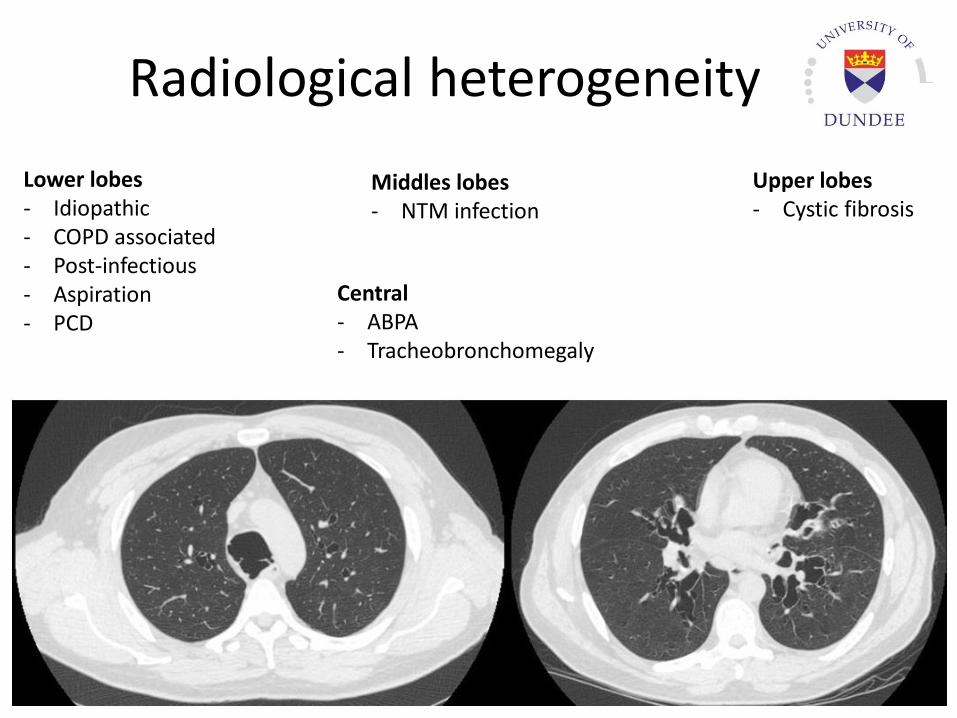
Radiological heterogeneity
Lower lobes- Idiopathic- COPD associated- Post-infectious- Aspiration- PCD
Central- ABPA- Tracheobronchomegaly
Middles lobes- NTM infection
Upper lobes- Cystic fibrosis
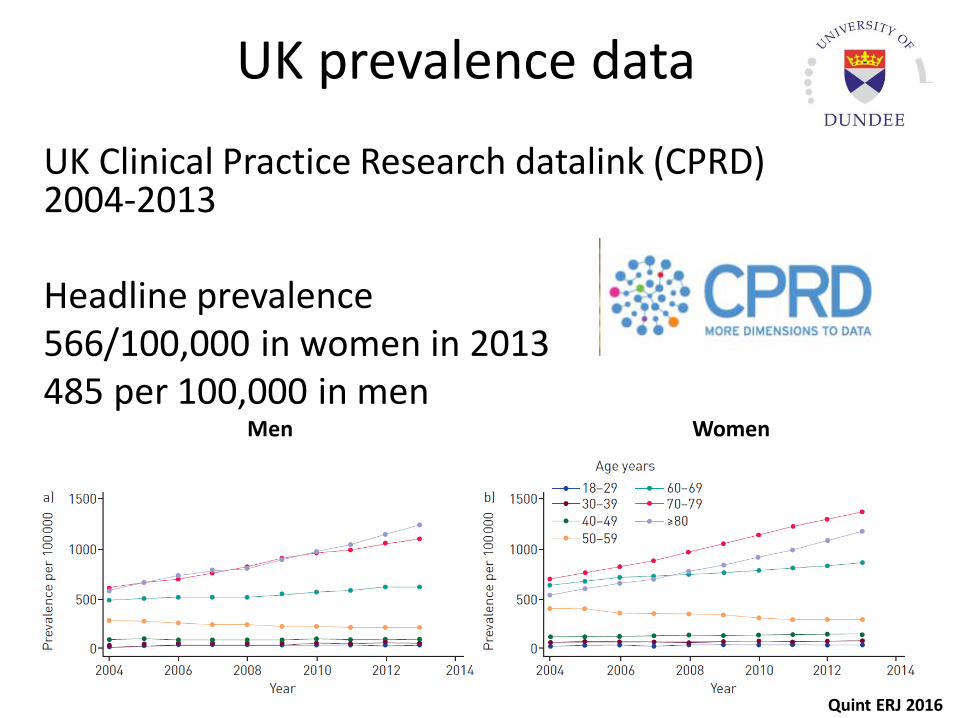
UK prevalence data
UK Clinical Practice Research datalink (CPRD) 2004-2013
Headline prevalence566/100,000 in women in 2013485 per 100,000 in men
Men Women
Quint ERJ 2016
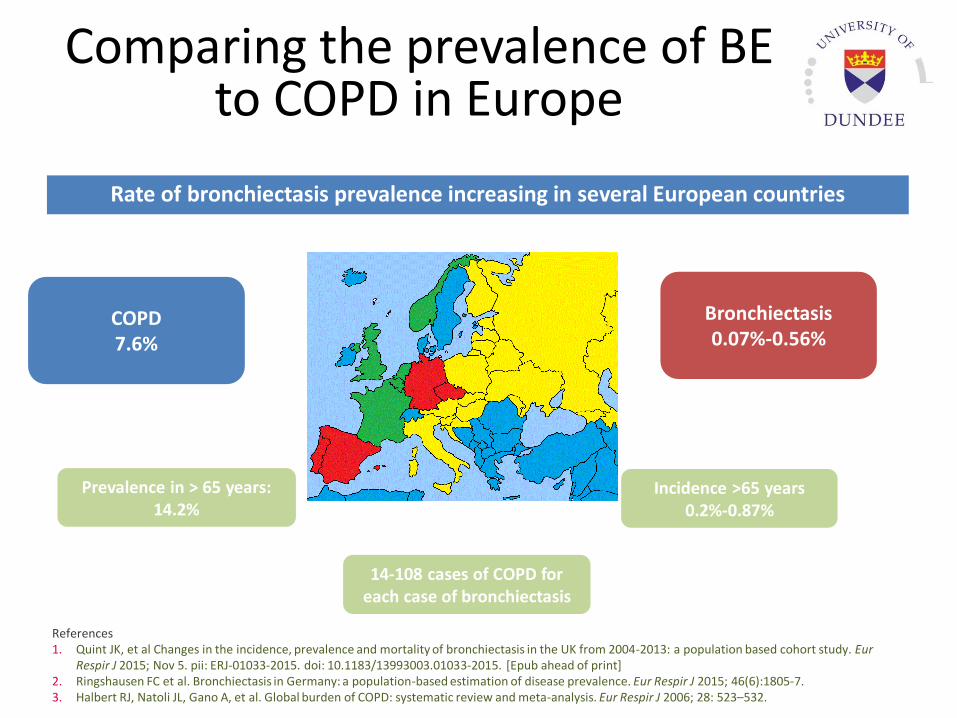
Comparing the prevalence of BE to COPD in Europe
7
COPD7.6%
Bronchiectasis0.07%-0.56%
Incidence >65 years0.2%-0.87%
14-108 cases of COPD for each case of bronchiectasis
Prevalence in > 65 years:14.2%
Rate of bronchiectasis prevalence increasing in several European countries
References1. Quint JK, et al Changes in the incidence, prevalence and mortality of bronchiectasis in the UK from 2004-2013: a population based cohort study. Eur
Respir J 2015; Nov 5. pii: ERJ-01033-2015. doi: 10.1183/13993003.01033-2015. [Epub ahead of print]2. Ringshausen FC et al. Bronchiectasis in Germany: a population-based estimation of disease prevalence. Eur Respir J 2015; 46(6):1805-7. 3. Halbert RJ, Natoli JL, Gano A, et al. Global burden of COPD: systematic review and meta-analysis. Eur Respir J 2006; 28: 523–532.
