brian haynes€¦ · updates, dynamed, macplus fs, ... clinicians like you usually have more than 5...
TRANSCRIPT


Brian Haynes
McMaster University
EBHC Workshop,
2013

The Health Information Research Unit at
McMaster has developed, and produces or
supports, several resources that will be
discussed (ACP Journal Club, Evidence
Updates, DynaMed, MacPLUS FS,
ACCESSSS).
(IP belongs to McMaster; most services free)

Agenda (negotiate!)
1. Intros – and your most frustrating or rewarding
teaching or personal experience in acquiring
“current best evidence for clinical practice”
2. Favorite sources of EB info?
3. Sign up: http://plus.mcmaster.ca/ACCESSSS
(suggest that you subscribe, but can use
ID/PW: guestn/guestn)

1. To define/personalize the nature of the
problems in translating evidence into clinical
practice
2. To explore a hierarchy of
evidence resources to support clinical care
decisions:
3. To demonstrate and practice how you can
use/teach the pyramid to keep up to date
(“push services”) and find current best
evidence (“pull services”)

1. Making decisions consistently
based on current best evidence ?
2. Keeping up to date with current
best evidence ?

Clinicians like you usually have more than 5 questions a day that can be answered by current best evidence
Green. Residents' medical information needs in clinic: are they being met? Am J Med 2000

But…
2,000 new articles every day
including 75 trials
and 11 systematic reviews
Bastian, Seventy-five trials and eleven systematic reviews a day: how will we ever keep up? PLoS Med. 2010
Bastian, Seventy-five trials and eleven systematic reviews a day: how will we ever keep up? PLoS Med. 2010

By the year 2020, 90% of clinical decisions
will be supported by accurate, timely, and
up-to-date clinical information and will reflect
the best available evidence.
IOM Roundtable on Evidence-Based Medicine
This can’t happen without excellent connections
between best evidence and decisions for and by
individual patients.

years since
graduation
r = -0.54
p<0.001
...
...
. .. . . .... .
....
....
... ..
... knowledge
of current
best care
100%
0%
50%
Choudhry, Fletcher and Soumerai,
Ann Intern Med 2005;142:260-73
94% of 62 studies found decreasing competence for at
least some tasks, with increasing physician age.

McMaster vs U of Toronto
years since
graduation
knowledge
of current
best care
100%
0%
50%
From Shin et al,
CMAJ 1993

The Slippery Slope
years since
graduation
...
...
. .. . . .... .
....
....
...
..
... knowledge
of best
evidence
100%
0%
50%
You could be the first generation to stay
on top and avoid the slippery slope…

…17 to 20 years

1. To define the nature of the problems in
translating evidence into clinical practice
2. To explore a hierarchy of
evidence resources to support clinical care
decisions:
3. To demonstrate how you can use the pyramid
to keep up to date (“push services”) and find
current best evidence *fast* (“pull services”)
Finding current best evidence
is becoming much easier.

Personalized EBM “push” Alerts?
eg EvidenceUpdates, ACPJournalWise
EBM “pull” Resources?
eg UTD, DynaMed, Best Practice, ACP PIER
EBM Federated Resources?
eg TRIP, ACCESSSS

Many evidence-based resources help you answer your questions

But no single resource provides all answers or is sufficiently updated

shows results in a pyramid of resources in a few seconds

showing results in a pyramid of resources in a few seconds

Summaries
Pre-appraised
research
Non-preappraised
research

Summaries
• are E-B clinical textbooks and
E-B guidelines
• integrate best evidence
for individual care topics
• provide actionable
recommendations
But which
summary to
choose?
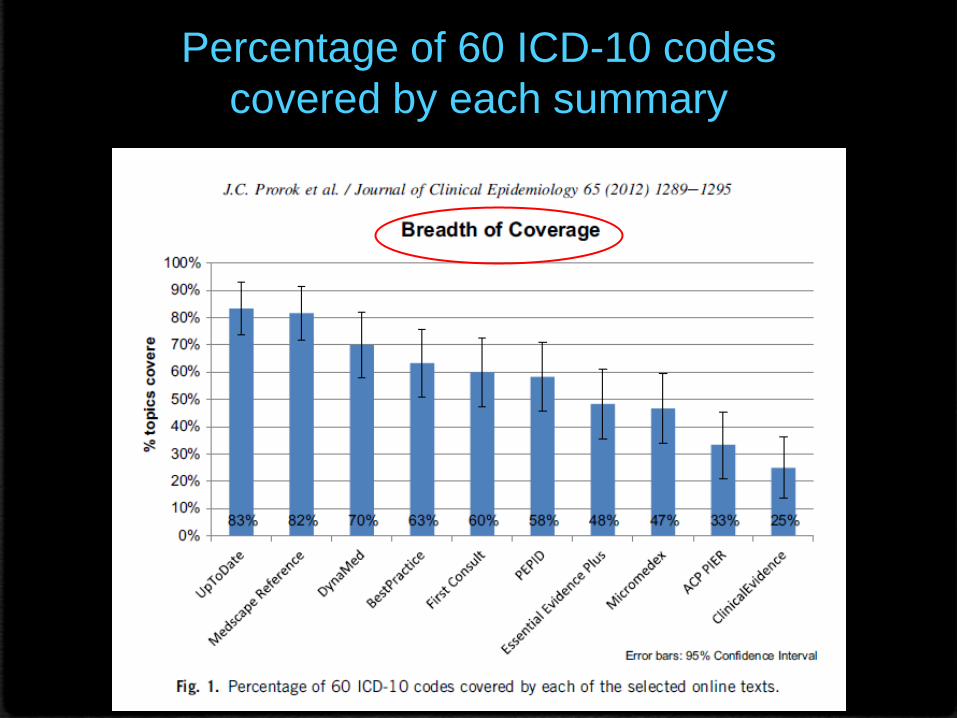
Percentage of 60 ICD-10 codes
covered by each summary

