brain lesions and criminal behavior 2009
TRANSCRIPT
Brain Lesions and theirImplications in CriminalResponsibility
Shelley Batts, Ph.D.*
For over 200 years, Western courts have considered pleas of‘‘not guilty by reason of insanity’’ (NGRI) for defendants inpossession of a mental defect rendering them unable tounderstand the wrongfulness of their act. Until recently,determining the mental state of a defendant has fallenlargely upon the shoulders of court psychologists andexperts in psychiatry for qualitative assessments relatedto NGRI pleas and mitigation at sentencing. However,advances in neuroscience—particularly neurological scan-ning techniques such as magnetic resonance imaging(MRI), functional magnetic resonance imaging (fMRI),computed tomography scanning (CT), and positron emis-sion tomography scanning (PET)—may provideadditional, pertinent biological evidence as to whether anorganically based mental defect exists. With increasingfrequency, criminal defense attorneys are integrating neu-roimaging data into hearings related to determinations ofguilt and sentencing mitigation. This is of concern, sincenot all brain lesions and abnormalities indicate a com-promised mental state that is relevant to knowing whetherthe act was wrong at the time of commission, and juriesmay be swayed by neuroscientific evidence that is notrelevant to the determination of the legal question beforethem. This review discusses historical and modern casesinvolving the intersection of brain lesions and criminality,neuroscientific perspectives of how particular types oflesions may contribute to a legally relevant mental defect,and how such evidence might best be integrated into acriminal trial. Copyright # 2009 John Wiley & Sons, Ltd.
Behavioral Sciences and the Law
Behav. Sci. Law 27: 261–272 (2009)
Published online in Wiley InterScience
(www.interscience.wiley.com) DOI: 10.1002/bsl.857
*Correspondence to: Shelley Batts, Ph.D., Neuroscience Program, The University of Michigan, U.S.A.E-mail: [email protected]
Copyright # 2009 John Wiley & Sons, Ltd.
NEUROSCIENCE AND THE LAW:THE TWAIN HAVE MET
The development of noninvasive techniques to observe blood flow (either directly or
indirectly, as with glucose uptake) and structures in the functioning human brain has
been a boon to advancing knowledge of how damage to particular neural structures
can correlate with shifts in behavior. As important determinations in criminal
proceedings rely on judgments of a defendant’s state of mind at the time of the crime,
it may have been only a matter of time before neuroimaging evidence found its way
into the courtroom. An influential instance where structural neuroimaging evidence
was presented in a criminal proceeding was in 1991, in the second-degree murder
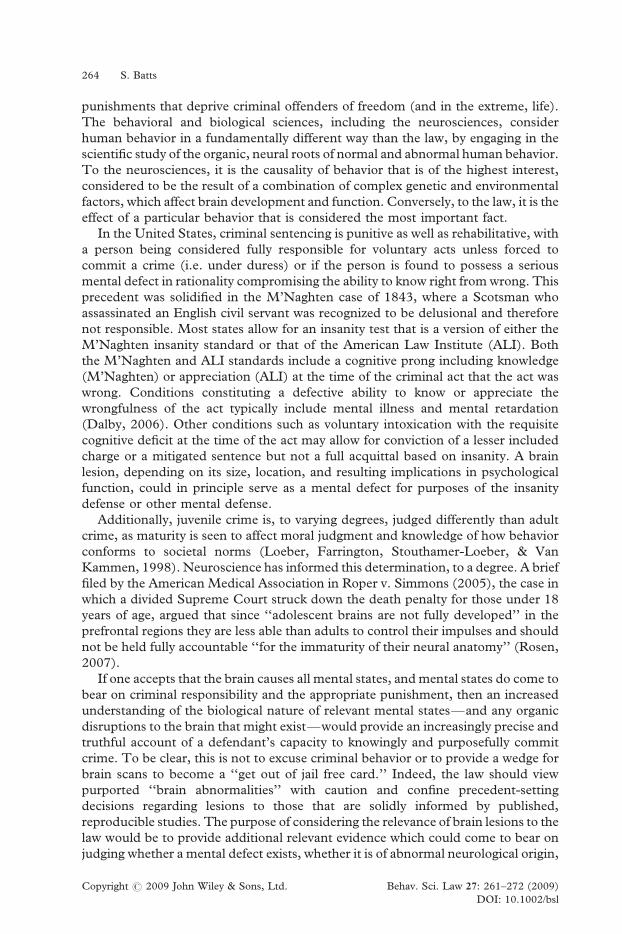
case involving 64-year-old defendant Herbert Weinstein. During a heated argument
with his wife, the advertising executive strangled her to death and then threw her
body from the window of their apartment to make it appear a suicide (Rojas-Burke,
1993). Weinstein’s lawyer claimed that his client was not responsible for his actions
due to a mental defect: a large cyst located in the membranous casing of the brain
(the arachnoid membrane) had increased the pressure on his frontal cortex, creating
metabolic imbalances in the region, which decreased his ability to tell right from
wrong (Figure 1). Expert testimony from a forensic psychologist for the prosecution
was presented arguing that arachnoid brain cysts were often benign and that no
established correlation existed connecting such cysts to criminal actions. However,
at a pretrial hearing, the judge ruled that the jury could hear that Weinstein had a
brain cyst, but not that such cysts or abnormal brain metabolism increase violent
tendencies. Weinstein pled guilty to the reduced charge of manslaughter.
