bringing pharmacogenomics into clinical practice: the why ...€¦ · bringing pharmacogenomics...
TRANSCRIPT

Bringing Pharmacogenomics into Clinical Practice:
The Why, When and How
Laura Chadwick, PharmD Clinical Specialist
Boston Children’s Hospital [email protected]
6/22/2017

How often do you apply pharmacogenomics in your area of
practice?
A. Frequently
B. Sometimes
C. Rarely
D. Never

How comfortable are you with applying pharmacogenomic results in
clinical decision making?
A. Very
B. Somewhat
C. Not comfortable at all

Today's Objectives
• Describe the science of pharmacogenomics and how it applies to clinical practice
• Identify genetic variant effects as pharmacokinetic, pharmacodynamics or immunologic
• Recognize therapeutic modification based on published guidelines and available pharmacogenomics results
• Express methods for incorporating pharmacogenomics into clinical practice and describe challenges faced in doing so

What is “Pharmacogenomics” or PGx?
• Study of genetic changes impacting proteins involved in drug metabolism, action and response
– Personalized medicine
– Precision medicine
– Targeted therapy

What is the goal of PGx?
Image: http://www.pharmainfo.net/reviews/role-pharmacogenomics-drug-development

What is the goal of PGx?
• Benefits of clinical implementation:
– Reduction of adverse drug events (ADEs)
• 2 million per year in the US alone
• 100,000 deaths
• 6% of hospital admissions
• $20.6 billion per year
– Improved drug efficacy and outcomes
– Salvaging drugs with high toxicity profiles
– Improved adherence

Clinical Use of Pharmacogenomics
• Pre-emptive testing not currently in wide use
– Teaching/university hospitals, cancer centers
– Limited by time, funding, policy development
• Clinical Pharmacogenomics Implementation Consortium (CPIC)
– Published Level I evidence dosing guidelines
– Key limitation: Does not address who should be tested

PGx Resources • Homepage: www.pharmgkb.org
Search Drug or Gene
CPIC GUIDELINES
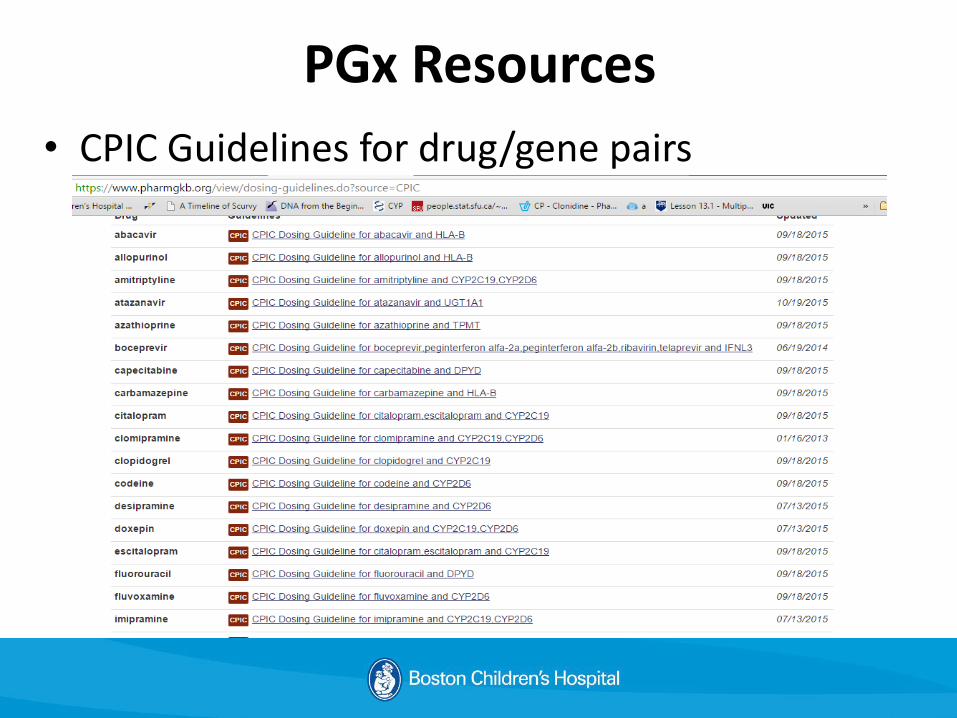
PGx Resources
• CPIC Guidelines for drug/gene pairs