Error bars: 95% Confidence Interval
Timeliness of updates of 10
online evidence-based texts Average time of updating of 60 topics
(randomly selected) as of July 2011
Ranging from
3.5 to 29 months

Summary Timeliness Breadth Quality
DynaMed 1 3 2
UpToDate 5 1 2
Micromedex 2 8 2
Best Practice 3 4 7
Essential Evidence Plus 7 7 2
First Consult 9 5 2
Medscape Reference 6 2 9
Clinical Evidence 8 10 1
ACP PIER 4 9 7
PEPID N/A 6 10
Rank order of 10 Online Summaries

No answer?
or more recent evidence?

Summaries
Pre-appraised
Research

synopses of systematic reviews
systematic reviews
synopses of studies


only a tiny proportion of all research is “ready for application”
only a tiny fraction of the “ready” research is “relevant” for a given clinician
only a tiny proportion of the “relevant” research for a given clinician is “interesting” in the sense of being something new, important, and actionable.

Haynes, B. The Best New Evidence for Patient Care. Ann Intern Med. 2008;148(10):JC3-2
~3300 articles
per year
Critical Appraisal Filters
Clinical Relevance Filters
+ 35,000 articles
screened per
year
~20 articles per clinician
Up to 99.9 %
‘Noise’ Reduction
Is‘information overload’ no longer
a valid excuse for ignorance?

Al-Khatib SM, Thomas L, Wallentin L, et al.
Outcomes of apixaban vs. warfarin by type
and duration of atrial fibrillation: results from
the ARISTOTLE trial. Eur Heart J. 2013 Apr 17.
4 internists
4 neurologists
4 cardiologists
4 hematologists

DISCIPLINE RELEVANCE NEW?
Internal Medicine 6/7 6/7
Neurology 6/7 6/7
Cardiology
5/7 6/7
Hematology 5/7 5/7

Internists
Neurologists
Cardiologists
Hematologists 7/6 6/5 7/7

is published in evidence-
based journals and resources

• is continuously sent to
you through MacPLUS,
ACCESSSS, ACPJW,
EvidenceUPDATES alerts
http://plus.mcmaster.ca/EvidenceUpdates

Methods • Select 4 leading evidence-based texts • Select 200 topics that are common to all
• Identify date of most recent update for each topic in each text
• Identify each article in MacPLUS that is more recent than text
update • Compare conclusions of MacPLUS studies with conclusions in
text
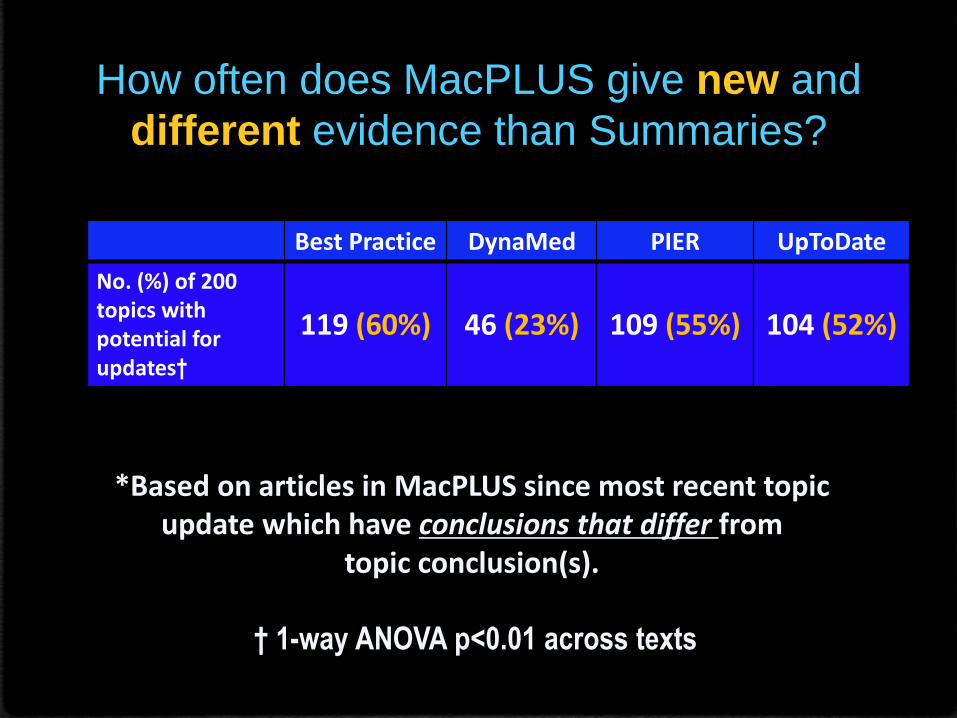
How often does MacPLUS give new and
different evidence than Summaries?
Best Practice DynaMed PIER UpToDate
No. (%) of 200 topics with potential for updates†
119 (60%)
46 (23%)
109 (55%)
104 (52%)
*Based on articles in MacPLUS since most recent topic
update which have conclusions that differ from topic conclusion(s).
† 1-way ANOVA p<0.01 across texts