Prior to the Weinstein case, neuroimaging evidence had been presented in a few
rare cases. In 1981, the attorneys for John Hinckley, Jr. tried to introduce a CAT
scan of Hinckley’s brain through expert witness Dr. David Bear as part of an NGRI
defense (Dumit, 1999). Both the defense and prosecution said such evidence had
never been admitted as evidence in an American courtroom, and the judge decided
to dismiss the jury, during which time he heard arguments about the CAT scan’s
Figure 1. PET and MRI images from defendant Herbert Weinstein, performed by Dr. Abass Alavi at theUniversity of Pennsylvania Hospital in 1991. Left: MRI scan reveals the neural architecture of Weinstein’sbrain, with the large black area representing the cyst in the frontal temporal area of the brain. Right: FDG-PET scan of Weinstein’s brain, showing altered (lowered) glucose metabolism in the brain areas around
the cyst. Adapted from The Journal of Nuclear Medicine, 34(1), Jan 1993
Copyright # 2009 John Wiley & Sons, Ltd. Behav. Sci. Law 27: 261–272 (2009)
DOI: 10.1002/bsl
262 S. Batts

relevancy. The expert explained to the judge that the CAT scan illustrated that
Hinckley had widened sulci—the ridges in the brain formed by its folds (Taylor,
1982). Histopathological studies consistently reveal that people with schizophrenia
are more likely to have widened sulci than normal controls, with an estimated one-
third of the schizophrenic population exhibiting this particular brain defect while less
than one in 50 normal controls show the same abnormal structures (Dumit, 1999).
After several rounds of arguments, the CAT scan was eventually admitted into
evidence and was considered alongside more traditional neuropsychological
evidence and testimony, despite the unknown significance of widened sulci to the
ultimate issue of Hinckley’s sanity. Ultimately, Hinckley was acquitted and
committed to St. Elizabeths Hospital.
In a similar case, defense attorneys in the embezzlement trial of a former United
Way executive William Aramony used an MRI scan to argue a ‘‘shrinking brain’’
defense for their client; the scan also showed widened sulci (Chandrasekaran &
Miller, 1994). Due to Aramony’s supposed diminished mental capacity, it was
argued he was unable to form the requisite criminal intent to commit the crime of
embezzlement. Both Weinstein and Aramony were plead guilty to lesser charges,
suggesting that the impact of neuroimaging—with or without merit—is not a trivial
one.
Neuroimaging evidence is by no means a guarantee of a successful NGRI or
mitigation defense though. In 2002, in United States v. Mezvinsky the defense
argued following his indictments on 66 counts of fraud (2002) that the defendant
suffered from mental illness, specifically bipolar disorder and frontal lobe damage.
Defense attorneys wanted to present PET scans to support the claim that the
defendant was incapable of deception, the requisite mens rea for the fraud charges,
but this request was denied because the judge considered the evidence more
prejudicial than probative.
Neuroimaging has also been presented as evidence for mental illness and
sentencing mitigation, as in the case where a PET scan saved mass murderer Barry
Wayne McNamara from the death penalty in 1985 (Emmons, 1989), although the
presentation of neurological evidence as part of a criminal defense or sentencing
mitigation is more common (Snead, 2007). However, it is yet to be determined what
the proper impact and role of such evidence should be in legal proceedings: how
neuroscience can best assist the law without encouraging bias or allowing
rationalization of crime. Furthermore, while neurological scans are invaluable in
medical diagnoses and neuroscientific studies of brain regions, their use in
connecting data about brain lesions to criminal behavior should not be over-
estimated. The usefulness of neurological scans may be limited to the detection of
lesions rather than a tool to explicate brain states, and this should be considered a
caveat of any discussion of brain lesions and behavioral changes (Morse, 2006).
In comparison to the multi-faceted descriptions of behavior in psychology, the
viewpoint of the courts is simpler. To the law, human behavior generally exists in a
dichotomy of guilty and not guilty. Between these ‘‘black and white’’ extremes lie
pleas of ‘‘not guilty by reason of insanity’’ as well as various intermediate mental
defenses and arguments for sentencing mitigation (e.g. mens rea defense). These rest
upon the notion that impaired mental states should reduce criminal liability. The
legal system’s analysis of behavior is aimed at creating a fair judicial system that
discourages and punishes actions deemed socially malevolent by dispensing
Copyright # 2009 John Wiley & Sons, Ltd. Behav. Sci. Law 27: 261–272 (2009)
DOI: 10.1002/bsl
Brain lesions and criminality 263
punishments that deprive criminal offenders of freedom (and in the extreme, life).
