branched chain aminoacids
DESCRIPTION
BIOCHEMISTRY - PowerPoint PPT PresentationTRANSCRIPT
Three targets of branched-chain aminoacid supplementation in the
treatment of liver disease.
M.Prasad NaiduMSc Medical Biochemistry,
Ph.D.Research Scholar
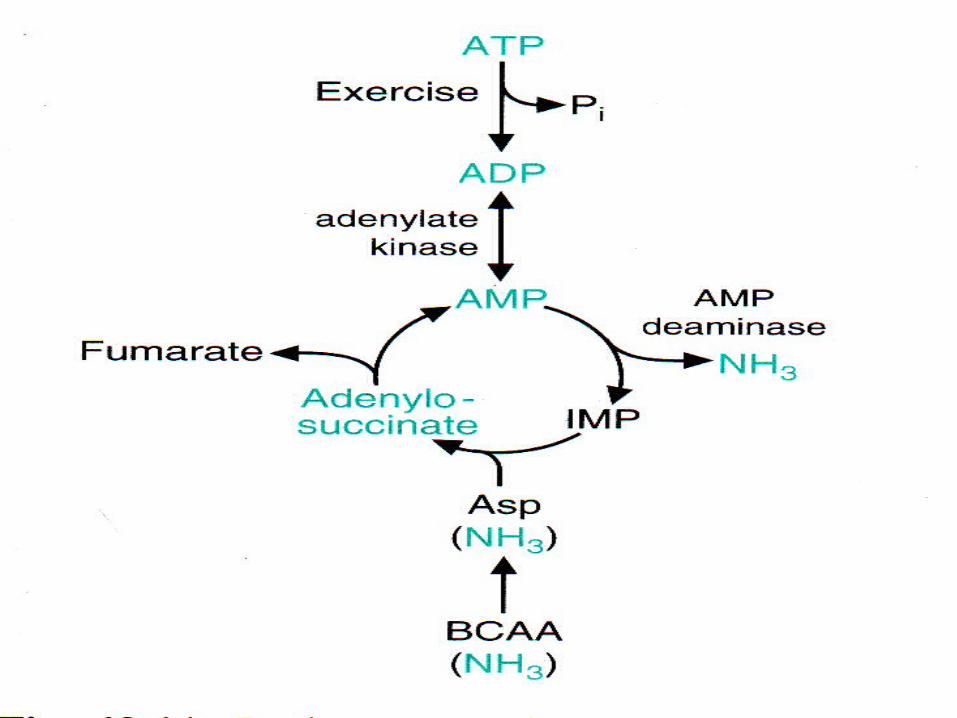
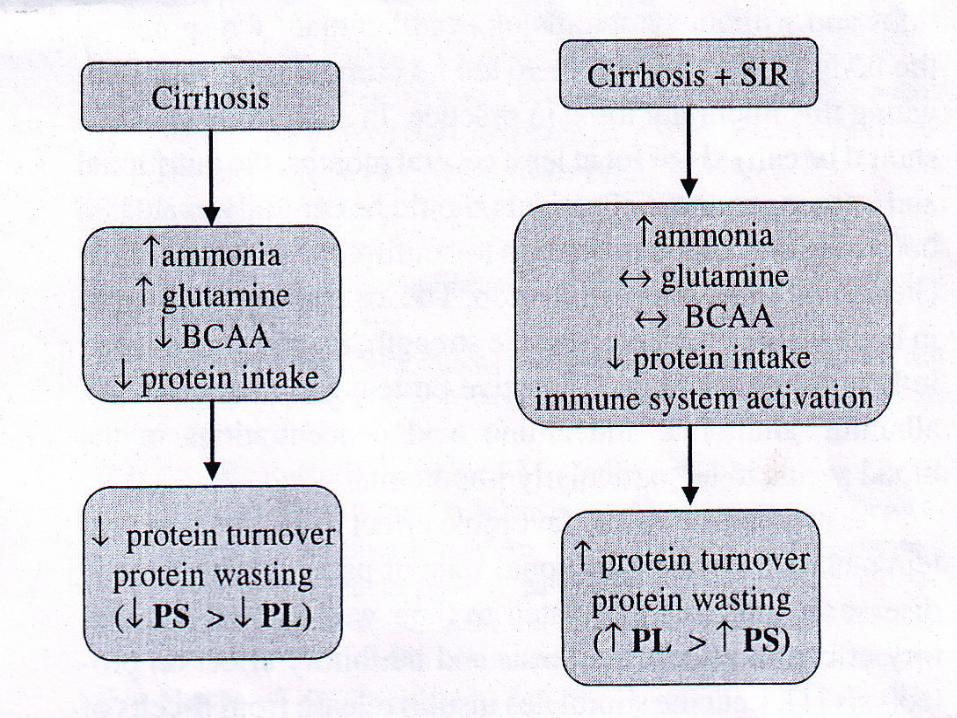
The BCAA & protein metabolism in various forms of hepatic injury & it is suggested that the main cause of decrease in plasma BCAA conc in liver cirrhosis is hyperammonemia