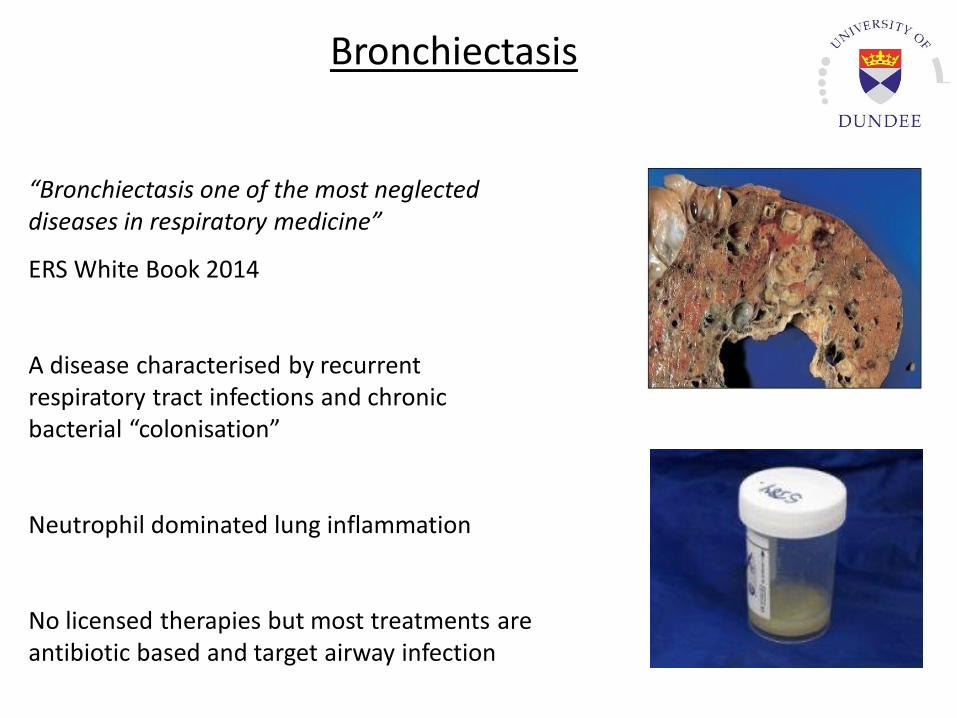
“Bronchiectasis one of the most neglected diseases in respiratory medicine”
ERS White Book 2014
A disease characterised by recurrent respiratory tract infections and chronic bacterial “colonisation”
Neutrophil dominated lung inflammation
No licensed therapies but most treatments are antibiotic based and target airway infection
Bronchiectasis
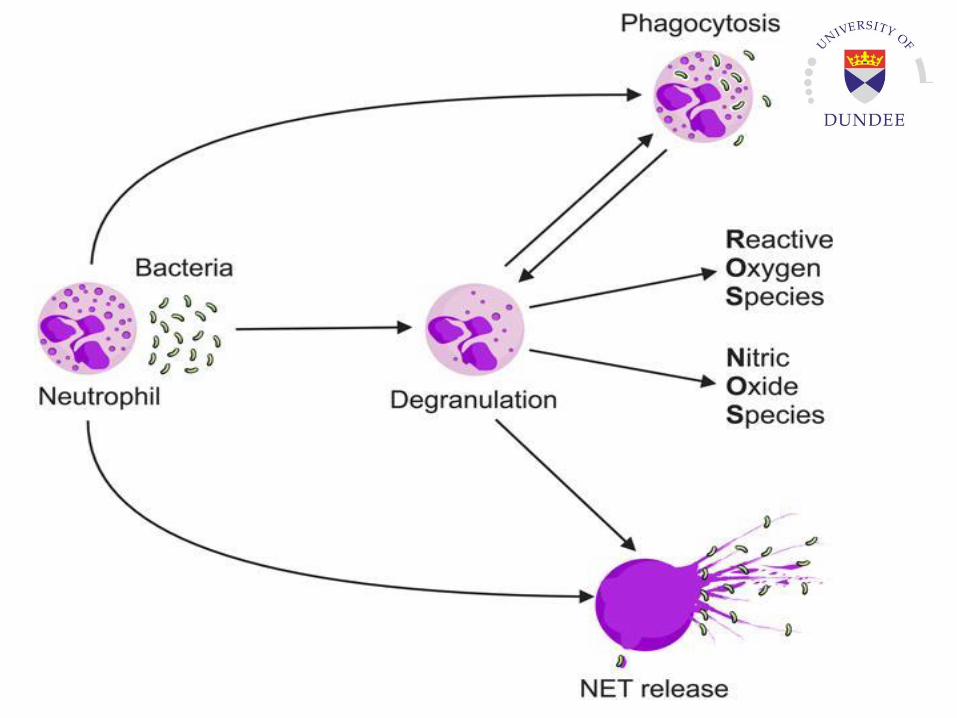
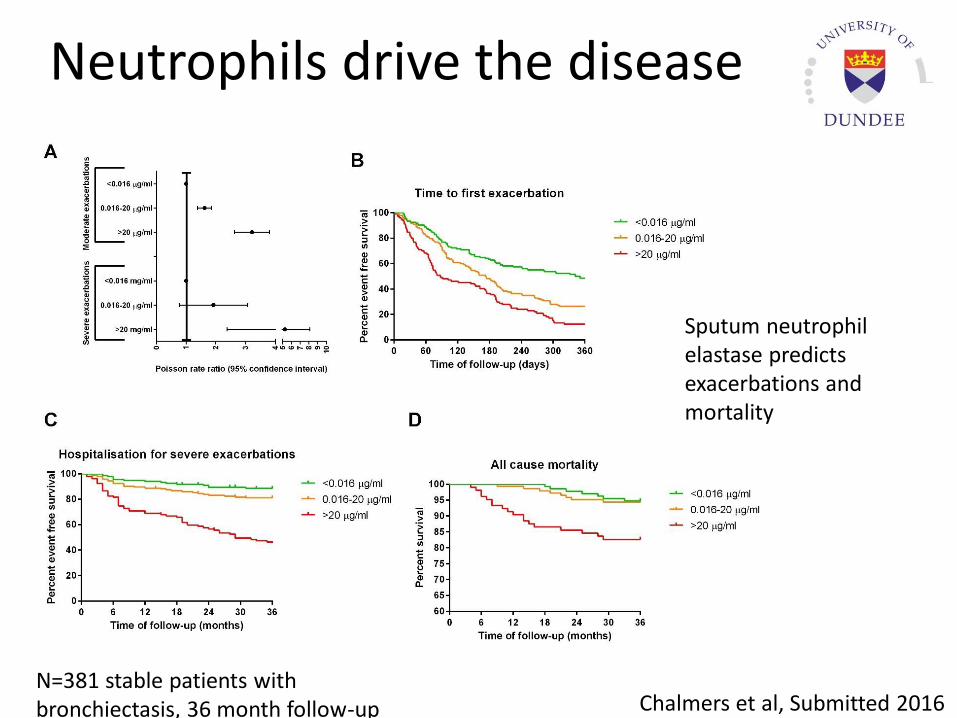
Neutrophils drive the disease
Chalmers et al, Submitted 2016N=381 stable patients with bronchiectasis, 36 month follow-up
Sputum neutrophil elastase predicts exacerbations and mortality
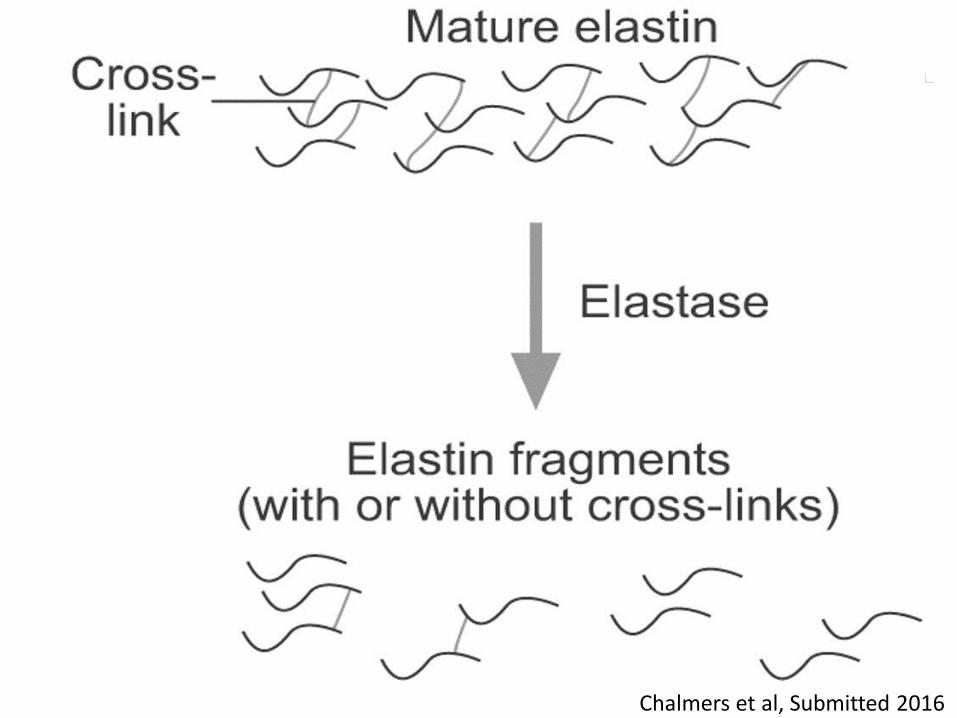
Chalmers et al, Submitted 2016
Released desmosine and isodesmosine
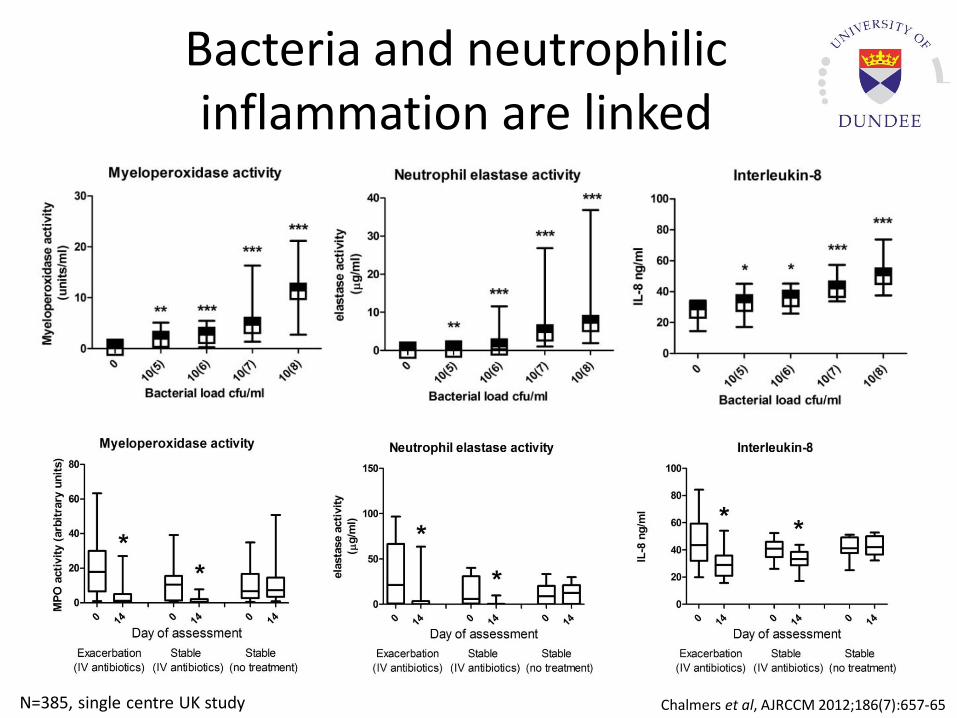
Bacteria and neutrophilic inflammation are linked
Chalmers et al, AJRCCM 2012;186(7):657-65N=385, single centre UK study
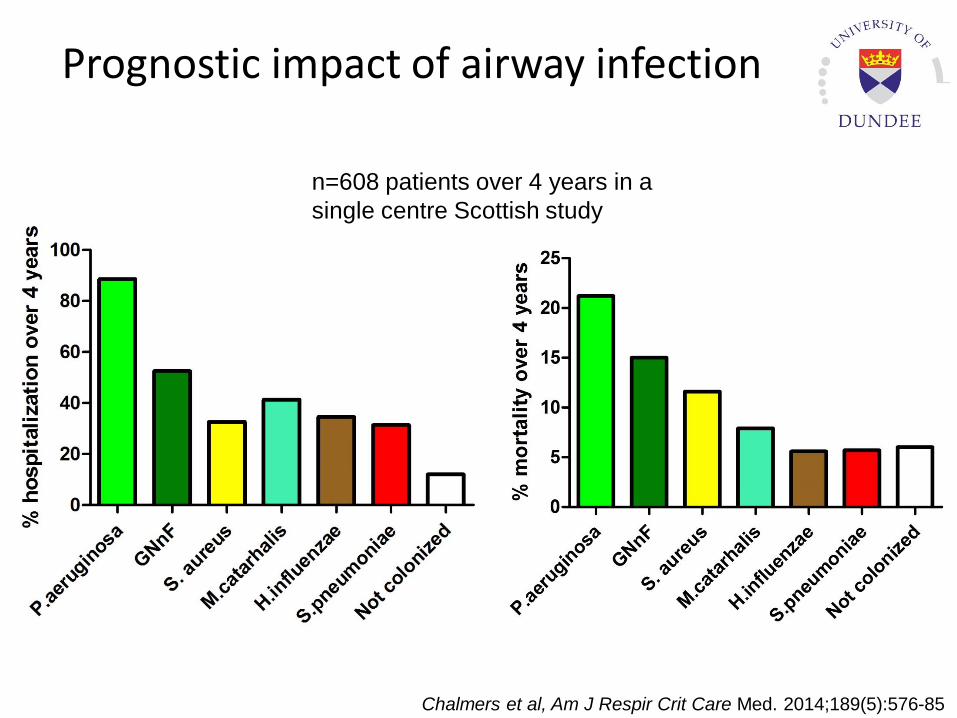