The behavioral and biological sciences, including the neurosciences, consider
human behavior in a fundamentally different way than the law, by engaging in the
scientific study of the organic, neural roots of normal and abnormal human behavior.
To the neurosciences, it is the causality of behavior that is of the highest interest,
considered to be the result of a combination of complex genetic and environmental
factors, which affect brain development and function. Conversely, to the law, it is the
effect of a particular behavior that is considered the most important fact.
In the United States, criminal sentencing is punitive as well as rehabilitative, with
a person being considered fully responsible for voluntary acts unless forced to
commit a crime (i.e. under duress) or if the person is found to possess a serious
mental defect in rationality compromising the ability to know right from wrong. This
precedent was solidified in the M’Naghten case of 1843, where a Scotsman who
assassinated an English civil servant was recognized to be delusional and therefore
not responsible. Most states allow for an insanity test that is a version of either the
M’Naghten insanity standard or that of the American Law Institute (ALI). Both
the M’Naghten and ALI standards include a cognitive prong including knowledge
(M’Naghten) or appreciation (ALI) at the time of the criminal act that the act was
wrong. Conditions constituting a defective ability to know or appreciate the
wrongfulness of the act typically include mental illness and mental retardation
(Dalby, 2006). Other conditions such as voluntary intoxication with the requisite
cognitive deficit at the time of the act may allow for conviction of a lesser included
charge or a mitigated sentence but not a full acquittal based on insanity. A brain
lesion, depending on its size, location, and resulting implications in psychological
function, could in principle serve as a mental defect for purposes of the insanity
defense or other mental defense.
Additionally, juvenile crime is, to varying degrees, judged differently than adult
crime, as maturity is seen to affect moral judgment and knowledge of how behavior
conforms to societal norms (Loeber, Farrington, Stouthamer-Loeber, & Van
Kammen, 1998). Neuroscience has informed this determination, to a degree. A brief
filed by the American Medical Association in Roper v. Simmons (2005), the case in
which a divided Supreme Court struck down the death penalty for those under 18
years of age, argued that since ‘‘adolescent brains are not fully developed’’ in the
prefrontal regions they are less able than adults to control their impulses and should
not be held fully accountable ‘‘for the immaturity of their neural anatomy’’ (Rosen,
2007).
If one accepts that the brain causes all mental states, and mental states do come to
bear on criminal responsibility and the appropriate punishment, then an increased
understanding of the biological nature of relevant mental states—and any organic
disruptions to the brain that might exist—would provide an increasingly precise and
truthful account of a defendant’s capacity to knowingly and purposefully commit
crime. To be clear, this is not to excuse criminal behavior or to provide a wedge for
brain scans to become a ‘‘get out of jail free card.’’ Indeed, the law should view
purported ‘‘brain abnormalities’’ with caution and confine precedent-setting
decisions regarding lesions to those that are solidly informed by published,
reproducible studies. The purpose of considering the relevance of brain lesions to the
law would be to provide additional relevant evidence which could come to bear on
judging whether a mental defect exists, whether it is of abnormal neurological origin,
Copyright # 2009 John Wiley & Sons, Ltd. Behav. Sci. Law 27: 261–272 (2009)
DOI: 10.1002/bsl
264 S. Batts

and whether it is possible that the defect either increased the likelihood of
committing a crime or reduced the ability to exert control and moral judgment.
FOCAL LESIONS CAN PRODUCE SPECIFICALTERATIONS IN BEHAVIOR
It is important to assess whether a neurological lesion could provide a reasonable
foothold for arguing that a particular cognitive faculty had been compromised. The
brain is an immensely complex organ presenting unique challenges for those who
wish to reduce it simply. However, the dominant paradigm of current neuroscientific
studies suggests that localized areas of the brain are responsible for some discrete
behaviors, and when impaired through injury or disease may explain aberrant
behaviors. For example, the motor and pre-motor cortices have neural regions that
precisely correspond to the movement of particular parts of the body. Strokes or head
trauma in this region can result in the loss of movement in just one or two isolated
body parts, depending on the size and location of the damage. Complex cognitive
processing can be focally damaged as well. The neural structures responsible for
understanding, processing, and producing language are lateralized to the left
hemisphere in the vast majority of people, with two small regions called Broca’s and
Wernicke’s areas completely dedicated to this function (Figure 2). Injuries that result
in the destruction of Broca’s area, responsible for language processing and speech
production, leave the person unable to effectively communicate in fluent,
Figure 2. Map of relevant human brain regions mentioned, including the prefrontal area, Broca’s andWernicke’s areas, and the primary motor cortex. Retrieved October 13, 2008, from Review of the Universe,
www.universe-review.ca
Copyright # 2009 John Wiley & Sons, Ltd. Behav. Sci. Law 27: 261–272 (2009)
DOI: 10.1002/bsl
Brain lesions and criminality 265

grammatical sentences although they can understand what is being said and transmit
halting speech that has content. Conversely, the destruction of Wernicke’s area
results in a completely different type of deficit—a person can no longer understand
or meaningfully use language, and while the person can produce copious speech, it is
‘‘word salad,’’ a perfectly grammatical jumble of nonsense. These specific deficits
illustrate how the loss of a particular brain region due to injury can result in
substantial changes in behavioral output, of which the neurologically damaged
person may or may not be aware. Equally, focal lesions have been described in
regions of the brain noted to be involved in components of intentional action,
regulation of emotion and aggression, self-control, and the ability to judge and act
morally. Some of the case studies and investigations involving the better-established
and most relevant lesions will be discussed, beginning with a case that has shaped the
field of neuroscience.