Summaries
Pre-appraised
Research
Non-preappraised
Research

Why search
last?
• Studies are not critically appraised
• Searches yield large outputs with few relevant
studies in the first pages
• Current evidence is diluted and more difficult
to find, but less so if you use filters

Use Clinical Queries filters for questions of
• Prediction Guides
• Prognosis
• Etiology
• Diagnosis
• Therapy

Sensitivity/
Specificity PubMed Equivalent
broad
filter 99% / 70%
((clinical[Title/Abstract] AND trial[Title/Abstract])
OR clinical trials[MeSH Terms] OR clinical
trial[Publication Type] OR
random*[Title/Abstract] OR random
allocation[MeSH Terms] OR therapeutic
use[MeSH Subheading])
narrow
filter 93% / 97%
(randomized controlled trial[Publication Type]
OR (randomized[Title/Abstract] AND
controlled[Title/Abstract] AND
trial[Title/Abstract]))
E.g. CQ therapy filters

How many search terms to use?
Patients
Intervention
Comparison
Outcomes

Patient
Pre-appraised research
Works better for Summaries
E.g. COPD mucolytics
+ Intervention
and
Using Keep it simple!

Works better for unappraised evidence
COPD mucolytics
Combining more terms from your PICO elements
(exacerbation OR mortality)

looks for you in all resources and displays results in a pyramid



PICO question from the audience
• …

Did I miss any
important
evidence with
my search?
Is there any way I
could have
retrieved less
“junk”?
What is the best current evidence?

Alternatives
TRIP Database – EB search, guidelines, patient info, fulltext links, videos, news
SUMSearch – DARE at highest level
STAT!Ref
Corporate collections – professional organizations; commercial publishers

Additional slides

Search strategies in PubMed
Search strategy = PICO query AND filters AND additional strategy
Search terms
Previous knowledge
Trial and Error MeSH Thesaurus
Boolean operators = OR, AND Combination
Initial question
P – Patient, Population
I – Intervention, Exposure…
C – Controls, Comparators
Search forward from:
Related Articles in
Pubmed
Screen the
bibliography of
relevant articles
Methodological filters:
Ex: Clinical Queries
Content filters (topic,specialty) O – Outomes
T – Type of question, design
AND
AND
Dynamic
Agoritsas & al. Sensitivity and Predictive Value of 15 PubMed Search Strategies to Answer Clinical Questions Rated Against Full Systematic Reviews. JMIR, 2012.

Balance between Sensitivity & Precision
Factors increasing Sensitivity:
• Many search terms for a similar concept, linked with OR.
• Truncated terms, Wildcards (e.g. tox*, wom?n)
• Synonyms (pressure sore, decubitus ulcer)
• Variant spelling (tumour, tumor)
• Explosion of MeSH terms
• Proximity search through «Related articles», Bibliography
Factors increasing Precision
• Concepts linked with AND (P) AND (I) AND (C) AND (O)
• Use of NOT Cochrane
• Limits
• Methodological Filters
• Content Filters
(P1 OR P2 OR P3) AND (I1 OR I2 … ) AND (C1 OR C2 …) AND (O1 OR O2 OR O3 …)
Population Intervention Comparators Outcomes

54
Question Effects of oral mucolytics agents in adults with stable
chronic bronchitis or COPD.
P stable chronic bronchitis
COPD (chronic bronchitis) OR COPD
I Mucolytic agents
oral mucolytic therapy mucolytics
C Placebo placebo
O number of exacerbations exacerbation
First try chronic bronchitis mucolytics
Example of PICO query

Less effective strategy (no filter)
Agoritsas & al. Sensitivity and Predictive Value of 15 PubMed Search Strategies to Answer Clinical Questions Rated Against Full Systematic Reviews. JMIR, 2012.

More effective strategy (with narrow filter)
Agoritsas & al. Sensitivity and Predictive Value of 15 PubMed Search Strategies to Answer Clinical Questions Rated Against Full Systematic Reviews. JMIR, 2012.

McMaster Online Rating of Evidence: >5000 clinicians
RELEVANCE
