bringing the “power” to cerner's powerchart for antimicrobial
TRANSCRIPT
C L I N I C A L P R A C T I C E I N V I T E D A R T I C L EEllie J. C. Goldstein, Section Editor
Bringing the “Power” to Cerner’s PowerChart forAntimicrobial Stewardship
Jason M. Pogue,1,2 Brian A. Potoski,3,4 Michael Postelnick,5 Ryan P. Mynatt,6 David P. Trupiano,7 Gregory A. Eschenauer,8
and Keith S. Kaye9
1Department of Pharmacy Services, Sinai-Grace Hospital, Detroit Medical Center, and 2Wayne State University School of Medicine, Detroit, Michigan;3Antibiotic Management Program, UPMC Presbyterian Hospital, and 4University of Pittsburgh School of Pharmacy, Pennsylvania; 5Department ofPharmacy, Northwestern Memorial Hospital, Chicago, Illinois; 6Department of Pharmacy Services, Detroit Receiving Hospital, Detroit Medical Center,7Department of Pharmacy, Detroit Medical Center, 8University of Michigan Health System and College of Pharmacy, and 9Infection Prevention,Epidemiology and Antimicrobial Stewardship, Detroit Medical Center and Wayne State University, Detroit, Michigan
The electronic medical record (EMR) has huge potential for facilitating antimicrobial stewardship efforts by di-recting providers to preferred antimicrobials. Cerner PowerChart currently holds the number 2 position in theEMR market. Although PowerChart has limited “out of the box” functionalities to optimize stewardship efforts,there are many potential utilities that can be developed to assist in stewardship practice. However, to harness thestewardship potential of the EMR system, significant hospital information technology resources are needed. Here-in we describe the experiences of 3 large healthcare systems utilizing Cerner to facilitate prior authorization ofantimicrobials, prospective audit and feedback of antimicrobials, and supplemental stewardship strategies.
Keywords. antibiotic stewardship; EMR; Cerner; PowerChart; CPOE.
Recently, Kullar et al discussed the role of the currentelectronic medical record (EMR) leader, Epic, in antimi-crobial stewardship [1]. The authors described the use ofEMR systems in stewardship efforts and the role of add-on systems such as Theradoc and Medmined that areprovided by third-party vendors. Kullar et al also high-lighted various tools, such as iVents and Navigator andBest Practice Alerts, provided by Epic to optimize Anti-microbial Stewardship programs [1]. Currently, Cerner(Kansas City, Missouri), maker of Cerner PowerChart,holds the number 2 position in the EMR market [2].
Early versions of the Cerner system provided little “outof the box” utility for antimicrobial stewardship, whichcreated opportunities for third-party vendors [1]. Thesethird-party vendor systems addressed some functionality
limitations of Cerner with regard to stewardship. Overtime, the potential utility of the Cerner software for anti-microbial stewardship has improved, although local in-formation technology resources are required to unleashthis utility. We describe utilization of Cerner for antimi-crobial stewardship at 3 large healthcare systems, North-western Memorial Hospital (NMH), Detroit MedicalCenter (DMC), and University of Pittsburgh MedicalCenter (UPMC) to demonstrate capabilities of the plat-form that other institutions with Cerner EMR can utilizeto facilitate stewardship efforts at their hospitals.
FACILITATING FORMULARYRESTRICTION AND PRIORAUTHORIZATION
One of the 2 core strategies of antimicrobial stewardshipis formulary restriction and preauthorization [3]. Thisstrategy focuses on providers obtaining approval, priorto antimicrobial dispensation. Cerner provides excellentfunctionality to facilitate the preapproval process, aslong as institutional information technology (IT) re-sources are available in terms of personnel and theirtime to build this functionality. Below we describe how2 large healthcare facilities utilize this functionality.
Received 22 January 2014; accepted 10 April 2014; electronically published 18April 2014.
Correspondence: Jason M. Pogue, PharmD, BCPS-ID, Infectious Diseases, Sinai-Grace Hospital, Detroit Medical Center, 6071 W Outer Dr, Detroit, MI 48235([email protected]).