Three possible targets of BCAA supplementation in liver disease are suggested
1. Hepatic encephalopathy2.Liver regeneration 3.Hepatic cachexia.
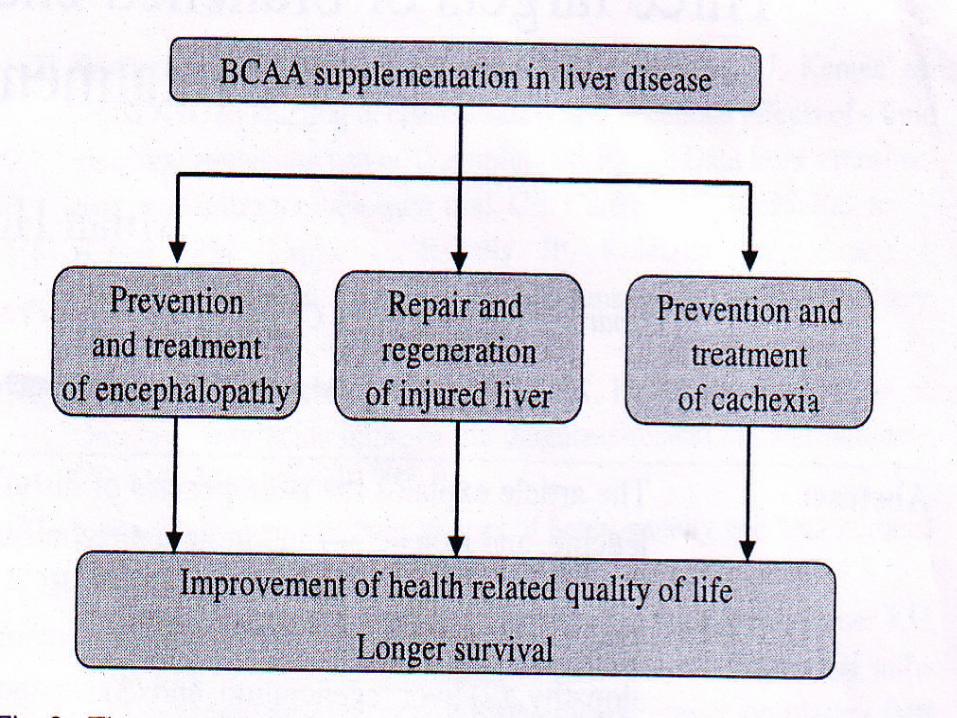
The BCAA may ameliorate hephatic encephalopathy by promoting ammonia detoxification,correction of plasma aminoacid imbalance and by reduced brain influx of AAA
The favourable effect of BCAA on liver regeneration and nutritional state of the body is related to their stimulatory effect on protein synthesis,secretion of hepatocyte growth factor ,glutamine production and inhibitory effect on proteolysis.
Presumably the beneficial effect of BCAA on hepatic cachexia is significant in compensated liver disease with decreased plasma BCAA conc ,where as it is less pronounced in hepatic diseases with inflammatory complications and enhanced protein turn over.
Introduction
The BCAAs valine,leucine and isoleucine are indispensible aminoacids of special interest
Several studies have demonstrated the stimulatory effect of BCAAs and/or their metabolites on protein synthesis and/or inhibitory effect on proteolysis
They play a major role in muscle and most other tissues because they are major AAs that can be oxidised in tissues

Acute liver injury Is a clinical condition resulting from damage of
liver cells One characteristic feature of acute liver
failure is a marked increase in aminoacidemia The main cause of increased AA concentrations
is due to their leaking from the dying hepatocytes.
The changes in BCAA conc are less pronounced (compared to other AA s) because they are catabolised significantly in extrahepatic tissues
Chronic injury Decreased blood conc of BCAA and increased
conc of AAA and methionine are characteristic of chronic liver disease esp.,cirrhosis
The abnorm alities in BCAA and AAA levels in cirrhosis are expressed as molar ratio (BCAA/AAA)
Physiologically ,the ratio is 3.0 -3.5.,where as in patients with hepatic cirrhosis it is significantly lower.
It is a serious neuropsychiatric abnormality associated with chronic or acute liver injury
Signs Impaired cognition A flapping tremor Decreased level of consciousness,including
coma, cerebral edema and ultimately death.