PREFRONTAL CORTEX: MORAL ACTIONAND SELF CONTROL
For hundreds of years before modern medicine, the frontal lobes had been
considered the seat of intelligence, individual personality, and decision-making—
but it was the published medical case of Phineas Gage that solidified the theory. On
September 13, 1848, railroad worker Phineas Gage suffered a devastating brain
injury when a three-and-a-half foot long tamping iron packed with gunpowder
blasted through the left side of his face, shattering his upper jaw and destroying his
left ventromedial frontal cortex (Figure 3). Despite this incredible injury, he was
coherent and conscious for the ride into town to see physicians Edward H. Williams
and John Martyn Harlow, who marveled that their patient had survived seemingly
Figure 3. Rendered computer generated image (CGI), using a standard human skull as reference,plotting how the tamping iron entered Gage’s skull at a diagonal angle and destroyed a large part ofhis prefrontal cortex. Retrieved October 21, 2008, from National Institute of Neurological Disorders and
Stroke (NINDS) public domain website: www.ninds.nih.gov/health_and_medical/pubs/tbi.htm
Copyright # 2009 John Wiley & Sons, Ltd. Behav. Sci. Law 27: 261–272 (2009)
DOI: 10.1002/bsl
266 S. Batts

with faculties intact, and saw fit to publish articles about Gage’s injury and
subsequent recovery. Although Harlow’s initial report did not emphasize
psychological changes that occurred as a result of Gage’s injury, a later article in
1868 described the now-classic case of a severe personality disruption associated
with damage to the prefrontal cortex (Harlow, 1848, 1868). Harlow contrasted a
hard-working, polite, and well liked Gage prior to the injury, with a Gage now:
. . .fitful, irreverent, indulging at times in the grossest profanity (which was notpreviously his custom), manifesting but little deference for his fellows, impatient ofrestraint or advice when it conflicts with his desires, at times pertinaciously obstinate, yetcapricious and vacillating, devising many plans of future operations which are no soonerarranged than they are abandoned. . . A child in his intellectual capacity andmanifestations, he has the animal passions of a strong man (Macmillan, 2000, p. 52).
Harlow’s account was further embellished over the years by others in the popular
and medical press, until by the early 20th century the long-dead Gage came to
represent a Dr. Jeckyll/Mr. Hyde persona whose every fault could be attributed to his
amazing injury (Macmillan, 2000). However, it is now accepted that, while the exact
extent of personality change due to Gage’s lesion cannot be quantified, some real
qualitative, negative change in Gage’s ability to make moral decisions did occur
following the damage—mirroring other modern cases of prefrontal damage. And
beneath the tall tales and fish stories, a basic truth is embedded in Gage’s story that
has played a tremendous role in shaping modern neuroscience: that the brain is the
physical manifestation of the personality and sense of self, and that focal damage to
brain areas can results in focal changes in behavior and personality while leaving
other aspects of the self unchanged.
More than a century after Phineas Gage had died, the involvement of the
ventromedial frontal cortex in moral action was further explored by neuroscientist
Antonio Damasio in the case study of EVR, a 35 year old man whose left and right
orbital and lower mesial cortices (including the prefrontal area) were removed after the
diagnosis of a cancer called orbitofrontal meningioma (Eslinger & Damasio, 1985).
Prior to the cancer, EVR had been described as a paragon of morality, loved by his
friends, his wife, and his two children. Following his surgery to remove the cancerous
lesion in his brain, while his intelligence and memory remained unchanged, his ability to
act appropriately and morally had been dramatically compromised. A string of poor
decisions led to his financial ruin, the loss of his family and job, and a marriage to a
prostitute who he divorced six months later (Damasio, Tranel, & Damasio, 1990).