Clinical Infectious Diseases 2014;59(3):416–24© The Author 2014. Published by Oxford University Press on behalf of the InfectiousDiseases Society of America. All rights reserved. For Permissions, please e-mail:[email protected]: 10.1093/cid/ciu271
416 • CID 2014:59 (1 August) • CLINICAL PRACTICE
Downloaded from https://academic.oup.com/cid/article-abstract/59/3/416/2895325by gueston 11 April 2018

Criteria Monitored DrugsThe DMC has successfully used the criteria-monitored drug(CMD) system (Figure 1) since 1987 [4]. The CMD processhas 2 tiers of restriction for antimicrobials. The first is for agentsthat require infectious diseases approval and appropriate criteriafor use prior to dispensing (eg, carbapenems, daptomycin, mica-fungin). For second-tier restricted agents (eg, fluoroquinolones),only clinical criteria, predefined by the Antimicrobial Subcom-mittee, are needed for the agent to be dispensed. For tier 2 anti-microbials, prescribers have the ability to override criteria.
This CMD process is facilitated in an automated formatthrough computerized prescriber order-entry (CPOE). Current-ly, DMC utilizes an automated prompt when a restricted anti-microbial is ordered, requiring the prescriber to select one of thepredefined criteria, or to select “Other–pharmacy to contactme” option prior to the routing of the order to pharmacy forverification. The verifying pharmacist determines whether ornot criteria were met, and if applicable, whether infectious dis-eases approval was obtained and documented. The verifyingpharmacist can then complete the documentation process, se-lecting 1 of 4 predetermined options (approved by monitoringservice, attending physician override, changed on follow-up,and meets criteria) and document other pertinent information.
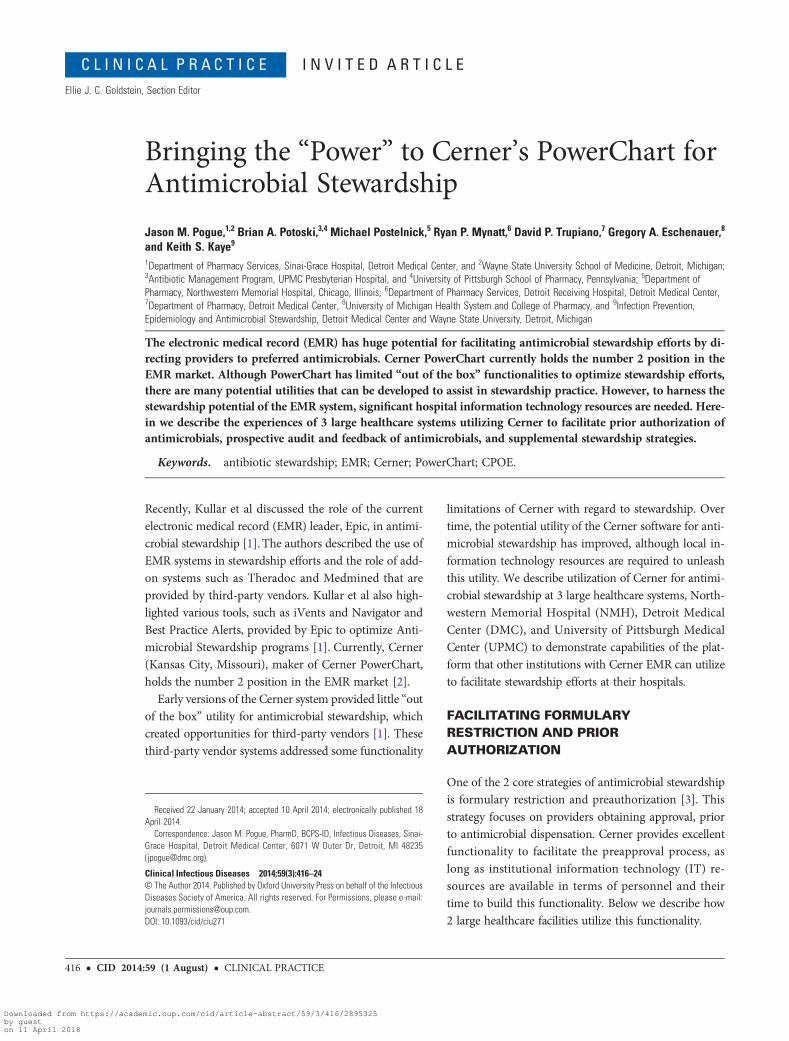
Cerner Special Instructions ApprovalAt UPMC, when a restricted antibiotic is ordered, a “pop-up”screen fires (Figure 2A), reminds the ordering physician ofthe level of prior authorization needed for the chosen antimi-crobial, and provides directions on how to obtain the agent. Ad-ditionally, a specific field within the order itself can be used forrecording an approval code documenting approval by the stew-ardship team. An order entry pharmacist subsequently verifiesthe order provided (Figure 2B). If the process is not followed,the pharmacist can page the provider to convey that the antimi-crobial requires approval.