BCAA and hepatic encephalopaty
Substances contributing to symptoms of hepatic encephalopathy include
AMMONIA Mercaptans Short chain FAs Increased conc of AAAs GABA Endogenous benzodiazepines etc.,In the pathogenesis of HE ,changes induced by
impaired liver function and portal systemic shunting interact,resulting in accumulation of substances that are normally removed by liver.
Presumed mechanism of the direct effect of hyperammonemia on brain functions include
-Its effect on inhibitory post synaptic potentials by blocking the chloride pump
-Impairment of brain ATPsynthesis due to depletion of krebs cycle intermediates
-Cell swelling by ammonia induced blood flow and
synthesis
-Accumulation of glutamine in astrocytes
Activation ofn-MDA receptors
Intracellular excess of calcium
Increased NO formation
Increased production of free radicals
Impaired mitochondrial respiration
ATP depletion Contributing to
ammonia induced death in acute liver failure
Hyperammonemia affects neurotransmission associated with n-MDA receptors(acute effects)
Chronic hyperammonemia Seems to induce impaired signal
transduction associated with n-MDA receptors
Thereby contributing to some neurological alterations observed in hepatic encephalopathy
Indirectly , hyper ammonemia may contribute to hepatic encepha lopathy by
A decrease in BCAA levels in the blood
Alterations in AA transport across the BBB.
AAAs flood the CNS due to high blood plasma conc of AAA and low conc of BCAAs,which compete for entry by the L-system(system that serves for transport of neutral AAs) across the BBB.
Augmented uptake of AAAs results in An imbalance in the synthesis of dopamine,
noradrenaline and serotonin in the brain.
Inaddition, increased availability of AAAs may cause the formation of false neuro transmitters like octopamine,phenyl ethanolamine,andtyramine
The rationale of BCAAs in the treatment of hepatic encephalopathy was based on assumptions that providing BCAAs
Would facilitate ammonia detoxification by supporting glutamine synthesis in skeletal muscle and brain
Would normalise plasma AA concentrations and
Decrease brain influx of AAAs
The survival of patients with liver injury of varying etiology depends on the ability of the remaining hepatocytes to regenerate
Nutritional and metabolic support of liver regeneration seem to be very important
Carbohydrate source, primarily glucose, is recommended
BCAA and liver regeneration

Results of several studies have indicated that preservation of hepatic glycogen increases the liver’s tolerance to oxidative and ischaemic damage
Perioperative glucose/insulin infusion may prevent or attenuate hepatic dysfunction after extensive liver resection
The mechanism of the favourable effect of BCAAs on hepatic tissue repair is multifactorial
The well known synergestic effect of glucagon and insulin on liver regeneration
The stimulatory effect of leucine on protein synthesis
The stimulatory effect of leucine on hepatocyte growth factor by hepatic stellate cells may be involved.
Some effects of BCAAs may be associated with enhanced production of glutamine
BCAA treatment promoted recovery of serum albumin and lowered bilirubin levels after partial hepatectomy for liver cancer and improved patient’s prognosis after livertransplantation

Glucose administation inhibits
Inhibition of Hs lipase by insulin
Decreased mobilization of fattyacids
Increase in insulin / glucagon quotient
Infusion of fatty emulsion stimulates
Regenerating liver generates ATP primarily by FA oxidation
The beneficial effect of carnitine
FAs act as substrates for synthesis of phospholipids and esterification of cholesterol.
Many studies have demonstrated that lipids are well tolerated ,even in cirrhotic patients , if administered parenterally
Clinical trials will have to determine whether lipid therapy can improve liver regeneration and function after liver resection and in hepatic disease.
Cachexia is defined as a complex metabolic syndrome associated with underlying illness and characterised by loss of fat mass.