Interestingly, Damasio’s further work with EVR parsed out that, while his ability to
morally judge situations was not largely impaired, his ability to act effectively in
‘‘ethically charged’’ situations was now extremely poor (Bechara, Damasio, & Damasio,
2000). When removed from a situation, EVR could report what the proper moral
response would be in certain circumstances. However, when forced to perform, EVR
and similar patients chose actions that resulted in immediate gratification even when
they knew that the long-term outcome could be disastrous or objectively immoral.
The prefrontal cortex is known to provide essential neurological inhibition to
many cognitive processes, and several types of human mental illness, such as
schizophrenia, bipolar disorder, and ADHD, have abnormal patterns of activation in
the prefrontal cortex (Krawczyk, 2002). Recent brain imaging studies have also
found that reduced prefrontal volume, abnormal activity, and fewer interconnec-
tions from the frontal lobes to the rest of the brain are common in depressed people
Copyright # 2009 John Wiley & Sons, Ltd. Behav. Sci. Law 27: 261–272 (2009)
DOI: 10.1002/bsl
Brain lesions and criminality 267

(Ongur, Drevets, & Price, 1998), people who are under constant stress (Miner et al.,
2006), suicide victims (Rajkowska, 1997), incarcerated criminals (Yang et al.,
1999), sociopaths (Barkataki, Kumari, Das, Taylor, & Sharma, 2006), and female
cocaine users (Li, Kosten, & Sinha, 2006). Additionally, the prefrontal cortex
receives input from many sensory and non-sensory areas of the brain, and integrates
them into a unified informational set which informs choices and decisions. A severely
damaged prefrontal cortex would suggest that more cognitive processes, many of
which would normally be repressed or delayed, could translate into action despite a
person being aware that an action was wrong or unwise. Essentially, many types of
available information will never even enter the scope of the decision-making process.
These case studies and others suggest that the prefrontal cortex plays an important
role in self-control and the ability to effectively act morally, as well as in the delay of
immediate gratification in order to achieve a more rational or eventually more
rewarding long-term goal.
THE AMYGDALA: AGGRESSION, EMPATHYAND EMOTIONAL INTELLIGENCE
The amygdala is part of the limbic system, implicated in a variety of emotional and
motivational behaviors including aggression. In animals the amygdala also supports
perceptual vigilance—in humans, it may influence the likelihood that certain events
of affective importance reach awareness, segregating the neural representations of
the significant from the mundane. Neuroscientific studies also suggest that increased
stimulation of the amygdala can result in increased feelings of aggression and fear.
One famous historical instance of a brain lesion potentially contributing to
uncontrollable and unexplained violence is the case of a 25-year-old University of
Texas (UT) student, Charles Whitman (Lavergne, 1997). Whitman, an Eagle Scout
who joined the Marines, was an intelligent scholarship student at UT who began to
suffer from excruciating headaches, disturbing thoughts, and a compulsion for
writing. His behavior, once exemplary, changed drastically for the worse until he was
court-martialed, lost his scholarship, began hitting his wife, and noted an increasing
desire to ‘‘take a deer rifle and start shooting people’’—a fear that he related to a
campus psychologist along with the worry that something was wrong with him. In
1966, two weeks after that encounter with the psychologist, Whitman brutally killed
his wife and his mother, leaving notes expressing his bewilderment as to why he had
done it as well as how much he loved them. He then methodically shot and killed
14 people, wounding 31 others, while holed up with a small arsenal atop a 32-story
UT campus building. Whitman was killed by Austin police, and a subsequent
autopsy (which he requested in his suicide note, to determine if anything could
explain the disturbing thoughts and severe headaches he had developed) revealed
something surprising: he had a glioblastoma brain tumor the size of a walnut in the
hypothalamus region of his brain. The tumor was impacting the hypothalamus and
compressing his amygdala, hypothetically causing over-stimulation, although even
after autopsy experts were not in agreement that the lesion changed his behavior. At
that time there were no imaging analyses available that could have detected the
presence of the tumor when Whitman was alive.