Whereas these processes at DMC and UPMC facilitate com-pliance with restriction policies, they are not without limita-tions. Ultimately, restriction is dependent upon the verifyingpharmacist’s assessment of the medication order and/or theCMD form, as well as the amount and quality of documentationpresent. If the pharmacist fails to properly assess the necessaryapproval process components, the stewardship process can fail.
FACILITATING PROSPECTIVE AUDIT ANDFEEDBACK
Prospective audit of antimicrobial use with intervention andfeedback is the other core stewardship strategy [3], and focuseson real-time follow-up by the stewardship team with the provi-sion of recommendations to the prescribers. Although Cerneroffers some utility with regards to prospective audit and feed-back (see below), its capabilities are limited. Third-party ven-dors offer more effective processes to identify patients forwhom targeted interventions are appropriate (eg, patientswho have organism–drug mismatches, patients on broad-spectrum antibiotics with isolates susceptible to narrower-spectrum therapies). Utilization of Cerner alone for prospectiveaudit and feedback may result in inefficiencies (eg, stewardshippersonnel spending time on patients for whom intervention isnot needed) and might not identify patients who could mostbenefit from stewardship intervention.
InfoView Reports for Patient IdentificationWith institutional IT support, InfoView reports can be createdlisting each patient who is receiving antimicrobial therapy, andthe number of days of therapy received (Figure 3A). Unfortu-nately, this information does not help to identify which patientsrequire intervention (ie, does not evaluate the appropriatenessof prescribed antimicrobials). However, when institutions donot have electronic data capture systems to identify patients
Figure 1. The criteria-monitored drug form.
CLINICAL PRACTICE • CID 2014:59 (1 August) • 417
Downloaded from https://academic.oup.com/cid/article-abstract/59/3/416/2895325by gueston 11 April 2018
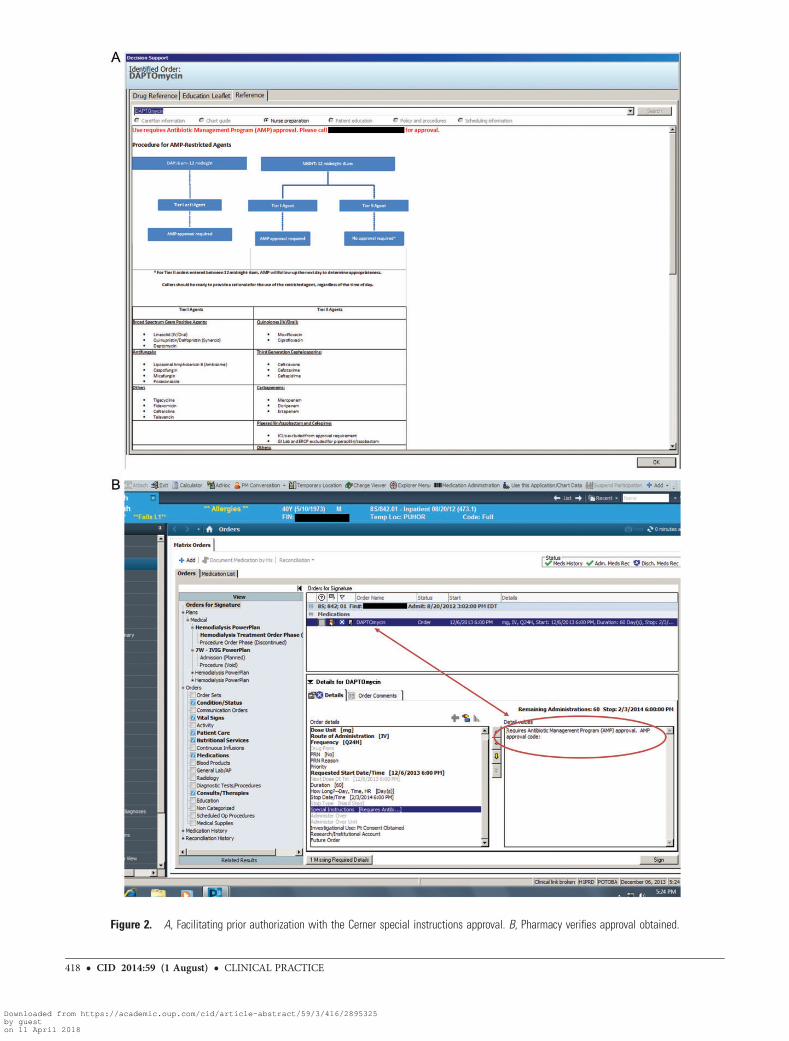
Figure 2. A, Facilitating prior authorization with the Cerner special instructions approval. B, Pharmacy verifies approval obtained.
418 • CID 2014:59 (1 August) • CLINICAL PRACTICE
Downloaded from https://academic.oup.com/cid/article-abstract/59/3/416/2895325by gueston 11 April 2018