Prevalence 20% in patients with compensated liver
disease 100% in patients with acute alcoholic
hepatitis 50% in patients with liver cirrhosis
BCAA and hepatic cachexia
Pathogenesis Poor dietary intake Malabsorption Maldigestion Metabolic
disturbances Resulting in changes
in protein synthesis and proteolysis
Characterised by Impaired glucose
tolerance- -DM Impaired post prandial
glucose utilization – -decreased glycogen contents in the liver and skeletal muscle
Enhanced utilization of lipids and proteins for energy

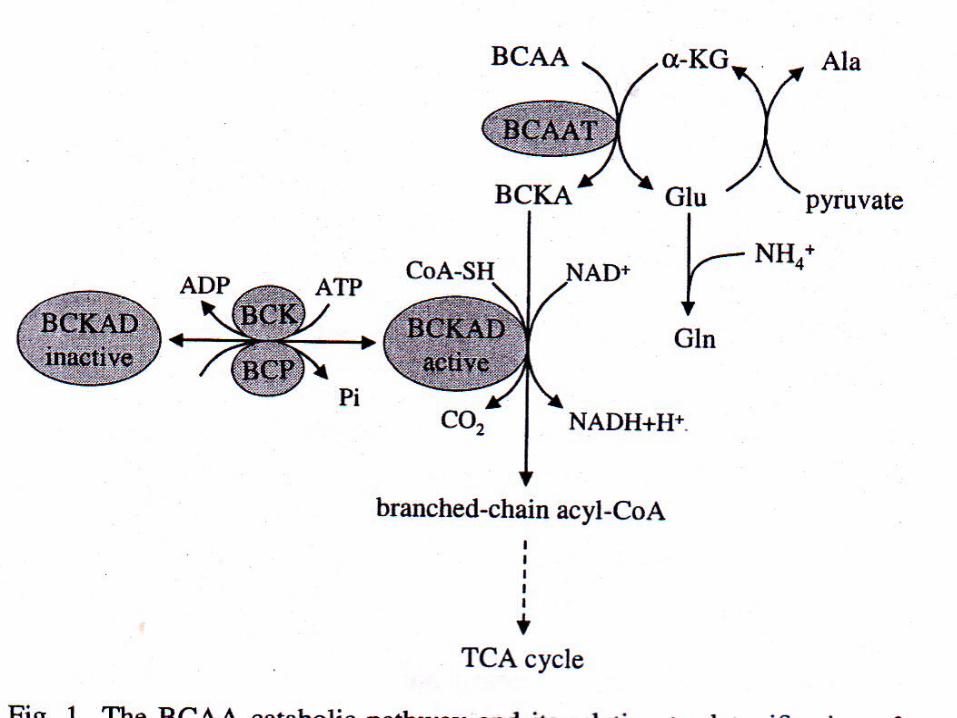
BCAA taken up from plasma and muscle proteins are the important energy substrate in liver cirrhosis
In the first step of their catabolism they are used for glutamate synthesis in mitochondria to clear blood ammonia by enhanced production of glutamine
In the second step, most BCKAs produced in BCAAT reaction are oxidised, probably mostly in skeletal muscle
The mechanism of favourable effect of BCAAs on protein metabolism and nutritional state of pts with hepatic disease is related to
Stimulatory effect on protein synthesis and inhibitory effect on proteolysis
Leucine stimulates insulin release from βcells of pancreas
Leucine also stimulates protein synthesis through phosphorylation of translation initiation factors and ribosomal proteins
These effects may contribute to the improvement of insulin resistance and beta cell function in chronic liver disease.
BCAA supplementation is more effective in compensated cirrrhosis with decreased plasma BCAA conc and with out SIR
The nutritional and immune status of the pt
should be carefully evaluated before BCAA supplementation to confirm the signs of inflammation and cachexia.
The assessment of changes in body weight Apetite Muscle strength Fat free mass index Inflammatory markers(CRP and IL-6) Albumin Aminoacid concentrations …seems to be
particularly important
Conclusions and suggestionsMost experimental studies have revealed the
favourable effects of BCAAs on nutritional status, development of liver illness and quality of life
.This favourable effect is related to their
stimulatory effect on protein synthesis ,insulinsecretion and liver regeneration
These favourable effects BCAA supplementation seem to be more apparent when BCAA concentration decrease as in liver cirrhosis with portasystemic shunts and particularly when not complicated by a systemic inflammatory response.
Formulas for oral,enteral and parenteral BCAA supplementation are commercially available and the appropriate administration should be considered.
Oral route is advantageous than parenteral feeding eg; danger of liver steatosis
impaired gut hormonal and immunological responses phlebitis or thrombosis of veins
An adverse property of BCAAs is their extremely bitter taste,and the low palatability of nutritive drinks is a major problem with respect to patient compliance.
BCAA enriched mixtures should contain not only BCAAs but also glucose,lipids, and other nutrients that should have beneficial effects on the course of hepatic illness.
Coadministration of BCAA s with carnitine or zinc has a beneficial effect.
BCAA with zinc supplementations showed greater ability to metabolise ammonia and higher efficacy in correcting AA alterations
The aministration of BCAA with L-acetyl carnitine revealed improvement of neurologic symptoms and serum ammonia in cirrhotic patients
Dietary supplementationwith BCAA improved the impaired transthyretin turnover in rats with liver cirrhosis
In conclusion ,although critical objections regarding the effects of BCAA supplementation can still be raised..,
the rationale of BCAA in chronic hepatic illness their favourable effect on nutritional state Repair and regeneration of hepatic tissue Safety of their administration Positive results of several randomised trials
conducted in recent years …. Are strong arguments for BCAA supplementation as a standard nutritional approach in treating pts with hepatic disease ,particularly cirrhosis.
Thank you