PGx: Genetic Testing & Results • Testing options
– Next Generation Sequencing
– Targeted sequencing of regions of interest
– SNP-based panels
• Variant forms
– IN/DELs
– SNPs
– Duplication
• Defining variants
– RS ID
– Star alleles haplotypes
• Associated protein expression/enzyme activity level
Image source: http://uvmgg.wikia.com/wiki/SNP

PGx at BCH
• Clinical Pharmacogenomics Services
– Inpatient service & outpatient clinic
• Referrals from providers at BCH and neighboring institutions
• Adult and pediatric patients with history of adverse drug events or non-response
• 2 appointment structure – Visit 1: patient PMH, review of testing information and
limitations
– Visit 2: result return
– InforMED Kids Research Study

PGx at BCH
• SNP based panel
– Affymetrix DMET Plus: 225 genes
– Pros:
• Detect major common variants
• Limited incidental findings
– Cons:
• Miss rare variants
• Genes of interest possibly unavailable

PGx at BCH
• Return of results to the EHR problem list
• Alerts firing for variants of clinical significance

PGx: Protein Effects
• Pharmacokinetic (PK)
– ADME
• Drug metabolism: CYP enzymes, TPMT, NAT2
• Drug transport: SLCO1B1, ABCG2
• Pharmacodynamic (PD)
– Drug targets: VKORC1, HER2, CFTR
• Immunologic
– Drug allergies: HLAs

PGx: PK
Enzyme Expression
[Parent Drug]
Active Parent Drug
Pro-drug
↑ ↓
↓ ↑
Image: http://www.gbhealthwatch.com/Trait-Beta-Blocker-Response.php

PGx: PK of Codeine
• Which certain children are affected?

• Metabolism
– Pro-drug
– Primary pathway: CYP2D6
PGx: PK of Codeine
Image: http://www.pharmgkb.org

• CPIC Guidelines for Codeine Dosing
CYP2D9 Genotype CYP2D6 Metabolizer Phenotype
CPIC Codeine Recommendation
Gene Duplication (*1/*1XN)
Ultra-rapid Avoid due to toxicity
Homozygous Wild-Type (*1/*1)
Normal/Extensive Standard dosing
Heterozygous (*1/*2, *1/*3)
Intermediate Standard dosing
Homozygous Variant (*2/*2, *2,*3, *3/*3)
Poor Avoid due to lack of efficacy
PGx: PK of Codeine

PGx: Phenytoin Case • 10 yo male admitted for status epilepticus, treated
with:
– IV Fosphenytoin 18 mg PE/kg (500 mg PE) on presentation
– Single maintenance dose of 140 mg PE (5 mg PE/kg) five hours later on day 1 of the hospitalization
• PMH:
– Congenital hydrocephalus
– VP shunt
– Refractory epilepsy secondary to an in utero right MCA stroke

PGx: Phenytoin Case • On day 5 of his hospitalization
– Extremely lethargic
– Free Phenytoin level is high (Ref: 0.4 – 1.4 mcg/mL)
• Day 2: 3 mcg/mL
• Day 5: 1.4 mcg/mL
• No clinically relevant drug-drug interactions and his albumin is normal.
• What is a possible pharmacogenomic reason for the toxicity TB is experiencing?

PGx: Phenytoin Case • Fosphenytoin/Phenytoin toxicities
– Chronic effects associated with long-term use: • Hepatotoxicity • Osteoporosis • Megaloblastic anemia • Gingival hyperplasia • Hirsutism • Peripheral neuropathy
– Acute effects with toxic plasma concentrations • CNS effects (dizziness, confusion, drowsiness, and ataxia) • GI upset and nausea
– Immunologic reactions: • Severe cutaneous reactions (SJS, TEN)

PGx: Phenytoin Case • Fosphenytoin/Phenytoin metabolism
– Fosphenytoin Phenytoin via plasma esterases
– Phenytoin 90% metabolized by CYP2C9
• *2, *3 common loss of function alleles
– Non-linear saturatable kinetics
Image: http://www.pharmgkb.org

PGx: Phenytoin Case
TOXIC
THERAPEUTIC

PGx: Phenytoin Case
• Phenytoin Dosing Based on Genotype
CYP2C9
Metabolizer Status
Sample
Genotype(s)
Recommendation
Extensive
Metabolizer
*1/*1 Initiate therapy with recommended maintenance
dose.
Intermediate
Metabolizer
*1/*2, *1/*3 Consider 25% reduction of recommended
starting maintenance dose and adjust according
to therapeutic drug monitoring and response.
Poor Metabolizer *2/*2, *3/*3,
*2/*3
Consider 50% reduction of recommended
starting maintenance dose and adjust according
to therapeutic drug monitoring and response.