for interventions, this Cerner functionality can serve as a start-ing point for identification of patients for intervention. Info-View reports can also be designed to identify all patients onan intravenous formulation of antimicrobials that possess excel-lent bioavailability and who are taking other medications orally(Figure 3B), facilitating intravenous to oral conversion. Thiscan be important “low-hanging fruit” for newer stewardshipprograms, or those programs with limited personnel resources.The active list antibiotic report took 30–40 hours to build,whereas the intravenous to oral report took between 8 and16 hours.
mPage CapabilitiesCerner mPages are essentially web pages supported by EMRdata. They utilize common web technologies (HTML and Java-Script) to create a customizable view that can be tailored to aninstitution’s need. At DMC, an antimicrobial stewardshipmPage, “Stew View” (Figure 4), focuses on the informationthat stewardship or infectious diseases personnel need tomake informed antimicrobial-related decisions. Once a patientis identified, all antimicrobial orders for the current admission,antimicrobials administered within the previous 90 days, cul-ture data from the current admission as well as for the previous
Figure 3. A, Patients in the hospital currently on antibiotics. B, Intravenous to oral eligible patients.
CLINICAL PRACTICE • CID 2014:59 (1 August) • 419
Downloaded from https://academic.oup.com/cid/article-abstract/59/3/416/2895325by gueston 11 April 2018

year, serology data, serum drug concentrations (vancomycin,aminoglycosides), and relevant laboratory values, vital signs,heights, and weights are displayed. Importantly, this display in-cludes all antimicrobials ordered, and not only those adminis-tered. The electronic medication administration record would
need to be referenced to review doses administered. This fo-cused display allows stewardship personnel to quickly scan rel-evant parts of the medical record to facilitate antimicrobial drugand dose optimization. Although this functionality is robust, itrequires significant IT resources. In addition to the planning
Figure 4. “Stew View.”
420 • CID 2014:59 (1 August) • CLINICAL PRACTICE
Downloaded from https://academic.oup.com/cid/article-abstract/59/3/416/2895325by gueston 11 April 2018
phase, building Stew View took an estimated 160–320 IT hours.Furthermore, it is useful only after the stewardship team hasidentified a patient for intervention.