Prognostic impact of airway infection
n=608 patients over 4 years in a
single centre Scottish study
Chalmers et al, Am J Respir Crit Care Med. 2014;189(5):576-85
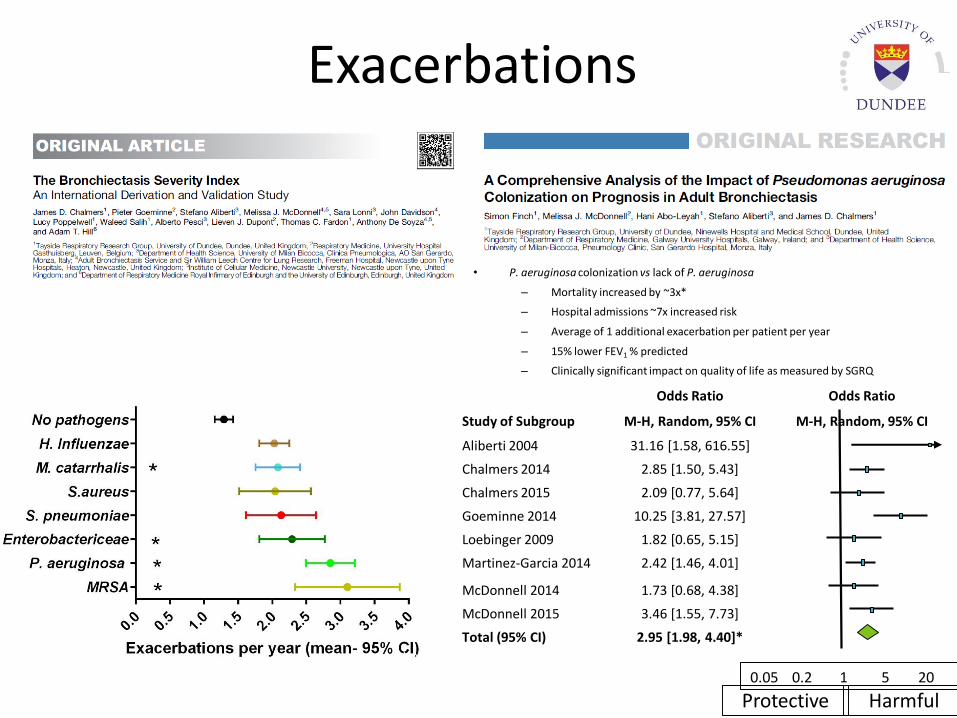
Exacerbations
• P. aeruginosa colonization vs lack of P. aeruginosa
– Mortality increased by ~3x*
– Hospital admissions ~7x increased risk
– Average of 1 additional exacerbation per patient per year
– 15% lower FEV1 % predicted
– Clinically significant impact on quality of life as measured by SGRQ
Finch et al, Ann Am Thoracic Soc. 2015 12(11):1602-11
Study of Subgroup
Odds Ratio Odds Ratio
M-H, Random, 95% CI M-H, Random, 95% CI
Aliberti 2004 31.16 [1.58, 616.55]
Chalmers 2014 2.85 [1.50, 5.43]
Chalmers 2015 2.09 [0.77, 5.64]
Goeminne 2014 10.25 [3.81, 27.57]
Loebinger 2009 1.82 [0.65, 5.15]
Martinez-Garcia 2014 2.42 [1.46, 4.01]
McDonnell 2014 1.73 [0.68, 4.38]
McDonnell 2015 3.46 [1.55, 7.73]
Total (95% CI) 2.95 [1.98, 4.40]*
0.05 0.2 1 5 20
Protective Harmful