PGx : TPMT
Image: http://www.rxresource.org/prescription-information/Azathioprine-Mylan-Pharmaceuticals-Inc.html

PGx: TPMT
• Detoxifying pathway
– Decreased TPMT activity accumulation of toxic metabolites myelosuppression and neutropenia
– Alleles associated with decreased activity: *2,*3A, *3B, *3C, *4
– Prevalence of variants:
• ~89% of the population *1/*1
• ~11% heterozygous
• ~0.3% homozygous variant

PGx: TPMT
Phenotype (Genotype)
Examples of diplotypes
Implications for azathioprine pharmacologic measures
Dosing recommendations for azathioprine
Homozygous wild-type or normal, high activity
*1/*1 Lower concentrations of TGN metabolites
Start with normal starting dose (e.g., 2-3 mg/kg/d) and adjust doses of azathioprine based on disease-specific guidelines.
Heterozygote or intermediate activity
*1/*2, *1/*3A, *1/*3B, *1/*3C,
Moderate to high concentrations of TGN metabolites
If disease treatment normally starts at the "full dose", consider starting at 30-70% of target dose (e.g., 1-1.5 mg/kg/d), and titrate based on tolerance.
Homozygous variant or low activity
*3A/*3A, *2/*3A, *3C/*3A, *3C/*4,
Extremely high concentrations of TGN metabolites; fatal toxicity possible
Consider alternative agents or drastically reduced doses (reduce daily dose by 10-fold and dose thrice weekly instead of daily).
Image: http://www.pharmgkb.org

PGx: TPMT
• Defining Star Alleles PA166128346 7/24/2015 A80P Y240C A154TCPIC TMPT
Haplotype Set *Nucleotide change on gene per http://www.imh.liu.se/tpmtalleles/tabell-over-tpmt-alleler?l=en **Note that dbSNP reports G>A at this position: however the TPMT nomenclature committee has defined wildtype as having allele A at this position (positive chromosomal strand) and the *1S allele as having allele G at this position (positive chromosomal strand)238G>C* 719A>G* 460G>A* 626-1G>A*
TPMT TAG(S) rs1800462 rs1142345 rs1800460 rs1800584
*1 C T C C
*2 G
*3A C T
*3B T
*3C C
*4 T
Image: http://www.pharmgkb.org
PGx: Star Alleles Defined
• Which of the following star alleles corresponds with the genetic results descriped below:
– rs1800462 (C > G) C
– rs1142345 (T > C) C
– rs1800460 (C > T) C
– rs1800584 (C > T) C

PGx: Pediatric PK
Lu H, Rosenbaum S. Developmental pharmacokinetics in pediatric populations. J Pediatr Pharmacol Ther. 2014;19(4):262–276.

PGx: PK Summary Gene/Enzyme Drug(s)
CYP2C19 PPIs, TCAs, SSRIs, Clopidogrel
CYP2C9 Phenytoin, Celecoxib, Sulfonylureas, Warfarin
CYP2D6 SSRIs, TCAs, Codeine, Ondansetron, Tramadol, Oxycodone
TPMT 6-mercaptopurine, Azathioprine
CYP3A5 Tacrolimus
NAT2 Isoniazid
SLCO1B1 Statins
DPYD 5-Fluoruracil

PGx: PD
• Drug target variation: shape, amount
• May determine drug efficacy (i.e. Herceptin)
Image source:http://www.kadcyla.com/sites/kadcyla.com.patient/files/Normal-Vs_HER2Cell.png

PGx: Warfarin
• Review: warfarin MOA – Reduced Vit K required for coagulation factors II, VII, IX,
and X and Protein C & S – VKORC1 reduces Vit K – Warfarin inhibits subunit 1 of VKORC1 – S-warfarin = active isomer
• Highly variable dosing & narrow therapeutic index
– Age, height, weight – Race – Enzyme inducers & inducers – Drug-food interactions