FACILITATING SUPPLEMENTARYSTEWARDSHIP METHODS
The Infectious Diseases Society of America guidelines recom-mend a series of supplementary techniques to enhance the in-stitutional stewardship program [3], including education,guideline, and pathway utilization, de-escalation, and dose op-timization. These supplementary techniques are perhaps whereCerner offers its best functionality.
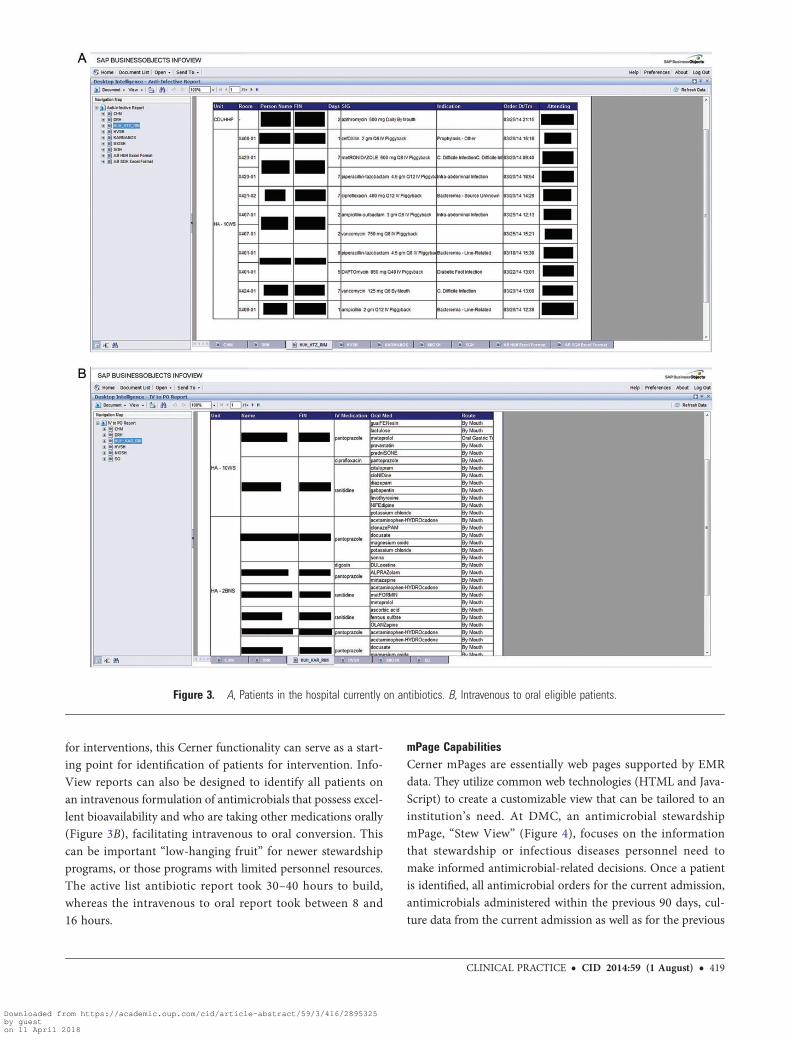
Antibiotic IndicationsOne impressive feature within Cerner that cannot be met withthird-party vendors is the ability to capture antibiotic
indications within the system (Figure 5). At Northwestern,problems tracking compliance with surgical care improvementproject indicators provided the impetus for development of acomprehensive, real-time antibiotic indication documentationrequirement within the Cerner medication ordering process.A list of 51 antibiotic indications was created by the Antimicro-bial Subcommittee as a drop-down field. An indication was re-quired to be completed during CPOE by the ordering physician.Indications are organized by organ system and/or defined bycommon clinical syndromes such as genitourinary (GU)–pyelo-nephritis and GU-prostatitis. There is also an “other” optionthat allows the clinician to free text an indication for infrequentscenarios. This method provides an easy-to-navigate list, whereindications for all antimicrobial orders are documented. Thesedata provided facilitate audits for appropriate empiric antibioticchoice and duration of therapy by antibiotic indication. The in-dication is not modified during the course of therapy. Shortly
Figure 5. Antibiotic indication field.