Heterogeneity: Tau2=0.13; Chi2=11.72, df=7 (P=0.11); I2=40%Test for overall effect: Z=5.29 (P < 0.00001)
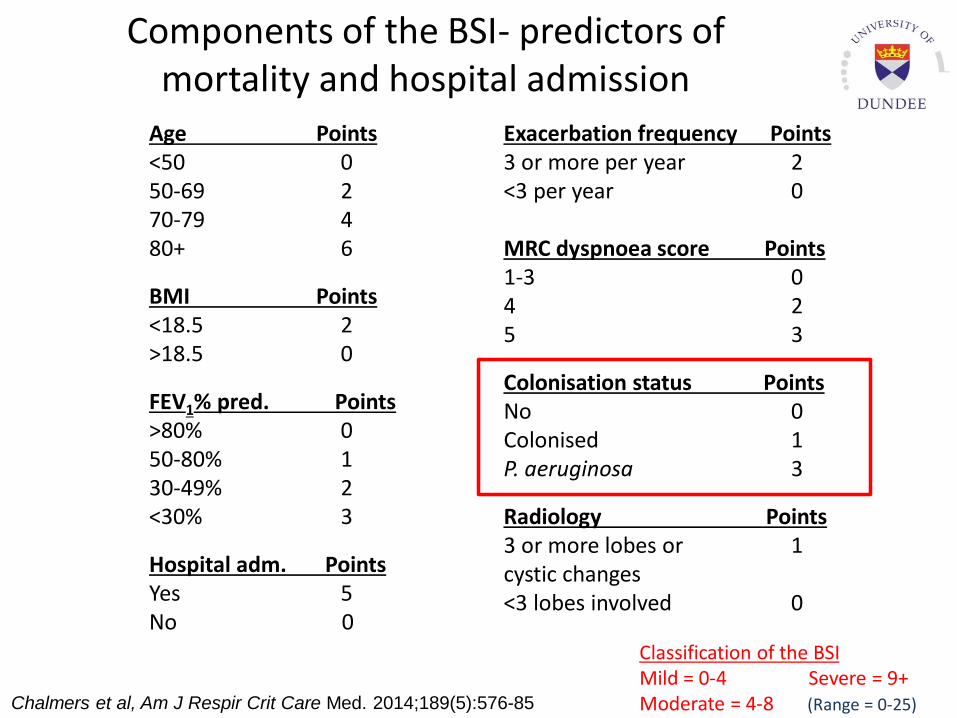
Components of the BSI- predictors of mortality and hospital admission
Age Points<50 050-69 270-79 480+ 6
BMI Points<18.5 2>18.5 0
FEV1% pred. Points>80% 050-80% 130-49% 2<30% 3
Hospital adm. PointsYes 5No 0
Exacerbation frequency Points3 or more per year 2<3 per year 0
MRC dyspnoea score Points1-3 04 25 3
Colonisation status PointsNo 0Colonised 1P. aeruginosa 3
Radiology Points3 or more lobes or 1 cystic changes<3 lobes involved 0
Classification of the BSIMild = 0-4 Severe = 9+Moderate = 4-8 (Range = 0-25)Chalmers et al, Am J Respir Crit Care Med. 2014;189(5):576-85
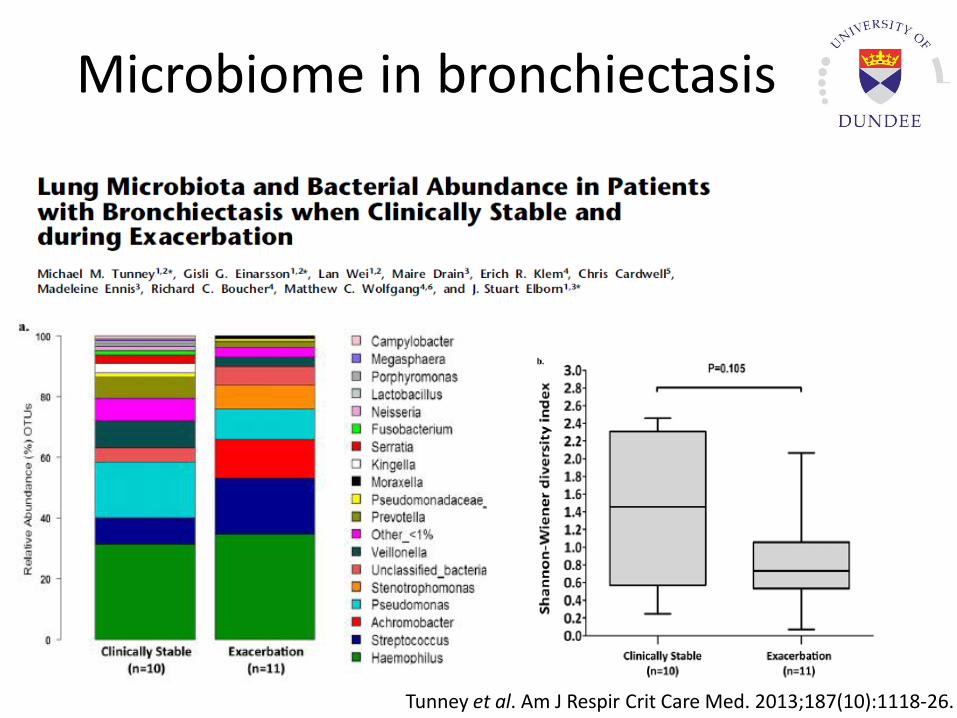
Microbiome in bronchiectasis
Tunney et al. Am J Respir Crit Care Med. 2013;187(10):1118-26.
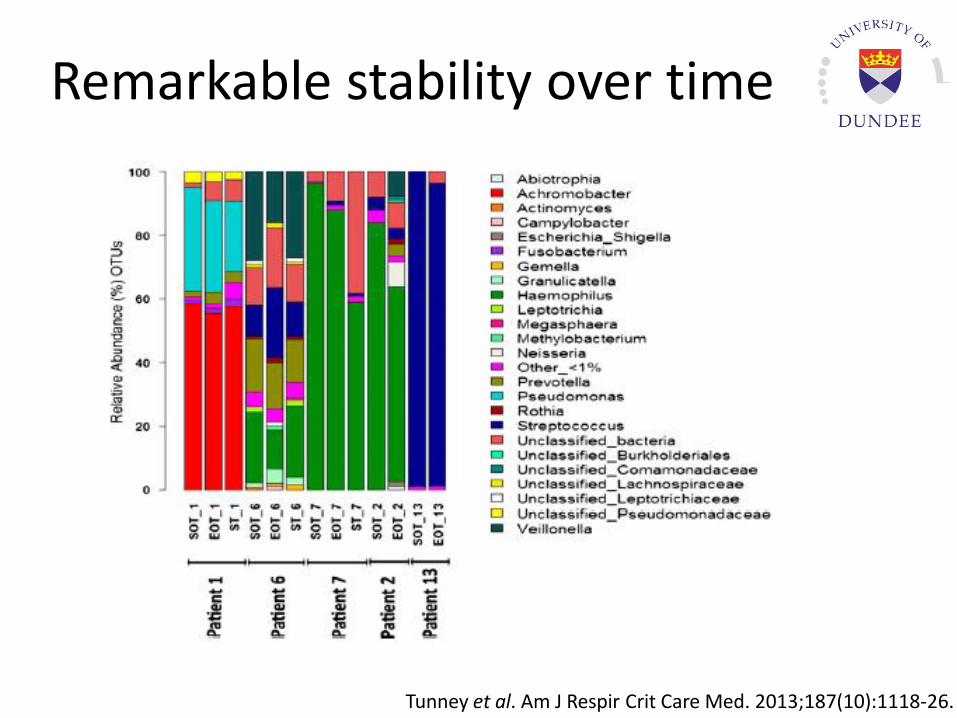
Remarkable stability over time
Tunney et al. Am J Respir Crit Care Med. 2013;187(10):1118-26.