As over-stimulation of the amygdala may result in uncontrollable, violent
emotions, lesions of the amygdala that impair its function result in a person with flat
Copyright # 2009 John Wiley & Sons, Ltd. Behav. Sci. Law 27: 261–272 (2009)
DOI: 10.1002/bsl
268 S. Batts
affect unable to assign the proper emotional response or meaning to memories and
actions (Volavka, 2002[SH1]). This may be relvant to NGRI or as a mitigating factor
at sentencing, since a person’s behavior might not follow from a proper emotional
response—such as being unaware that someone is in severe distress, or over-reacting
with extreme violence in response to a minor insult. Patients with amygdala lesions
exhibit normal subjective and psychophysiological responses to aversive word types
(i.e. galvanic skin response) but do not show the normal retention advantage
associated with these words (Anderson & Phelps, 2001). Damage to the human
amygdala impairs the initial perception of stimuli which have emotional significance,
suggesting that identifying emotional events is problematic for these people
(Anderson & Phelps, 2001). Normally, the amygdala enhances the perception and
memory consolidation of stimuli that have a strong emotional link (for example, the
birth of one’s child or a scene where one witnessed a murder), due to its role as neural
mediator between the limbic system and brain structures involved in memory
processing. The amygdala is also found to be activated when someone is exposed to a
linguistic threat (Isenberg et al., 1999). A patient (S.P.) with a bilateral amygdala
lesion was found to have no enhanced perception for aversive stimulus events or
emotionally charged words, where normal controls both remembered and reacted
strongly to items with emotional content (Anderson & Phelps, 2001). However, the
left amygdala seems particular important—an examination of patients with either a
left or right amygdala lesion shows that the enhanced perception of aversive words is
specifically related to the left amygdala, and fMRI confirmed that the left amygdala is
activated with the presentation of emotional, linguistic stimuli. The amygdala is also
divided into several regions with different functions, and lesions of particular areas
may result in different deficits. For example, whereas the lateral amygdala exerts
excitatory influences on the hypothalamus, the medial amygdala exerts inhibitory
influences. This means that the amygdala can exert direct excitatory/inhibitory
influence on hunger, thirst, sexual arousal, rage as well as hormonal, endocrine, and
other functions associated with the hypothalamic nucleus (Dreifuss & Murphy,
1968; Gloor, 1975; Joseph, 1992).
As these scientific and case studies illustrate, there exist many types of organic
brain lesion that can have drastic and direct effects on judgment, aggression, and
self-control. The observations from these case studies hold up when very large
numbers of subjects are included, as illustrated in a longitudinal study of 279
Vietnam War veterans who experienced frontal lobe lesions (Grafman et al., 1996).
Subjects who had frontal lobe lesions in the ventromedial area demonstrated
measures of violence and aggression that were significantly higher than those of
controls, suggesting that this type of lesion increases the risk for aggression and
violence. The presence and severity of such lesions, as judged by medical experts,
could provide additional information as to the causes of mental defects, although the
proper way to wield this information remains to be worked out.
THE ROLES OF NEUROIMAGING DATAIN THE COURTROOM
Although there are many discretely-functioning parts of the brain, the brain is also
known for its redundancy of function (i.e., more than one area of the brain may be
involved in a behavior), its interconnectivity between areas, and its plasticity.
Copyright # 2009 John Wiley & Sons, Ltd. Behav. Sci. Law 27: 261–272 (2009)
DOI: 10.1002/bsl
Brain lesions and criminality 269
Essentially, while brain injury or lesions may impair decision-making or influence
violent tendencies, there is no one ‘‘moral’’ region of the brain. As the case of Phineas
Gage shows, it is possible to suffer an extremely traumatic frontal lobe brain injury—
even one that results in drastic personality changes—and still refrain from engaging
in anything inherently criminal or violent. We must resist the urge to be entirely
deterministic. While neuroscience has contributed a vast amount to understanding
of the brain, there is still no consensus as to what constitutes normal variation in the
size of regions, whether a lesion actually indicates that a region of the brain is
impaired, and whether impairment of a particular region provides a direct link to
behavior. Currently, the best neuroscience has to offer may be the bolstering of an
already established case for mental defect—to provide another piece of the puzzle
rather than stand alone evidence.
Additionally, neuroimaging evidence might provide insight for parole hearings,
especially if a tumor or lesion that had been argued to be affecting behavior had been
surgically removed. If the behavior had been judged to be improved, the chance of re-
offending might be low. This observation is reflected in the case of a 40 year old man
who experienced sudden and uncontrollable pedophilia which was later thought to
be caused by an egg-sized tumor in the orbitofrontal cortex (Burns & Swerdlow,
2003). After the tumor was successfully removed, the urges disappeared and he
successfully completed a therapy program. When the tumor began to re-grow, the
behavior once again returned, and when the tumor was again removed, so did the
urges. Consistent with other reports of prefrontal damage, the man knew that the
urges and behavior was morally wrong, yet he was still unable to stop himself. This
leads to another question: should people who are biologically unable to control their
behavior, or predisposed to anti-social behavior, be released from custody if the
behavior can return as a result of the disorder? Surgical interventions, such as
orchidectomy, could conceivably be considered as factors for determining parole and
sentence length. However the Texas orchidectomy law attempts to dissociate
castration from legal consequences in order to preserve the voluntary nature of
offenders’ decisions to undergo the procedure (Voluntary Castration for Sex
Offenders, 2007). Neurological follow-up visits could become mandatory for
offenders who suffered from a lesion that could recur.