CLINICAL PRACTICE • CID 2014:59 (1 August) • 421
Downloaded from https://academic.oup.com/cid/article-abstract/59/3/416/2895325by gueston 11 April 2018

after implementation, the investigators evaluated the accuracyof entered indications by auditing a representative sample ofantimicrobial orders in a single month. The audit demonstrat-ed 100% accuracy of documentation for surgical prophylaxisorders and 86% accuracy for empiric orders [5]. Practitionersat NMH are comfortable utilizing the indication data to auditantimicrobial utilization, which allows the stewardship teamto identify problem areas with regards to appropriate utiliza-tion of empiric and prophylactic antimicrobial utilization. Theindication data have little impact on de-escalation. It took ap-proximately 40 IT hours to design and implement this feature.Systemwide education geared toward providers about the ra-tionale for adding these indications and directions for com-pleting the indication process also takes multidisciplinarycollaboration. At our institutions, sessions targeted to theinternal medicine, emergency medicine, and surgical groupsfocused on clinical indication education and process, andinformation.
Order Sets and PowerPlansIntegrated disease-specific order sets are well-characterizedtools to achieve consistency in practice for common infectionssuch as community-acquired and ventilator-associated pneu-monia and Clostridium difficile infection [6–8]. These ordersets can also be made to be flexible and thus also useful for un-common scenarios or indications. The advantage of CPOE (vspaper) systems is that order sets can be customized to the needsof the creating institution.
Ethanol Lock Order SetAt UPMC an order set was developed for ethanol lock therapy,which involves instilling an ethanol solution into an intravenouscatheter and allowing it to dwell for a period of time to preventcatheter-related bloodstream infections [9]. Ethanol lock thera-py has been increasingly recommended and prescribed atUPMC. Each time a prescriber wished to use this therapy, sig-nificant stewardship resources were devoted to assure that
Figure 6. Use of toolbars.
422 • CID 2014:59 (1 August) • CLINICAL PRACTICE
Downloaded from https://academic.oup.com/cid/article-abstract/59/3/416/2895325by gueston 11 April 2018

processes were appropriately performed. To facilitate these or-ders, a CPOE ethanol lock order set was developed with dose,volume, route (affected catheter), dwell time, and special con-cerns (such as the need to verify catheter compatibility with eth-anol) autopopulated in the form. Since CPOE queries forethanol lock have been directed to this order set, compliancehas been excellent. Similar order sets have also been implement-ed for antibiotic lock therapies.
Improving ConsistencyWith Inhaled Antimicrobials ThroughOrder SetsGiven the large cystic fibrosis and lung transplant patient pop-ulation at UPMC, there is significant use of aerosolized antibi-otics and antifungals. However, given the sparse literature onaerosolized antibiotic indications and dosage, patients with sim-ilar indications might be prescribed discrepant dosages, with re-sultant confusion among clinicians and extra work forpharmacy in terms of preparation. As such, drug-specific aero-solized antibiotic order sets were created which standardize dos-ages as well as clinical indications.
Phased PowerPlansThe utility of order sets has been demonstrated previously, andhistorically, preprinted order sets were utilized prior to CPOE.However, within Cerner, the employment of the “phasedPowerPlan” has many characteristics that differ from a typicalorder set. A PowerPlan, unlike a historical order set, is designedwith single or multiple stages (or “phases”). Each of these phas-es can be designed to enter a “planned” status. In this plannedstatus, orders within the phase are signed and ready to be exe-cuted; however, the orders do not appear in their respective de-partments (pharmacy, lab, etc) or generate nursing tasks untilthe plan is “initiated.” Plans can be initiated by preidentifiedhealthcare personnel (ie, a nurse, pharmacist, physician assis-tant, or physician). This system allows for strategic applicationin areas where flexibility in start times of antimicrobials isdesired.