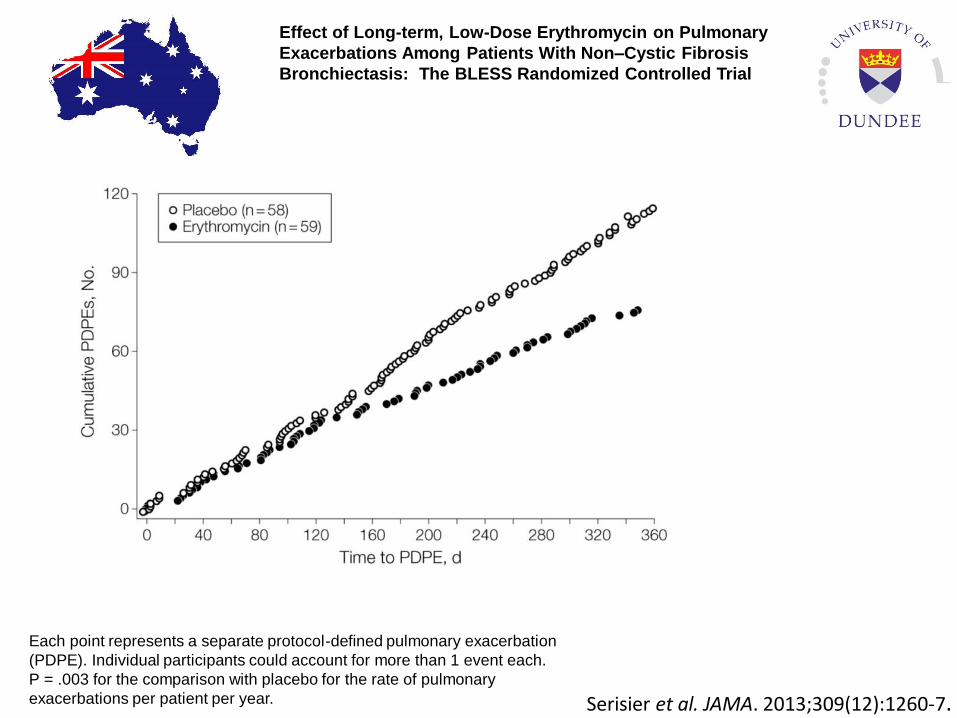
Effect of Long-term, Low-Dose Erythromycin on Pulmonary
Exacerbations Among Patients With Non–Cystic Fibrosis
Bronchiectasis: The BLESS Randomized Controlled Trial
Each point represents a separate protocol-defined pulmonary exacerbation
(PDPE). Individual participants could account for more than 1 event each.
P = .003 for the comparison with placebo for the rate of pulmonary
exacerbations per patient per year. Serisier et al. JAMA. 2013;309(12):1260-7.
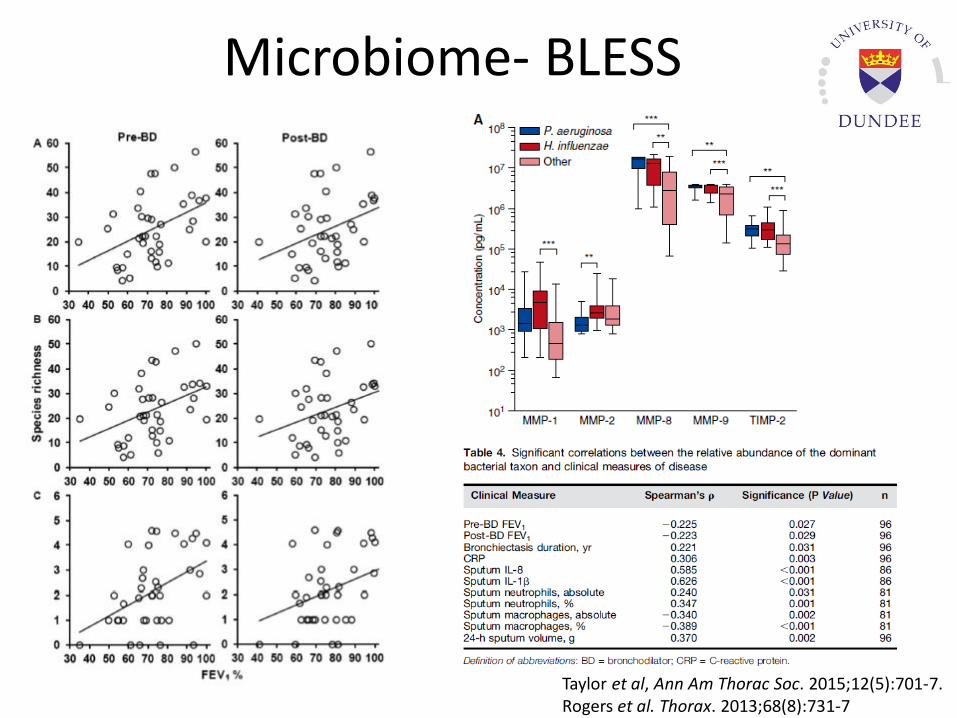
Microbiome- BLESS
Taylor et al, Ann Am Thorac Soc. 2015;12(5):701-7.Rogers et al. Thorax. 2013;68(8):731-7
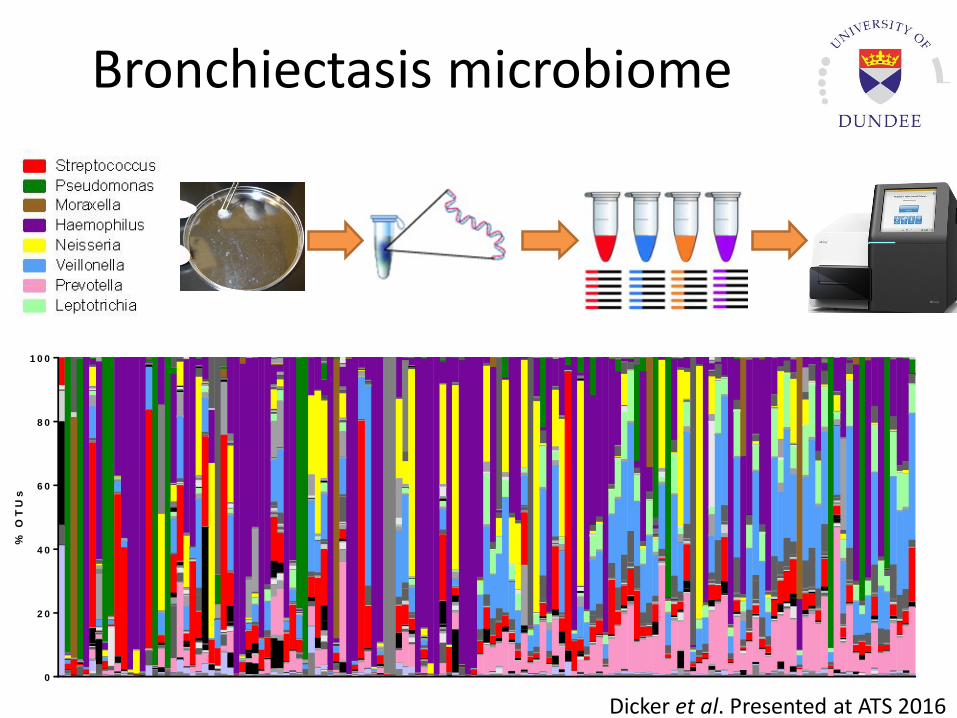
Bronchiectasis microbiome
B20R
B
B77N
RO
B177A
B
B206JW
B771JD
B1006JC
B1425K
BE
99W
D
TB
S004
TB
S005
TB
S008
TB
S010
TB
S014
TB
S018
TB
S024
TB
S026
TB
S028
TB
S029
TB
S030
TB
S036
TB
S039
TB
S045
TB
S046
TB
S049
TB
S050
TB
S055
TB
S059
TB
S065
TB
S067
TB
S068
TB
S070A
TB
S070B
TB
S071A
TB
S071B
TB
S074A
TB
S074B
TB
S076
TB
S077
TB
S080
TB
S082
TB
S086
TB
S087
TB
S088
TB
S091
TB
S092
TB
S100
TB
S102
TB
S107
TB
S110
TB
S111
TB
S118
TB
S119
TB
S121
TB
S122
TB
S125
TB
S126
TB
S127
TB
S128
TB
S129
TB
S132
TB
S136
TB
S137
TB
S142
TB
S143
TB
S144
TB
S145
TB
S147
TB
S148
TB
S149
TB
S152
TB
S154
TB
S157
TB
S159
TB
S162
TB
S165
TB
S166
TB
S167
TB
S169
TB
S172
TB
S173
TB
S175
TB
S177
TB
S178
TB
S182
TB
S185
TB
S187
TB
S191
TB
S193
TB
S194
TB
S196
TB
S199
TB
S204
TB
S205A
TB
S206
TB
S207
TB
S209
TB
S212
TB
S213
TB
S217
TB
S220
TB
S222
TB
S225
TB
S227
TB
S228
TB
S229
TB
S233
TB
S238
TB
S239
TB
S246
TB
S247
TB
S252
TB
S253
TB
S254
TB