It is important that the integration of neuroimaging evidence into legal
proceedings occur in a way that is scientific, logical, and free of bias. The alternative
could be a legal system overwhelmed with criminal defense lawyers attempting to
rationalize away any crime as the result of neurological disease, and juries
overwhelmed by the vividness and ‘‘scientific’’ nature of such data. Recent research
suggests that presenting neuroimaging evidence at trial may sway juries’ beliefs about
a defendant’s culpability. In one study, ‘‘mock jurors’’ were asked to render a verdict
in staged insanity trials where various types of evidence, including neuroimaging
evidence such as MRI data, was presented. The jurors were more likely to find the
defendant not guilty by reason of insanity if the defendant had a history of brain
injury, had been diagnosed with a psychotic disorder, or could prove the existence of
a brain lesion via MRI. Furthermore, the jurors who stated that the neuroimaging
data had influenced them were nearly six times as likely to render a not guilty verdict
(Gurley & Marcus, 2008). This is illustrated in the previously mentioned 1989 trial
of Barry Wayne McNamara, whose sentencing of life in prison (as opposed to the
death penalty) was handed down due to mitigation from mental illness (Emmons,
Copyright # 2009 John Wiley & Sons, Ltd. Behav. Sci. Law 27: 261–272 (2009)
DOI: 10.1002/bsl
270 S. Batts

1989). Following the hearing, jurors acknowledged that the neuroimaging visual aids
were given considerable credence in mitigating the sentence. How is the average jury,
comprised of laypeople not well versed in neurological deficits, supposed to judge a
normal, functioning brain from a damaged, abnormal one? Even expert
neuroscientists may be unable to testify that, with reasonable medical certainty, a
brain lesion caused a defendant’s behavior at the time a crime was committed.
However, between 60 and 77% of all defendants found not guilty by reason of
insanity are diagnosed with a psychosis, and at least 10% of these individuals have a
diagnosis of neurologically based psychosis (Cochrane, Grisso, & Frederick, 2001;
Warren et al., 2006). This suggests that, while neuroimaging evidence might
currently pose unfair bias in some criminal trials, the evidence is certainly relevant to
many cases and should not be excluded wholesale. Mediating how and when to
introduce such evidence will require that judges, and likely juries, become educated
to some degree about the relevant neurological disorders that may impact
responsibility or contribute to legal insanity. It is not difficult to foresee a future
where law schools teach relevant areas of neuroscience, creating a new type of
‘‘neurolaw’’ expert capable of bridging this gap. Clinical neuroscientists interested in
how neuroimaging impacts the law might empirically explain how many people who
have high-risk lesions do not exhibit criminality. Of particular importance for the
medical community is the determination of what constitutes the legally significant
threshold for structural damage to a brain structure and the extent of behavioral
impairment required for mitigation or NGRI to be justified. Ideally, neuroimaging
information could be integrated into the milieu of evidence about defendants’ mental
functioning, and, along with psychiatric and neuropsychological testing, provide a
more complete picture without eclipsing the other facts in the case.
REFERENCES
Anderson, A. K., & Phelps, E. A. (2001). Lesions of the human amygdala impair enhanced perception ofemotionally salient events. Nature, 411(6835), 305–309.
Barkataki, I., Kumari, V., Das, M., Taylor, P., & Sharma, T. (2006). Volumetric structural brainabnormalities in men with schizophrenia or antisocial personality disorder. Behavioural Brain Research,169(2), 239–247.
Bechara, A., Damasio, H., & Damasio, A. (2000). Emotion, decision making and the orbitofrontal cortex.Cerebral Cortex, 10, 295–307.
Burns, J., & Swerdlow, R. (2003). Right orbitofrontal tumor with pedophilia symptom and constructionalapraxia sign. Archives of Neurology, 60, 437–440.
Chandrasekaran, R., & Miller, B. (1994 , March 8). Aramony’s defense strategy called creative but risky.Washington Post.
Cochrane, R., Grisso, T., & Frederick, R. (2001). The relationship between criminal charges, diagnoses,and psycholegal opinions among federal pretrial defendants. Behavioral Sciences and the Law, 19(4),565–582.
Dalby, J. (2006). The case of Daniel McNaughton: Let’s get the story straight.American Journal of ForensicPsychiatry, 27, 17–32.
Damasio, A., Tranel, D., & Damasio, H. (1990). Individuals with sociopathic behavior caused by frontaldamage fail to respond autonomically to social stimuli. Behavioral Brain Research, 41, 81–89.
Dreifuss, J., & Murphy, J. (1968). Contrasting effects of two identified amygdaloid efferent pathways onsingle hypothalamic neurons. Journal of Neurophysiology, 31(2), 237.
Dumit, J. (1999). Objective brains, prejudicial images. Science in Context, 12, 173–201.Emmons, S. (1989 , July 14). Hunting for brain disorders attorneys turn to UCI scanner as defense tool.
L.A. Times.Eslinger, P., & Damasio, A. (1985). Severe disturbance of higher cognition after bilateral frontal lobe
ablation: Patient EVR. Neurology, 35, 1731–1741.