To streamline a complicated process at DMC, phased Power-Plans have been utilized for roughly 2 years for penicillin desen-sitization. Prescribers begin by searching the order catalog forthe appropriate desensitization plan (eg, “Penicillin Desensiti-zation”), as they would for any other order. Once the appropri-ate desensitization plan is chosen, the physician is prompted foran estimated start time. It is important to note that this is onlyan estimated start time, and the entire plan can be “resched-uled” at any point before the plan is fully initiated. Once theplan is signed, the first phase begins. During the first phase ofthe PowerPlan, a notification that desensitization is taking placeis routed to pharmacy, initiating the communication processbetween prescriber, nursing, and pharmacy. It is important tonote that the PowerPlan itself has no communication orders
to discuss these specific steps to be undertaken, but rather it fa-cilitates communication, which occurs usually in the form of aphone call or face-to-face discussion, between the involved par-ties. Also, once the plan is initiated, the second phase of the planmoves into a “planned” status. In this second phase, all the ap-propriate timings and doses of penicillin are predefined (ie, the14-dose desensitization schedule at 15-minute intervals). Afterclarification that the estimated start time is deemed to be appro-priate, the pharmacist, nurse, or physician then initiates the sec-ond phase of the plan. Once initiated, the orders from thesecond phase are activated and routed to the necessary health-care personnel (ie, nursing, pharmacy, etc). Timing of all dosesand orders are automatically calculated relative to the estimatedstart time of the initial dose. If the start time is not feasible (eg,due to a 1:1 nursing to patient ratio not being available), theplan will remain in the planned stage until the second phaseis initiated. Once this phase of the plan is initiated, all of thesubsequent start times will be automatically calculated and up-dated. Because timing delays can compromise the entire desen-sitization process, PowerPlans have the ability to significantlyimprove patient care. Additionally, in standardizing the desen-sitization process, significant stewardship resources (time) donot need to be spent reinventing the wheel every time the pro-cess is needed for patient care. Since implementation of thePowerPlan for desensitization, the stewardship team has target-ed other areas where ordering and timing of antibiotic admin-istrations is complex. We are currently targeting perioperativeantimicrobial prescribing where start times for procedures aredynamic and contingent on multiple factors.
Order sets and PowerPlans offer the ability to both ensurecompliance with stewardship recommendations and allow flex-ibility for prescribing practices, but there are significant limita-tions. First and foremost is the significant time commitmentneeded for both the development of the order sets and Power-Plans, as well as for education regarding how the process worksfor all involved parties (eg, nursing, physicians, and pharmacy).In addition to the time for education, the development of ordersets and PowerPlans can take anywhere from 2–3 hours to 80–100 hours to design, depending on the degree of complexity andthe number of different providers who need to be involved. Thedesensitization protocol described above took approximately 80hours to build, due to the complexities pertaining to the variousdilutions needed for the 14-dose protocol. Unfortunately, de-spite education, it can be difficult to convince providers to con-sistently use order sets, particularly if they have alreadydeveloped their own processes for managing common clinicalscenarios.
Dose Range CheckA safety feature that is included in the standard Cerner applica-tion is the dose range check. This function uses predefined dose
CLINICAL PRACTICE • CID 2014:59 (1 August) • 423
Downloaded from https://academic.oup.com/cid/article-abstract/59/3/416/2895325by gueston 11 April 2018

ranges to inform the prescriber and verifying pharmacist, in theform of a pop-up window, if an entered dose is out of range. Thepharmacist, after investigation, can either suppress the alert orcontact the prescriber and recommend an alternative dose. Themain limitation with this check is that the Cerner dose rangesmay conflict with local dosing guidelines, resulting in confusionamong prescribers, who may act on an alert, and verifying phar-macists, who are educated to dose per institutional guidelines.However, the ranges are modifiable for any drug and take aminimal amount of time (5–10 minutes per drug) to change.
Promoting Education Through ToolbarsA number of potential tools exist that enable the stewardshipteam to assist in both provider education and the disseminationof clinical pathways. An example of these tools are the toolbarlinks (Figure 6) such as the “print on demand” function, whichat UPMC links to the institution’s annual Guide to Antimicro-bial Chemotherapy. Although this pocket guide is printed anddistributed annually to all providers, this real-time automatedfunctionality provides information redundancy. It also servesas a passive mechanism for drug and dose selection, as theguide provides a comprehensive resource regarding formularyagents, institution-endorsed first-line and alternative agentsby indication, antibiogram data, and dosing across the renalfunction spectrum. Even if individual institutions do not havea similar comprehensive resource like the aforementionedguide, this functionality can still provide a link to any documentor series of documents deemed relevant to antimicrobial stew-ardship including guidelines, pathways, or antibiogram data.