S256
TB
S261
TB
S263
TB
S267
TB
S268
TB
S269
TB
S281
TB
S283
TB
S284
TB
S285
TB
S288
TB
S289
TB
S291
TB
S294
TB
S298
TB
S299
TB
S303
TB
S307
TB
S312
TB
S313
TB
S314A
TB
S314B
TB
S319
TB
S323B
0
2 0
4 0
6 0
8 0
1 0 0
% O
TU
s
Dicker et al. Presented at ATS 2016
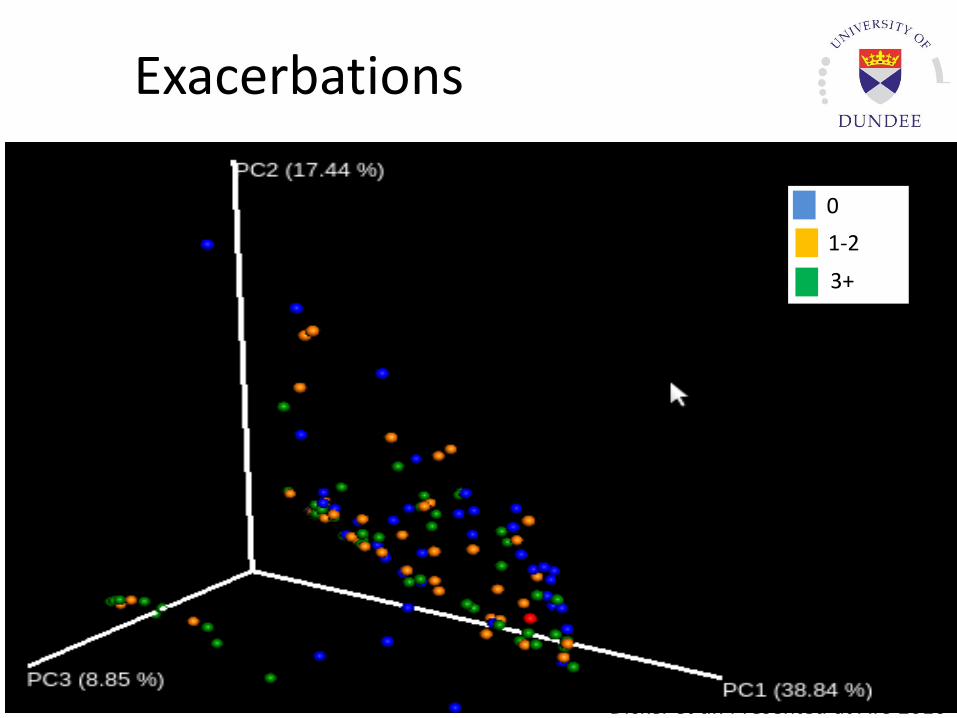
Exacerbations
0
1-2
3+
Dicker et al. Presented at ATS 2016
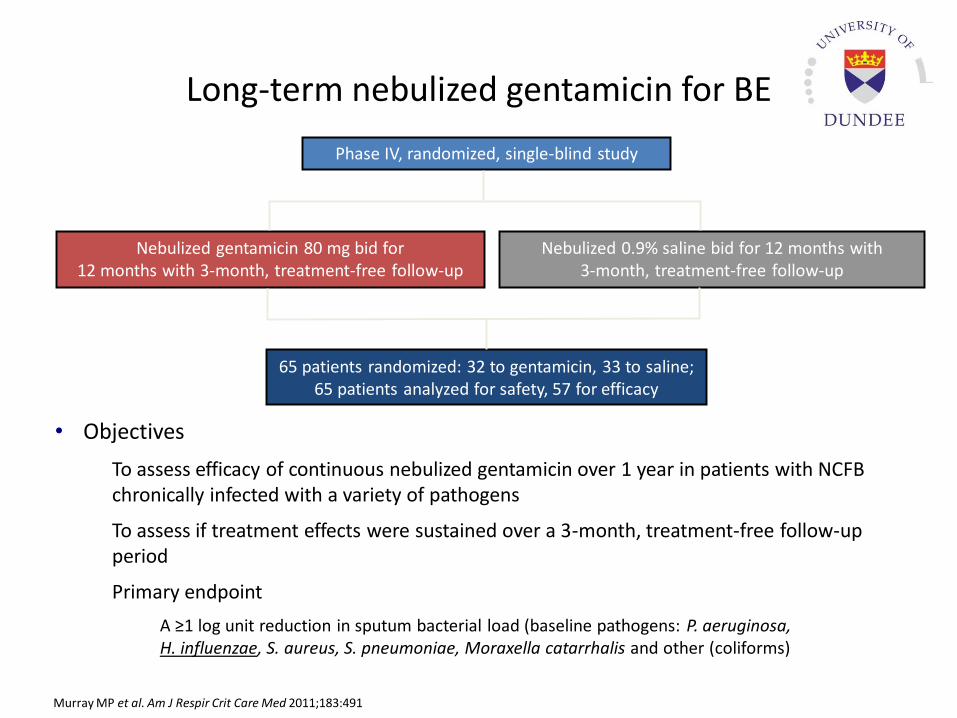
Long-term nebulized gentamicin for BE
• Objectives
– To assess efficacy of continuous nebulized gentamicin over 1 year in patients with NCFB chronically infected with a variety of pathogens
– To assess if treatment effects were sustained over a 3-month, treatment-free follow-up period
– Primary endpoint
– A ≥1 log unit reduction in sputum bacterial load (baseline pathogens: P. aeruginosa, H. influenzae, S. aureus, S. pneumoniae, Moraxella catarrhalis and other (coliforms)
Murray MP et al. Am J Respir Crit Care Med 2011;183:491
Phase IV, randomized, single-blind study
Nebulized gentamicin 80 mg bid for 12 months with 3-month, treatment-free follow-up
Nebulized 0.9% saline bid for 12 months with 3-month, treatment-free follow-up
65 patients randomized: 32 to gentamicin, 33 to saline;65 patients analyzed for safety, 57 for efficacy
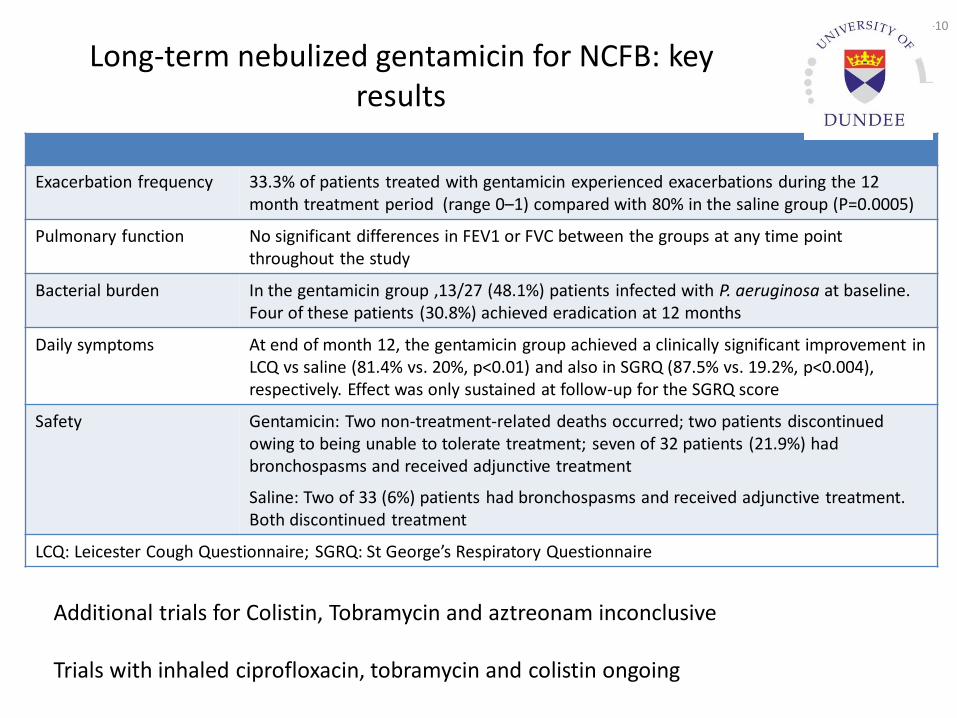
Long-term nebulized gentamicin for NCFB: key results
Exacerbation frequency 33.3% of patients treated with gentamicin experienced exacerbations during the 12 month treatment period (range 0–1) compared with 80% in the saline group (P=0.0005)
Pulmonary function No significant differences in FEV1 or FVC between the groups at any time point throughout the study