Copyright # 2009 John Wiley & Sons, Ltd. Behav. Sci. Law 27: 261–272 (2009)
DOI: 10.1002/bsl
Brain lesions and criminality 271

Gloor, P. (1975). Physiology of the limbic system. Advances in Neurology, 11, 27–55.Grafman, J., Schwab, K., Warden, D., Pridgen, A., Brown, H., & Salazar, A. (1996). Frontal lobe injuries,
violence, and aggression: A report of the Vietnam Head Injury Study. Neurology, 46, 1231.Gurley, J., & Marcus, D. (2008). The effects of neuroimaging and brain injury on insanity defenses.Behavioral Sciences and the Law, 26(1), 85–8597.
Harlow, J. (1848). Passage of an iron rod through the head. Boston Medical and Surgical Journal, 39, 389–393. (Republished in the Journal of Neuropsychiatry and Clinical Neuroscience, 11, 281–283.).
Harlow, J. (1868). Recovery from a passage of an iron bar through the head. Publications of theMassachusetts Medical Society, 2, 327–347.
Isenberg, N., Silbersweig, D., Engelien, A., Emmerich, S., Malavade, K., Beattie, B., Leon, A., & Stern,E. (1999). Linguistic threat activates the human amygdala. Proceedings of the National Academy ofSciences USA, 96(18), 10 456–10 459.
Joseph, R. (1992). The limbic system: Emotion, laterality, and unconscious mind. Psychoanalytic Review,79(3), 405–456.
Krawczyk, D. C. (2002). Contributions of the prefrontal cortex to the neural basis of human decisionmaking. Neuroscience and Biobehavioral Reviews, 26(6), 631–664.
Lavergne, G. (1997). A sniper in the tower: The Charles Whitman murders. Austin, TX: University of NorthTexas Press.
Li, C., Kosten, T., & Sinha, R. (2006). Antisocial personality and stress-induced brain activation incocaine-dependent patients. Neuroreport, 17(3), 243–247.
Loeber, R., Farrington, D., Stouthamer-Loeber, M., & Van Kammen, W. (1998). Antisocial behavior andmental health problems: Explanatory factors in childhood and adolescence. Mahwah, NJ: Erlbaum.
Macmillan, M. (2000). Restoring Phineas Gage: A 150th retrospective. Journal of the History of theNeurosciences, 9(1), 42–62.
Miner, L., Jedema, H., Moore, F., Blakely, R., Grace, A., & Sesack, S. (2006). Chronic stress increases theplasmalemmal distribution of the norepinephrine transporter and the coexpression of tyrosine hydroxyl-ase in norepinephrine axons in the prefrontal cortex. Journal of Neuroscience, 26(5), 1571–1578.
Morse, S. (2006). Brain overclaim syndrome and criminal responsibility: A diagnostic note. Ohio StateJournal of Criminal Law, 3, 397.
Ongur, D., Drevets, W., & Price, J. (1998). Glial reduction in the subgenual prefrontal cortex in mooddisorders. Proceedings of the National Academy of Sciences USA., 95(22), 13 290–213 295.
Rajkowska, G. (1997). Morphometric methods for studying the prefrontal cortex in suicide victims andpsychiatric patients. Annuls of the New York Academy of Sciences, 836, 253–268.
Rojas-Burke, J. (1993). PET scans advance as tool in insanity defense. The Journal of Nuclear Medicine,34(1), 13–26.
Roper v. Simmons, 543 U.S. 551 (2005).Rosen, J. (2007 , March 11). The brain on the stand. The New York Times. Retrieved July 20, 2008, from
http://www.nytimes.com/2007/03/11/magazine/11Neurolaw.t.html.Snead, O. (2007). Neuroimaging and the ‘‘complexity’’ of capital punishment. Notre Dame Legal Paper No.
07-03. 1265–1339.Taylor, S. Jr., (1982 , June 2). Cat scans said to show shrunken Hinckley brain. The New York Times.United States v. Mezvinsky. 206 F.Supp.2d 661 (E.D.Pa. 2002).Volavka, J. (2002). Neurobiology of Violence. New York: American Psychiatric Publishing, Inc.Voluntary Castration for Sex Offenders. S. 123, 75th Leg. (Texas 2007).Warren, J., Murrie, D., Steskal, W., Colwell, L., Morris, J., Chauhan, P., & Dietz, P. (2006). Opinion
formation in evaluating the adjudicative competence and restorability of criminal defendants: A reviewof 8,000 evaluations. Behavioral Sciences and the Law, 24(2), 113–132.
Yang, Y., Raine, A., Lencz, T., Bihrle, S., LaCasse, L., & Colletti, P. (2005). Volume reduction inprefrontal gray matter in unsuccessful criminal psychopaths. Biological Psychiatry, 57(10), 1103–1108.
Copyright # 2009 John Wiley & Sons, Ltd. Behav. Sci. Law 27: 261–272 (2009)
DOI: 10.1002/bsl
272 S. Batts