Summary and LimitationsCerner has made significant advancements in its functionalityto promote institutional stewardship. Unfortunately, at the pre-sent time, little of this functionality is readily available in an“out of the box” format, and significant information technologyinvestments from the individual institution are required to har-ness much of the functionality. Cerner does not currently em-ploy dedicated stewardship personnel, although the companyhas described an interest in focusing more toward antimicrobialstewardship in the future. On the plus side, the functionality de-scribed in this manuscript allows an institution to create anylogic they want, provided the resources are available. Addition-ally, these processes only function in the classical scenario of aprescriber entering an order in the EMR and a pharmacist
subsequently checking the order. Increasingly, pharmacistsrounding with medical teams are placing orders themselves di-rectly into the “pharmacy side” of the EMR system, potentiallybypassing stewardship mechanisms. From a stewardship pro-spective, the biggest limitation of the current Cerner function-ality is that it fails to effectively identify appropriate patients forantimicrobial-related follow-up and interventions.
As rates of multidrug-resistant organisms continue to rise inboth the hospital and the community, so will the need for em-piric broad-spectrum therapy. For these reasons, the success ofstewardship is largely driven by prospective audit and feedbackto identify opportunities for antimicrobial de-escalation anddiscontinuation. Until Cerner prioritizes development of func-tionality to identify patients in “real time” who can benefit fromreview and intervention by stewardship personnel, the need forthird-party vendors outside of the Cerner system will continue.
Note
Potential conflicts of interest. All authors: No reported conflicts.All authors have submitted the ICMJE Form for Disclosure of Potential
Conflicts of Interest. Conflicts that the editors consider relevant to the con-tent of the manuscript have been disclosed.
References
1. Kullar R, Goff DA, Schulz LT, Fox BC, Rose WE. The “epic” challenge ofoptimizing antimicrobial stewardship: the role of electronic medical re-cords and technology. Clin Infect Dis 2013; 57:1005–13.
2. Buckley C. Clinical market share: More than meaningful use. Available at:www.klausresearch.com. Accessed 28 October 2013.
3. Dellit TH, Owens RC, McGowan JE Jr, et al. Infectious Diseases Societyof America and the Society for Healthcare Epidemiology of Americaguidelines for developing an institutional program to enhance antimicro-bial stewardship. Clin Infect Dis 2007; 44:159–77.
4. Berman JR, Zaran FK, Rybak MJ. Pharmacy-based antimicrobial-moni-toring service. Am J Hosp Pharm 1992; 49:1701–6.
5. Patel JA, Esterly JS, Scheetz MH, Postelnick MJ. An analysis of the accu-racy of physician-entered indications on computerized antimicrobial or-ders. Infect Control Hosp Epidemiol 2012; 33:1066–7.
6. Fleming NS, Ogola G, Ballard DJ. Implementing a standardized order setfor community-acquired pneumonia: impact on mortality and cost. JtComm J Qual Patient Saf 2009; 35:414–21.
7. Paterson DL. The role of antimicrobial management programs in opti-mizing antibiotic prescribing within hospitals. Clin Infect Dis 2006;42:S90–5.
8. Owens RC Jr. Antimicrobial stewardship: concepts and strategies in the21st century. Diagn Microbiol Infect Dis 2008; 61:110–28.
9. Maiefski M, Rupp ME, Hermsen ED. Ethanol lock technique: review ofthe literature. Infect Control Hosp Epidemiol 2009; 30:1096–108.
424 • CID 2014:59 (1 August) • CLINICAL PRACTICE
Downloaded from https://academic.oup.com/cid/article-abstract/59/3/416/2895325by gueston 11 April 2018