Bacterial burden In the gentamicin group ,13/27 (48.1%) patients infected with P. aeruginosa at baseline. Four of these patients (30.8%) achieved eradication at 12 months
Daily symptoms At end of month 12, the gentamicin group achieved a clinically significant improvement in LCQ vs saline (81.4% vs. 20%, p<0.01) and also in SGRQ (87.5% vs. 19.2%, p<0.004), respectively. Effect was only sustained at follow-up for the SGRQ score
Safety Gentamicin: Two non-treatment-related deaths occurred; two patients discontinued owing to being unable to tolerate treatment; seven of 32 patients (21.9%) had bronchospasms and received adjunctive treatment
Saline: Two of 33 (6%) patients had bronchospasms and received adjunctive treatment. Both discontinued treatment
LCQ: Leicester Cough Questionnaire; SGRQ: St George’s Respiratory Questionnaire
Murray MP et al. Am J Respir Crit Care Med 2011;183:491
2014-02-10
Additional trials for Colistin, Tobramycin and aztreonam inconclusive
Trials with inhaled ciprofloxacin, tobramycin and colistin ongoing
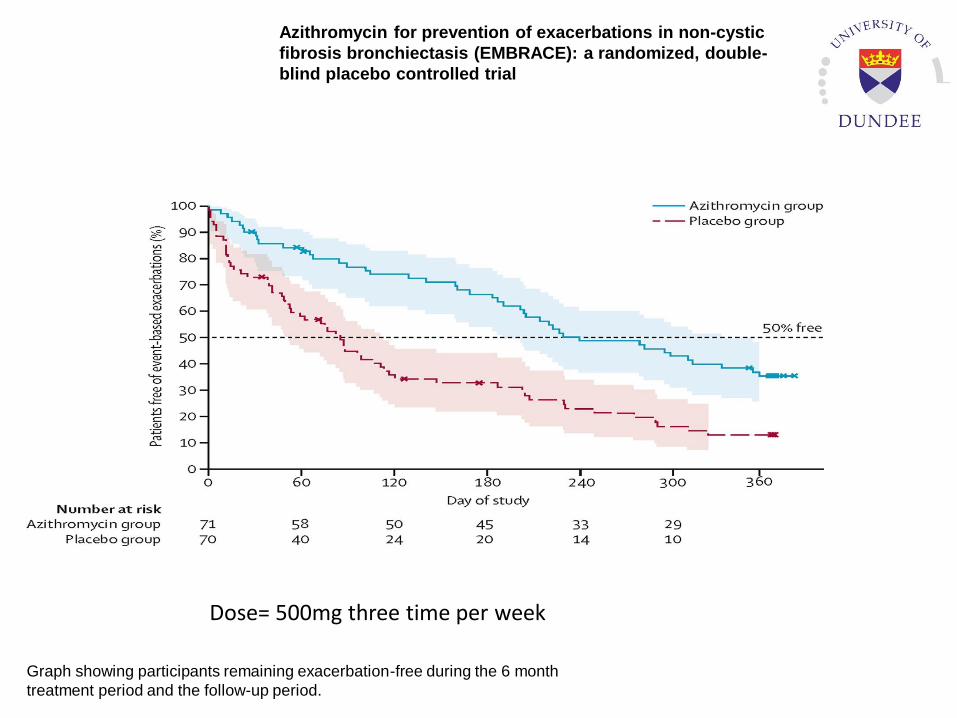
Graph showing participants remaining exacerbation-free during the 6 month
treatment period and the follow-up period.
Azithromycin for prevention of exacerbations in non-cystic
fibrosis bronchiectasis (EMBRACE): a randomized, double-
blind placebo controlled trial
Dose= 500mg three time per week
Participants from 40 countries
232 registered centres
TARGET:
•1000 patients by April 2016
•10,000 patients by March 2020
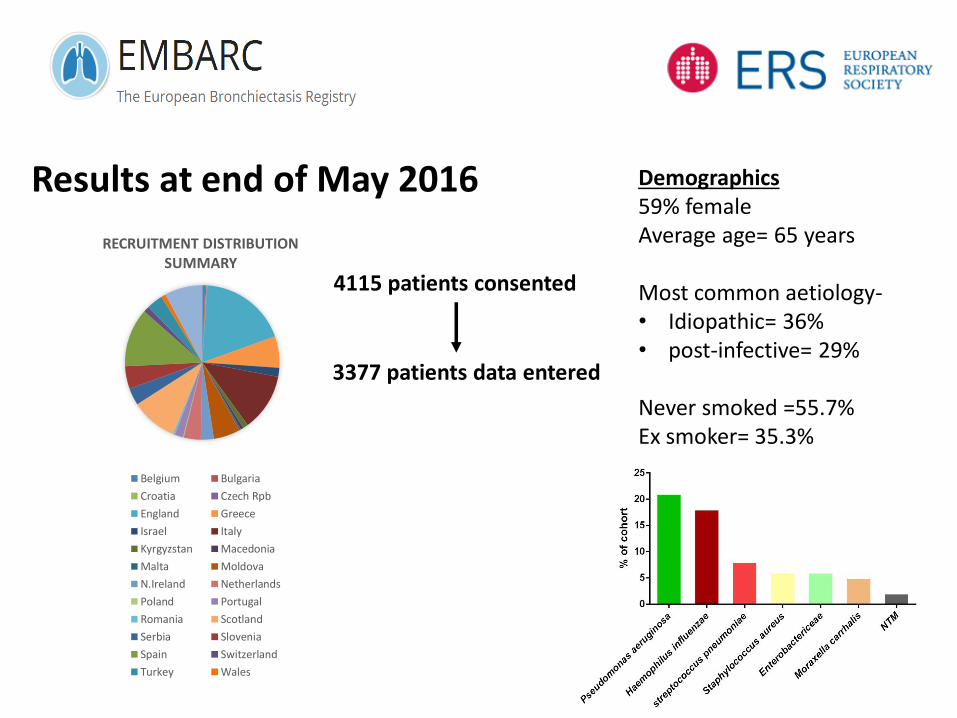
Results at end of May 2016
3377 patients data entered