PGx: Warfarin • Gene(s) of interest?
Image: http://pharmrev.aspetjournals.org/content/63/2/437/F3.expansion.html

PGx: Warfarin
• CYP2C9: primary metabolic pathway of S-warfarin
• VKORC1: S-warfarin drug target
– Common variant (−1639G>A, rs9923231)
• −1639A: less VKORC1 expressed
CYP2C9 Allele Metabolism Reduction
Implication at Standard Doses
*2 30-40% ↑ [S-warfarin] Over-anticoagulation
↑ INR & risk of bleeding *3 80-90%

PGx: Warfarin
• Warfarin starting dose by genotype
• Algorithms available: www.warfarindosing.org
– NOTE: NOT applicable for patients under 18 years old

PGx: Immunologic HLA
• HLA variants recognition of drugs as foreign increased risk of cutaneous reactions (SJS, TEN)
http://www.pharmacologyweekly.com/content/images/newsletterimages/pgeneticsv1i3.gif

PGx: HLA
• HLA Class I complex on all nucleated cells
• Complex components
– Heavy a chain w/ peptide binding cleft
– Light β2-macroglobulin chain
– Antigenic peptide
• Self-peptides
• Foreign peptides (drug, virus, tumor antigen, etc.)
• Foreign peptides T-cell immune response

PGx: HLA

PGx: HLA
• Severe Cutaneous Adverse Reactions (SCARs) – Maculopapular rash
– Stevens Johnson Syndrome (SJS)
– Toxic Epidermal Necrosis (TEN)
• Onset: delayed
• Mortality (> 30% w/ TEN)
• Treatment: – Typically requires hospitalization, ICU
– D/C precipitating medication
– Fluids, steroids, antihistamines, analgesics, antibiotics, etc.

PGx: HLA
• DNA test for allele carrier status
• Strong ethnic associations (see following slide)
• Result reported:
– Positive: present on one or both gene copies
– Negative: not present on either gene copy

PGx: HLA Summary Drug Allele Race/Ethnicities of High
Prevalence
Abacavir HLA-B*57:01 European: 6-7% Southwest Asian: 20%
Allopurinol HLA-B*58:01 Han Chinese: 6-8% Korean: 12%
Carbamazepine HLA-B*15:02 Han Chinese, Taiwanese: 10% Populations from Hong Kong, Thailand, Malaysia, Vietnam, Philippines, India and Indonesia: >5%
HLA-A*31:01 Northern European: 2-5% Japanese: 9%
Fosphenytoin/Phenytoin HLA-B*15:02 See Above

PGx: HLA
• CPIC recommendations vary by drug
– Who to test?
• Abacavir: all patients
• Fosphenytoin/Phenytoin, carbamazepine: certain Asian ethnicities
– If positive related allele variant known?
• Drug is contraindicated if positive
• In case of Fosphenytoin/Phenytoin: if patient has taken drug > 3 months previously without incident, may reinitiate

PGx: What’s next?
• Educating pharmacists and prescribers
• Incorporation into RCT criteria
• Incidental findings
• Discovery of novel drug-gene associations and the development of corresponding guidelines
• Insurance coverage for testing
• Implementation of pre-emptive testing protocols

PGx: Assessment Question 1
• Which of the following statements is true of HLA associated CPIC recommendations?
A. Universal testing of all patients is recommended prior to initiating abacavir therapy.
B. Variants associated with cutaneous reactions and carbamazepine are most prevalent in European populations.
C. A patient who has taken phenytoin for at least 1 month without incident may reinitiate therapy regardless of HLA variant status.
D. Cutaneous reactions associated with HLA variants typically happen immediately following the first medication dose.