Demographics59% femaleAverage age= 65 years
Most common aetiology-• Idiopathic= 36%• post-infective= 29%
Never smoked =55.7%Ex smoker= 35.3%
RECRUITMENT DISTRIBUTION SUMMARY
Belgium Bulgaria
Croatia Czech Rpb
England Greece
Israel Italy
Kyrgyzstan Macedonia
Malta Moldova
N.Ireland Netherlands
Poland Portugal
Romania Scotland
Serbia Slovenia
Spain Switzerland
Turkey Wales
4115 patients consented
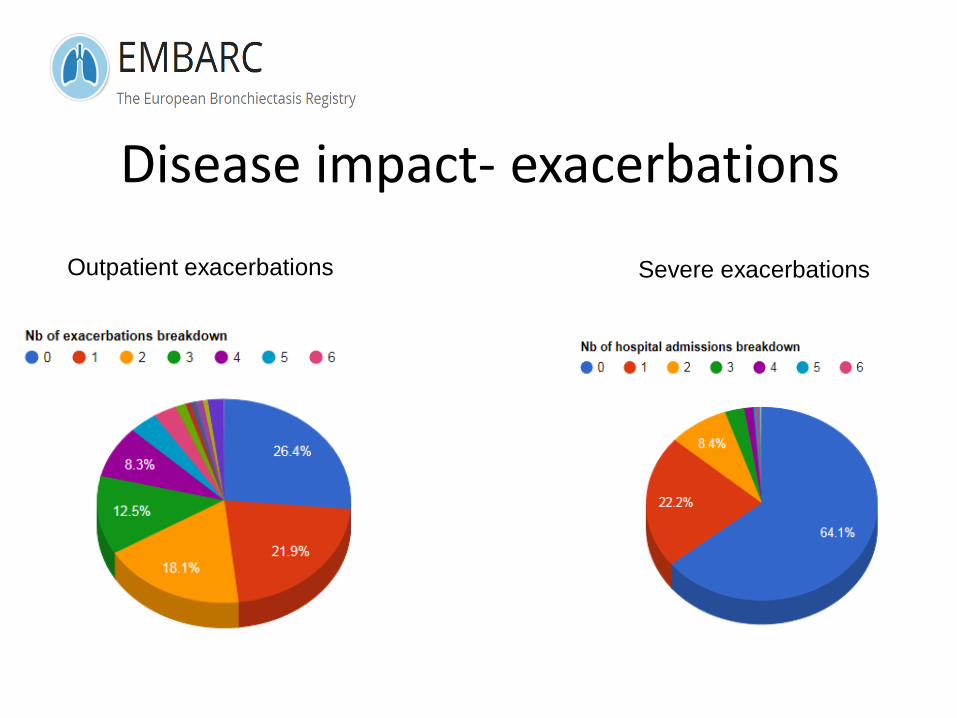
Disease impact- exacerbations
Outpatient exacerbations Severe exacerbations
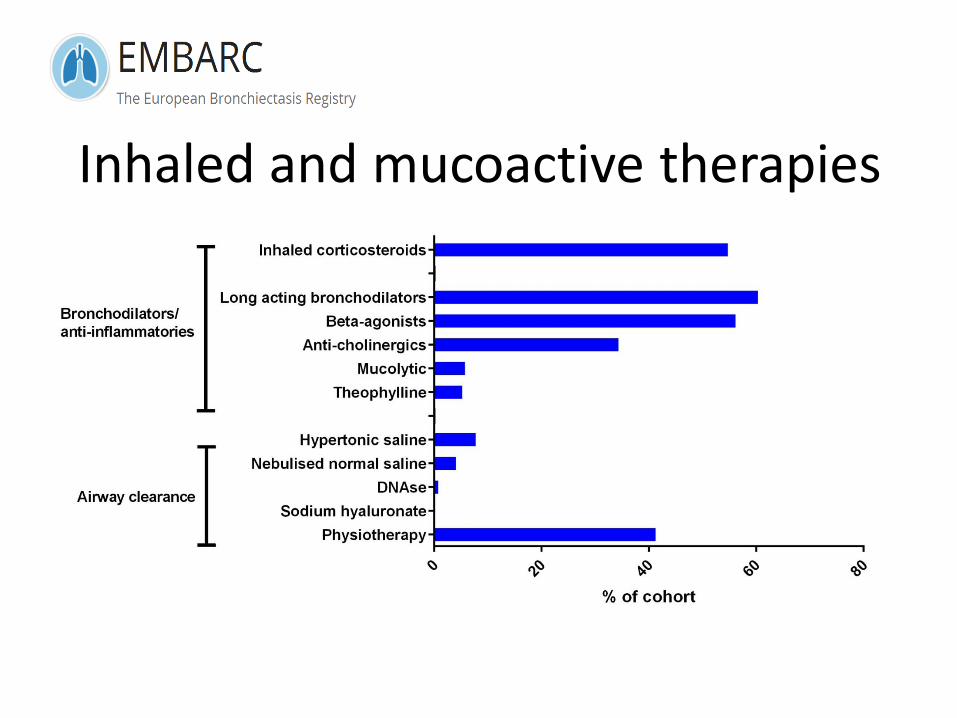
Inhaled and mucoactive therapies
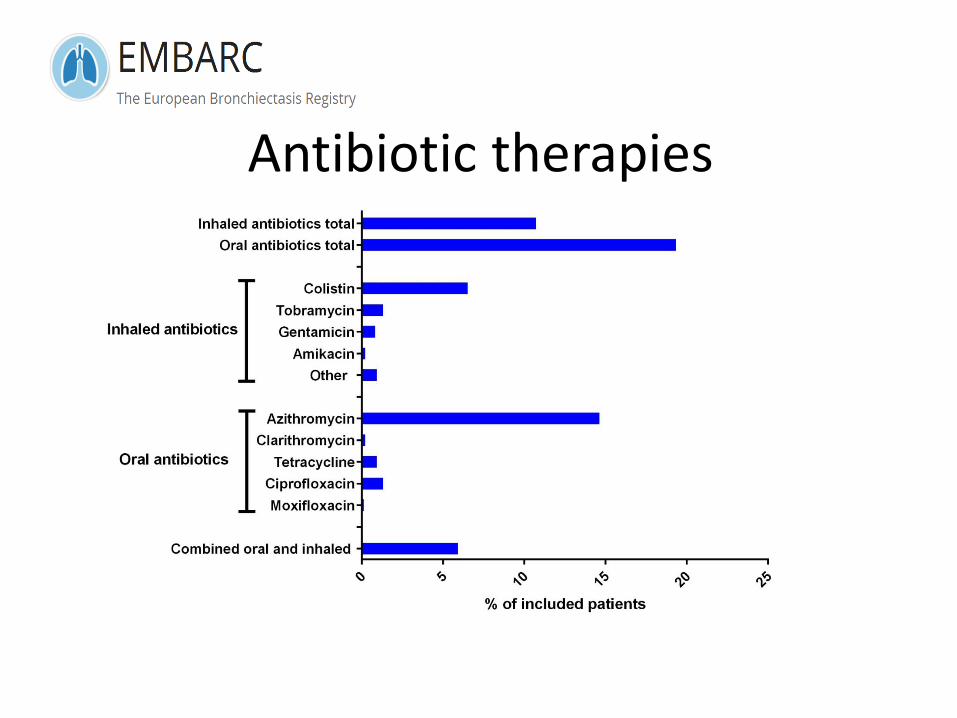
Antibiotic therapies
Summary
• Bronchiectasis is driven by neutrophilic inflammation and bacterial infection
• The most effective therapies are chest clearance and prophylactic oral and inhaled antibiotics for severe patients.
• Current data suggests in much of Europe bronchiectasis is treated “like COPD” and there remains are high burden of disease

Acknowledgements
www.bronchiectasis.eu
Executive groupEva PolverinoStefano Aliberti
iABC co-ordinatorStuart Elborn
Steering committeeFrancesco BlasiDiana BiltonWim BoermaAnthony De SoyzaKaterina DimakouMichael LoebingerCharlie HaworthAdam HillRosario MenendezMarlene MurrisFelix RingshausenAntoni TorresMontserrat VendrellTobias WelteRobert Wilson
ELFSarah MasefieldPippa PowellPatient advisory grp.
Advisory groupTim AksamitAnne O’DonnellCharles FeldmanOscar RizzoLucy Morgan
National leadsDaiana StolzMichal SchteinbergVictor BotnaruCharlotte UlrikMenno van EerdenGernot Rohde Branislava MilenkovicPerluigi Paggiaro
Study co-ordinatorMegan Crichton