PGx: Assessment Question 2
• Which of the following drugs and genes provide an example of pharmacogenetics testing for pharmacodynamic protein effects?
I. Herceptin & HER2/neu
II. Ivacaftor & CFTR mutations
III. Warfarin & VKORC1 rs9923231
A. I only
B. I & II
C. II & III
D. I, II, & III

PGx: Assessment Question 3 • A provider orders a warfarin PGx panel for a patient CT prior to initiating
therapy. The results come back as follows: CYP2C9 *2/*3, VKORC1 rs9923231 AA. How will CT’s variants affect the recommended starting dose for warfarin versus a patient who is wild-type for CYP2C9 and VKORC1 rs9923231? Assume ALL other clinical factors (height, weight, age, diet, smoking status, etc.) between the patients are equal.
A. CT’s CYP2C9 genotype is associated with a required increase in starting dose,
but the VKORC1 rs9923231 genotype suggests a decrease may be necessary.
B. CT’s CYP2C9 genotype is associated with a required decrease in starting dose, but the VKORC1 rs9923231 genotype suggests an increase may be necessary.
C. Both CT’s CYP2C9 and VKORC1 rs9923231 genotypes are associated with a required increase in starting dose.
D. Both CT’s CYP2C9 and VKORC1 rs9923231 genotypes are associated with a required decrease in starting dose.

Questions?

References • Shabaruddin FH et al. Economic evaluations of personalized medicine: existing challenges and current developments. Pharmacogenomics Pers Med. 2015;8:115–
126. • Scott S. Personalizing medicine with clinical pharmacogenetics. Genet Med. 2011;13(12):987–995. • Motulsky AG. Drug reaction enzymes and biochemical genetics. J Am Med Assoc. 1957;165:835–837. • Samer CF et al. Applications of CYP450 testing in the clinical setting. Mol Diagn Ther. 2013;17:165–184. • Sim SC, Ingelmann-Sundberg M. The human cytochrome P450 (CYP) allele nomenclature website: a peer-reviewed database of CYP variants and their associated
effects. Hum Genomics. 2010;4(4):278–281. • Kohn LT et al, eds. To Err Is human: Building a Safer Health System. Washington, DC: National Academy of Sciences; 2000. • Sikka R et al. Bench to bedside: pharmacogenomics, adverse drug interactions, and the cytochrome P450 system. Acad Emerg Med. 2005;12(12):1227–1235. • Beitelshees AL, Veenstra DL. Evolving research and stakeholder perspectives on pharmacogenomics. J Am Med Assoc. 2011;306(11):1252–1253. • Lexicomp. Warfarin. Copyright 1978–2015. Hudson, OH: Lexicomp. Accessed • September 8, 2015. • Johnson JA et al. Clinical pharmacogenetics implementation consortium guidelines for CYP2C9 and VKORC1 genotypes and warfarin dosing. Clin • Pharmacol Ther. 2011;90(4):625–629. • Caldwell MD et al. CYP4F2 genetic variant alters required warfarin dose. Blood. 2008;111(8):4106–4112. • Limdi NA et al. Race influences warfarin dose changes associated with genetic factors. Blood. 2015;126(4):539–545. • Millares-Sipin CA et al. Phenytoin and fosphenytoin. In: Cohen H, ed. Casebook in Clinical Pharmacokinetics and Drug Dosing. New York, NY: McGraw-Hill; 2015. • Lexicomp. Phenytoin. Copyright 1978–2015. Hudson, OH: Lexicomp. Accessed September 8, 2015. • Caudle KE et al. Clinical pharmacogenetics implementation consortium guidelines for CYP2C9 and HLA-B genotypes and phenytoin dosing. Clin Pharmacol Ther.
2014;96(5):542–548. • Relling MV et al. Clinical pharmacogenetics implementation consortium guidelines for thiopurine methyltransferase genotype and thiopurine dosing. Clin
Pharmacol Ther. 2011;89:387–391. • Wilke RA et al. The clinical pharmacogenomics implementation consortium: CPIC guideline for SLCO1B1 and simvastatin-induced myopathy. Clin Pharmacol Ther.
2012;92(1):112–117. • Ramsey LB et al. The clinical pharmacogenetics implementation consortium guideline for SLCO1B1 and simvastatin-induced myopathy: 2014 update. Clin
Pharmacol Ther. 2014;96(4):423–428. • Leckband SG et al. Clinical pharmacogenetics implementation consortium guidelines for HLA-B genotype and carbamazepine dosing. Clin Pharmacol Ther.
2013;94(3):324–328. • McCormack M, et al. HLA-A*3101 and carbamazepine-induced hypersensitivity reactions in Europeans. N Engl J Med. 2011;364:1134–1143. • Nepom GT. The major histocompatibility complex. In: Kasper D et al, eds. Harrison’s Principles of Internal Medicine. 19th ed. New York, NY:McGraw-Hill; 2015. • Wilson JT et al. High incidence of a concentration-dependent skin reaction in children treated with phenytoin. Br Med J. 1978;1(6127):1583–1586.

References • Martin MA et al. Clinical pharmacogenetics implementation consortium guidelines for HLA-B genotype and abacavir dosing. Clin Pharmacol Ther.
2012;91(4):734–738. • Ma JD et al. HLA-B*5701 testing to predict abacavir hypersensitivity. PLoS Curr. 2010;2:RRN1203. • Dean L. Allopurinol therapy and HLA-B*58:01 genotype. In: Medical Genetics Summaries [Internet]. Bethesda, MD: National Center for Biotechnology
Information; Created: March 26, 2013. http://www.ncbi.nlm.nih.gov/books/NBK127547/. • Ferrell PB, McLeod HL. Carbamazepine, HLA-B*1502 and risk of Stevens–Johnson syndrome and toxic epidermal necrolysis: US FDA recommendations.
Pharmacogenomics. 2008;9(10):1543–1546. • Gaedigk A. Complexities of CYP2D6 gene analysis and interpretation. Int Rev Psychiatry. 2013;25(5):534–553. • Hicks JK et al. Clinical pharmacogenetics implementation consortium (CPIC) guideline for CYP2D6 and CYP2C19 genotypes and dosing of selective serotonin
reuptake inhibitors. Clin Pharmacol Ther. 2015;98(2):127–134. • Crews KR et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) guidelines for cytochrome P450 2D6 (CYP2D6) genotype and codeine therapy: 2014
Update. Clin Pharmacol Ther. 2014;95(4):376–382. • Lexicomp. Codeine. Copyright 1978–2015. Hudson, OH: Lexicomp. Accessed September 13, 2015. • Zhou SF. Polymorphisms of human cytochrome P450 2D6 and its clinical significance, Part II. Clin Pharmacokinet. 2009;48(12):761–804. • Abidi MZ et al. CYP2C19*17 genetic polymorphism—an uncommon cause • of voriconazole treatment failure. Diagn Microbiol Infect Dis. 2015;83(1):46–48. • Kearns GL et al. Developmental pharmacology—drug disposition, action, and therapy in infants and children. N Engl J Med. 2003;349:1157–1167. • Lu H, Rosenbaum S. Developmental pharmacokinetics in pediatric populations. J Pediatr Pharmacol Ther. 2014;19(4):262–276. • Koukouritaki SB et al. Developmental expression of human hepatic CYP2C9 and CYP2C19. J Pharmacol Exp Ther. 2004;308(3):965–974. • Netzer C, Biller-Andorno N. Pharmacogenetic testing, informed consent and the problem of secondary information. Bioethics. 2004;18(4):344–360. • Haga SB, LaPointe NMA. The potential impact of pharmacogenetic testing on medication adherence. Pharmacogenomics J. 2013;13(6):481–483. • Stanek EJ et al. Adoption of pharmacogenomic testing by US physicians: results of a nationwide survey. Clin Pharmacol Ther. 2012;91(3):450–458. • Ehmann F et al. Pharmacogenomic information in drug labels: European • Medicines Agency perspective. Pharmacogenomics J. 2015;15:201–201. • Whirl-Carrillo M et al. Pharmacogenomics knowledge for personalized medicine. Clin Pharmacol Ther. 2012;92(4):414–417. • Bell GC et al. Development and use of active clinical decision support for preemptive pharmacogenomics. J Am Med Inform Assoc. 2013;21(e1):e93–e99. • Green RC et al. ACMG recommendations for reporting of incidental findings fin clinical exome and genome sequencing. Genet Med. 2013;15(7):565–574. • AAP. Ethical and policy issues in genetic testing and screening of children. Pediatrics. 2013;131(3):620–622. • ACMG. Incidental findings in clinical genomics: a clarification. A Policy Statement of the American College of Medical Genetics Genomics. Genet Med.
2013;15:664–666. • The Personalized Medicine Coalition. The Case for Personalized Medicine. 4th ed. Washington, DC: PMC; 2014:34–35.